Rh phenotype prediction by DNA typing and its application to … · 1999. 1. 4. · Other...
22
REVIEW ARTICLE Rh phenotype prediction by DNA typing and its application to practice W. A. Flegel,* F. F. Wagner,* T. H. Mu ¨ller² and C. Gassner‡ *Abteilung Transfusionsmedizin, Universita ¨tsklinikum Ulm and DRK-Blutspendedienst Baden-Wu ¨rttemberg, Institut Ulm, Ulm, Germany, ² DRK-Blutspendedienst Niedersachsen- Oldenburg, Institut Oldenburg, Oldenburg, Germany, and ‡Zentralinstitut fu ¨r Bluttransfusion und Immunologische Abteilung Innsbruck, Innsbruck, Austria Received 27 April 1998; accepted for publication 20 August 1998 SUMMARY. The complexity of the RHD and RHCE genes, which is the greatest of all blood group systems, con- founds analysis at the molecular level. RH DNA typing was introduced in 1993 and has been applied to prenatal testing. PCR-SSP analysis covering multiple polymorph- isms was recently introduced for the screening and initial characterization of partial D. Our objective is to sum- marize the accrued knowledge relevant to the approaches to Rh phenotype prediction by DNA typing, their possi- ble applications beyond research laboratories and their limitations. The procedures, results and problems encountered are highly detailed. It is recommended that DNA typing comprises an analysis of more than one polymorphism. We discuss future directions and propose a piecemeal approach to improve reliability and cost- efficiency of blood group genotyping that may eventually replace the prevalent serology-based techniques even for many routine tasks. Transfusion medicine is in the unique position of being able to utilize the most exten- sive phenotype databases available to check and develop genotyping strategies. Key words: blood group, DNA typing, genomic analysis, genotyping, human diversity, partial D, PCR-RFLP, PCR-SSO, PCR-SSP, phenotype prediction, red blood cell, Rh, RHCE, RhD, RHD, Rhesus, RT-PCR, transfusion. The genes of almost all blood group systems have been cloned and the molecular bases of their major antigens elucidated. Hence, DNA typing has become possible for many blood group antigens that are mostly defined by single amino acid polymorphisms and expressed by proteins of the red blood cell surface (Anstee, 1995; Avent, 1997; Huang, 1997b). Suitable PCR techniques for genotyping of ABO (Gassner et al., 1996), Kell (Hessner et al., 1996), Duffy (Mallinson et al., 1995), Kidd (Olives et al., 1997), MN and Ss (Eshle- man et al., 1995) have been described. In a similar fashion, DNA typing for alleles of both RH genes can be performed. The first application of Rh phenotype prediction by DNA typing was published in 1993 (Bennett et al., 1993; Lo et al., 1993). A rather high rate of false positive results (Simsek et al., 1994) and false negative results (Bennett & Cartron, 1994; Simsek et al., 1994) was immediately recognized and the authors proposed that ‘the use of two independent primer sets should reduce the risk of incorrect genotyping.’ (Bennett & Cartron, 1994; Simsek et al., 1994). Many polymorphisms have been utilized for RhD phenotype prediction since then (pre- viously reviewed by Wolter et al., 1993; Hyland et al., 1995; van den Veyver & Moise, 1996; Aubin et al., 1997). No consensus has yet been achieved as to which polymorphism may be most reliable for testing of any given population. RH and particularly RHD DNA typing is much con- founded by the presence of two highly homologous genes, RHCE and RHD, and the complex polymorphisms between both genes. In contrast to most other blood group antigens, the RhD antigen does not derive from amino acid polymorphisms, but from the presence of a separate protein absent in the RhD-negative phenotypes. Furthermore, there are proteins, such as R 0 Har and D VI , that express RhD-immunoreactivity but do not share any common RHD-specific nucleotide sequences. To estab- lish reliable and workable solutions for RH DNA typing Transfusion Medicine, 1998, 8, 281–302 281 q 1998 Blackwell Science Ltd Correspondence to: Willy A. Flegel, Priv.-Doz. Dr med., Abteilung Transfusionsmedizin, Universita ¨tsklinikum Ulm, and DRK- Blutspendedienst Baden-Wu ¨rttemberg, Institut Ulm, Helmholtzstrasse 10, D-89081 Ulm, Germany. Tel: þ49 731 150 600; fax: þ49 731 150 602; e-mail: [email protected]
Transcript of Rh phenotype prediction by DNA typing and its application to … · 1999. 1. 4. · Other...

REVIEW ARTICLE
Rh phenotype prediction by DNA typing and its application topracticeW. A. Flegel,* F. F. Wagner,* T. H. Mu¨ller† and C. Gassner‡*Abteilung Transfusionsmedizin,
Universitatsklinikum Ulm and DRK-Blutspendedienst Baden-Wu¨rttemberg, Institut Ulm, Ulm, Germany,†DRK-Blutspendedienst Niedersachsen-
Oldenburg, Institut Oldenburg, Oldenburg, Germany, and‡Zentralinstitut fur Bluttransfusion und Immunologische Abteilung Innsbruck, Innsbruck,
Austria
Received 27 April 1998; accepted for publication 20 August 1998
SUMMARY. The complexity of theRHDandRHCEgenes,which is the greatest of all blood group systems, con-founds analysis at the molecular level.RH DNA typingwas introduced in 1993 and has been applied to prenataltesting. PCR-SSP analysis covering multiple polymorph-isms was recently introduced for the screening and initialcharacterization of partial D. Our objective is to sum-marize the accrued knowledge relevant to the approachesto Rh phenotype prediction by DNA typing, their possi-ble applications beyond research laboratories and theirlimitations. The procedures, results and problemsencountered are highly detailed. It is recommended thatDNA typing comprises an analysis of more than one
polymorphism. We discuss future directions and proposea piecemeal approach to improve reliability and cost-efficiency of blood group genotyping that may eventuallyreplace the prevalent serology-based techniques even formany routine tasks. Transfusion medicine is in theunique position of being able to utilize the most exten-sive phenotype databases available to check and developgenotyping strategies.
Key words: blood group, DNA typing, genomic analysis,genotyping, human diversity, partial D, PCR-RFLP,PCR-SSO, PCR-SSP, phenotype prediction, red bloodcell, Rh,RHCE, RhD,RHD, Rhesus, RT-PCR, transfusion.
The genes of almost all blood group systems have beencloned and the molecular bases of their majorantigens elucidated. Hence, DNA typing has becomepossible for many blood group antigens that are mostlydefined by single amino acid polymorphisms andexpressed by proteins of the red blood cell surface(Anstee, 1995; Avent, 1997; Huang, 1997b). SuitablePCR techniques for genotyping ofABO (Gassneret al.,1996),Kell (Hessneret al., 1996),Duffy (Mallinson etal., 1995),Kidd (Oliveset al., 1997),MN andSs(Eshle-man et al., 1995) have been described. In a similarfashion, DNA typing for alleles of bothRH genes canbe performed.
The first application of Rh phenotype prediction byDNA typing was published in 1993 (Bennettet al., 1993;Lo et al., 1993). A rather high rate of false positiveresults (Simseket al., 1994) and false negative results
(Bennett & Cartron, 1994; Simseket al., 1994) wasimmediately recognized and the authors proposed that‘the use of two independent primer sets should reduce therisk of incorrect genotyping.’ (Bennett & Cartron, 1994;Simseket al., 1994). Many polymorphisms have beenutilized for RhD phenotype prediction since then (pre-viously reviewed by Wolteret al., 1993; Hylandet al.,1995; van den Veyver & Moise, 1996; Aubinet al.,1997). No consensus has yet been achieved as to whichpolymorphism may be most reliable for testing of anygiven population.
RH and particularlyRHD DNA typing is much con-founded by the presence of two highly homologousgenes,RHCEandRHD, and the complex polymorphismsbetween both genes. In contrast to most other bloodgroup antigens, the RhD antigen does not derive fromamino acid polymorphisms, but from the presence of aseparate protein absent in the RhD-negative phenotypes.Furthermore, there are proteins, such as R0
Har and DVI,that express RhD-immunoreactivity but do not share anycommonRHD-specific nucleotide sequences. To estab-lish reliable and workable solutions forRH DNA typing
Transfusion Medicine, 1998,8, 281–302
281q 1998 Blackwell Science Ltd
Correspondence to: Willy A. Flegel, Priv.-Doz. Dr med., AbteilungTransfusionsmedizin, Universita¨tsklinikum Ulm, and DRK-Blutspendedienst Baden-Wu¨rttemberg, Institut Ulm, Helmholtzstrasse10, D-89081 Ulm, Germany. Tel:þ49 731 150 600; fax:þ49 731150 602; e-mail: [email protected]

