Hybrid tevar for the treatment of aortic dissection
52
Chia-Hsun Lin, MD Chia-Hsun Lin, MD Chief, Cardiovascular Chief, Cardiovascular Surgery Surgery Shin Kong Memorial Shin Kong Memorial Hospital Hospital Assistant Professor Assistant Professor Fu Jen Catholic Fu Jen Catholic University University Taipei, Taiwan Taipei, Taiwan Hybrid TEVAR for the Hybrid TEVAR for the Treatment of Aortic Treatment of Aortic Dissection Dissection
-
Upload
uvcd -
Category
Presentations & Public Speaking
-
view
185 -
download
0
Transcript of Hybrid tevar for the treatment of aortic dissection
Chia-Hsun Lin, MDChia-Hsun Lin, MDChief, Cardiovascular Chief, Cardiovascular
SurgerySurgeryShin Kong Memorial HospitalShin Kong Memorial Hospital
Assistant Professor Assistant Professor Fu Jen Catholic UniversityFu Jen Catholic University
Taipei, TaiwanTaipei, Taiwan
Hybrid TEVAR for the Hybrid TEVAR for the Treatment of Aortic Treatment of Aortic
DissectionDissection
• Acute type A dissectionAcute type A dissection
- indicated for total arch - indicated for total arch repairrepair• Chronic type B dissectionChronic type B dissection
- indicated for TEVAR with - indicated for TEVAR with no no
suitable proximal landing suitable proximal landing sitesite
at zone 2at zone 2
Hybrid TEVAR for the Hybrid TEVAR for the Treatment of Aortic Treatment of Aortic
DissectionDissection
