Rhinitis Alergic
26
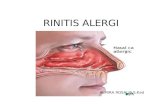
Rhinitis Alergic Allergic rhinitis (AR) is an inflammatory disorder of the nasal mucosa characterized by nasal congestion, rhinorrhea, and itching, often accompanied by sneezing and conjunctival irritation. Its categorization as a major chronic respiratory disease of children is predicated on its high prevalence, detrimental effects on quality of life and school performance, and co-morbidities. Children with AR often have related sinusitis, conjunctivitis, otitis media, serous otitis, hypertrophic tonsils and adenoids, and eczema. Childhood allergic rhinitis is associated with at least twofold increase in risk for asthma at an older age. Over the past 40 yr an upsurge in AR has taken place throughout the world, sparing rural and underdeveloped regions. In prosperous societies, 20-40% of children suffer from AR. Its symptoms may appear in infancy, with the diagnosis generally established by the time the child reaches age 6 yr. The prevalence peaks late in childhood. Risk factors include family history of atopy and serum immunoglobulin (Ig) E higher than 100 IU/mL before age 6 yr. The risk increases in children introduced to foods or formula early in infancy, those whose mothers smoke heavily, especially before the children are 1 yr old, and those with heavy exposure to indoor allergens. A critical period appears to exist early in infancy when the genetically susceptible individual is at greatest risk of sensitization. Breast-feeding of high-risk infants and exposure to dogs, cats, and endotoxin early in childhood protect against atopy and early wheezing. Delivery by cesarean section is associated with allergic rhinitis and atopy among children with a parental history of asthma or allergies. This association may be explained by the lack of exposure to maternal vaginal/fecal flora during delivery. Children between 2 and 3 yr old who have elevated anti-cockroach and anti-mouse IgE are at increased risk of wheezing, rhinitis, and atopic dermatitis. The occurrence of 3 or more episodes of rhinorrhea in the first year of life is associated with allergic rhinitis at age 7 yr. Early life exposures or their absence have a profound influence on the development of the allergic phenotype.
-
Upload
zakia-imani -
Category
Documents
-
view
220 -
download
0
description
reghd
Transcript of Rhinitis Alergic

Rhinitis Alergic
Allergic rhinitis (AR) is an inflammatory disorder of the nasal mucosa characterized by nasal congestion, rhinorrhea, and itching, often accompanied by sneezing and conjunctival irritation. Its categorization as a major chronic respiratory disease of children is predicated on its high prevalence, detrimental effects on quality of life and school performance, and co-morbidities. Children with AR often have related sinusitis, conjunctivitis, otitis media, serous otitis, hypertrophic tonsils and adenoids, and eczema. Childhood allergic rhinitis is associated with at least twofold increase in risk for asthma at an older age. Over the past 40 yr an upsurge in AR has taken place throughout the world, sparing rural and underdeveloped regions. In prosperous societies, 20-40% of children suffer from AR. Its symptoms may appear in infancy, with the diagnosis generally established by the time the child reaches age 6 yr. The prevalence peaks late in childhood. Risk factors include family history of atopy and serum immunoglobulin (Ig) E higher than 100 IU/mL before age 6 yr. The risk increases in children introduced to foods or formula early in infancy, those whose mothers smoke heavily, especially before the children are 1 yr old, and those with heavy exposure to indoor allergens. A critical period appears to exist early in infancy when the genetically susceptible individual is at greatest risk of sensitization. Breast-feeding of high-risk infants and exposure to dogs, cats, and endotoxin early in childhood protect against atopy and early wheezing. Delivery by cesarean section is associated with allergic rhinitis and atopy among children with a parental history of asthma or allergies. This association may be explained by the lack of exposure to maternal vaginal/fecal flora during delivery. Children between 2 and 3 yr old who have elevated anti-cockroach and anti-mouse IgE are at increased risk of wheezing, rhinitis, and atopic dermatitis. The occurrence of 3 or more episodes of rhinorrhea in the first year of life is associated with allergic rhinitis at age 7 yr. Early life exposures or their absence have a profound influence on the development of the allergic phenotype.
Etiology
Two factors necessary for expression of AR are sensitivity to an allergen and the presence of an allergen in the environment. AR is currently classified as seasonal (SAR) or perennial (PAR), although these terms may soon be replaced by intermittent allergic rhinitis (IAR) and persistent rhinitis (PER). The 2 sets of terms are based on different premises, but inhalant allergens are the main cause of all forms of rhinitis irrespective of the terminology. SAR follows a well-defined course of cyclical exacerbation, whereas PAR causes year-round symptoms. Approximately 20% of cases are strictly seasonal, 40% perennial, and 40% mixed (perennial with seasonal exacerbations). In temperate climates, airborne pollens responsible for SAR appear in distinct phases: trees pollinate in the spring, grasses in the early summer, and weeds in the late summer. In temperate climates, mold spores persist outdoors only in the summer, and in warm climates, mold spores persist throughout the year. Symptoms of seasonal allergies cease with the appearance of frost. Knowledge of the occurrence of seasonal symptoms, of the regional patterns of pollination and mold sporulation, and of the patient's specific IgE is necessary to recognition of the cause of SAR. PAR is most often associated with the indoor allergens: house dust mites, animal danders, mice, and cockroaches. Cat and dog allergies are of major importance in the United States. The allergens from the saliva and sebaceous secretions may remain airborne for a

