Rito Mitra Welsh April - NHS Wales - NOACs in Wales.pdf · 5.0% 10.0% Stroke Admission with AF 0.0%...
72
NOACs in Wales Rito Mitra Welsh Cardiovascular Society April 2015
Transcript of Rito Mitra Welsh April - NHS Wales - NOACs in Wales.pdf · 5.0% 10.0% Stroke Admission with AF 0.0%...

NOACs in Wales
Rito MitraWelsh Cardiovascular Society April 2015
DisclosuresDisclosures
• Speaker & conference fees from thefees from the following:A Z Pfi B h i• A‐Z, Pfizer, Boehringer, Menarini, Bayer, Lilly, S i B tServier, Boston Scientific, Biosensors
I'm not here to talk aboutI m not here to talk about …..
• Trial data• Efficacy• Efficacy• Side effects 'Although cost is a perceived
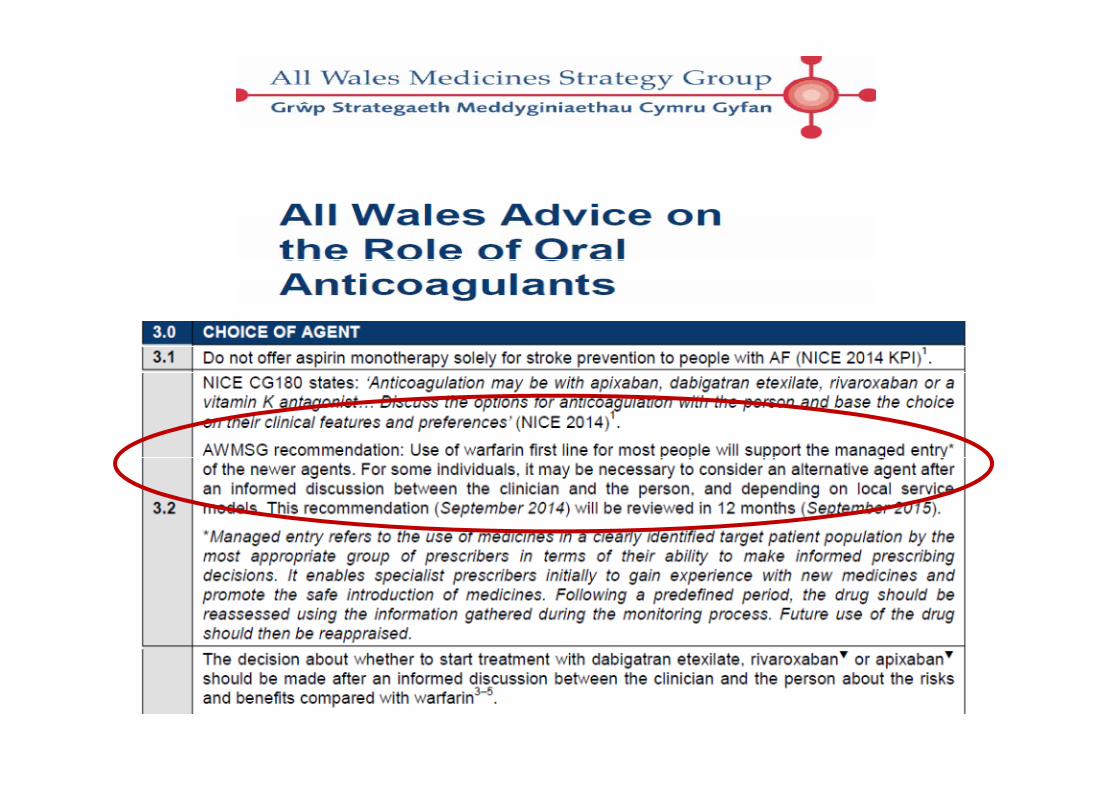
NICE ratified
• Drug interactions• Cost effectiveness
g pbarrier to the use of NOACs, NICE has concluded that the drugs are cost-effective and must be Cost effectiveness available to patients within their licensed indications'.
• Literature readily available
In WalesIn Wales ……..
• How good are we at stroke prevention in AF?• Who are prescribing NOACs in Wales?• How are they being prescribed?• How are they chosen? Should one size fit all?• How are they chosen? Should one size fit all?• Attacking AF prevalence: What happens when a Cardiologist is sent o t to a GP S rger ?Cardiologist is sent out to a GP Surgery?
• What are the Estimations and Projections?• Who should be prescribing NOACs in Wales?

Quality and Outcomes Framework 2015‐16 Future
• Biggest change for AF domain in QOF since 2011 has been the emphasis on anti‐coagulation treatment as opposed to treatment with anti‐coagulation or anti‐platelet. QOF 2015‐16 proposes to remove the use of anti‐platelets altogether.
Future
p g
http://www.nhsemployers.org/~/media/Employers/Documents/Primary%20care%20contracts/QOF/QOF%20Home%20Page/2015-16%20Summary%20of%20changes%20to%20QOF.pdf
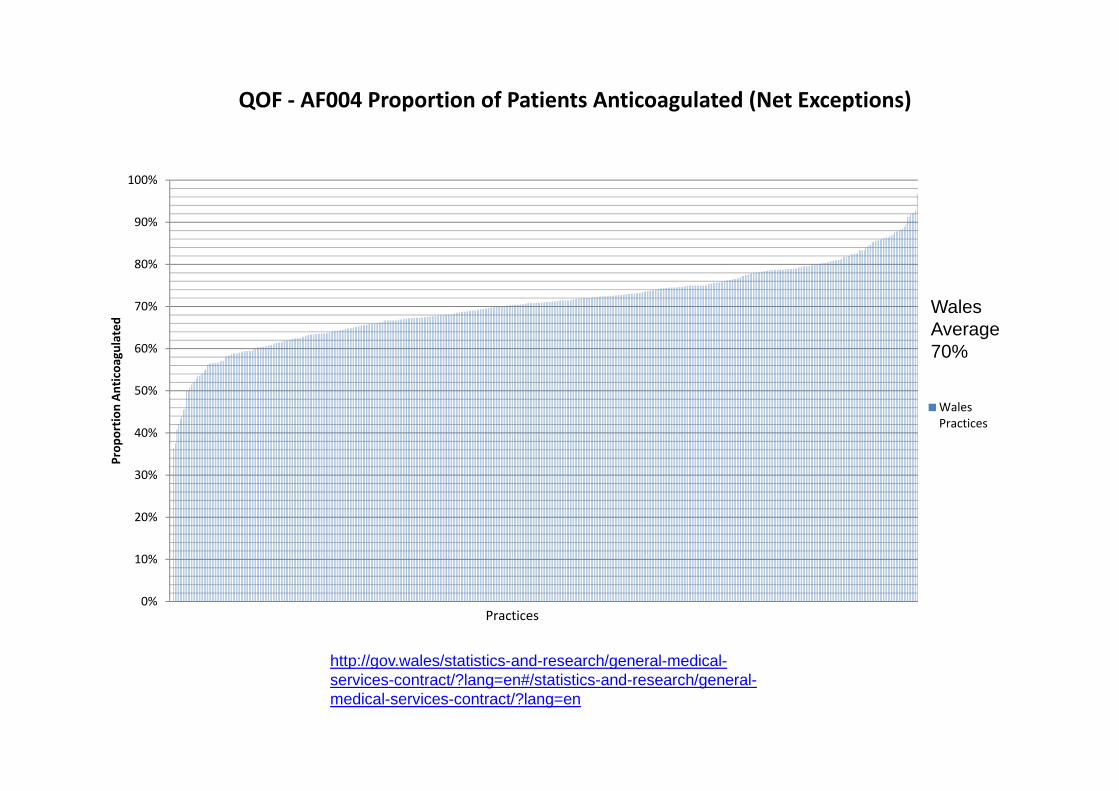
QOF ‐ AF004 Proportion of Patients Anticoagulated (Net Exceptions)
100%
70%
80%
90%
Wales
50%
60%
70%
Anticoa
gulated
Wales Average 70%
30%
40%
Prop
ortio
n A
Wales Practices
10%
20%
0%Practices
http://gov.wales/statistics-and-research/general-medical-http://gov.wales/statistics and research/general medicalservices-contract/?lang=en#/statistics-and-research/general-medical-services-contract/?lang=en

Sentinel Stroke National Audit Programme g(SSNAP)( )
https://www strokeaudit org/results/nationalhttps://www.strokeaudit.org/results/national
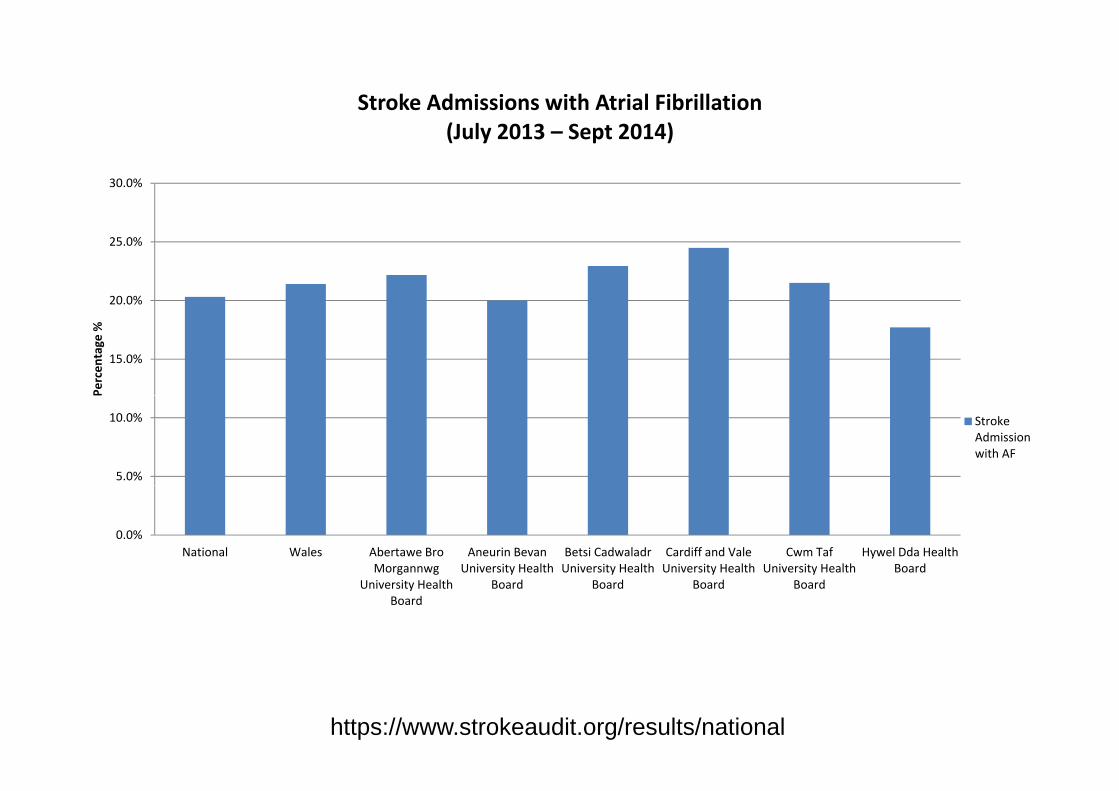
Stroke Admissions with Atrial Fibrillation(J l 2013 S t 2014)
30.0%
(July 2013 – Sept 2014)
20.0%
25.0%
15.0%
Percen
tage
%
5.0%
10.0% Stroke Admission with AF