is probably the most challenging task among all bloodgroup genotyping applications.
The discrimination ofRHD homozygotes fromRHDheterozygotes is hampered (Cossuet al., 1996) becausethe most prevalentRHD-negative allele cannot yet bedetected specifically. For the time being, we prefertherefore the term DNA typing rather than genotyping,when an RhD phenotype prediction by molecular tech-niques is attempted.
We have summarized the molecular genetics of theRHgenes according to the current understanding. A list ofRHD alleles, catalogued by molecular rather than sero-logical criteria, and of polymorphisms betweenRHDandRHCE, useful for DNA typing, is provided. The develop-ment of suitable DNA techniques is discussed. Wepresent a survey of publishedRH DNA typing methods.The propagation of DNA typing methods for bloodgroups, like Rh, from the benches of some specializedlaboratories to a widely established routine tool fortransfusion medicine is under way. Efficient and afford-able solutions should be widely adapted.
CLINICAL SIGNIFICANCE
The first application ofRH DNA typing was prenataltesting for fetal RhD status to indicate the requirementfor anti-D prophylaxis and clinical management of preg-nant women with anti-D (Bennettet al., 1993; Loet al.,1993). DNA typing may require less fetal tissue and canbe performed before the Rh proteins are expressed,rendering the fetal DNA typing less invasive than ser-ological phenotyping. The DNA typing can be done withany fetal tissue, such as amniotic fluid (’amniocytes’),trophoblastic cells (’chorionic villi’) or cord blood (’fetalblood cells’). Essentially noninvasive methods for fetaltesting by retrieving fetal (trophoblastic) cells shed intothe endocervical canal (Adinolfiet al., 1995) or fetalcells circulating in the mother’s peripheral blood (Loetal., 1994a,b) appear possible. For the latter application,selection of the appropriate fetal cell type is crucial,because fetal lymphocytes may persist for many years inthe mother’s circulation (Bianchiet al., 1996) preventinga meaningful test interpretation in multiparous women.Recent approaches stressed the importance of test sensi-tivity (Hengstschlageret al., 1997; Tonnet al., 1997) andfocused on fetal nucleated red blood cells, which may beenriched (Ga¨nshirt-Ahlert et al., 1993; Buschet al.,1994; Geifman-Holtzmanet al., 1996b; Sekizawaetal., 1996), tested as single cells (Ferguson-Smithet al.,1994; van den Veyveret al., 1995; Sekizawaet al., 1996;Reubinoff et al., 1996) or assayed forRHD mRNA(Hamlington et al., 1997). Prenatal genotyping hasalready been applied to many other blood group proteinslike RhCE (Le Van Kim et al., 1994; Spenceet al.,
1995b; Dildy et al., 1996; Geifman-Holtzmanet al.,1996a), Kell (Leeet al., 1996; Spenceet al., 1997),MN and Ss (Eshlemanet al., 1995).
Other applications ofRH DNA typing are in paternitytesting and forensic medicine (Ikemotoet al., 1996). Likeall genetic testing,RH DNA typing would be feasiblewith any source of human tissue carrying nucleated cellsor remnants thereof, including blood, serum, plasma,skin, hair, hair follicle, bone, semen or urine.
Emerging evidence is pointing to the possibility thatDNA-based phenotype prediction is superior to serotyp-ing, when serological typing cannot be accomplishedwith its usual ease. After massive transfusion of bloodcomponents, the serological typing is frequently ham-pered by the admixture of allogeneic red blood cellsobscuring the recipient’s antigens. Despite the transfer ofdonor leucocytes, DNA typing was feasible forHLA(Wenk & Chiafari, 1997),MN andSs(Eshlemanet al.,1995). It seems promising that suitable methods will bedeveloped for other blood groups so that a reliable typingcan be provided even after massive transfusions. Inpartial D with reduced antigen density, serological dis-crimination is often hampered by limiting antibodysensitivity. DNA-based phenotype prediction wasshown to be superior to serological discrimination ofsuch RhD phenotypes, as exemplified by the differentDVI types (Wagneret al., 1998a).
The relevance ofRHDNA typing for clinical manage-ment depends critically on the reliability of the Rhphenotype prediction. Allele variants, especiallyRHD/CEhybrid alleles, and random nucleotide substitutions inthe gene account for discrepancies between the results ofDNA-based phenotype prediction and of serology-basedphenotyping.RH genotyping may eventually replacecurrent serological Rhesus testing, if two major obstaclescan be overcome. A more comprehensive understandingof the RH locus and its variant organization in differentpopulations needs to be achieved (Carrittet al., 1994)and, more importantly, the cost-efficiency needs to bevastly improved.
SCIENTIFIC SIGNIFICANCE
A unique combination of features applying to theRHgenes and Rh proteins qualifies them as an attractivemodel system. They represent two highly homologousgenes that are located closely adjacent on a chromosome.Their polymorphism is shaped by a recent duplicationand later deletion events. A multitude of gene conversionand recombination events are evident from the limitedcharacterization of the extant alleles, which has beenconducted to date. With a prudent combination of sero-logical and molecular screens the knowledge will soonincrease considerably. Hence, theRH polymorphism
282 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

presents itself as a model system for the group ofhomologous adjacent genes, which comprise a largenumber of members and are frequent throughout thegenomes of all species. With the exception of theHLAgenes’ locus theRH genes already represent the bestcharacterized members of that group. It is a potentialadvantage that in contrast to HLA the Rh proteins do notseem to be exposed to stringent selective pressure andmay therefore represent more faithfully the processesinvolved in near-random molecular evolution.
RH allele polymorphism will also be of interest topopulation biology because it has become feasible todetermine in a massive way the frequencies of molecu-larly defined rare alleles in natural populations. Poisson-like allele distributions were predicted by mathematicalmodels (Joyce & Tavare, 1995), which have so far notbeen checked in any real population.
The observation of alleles with multiple nucleotidesubstitutions in theRHDgene that were characteristic fortheRHCEgene, but interspersed byRHD-specific DNAsegments, cannot be explained by a single gene conver-sion event. This observation pointed to more complicatedmechanisms shaping the polymorphism of proteins. Theoccurrence of various Rh proteins seems to represent anatural experiment for protein membrane integration.The mechanisms involved can be more completelyexplained once the function of the Rh protein has been
discerned and the relationship of function and proteinmorphology has been checked.
RELEVANCE OF THE MOLECULARGENETICS OF THERH LOCUS
All antigens of the Rh blood group system are carried bytwo proteins encoded by two highly homologous genes,RHD andRHCE, with adjacent chromosomal positions.Recent reviews (Cartron, 1994; Rouger & Muller, 1996;Huang, 1997b; Scottet al., 1997; Sonneborn & Voak,1997) summarize the accrued knowledge. The geneswere derived from an older duplication process thatwas followed far more recently by a deletion encom-passing the wholeRHD gene in the prevalent RhD-negative haplotype. The allelic variability known fromserological studies was confirmed by the current mole-cular work-up, which revealed many more alleles thananticipated by serology. A multitude of genetic mechan-isms seems to have contributed to this allelic variabilityincluding multiple exchanges of DNA stretches betweenor recombination events affecting both genes, andnumerous nucleotide substitutions occurring in bothgenes (Carrittet al., 1997).
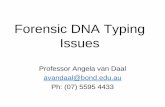
The complex organization of theRH locus (Fig. 1) andthe variable distribution ofRH haplotypes amongpopulations confound molecular genetics analysis and
Rh phenotype prediction by DNA typing283
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Fig. 1. Chromosomal organization of theRHCEandRHD genes according to the current understanding. The locus (top) spans lessthan 450 kb on the short arm of chromosome 1 between the positions 1p34·3 and 1p36·1 (Cherif-Zaharet al., 1991; MacGeochet al.,1992). The physical distance between both genes is unknown. TheRHD gene is located 30 to theRHCEgene. The orientation of thegenes in regard to each other and to the centromere is still unresolved. The genomic structure was analysed for theRHCEgene (Cherif-Zaharet al., 1994). TheRHD gene is believed to have a very similar structure (bottom). There are 37 amino acid positions varyingbetween theceallele ofRHCEand the prevalentRHD allele (thin lines in the 10 exons). The 30 untranslated region (UTR) ofRHDexon 10 (hatched) covers more than 1500 bp (Le Van Kimet al., 1992); a shorter stretch is known forRHCE(Cherif-Zaharet al.,1990), which deviated considerably (asterisks above 30 UTR). Many of these exon polymorphisms have been utilized to detect thepresence of theRHDallele (see Table 1). There is a 4247-bp stretch of near nucleotide identity between theC allele ofRHCEand theRHDalleles spanning from intron 1 to intron 2 (asterisks around exon 2). The positions of nucleotide deletions occurring in introns oftheRHCEgene are indicated by arrows: All three deletions (109 bp in intron 2, 288 bp in intron 3 and 651 bp in the very short intron 4)have been utilized for DNA typing to detect the presence of theRHD allele (see Table 4).

its exploitation for DNA typing. Whilst understandingof the arrangement of theRH genes is far from com-plete, many polymorphisms between both genes alongwith allele polymorphisms have been established. Apartfrom exon sequences, polymorphisms in intron 2(Poulter et al., 1996), 3 (Wagneret al., 1998a), 4(Arce et al., 1993) and 8 (Kempet al., 1996; Carrittet al., 1997) were utilized to predict the phenotype formany Rh antigens. Examples for ’diagnostic sites’ suit-able for PCR using sequence-specific priming are givenin Table 1.
Partial D phenotypes
Anti-D immunization in RhD-positive individuals(Argall et al., 1953) was exploited to classify someRhD proteins into ‘D categories’ (Tippett & Sanger,1962). The term ’partial D’ (Salmonet al., 1984) refersto RhD proteins lacking epitopes that are often defined bymonoclonal anti-D. Several partial D antigens permitanti-D immunization in their carriers. Rather good dataon anti-D immunization is available for the more
frequent DVI and DVII phenotypes. Only further studieswill reveal which other partial D are frequently, rarely ornever permissible for anti-D immunization. AberrantRHD coding sequences have been shown for all investi-gated partial D. The molecular causes comprise (i)exchange of large gene segments betweenRHD andRHCE resulting in RhD/RhCE hybrid proteins; (ii)single or multiple nucleotide exchanges betweenRHDandRHCEnot involving larger gene segments; and (iii)mis-sense mutations. Molecular alterations in partial Dgenerally affect at least one extrafacial amino acid aspredicted by the model for RhD membrane integration(Wagneret al., 1998b).
Several of theseRHD alleles with aberrantRHDcoding sequences are clinically important. Their discri-mination from the prevalentRHD allele in transfusionrecipients would be advantageous to guide RhD-negativetransfusion therapy. The best characterized partial D tobe set apart from RhD-positive in routine serologicaltesting are the different DVI types (Wagneret al., 1998a).However, as more data for the partial D populationfrequencies (Flegel & Wagner, 1996; Roubinetet al.,
284 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Table 1. Rh antigen prediction by sequence-specific detection of polymorphic nucleotide positions in various exons and introns ofthe RHD andRHCEgenes
Polymorphic SpecificcDNA nucleotide(s) Gene for
Antigen position(s) assayed segment antigen Problems and notes
D (RH1) 383 A exon 3 yes –602 C exon 4 yes –n.a. deletion intron 4 yes –676/787 G/G exon 5 yes –916 G exon 6 yes –1048 G exon 7 yes –1193 A exon 9 yes –1358 C 30 UTR yes –
C (RH2) 48 C exon 1 no Cw, c(cyt48) positiven.a. insertion intron 2 yes –
E (RH3) 676/787 C/A exon 5 yes –c (RH4) 201/307 A/C exon 2 yes –e (RH5) 676/787 G/A exon 5 yes –Cw (RH8) 122 G exon 1 yes –G (RH12) 201/307 G/T exon 2 yes D and C positiveDVII (RH40) 329 C exon 2 yes –
The specificity is indicated for the prevalent alleles at theRH locus in Caucasians. Rare alleles may limit the specificity as discussed in the text(see Tables 2 and 3). At least one nucleotide position in each exon and intron with known polymorphisms is tested. There are no polymorphisms inexon 8 or in the coding sequence of exon 10 (see Fig. 1) and no suitable polymorphism for SSP in intron 3. DVII representsRHD(L110P); Cw –RHC(Q41R);c(cyt48) – thec(W16C) allele ofRHCEwhich is frequent in the cDe haplotype and serologically indistinguishable from theprevalentc alleles ofRHCE(Gassneret al., 1997b); 30 UTR – 30 untranslated region of exon 10; n.a. – not applicable because of intronic locationof the polymorphism. Primer sequences may be found in Gassneret al. (1997b) and for intron 4 in Aventet al. (1997c). For intron 2, Cw and DVII
the method is given in Gassneret al. (1997a), although no PCR-SSP primer sequences have yet been published.