prolonged time. The ubiquitous major cat allergen, Fel d 1, may be carried on cat owners’ clothing into such “cat-free” settings as schools and hospitals.
Pathogenesis
The exposure of an atopic host to an allergen leads to specific IgE production. The clinical reactions on re-exposure to the allergen have been designated as early-phase and late-phase allergic responses (EPRs and LPRs). Bridging of the IgE molecules on the surface of mast cells by allergen initiates EPR, characterized by degranulation of mast cells and release of preformed and newly generated inflammatory mediators including histamine, prostaglandin 2, and the cysteinyl leukotrienes. LPR arises 4 to 8 hr following allergen exposure. Inflammatory cells, including basophils, eosinophils, neutrophils, mast cells, and mononuclear cells, infiltrate the nasal mucosa. Eosinophils release proinflammatory mediators, including cysteinyl leukotrienes, cationic proteins, eosinophil peroxidase, and major basic protein, and serve as a source of interleukin-3 (IL-3), IL-5, granulocyte-macrophage colony-stimulating factor (GM-CSF), and IL-13. Repeated intranasal introduction of allergens causes “priming”—a brisk response to reduced provocation. Over the course of an allergy season a multifold increase in epithelial and submucosal mast cells takes place. These cells were once thought to have a role exclusively in the EPR but now appear to have an important function in sustaining chronic allergic disease. Allergens, autoantigens, and components of superimposed infectious agents activate the immune system. Immune regulation in the lymphatic organs and in the tissue has an important role in the control and suppression of allergic disease in all stages of the inflammatory process, such as inflammatory cell migration to tissues, inflammatory cell–mediated destruction in tissues, and inflammatory cell interaction with resident tissue cells to enhance inflammation.
Clinical Manifestations
Symptoms of AR are often ignored or are mistakenly attributed to a respiratory infection. Older children blow their noses, but younger children tend to sniff and snort. Nasal itching brings on grimacing, twitching, and picking of the nose that may result in epistaxis. Children with AR often perform the allergic salute, an upward rubbing of the nose with an open palm or extended index finger. This maneuver relieves itching and briefly unblocks the airway. It also gives rise to the nasal crease, a horizontal skin fold over the bridge of the nose. The diagnosis of AR is based on symptoms in the absence of an upper respiratory tract infection and structural abnormalities. Typical complaints include intermittent nasal congestion, itching, sneezing, clear rhinorrhea, and conjunctival irritation. Symptoms increase with greater exposure to the responsible allergen. The patients may lose their senses of smell and taste. Some experience headaches, wheezing, and coughing. Nasal congestion is often more severe at night, causing mouth-breathing and snoring, interfering with sleep, and inciting irritability.
Signs on physical exam include abnormalities of facial development, dental malocclusion, and the “allergic gape” or continuous open-mouth breathing, chapped lips, “allergic shiners” (dark circles under the eyes), and the transverse nasal crease. Conjunctival edema, itching, tearing, and hyperemia are frequent findings. A nasal exam performed with a source of light and a speculum may reveal clear nasal secretions; edematous, boggy, and bluish mucus membranes with little or