0.0%National Wales Abertawe Bro
Morgannwg Aneurin Bevan
University Health Betsi Cadwaladr University Health
Cardiff and Vale University Health
Cwm Taf University Health
Hywel Dda Health Board
University Health Board
Board Board Board Board
https://www.strokeaudit.org/results/national
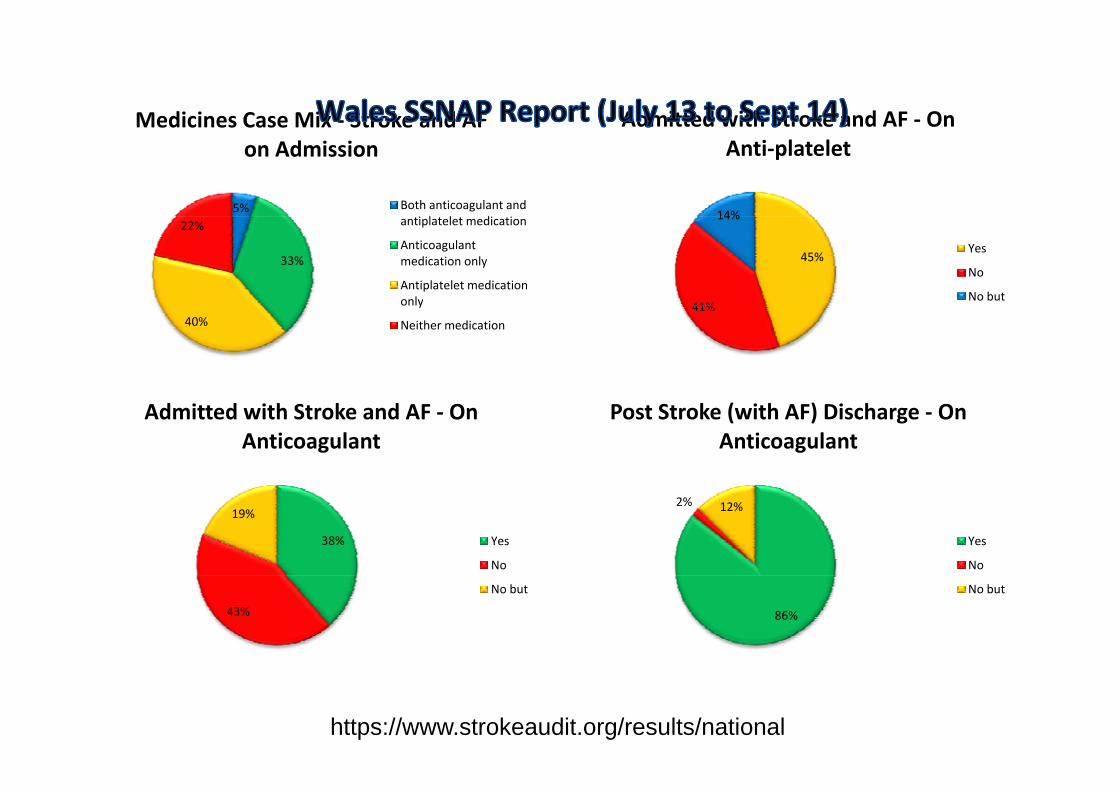
Admitted with Stroke and AF ‐ OnMedicines Case Mix ‐ Stroke and AF
14%
Admitted with Stroke and AF On Anti‐platelet
5%
Medicines Case Mix Stroke and AF on Admission
Both anticoagulant and
45%
41%
14%
Yes
No
No but
33%
22% antiplatelet medication
Anticoagulant medication only
Antiplatelet medication only 41%
40%y
Neither medication
Post Stroke (with AF) Discharge ‐ On Anticoagulant
Admitted with Stroke and AF ‐ On Anticoagulant
2% 12%
Yes
No
38%
19%
Yes
No
86%
No but
43%
No but
11https://www.strokeaudit.org/results/national
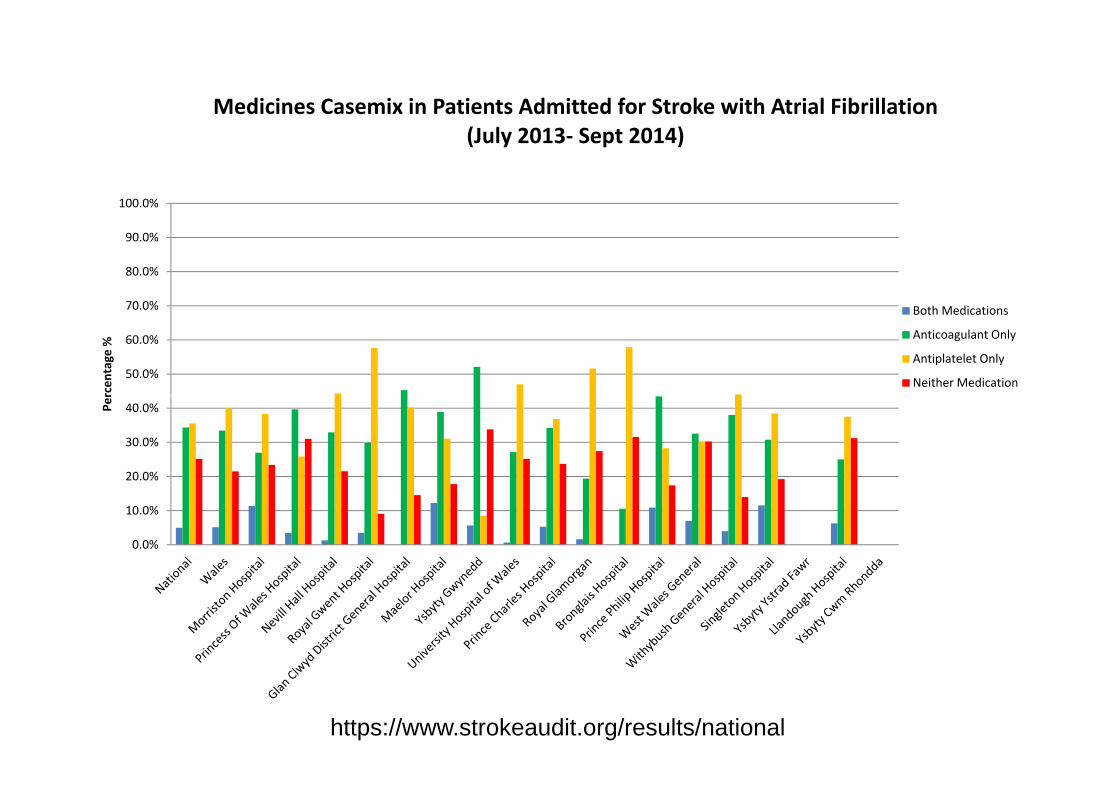
Medicines Casemix in Patients Admitted for Stroke with Atrial Fibrillation
100.0%
(July 2013‐ Sept 2014)
70 0%
80.0%
90.0%
h d
50.0%
60.0%
70.0%
rcen
tage
%
Both Medications
Anticoagulant Only
Antiplatelet Only
Neither Medication
20.0%
30.0%
40.0%Per
0.0%
10.0%
https://www.strokeaudit.org/results/national
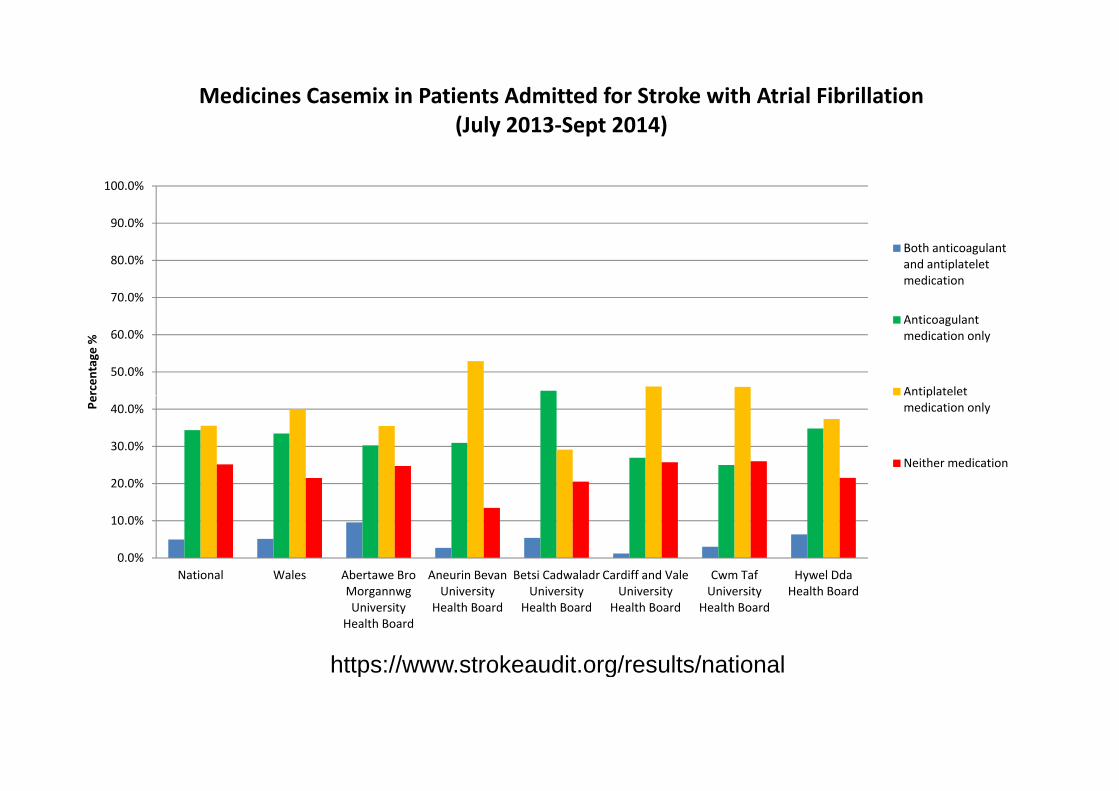
Medicines Casemix in Patients Admitted for Stroke with Atrial Fibrillation (July 2013‐Sept 2014)
100.0%
(July 2013‐Sept 2014)
70.0%
80.0%
90.0%
Both anticoagulant and antiplatelet medication
50.0%
60.0%
rcen
tage
%
Anticoagulant medication only
Antiplatelet
20 0%
30.0%
40.0%Pe
pmedication only
Neither medication
0.0%
10.0%
20.0%
National Wales Abertawe Bro Aneurin Bevan Betsi Cadwaladr Cardiff and Vale Cwm Taf Hywel DdaNational Wales Abertawe Bro Morgannwg University
Health Board
Aneurin Bevan University
Health Board
Betsi Cadwaladr University
Health Board
Cardiff and Vale University
Health Board
Cwm Taf University
Health Board
Hywel Dda Health Board
https://www strokeaudit org/results/nationalhttps://www.strokeaudit.org/results/national
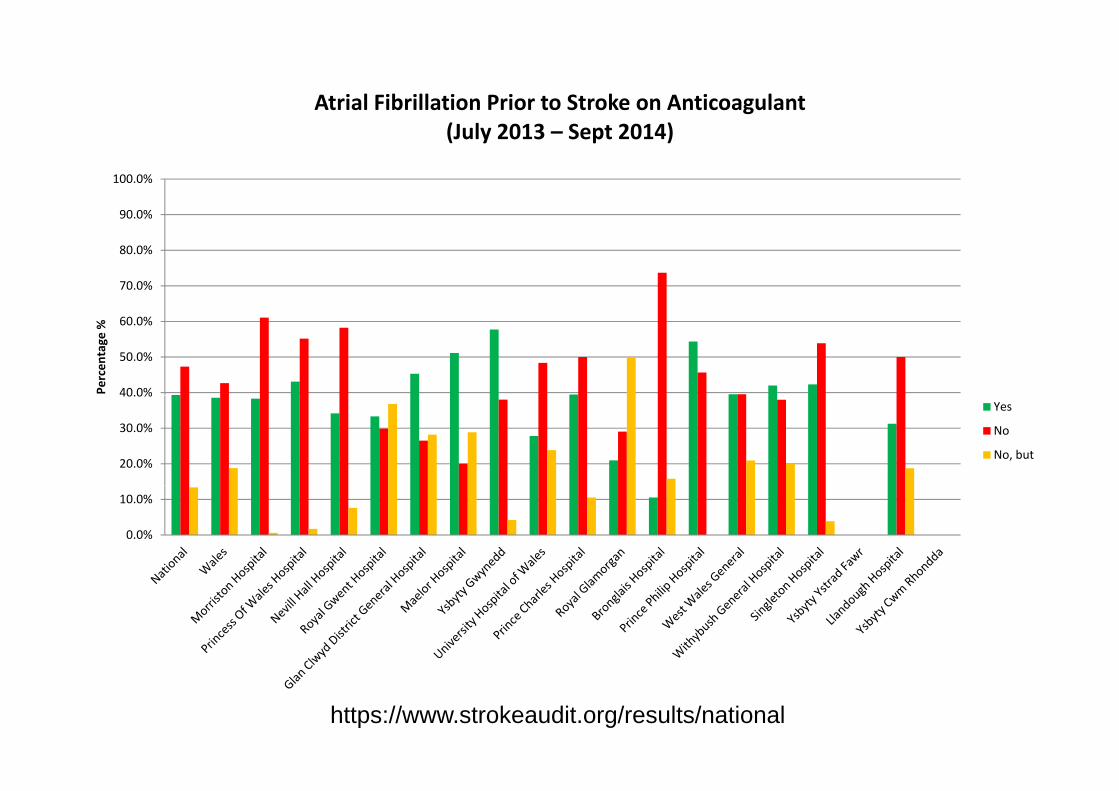
Atrial Fibrillation Prior to Stroke on Anticoagulant (J l 2013 S t 2014)
90 0%
100.0%
(July 2013 – Sept 2014)
70.0%
80.0%
90.0%
40.0%
50.0%
60.0%
Percen
tage
%
20.0%
30.0%
40.0%Yes
No
No, but
0.0%
10.0%
https://www.strokeaudit.org/results/national
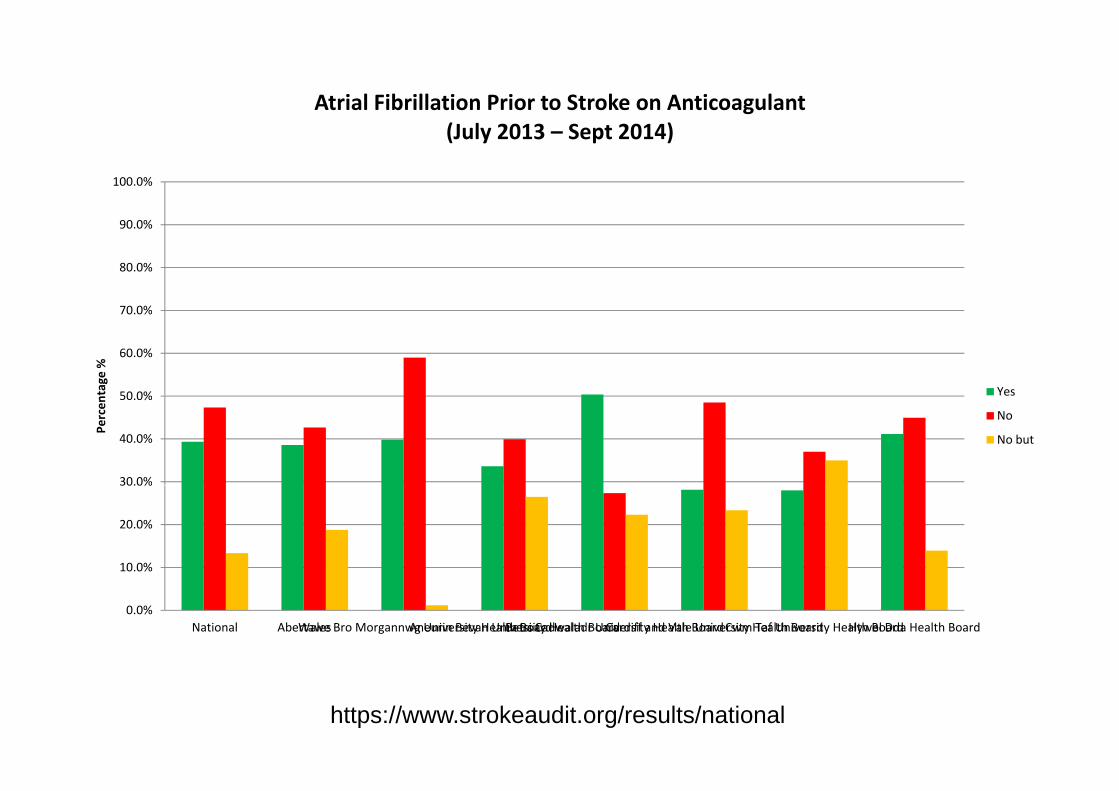
Atrial Fibrillation Prior to Stroke on Anticoagulant (J l 2013 S t 2014)
100.0%
(July 2013 – Sept 2014)
70 0%
80.0%
90.0%
50 0%
60.0%
70.0%
tage
%
Yes
30.0%
40.0%
50.0%
Percen
es
No
No but
10.0%
20.0%
30.0%
