Ring Enhancing Lesions
50
Approach to ring enhancing lesion CT/MRI Speaker. Dr. Vivek kumar gupta Moderator .Dr Deepak Sachan(asst. prof.) Dr vivek chaudhary (SR)
-
Upload
vivek-gupta -
Category
Documents
-
view
45 -
download
7
Transcript of Ring Enhancing Lesions

Approach to ring
enhancing lesion CT/MRI
Speaker. Dr. Vivek kumar gupta
Moderator .Dr Deepak Sachan(asst. prof.)
Dr vivek chaudhary (SR)

Ring Enhancing lesions
Lesions having hypodense centre
with hyperdense
sorrounding on contrast CT/MRI scan of the brain.

CausesA) Infectious Neurocysticercosis (NCC)
Tuberculoma
Brain abscess
Toxoplasmosis
Fungal granuloma
Syphilitic gumma
Nocardia
Actinomycosis
Cryptococcus neoformans
Candida Albicans
Aspergillosis
Mucoromycosis
B) Neoplastic Lymphoma
Glioma
Metastasis
C) Degenerative Demyelinating plaques
Ring Enhancing lesions

Neurocysticercosis
Most common CNS parasitic infection (60-70%)
Endemic in Central South America, Parts of Asia, EasternEurope, in developed countries due to immigrants fromendemic areas.

Mode of infestation
Contaminated food or water
with eggs of pork tapeworm
Oncospheres in Gut
(Primary larvae)
Intestinal mucosa
Circulatory system
Muscle EyeBrain

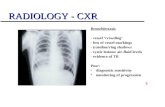
Right frontal inflammatory
granuloma
Neurocysticercosis
Location
1) Parenchymal (MC ) in corticomedullary region
2) Extraparenchymal
a) In ventricle
b) In basal cistern(racemose cysticercosis)

Pathologic stages of parenchyma cysticercosis
Vesicular stage
First stage, cysticercus consist of a thin capsulethat surrounds a viable larva and clear fluid.

IInd pathological stage
Vesicular Colloidal stage
Dead larvum degenerates,the cystic fluid becomesturbid, cyst shrinks, capsulethickens.
Degenerating larvae releasemetabolic products resultinghost inflammatory response(surrounding edema).

Pathologic stage IIIrd
Granular nodular stage
Cyst retracts thickens and calcifies.

IVth pathological stage
Nodular calcified stage
Granulomatous lesion has contracted small calcified nodule without enhancement effect is visible on CT.

Diagnosis criteria advised by de brutto et al,2001
1. Absolute criteria 2. Major criteria3. Minor criteria 4. Epidemiological criteria

Diagnosis of Neurocysticercosis
Neuroimaging is the mainstay of diagnosis
Absolute Diagnostic Criteria
Histological demonstration of theparasite from biopsy of brain.
Cystic lesions with scolex on CT or MRI
Direct visualization of subretinalparasite by fundoscopy.

Diagnosis of neurocysticercosis
Major Criteria
CT or MRI showing cystic lesions without scolex,enhancing lesions or typical brain calcifications.
Positive serum immunoelectrotransfer blot(EITB)
for detection of anticysticercal antibodies.
Resolution of cysts after antiparasite therapy.
Spontaneous resolution of small single enhancinglesions.

Diagnosis of neurocysticercosis
Minor Criteria
CT or MRI showing hydrocephalus or abnormalenhancement of meninges.
Seizures, focal signs, intracranial hypertension anddementia.
Positive CSF ELISA for anti cysticercal antibodies.
Cysticercosis outside the CNS.
Epidemiologic Criteria
Evidence of household contact with Taenia soliuminfection.
Individual coming from living in an endemic area,
History of travel to an endemic area.

Diagnosis of neurocysticercosis
Definitive
Presence of one absolute criterion (1/3).
Two major (2/4) + one minor (1/4) and + oneepidemiologic criteria (1/3).
Probable
Presence of one major + two minor criteria.
One major + one minor and + one epidemiologiccriteria.
Three minor + one epidemiologic criteria.