no erythema; and swollen turbinates that may block the nasal airway. It may be necessary to use a topical decongestant to perform an adequate examination. Thick, purulent nasal secretions indicate the presence of infection.
Differential Diagnosis
Evaluation of AR calls for a thorough history, including details of the patient's environment and diet and family history of allergic conditions such as eczema, asthma, and AR, physical examination, and laboratory evaluation. The history and laboratory findings provide clues to the provoking factors. Symptoms that include sneezing, rhinorrhea, nasal itching, and congestion and the laboratory findings of elevated IgE, specific IgE antibodies, and positive allergy skin test results typify AR. SAR differs from PAR by history and skin test results. Nonallergic rhinitides cause sporadic symptoms and may resemble PAR. Their causes are often unknown. Nonallergic inflammatory rhinitis with eosinophils (NARES) imitates AR in presentation and response to treatment, but without elevated IgE antibodies. Vasomotor rhinitis is characterized by excessive responsiveness of the nasal mucosa to physical stimuli. Other nonallergic conditions, such as infectious rhinitis, structural problems including nasal polyps and septal deviation, rhinitis medicamentosa (due to the overuse of topical vasoconstrictors), hormonal rhinitis associated with pregnancy or hypothyroidism, neoplasms, vasculitides, and granulomatous disorders may mimic AR (Table 137-1).
Table 137-1 -- CAUSES OF RHINITIS
Allergic rhinitis Seasonal Perennial Perennial with seasonal exacerbation
Nonallergic rhinitis
Structural/mechanical factors: Deviated septum/septal wall anomalies Hypertrophic turbinates Adenoidal hypertrophy Foreign bodies
Nasal tumors: Benign Malignant
Choanal atresia
Infectious: Acute Chronic
Inflammatory/immunologic: Wegener granulomatosis

Sarcoidosis Midline granuloma Systemic lupus erythematosus Sjogren syndrome Nasal polyposis
Physiologic: Ciliary dyskinesia syndrome Atrophic rhinitis
Hormonally induced: Hypothyroidism Pregnancy Oral contraceptives Menstrual cycle
Exercise Atrophic
Drug induced: Rhinitis medicamentosa Oral contraceptives Antihypertensive therapy Aspirin Nonsteroidal anti-inflammatory drugs
Reflex induced: Gustatory rhinitis Chemical or irritant induced Posture reflexes Nasal cycle
Environmental factors: Odors Temperature Weather/barometric pressure Occupational
Nonallergic rhinitis with eosinophilia syndrome Perennial nonallergic rhinitis (vasomotor rhinitis) Emotional factors
Complications
AR is frequently associated with complications and co-morbid conditions. Children with AR experience frustration over their appearance. Chronic sinusitis is a common complication of AR, sometimes associated with purulent infection, but in the majority of patients, marked mucosal thickening, sinus opacification, and nasal polyposis with inflammation but negative culture

results develop. The inflammatory process is characterized by marked eosinophilia. Allergens, possibly fungal, may be the inciting agents. The sinusitis of triad asthma (asthma, sinusitis with nasal polyposis, and aspirin sensitivity) often responds poorly to therapy. Patients who undergo repeated endoscopic surgery derive diminishing benefit with each successive procedure.
Rhinitis that coexists with asthma may be taken too lightly or completely overlooked. Up to 78% of patients with asthma have AR, and 38% of patients with AR have asthma. Aggravation of AR coincides with exacerbation of asthma, and treatment of nasal inflammation reduces bronchospasm, asthma-related emergency department visits, and hospitalizations. Postnasal drip associated with AR commonly causes persistent or recurrent cough. Eustachian tube obstruction and middle ear effusion are frequent complications. Chronic allergic inflammation causes hypertrophy of adenoids and tonsils that may be associated with eustachian tube obstruction, serous effusion, otitis media, and obstructive sleep apnea. AR is strongly associated with snoring in children. The association between rhinitis and sleep abnormalities and subsequent daytime fatigue is well documented, but the mechanisms remain poorly understood.
Quality of life indices have been developed to explore the effects of the disease and of therapeutic interventions. The Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ) is suitable for children from 6 to 12 yr old, and the Adolescent RQLQ is appropriate for patients between 12 and 17. Studies using the PRQLQ in children with rhinitis have documented anxiety and physical, social, and emotional issues that affect learning and the ability to integrate with peers. The disorder contributes to headaches and fatigue, limits daily activities, and interferes with sleep. There is evidence of impaired cognitive functioning and learning that may be further threatened by the adverse effects of sedating medications. Rhinitis is an important cause of lost school attendance, resulting in more than 2 million absent days in the United States annually. A classification based on severity is shown in Figure 137-1.
Laboratory Findings
Epicutaneous skin tests provide the best method for detection of allergen-specific IgE (positive predictive value of 48.7% for the epidemiologic diagnosis of allergic rhinitis). They are inexpensive and sensitive, and the risks and discomfort are minimal. Responses to seasonal respiratory allergens are rare before two seasons of exposure, and children younger than 1 yr

