Efficient handoff rerouting algorithms: a competitive on ...

Risks for Retrograde Type-A Dissection After TEVAR
Frank R. Arko, III, MD
Chief, Vascular and Endovascular Surgery
Professor, Cardiovascular Surgery
Co-Director , Aortic Institute Sanger Heart and Vascular Institute
Charlotte, NC

Retrograde Type-A Dissection After TEVAR
TEVAR has shown to be an effective and durable repair option in the treatment of thoracic aortic pathology
Retrograde Type A dissection (RTAD) following TEVAR remains a highly lethal complication
Nearly two-thirds of the RTAD cases present within the first month
RTAD risk factors as described in literature are:
1. Hogendoorn W, Hunink MG, Schlosser FJ, Moll FL, Sumpio BE, Muhs BE. Endovascular vs: open repair of complicated acute type B aortic dissections. J Endovasc Ther 2014;21:503–14 2. Makaroun MS, Dillavou ED, Wheatley GH, Cambria RP, Gore TAGI. Five-year results of endovascular treatment with the Gore TAG device compared with open repair of thoracic aortic aneurysms. Journal of Vascular Surgery
2008;47:912–8 3. Canaud L, Ozdemir BA, Patterson BO, et al: Retrograde aortic dissection after thoracic endovascular aortic repair. Ann Surg 2014;260(2):389–395
Device Oversizing (>20%)
Large Stent Graft Diameter
Proximal Landing Zone
Ascending Aortic Diameter (> 40mm)
Gender Ballooning/Iatrogenic
injury Smoking
Arch Angulation and STJ Dilation

Retrograde Type-A Timing
Intra–op – 20.9%
<30d – 50.0%
>30d – 29.1%
Range: 0 – 1825 days Canaud et al. Ann Surg 2014;00:1-7
Over 70% occur within the first 30-days
Delayed onset suggests disease progression
37% overall mortality

Pathology Treated
Patients treated for Aortic Dissection have the highest pooled rates of RTAD4
Acute TBAD had the highest associated rate for RTAD at 8.4%
Chronic TBAD associated rate for RTAD at 3%
The influence of acute dissection and aortic fragility on RTAD has been illustrated in other reports5
Retrograde Type A Aortic Dissection After Thoracic Endovascular Aortic Repair: A Systematic Review and Meta-Analysis
Yanqing Chen, MD;* Simeng Zhang, MD;* Lei Liu, MD;* Qingsheng Lu, MD; Tianyi Zhang, MD; Zaiping Jing, MD
Hata M, Shiono M, Inoue T, Sezai A, Niino T, Negishi N, Sezai Y. Optimal treatment of type B acute aortic dissection: long-term medical follow-up results. Ann Thorac Surg. 2003;75:1781–1784

Landing Zone and RTAD
Landing Zone
RTAD (%)
OR (relative to zones 3/4)
0 6.8 5.7
1 2.4 1.9
2 4.1 3.3
3/4 1.3 1
RTAD rates vary significantly based on zone6
Significantly higher in Zones 0-2
7.5% during zone 0 total debranching7
Significant correlation between pathology, zone and repair complexity
Czerny M, Weigang E, Sodeck G, et al. Targeting landing zone 0 by total arch rerouting and TEVAR: midterm results of a transcontinental registry. Ann Thorac Surg. 2012;94:84–89
Canaud et al. Ann Surg 2014;00:1-7

Device Oversizing
Patients with RTAD had significantly
greater device oversizing8
• 22.0% vs. 10.3% (p<0.0001)
Each 1% oversizing above 9%
• Increase in OR of RTAD - 14% (p<0.0001)
Device Oversizing in TBAD resulted in a
higher RTAD rate - 24.4% vs 14.1%
Canaud et al. Ann Surg 2014;00:1-7

Ascending Arch Condition
Several arch characteristics for RTAD
• Enlarged aortic diameter >40mm (4.8% vs 0.9%; P =
.047)9
• Bicuspid valve
• Presence of angulated (>60°) “Gothic” arch type
• Abnormal aortic root morphology10 o Valsalva diameter >40mm (33% vs 15%, P ¼ .31) o Loss of STJ (> diameter of aortic root)
Williams JB, Andersen ND, Bhattacharya SD, et al. Retrograde ascending aortic dissection as an early complication of thoracic endovascular aortic repair. J Vasc Surg. 2012;55:1255-1262 Factors favoring retrograde aortic dissection after endovascular aortic arch repair Thomas Gandet, MD, Ludovic Canaud, MD, PhD, Baris Ata Ozdemir, MBBS, Vincent Ziza, MD, Roland Demaria, MD, PhD, Bernard Albat, MD, PhD, and Pierre Alric, MD, PhD; (J Thorac Cardiovasc Surg 2015;150:136-42)

Proximal Configuration
No significant differences between the proximal configuration of devices 2.8% Proximal Bare Stent (48/1724) VS 2.4% NBS, p=0.5895 (28/1159)
Zone placement and dynamic arch motion may also play a role

RTAD Experience at Carolinas Medical Center
Retrospective review of TBAD treated with TEVAR (2012 – 2017)
186 patients; Mean follow-up 569 days
Overall incidence of RTAD – 8.0% (15/186)
Number
Presentation (Days)
Percentage
1 Intra-Op 0.5%
5 1 – 30 2.6%
6 31 - 365 3.2%
3 366 - 569 1.6%