0.0%National WalesAbertawe Bro Morgannwg University Health BoardAneurin Bevan University Health BoardBetsi Cadwaladr University Health BoardCardiff and Vale University Health BoardCwm Taf University Health BoardHywel Dda Health Board
https://www.strokeaudit.org/results/national
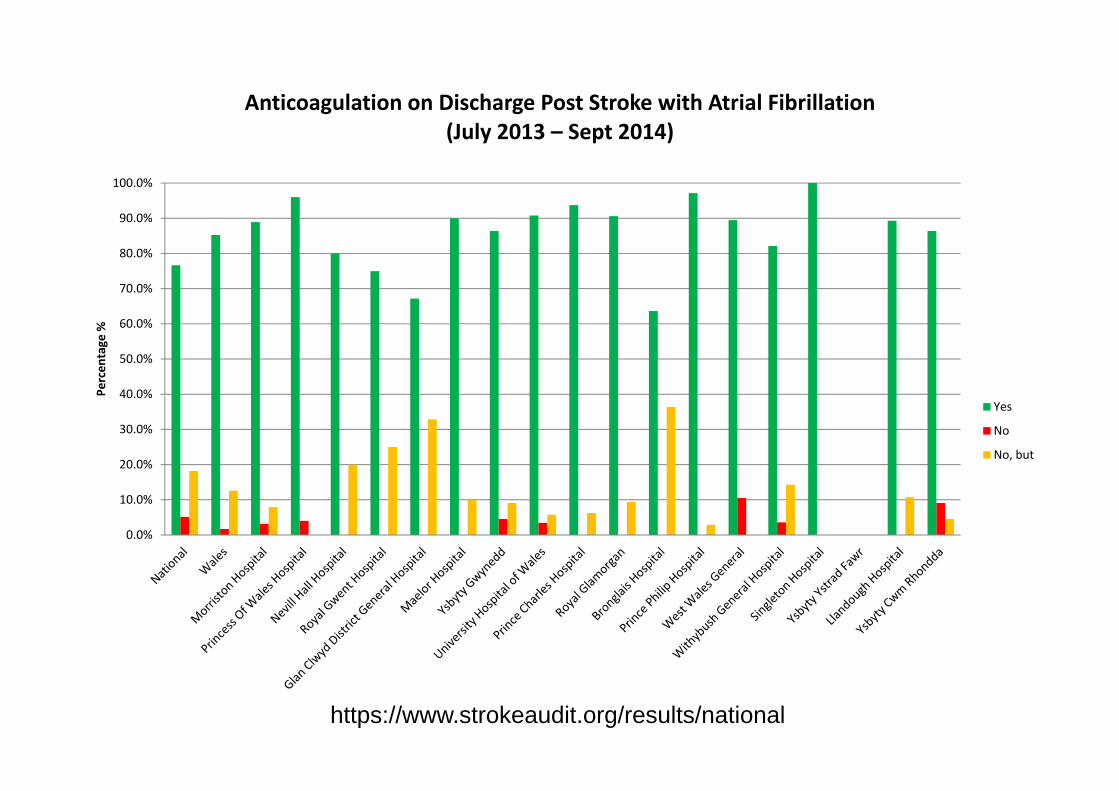
Anticoagulation on Discharge Post Stroke with Atrial Fibrillation (J l 2013 S t 2014)
90 0%
100.0%
(July 2013 – Sept 2014)
70.0%
80.0%
90.0%
40 0%
50.0%
60.0%
Percen
tage
%
20.0%
30.0%
40.0%Yes
No
No, but
0.0%
10.0%
https://www.strokeaudit.org/results/national
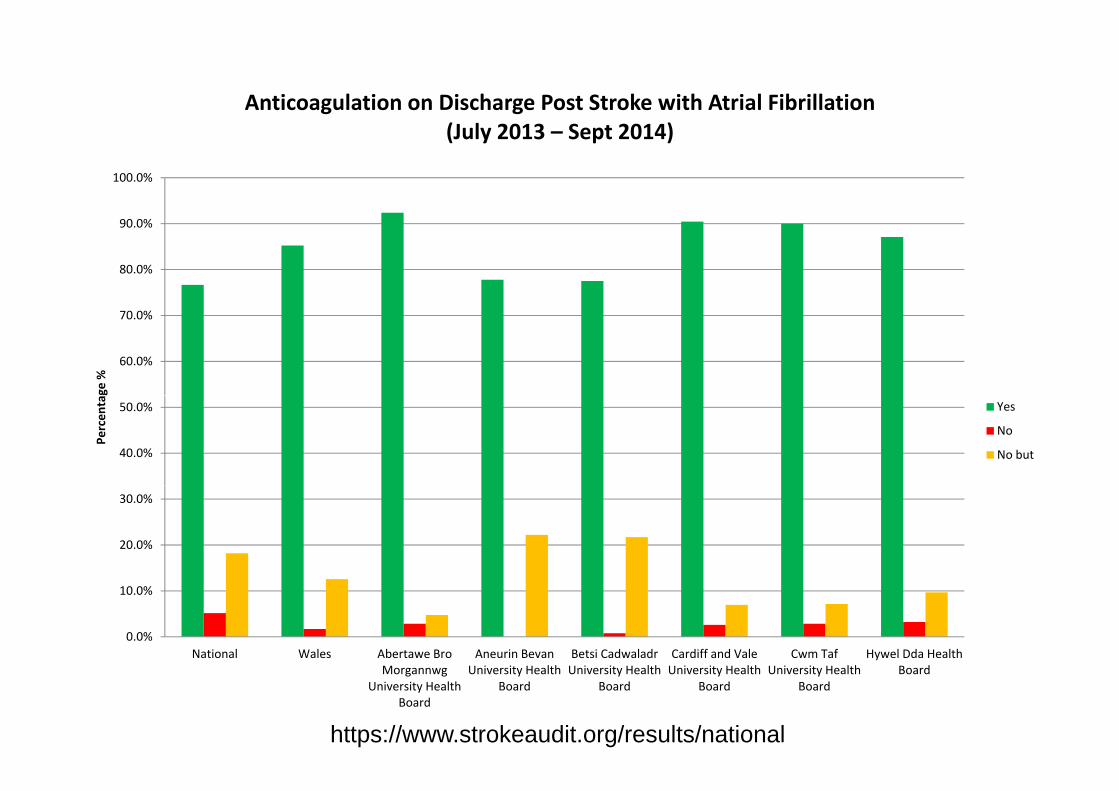
Anticoagulation on Discharge Post Stroke with Atrial Fibrillation(J l 2013 S t 2014)
100.0%
(July 2013 – Sept 2014)
80.0%
90.0%
60.0%
70.0%
ge %
40.0%
50.0%
Percen
ta Yes
No
No but
20.0%
30.0%
0.0%
10.0%
National Wales Abertawe Bro Aneurin Bevan Betsi Cadwaladr Cardiff and Vale Cwm Taf Hywel Dda Health Morgannwg
University Health Board
University Health Board
University Health Board
University Health Board
University Health Board
Board
https://www.strokeaudit.org/results/national
How good are we with SPAF in Wales?How good are we with SPAF in Wales?
• Pretty good once you’ve had a stroke.y g y
• Not so good for primary prevention• Not so good for primary prevention.
• Significant numbers on antiplatelets only.
Who are prescribing NOACs inWho are prescribing NOACs in Wales?
How are they being prescribed?
• Cwm Taf: Relatively large dataC&V D t i• C&V: Data emerging
• Other HBs: NA (at least for this presentation)
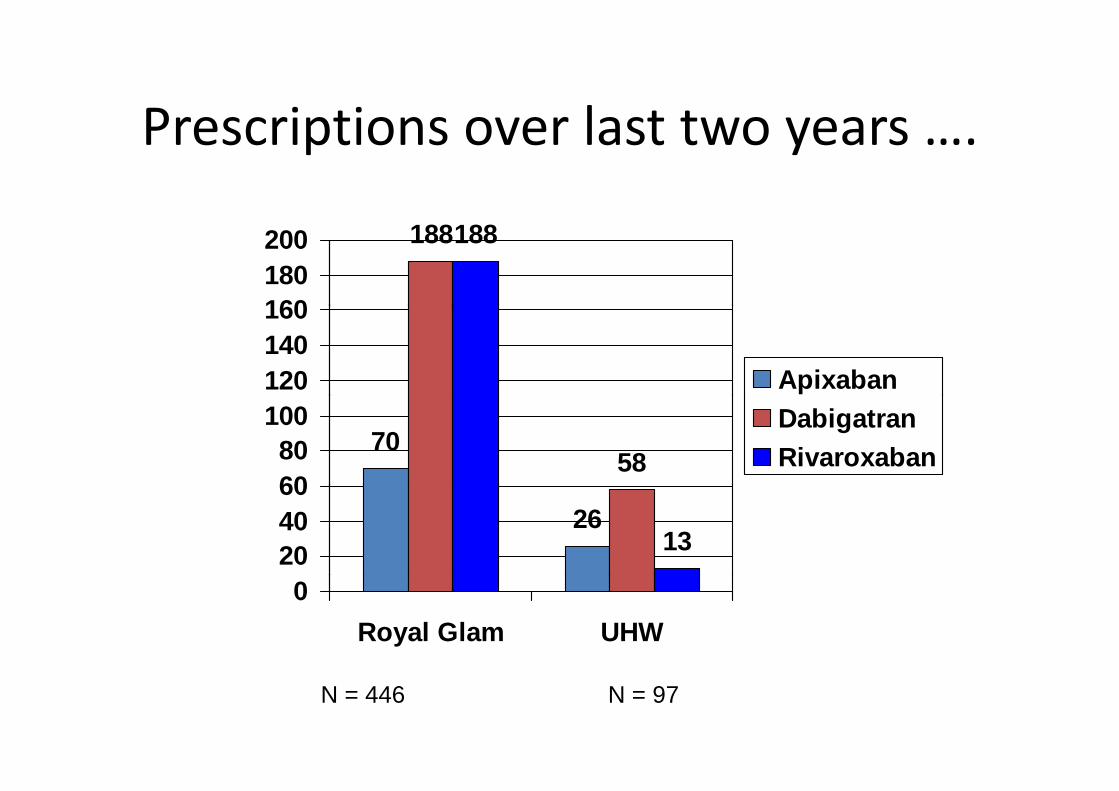
Prescriptions over last two yearsPrescriptions over last two years ….
188188
160180200
120140160
Apixaban
7058
6080
100 DabigatranRivaroxaban
261320
4060
0Royal Glam UHW
N = 446 N = 97
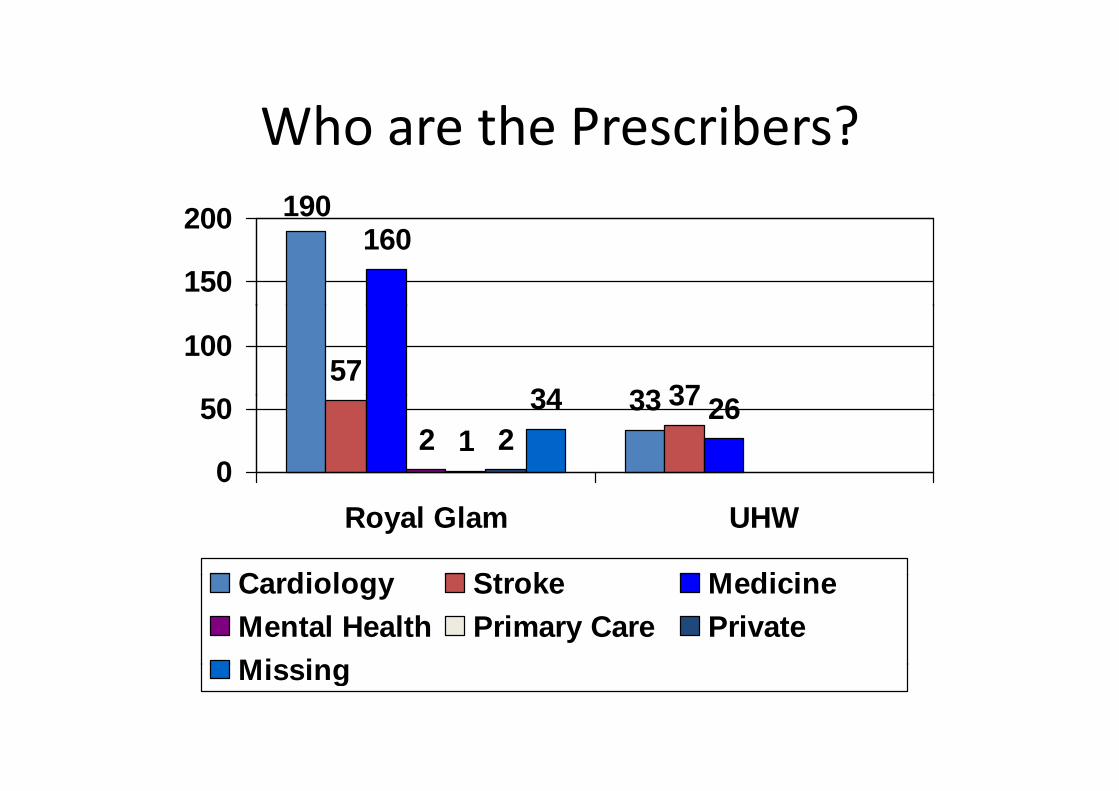
Who are the Prescribers?Who are the Prescribers?190200 190
160150
200
3357
3734
100
33 37 262 1 2
34
0
50
Royal Glam UHW
C di l St k M di iCardiology Stroke MedicineMental Health Primary Care PrivateMissingMissing
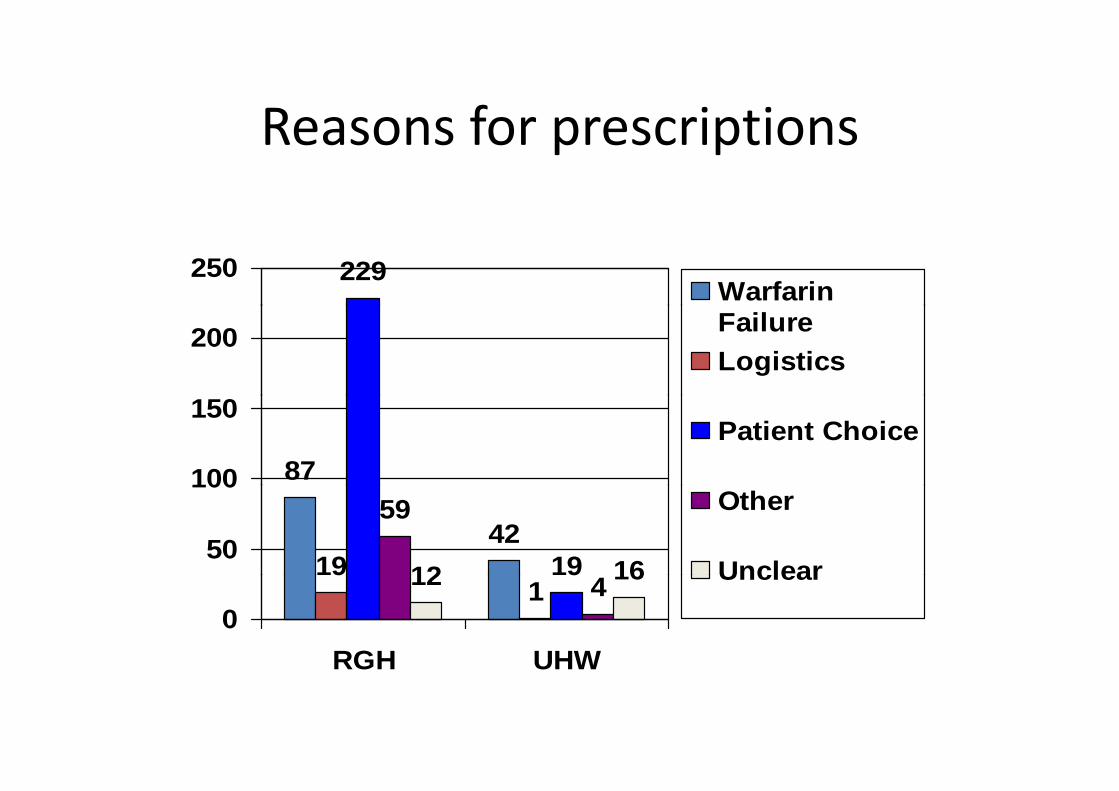
Reasons for prescriptionsReasons for prescriptions
229250Warfarin
200 FailureLogistics
87100
150Patient Choice
4219 19
59
12 1650
100Other
Unclear91
9412 16
0RGH UHW
Unclear
RGH UHW
NOAC use at Cwm Taf HB for SPAFNOAC use at Cwm Taf HB for SPAF
• Initiated in secondary carecare
• Maintained in primary (andprimary (and secondary) care
• Long term use –compliance and renal function/comorbidity
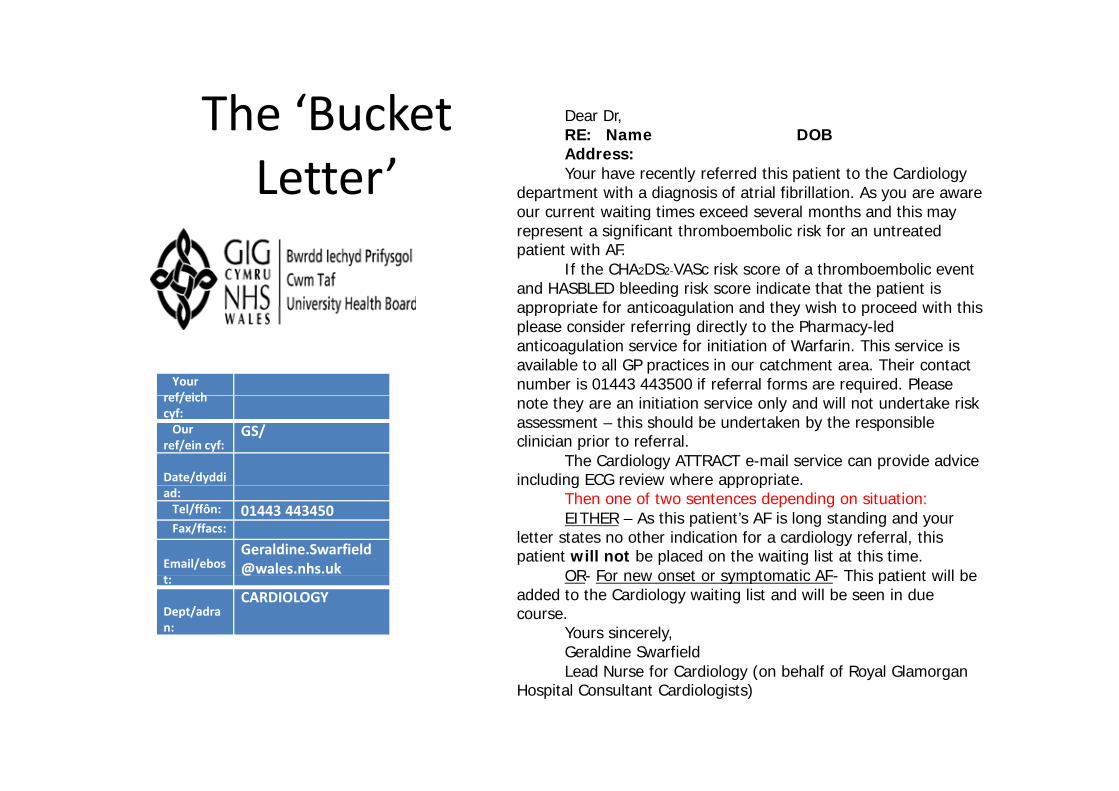
The ‘Bucket Dear Dr, The Bucket Letter’
RE: Name DOB Address: Your have recently referred this patient to the Cardiology
department with a diagnosis of atrial fibrillation. As you are aware our current waiting times exceed several months and this mayour current waiting times exceed several months and this may represent a significant thromboembolic risk for an untreated patient with AF.