Can CT differentiate between tuberculoma
and Neurocysticercosis
Not with certainty, factors may be taken into account are-
NCC TUBERCULOMA
Location Parietal (subcortical interface), temporal, Frontal, Occipital
Basal regions in posterior fossa in younger children
Number Single or more Often multiple, satellite lesion
Size Smaller Larger (over 20mm)
Wall Smooth Thicker and shaggy
Cystic component
In early stage Not there
Mid line shift Usually not May

Is the MRI scan more helpful in thedifferential diagnosis?
1. Contrast MRI may be able to identify smaller lesions that areoccasionally missed by CT.
2. Single REL on the CT scan might actually turn out to be multiplelesions on the MRI.
3. RELs which have disappeared on follow up CT scans, are oftenpicked up on high resolution contrast MRI.
4. MRI characteristics – Tuberculomas typically demonstratehypointensity centrally due to caseating material. While NCC inearly stage is hyperintense.
5. MR Spectroscopy – Identifies specific biochemical
components in the granuloma. Tuberculomas typically have lipidand lactate peaks.
6. MRI also carries the advantage of lack of radiation exposure.

MRI is also associated with certaindisadvantages
1. Calcification, often missed by MRI which is importantfor differentiating between NCC and tuberculoma. For staging the parasitic lesions and Judging the effects of therapy.
2. Longer scan time, so child should be cooperative orneed to use anesthetic agents.
3. Higher cost.
Thus, CT and MRI both may need to be performed formaximizing information yield.
If there are financial constraints, it is better to perform a CTscan with contrast study.
One should remember that a non contrast MRI is inferior to acontrast enhanced CT.

Are there any other tests that can helpdifferentiate between NCC & tuberculoma?
1. Serological tests (on blood or CSF samples)
a) Serum EITB(enzyme immunotransfer blot assay) specifity 100% ,
sesitivity 90% in >2 lesion , sensitivity 70% with single lesion
b) Hp 10 antigen assay helpful in diagnosis and follow up with treatment
with sever neurocysticercosis.
c) PCR in csf is under study.
2. Radiological scans of thigh muscles or stool examination for detecting
cysticercal disease elsewhere is usually unrewarding.
3. Finding the evidence of tuberculosis elsewhere in the body, may be
useful.

What is the place of biopsy in the
evaluation of a child with REL?
1. If there is a strong suspicion of a tumor.
2. Remains symptomatic or worsens while
on therapy,
3. If the lesion persists or increases in size
despite therapy on CT /MRI.

Is there a role for repeating theimaging procedure?
When the diagnosis of the REL is uncertain,repeating the imaging procedure after 3 monthsprovides clues.
Disappearance or evolution of imagingcharacteristics in REL can help diagnose NCC.
REL with edema Granular nodular stage Finally calcified stage

Neurocysticercosis
Clinical manifestations
Usually due to cerebral oedema as a result of
intense host inflammatory response towards
dead larvae.
Epilepsy is the most frequent symptom (50 to
80%).
Simple or complex partial in half the cases.
Other symptom is hemiparesis,symptom of
raised ICT (papilledema ,headach ,vomitting)

Guidelines for antiparasite treatment of neurocysticercosis
Type Infection burden
Recommendation evidence
Parenchymal (cyst)
Mild (1-5 cyst)
Larvicidal+steriod II-3
Larvicidal+steroid only if therapy related side effect
II-3
No larvicidal therapy , only radiological follow up
II-3
Moderate(>5 cyst)
Consesus: larvicidal + steroid II-3
>100 cyst heavy cyst
larvicidal +high dose steroid III
Chronic steroid treatment ,no larvicidal, neuroimaging follow up
III

Guidelines for use of anti parasite treatment in neurocysticercosis
ctd
Type Infection burden
Recommendation Evidence
Enhancing lesion(degenratingcyst)
Mild or moderate
A. Neuro imaging follow up , no larvicidal
I
B. Larvicidal with steriod II-3
C. Larvicidal , steroid only if side effect develop
II-3
Heavy (cysticercoticencephalitis)
Consensus No larvicidal , high dose steroid and osmotic diuretic
III
Calcified cysticerci Any number Consensus No larvicidaltherapy
III