1996) and the propensity for immunization by RhD-positive transfusion and pregnancy are gathered, the spe-cific detection of other partial D may become desirable.
Weak D antigen expression
In contrast to the previously accepted dogma (Issitt &Telen, 1996; Roubinetet al., 1996; Rouillacet al., 1996;Aubin et al., 1997; Beckerset al., 1997; Fukumoriet al.,1997; Huang, 1997b), the vast majority ofRHD allelesfound with weak D antigen expression encode aberrantRhD with amino acid substitutions (Flegelet al., 1998).We noted that in all weak D samples characterized at themolecular level the substituted residues were located intransmembranous and intracellular RhD protein seg-ments (Wagneret al., 1998b).
Towards a molecular-based Rh nomenclature
For the purpose of anRH-allele-based nomenclature, wewould favour the term ’aberrantRHD’ allele referring toall RHD alleles coding for one or more amino acidsubstitutions compared to the prevalent, standardRHDallele. This DNA-based definition would broaden theserology-based definition of partial D and encompass awider range ofRHD alleles and the proteins/antigensencoded by these alleles. The name reflects the sporadicoccurrence of these alleles and, hence, of their ’aberrantRhD’ phenotypes, including but not limited to partial D.The proposed nomenclature has the advantage of cover-ing almost all knownRHDalleles (Table 2) including allknown clinically relevant partial D and molecular weakD types (Wagneret al., 1998b). The nomenclature isunequivocally defined and does not depend on the avail-ability of suitable anti-D. With regard toRHCE, forexample, theRh33allele and its protein would likewisebe called aberrantRHCEand aberrant RhCE. Null allelesof the RHD gene, which are associated with ineffectiveRhD protein expression, likeRHD(Q41X) (Aventet al.,1997c), may be referred to as nonfunctionalRHD.
RhD-negative phenotype and nonfunctional alleles
The characterization of molecular structure(s) underlyingthe RHD-negative haplotype is incomplete. Lack of thewhole RHD gene leads to the prevalence of the RhD-negative phenotype (Colinet al., 1991; Arce et al.,1993). Only the knowledge of theRHD-negative mole-cular structure(s) in various populations will permit ’RHgenotyping’ for RhD phenotype prediction in the future.
It is noteworthy that nonfunctional alleles generallyoccur rather frequently in most genes, as originallyshown by electrophoresis studies of enzymes inDroso-phila melanogaster(Langleyet al., 1981; Ohnishiet al.,
1982). Similar results were obtained for the populationfrequency of nonfunctional alleles in the human Htransferase gene (FUT1) (Wagner & Flegel, 1997). Themajority of nonfunctional alleles are due to mis-sense,frame shift and non-sense mutations in the codingsequence (Cooper & Krawczak, 1993); promoter defects,loss of start codon and alterations of splice sites may alsooccur. Nonfunctional alleles are of principal practicalimportance for the specificity of any genotyping strategyaiming for a phenotype prediction (Flegel, 1997).
Thus, it was not surprising frequently to encounterRhD-negative samples harbouringRHD-specific DNAstretches (Table 3). This list of nonfunctionalRHDalleles is expected to grow considerably. Their morefrequent occurrence among RhD-negative samples innon-Caucasian populations (Danielset al., 1997; Fuku-mori et al., 1997; Okudaet al., 1997) is explained in partby the lower prevalence of RhD-negative phenotypes inthese populations. These alleles confound DNA typing,because they are refractory to some, most or all currentDNA typing approaches.
The Rhnull phenotype of the regulator variant (Cherif-Zahar et al., 1996; Hylandet al., 1998) may carry anintact and functionalRHD allele and, hence, cannot bespecifically detected by any molecular analysis of theRHgene locus. Fortunately, this phenotype is even lessfrequent than the very rare Bombay phenotype in Cau-casians (Wagneret al., 1995).
GENERAL TECHNICAL ASPECTS FOR DNATYPING TECHNIQUES
DNA typing by PCR requires sample preparation andnucleic acid extraction; amplification of the desired’diagnostic’ DNA fragments; and the specific detectionof the amplicons. Robust methods, starting from thesample preparation to the final interpretation of theresults, are mandatory for any genotyping strategy. Thedevelopment of convenient procedures and reliableinstrumentation is anticipated to allow efficient andsafe handling. The total number of pipetting and transfersteps should be minimized to avoid contamination andsample mix-ups. Automatic pipetting robots are availablefor contamination-free and reliable pipetting of smallvolumes of reagents.
DNA extraction and DNA amplification by PCR
Extraction of DNA from the biological sample deservesspecial attention to ensure adequate purity (includingefficient removal of inhibitors such as haemoglobin) andadequate yield (even with relatively low numbers ofamniotic cells) for the ensuing PCR. Adsorption-basedextraction methods (e.g. spin-columns) have been
Rh phenotype prediction by DNA typing285
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

286 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Tab
le2.
Am
olec
ular
base
dno
men
clat
ure
for
aber
rant
RH
Dal
lele
san
daR
HC
Eal
lele
carr
ying
RH
Dsp
ecifi
cD
NA
stre
tche
s*
Phe
noty
pe
Nuc
leot
ide
Triv
ialn
ame†
Add
ition
al
Alle
leLo
catio
nch
ange
Par
tialD
Hap
loty
pe(s
)an
tigen
(s)
Ant
i-Dim
mun
izat
ion‡
Ref
eren
ces
Mis
sens
em
utat
ions
RH
D(L
110P
)ex
on2
T→C
at32
9DV
IIC
De
RH
40(T
ar)
wea
k,in
freq
uent
(Rou
illace
tal.,
1995
b;F
lege
leta
l.,19
96)
RH
D(R
229
L)ex
on5
G→A
at68
6D
HR
cDE
–no
tre
port
ed(J
oneset
al.,
1997
)
RH
D(T
283I
)ex
on6
C→T
at84
8D
HM
ic(
D)E
–st
rong
,on
esa
mpl
e(J
ones
,19
95;
Liu
eta
l.,19
96;
Wag
nere
tal.,
1998
b)
RH
D(G
353R
)ex
on7
G→A
at10
59D
NU
CD
e–
not
repo
rted
(Ave
nteta
l.,19
97a)
RH
D/R
HC
Eal
lele
sw
ithsi
ngle
orm
ultip
lesh
ort
conv
ersi
ons
RH
D(S
103P
)ex
on2
T→C
at30
7D
(Gne
gativ
e)cD
ER
H12
(G)
neg.
anti-
G,
one
sam
ple
(Faa
se
tal.,
1996
)
RH
D(A
354D
)ex
on7
C→A
at10
63DII
CD
e–
stro
ng,
rare
(Ave
nteta
l.,19
97a)
RH
D(N
152T
,T20
1R,F22
3V
)ex
on3,
4an
d5
conv
ersi
ons
DII
IacD
eR
H20
(VS
)st
rong
,fe
wsa
mpl
es(H
uanget
al.,
1997
;H
uang
,19
97b)
RH
D(L
62F
,N15
2T,D
350H
)ex
on3
and
7co
nver
sion
sD
IVa
(DIV
type
I)cD
e,C
De,
cDE
RH
30(G
oa )st
rong
,fe
wsa
mpl
es(R
ouill
aceta
l.,19
95a;
Hua
ng,
1997
b)
RH
D/R
HC
Ehy
brid
alle
les
(sin
gle
larg
erco
nver
sion
s)
RH
D-C
E(2
)-D
exon
2hy
brid
DIIIb
cDe
RH
12(G
)ne
g.;
RH
20(V
S)
stro
ng(R
ouill
aceta
l.,19
95c)
RH
D-C
E(3
)-D
exon
3hy
brid
DIIIc
CD
e–
stro
ng,
seve
rals
ampl
es(B
ecke
rse
tal.,
1996
a)
RH
D-C
E(3
–5
)-D§
exon
3–
5hy
brid
DH
Mii
cDE
–no
tre
port
ed(J
ones
,19
95;
Liu
eta
l.,19
96)
RH
D-C
e(3
–6
)-D
exon
3–
6hy
brid
DVI
type
IIIC
(D)e
RH
52(B
AR
C)
stro
ng,
one
sam
ple
¶(W
agne
reta
l.,19
98a)
RH
D-C
E(4
)-D
exon
4pa
rtia
lhy
brid
DF
RC
De>
cDE
RH
50(F
PT
T)
wea
k,on
esa
mpl
e(L
omaset
al.,
1994
;R
ouill
ace
tal.,
1995
a)
RH
D-c
E(4
–5
)-D
exon
4–
5hy
brid
DVI
type
Ic(
D)E
–st
rong
,fr
eque
nt(M
aask
ant-
van
Wijket
al.,
1997
a;A
vent
eta
l.,
1997
b;H
uang
,19
97a)
RH
D-C
E(4
–6
)-D
exon
4–
6hy
brid
DVI
type
IIC
(D)e
RH
52(B
AR
C)
stro
ng,
freq
uent
(Mou
roeta
l.,19
94)
RH
D-C
E(5
)-D
exon
5hy
brid
DVa
cDe,
CD
e,cD
ER
H23
(Dw)
stro
ng,
few
sam
ples
(Rou
illace
tal.,
1995
a)
RH
D-C
E(5
–7
)-D
exon
5–
7hy
brid
DB
TC
De
RH
32st
rong
,fe
wsa
mpl
es(B
ecke
rse
tal.,
1996
b;W
alla
cee
tal.,
1997
)
RH
D-C
E(6
–9
)-D
exon
6–
9hy
brid
DIVty
peIII
C(D
)e–
not
repo
rted
(Wag
neret
al.,
1998
b)
RH
D-C
E(7
–9
)-D
exon
7pa
rtto
9hy
brid
DIVb
(DIV
type
II)C
De
–st
rong
,ra
re(R
ouill
aceta
l.,19
95a)
RH
CE
/RH
Dhy
brid
alle
les
RH
CE
-D(5
)-C
Eex
on5
hybr
idR
h33,
R 0Ha
rc(
D)(
e)R
H33
,R
H50
(FP
TT
)w
eak,
few
sam
ples
(Bec
kers
eta
l.,19
96c;
Bec
kerse
tal.,
1996
d)
*Alle
leno
men
clat
ure
inac
cord
ance
with
publ
ishe
dre
com
men
datio
ns(B
eaud
ete
tal.,
1996
;B
eutle
reta
l.,19
96).
Mos
tkn
own
aber
rantR
HD
alle
les
are
show
nex
clud
ing
D–
–,
mol
ecul
arw
eak
Dty
pes
(Fle
gele
tal.,
1998
)an
dR
hD-n
egat
ive
phen
otyp
es(s
eeT
able
3).
Ach
arac
teriz
atio
nof
mor
eth
an15
alle
les,
allr
epre
sent
edby
mis
-sen
sem
utat
ions
,fo
rm
olec
ular
wea
kD
type
sis
fort
hcom
ing
(Wag
nere
tal.,
1998
b).
†Rev
iew
edby
Tip
pettet
al.
(199
6).
Par
tialD
was
defin
ed(S
alm
oneta
l.,19
84),
amon
got
her
feat
ures
,by
itsex
pres
sing
ofth
ean
tigen
Din
conj
unct
ion
with
the
esta
blis
hed
lack
ofon
eor
mor
eD
epito
pes
oral
lo-a
nti-D
imm
uniz
atio
nor
both
.T
heph
enot
ypes
ofD
cate
gorie
sco
nstit
ute
asu
bgro
upof
part
ialD
.T
helis
ting
ofD
cate
gorie
s(D
IIto
DV
II)
isco
mpl
ete,
sinc
eno
furt
her
part
ialD
will
bede
sign
ated
a’D
cate
gory
’:D
Ian
dDV
car
eob
sole
te(T
ippe
tt&
San
ger,
1977
;Lo
maset
al.,
1989
);DV
bch
arac
teriz
atio
nis
pend
ing.
As
exem
plifi
edby
DIV
and
DVI ,
the
Dca
tego
ryph
enot
ypes
can
besu
bdiv
ided
bym
olec
ular
char
acte
rizat
ion.
‡Sum
mar
ize
dby
Jone
se
tal.
(199
5)an
din
the
cite
dso
urce
repo
rts.
§Une
xpec
tedl
y,R
HD
intr
on4
was
repo
rted
tobe
pres
ent
(Jon
es,
1995
).A
full
char
acte
rizat
ion
ispe
ndin
g.¶In
abl
ood
sam
ple
kind
lypr
ovid
edby
Zhu
Zi-y
an,
Sha
ngha
i,C
hina
(Fle
gel&
Wag
ner,
1998
).