If the CHA2DS2-VASc risk score of a thromboembolic event and HASBLED bleeding risk score indicate that the patient is appropriate for anticoagulation and they wish to proceed with this
Your ref/eich
appropriate for anticoagulation and they wish to proceed with this please consider referring directly to the Pharmacy-led anticoagulation service for initiation of Warfarin. This service is available to all GP practices in our catchment area. Their contact number is 01443 443500 if referral forms are required. Please
ref/eichcyf:Our
ref/ein cyf:GS/
Date/dyddi
note they are an initiation service only and will not undertake risk assessment – this should be undertaken by the responsible clinician prior to referral.
The Cardiology ATTRACT e-mail service can provide advice including ECG review where appropriate.
ad:Tel/ffôn: 01443 443450Fax/ffacs:
Email/[email protected]
g pp pThen one of two sentences depending on situation:EITHER – As this patient’s AF is long standing and your
letter states no other indication for a cardiology referral, this patient will not be placed on the waiting list at this time.
OR For new onset or symptomatic AF This patient will bet:@
Dept/adran:
CARDIOLOGYOR- For new onset or symptomatic AF- This patient will be
added to the Cardiology waiting list and will be seen in due course.
Yours sincerely,Geraldine Swarfield
d f C d l ( b h lf f l GlLead Nurse for Cardiology (on behalf of Royal Glamorgan Hospital Consultant Cardiologists)
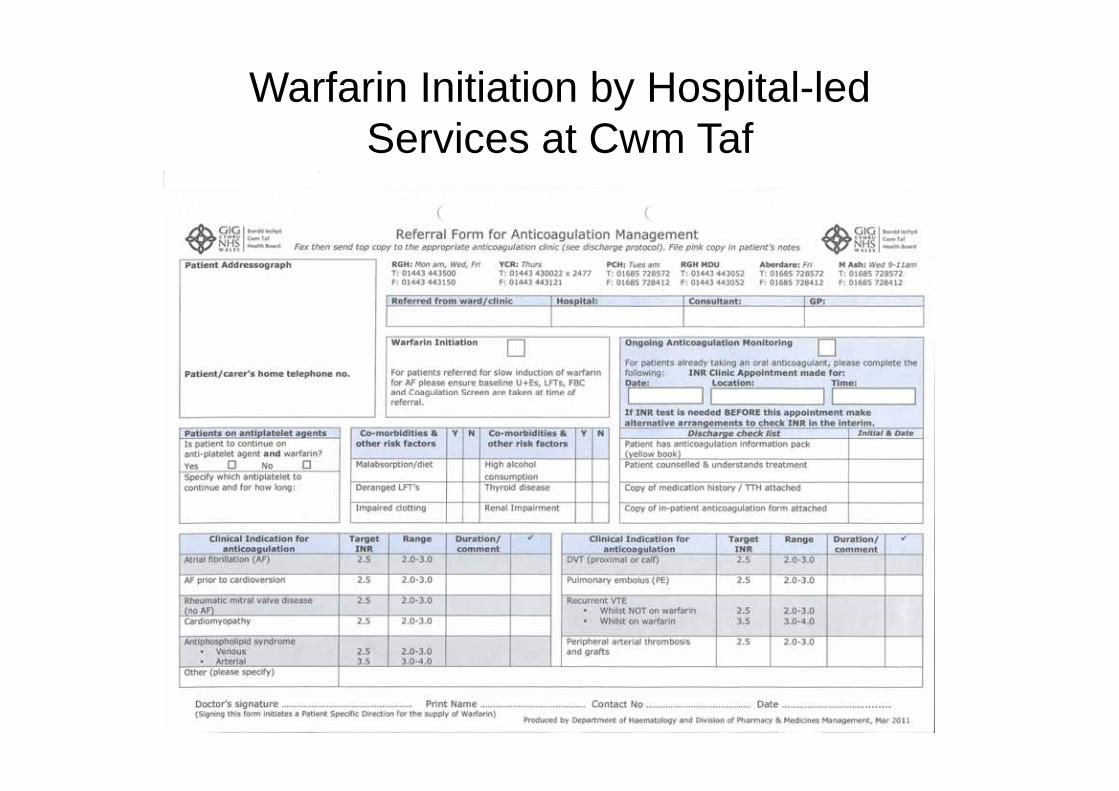
Warfarin Initiation by Hospital-led S i t C T fServices at Cwm Taf
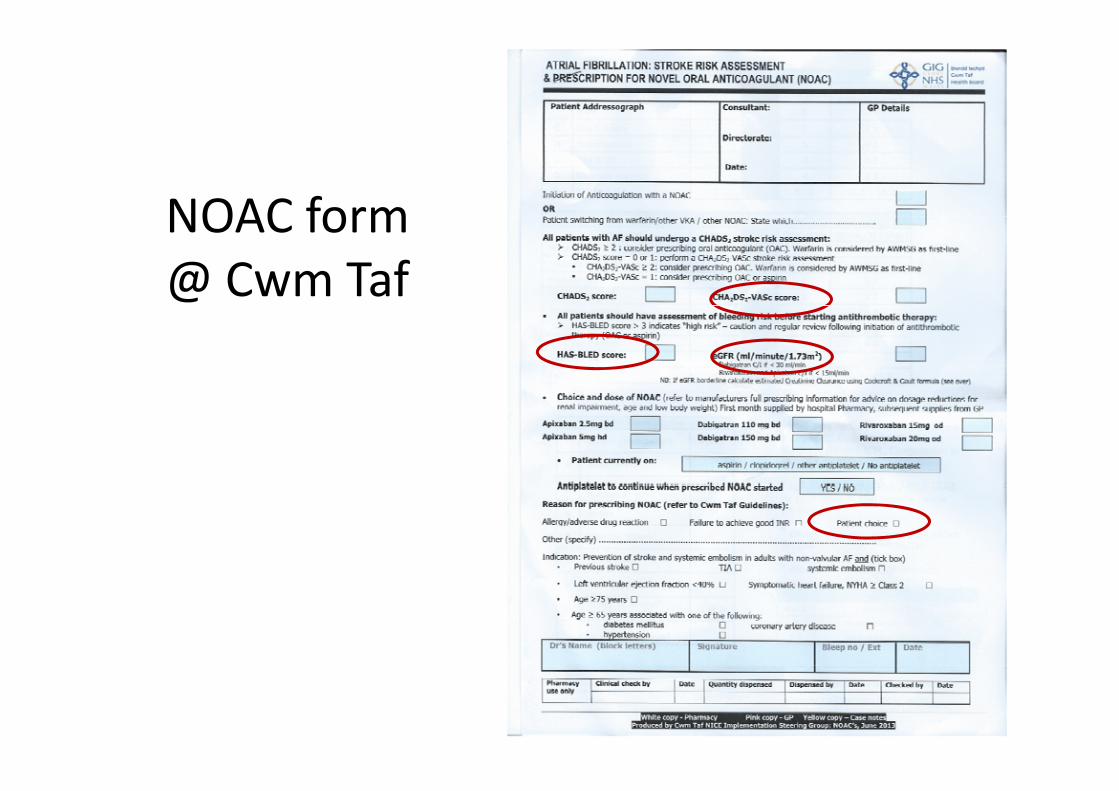
NOAC formNOAC form @ Cwm Taf
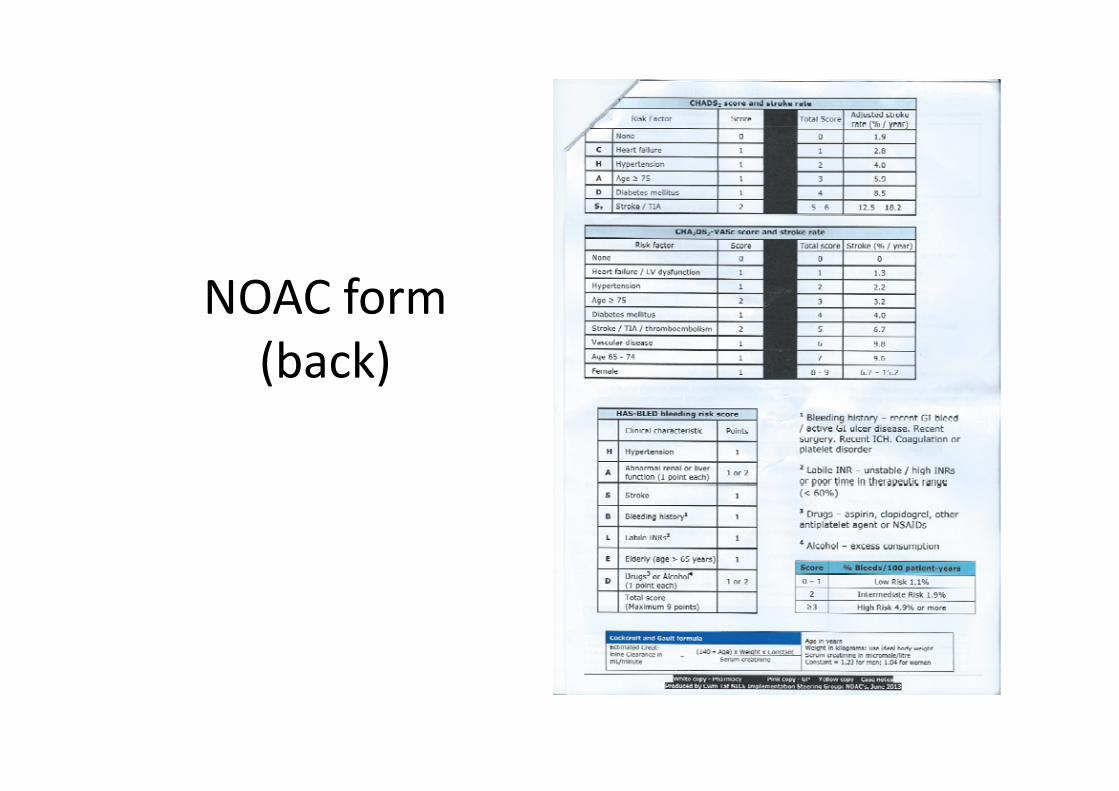
NOAC formNOAC form (back)
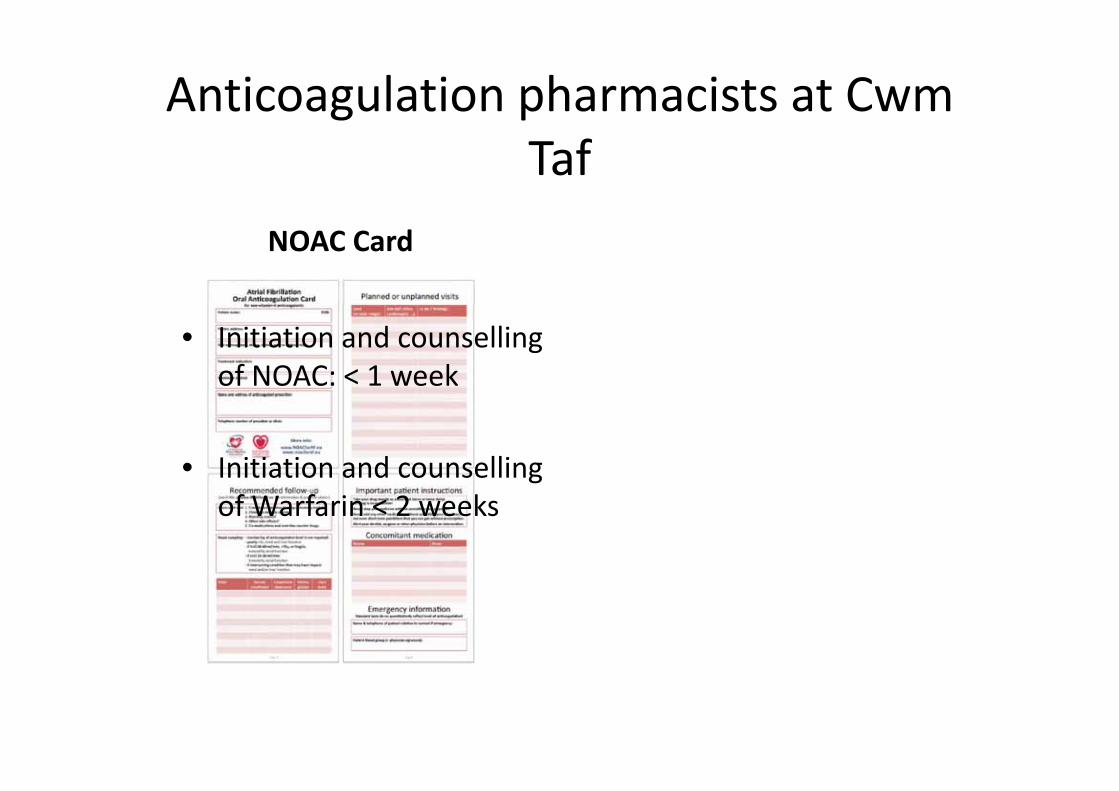
Anticoagulation pharmacists at Cwm Taf
NOAC Card
• Initiation and counselling of NOAC: < 1 week
• Initiation and counselling of Warfarin < 2 weeks

What is happening in other HBs?C&V
Th UHB B d t d th d ti f• The UHB Board supported the recommendations of the prioritisation panel, but the UHB cannot afford the full amount of all 3 recommendations. The Boardthe full amount of all 3 recommendations. The Board hasn’t yet signed off its financial framework for 2015‐16 and the amount that will be allocated to NICE d h t t b ti l t d Wh thiNICE drugs has not yet been stipulated. When this amount is clear Sharon and Graham will discuss apportionment across the 3 drug areas; we will letapportionment across the 3 drug areas; we will let you know as soon as we can.