• Acute type A dissection -Acute type A dissection -
indicated for total arch repair,indicated for total arch repair, due to arch aneurysm formation (>4cm), tears in arch or proximal DTA, or supra-aortic arteries dissection• Chronic type B dissectionChronic type B dissection
Hybrid TEVAR for the Hybrid TEVAR for the Treatment of Aortic Treatment of Aortic
DissectionDissection
• Most challenging, perioperative mortality is still significant despite improvement in surgical techniques
• Emergent ascending aorta or hemiarch replacement to achieve primary goal of immediate survival
Type A Aortic DissectionType A Aortic Dissection
• Residual distal false lumen patency 50-70%of patients after ascending aorta replacement
• Residual distal false lumen patency 15-30%of patients after total arch replacement
- Ann Thorac Surg 2007;84:1955-64
- J Thorac Cardiovasc Surg 2006;131: 862-7
Type A Aortic DissectionType A Aortic Dissection
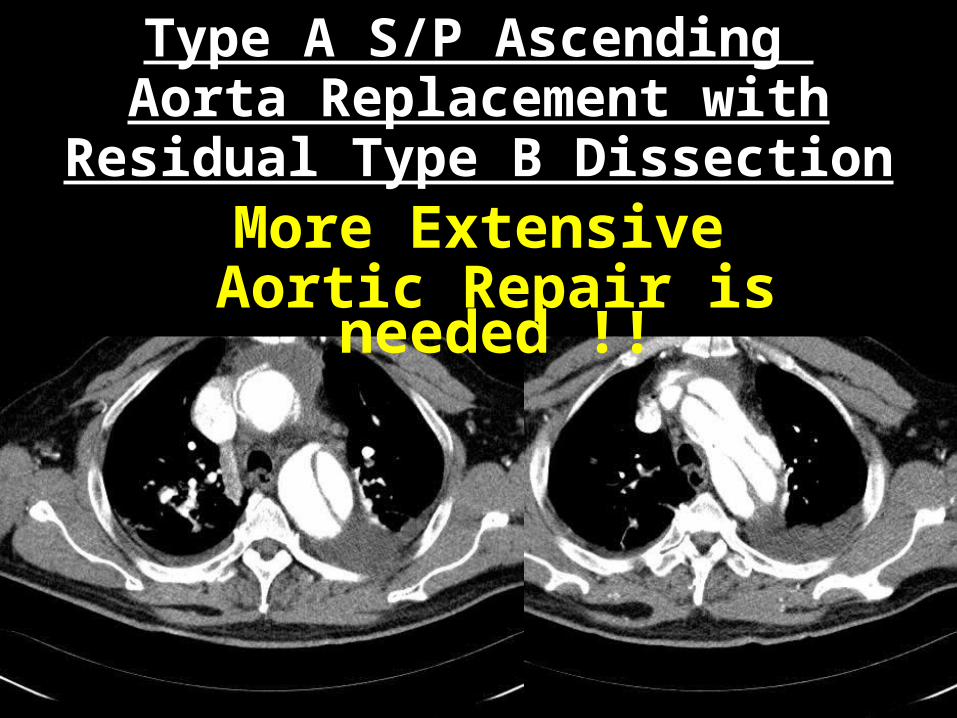
Type A S/P Ascending Aorta Replacement with
Residual Type B DissectionMore Extensive
Aortic Repair is needed !!
Hybrid TEVAR for Type Hybrid TEVAR for Type A Aortic DissectionA Aortic Dissection
One-stop treatment of the entire thoracic aorta•Open repair for proximal aorta and aortic arch•TEVAR for DTA tear coverage and apposition of intimal dissecting membrane to the adventitia