Demographics and Comorbidities
Variable; n (%)/ Mean (SD) RTAD (n-15) Non-RTAD (n-171) P-value
Male Sex 8 (46.7) 0.6
Age 61.5 (14.4) 0.9
Race 0.5
African-American 8 (53.3) 72 (42.1)
White 7 (46.7) 94 (55.0)
CAD 1 (6.7) 45 (26.3) 0.1
CKD/CRI 3 (20.0) 44 (25.7) 0.8
COPD 1 (6.7) 36 (21.1) 0.3
Diabetes 1 (6.7) 30 (17.5) 0.5
HLD 6 (40.0) 71 (41.5) 0.9
HTN 13 (86.7) 160 (93.6) 0.3
Smoking < 1yr 7 (46.7) 85 (49.7) 0.8
Marfans 1 (6.7) 5 (2.9) 0.4
Other Genetic/Connective Tissue 0 (0) 2 (1.2) 1.0
Previous Ascending/Arch Repair 2 (13.3) 11 (6.4) 0.3

Indication for Intervention
RTAD (n = 15) Non-RTAD (n = 171) P-value
Mesenteric Ischemia 2 (13.3) 8 (4.7) 0.2
Renal Ischemia 6 (40.0) 29 (17.0) 0.04
Lower Limb Ischemia 1 (6.7) 11 (6.4) 1.0
Spinal Ischemia 1 (6.7) 3 (1.8) 0.3
Aneurysm (> 6cm) 0 (0.0) 4 (2.3) 1.0
Rupture 1 (6.7) 6 (3.5) 0.5
High Risk: Refractory HTN 0 (0.0) 11 (6.4) 0.6
High Risk: Continued Pain 2 (13.3) 32 (18.7) 1.0
High Risk: Pain and HTN 1 (6.7) 23 (13.5) 0.7
Variable n(%) or Mean (SD) RTAD (n - 15)
Non-RTAD (n – 171)
Acute Complicated 8 (53.3) 50 (29.2)
Acute High Risk 3 (20.0) 69 (40.8)
Acute Uncomplicated
2 (13.3) 17 (9.9)
Chronic 2 (13.3) 35 (20.5)
Procedural Indication

Intervention Timing
Variable; n(%) or mean(SD) RTAD (n=15) No RTAD (n=171) p-value
Acute (less than two weeks) Presentation 10 (66.7) 94 (55.6) 0.4
Time to Intervention 0.4
Acute Early (<48 hours) 1 (6.7) 30 (17.5)
Acute Delayed (48 hrs-2 weeks) 9 (60) 64 (37.4)
Subacute (2-6 weeks) 1 (6.67) 19 (11.1)
Chronic 4 (26.7) 56 (32.8)
Unknown 0 (0) 2 (1.2)

Aorta Characteristics
Mean (SD); Frequency (%) RTAD (n=15) No-RTAD (n=171) P-value
Ascending Diameter 37.1 (4.9) 36.4 (4.3) 0.5
Ascending > 4cm 7 (46.7) 35 (21.5) 0.05
Arch Type 0.6
Type I 6 (40.00) 49 (28.99)
Type II 3 (20.00) 53 (31.36)
Type III 6 (40.00) 67 (39.64)
Bovine 5 (33.33) 49 (28.65) 0.8
Dissection proximal to LSA 5 (33.3) 26 (15.3) 0.1
Presence of IMH 10 (66.67) 65 (38.01) 0.03
IMH in Arch 3 (20.00) 12 (7.02) 0.1

Procedural Details
Variable; n(%) or mean(SD) RTAD (n=15) No RTAD (n=171) p-value
Proximal Landing Zone 0 - 2 14 (93.3) 109 (63.7) 0.02
Zone 0 1 (6.7) 2 (1.17)
Zone 1 4 (26.7) 8 (4.68)
Zone 2 9 (60.0) 99 (57.9)
Zone 3 1 (6.7) 44 (25.7)
Zone 4 - 5 0 (0.0) 18 (10.6)
Struts at most proximal attachment 11 (73.3) 124 (77.5) 0.7
Graft oversizing (based on CTA) 4.6 (6.1) 5.4 (6.9) 0.2
Diameter of most proximal graft 33.3 (3.3) 31.8 (4.1) 0.1
Length of most proximal graft 173.3 (25.8) 159.3 (35.1) 0.2
Number of stent grafts in thoracic aorta 1.8 (0.4) 1.7 (0.7) 0.2
Number of stents in visceral arteries 0.7 (1.0) 0.3 (0.8) 0.05
Had stents placed in visceral arteries 5 (33.3) 26 (15.2%) 0.1

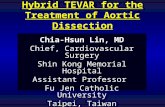
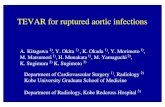
Case Review
“Snorkel” repair of LSA and LCA with TEVAR in 2011
Routine follow-up (2 – year) with a Type A dissection and occlusion of LSA stent
Non-operative candidate for standard repair of ascending arch
Additional “snorkel” of innominate artery and placement of graft decided as treatment plan
Patient Presentation

Initial Angiogram
Type A Dissection

Device Placement

Final Angiogram

Minimizing Risks for RTAD
Careful patient presentation BEFORE determining treatment approach
Establish a systematic protocol to minimize threat of RTAD
Iatrogenic injury is REAL - minimize manipulation and wire/catheter movement
Size appropriately based on pathology and treatment zone
Use IVUS for all aortic procedures

Conclusions
The occurrence of RTAD after TEVAR remains relatively infrequent but devastating
Several risk factors influence risks for RTAD:
Pathology Anatomy, Procedural techniques Device selection Continued Cocaine Use
At risk patients for RTAD may require enhanced surveillance
Additional R & D and investigation must continue to further reduce the risk of
RTAD
Oversizing Treatment timing Acute Complicated TBAD Ischemia of Visceral/Renal
Arteries

Thank You Frank R. Arko, III, MD
Chief, Vascular and Endovascular Surgery
Professor, Cardiovascular Surgery
Co-Director , Aortic Institute Sanger Heart and Vascular Institute
Charlotte, NC