What is happening in other HBs? Hywel Dda 1What is happening in other HBs? Hywel Dda 1• 1) Potential discrepancy between Local/All Wales guidance and NICE Guidance• I raise this in response to the email sent out a few months ago from Ceri BrownI raise this in response to the email sent out a few months ago from Ceri Brown
highlighting the case from Kent where a court found against a local commissioning group on the basis that local guidance could not override the recommendations of NICE and there was a duty of care to deliver guidance as per NICE recommendation.
• If I interpret correctly our current Health Board Guidance mandates the use of warfarin as a first line anticoagulant limiting NOACS as first line only in specificwarfarin as a first line anticoagulant‐limiting NOACS as first line only in specific situations
• If a patient is offered anticoagulation but chooses a NOAC rather than warfarin (as many well informed pts do)‐then if we say no then we could potentially be open to litigation if that pt goes on to have a stroke.
• 2) How can we deliver antiocoagulation services to patients with AF (including NOACS)
• Current HB guidance suggests that GP’s cannot initiate NOAC’s and yet there is no capacity/provision in secondary care to deliver the counselling and administrationcapacity/provision in secondary care to deliver the counselling and administration necessary. Cardiology and haematology clinics are already struggling with long waits.
• I propose one of 2 options• 1) Develop a nurse led AF service (across the 3 counties) that incorporate
anticoagulation as part of the service (This is done in many areas in the UK)anticoagulation as part of the service (This is done in many areas in the UK)• 2) Allow initiation in primary and as per NICE recommendation‐encourage local GP
‘champions’‐recognising that not all GP’s can experts in anticoagulation. This could be supported by a training day covering issues of AF, anticoagulation and specific issues relating to the NOACS and appropriate counselling. Those wishing (perhaps I am being over optimistic!) to become champions could be ‘signed off as to having theover optimistic!) to become champions could be signed off as to having the appropriate training and knowledge.

What is happening in other HBs?Hywel Dda 2
• We do not have a policy other than the NICE guidance and AWMSG. We tend to use both to be honest and when we do elect to use a NOAC we arrange counselling with either the cardiac nursearrange counselling with either the cardiac nurse or clinical pharmacist. I choose the agent based on age, renal function, stroke risk and compliance likelihood.likelihood.
• The delay is in getting the counselling underway, this is just one of the reasons that warfarin remainsthis is just one of the reasons that warfarin remains first line as we can arrange anticoagulation on the day of clinic. We are working on streamlining the NOAC patients to prevent delays. We have a form th t f lli th t i i d b ththat we use for counselling that is signed by the patient and nurse at the end of the session and we have a compliance form we ask the patient to sign prior to cardioversionprior to cardioversion.

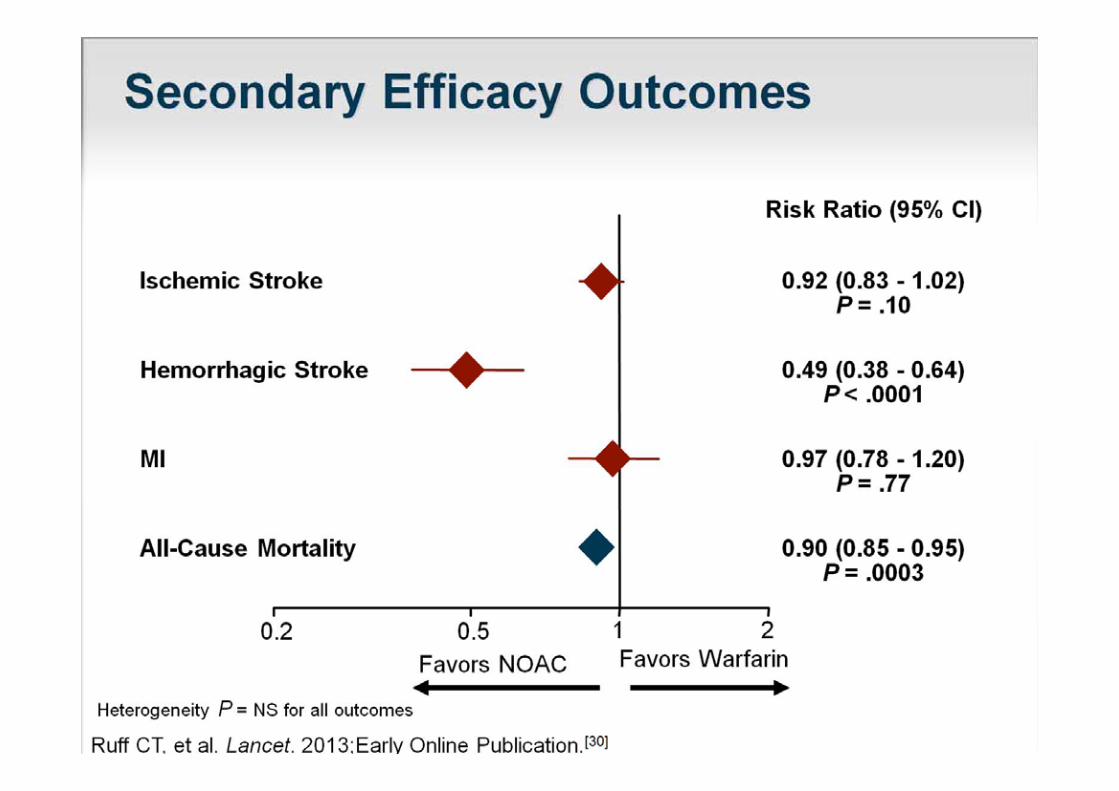




Warfarin or NOAC?Warfarin or NOAC?
• Monitoring issues• InteractionsInteractions• Longterm data• Antidote• Valvular AF : WarfarinValvular AF : Warfarin• Mechanical heart valves: Warfarin• Coronary stents: ? Warfarin• Unknown clinical scenarios: ? Warfarin• Unknown clinical scenarios: ? Warfarin• CKD 5: Warfarin
How I choose a NOACHow I choose a NOAC …….
• I don’t always have a ready answer……….I don t always have a ready answer……….
• Assess clinical factors (Things that I do)
• Offer patient three questions…. (Things I ask the patient to do)

Patient Question 1Patient Question 1
• Which is worse for you: having a stroke orWhich is worse for you: having a stroke or having a bleed?
• The best stroke medicine will have roughly the g ysame bleeding risk as Warfarin.
Patient Question 2Patient Question 2
• Do you want equivalent stroke protection riskDo you want equivalent stroke protection risk but lower bleeding risk than Warfarin?
Patient Question 3Patient Question 3
• Would you prefer once a day or twice a day?• Are you good with tablets?
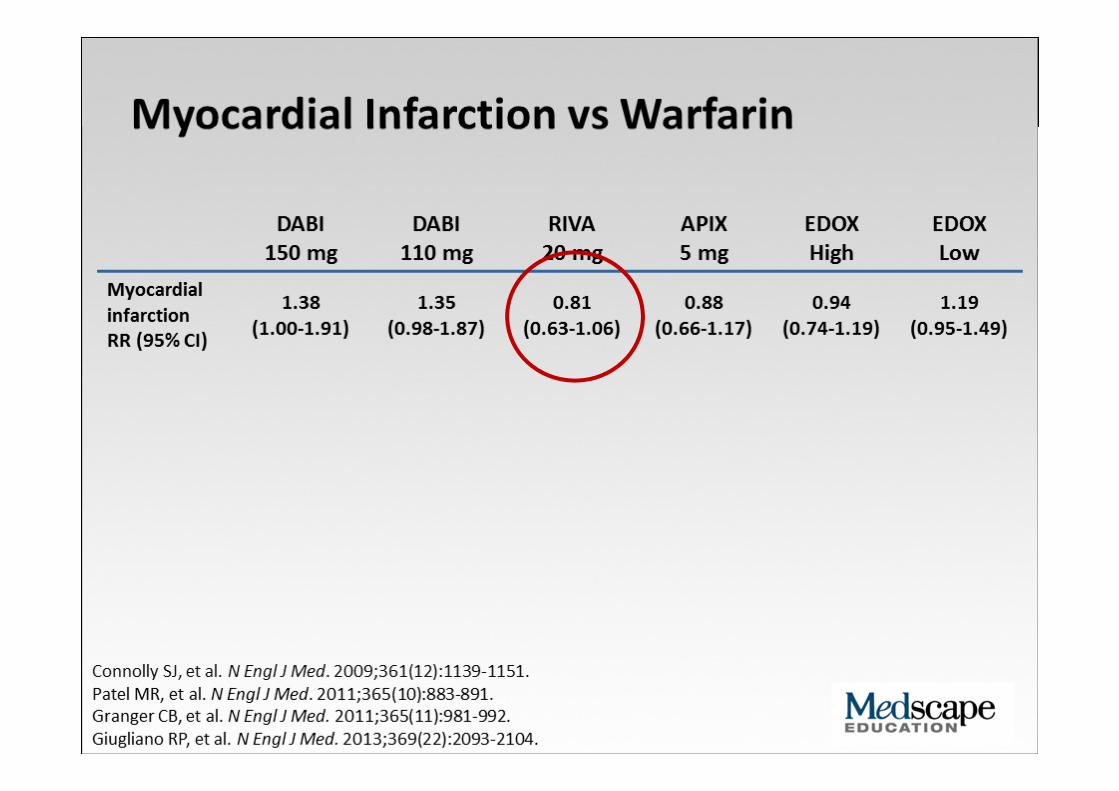
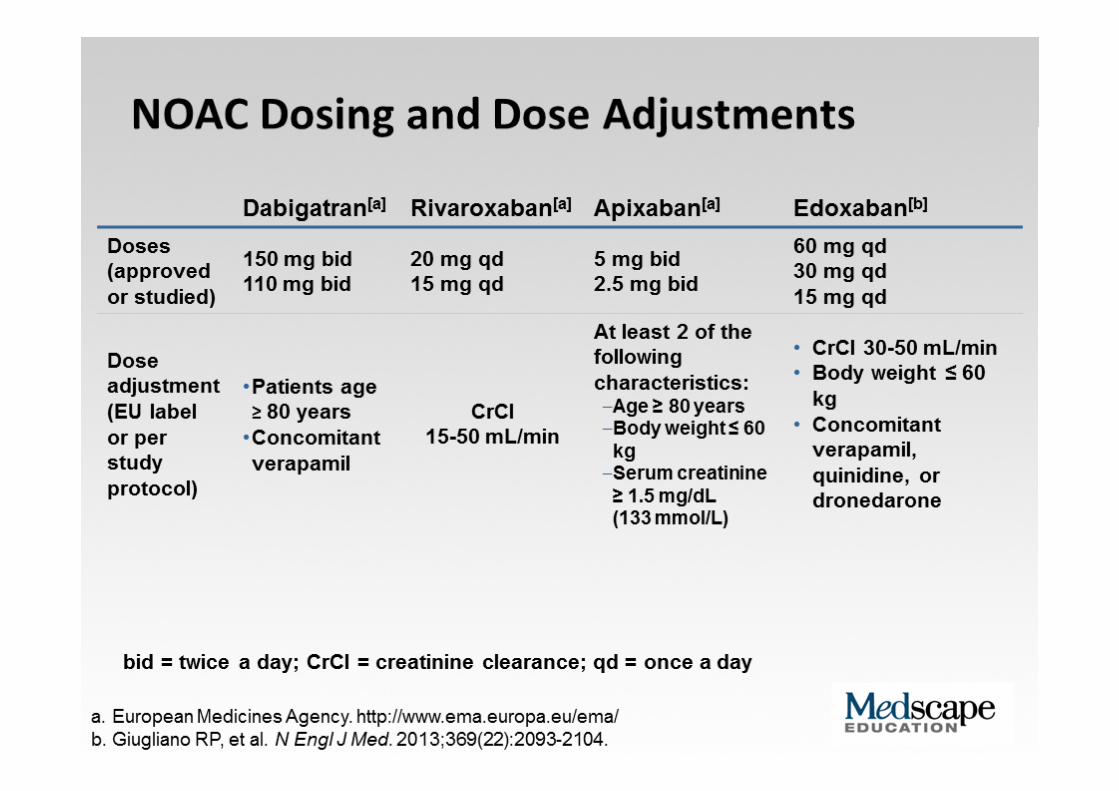
Questions I think aboutQuestions I think about …
• History of MI?History of MI?• Drug interactions?• GI bleeding risk / dyspepsia?• Renal function?Renal function?• Compliance?• Tablet box / dispensing issues?