“High-risk” Arch Repair
Profound hypothermia• Prolonged CPB time - end organs
dysfunction• Prolonged myocardial ischemic time - deteriorated myocardial function • Induced coagulopathy – excessive bleeding
Circulatory arrest• Antegrade cerebral perfusion - clustered tubes in surgical field - emboli from carotid cannulation
Our Operative Techniques
NO Deep Hypothermic Circulatory Arrest •32℃ CPB•Bi-arterial perfusion, right axillary and femoral artery•Ascending aortic cross-clamping•HTK arrest
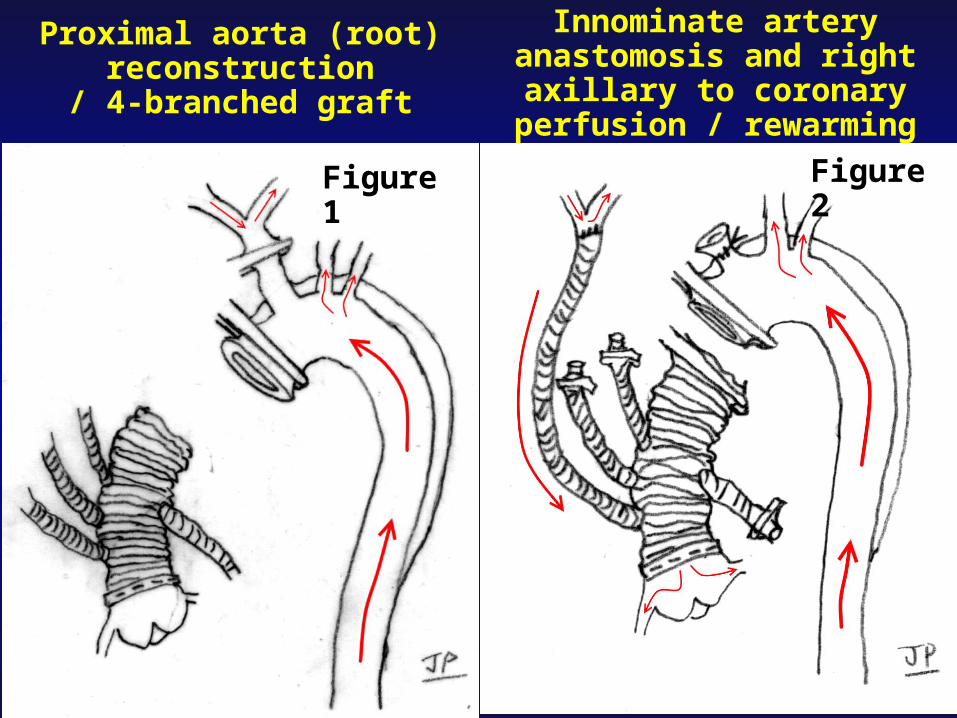
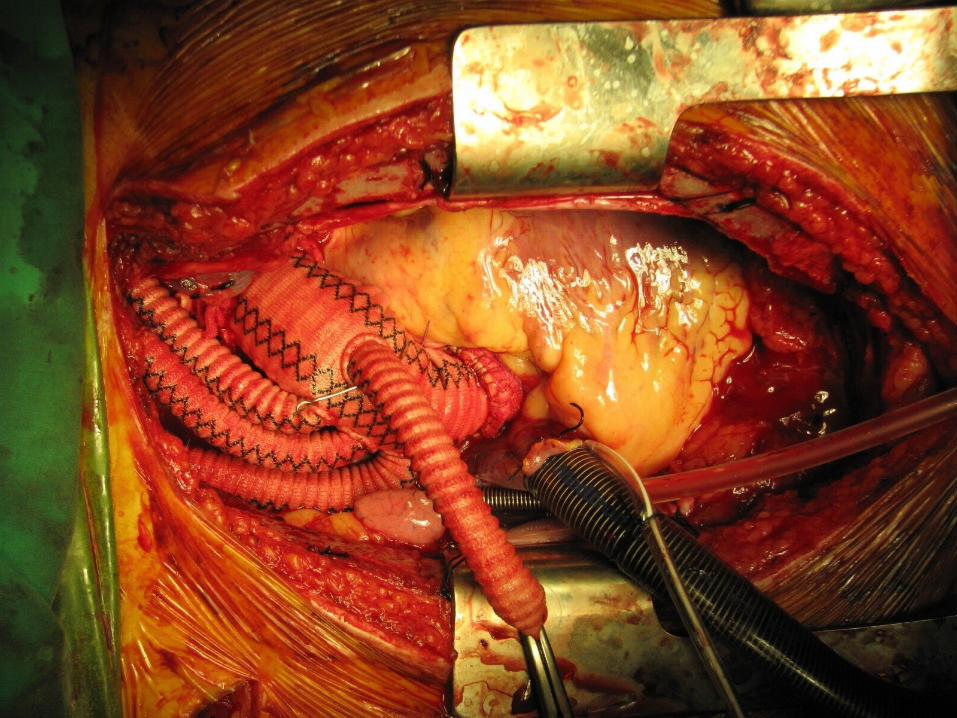
Proximal aorta (root) reconstruction
/ 4-branched graft
Innominate artery anastomosis and right
axillary to coronary perfusion / rewarming
Figure 1
Figure 2
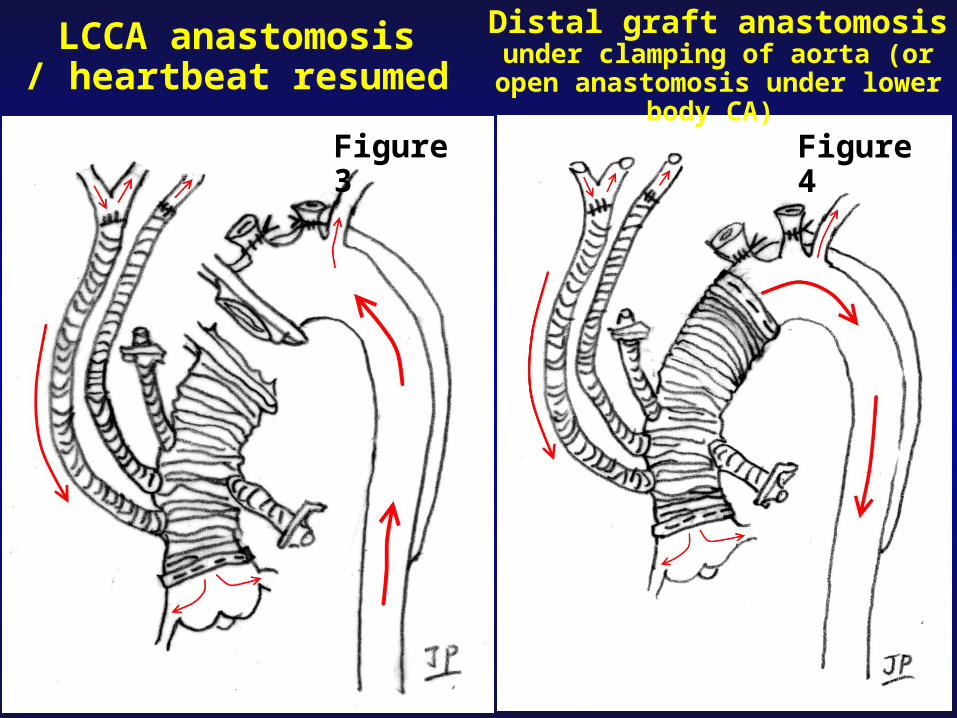
LCCA anastomosis/ heartbeat resumed
Distal graft anastomosis under clamping of aorta (or
open anastomosis under lower body CA)
Figure 3
Figure 4
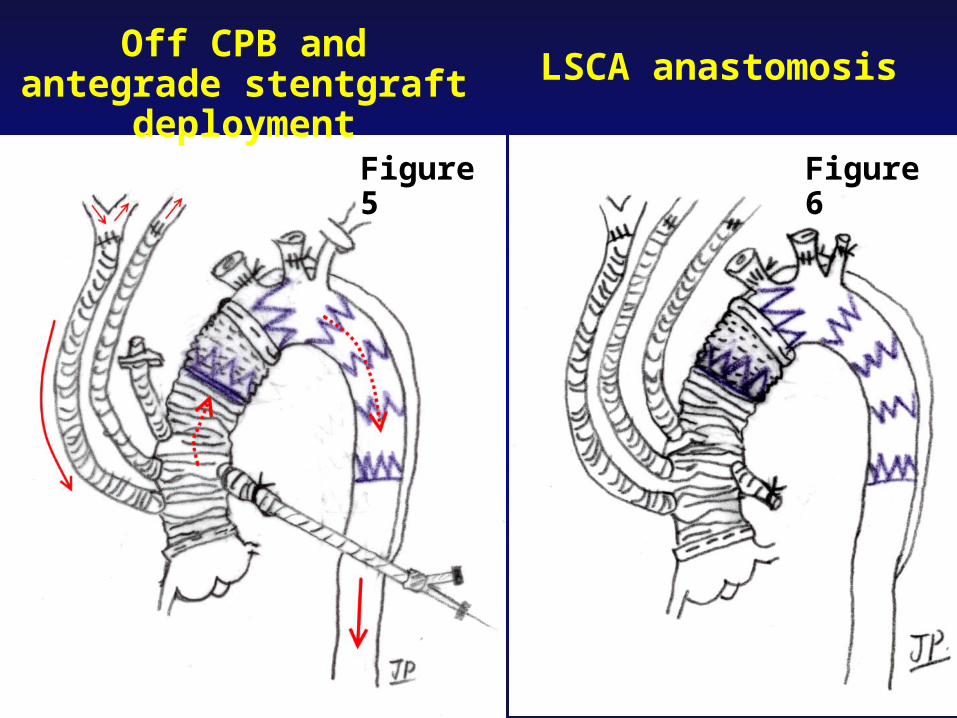
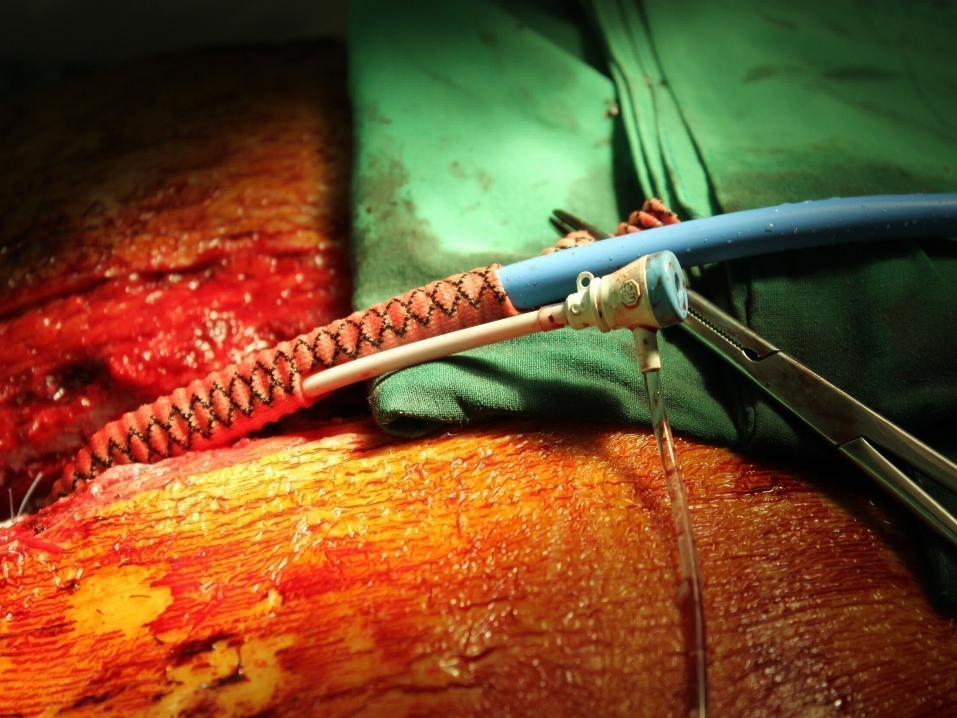
Off CPB and antegrade stentgraft
deployment
LSCA anastomosis
Figure 5
Figure 6
Stentgraft in Hybrid Arch Deployed after Circulation
Restoration• Frozen elephant trunk,
extending the proximal graft into DTA
• Endovascular repair, covering the DTA entries accurately
• Hemostasis of anastomosis, landing in proximal graft
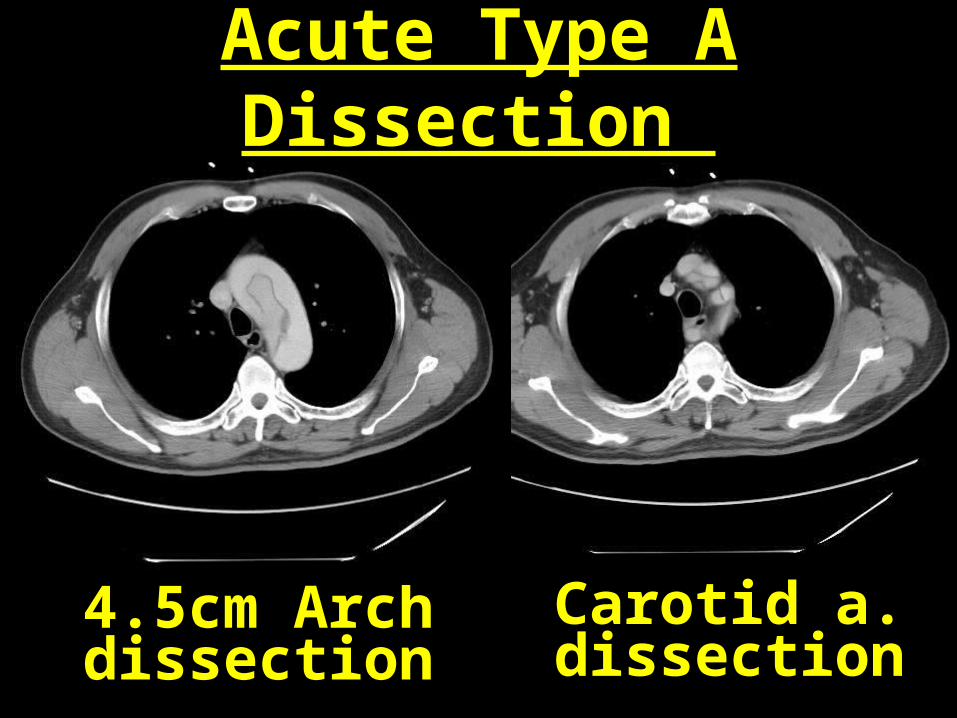