rarely display positive skin test responses to these allergens. To avoid false-negative results, montelukast should be withheld for 1 day, most sedating antihistamine preparations for 3-4 days, and nonsedating antihistamines for 5-7 days. Serum immunoassays for IgE to allergens provide a suitable alternative (positive predictive value 43.5%) for patients with dermatographism or extensive dermatitis, patients taking medications that interfere with mast cell degranulation, others at high risk for anaphylaxis, and some who cannot cooperate with the procedure. Presence of eosinophils in nasal smear supports the diagnosis of AR, and that of neutrophils, of infectious rhinitis. Eosinophilia and measurements of total serum IgE concentrations have relatively low sensitivity. Improved methods for objective evaluation are still needed to assess the effects of treatment and to guide future developments.
Treatment
Safe and effective prevention or relief of symptoms is the goal of treatment. Specific measures to reduce indoor allergen exposure may reduce the risk of sensitization and symptoms of allergic respiratory disease, although existing studies report contradictory results. Sealing the patient's mattress, pillow, and covers in allergen-proof encasings reduces the exposure to mite allergen. Bed linen and blankets should be washed every week in hot water (>130?F). The only effective measure for avoiding animal allergens in the home is the removal of the pet. Avoidance of pollen and outdoor molds can be accomplished by staying in a controlled environment. Air conditioning allows for keeping windows and doors closed, reducing the pollen exposure. HEPA filters lower the counts of airborne mold spores.
The direct costs of allergic rhinitis have increased substantially since the introduction of second-generation antihistamines and intranasal corticosteroids (Tables 137-2 through 137-4). Oral antihistamines administered as needed constitute acceptable pharmacotherapy of mild, intermittent symptoms; however, first- and second-generation antihistamines available over the counter (OTC) may be associated with adverse effects on cognitive function and learning as a result of their sedative properties. Antihistamines relieve sneezing and rhinorrhea. Second-generation antihistamines are preferred because they cause less sedation. Five second-generation oral preparations are currently available:
Cetirizine: 6-12 mo: 2.5 mg qd; 1-2 yr: 2.5 mg qd, dosage may be increased to 2.5 mg bid; 2-5 yr: 2.5 mg/day, dosage may be increased to a maximum of 5 mg/day given either as a single dose or divided into 2 doses; >6 yr: 5-10 mg/day as a single dose or divided into 2 doses.
Levocetirizine: 6-11 yr: 2.5 mg PO once daily; >12 yr: 5 mg PO once daily. Loratadine (available OTC): 2-5 yr: 5 mg qd; >6 yr: 10 mg qd. Fexofenadine: 6-11 yr: 30 mg PO bid; >12 yr: 60 mg bid or 180 mg PO qd.
Desloratadine: 6-11 mo: 1 mg qd; 1-5 yr: 1.25 mg qd; 6-11 yr: 2.5 mg qd; >12 yr: 5 mg qd.
Table 137-2 -- ANTIHISTAMINES AND PSEUDOEPHEDRINE

DRUG AND TRADE NAME(S)
INDICATIONS (I), MECHANISM OF ACTION
(M), AND DOSING*
COMMENTS, CAUTIONS, AND ADVERSE EVENTS
Diphenhydramine (OTC):
I: Allergic rhinitis, atopic dermatitis, urticaria, night-time sedation.
M: Histamine H1-receptor antagonist.
Diphenhydramine has marked anticholinergic and sedating properties.
Chewable tablets contain phenylalanine.
New product labeling for OTC antihistamines will state, “Do not use in children under four years of age.”
Adverse effects: Hypotension, tachycardia, drowsiness, paradoxical excitement, dry mouth.
Benadryl
2-6 yr: 6.25 mg q4-6h; max 37.5 mg/24 hr
6-12 yr: 12.5-25 mg q4-6h; max 150 mg/24 hr
>12 yr: 25-50 mg q4-6h; max 300 mg/24 hr
Chlorpheniramine (OTC):
I: Allergic rhinitis, atopic dermatitis, urticaria, night-time sedation.
M: Histamine H1 receptor antagonist.
Chlorpheniramine is available in many preparations recommended for cough and cold. Its use for treatment of upper respiratory infections is unfounded.
Chlorpheniramine has anticholinergic and sedating properties.
New product labeling for OTC antihistamines will state, “Do not use in children under four years of age.”
Adverse effects: Slight to moderate drowsiness, headache, excitability, fatigue, nervousness, dizziness.
Chlor-Trimeton
2-6 yr: 1 mg q4-6h; max 6 mg/24 hr
6-12 yr: 2 mg q4-6h; max 12 mg/24 hr
>12 yr: 4 mg q4-6h; max 24 mg/ 24 hr
Sustained-release preparation: 6-12 yr: 8 mg hs >12 yr: 8-12 mg q8-12h
Brompheniramine (OTC):
I: Allergic rhinitis.
M: Histamine H1 receptor antagonist.
Brompheniramine is used primarily in combination preparations, most commonly with pseudoephedrine, recommended for cough and cold. Base the dose of combined preparations containing pseudoephedrine on pseudoephedrine.
The use of brompheniramine for treatment of upper respiratory infections is unfounded.
Brompheniramine has anticholinergic and sedating
Dimetapp
<6 yr: 0.125 mg/kg/dose q6h; max 1 mg/24 hr
6-12 yr: 2-4 mg/dose q6-8h; max 12 mg/24 hr
>12 yr: 4-8 mg/dose q4-6h; max 24 mg/24 hr