Should one size fit all in Wales?Should one size fit all in Wales?
• So far these drugs are being initiated / approved by Senior Clinicianspp y
• Ample evidence in local data that switches are occurring due to variety of reasonsoccurring due to variety of reasons
• Evidence shows that these drugs are not all the same: each has unique advantages / disadvantagesdisadvantages
• Database shows specific reasons for ibi diff t NOACprescribing different NOACs
• Current treatment practice in Wales suggests case
In WalesIn Wales ……..
• How good are we at stroke prevention in AF?• Who are prescribing NOACs in Wales?• How are they being prescribed?• How are they chosen? Should one size fit all?• How are they chosen? Should one size fit all?• Attacking AF prevalence: What happens when a Cardiologist is sent out to a GP Surgery?Cardiologist is sent out to a GP Surgery?
• What are the Estimations and Projections?• Who should be prescribing NOACs in Wales?
A review of AF cases in the community: Ferndale Medical Centrecommunity: Ferndale Medical Centre
2015
• Serves 7600• GPs = 2 (+2)GPs 2 ( 2)• Anticoagulation
i Yservices = Yes• Aim: Review of stroke prevention in AF casesAF cases
• Industry support
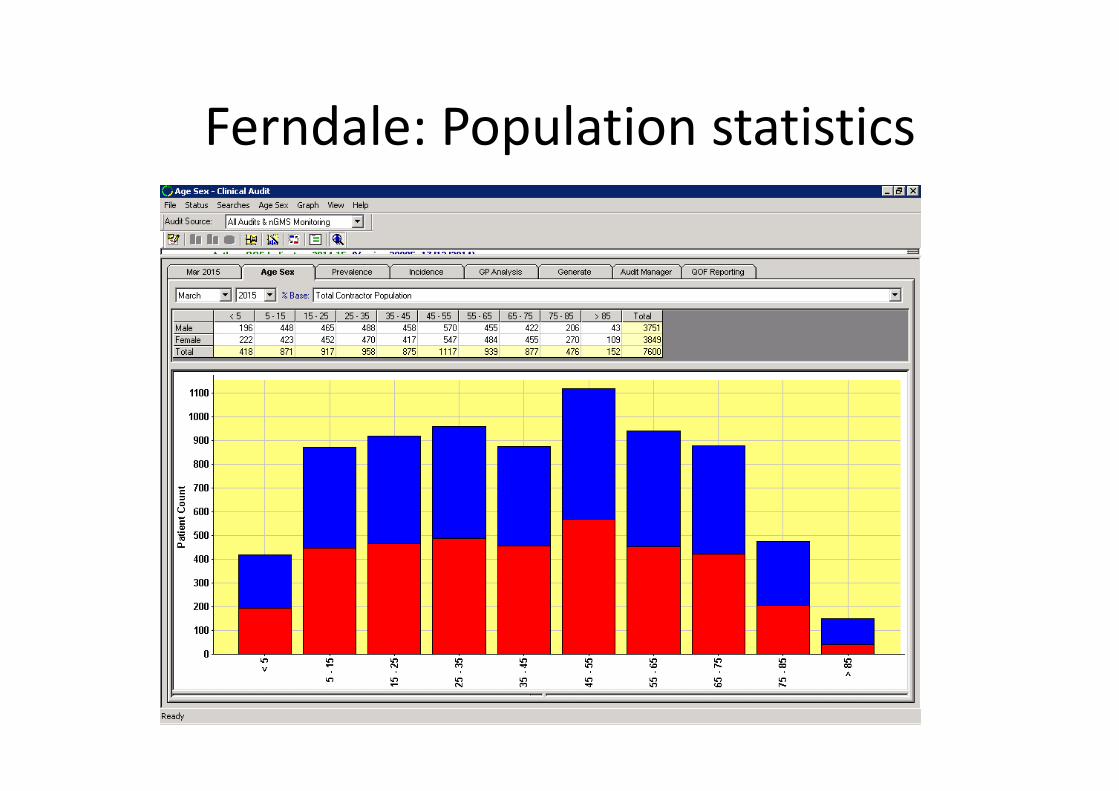
Ferndale: Population statisticsFerndale: Population statistics
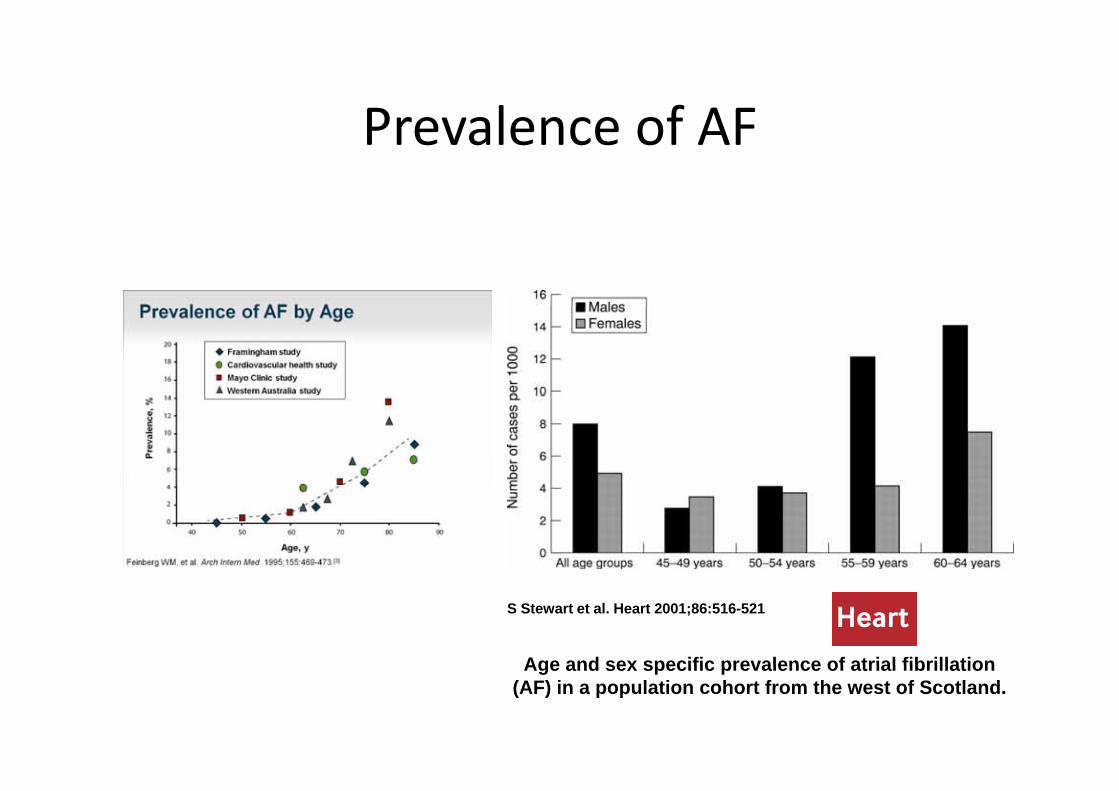
Prevalence of AFPrevalence of AF
S Stewart et al. Heart 2001;86:516-521
Age and sex specific prevalence of atrial fibrillationAge and sex specific prevalence of atrial fibrillation (AF) in a population cohort from the west of Scotland.
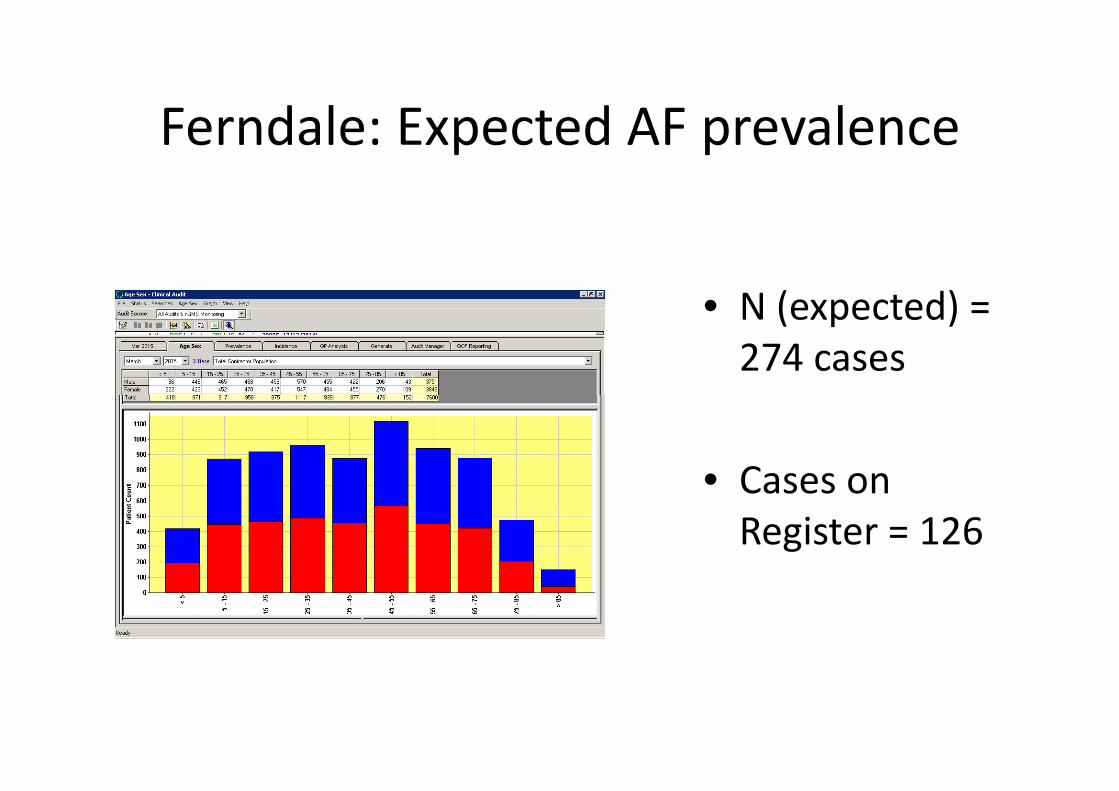
Ferndale: Expected AF prevalenceFerndale: Expected AF prevalence
• N (expected) =• N (expected) = 274 cases
• Cases onCases on Register = 126
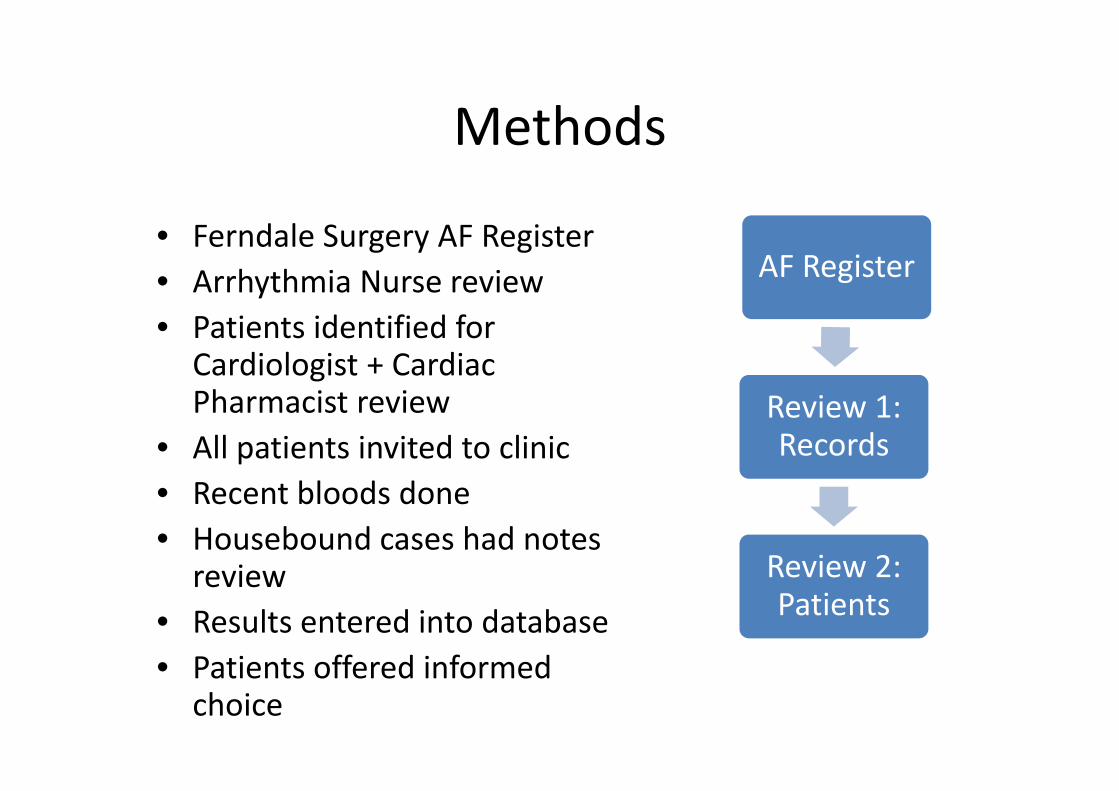
MethodsMethods
• Ferndale Surgery AF Register• Arrhythmia Nurse review AF Register
• Patients identified for Cardiologist + Cardiac Ph i t i i 1Pharmacist review
• All patients invited to clinicR t bl d d
Review 1: Records
• Recent bloods done• Housebound cases had notes
review Review 2:review• Results entered into database• Patients offered informed
Review 2: Patients
• Patients offered informed choice
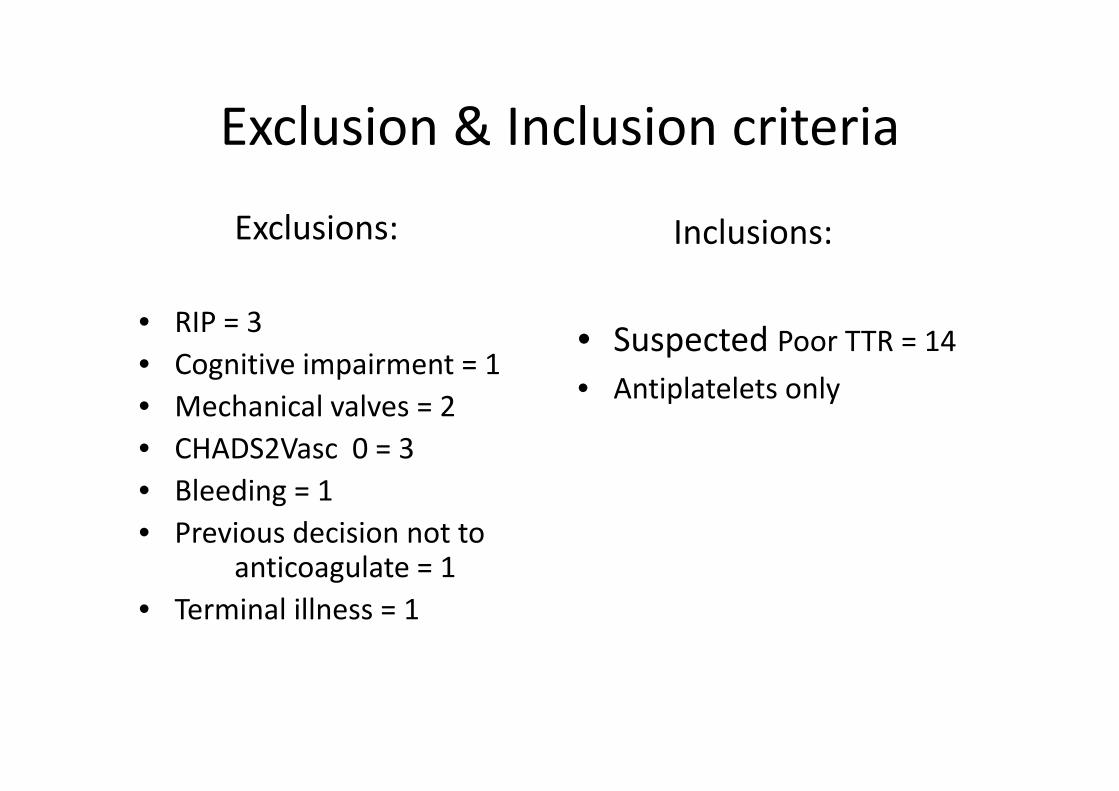
Exclusion & Inclusion criteriaExclusion & Inclusion criteria
E l iExclusions: Inclusions:
• RIP = 3• Cognitive impairment = 1
h i l l
• Suspected Poor TTR = 14• Antiplatelets only• Mechanical valves = 2
• CHADS2Vasc 0 = 3• Bleeding 1
Antiplatelets only
• Bleeding = 1• Previous decision not to
anticoagulate = 1anticoagulate 1• Terminal illness = 1
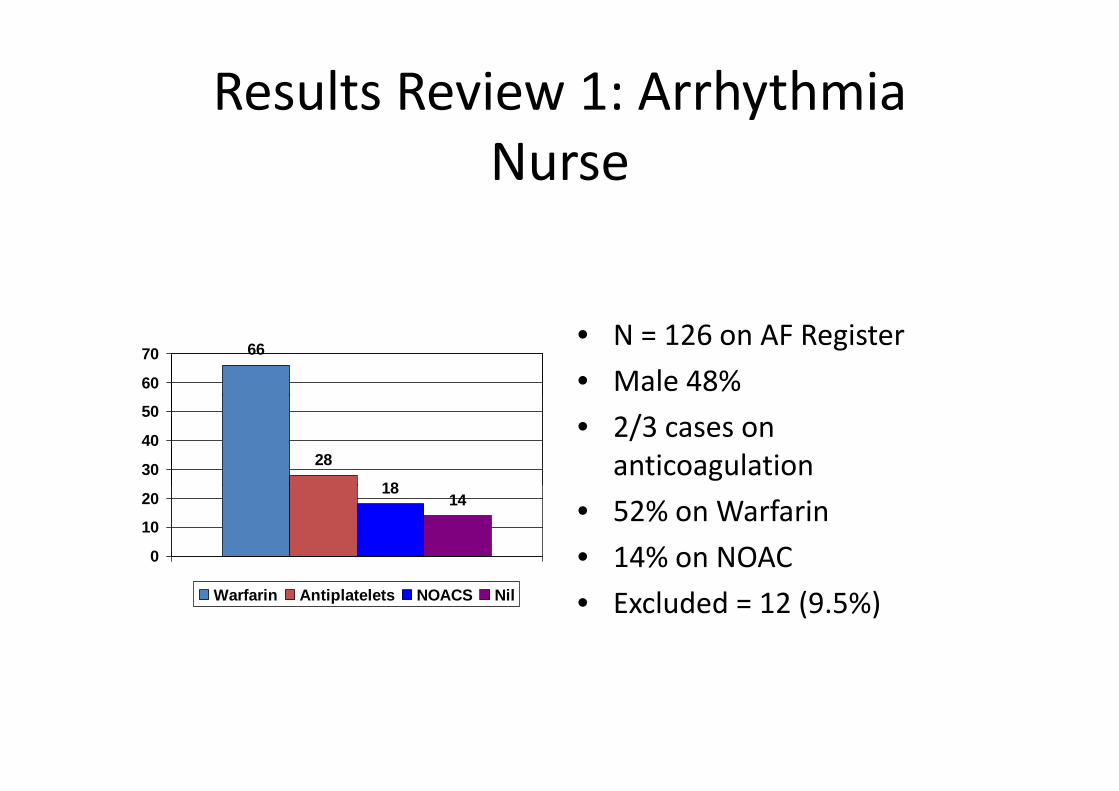