4.5cm Arch dissection
Carotid a. dissection
Acute Type A Dissection
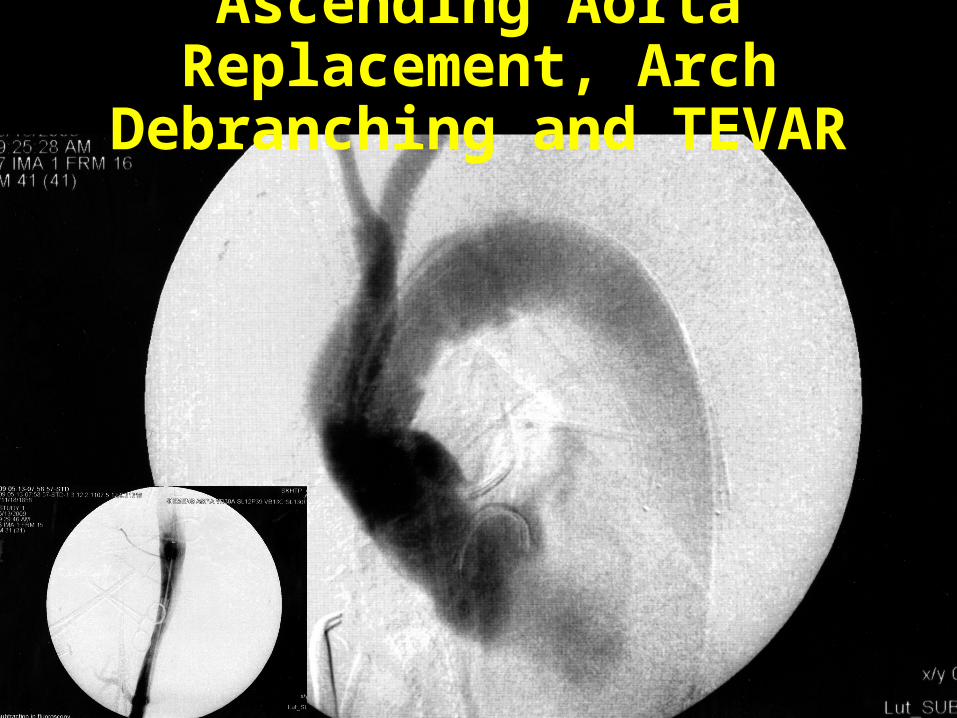
Ascending Aorta Replacement, Arch
Debranching and TEVAR


Post-op 2M
Post-op 2M
Post-op 1M
Aorta Remodeling within Stent
Post-op 6M
Post-op 9M
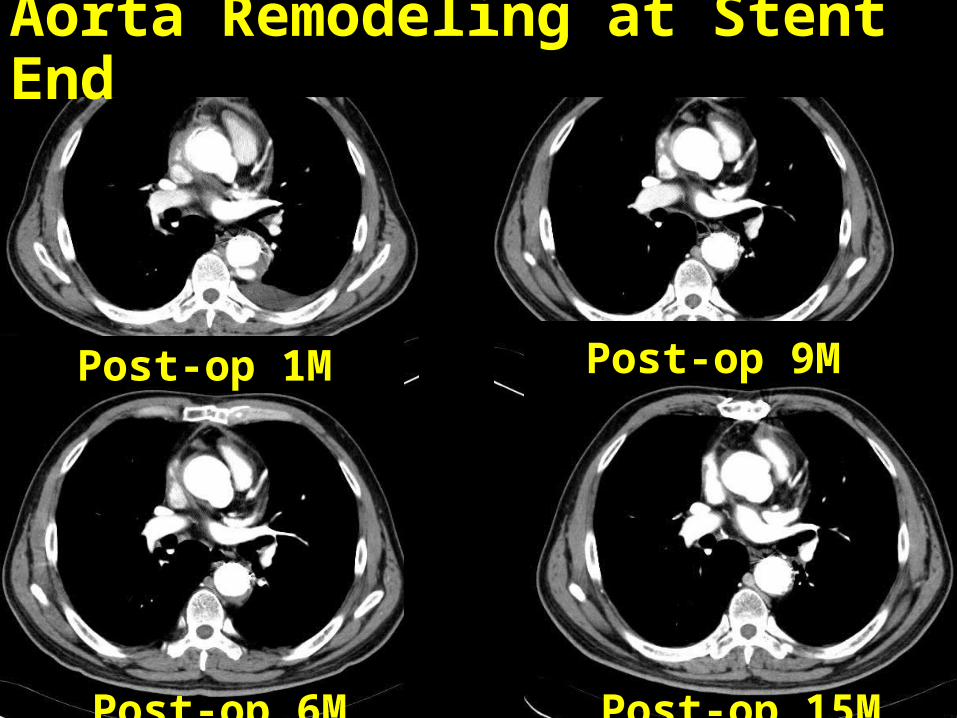
Post-op 6M
Post-op 1M
Aorta Remodeling at Stent End
Post-op 15M
Post-op 9M
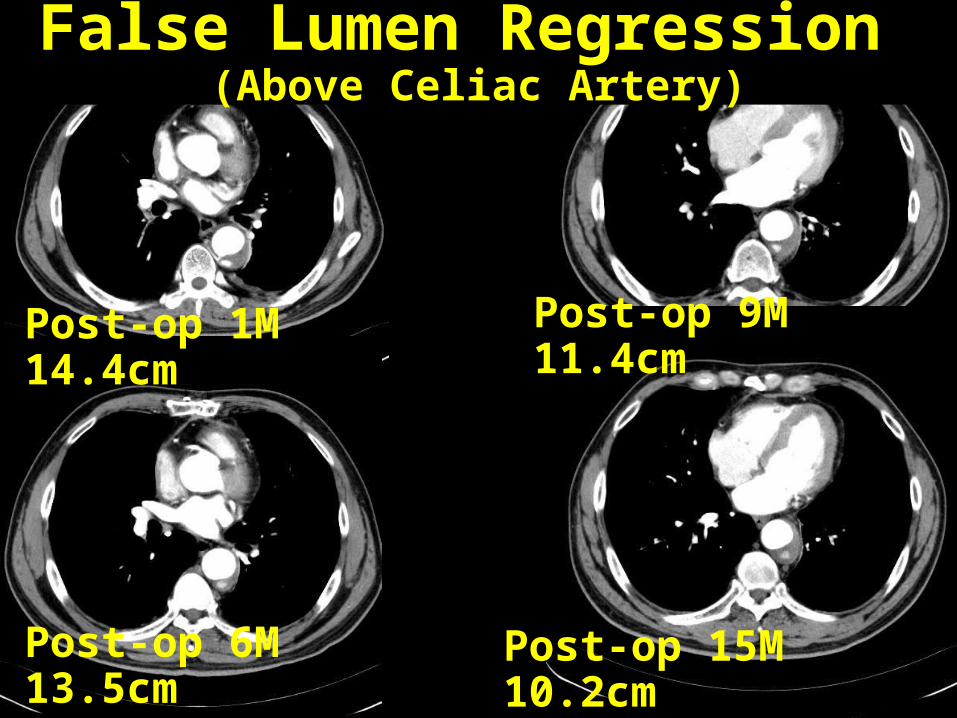
Post-op 6M 13.5cm
Post-op 15M 10.2cm
False Lumen Regression (Above Celiac Artery)
Post-op 9M 11.4cm
Post-op 1M 14.4cm

• Acute type A dissectionAcute type A dissection
• Chronic type B dissection Chronic type B dissection --
indicated for TEVAR with no indicated for TEVAR with no suitable proximal landing suitable proximal landing site at zone 2site at zone 2
Hybrid TEVAR for the Hybrid TEVAR for the Treatment of Aortic Treatment of Aortic
DissectionDissection
Chronic Type B Chronic Type B DissectionDissection
• Mortality with nearly one in four patients (24.9%) within 3 years
• The poor long-term prognosis is determined by patient-specific risk factors and dissection-related late sequelae in 20-50% of patients, including new dissection associated with new complications, rupture of a weak false channel and saccular or fusiform aneurysmal degeneration
- Ann Thorac Surg 2002;74;S1840-3, 1857-63
- N Engl J Med 2007;357:349-59