Guidelines for use of antiparasitetreatment in neurocysticercosisType Infection
burdenRecommendation Evidence
Ventri cularneurocysticercosis
Cosensus :Neuro endoscopic removal when avaliable if not avliable then following option
III
CSF diversion followed by anti parasite treatment
III
Open surgery (for mainly ventricular cyst)
II-3
Sabarachinoidcyst (gaint cyst , racemose cyst)
Larvicidal+steroid+VPshunt if hydrocephalous
III

Guidelines for use of antiparasitictreatment in neurocysticercosis
Type Infection burden
Recommendation Evidence
Spinal (intra or extra medullary)
Consensus: Primary surgical
III
Ophthalmic cysticercosis
Consensus: Surgical resection of cyst
II-3

Cysticidal drugs
Drugs Dose Duration Efficacy
Praziquantel 50 mg/kg/d 15 days 60-70%
Albendazole 15mg/kg/d 28 days (recent data 1 wk)
75-90%

Condition where csyticidal drug is not used
1. ocular cysticercosis2.cysticercous encephalitis

Any adverse effects of cysticidal therapy?
Increased seizure frequency
Rise in ICT
Due to the host response following
destruction of parasite leading to release
of metabolic products.

Corticosteroids in NCC
Oral prednisolone is preferred and started2-3 days before cysticidal therapy andcontinued for 7 days.
However, high dose corticosteroids are theprimary therapy for cysticercoticencephalitis.
It also has role in presence of raised ICT.

Antiepileptic drugs
1. Carbamazepine, phenytoin
Duration
1) Provocative lesions : 6 months
2) Nonprovocative lesions : 2-3 years

Prognosis
1. Nearly, 85% of patients with single granulomahave a good seizure outcome.
2. Patients with more than two seizures, andthose whose follow up CT scan shows a calcificresidue of the granuloma, have a higher risk ofrecurrence and therefore epileptic drugs to begiven for longer duration.
3. The outcome of patients with multiple braincysts and extraparenchymal NCC depends uponthe location and severity of infestation.

What is the ultimate imagingoutcome?
High end CT and MRI suggests lesions
often calcify but do not disappear.
Occasionally heal with gliosis, a risk
factor for chronic epilepsy.

TuberculomasIncidence
Upto 40% of brain ICSOL, usually supratentorial in older and infratentorial in younger.
Presentation
Fever
As slowly expending mass lesions ( ICT in 25%)
Headache, Visual or gait disturbances
Seizures usually partial (75%)
Focal neurological defects
Diagnosis
Mx usually positive
X-ray chest – evidence of pulm disease (40-50%)
X-ray skull – calcification in 6%
CT scan/MRI – REL
Serology – ELISA
PCR for mycobacterium tuberculosis DNA

Treatment –
ATT for 1 year(2 HRZE 10 HR)
Corticosteroids for 8 to 10 week
Prognosis – Complete disappearance in majority in CT scan after one year.

Brain abscess
It is focal ,suppurative infection within brain parenchyma surrounded by vascular capsule
Age :- any age but most common age group is 4-8yr
Etiology:-
1. Direct spread:- eg mastoiditis ,chr ottitis media, sinusitis, dental infection.
2. Head trauma or neuro surgical procedure
3. Hematogenous spread:- congenital heart disease with right to left shunt eg. tetralogy of fallot.it usually lies at junction of gray and white matter
4. cryptogenic

Brain abscess
Stages :
Early cerebritis:- perivascular infilteration of inflammatory cell,which sarround a central core of coagulative necrosis,with marked edema
Late cerebritis:- pus formation lead
to enlargement of necrotic centre.
Stage of late cerebritis - ill defined
capsule with large surrounding edema.