developed and are faster and easier than conventionalphenol-chloroform and salting-out procedures, but shouldbe carefully controlled for batch-to-batch variations. Fullyautomated validated commercial systems to extract nucleicacids from cells will help to facilitate and standardize thiscrucial step, which should be checked in quality controlprogrammes.
Substantial advances in the quality of commercialthermocyclers during the past decade have shifted therealization of adequate reaction conditions for the PCRfrom a delicate technical problem to a highly reproduci-ble routine procedure. Hot-start PCR techniques effi-ciently suppress mispriming. In a modular set-upseveral PCR-SSPs are performed in separate test tubesand analysed in parallel. In a multiplex set-up two ormore PCR-SSPs are run in one test tube. Integratingseveral different primer pairs into a multiplex PCR in asingle tube offers the important advantage of increasingthe efficiency of genotyping by reducing the number ofprocedures and the required amounts of both DNA andreagents. PCR methods for successfully accommodating11 or even more primer pairs in a single tube have beendescribed (Linet al., 1996). In DNA samples that containonly small amounts of contaminants interfering withPCR the yield of amplicons from a few primer pairsmay still be sufficient; DNA samples of lesser purityand quality may be more representative of the routinesituation and prone to yield less reliable results. Thus,
multiplex PCR has to be most thoroughly optimized andstandardized to accommodate adequate amplificationfrom DNA samples of variable quality.
Amplicon detection
RHDandRHCEallele-specific amplicons synthesized byPCR are easily detected by electrophoresis in agarosegels followed by ethidium bromide staining. Sensitivityof this step is appropriate for the investigation of manysamples and can be further improved by using eitheracrylamide gels or different dyes for staining, such asSYBR green I or silver. When testing a large number ofsamples, gel electrophoresis can easily limit the samplethroughput. ELISA detection of amplicons is feasible bydigoxigenin- or fluorescein-labelled primers used incombination with a biotinylated primer (Legleret al.,1996; Muller et al., 1997a). Incorporation of biotin intothe PCR products allows capture of the amplicons on anavidin-coated microtitre plate (Fischeret al., 1995);digoxigenin and fluorescein antibodies then offer con-venient means for detection of amplicons in hundreds ofsamples and for automation (Mu¨ller et al., 1997a).Simultaneous generation of several different ampliconsby multiplex PCR requires not only adequate detectionsensitivity but also high separation efficiency, especiallyfor amplicons of similar size. Excellent resolution of
Rh phenotype prediction by DNA typing287
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Table 3. RhD-negative phenotypes harboringRHD-specific DNA sequences*
Nucleotide ProbableAllele Location change haplotype Populations References
RHD(Q41X) exon 1 C→T at 121 Cde White (Aventet al., 1997c)RHD-CE(2–9)-D exon 2 or 3–9 possible hybrid allele Cde White† & African (Hylandet al., 1994;
Andrewset al., 1998b)(Huang, 1996)
RHD-CE(3–7)-D exon 3–7 hybrid allele Cdes African & Asian (Bluntet al., 1994;Carritt et al., 1994;Faaset al., 1997a)
RHD(488del4) exon 4 deletion of 4 bp Cde White (Hylandet al., 1994;from 488: frameshift
Andrewset al., 1998a,b)RHD-CE(4–7)-D exon 4–7 hybrid allele cdE White† (Faaset al., 1996,1997a;
Avent et al., 1997c;RHD(exon 5 variant) exon 5 not communicated‡ cde not communicated (Carrittet al., 1994)RHD(G314 V) exon 7 G→T at 941 Cde Japanese (Okudaet al., 1997)RHD(exon 9 variant) exon 9 unknown Cde White (Gassneret al., 1997b)
*Although no data have been gathered, frequent anti-D immunizations would be expected, if carriers were transfused RhD positive. †Australianblood donors of white descent (C. A. Hyland and B. H. W. Faas, written and personal communications). ‡The presence of a stop codon in exon 5was reported without indicating the affected nucleotide position(s); no full report has been published since.

288 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Tab
le4.
Res
ults
ofso
me
publ
ishe
dP
CR
set-
ups
appl
ied
toR
HD
NA
typi
ng
Pol
ymor
phis
ms
test
ed
Abe
rran
tal
lele
Tec
hnic
alpr
oble
m§
PC
RM
othe
r(M
)Lo
catio
nS
ampl
es
fetu
s(F
)G
enes
/S
ites
test
edD
etec
ted†
Mis
type
d‡M
isty
ped
No
ampl
icon
Ref
eren
ces
set-
upm
etho
ds*
test
edal
lele
s(
n)In
tron
Exo
n(n)
(n)
(n)
(n)
(n)
Loe
tal.
(199
3)si
ngle
SS
PF
RH
D1
–10
¶71
00
20
Arc
ee
tal.
(199
3)si
ngle
LPno
RH
D1
4–
80
00
0
Ben
nette
tal.
(199
3)si
ngle
SS
PF
RH
D1
–10
150
00
0
Wol
tere
tal.
(199
3)si
ngle
SS
Pno
RH
D1
–7
30
00
0
Ros
site
reta
l.(1
994)
sing
leLP
FR
HD
14
–28
00
00
Yan
kow
itze
tal.
(199
5)si
ngle
LPno
RH
D1
4–
765
09
01
van
den
Vey
vere
tal.
(199
5)si
ngle
SS
PF
RH
D1
–7
100
00
21
Ligh
ten
eta
l.(1
995)
sing
leS
SP
FR
HD
1–
1013
50
02
1
Adi
nolfi
eta
l.(1
995)
sing
leS
SP
FR
HD
1–
1012
00
20
Sim
seke
tal.
(199
4,19
95)
mod
ular
LP/S
SP
FR
HD
34
7an
d10
234
50
00
Spe
ncee
tal.
(199
5a)
mul
tiple
xLP
/SS
PF
RH
D2
410
500
00
0
Pop
eeta
l.(1
995)
mul
tiple
xLP
/SS
PF
RH
D2
410
631
00
0
Pou
ltere
tal.
(199
6)si
ngle
RF
LPno
RH
D1
2–
105
00
00
van
den
Vey
vere
tal.
(199
6)si
ngle
SS
PF
RH
D1
–7
108
00
00
Sek
izaw
aeta
l.(1
996)
sing
leS
SP
MR
HD
1–
710
00
04
Dild
ye
tal.
(199
6)si
ngle
SS
PF
RH
D1
–10
347
00
10
Ton
ne
tal.
(199
7)si
ngle
SS
Pno
RH
D1
–10
780
00
0
Maa
seta
l.(1
997)
mod
ular
SS
P/L
CR
noR
HD
3–
2,5
and
720
70
00
0
Gas
sner
eta
l.(1
997b
)**
mod
ular
SS
Pno
RH
D8
–2
–7,
9an
d10
354
20
00
Ave
nte
tal.
(199
7c)
mul
tiple
xS
SP
FR
HD
24
1035
713
70
0
Maa
skan
t-va
nW
ijke
ta
l.(1
997b
)m
ultip
lex
SS
Pno
RH
D6
–3,
4,5,
6,7
and
912
64
00
0
Mul
ler
eta
l.(1
997b
)††
mul
tiple
xS
SP
FR
HD
9–
2–
7,9
and
1011
00
00
0
Wag
nere
tal.
(199
8b)
sing
leLP
noR
HD
13
–27
00
00
Tot
alsa
mpl
enu
mbe
ras
saye
dfo
rR
HD
3313
25(0
·75%
)16
(0·5
%)
LeV
anK
ime
tal.
(199
4)m
ultip
lex
SS
PF
ca
nd
E2
–2
and
514
00
00
Faa
seta
l.(1
995)
mod
ular
SS
Pno
Ea
nd
e1
–5
158
00
00
Pou
ltere
tal.
(199
6)m
odul
arS
SP
noC
an
dc
12
–10
50
00
0
Yan
kow
itze
tal.
(199
7)m
odul
arR
FLP
noC
,c
an
dE
3–
1,2
and
565
50
23/1
7/8
00