Contemporary Results of Open Repair of DTA
On the basis of 1898 reported cases in the hands of experienced surgeons•Mortality rate 4.8%•Stroke rate 2.7%•Lower extremity paralysis rate 3.4%•Overall 5 and 10-year survival estimates are 60% and 38%
Contemporary Results of Contemporary Results of Open Repair of DTAOpen Repair of DTA
• US Medicare data analysis Mortality risk 20% at 30 days and 31%
at 12 months (J Vasc Surg 2006;43:217-222)
• UK National adult cardiac surgical database in 2000
31.5% mortality rates for descending aorta replacement
Contemporary Results of Contemporary Results of TEVARTEVAR
A Meta-analysis in Aortic Dissection
(Eur Heart J 2006;27:489-98)
• 39 published studies, 609 patients• 96% type B dissection (58% acute, 42% chronic)• Procedure success 98.2+0.5%• 30-day mortality 5.3%• Stroke 1.9% and paraplegia 0.8%• False lumen thrombosis 75.5%• Total re-intervention rate 11.9%• Aortic rupture during follow-up 2.3%
Endoleak in TEVAR for Endoleak in TEVAR for Type B Aortic DissectionType B Aortic Dissection
• The prognosis of type I endoleak is poor and all efforts to avoid it should be made
• The shorter the distance between the opening of the LSCA and the entry tear, the greater the chance of an endoleak
- J Thorac Cardiovasc Surg 2010;139:1548-53
Hybrid TEVAR for Type Hybrid TEVAR for Type B Aortic DissectionB Aortic Dissection