Results Review 1: Arrhythmia Nurse
66
60
70• N = 126 on AF Register • Male 48%
28
1830
40
50 • 2/3 cases on anticoagulation
1814
0
10
20 • 52% on Warfarin• 14% on NOAC
Warfarin Antiplatelets NOACS Nil • Excluded = 12 (9.5%)
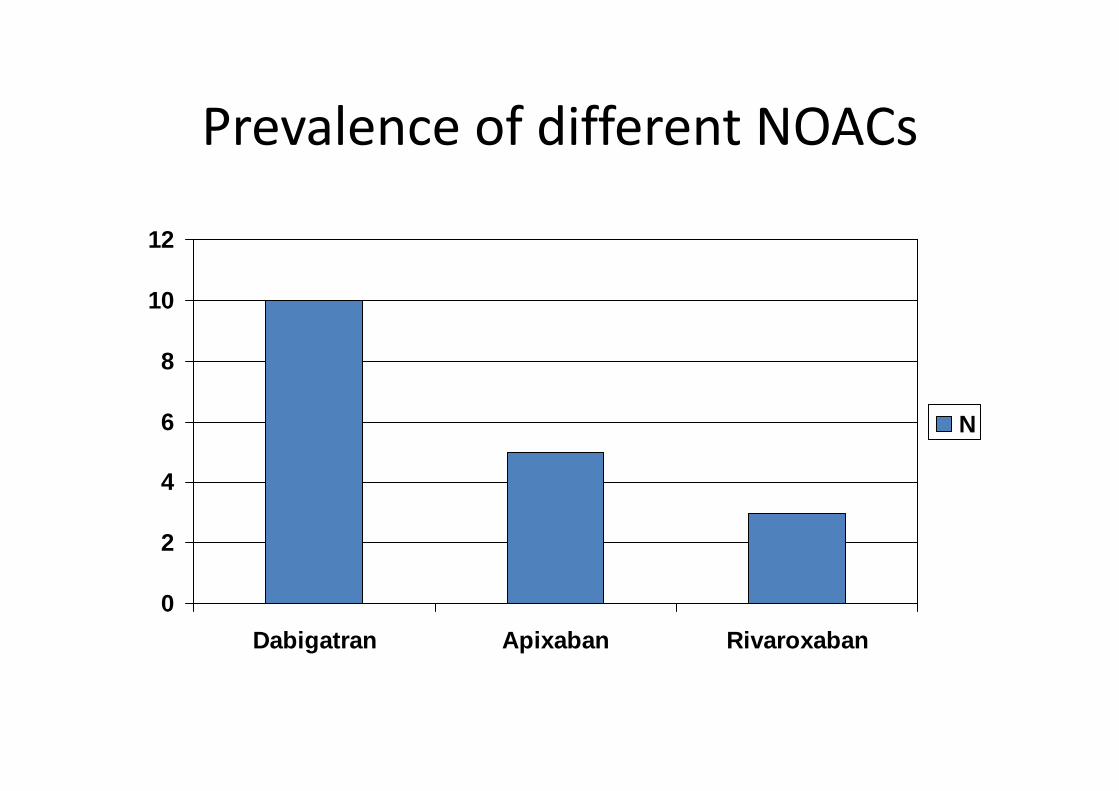
Prevalence of different NOACsPrevalence of different NOACs
10
12
8
10
4
6 N
2
4
0Dabigatran Apixaban Rivaroxaban
Results Review 2: Cardiologist + Cardiac Pharmacist
• Reviewed = 42 • Age range 49 – 95 years• Not in AF = 9 (9/126 = 7%)• Not in AF = 9 (9/126 = 7%)• Mean CHADS2Vasc = 3.1• On Warfarin = 14• No conclusion / unsuitable = 6No conclusion / unsuitable 6• New Cardiology = 12 (12/126 = 9.5%)
Results Review 2 (contd)Results Review 2 (contd)
• Changes made = 13 (13/126 = 10.3%)• New Warfarin = 2 (2/126 = 1.6%)• New NOAC = 8 (8/126= 6.4%)• Switch Warfarin to NOAC = 3 (3/66 = 4.5%)• Refused anticoagulation = 2 (2/126 = 1.6%)e used a coagu a o ( / 6 6%)
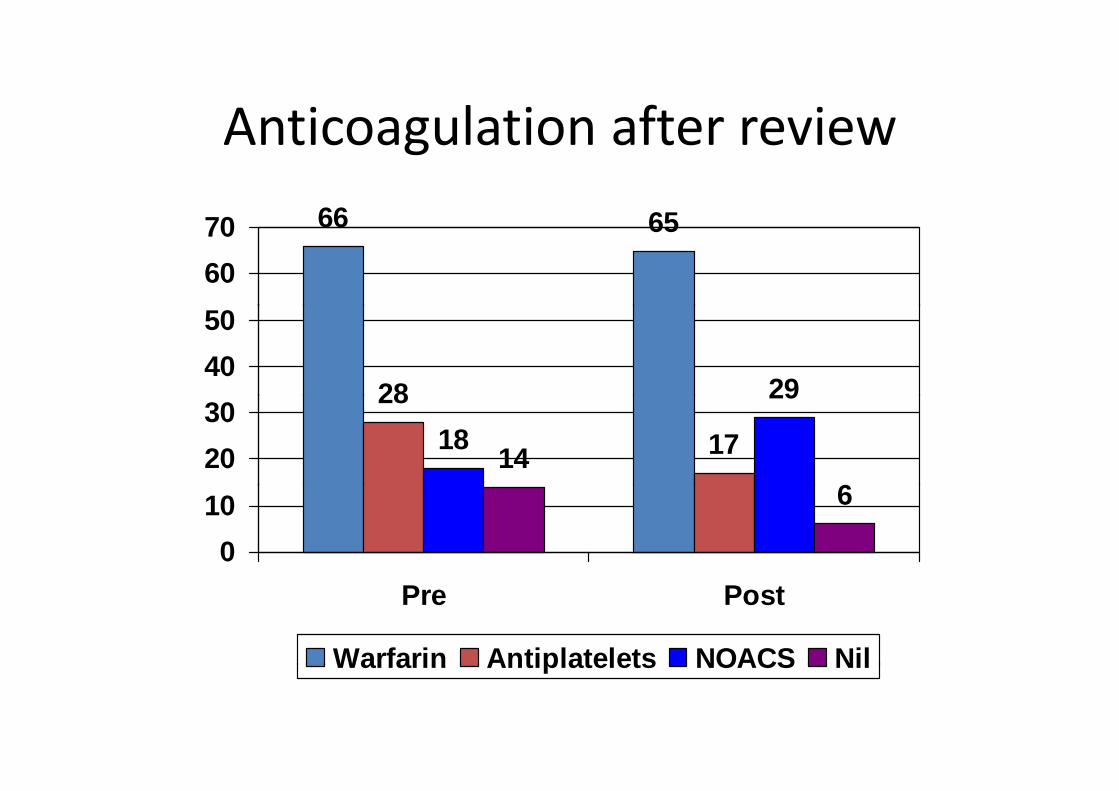
Anticoagulation after reviewAnticoagulation after review66 6566 65
6070
28 294050
28
1718
29
146
2030
6
010
Pre Post
Warfarin Antiplatelets NOACS NilWarfarin Antiplatelets NOACS Nil

NOACs after reviewNOACs after review
14
16
10
12
6
8 PrePost
2
4
0Dabigatran Apixaban Rivaroxaban

Study Conclusions 1Study Conclusions 1
• Good turnout 88%Good turnout 88%• 7% do not have AF • 52% are established on Warfarin• No conclusion / unsuitable: 18/126 = 14 3%No conclusion / unsuitable: 18/126 = 14.3%• 11% have Rx changes for stroke prevention• 9.5% new Cardiology referrals generated

Study Conclusions 2Study Conclusions 2
• Majority of patients on warfarin are stable in a practice run via Anticoagulation specialists (95.5%)
• No significant change in Warfarin total numbers:No significant change in Warfarin total numbers: switches offset by new prescriptionsNOAC i ti i b 9% (f 14% t• NOAC prescriptions increase by 9% (from 14% to 23%)
• Antiplatelet prescription fell from 11% to 4.8%• 80% of new Rx are NOACs80% of new Rx are NOACs
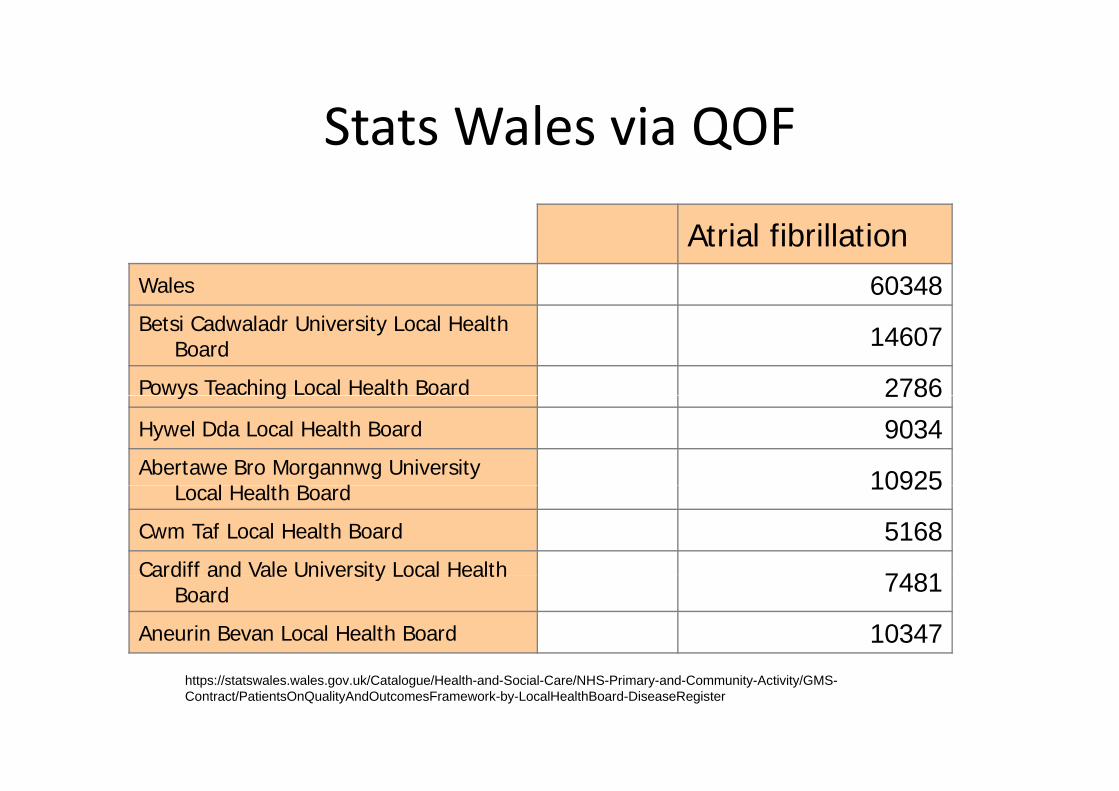
Stats Wales via QOFStats Wales via QOF
Atrial fibrillationWales 60348Betsi Cadwaladr University Local Health
Board 14607
Powys Teaching Local Health Board 2786y g 2786Hywel Dda Local Health Board 9034Abertawe Bro Morgannwg University
L l H lth B d 10925Local Health Board 10925
Cwm Taf Local Health Board 5168Cardiff and Vale University Local Health 7481Cardiff and Vale University Local Health
Board 7481
Aneurin Bevan Local Health Board 10347
https://statswales.wales.gov.uk/Catalogue/Health-and-Social-Care/NHS-Primary-and-Community-Activity/GMS-Contract/PatientsOnQualityAndOutcomesFramework-by-LocalHealthBoard-DiseaseRegister