the amplicon separation is routinely achieved by thetechniques established for DNA sequencing.
APPLICATION OF PCR-SSP TORH DNATYPING
PCR using sequence-specific priming (PCR-SSP), alsoknown as allele-specific primer amplification (ASPA),allows the specific detection of nucleotides at predeter-mined sequence positions. PCR-SSP can be devised tosuit modular and multiplex PCR set-ups, may be adaptedfor detection of most nucleotide polymorphisms and forstandardized thermocycling conditions, and is rapid. Thus,PCR-SSP is preferred forRH DNA typing by mostresearch groups and in more recent PCR set-ups (Table 4).
Single primer pairs
As noted previously, PCR set-ups with a single primerpair only are not considered reliable and should notgenerally be applied for diagnostic purposes. They maybe very useful to distinguish and characterize rare alleles.Limited studies with new primer pairs for single sites areconducted to establish specificity and robustness, beforea primer pair is added to established modular or multi-plex systems.
Modular systems
With PCR set-ups comprising two or more primer pairsthe rate of false positive and false negative results can bediminished. However, samples of unknownRHD struc-ture may still be retrieved, whose clinical relevance is notimmediately apparent.
We developed a modularRHD PCR-SSP systemconsisting of seven PCR reactions specific forRHDexons 3–7, 9 and 10 plus one PCR reaction detectingexon 2 ofRHDor theC allele ofRHCE(Table 1 and Fig.2). To maximize the information obtained about theprotein sequence, only nucleotide substitutions determin-ing amino acid polymorphisms were chosen for detec-tion. The screening of allRHD exons differing fromRHCE allows the identification of anyRHD–CE–Dhybrid allele that involves at least one full exon, becausethe lack of anyRHD-specific exon would always bedetected by one or more negativeRHD-specific reaction.This system proved very efficient for the rapid identifica-tion and preliminary characterization of new forms ofpartial D due toRHD–CE–Dhybrid proteins (Gassneretal., 1997b; Wagneret al., 1998a). Additional PCR-SSPreactions may be added to detect partial D, like DVII ,caused by mis-sense mutations (Fig. 2).
TheRHD typing system is complemented by six PCRreactions detecting the Rh antigens Cw, C, c, E and e
Rh phenotype prediction by DNA typing289
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Tab
le4.
Res
ults
ofso
me
publ
ishe
dP
CR
set-
ups
appl
ied
toR
HD
NA
typi
ng
Pol
ymor
phis
ms
test
ed
Abe
rran
tal
lele
Tec
hnic
alpr
oble
m§
PC
RM
othe
r(M
)Lo
catio
nS
ampl
es
fetu
s(F
)G
enes
/S
ites
test
edD
etec
ted†
Mis
type
d‡M
isty
ped
No.
ampl
icon
Ref
eren
ces
set-
upm
etho
ds*
test
edal
lele
s(
n)In
tron
Exo
n(n)
(n)
(n)
(n)
(n)
Gas
sner
eta
l.(1
997b
)**
mod
ular
SS
Pno
C,
c,E
an
de
4–
1,2
and
535
40
42/0
/0/0
00
Tan
akae
tal.
(199
7)m
odul
arS
SP
noC
,c,
Ea
nd
e5
–1,
2an
d5
513
02/
0/0/
00
0
Mul
ler
eta
l.(1
997b
)††
mul
tiple
xS
SP
FC
,C
w,
c,E
an
de
62
1,2
and
511
00
00
0
*SS
P–
sequ
ence
-spe
cific
prim
er;
LP–
leng
thpo
lym
orph
ism
;R
FLP
–re
stric
tion
frag
men
tLP
;LC
R–
ligas
ech
ain
reac
tion.
†Dis
crep
ant
resu
ltsno
tex
plai
ned
bykn
own
part
ialD
.‡T
hehi
ghra
teof
mis
typi
ngs
inso
me
stud
ies
was
ofte
nca
used
byhi
ghly
sele
cted
sam
ples
.§A
llte
chni
calp
robl
ems
wer
eca
used
byco
ntam
inat
ion
oram
plifi
catio
nfa
ilure
infe
talt
issu
ete
stin
g.¶B
ecau
seth
ere
isno
poly
mor
phic
site
inth
eco
ding
sequ
ence
ofex
on10
,th
e3
0un
tran
slat
ed
regi
on(U
TR
)of
exon
10is
assa
yed.
**M
odul
arex
tens
ions
ofth
eP
CR
set-
up(G
assn
ere
tal.,
1997
a)ha
vebe
ende
scrib
edsi
nce
(see
Fig
.2)
and
utili
zed
inth
em
ultip
lex
assa
yof
Mu
¨ lle
re
tal.
(199
7b).
††F
iftee
nsi
tes
repr
esen
ting
8R
HD
,5
RH
CE,
1D
VII
and
1C
Wsp
ecifi
csi
tes
wer
eut
ilize
dfo
ram
plifi
catio
nsin
four
mul
tiple
xP
CR
and
anal
ysed
inon
ese
mia
utom
ated
fluor
esce
nce
read
ing
(for
anou
tline
ofth
em
etho
dse
eF
ig.4
).

290 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

(Table 1 and Fig. 2) (Gassneret al., 1997b). Typing forthe C allele ofRHCEwas generally considered difficultand unreliable (Faaset al., 1997b): the identity ofRHDalleles and theC allele ofRHCE in exon 2 prevents thespecific detection of theC allele in RHD-positive sam-ples by these nucleotide positions. Typing for theC alleleat position 48 in exon 1 was also unreliable (Faaset al.,1997b; Gassneret al., 1997b; Faas, 1998). This wasrecently explained by our finding that C48 is shared by ac allele occurring in most cDe (Gassneret al., 1997b) anda few cde haplotypes (own unpublished observation;Tanakaet al., 1997). In the meantime we added aC-allele-specific PCR-SSP (Gassneret al., 1997a) based ona C-allele-specific intron 2 polymorphism (Poulteret al.,1996) to our modular PCR set-up. AC-allele-specificDNA typing performed with this reaction was concordantwith the C antigen serology without exception in more than500 samples investigated (unpublished observations) ren-dering this system reliable forC-allele-specific DNAtyping. Although data from the African populations arelacking, a similar excellent concordance is predicted, if thehigh false-positive rate in Africans can be explained by theprevalance of the cDe haplotype in that population.
The sequence of thec alleles of RHCE is identicaleither to the sequence of theC alleles ofRHCE or toRHDalleles in all exons but exon 2. Hence, typing for acallele of RHCE is performed utilizing two polymorphicnucleotide positions in exon 2 (Table 1). The onlydifference between theE ande alleles ofRHCE is a C(E alleles)/G (e alleles) polymorphism at position 676located in exon 5. TheRHD alleles share the G atposition 676. A PCR-SSP detecting this polymorphicnucleotide only may hence coamplify allRHD-positivehaplotypes. For this reason, the PCR-SSP reactions forthe E/e polymorphism utilizes two sequence-specificprimers: one primer detects anRHCE-specific nucleotideat position 787 and suppresses the coamplification of allRHD alleles, and the other discriminates theE/e poly-morphism at position 676 by being specific for either theE or thee alleles ofRHCE(Table 1). Finally, a reactiondetecting position 122 in exon 2 specific for theCw allelewas recently added to our modular typing system (Table1 and Fig. 2).
In summary, a total of 15 PCR-SSP reactions detect 17of about 41 amino acid polymorphisms crucial for mostantigen specificities of the Rh blood group system. Thisenabled us to type samples with an unprecedentedaccuracy. Since all PCR-SSP reactions are performedwith identical thermocycling conditions, the number ofPCR reactions does not affect the assay time. If thedetection of alleles, defined by many other mis-sensemutations and coding for Rh antigens, like DII, DNU,DHR, DHMi, Cx, RH26 and VS, is considered impor-tant, additional modules may be added easily. On theother hand,RHD-specific reactions may be omitted ifthey were shown redundant for a given accuracy in anydistinct population. Most importantly for a rationaltesting strategy,RHD PCR-SSP modules specific fornonfunctionalRHD alleles may be added as soon astheir occurrence and molecular cause is identified(Table 3). Once a modular system forRH DNAtyping is established, it may be easily transferred toapplications using fluorescence and otherwise labelledprimers.
Modular systems with fluorescence-labelled primers
Fluorescence detection in a modular PCR-SSP forRHD/CE DNA typing has been shown to enhance the assaysensitivity (Tonnet al., 1997). Promising technologieshave been introduced to detect newly formed ampliconswhilst the PCR amplification is still in progress (Heidetal., 1996; Morriset al., 1996; Kalininaet al., 1997; Wooet al., 1998). A relevant DNA stretch is amplified by PCRusing sequence-specific priming, for example. A shortoligonucleotide (‘TaqMan probe’) carrying a fluores-cence dye as reporter at its 50 end and a quencher dyeat its 30 end can hybridize specifically to the amplicon.The ensuing PCR releases the reporter dye from theprobe due to the 50 nuclease activity of the polymerase.The released fluorescence dye no longer being quenchedis indicative of the amount of amplicons produced. Inarrays of 96 samples, the change of fluorescence inclosed PCR tubes can be detected simultaneously andoffers an extraordinarily efficient and quantitative readout whilst the PCR thermocycling is still under way. This
Rh phenotype prediction by DNA typing291
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Fig. 2. Representative results of a modularRHPCR-SSP system. Panels A to D show agarose gel electrophoresis of 15RHPCR-SSPreactions. The Rh phenotypes (bold type) and the detected DNA type (italics) are indicated above each panel. TheRH PCR-SSPreactions are specified in the boxed interpretation scheme below the panels; the reactions 10 and 13 indicated by c* and C* aredetecting thec(W16C) allele ofRHCEin addition to thec andC alleles ofRHCEthat are prevalent among Caucasians. In the ccddeephenotype shown in panel A no reactions specific forRHDare detected. The reaction patterns in panel B, PCR-SSP positive forRHDexon 5, and in panel C, PCR-SSP negative forRHDexons 4 and 5, indicate the presence of theRh33andDVI type Ialleles. The CcDeephenotype in panel D shows specific products in all PCR-SSP reactions geared to detectRHDexons. Specific products were also foundin theRHCEPCR-SSP reaction of all four samples in concordance with their RhCE phenotypes. The 434-bp internal control amplicon,which was devised to be larger than anyRH-specific amplicon, may be suppressed because of competition, if a specific product isamplified.