• Sternotomy to create secure proximal landing zone, including in situ supra-aortic arteries bypass and aortic banding
• TEVAR for DTA tear coverage to induce the false lumen thrombosis and to promote the aortic remodeling
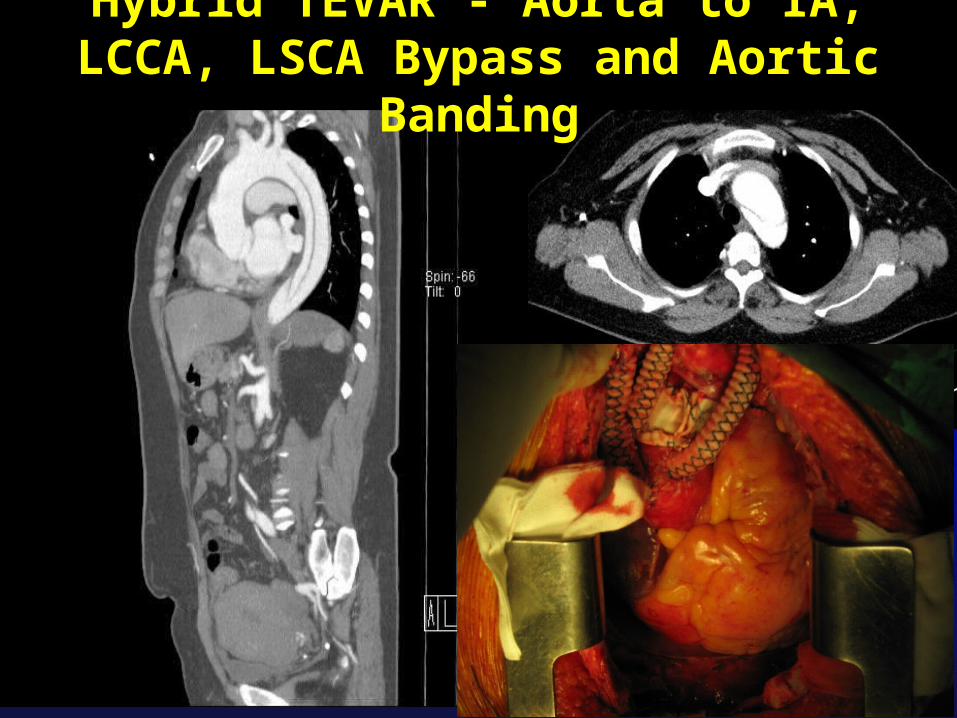
Hybrid TEVAR - Aorta to IA, LCCA, LSCA Bypass and Aortic Banding
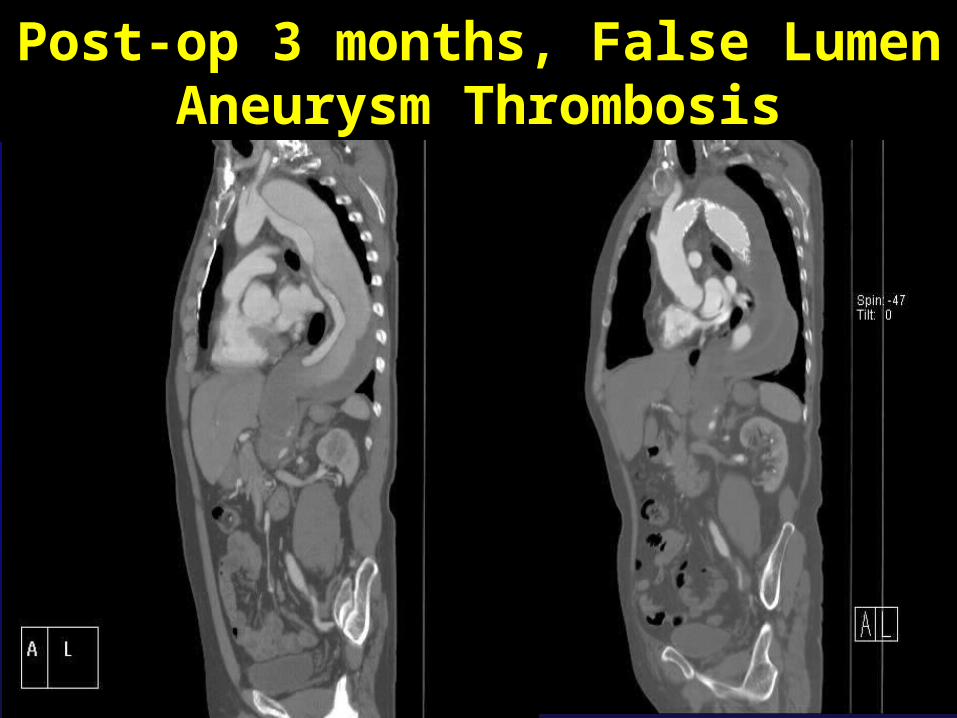
Post-op 3 months, False Lumen Aneurysm Thrombosis
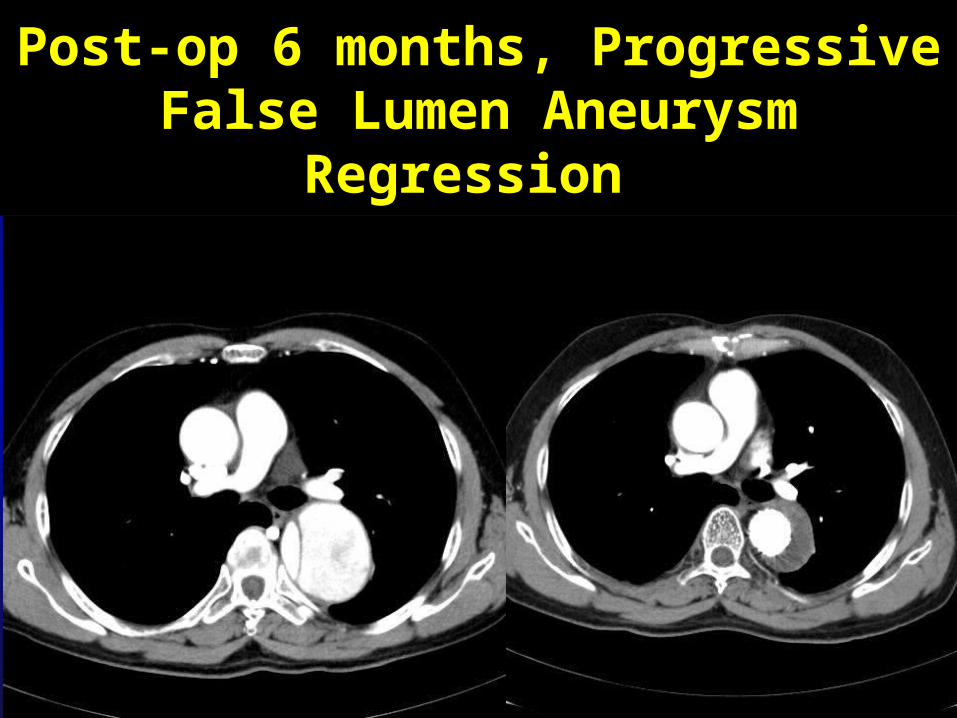
Post-op 6 months, ProgressiveFalse Lumen Aneurysm
Regression
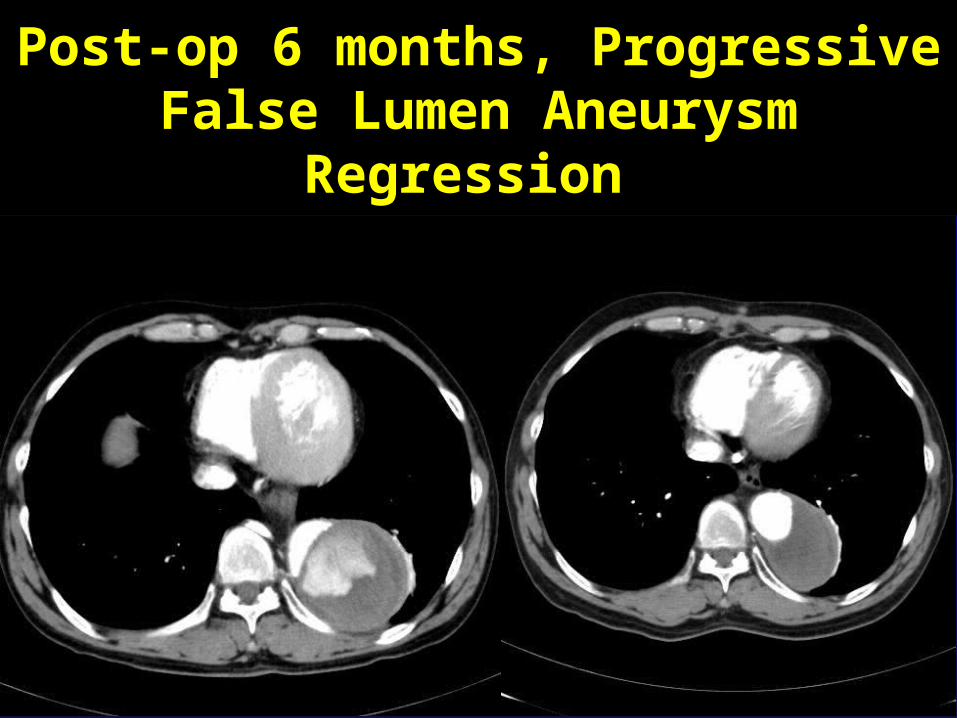
Post-op 6 months, ProgressiveFalse Lumen Aneurysm
Regression
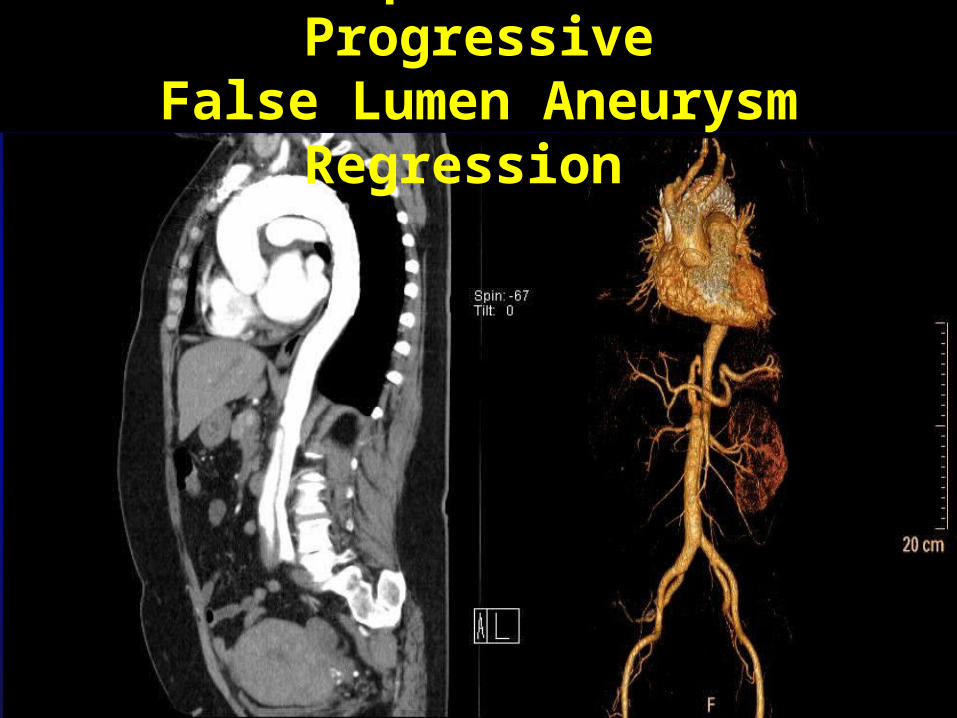
Post-op 12 months, Progressive
False Lumen Aneurysm Regression
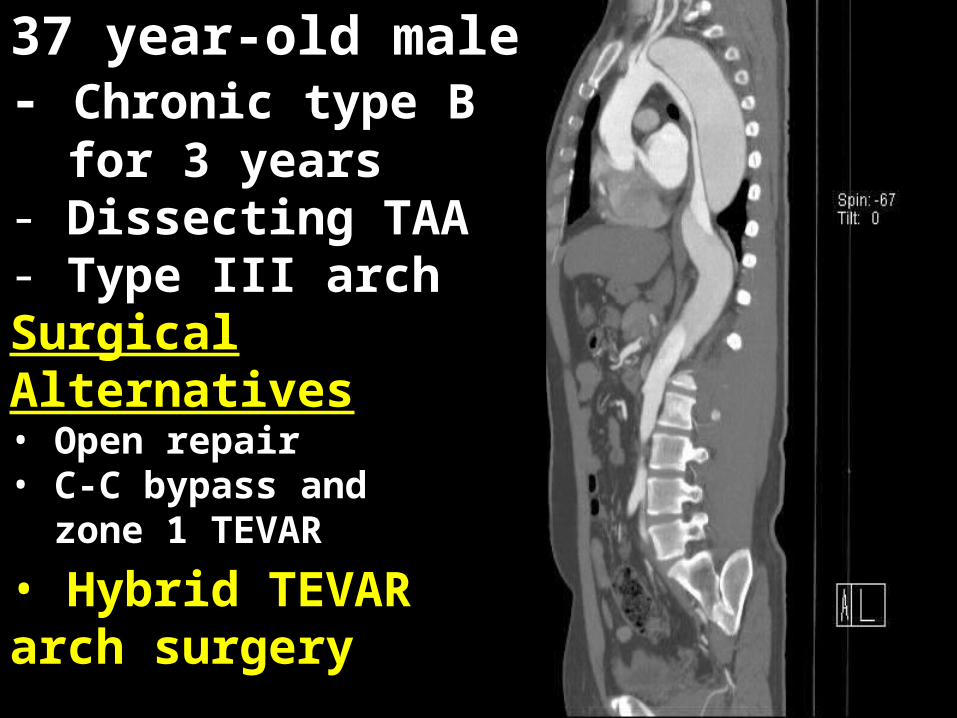
37 year-old male- Chronic type B for 3 years- Dissecting TAA- Type III archSurgical Alternatives• Open repair • C-C bypass and zone 1 TEVAR
• Hybrid TEVAR arch surgery

Ascending and proximal arch replacement,
arch debranching and TEVAR
Antegrade TEVAR
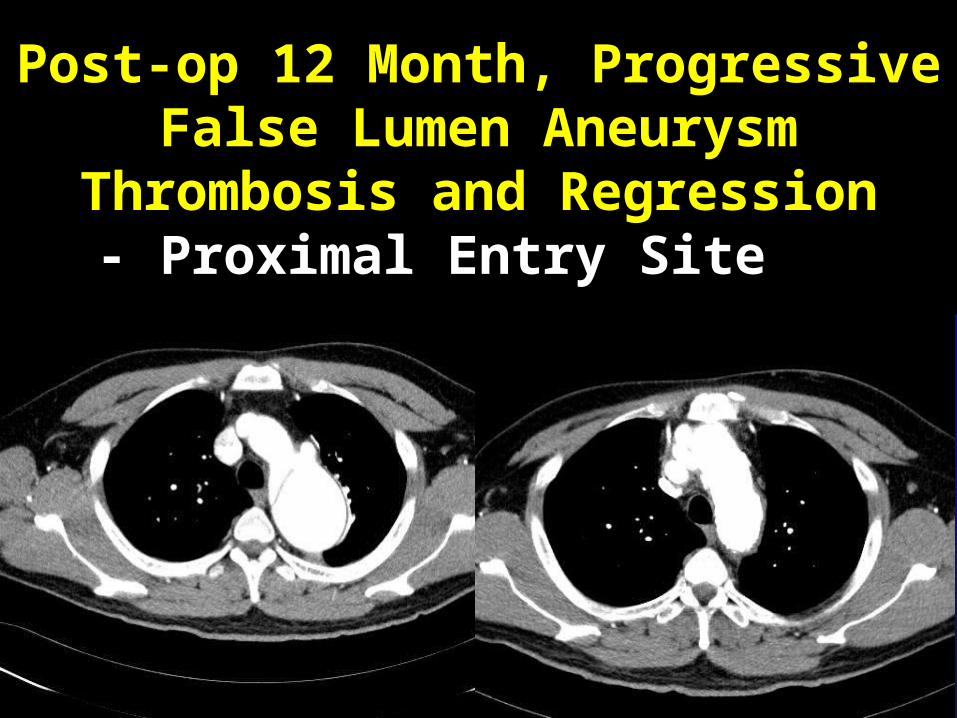
Post-op 12 Month, ProgressiveFalse Lumen Aneurysm
Thrombosis and Regression- Proximal Entry Site
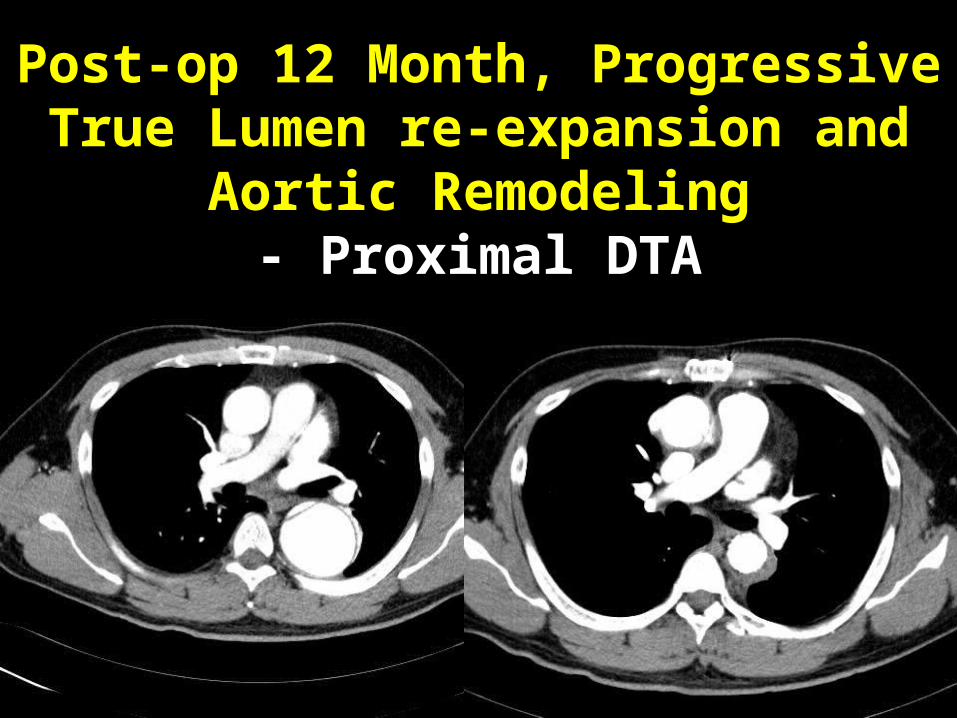
Post-op 12 Month, ProgressiveTrue Lumen re-expansion and
Aortic Remodeling- Proximal DTA
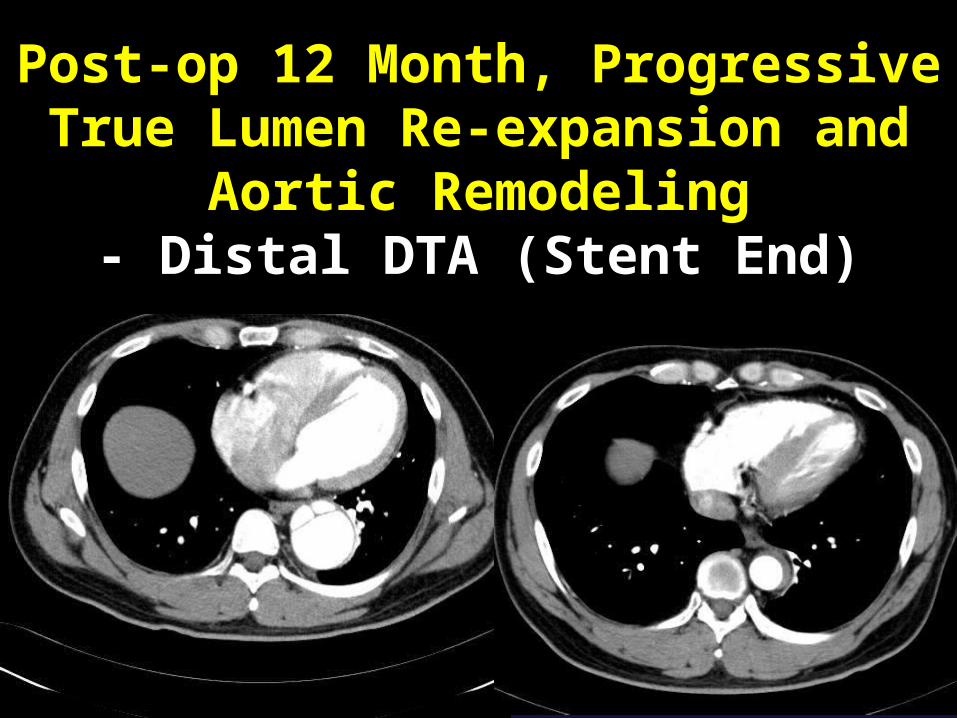
Post-op 12 Month, ProgressiveTrue Lumen Re-expansion and