Brain abscess
Early capsule formation:-
Formation of capsule that is better developed on cortical side
This stage correlate with appearance of ring enhancing capsule on neuroimaging.
CT with contrast. Note the large wall-enhancing abscess in the left
frontal lobe. The lesion is causing a shift of the brain to the right.
The patient had no neurologic signs
until just before the CT scan because the abscess is located in the
frontal lobe, a “silent” area of the brain
Late capsule formation:-
characterised by well defined
necrotic centre surrounded by
dense collagenous capsule .
Edema regress.
Stage of capsule formation -
well defined ring enhancement

•Brain abscess C/F : fever , head ach ,vomiting ,focal neurological deficit depending
on location of abscess.
Lab diagnosis:-
CSF :-it should not be done if brain abscess suspected because it is seldom useful and due to risk of herniation
WBC and protein:- normal or minimally elevated
Glucose :- normal or decreased
CSF culture rarely positive.
Blood culture :- positive in 10%
Bacteriological diagnosis :- by culture of aspirated pus
CT with contrast /MRI :- most reliable ( MRI investigation of choice)

Brain abscess
Treatment:-conservative management done if abscess <2cm ,short
duration illness(<2wk),no sign of ICT , child is neurologically intact
Emperical :- vancomycin+third gen.cephalosporin
+metronidazole
abscess after head trauma / neurosurgery :-
vancomycin +third gen. cephalosporin
Abscess in cyanotic heart disease:-
ampicillin-sulbactam /third gen. cephalosporin
+metronidazole
Abscess in VP shunt:- vancomycin +cefitizidime

Brain abscess Encapsulated causing mass effect :- treat with antibiotic and
aspiration
Surgery is indicated if abscess is>2.5 cm , gas in abscess , multiloculated, located in posterior fossa , or fungus is identified
Duration of antibiotic therapy depend on organism and response to treatment , usually 4-6 wk .

Nocardiosis:-mostly in immunocompromised persons, and produces poorly capsulated, frequently multiloculated, liquefied abscesses in the brain.
Syphilitic gumma:-
may be a solitary circumscribed lesion in the brain, but this lesion
would be unusual without evidence of syphilis elsewhere.
Actinomycosis:-
invades the nervous system in 1 to 3 % patients with systemic
infection, produces a well encapsulated pus filled cavity containing characteristic sulphur granules. Evidence of cervicofacial, thoracic or abdominal disease is invariably present

Candida albicans:-Immunocompromised host
multiple parenchymal brain abscess or granulomas . Resembles tuberculoma
Candida granuloma tends to be located predominantly in white matter rather
than in the cortex
Usually associated with spinal fluid pleocytosis. Evidence of candidiasis elsewhere in body should be present.
Acquired toxoplosmosis:-Immunocompromised host cicumscribed microglial nodule hemmorragic and necrotic lesion in parenchyma

Aspergillosis:-
bronchopulmonary infection in immune compromised patients can
also result in solitary or multiple brain abscesses which progress toform granuloma that may calcify.
Mucormycosis:-in uncontrolled diabetic
produces intracerebral granuloma

Metastatic Tumors:-often multiplefew appear hyperdense on CT scan
marked oedema
and mass effect on CT scan, no calcificationevidence of primary should be present.
Primary brain tumour:- especially oligodendroglioma is likely
to calcify and produce hyperdense lesion on CAT scan

Ring enhancing lesion on CT/MRI
Scolexpresent
NCC
Scolex absent
Correlate clinicaly and plan for other supportive evidence (EITB/ELISA NCC,
MONTOUX , X-ray chest , PCR /ELISA for tuberculosis)
EITB /ELISA +VE
NCC
Montoux ,x ray,ELISA/PCR s/o TB –tuberculoma
None of above + think of other
causes

Message :-
CT/MRI should be correlated with clinical finding , serological finding and other supportive evidence of disease for diagnosis

Bibliography Nelson text book of pediatrics vol 1 ,18th editionIAP test book of pediatrics 3rd edition clinical microbiology review ,oct,p.747-756 vol .15 no 4indian journal of tuberculosis,1996,43,45journal of indian academy of pediatrics vol 43,march 17,2006,227-23essential tuberculosis in children (vimlesh seth. Sk kabra)