technology reduces dramatically the risk of contamina-tion by amplicons generated during the PCR.
Multiplex systems
In multiplex systems, several specific PCR reactions areperformed in a single tube. This allows detection of morethan one polymorphism in a single DNA sample and inone PCR reaction. The development of advanced multi-plex systems is a laborious task. The different PCRreactions must be orchestrated to work with equal effi-ciencies under the same thermocycling conditions andwithout loss of specific bands due to competition.
The first multiplex systems proposed forRHD DNAtyping involved combinations of the intron 4 lengthpolymorphism with the exon 10 SSP reaction (Spenceet al., 1995a; Popeet al., 1995) and included specificPCR products of up to 600 bp length. To improve thestability of the intron 4 system, Aventet al. (1997c)engineered two PCR-SSP reactions whose sequence-specific primers are located in theRHCE intron 4sequence and span theRHD deletion point. These tworeactions were combined with an exon-10-basedRHD
PCR-SSP resulting in a true SSP multiplex systemdetectingRHD intron 4 and exon 10. This system wasuseful for screening a large number of samples foraberrantRHD alleles and led to the identification of theRHD(Q41X) allele. The authors’ data indicated that falsepositive results due to sporadic mutations may be fre-quent among Cde and cdE haplotypes and may remain aproblem even for multiplex systems.
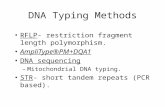
Maaskant-van Wijket al. (1997b) recently presented amultiplex system that incorporates reactions forRHDexons 3, 4, 5, 6, 7 and 9, all the informativeRHD exons,along with ab-actin control, in a single tube. Specificproducts range from 157 to 57 bp and were visualized ina polyacrylamide gel (Fig. 3, gel image courtesy of P. A.Maaskant-van Wijk). This elaborate system allowed thecorrect identification of all knownRHD–CE–D hybridalleles with the only exception of DIIIb. The inclusion ofso many reactions into a single tube is complicated, andinternal mismatch bases had to be introduced into severalprimers to increase specificity. Furthermore, strict qual-ity control is needed, because with a DNA concentrationof less than 10 ng, specific bands may be lost while thecontrol band is still amplified. Full concordance for all
292 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Fig. 3. Representative results of a multiplexRHD PCR-SSP system. Specific products of different lengths are amplified forRHDexons 3, 4, 5, 6, 7 and 9 and separated by polyacrylamide gel electrophoresis (PAGE). The regular RhD-positive phenotype, lane 2,carries allRHD-specific sites; the ccddee phenotype, lane 3, noRHD-specific site. R0
Har and partial D are represented by exon patternsthat may be diagnostic: lane 4,R0
Har; lane 5,DIVb; lane 6,DIVa; lane 7,DVI type I; lane 8,DVI type II; lane 9,DVa; lane 10,DFR;lane 11,DIIIc . Lane 1: DNA size markers (10-bp ladder); lane 12: water control; i.c.: 200-bp internal control amplicon. The gel imagewas kindly provided by Petra A. Maaskant-van Wijk.

systems was observed in 40 RhD-positive and 13 RhD-negative Caucasians. However, among 46 non-CaucasianRhD-positive individuals, two partial D (DIVa and DVa)were identified, suggesting that these partial D are frequentamong non-Caucasians. The authors proposed the applica-tion of this single tube system for prenatal testing and forpopulation screening, which would facilitate the immedi-ate identification and classification of most partial D.
Multiplex systems with fluorescence labelled primers
We have developed a strategy forRHD/CE DNA typingin large numbers of samples (Mu¨ller et al., 1997b), whichis outlined in Fig. 4. Fifteen primer pairs specific forRHD or RHCE(Gassneret al., 1997b) were used in fourmultiplex PCR reactions to amplifyRHD/CE-allele-spe-cific segments. One primer of each pair is labelled witheither 6-carboxy-fluorescein, tetrachloro-6-carboxy-fluorescein or hexachloro-6-carboxy-fluorescein. ThePCR products of all four tubes with the same DNAsample are pooled after completion of the PCR reactionsand the primers are removed by adsorption to columns.The pooled amplicons are finally separated by capillaryelectrophoresis and fluorescence detection of the labelsusing an automated nucleotide sequencer (ABI PrismGenetic Analyser 310; Applied Biosystems, Foster City,CA, USA). Electrophoretic separation of up to 15 dif-ferent products from the multiplex PCR in a 47-cm-longcapillary (0·05 mm internal diameter) filled with thePOP-6 polymer is completed within 25 min after injec-tion of the sample. A highly reproducible measurementof the size of the amplicons is ensured by comparison ofthe retention times of the amplicons to those of internalstandards of defined size. Combining these size measure-ments with analysis of the fluorescence of the differentdyes reliably identifies the products generated by multi-plex PCR. Up to 96 samples, which may contain themixed products of the four multiplex PCR, are automa-tically injected and analysed sequentially. Validationexperiments demonstrate the high reliability (concordantresults with serotyping for samples from 100 donors) andgood sensitivity (adequate for the analysis of samplesfrom amniotic fluid) of this approach. This method ofmultiplex PCR with fluorescent primers together withautomated identification of the pooled amplificationproducts allowed semiautomatedRHD/CE genotypingbased on a multitude of ’diagnostic’ DNA polymorphisms.
OTHER TECHNIQUES SUITABLE FORDETECTING KNOWN SEQUENCEPOLYMORPHISMS
Several alternatives to PCR-SSP are available todetect defined sequence polymorphisms. Some lack the
versatility of PCR-SSP or have not yet been applied toRH DNA typing.
Rh phenotype prediction by DNA typing293
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302
Fig. 4. Outline of a blood group genotyping strategy suitablefor testing large numbers of blood samples. As an example, theapplication to multiplexRHD/CE DNA typing is shown. PCRamplification of many DNA fragments is performed in amodular fashion using fluorescence-labelled sequence-specificprimers. After primer removal the amplicons can be specificallydetected according to their fragment length and colour. Thereading is achieved in an automated procedure by capillaryelectrophoresis followed by fluorescence detection. Theprocedure lends itself to automatic data retrieval, interpretationand documentation. Other large-scale genotyping procedurescurrently being developed are discussed in the text.

PCR amplicon hybridization with sequence-specificoligonucleotides (PCR-SSO)
PCR amplicon capturing to a solid phase, like filters andmicrotitre wells, followed by hybridization withsequence-specific oligonucleotides, or the ’reverse dottechnique’, is widely used forHLA genotyping. Althoughno applications forRH DNA typing have been estab-lished, the potential for automation, such as withenzyme-linked detection systems, is great. The knowl-edge of allele polymorphisms established by PCR-SSPcan be easily applied to PCR-SSO.
Ligase chain reaction
The ligase chain reaction involves cyclic, sequence-dependent ligation of two oligonucleotides and is oftenused as a second step following PCR amplification. Thecombination of a biotin-labelled oligonucleotide with adigoxygenin-labelled oligonucleotide allows detection ofthe ligation product by ELISA, making this methodamenable to automation. To date, a single application forRH DNA typing has been described (Maaset al., 1997).
PCR amplicon length polymorphism
In the introns of theRH genes, there are several inser-tions, deletions and repeat number polymorphisms.Amplification of these regions by flanking primersresults in amplicons of gene or allele-specific lengthsthat can be separated by gel electrophoresis.RHD-specific sequences andRHCE-specific controls areamplified in the same tube by the same primer pair,obviating the need for additional controls. The first and amajor application isRHD typing by an intron 4 deletion(Arceet al., 1993). The linkage of intron polymorphismsto RHphenotypes is excellent and some systems, like thedetection of theC allele by virtue of an intron 2 insertion(Poulteret al., 1996), are more informative than exon-based assays. Technical limitations may be encounteredbecause PCR conditions depend on the length of theinvestigated deletion. They tend to involve comparablylong extension periods, which often prevents the techni-que from being suitable for modular systems. Then,PCR-SSP devised for the same polymorphism (Aventet al., 1997c; Gassneret al., 1997a) may be more useful.
PCR combined with restiction fragment lengthpolymorphism (PCR-RFLP)
PCR amplicon digestion by restriction enzymes andanalysis of the restriction fragment length polymorphismmay detect single nucleotide substitutions located inrestriction sites. A major application is c/D typing in
intron 2 (Poulteret al., 1996). Enzyme digestion maytake less than 2 min if it is performed by microwaveheating (Poulteret al., 1996). Sufficient digestion shouldbe controlled by an additional restriction site present inall amplicons. PCR-RFLP is easy to establish if arestriction site happens to incorporate the polymorphicsite (Beckerset al., 1996b), but this is not the rule.Compared to PCR-SSP, there is more hands-on time andmuch less potential for modular set-ups.
TECHNIQUES SUITABLE TO DETECTUNEXPECTED SEQUENCEPOLYMORPHISMS
PCR-SSP and the similar methods presented in thepreceding sections are geared to detect distinct knownpolymorphisms and they will rarely detect other nucleo-tide sequence aberrations by chance. Several techniquesdo not aim for specific nucleotide polymorphisms butallow screening for aberrations occurring in longerstretches of a nucleotide sequence. Hence, for example,sporadic non-sense mutations may not escape detection,which furthers the test specificity. The enhanced infor-mation retrieval must be weighed against the increasedcomplexity of the assays. Furthermore, routine applica-tion may be hampered by the detection of frequent(Stoerkeret al., 1996), yet clinically irrelevant, silentor intronic mutations, which may incur clinically futilework-up. In the field ofRH typing, denaturing gradientgel electrophoresis, heteroduplex analysis, single-strandconformation polymorphism and conventional sequen-cing have been utilized.
Denaturing gradient gel electrophoresis (DGGE)
In DGGE, double-stranded PCR amplicons are electro-phoresed through a gradient of a denaturing agent ofincreasing concentration. At a characteristic concentra-tion, part of the double-stranded DNA sequence beginsmelting, which results in an abrupt decrease of mobilityand a characteristic sequence-dependent pattern (Fischer& Lerman, 1983). Electrophoresis usually takes 24 h andgel conditions must be specifically adapted for eachamplicon, restricting DGGE largely to research ques-tions. DGGE has been applied toRH exons 2 and 5(Steerset al., 1996).
Heteroduplex analysis
Heteroduplexes containing single base mismatches canbe separated from homoduplexes and other heterodu-plexes by nondenaturing gel electrophoresis. EngineeredDNA fragments with small deletions may ensure hetero-duplex generation for almost any allele. Heteroduplex
294 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