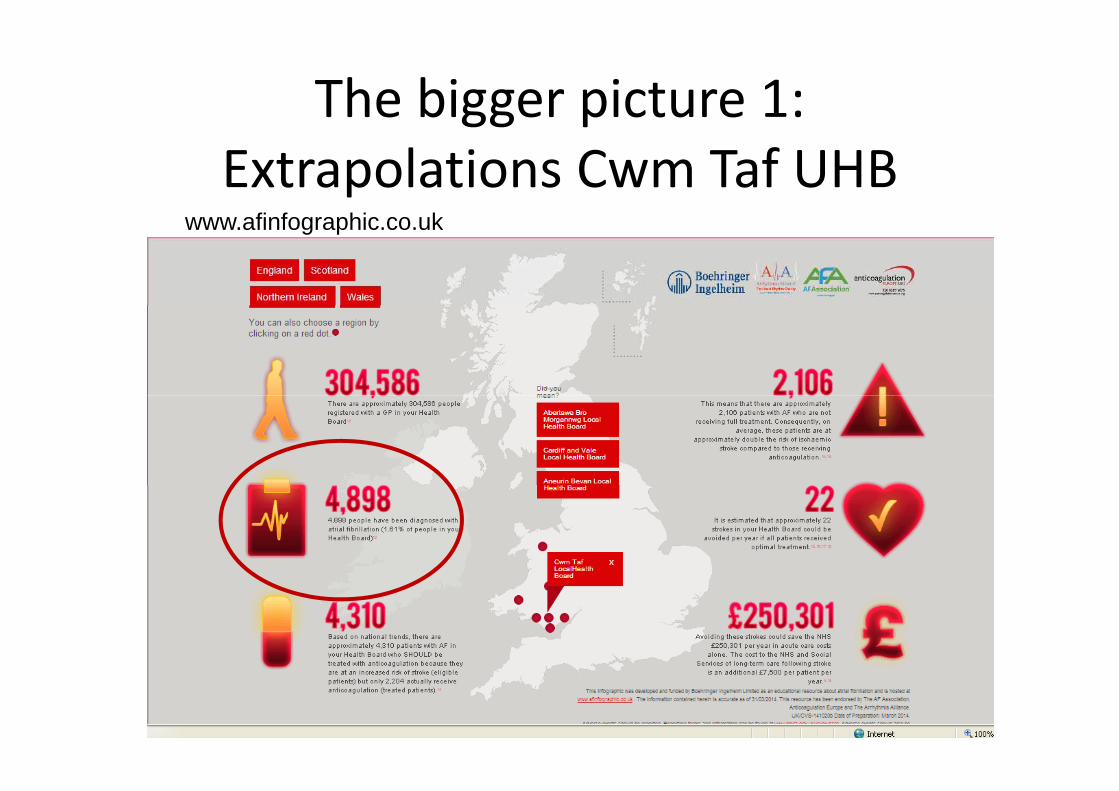
The bigger picture 1: gg pExtrapolations Cwm Taf UHB
fi f hi kwww.afinfographic.co.uk
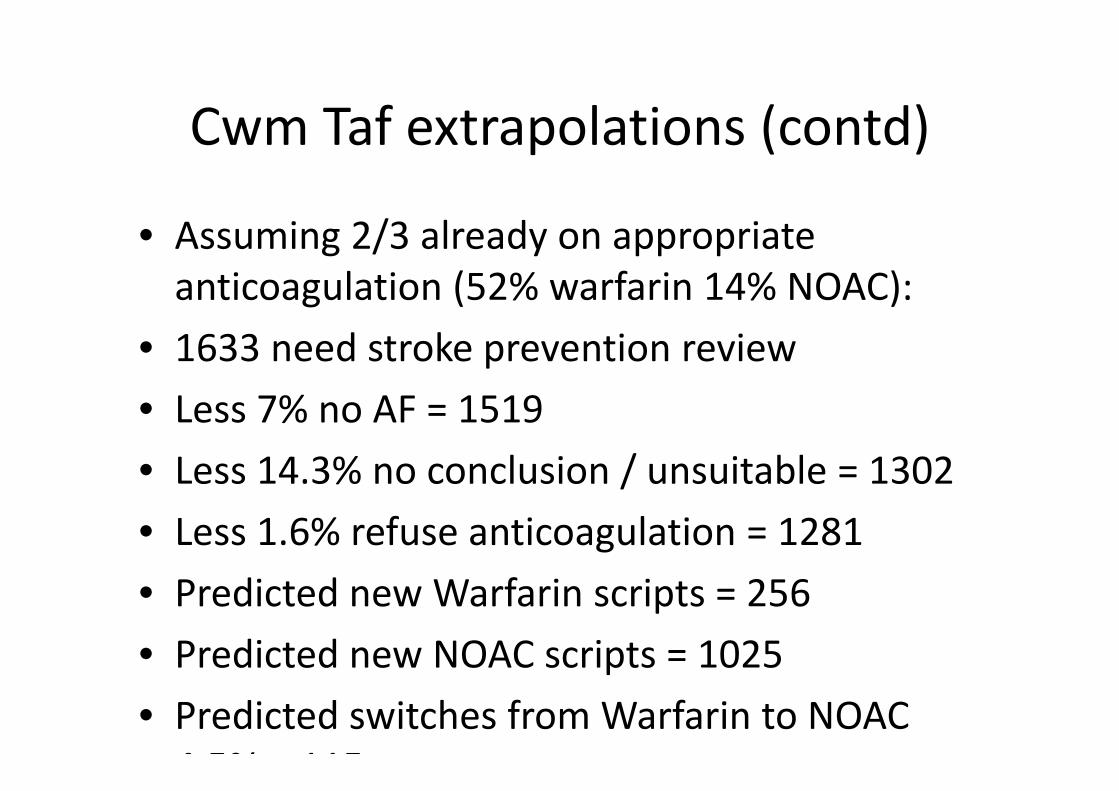
Cwm Taf extrapolations (contd)Cwm Taf extrapolations (contd)
• Assuming 2/3 already on appropriate anticoagulation (52% warfarin 14% NOAC):g ( )
• 1633 need stroke prevention reviewL 7% AF 1519• Less 7% no AF = 1519
• Less 14.3% no conclusion / unsuitable = 1302/• Less 1.6% refuse anticoagulation = 1281• Predicted new Warfarin scripts = 256• Predicted new NOAC scripts = 1025Predicted new NOAC scripts 1025• Predicted switches from Warfarin to NOAC 4 5% 115
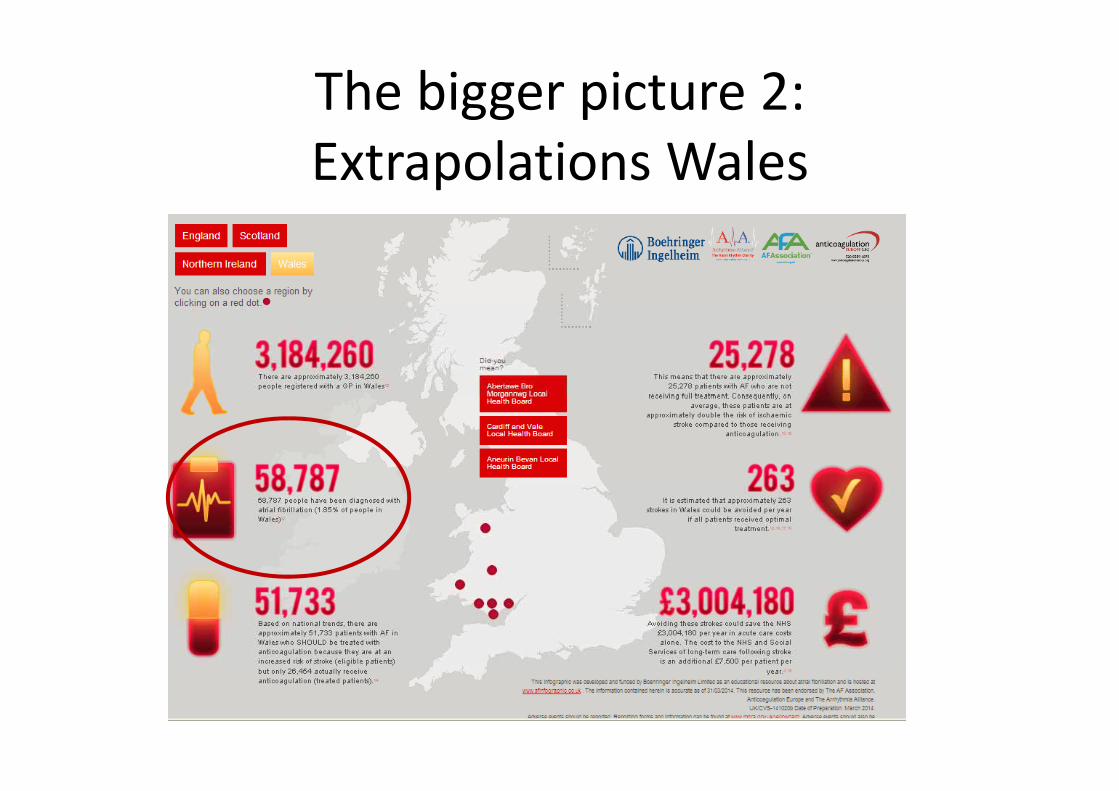
The bigger picture 2: Extrapolations Wales

Wales extrapolations (contd)Wales extrapolations (contd)
• Assuming 2/3 already on appropriate anticoagulation (52% warfarin 14% NOAC):g ( )
• 19596 need stroke prevention reviewL 7% AF 18224• Less 7% no AF = 18224
• Less 14.3% no conclusion / unsuitable = 15618/• Less 1.6% refuse anticoagulation = 15368• Predicted new Warfarin scripts = 3073• Predicted new NOAC scripts = 12294Predicted new NOAC scripts 12294• Predicted switches from Warfarin to NOAC 4 5% 1376
Prevalence not Incidence!Prevalence not Incidence!
• These calculations do not take into account N f AFNew cases of AF
• Incidence rates may help predict numbers of y p pnew prescriptions
Who should be prescribing NOACs in Wales? Food for thought
• Cardiologists …… but!!!!• Physicians• GPs ……… Starting with those who already run Level 4 Anticoagulation Services and those interestedAnticoagulation Services and those interested
• Role of Anticoagulation Pharmacists and AF Nurses• C m Taf proposition of centralised anticoag lation• Cwm Taf proposition of centralised anticoagulation services for HB
ConclusionsConclusions
• There is an urgent large currently unaddressed need in SPAF in Wales
• In addressing this need, substantial non‐AF related k ill b d f C di lwork will be generated for Cardiology
• A substantial increase in NOAC prescriptions can be di t dpredicted
• Current NOAC prescriptions show individualisationh ill h b i l i f• There will have to be capital investment from Health Boards: cost effectiveness has been validated by NICEvalidated by NICE

Thanks / QuestionsThanks / Questions
• Helen Mardon‐Davies, Sue Wooller, Rowena Havard, Angharad Thomas: Anticoagulation / g gCardiac Pharmacists
• Consultant Cardiologists Cwm Taf UHB• Consultant Cardiologists Cwm Taf UHB• Freya Lodge, Hansraj Shetty, Tim Kinnaird• Mandie Welch, Dawn Watkins Arrhythmia NursesNurses
• Ravi Srivastava: Practice Manager @ Ferndale• Anticoagulation implementation group Cwm Taf UHB