DRUG AND TRADE NAME(S)
INDICATIONS (I), MECHANISM OF ACTION
(M), AND DOSING*
COMMENTS, CAUTIONS, AND ADVERSE EVENTS
properties.
New product labeling for OTC antihistamines will state, “Do not use in children under four years of age.”
Loratadine (OTC):
I: Allergic rhinitis, urticaria.
M: Long-acting tricyclic antihistamine with selective peripheral histamine H1-receptor antagonistic properties.
Do not exceed recommended dose.
Note: Dimetapp Children's ND contains loratadine.
New product labeling for OTC antihistamines will state, “Do not use in children under four years of age.”
Adverse effects: Nervousness, fatigue, malaise, hyperkinesia, rash, abdominal pain.
Claritin, Alavert, Dimetapp Children's ND
2-5 yr: 5 mg qd >6 yr: 10 mg qd
Desloratadine (Rx):
I: Allergic rhinitis, urticaria.
M: Desloratadine, a major metabolite of loratadine, is a long-acting tricyclic antihistamine with selective peripheral histamine H1-receptor antagonistic properties.
Orally disintegrating tablets contain phenylalanine.
Adverse effects: Headache, fatigue, somnolence, dizziness.
Clarinex
6-12 mo: 1 mg qd 1-5 yr: 1.25 mg qd 6-12 yr: 2.5 mg qd >12 yr: 5 mg qd
Cetirizine (Rx and OTC):
I: Allergic rhinitis, urticaria.
M: Histamine H1-receptor antagonist.
Doses > 10 mg/day may cause significant drowsiness.
Adverse effects: Headache, somnolence, insomnia, abdominal pain. Zyrtec
6-24 mo: 2.5 mg qd (in children 12-24 mo, dose may be increased to 2.5 mg bid)
2-6 yr: 2.5-5 mg qd

DRUG AND TRADE NAME(S)
INDICATIONS (I), MECHANISM OF ACTION
(M), AND DOSING*
COMMENTS, CAUTIONS, AND ADVERSE EVENTS
>6 yr: 5-10 mg qd
Levocetirizine (Rx):
I: Allergic rhinitis, urticaria.
M: Levocetirizine is the R-enantiomer of cetirizine; it is a histamine H1-receptor antagonist.
Use with caution in patients with mild to moderate renal dysfunction, and adjust dosage.
Xyzal
6-12 yr; 2.5 mg qd in the evening
>12 yr: 5 mg qd in the evening
Fexofenadine (Rx):
I: Allergic rhinitis, urticaria.
M: Fexofenadine is an active metabolite of terfenadine; it is a histamine H1-receptor antagonist.
Good safety profile.
Adverse effects: Headache, fever, drowsiness, fatigue, dizziness.
Allegra
For chronic idiopathic urticaria: 6 mo–<2 yr: 15 mg bid 2-11 yr: 30 mg bid
≥12 yr: Refer to adult dosing.
For allergic rhinitis: 2-11 yr: 30 mg bid
≥12 yr: Refer to adult dosing.
Pseudoephedrine (OTC):
I: Temporary symptomatic relief of nasal congestion due to common cold, allergic rhinitis, and sinusitis.
M: α-Agonist, decongestant.
Dosing errors and accidental ingestions are an important cause of rare adverse events in children.
Use with caution in patients with hyperthyroidism, hypertension, diabetes, arrhythmias, or heart disease.
Chewable tablets contain phenylalanine.
OTC and prescribed antihistamines may be formulated in combination with pseudoephedrine. For combination preparations containing pseudoephedrine and an
Sudafed <2 yr: 4 mg/kg/dose q6h
2-5 yr: 15 mg q6h; max 60 mg/24 hr
6-12 yr: 30 mg q6h; max 120 mg/24 hr
<12 yr: 60 mg q6h ≥12 yr: 120 mg q12h or
240 mg qd; max