systems have been developed for exons 2 and 5 (Stoerkeret al., 1996) and applied for routine use (Roseet al.,1997).
Single-strand conformation polymorphism (SSCP)
The electrophoretic behaviour of single-stranded DNA innondenaturing gels depends on sequence-specific sec-ondary structures. This biological feature is utilized inSSCP. After denaturing by heat, electrophoresis can beperformed in about 15 min. SSCP is hence much fasterand simpler than DGGE or heteroduplex analysis. It isless sensitive and may miss about 20% of mutations.Recently, SSCP was utilized for screening for the G286Amutation determining the Rh:-26 phenotype (Faaset al.,1997c).
Conventional sequencing
The gold standard for nucleotide sequence determinationis the full length sequencing of the desired stretch of thenucleic acid. The classical approach for the definition ofaberrantRH alleles involves RNA isolation, reversetranscription, subcloning and plasmid sequencing. Theprocedure is very laborious and prone to mistakesbecause of splice variants, which are particularly abun-dant amongRH transcripts. Identification of mis-sensemutations may be hampered by misincorparated nucleo-tides introduced by PCR and selected by subcloning ofthe plasmids.
Genomic sequencing has been used for screening forthe DVII mutation (Flegelet al., 1996). It is less laboriousand obviates the need for subcloning, but the detectionrate for heterozygotes may be less than 100%. Recently,we developed anRHD-specific genomic sequencingsystem for all exons obviating the need for subcloning(Wagneret al., 1998b). If hybrid alleles involving largegene conversions are excluded by PCR-SSP, thisapproach allows sequence determination of the fullcoding sequence with an expected detection rate of100% within 3 working days. The utility of this systemhas been demonstrated by the identification of more than15 alleles constituting the molecular cause of the weak Dphenotype (Flegelet al., 1998).
FUTURE TECHNOLOGIES: BIOCHIPS
Biochips and PCR chips (Cheeet al., 1996; Wodickaetal., 1997) could be used to determine the nucleotides ateach of the< 37 exon positions differing between theRHCEand theRHDgenes. Presently it is doubtful if thisresolution is really needed for clinically relevantRHDNA typing. Only population-wide sequence character-ization of manyRHD andRHCEalleles will adequately
address this question. However, with much improvedcost-efficiency the resolution of all cDNA nucleotidepositions revealing all possible non-sense mutationsmight become feasible and would enhance the reliabilityfor futureRHgenotyping to unprecedented levels clearlyexceeding the precision of any serology-based method.
TOWARDS A RATIONAL TESTINGSTRATEGY
There is currently no optimalRH DNA typing strategysuiting all applications. DNA typing is performed fordifferent populations and for different purposes. It isapparent from the previous sections that the techniquesvary widely from few or multiple PCR reactions per-formed in separate tubes to multiplex reactions in singletubes. The use of two or more ’diagnostic sites’ isrecommended to limit the rate of false results. Further-more, the equipment for and experience with genotypingsystems, which may be available in a laboratory, willoften guide the selection for a particularRHDNA typingsystem. For the broader application in clinical routinelaboratories a PCR-based approach in conjunction withthe specific detection of certain nucleotide positions bysequence-specific oligonucleotides is generally favoured.
Importance of the population tested
The polymorphisms (alleles) of a gene, their populationfrequencies and distribution in the examined populationhave critical importance for the practical application ofDNA typing. Most RH DNA typing data derive fromCaucasians. In African and Japanese people, there is alarge fraction of RhD-negative alleles that harbourRHD-specific sequences and are not correctly recognized withalmost any published strategy. The more frequent partialD differ between non-Caucasian (DIVa) and Caucasian(DVII ) populations. ReliableRH DNA typing in non-Caucasian populations will have to await the identifica-tion of the more prevalent alleles in RhD-negativesamples present in those populations. DNA typing inrandom samples without reference to the allele poolinvolved, i.e. the genetic derivation of the probands, isprone to mistakes. At the moment, the rate of false Rhphenotype predictions in populations other than Cauca-sians cannot be estimated reliably. Admixtures to theallele pool introduced by non-Caucasians may hamperRH DNA typing even in Western populations.
The Japanese RhD-negative samples may represent aspecial problem because they were reported to possess anormal RHD promoter, plentifulRHD mRNA, and anRHD coding sequence with a single mis-sense mutation(Okudaet al., 1997) that appeared not to be diagnostic. Ifhigh-precision DNA typing is attempted, the prevalence
Rh phenotype prediction by DNA typing295
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

of rare variants may become more important. Genotypesunderlying partial D, for example D category VI, varyeven within closely related Caucasian populations(Wagneret al., 1998a). The relevant questions may beanswered by population-based approaches, which may, ifproperly conducted, yield interesting data for scientificproblems.
Which polymorphism should be tested?
The expense of a genotyping system must be weighedagainst its residual failure rate in phenotype prediction todetermine its cost-efficiency. In almost all current geno-typing strategies rather short nucleic acid sequences areutilized. Full coverage of the cDNA is not practicalwith the available technology, and full coverage of agene cannot even be attempted. Therefore, the phenotypeprediction depends critically on the functional integrityof the detected allele (Flegel, 1997). To limit falsepositive RHD DNA typing, there is unfortunately noexpedient alternative method to specifically detect themultiple RHD sequence aberrations occurring in RhD-negative phenotypes (Table 3). Because these allelesoccur with moderate frequencies even in Caucasians,genotyping strategies should address this problem.
DNA typing experience with rare phenotypes (Aventet al., 1997c) and the phenotype frequency data (Wagneret al., 1995) indicated that the correct Rh phenotype ispredicted in more than 99·5% of unselected samples fromCaucasians even by testing of a single polymorphismonly. The detection of a second polymorphism raisesaccuracy to about 99·9% (Table 4), which is currently therecommended approach (Bennett & Cartron, 1994;Simseket al., 1994; Lightenet al., 1995). If two poly-morphisms are to be tested, we favour two ’diagnosticsites’ located in exon 4/intron 4 and in exon 7 (Table 1).By this approach, the clinically most relevant partial D,DVI and DIV, are recognized and the RhD-negativealleles due toRHD–CE–Dhybrids involving substitu-tions in exons 4–7 (Table 3) are correctly predicted asRhD-negative. If three polymorphisms are to be tested,we recommend sites located in exons 4, 5 and 7 becausethis approach would test all three exofacial loops differ-ing betweenRHDand theC allele ofRHCE. To increasethe specificity further, allRHD-specific exons can betested (Table 1 and Fig. 2). However, the estimatedfrequency of partial D due toRHD–CE–Dhybrid allelesother than DVI and DIV is less than 1 : 10 000 amongunselected samples from Caucasians (Flegel & Wagner,1996; Roubinetet al., 1996).
Importance of the application
For paternity testing, usually DNA of the mother, childand putative father is available. As long as results are
obtained with the same method for all involved persons,mismatches between phenotype and DNA type will notaffect paternity prediction. The frequency discrepancybetween DNA-based and phenotypic haplotypes isusually too small to affect probability calculations sig-nificantly. Hence, a robust single polymorphism assaycan be considered sufficient (van den Veyveret al.,1996). Methods, like DGGE, that allow the detection ofsporadic aberrantRH alleles may enhance somewhat thepredictive value ofRHDNA typing in paternity testing ifone of the persons possesses a rare aberrant allele. Itremains doubtful whether this small advantage merits theadditional effort of more complicated test systems.
For prenatal prediction of the Rh phenotype in Cau-casians, typing errors due to technical problems includ-ing contamination with maternal blood are likely toinfluence the error rate more than the residual 0·1% ofrare alleles that may be mistyped. Hence, for prenataltesting, a robust modular or multiplex system involvingtwo or more polymorphisms may be chosen. Because ofthe lower rate of fetal loss incurred by the less invasivesampling procedures (van den Veyver & Moise, 1996),theRHDDNA typing is today clearly the method of firstchoice for predicting the fetal RhD phenotype.
On the other hand, a 99·9% accuracy is not sufficient ifa replacement for routine serological methods isrequired. Contrary to a common perception, the majorobstacle for Rh phenotype prediction is those RhD-negative phenotypes that carryRHD-specific DNAstretches (Table 3) rather than partial D. In Caucasians,such samples occurred with a frequency of about 5%among Ccddee and ccddEe samples (Aventet al.,1997c), resulting in an estimated population frequencyof about 1 : 1000–2000. This rate exceeds by far that ofclinically relevant partial D, like DVI (Wagneret al.,1995). Hence, further advances inRH DNA typing ofunselected individuals is unlikely to be achieved byadding more RHD exon-specific reactions only.Improvements will rather necessitate the identificationand specific detection of nonfunctionalRHD alleles. Inthis respect, modular approaches have the advantage thatadditional reactions may be easily incorporated.
A quite different situation concerns the screening ofphenotypically abnormal samples, for example partial Dand weak D. In partial D, an aberrantRHDsequence mayalmost always be detected, whereas a serological dis-crimination can be cumbersome or misleading. ExonscanningRHD PCR (Gassneret al., 1997b; Maaskant-van Wijk et al., 1997b) identifies those interestingsamples of hybridRHD/CE structure rapidly that meritfurther characterization by cDNA sequencing. ForRHDalleles with point mutations, genomic sequencing(Wagneret al., 1998b) is today the most straightforwardand rapid approach. The improved resolution achieved
296 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