Aortic Remodeling- Distal DTA (Stent End)

Post-op 12 Month, ProgressiveFalse Lumen Aneurysm
Thrombosis and Regression- Distal DTA
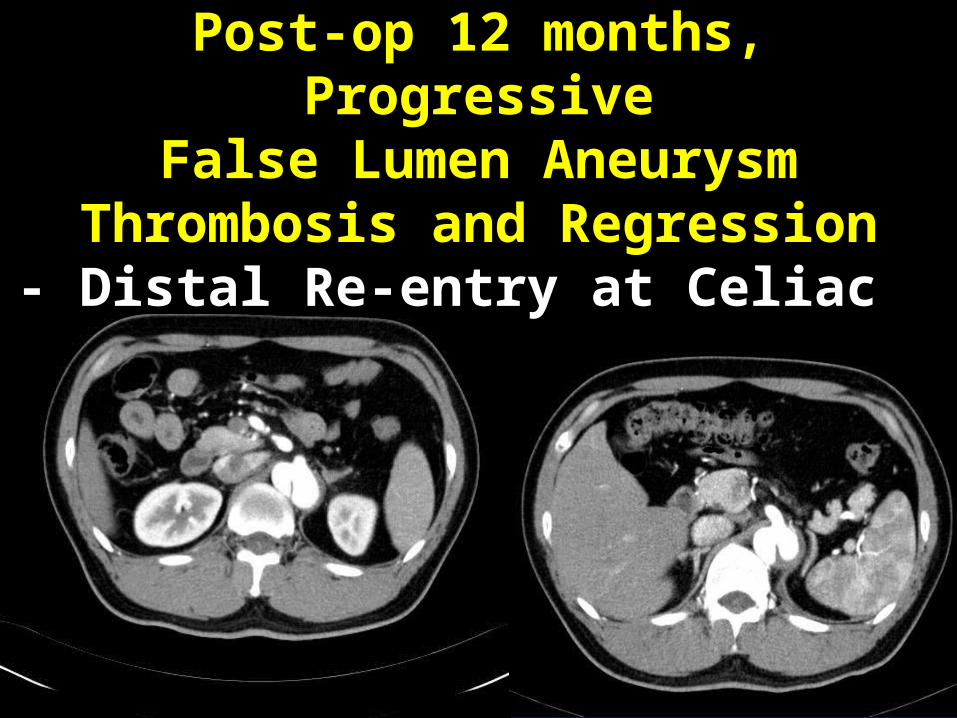
Post-op 12 months, Progressive
False Lumen Aneurysm Thrombosis and Regression- Distal Re-entry at Celiac

Post-op 18 months, Positive Aortic Remodeling
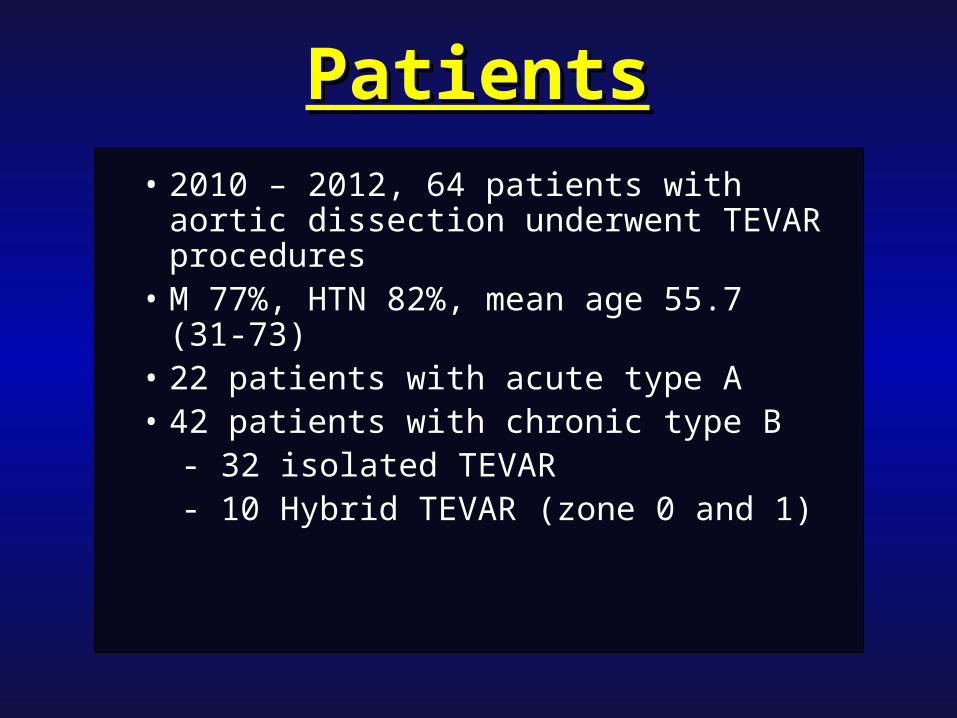
PatientsPatients• 2010 – 2012, 64 patients with aortic
dissection underwent TEVAR procedures
• M 77%, HTN 82%, mean age 55.7 (31-73)
• 22 patients with acute type A • 42 patients with chronic type B - 32 isolated TEVAR - 10 Hybrid TEVAR (zone 0 and 1)
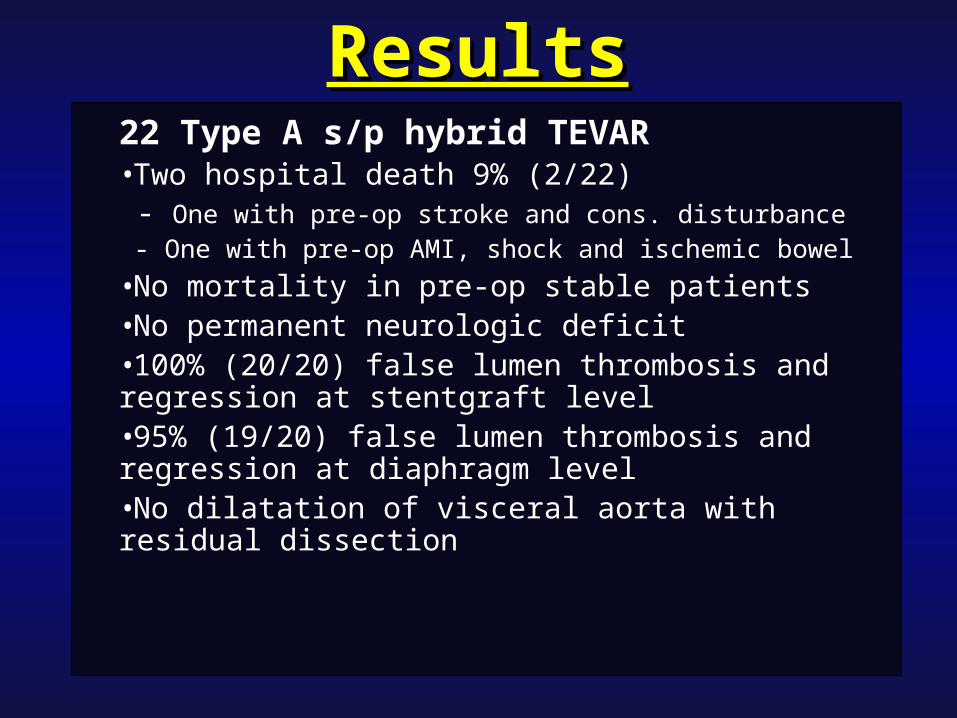
ResultsResults22 Type A s/p hybrid TEVAR•Two hospital death 9% (2/22) - One with pre-op stroke and cons. disturbance - One with pre-op AMI, shock and ischemic bowel
•No mortality in pre-op stable patients•No permanent neurologic deficit•100% (20/20) false lumen thrombosis and regression at stentgraft level•95% (19/20) false lumen thrombosis and regression at diaphragm level•No dilatation of visceral aorta with residual dissection

F
Post-op 1M
F
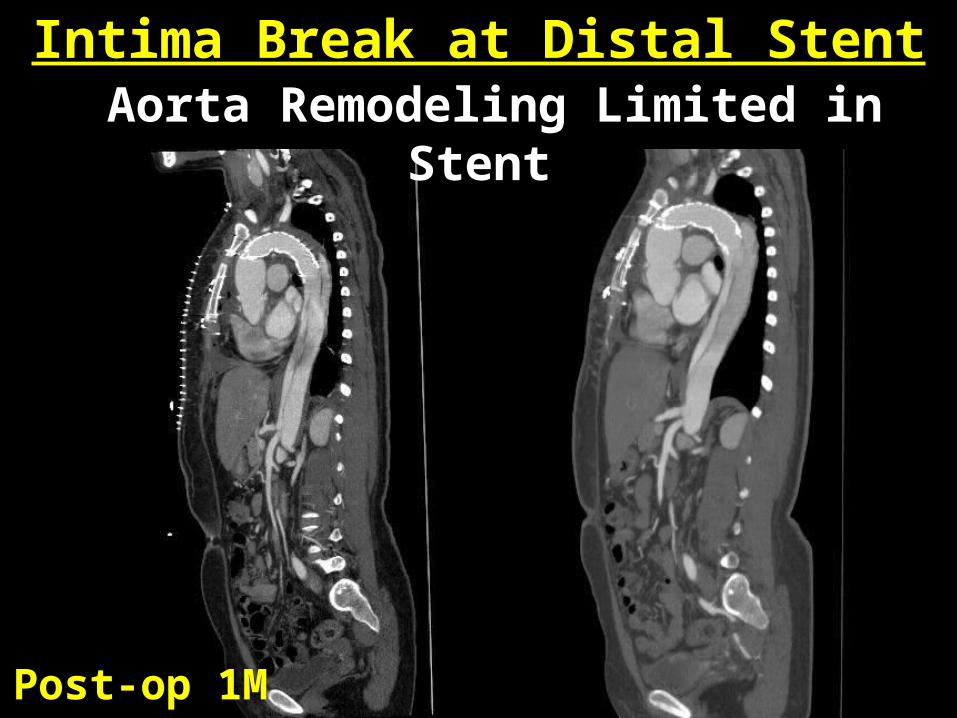
Intima Break at Distal Stent Aorta Remodeling Limited in
Stent
Post-op 1M
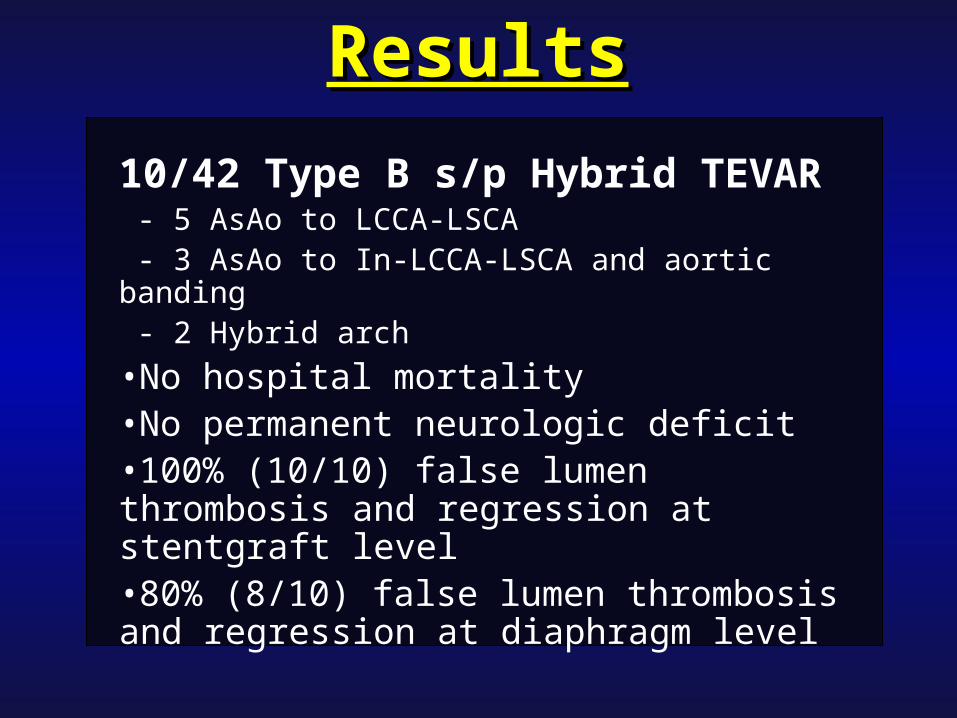
ResultsResults
10/42 Type B s/p Hybrid TEVAR - 5 AsAo to LCCA-LSCA - 3 AsAo to In-LCCA-LSCA and aortic banding - 2 Hybrid arch