DRUG AND TRADE NAME(S)
INDICATIONS (I), MECHANISM OF ACTION
(M), AND DOSING*
COMMENTS, CAUTIONS, AND ADVERSE EVENTS
240 mg/24 hrantihistamine, base the dose on pseudoephedrine.
Pseudoephedrine serves as the raw ingredient in the illicit production of methamphetamine.Adverse effects: Tachycardia,
OTC, available over the counter (nonprescription); Rx, prescription required.
* All of these agents are administered orally.
Table 137-3 -- INTRANASAL INHALED CORTICOSTEROIDS
DRUG, TRADE NAME(S), AND
FORMULATIONS
INDICATIONS (I), MECHANISM(S) OF ACTION
(M), AND DOSING
COMMENTS, CAUTIONS, ADVERSE EVENTS, AND
MONITORING
Beclomethasone: I: Allergic rhinitis.
M: Anti-inflammatory, immune modulator.
Shake container before use; blow nose; occlude one nostril, administer dose to the other nostril.
Adverse effects: Burning and irritation of nasal mucosa, epistaxis.
Monitor growth.
Beconase AQ (42 ?g/spray)
6-12 yr: 1 spray in each nostril bid
>12 yr: 1 or 2 spray in each nostril bid
Flunisolide
6-14 yr: 1 spray each nostril 3 times daily or 2 sprays in each nostril twice daily; not to exceed 4 sprays/day in each nostril
≥15 yr: 2 sprays each nostril twice daily (morning and evening); may increase to 2 sprays 3 times daily; maximum dose: 8 sprays/day in each nostril (400 ?g/day)
Shake container before use; blow nose; occlude one nostril, administer dose to the other nostril.
Adverse effects: Burning and irritation of nasal mucosa, epistaxis.
Monitor growth.Nasarel (25 ?g/spray) ≥6 yr: initial dose 1 spray tid or 2

DRUG, TRADE NAME(S), AND
FORMULATIONS
INDICATIONS (I), MECHANISM(S) OF ACTION
(M), AND DOSING
COMMENTS, CAUTIONS, ADVERSE EVENTS, AND
MONITORING
sprays in each nostril bid; reduce to lowest effective dose
Triamcinolone: I: Allergic rhinitis.
M: Anti-inflammatory, immune modulator.
Shake container before use; blow nose; occlude one nostril, administer dose to the other nostril.
Adverse effects: Burning and irritation of nasal mucosa, epistaxis.
Monitor growth.
Nasacort HFA (55 ?g/spray), Nasacort AQ (55 ?g/spray)
2-6 yr; 1 spray in each nostril qd
6-12 yr: 1-2 sprays in each nostril qd
≥12 yr: 2 sprays in each nostril qd
Fluticasone: I: Allergic rhinitis.
M: Anti-inflammatory, immune modulator.
Shake container before use; blow nose; occlude one nostril, administer dose to the other nostril.
Ritonavir significantly increases fluticasone serum concentrations and may result in systemic corticosteroid effects.
Use fluticasone with caution in patients receiving ketoconazole or other potent cytochrome P450 3A4 isoenzyme inhibitors.
Adverse effects: Burning and irritation of nasal mucosa, epistaxis.
Monitor growth.
Fluticasone propionate (available as a generic preparation):
Flonase (50 ?g/spray) ≥4 yr: 1-2 sprays in each nostril qd
Fluticasone furoate:
Veramyst (27.5 ?g/spray)
2-12 yr:
Initial dose: 1 spray (27.5 ?g/spray) per nostril once daily (55 ?g/day).
Patients who do not show adequate response may use 2

DRUG, TRADE NAME(S), AND
FORMULATIONS
INDICATIONS (I), MECHANISM(S) OF ACTION
(M), AND DOSING
COMMENTS, CAUTIONS, ADVERSE EVENTS, AND
MONITORING
sprays per nostril once daily (110 ?g/day).
Once symptoms are controlled, dosage may be reduced to 55 ?g once daily.
Total daily dosage should not exceed 2 sprays in each nostril (110 ?g)/day.
≥12 yr and adolescents:
Initial dose: 2 sprays (27.5 ?g/spray) per nostril once daily (110 ?g/day).
Once symptoms are controlled, dosage may be reduced to 1 spray per nostril once daily (55 ?g/day).
Total daily dosage should not exceed 2 sprays in each nostril (110 ?g)/day.
Mometasone: I: Allergic rhinitis.
M: Anti-inflammatory, immune modulator.
Mometasone and its major metabolites are undetectable in plasma after nasal administration of recommended doses.
Preventive treatment of seasonal allergic rhinitis should begin 2-4 wk prior to pollen season.
Shake container before use; blow nose; occlude one nostril, administer dose to the other nostril.
Adverse effects: Burning and irritation of nasal mucosa, epistaxis.
Monitor growth.
Nasonex (50 ?g/spray) 2-12 yr: 1 spray in each nostril qd >12 yr: 2 sprays in each nostril qd
Budesonide: I: Allergic rhinitis.
M: Anti-inflammatory, immune modulator.
Shake container before use; blow nose; occlude one nostril, administer dose to the other nostril.
Rhinocort AQ >6 yr: 1 spray in each nostril qd

DRUG, TRADE NAME(S), AND
FORMULATIONS
INDICATIONS (I), MECHANISM(S) OF ACTION
(M), AND DOSING
COMMENTS, CAUTIONS, ADVERSE EVENTS, AND
MONITORING
(32 ?g/spray)
6-12 yr: 2 sprays in each nostril qd
>12 yr: up to 4 sprays in each nostril qd (maximum dose)
Adverse effects: Burning and irritation of nasal
Ciclesonide: I: Allergic rhinitis.
M: Anti-inflammatory, immune modulator.
Prior to initial use, gently shake, then prime the pump by actuating eight times.
If the product is not used for 4 consecutive days, gently shake and reprime with one spray or until a fine mist appears.
Omnaris (50 ?g/spray) >6 yr: 2 sprays in each nostril qd
Table 137-4 -- MISCELLANEOUS INTRANASAL SPRAYS
DRUG, TRADE NAME(S), AND
FORMULATIONS
INDICATIONS (I), MECHANISM(S) OF ACTION
(M), AND DOSING
COMMENTS, CAUTIONS, ADVERSE EVENTS, AND
MONITORING
Ipratropium bromide:
I: Symptomatic relief of rhinorrhea.
M: Anticholinergic.
Atrovent inhalation aerosol is contraindicated in patients with hypersensitivity to soy lecithin.
Safety and efficacy of use beyond 4 days in patients with the common cold have not been established.
Adverse effects: Epistaxis, nasal dryness, nausea.
Atrovent nasal spray (0.06%)
Colds (symptomatic relief of rhinorrhea):
5-12 yr: 2 sprays in each nostril 3 times/day
≥12 yr and adults: 2 sprays in each nostril 3-4 times/day
Azelastine:
I: Treatment of rhinorrhea, sneezing, and nasal pruritus.
M: Antagonism of histamine H1-receptor.
May cause drowsiness.
Adverse effects: Headache, somnolence, bitter taste.
Astelin 6-12 yr: 1 spray bid >12 yr: 1-2 sprays bid
Cromolyn sodium: I: Allergic rhinitis.
M: Inhibition of mast cell degranulation.
Not effective immediately; requires frequent administration.
Nasalcrom >2 yr: 1 spray tid-qid; max 6

DRUG, TRADE NAME(S), AND
FORMULATIONS
INDICATIONS (I), MECHANISM(S) OF ACTION
(M), AND DOSING
COMMENTS, CAUTIONS, ADVERSE EVENTS, AND
MONITORING
?/day
Oxymetazoline:
I: Symptomatic relief of nasal mucosal congestion.
M: Adrenergic agonist, vasoconstricting agent.
Excessive dosage may cause profound CNS depression.
Use in excess of 3 days may result in severe rebound nasal congestion.
Do not repeat more than once a month.
Use with caution in patients with hyperthyroidism, heart disease, hypertension, and diabetes.
Adverse effects: Hypertension, palpitations, reflex bradycardia, nervousness, dizziness, insomnia, headache, CNS depression, convulsions, hallucinations, nausea, vomiting, mydriasis, elevated intraocular pressure, blurred vision.
Afrin, Nōstrilla0.05% solution: Instill 2-3 sprays into each nostril twice daily; therapy should not exceed 3 days
Phenylephrine:
I: Symptomatic relief of nasal mucosal congestion.
M: Adrenergic, vasoconstricting agent.
Use in excess of 3 days may result in severe rebound nasal congestion.
Do not repeat more than once a month.
0.16% and 0.125% solutions are not commercially available.
Adverse effects: Reflex bradycardia, excitability, headache, anxiety, and dizziness.
Neo-Synephrine
2-6 yr: 1 drop every 2-4 hr of 0.125% solution as needed. Note: Therapy should not exceed 3 continuous days.
6-12 yr: 1-2 sprays or 1-2 drops every 4 hr of 0.25% solution as needed. Note: Therapy should not exceed 3 continuous days.
>12 yr: 1-2 sprays or 1-2 drops every 4 hr of 0.25% to 0.5% solution as needed; 1% solution may be used in adults with extreme nasal congestion. Note: Therapy should not exceed 3