•No hospital mortality•No permanent neurologic deficit •100% (10/10) false lumen thrombosis and regression at stentgraft level•80% (8/10) false lumen thrombosis and regression at diaphragm level
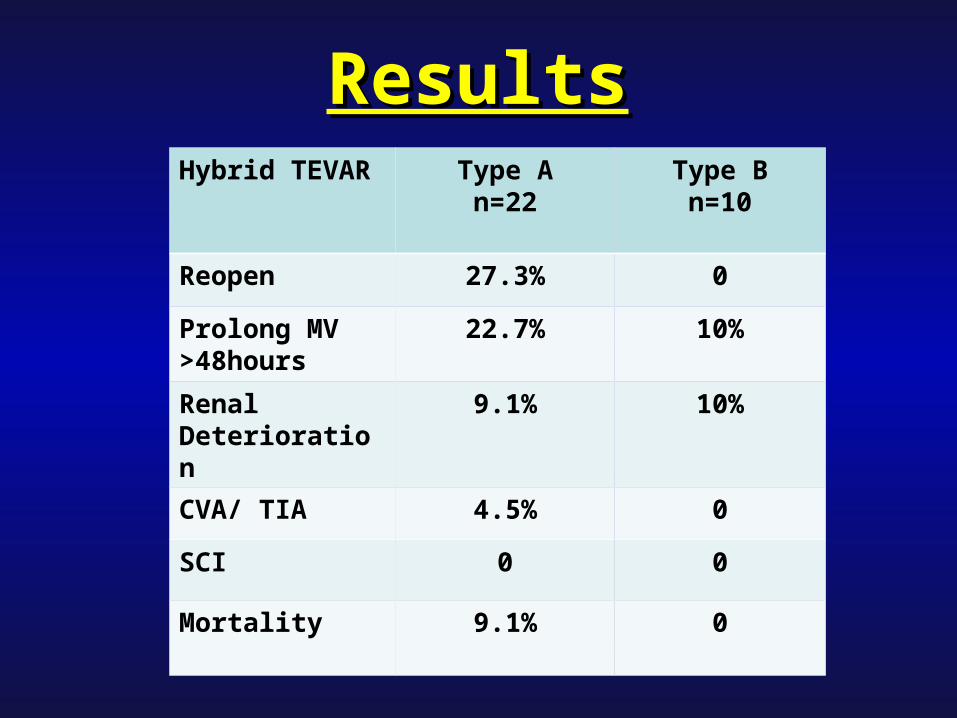
Hybrid TEVAR Type An=22
Type Bn=10
Reopen 27.3% 0
Prolong MV >48hours
22.7% 10%
Renal Deterioration
9.1% 10%
CVA/ TIA 4.5% 0
SCI 0 0
Mortality 9.1% 0
ResultsResults

Hybrid TEVAR Hybrid Aneurysm
n=33
Hybrid Dissection
n=7
MI 6% 0
Respiratory failure
33% 20%
Renal failure 15% 20%
CVA/ TIA 18% 40%
SCI 15% 0
Mortality 24% 0
Hybrid TEVAR: Pushing the Hybrid TEVAR: Pushing the EnvelopEnvelop
(J Vasc Surg 2010;51:259-66)(J Vasc Surg 2010;51:259-66)
ConclusionConclusion• Hybrid Arch surgery with
modified four-branched graft technique and TEVAR provided favorable early and mid-term outcomes in type A dissection
• Single-stage operation combined with antegrade TEVAR is feasible and effective to extend the repair down to the descending aorta
ConclusionConclusion
• Hybrid procedures successfully extend the TEVAR applications in type B dissection patients with no suitable proximal landing zone
• For younger patients population in type B aortic dissection, hybrid TEVAR is safe and demonstrates satisfactory early and mid-term results
Thanks for Thanks for Your Your
AttentionAttention