DRUG, TRADE NAME(S), AND
FORMULATIONS
INDICATIONS (I), MECHANISM(S) OF ACTION
(M), AND DOSING
COMMENTS, CAUTIONS, ADVERSE EVENTS, AND
MONITORING
continuous days.
Azelastine is a topically active antihistamine available as a nasal spray (5-12 yr: 1 spray per nostril bid; >12 yr :2 sprays/nostril bid) and as eye drops (>3 yr: 1 drop in each affected eye bid). Pseudoephedrine (available OTC, generally in combination with OTC antihistamines) is an oral vasoconstrictor known to cause irritability and insomnia and to be associated with infant mortality. The anticholinergic nasal spray ipratropium bromide (2 sprays/nostril bid or tid; use 0.03% preparation) is effective for the treatment of serous rhinorrhea. Intranasal decongestants should be used for less than 5 days, not to be repeated more than once a month. Sodium cromoglycate (available OTC) is effective but requires frequent administration, q4h. Leukotriene-modifying agents have a modest effect on rhinorrhea and nasal blockage. Nasal saline irrigation is a good adjunctive option with all other treatment of allergic rhinitis.
Patients with more persistent, severe symptoms require treatment with intranasal corticosteroids, the most effective therapy for AR. These agents reduce all symptoms of AR with eosinophilic inflammation but not those of rhinitis associated with neutrophils or free of inflammation. The older drugs beclomethasone, triamcinolone, and flunisolide are absorbed from the gastrointestinal (GI) tract as well as from the respiratory tract. New corticosteroid preparations—budesonide, fluticasone propionate, mometasone furoate, and ciclesonide—have been developed that offer greater topical activity with lower systemic exposure. Fluticasone (>4 yr: 1-2 sprays/nostril qd), mometasone (2-11 yr: 1 spray/nostril qd; >12 yr: 2 sprays/nostril qd), budesonide (>6 yr: 1 spray/nostril qd, dose may be increased if needed; maximum dose for children <12 yr: 2 sprays/nostril qd, and for children >12 yr: 4 sprays/nostril qd), and ciclesonide (>6 yr with SAR and >12 yr with PAR: 2 sprays/nostril qd) have lower systemic bioavailability and better safety profiles. More severely affected patients may benefit from simultaneous treatment with antihistamines and intranasal corticosteroids.
Specific allergen immunotherapy administered by subcutaneous injection should be considered for children in whom IgE-mediated allergic symptoms cannot be adequately controlled by avoidance and medication, especially in the presence of co-morbid conditions. Allergen immunotherapy interferes with IgE production and allergic symptoms. It has been found to be effective in the treatment of allergic rhinitis. Locally applied immunotherapy, which may be oral, sublingual, or nasal, has been used successfully in Europe and South America. Sublingual immunotherapy holds promise for the treatment for allergic rhinitis, but it is currently considered investigational in the USA until formulations approved by the U.S. Food and Drug Administration are available. Studies have now shown that anti-IgE reduces allergic responses in the nose. Treatment strategies that incorporate both anti-IgE and immunotherapy hold promise for the future.

Prognosis
Therapy with nonsedating antihistamines and intranasal corticosteroids significantly improves health-related quality of life measures in patients of all ages with AR, provided that they continue to take their medications. The reported rates of remission among children are between 10% and 23%. However, prognosis for the future is much brighter. It includes exciting measures to prevent atopy, induce immune tolerance, and hold back the expression of the allergic phenotype. Pharmacotherapy will target cells and cytokines involved in inflammation and treat allergy as a systemic process.







![Diagnosis and Management of Rhinitis: Complete Guidelines ... · different forms of rhinitis (allergic, non-allergic, occupational rhinitis, hormonal rhinitis [pregnancy and hypothyroidism],](https://static.fdocuments.in/doc/165x107/5d61f07588c993197b8b51b8/diagnosis-and-management-of-rhinitis-complete-guidelines-different-forms.jpg)