by PCR detection of multipleRHD-specific products isuseful for population surveys to elaborate the geneticbasis of the various RhD and RhCE phenotypes.
Laboratory-specific considerations
Within the mentioned framework ofRH DNA typingstrategies, the selection of a specific DNA typing systemmay be guided by practical considerations specific for aparticular laboratory. The more expedient of two other-wise comparable systems will generally be preferred.Often, it is advantageous to select anRH DNA typingsystem with thermocycling conditions already applied inthe laboratory for other purposes, such asHLA genotyp-ing. Investigators less experienced with DNA typing mayprefer robust test systems, which are only marginallyaffected by variable DNA quality. ELISA- or fluores-cence-based systems necessitate special equipment, butare likely to vastly outperform other systems if large-scale DNA typing is attempted.
CONCLUSION
Blood group phenotype prediction by molecular methodsis feasible and for some applications are already superiorto standard serological phenotyping. Examples forRHDNA typing are prenatal diagnostics and characteriza-tion of aberrant Rhesus proteins including partial D.
Personally, we will not be surprised if genotypingeventually replaces ’immunotyping’ as the standardprocedure in the blood group laboratory. This predictionis being questioned by some in the profession pointing tothe many major problems that are – at the moment –undeniably associated with blood group genotyping.Many technical increments are required to achieve vastimprovements in the reliability and cost-efficiency ofgenotyping, which are relatively low compared to stan-dard serological methods. Once the many problems areaddressed, they can be solved in a piecemeal approach,which will step by step reduce genotyping to routinepractice for most applications currently tackled by ser-ology. It is hoped that establishing the necessary popula-tion data will keep pace with the rapidly improvingtechnologies in genotyping. Our profession could con-tribute considerably to the improvement of genotypingstrategies that are vigorously developed in various med-ical fields.
ABO and RhD typing are among the most reliablediagnostic procedures. Being rather inexpensive is onereason that blood group serology is very cost-efficient, ifapplied prudently. In this situation, the demands requiredfor blood group genotyping are exceptional compared togenotyping for other purposes. By striving to meet thesedemands for blood group genotyping, transfusion
medicine may well contribute to the understanding ofand the solutions for the biological problems associatedwith genotyping strategies in general.
AUTHORS’ NOTE
We apologize for being unable to cite all of the papersthat are relevant to this topic and thank many of theparticipants of the 3rd Annual Molecular TransfusionMedicine Seminars organized by Friedrich Schunter andheld at the DRK-Blutspendezentrale Oldenburg on 3September 1997 for interesting discussions that contrib-uted to the ideas presented here. We are indebted to PetraA. Maaskant-van Wijk, Amsterdam, the Netherlands, forpreparing and providing the gel image of Fig. 3. We aregrateful to Catherine A. Hyland, Brisbane, Australia,Petra A. Maaskant-van Wijk and Brigitte H. W. Faas,Amsterdam, the Netherlands, for communicating dataprior to their publication. We thank Zhu Zi-yan, Shang-hai, China, for contributing a sample of D category VItype III with a strong anti-D alloantibody.
REFERENCES
Adinolfi, M., Sherlock, J., Kemp, T., Carritt, B., Southill, P.,Kingdom, J. & Rodeck, C. (1995) Prenatal detection of fetalRhD DNA sequences in transcervical samples.Lancet, 345,318–319.
Andrews, K.T., Wolter, L.C., Saul, A. & Hyland, C.A. (1998a)Analysis of the RH D gene in an RH D negative donor(Abstract).Vox Sanguinis, 74 (Suppl. 1), 53.
Andrews, K.T., Wolter, L.C., Saul, A. & Hyland, C.A. (1998b)The RhD-trait in a white blood donor with the RhCCeephenotype attributed to a four-nucleotide deletion in theRHD gene (Letter).Blood, in press.
Anstee, D.J. (1995) Blood group antigens definded by theamino acid sequences of red cell surface proteins.Transfu-sion Medicine, 5, 1–13.
Arce, M.A., Thompson, E.S., Wagner, S., Coyne, K.E., Ferd-man, B.A. & Lublin, D.M. (1993) Molecular cloning of RhDcDNA derived from a gene present in RhD-positive, but notRhD-negative individuals.Blood, 82, 651–655.
Argall, C.I., Ball, J.M. & Trentelman, E. (1953) Presence ofanti-D antibody in the serum of a Du patient. Journal ofLaboratory and Clinical Medicine, 41, 895–898.
Aubin, J.T., Le Van Kim, C., Mouro, I., Colin, Y., Bignozzi, C.,Brossard, Y. & Cartron, J.-P. (1997) Specificity and sensi-tivity of RHD genotyping methods by PCR-based DNAamplification.British Journal of Haematology, 98,356–364.
Avent, N.D. (1997) Human erythrocyte antigen expression: itsmolecular bases.British Journal of Biomedical Sciences, 54,16–37.
Avent, N.D., Jones, J.W., Liu, W., Scott, M.L., Voak, D.,Flegel, W.A., Wagner, F.F. & Green, C. (1997a) Molecularbasis of the D variant phenotypes DNU and DII allowslocalization of critical amino acids required for expression
Rh phenotype prediction by DNA typing297
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

of Rh D epitopes epD3, 4 and 9 to the sixth external domainof the Rh D protein.British Journal of Haematology, 97,366–371.
Avent, N.D., Liu, W., Jones, J.W., Scott, M.L., Voak, D.,Pisacka, M., Watt, J. & Fletcher, A. (1997b) Molecularanalysis of Rh transcripts and polypeptides from individualsexpressing the DVI variant phenotype: anRHDgene deletionevent does not generate all DVIccEe phenotypes.Blood, 89,1779–1786.
Avent, N.D., Martin, P.G., Armstrong-Fisher, S.S., Liu, W.,Finning, K.M., Maddocks, D. & Urbaniak, S.J. (1997c) Evi-dence of genetic diversity underlying Rh D negative, weak D(Du) and partial D phenotypes as determined by multiplex PCRanalysis of theRHD gene.Blood, 89, 2568–2577.
Beaudet, A.L., Antonarakis, S.E., Beutler, E., Cotton, R.G.H.,Desnick, R.J., Kazazian, H.H., McAlpine, P.J., McKusick,V.A., Motulsky, A.G., Scriver, C.R., Shows, T.B., Tsui, L.-C. & Valle, D. (1996) Update on nomenclature for humangene mutations.Human Mutation, 8, 197–202.
Beckers, E.A.M., Faas, B.H.W., Ligthart, P., Simsek, S., vonOverbeeke, M.A.M., dem Borne, A.E.G.K., van Rhenen, D.J.& van der Schoot, C.E. (1996a) Characterization of thehybrid RHD gene leading to the partial D category IIIcphenotype.Transfusion, 36, 567–574.
Beckers, E.A., Faas, B.H., Ligthart, P., von Overbeeke, M.A.,dem Borne, A.E., van der Schoot, C.E. & van Rhenen, D.J.(1997) Lower antigen site density and weak D immunogeni-city cannot be explained by structural genomic abnormalitiesor regulatory defects of the RHD gene.Transfusion, 37,616–623.
Beckers, E.A.M., Faas, B.H.W., Simsek, S., Overbeeke,M.A.M., van Rhenen, D.J., Wallace, M., von dem Borne,A.E.G.K. & van der Schoot, C.E. (1996b) The genetic basisof a new partial D antigen: DDBT. British Journal of Hae-matology, 93, 720–727.
Beckers, E.A.M., Porcelijn, L., Ligthart, P., Vermey, H., vondem Borne, A.E.G.K., Overbeeke, M.A.M. & van Rhenen,D.J. (1996d) The R0
Har antigenic complex is associated witha limited number of D epitopes and alloanti-D production: astudy in three unrelated individuals and their families.Transfusion, 36, 104–108.
Beckers, E.A.M., Faas, B.H.W., von dem Borne, A.E.G.K.,Overbeeke, M.A.M., van Rhenen, D.J. & van der Schoot,C.E. (1996c) The R0
Har Rh: 33 phenotype results fromsubstitution of exon 5 of theRHCEgene by the correspond-ing exon of the RHD gene.British Journal of Haematology,92, 751–757.
Bennett, P.R. & Cartron, J.-P. (1994) Prenatal determination offetal RhD type (Reply).New England Journal of Medicine,330,795–796.
Bennett, P.R., Le Van Kim, C., Colin, Y., Warwick, R.M.,Cherif-Zahar, B., Fisk, N.M. & Cartron, J.-P. (1993) Prenataldetermination of fetal RhD type by DNA amplification.NewEngland Journal of Medicine, 329,607–610.
Beutler, E., McKusick, V.A., Motulsky, A.G., Scriver, C.R. &Hutchinson, F. (1996) Mutation nomenclature: nicknames,
systematic names, and unique identifiers.Human Mutation,8, 203–206.
Bianchi, D.W., Zickwolf, G.K., Weil, G.J., Sylvester, S. &DeMaria, M.A. (1996) Male fetal progenitor cells persist inmaternal blood for as long as 27 years postpartum.Proceed-ings of the National Academy of Sciences USA, 93,705–708.
Blunt, T., Daniels, G. & Carritt, B. (1994) Serotype switchingin a partially deletedRHD gene.Vox Sanguinis, 67, 397–401.
Busch, J., Huber, P., Holtz, J., Pfluger, E. & Radbruch, A.(1994) Simple and fast ’double-MACS’ sorting of fetalerythroblasts from maternal blood for PCR-based paternityanalysis.Annals of the New York Academy of Science, 731,144–146.
Carritt, B., Kemp, T.J. & Poulter, M. (1997) Evolution of thehuman RH (rhesus) blood group genes: a 50 year oldprediction (partially) fulfilled.Human Molecular Genetics,6, 843–850.
Carritt, B., Steers, F.J. & Avent, N.D. (1994) Prenatal determi-nation of fetal RhD type.Lancet, 344,205–206.
Cartron, J.P. (1994) Defining the Rh blood group antigens.Biochemistry and molecular genetics.Blood Reviews, 8,199–212.
Chee, M., Yang, R., Hubbell, E., Berno, A., Huang, X.C., Stern,D., Winkler, J., Lockhart, D.J., Morris, M.S. & Fodor, S.P.A.(1996) Accessing genetic information with high-densityDNA arrays.Science, 274,610–614.
Cherif-Zahar, B., Bloy, C., Le Van Kim, C., Blanchard, D.,Bailly, P., Hermand, P., Salmon, C., Cartron, J.-P. & Colin,Y. (1990) Molecular cloning and protein structure of ahuman blood group Rh polypeptide.Proceedings of theNational Academy of Sciences USA, 87, 6243–6247.
Cherif-Zahar, B., Le Van Kim, C., Rouillac, C., Raynal, V.,Cartron, J.-P. & Colin, Y. (1994) Organization of the gene(RHCE) encoding the human blood group RhCcEe antigensand characterization of the promoter region.Genomics, 19,68–74.
Cherif-Zahar, B., Mattei, M.G., Le Van Kim, C., Bailly, P.,Cartron, J.-P. & Colin, Y. (1991) Localization of the humanRh blood group gene structure to chromosome region1p34.3–1p36.1 by in situ hybridization.Human Genetics,86, 398–400.
Cherif-Zahar, B., Raynal, V., Gane, P., Mattei, M.G., Bailly, P.,Gibbs, B., Colin, Y. & Cartron, J.-P. (1996) Candidate geneacting as a suppressor of theRH locus in most cases of Rh-deficiency.Nature Genetics, 12, 168–173.
Colin, Y., Cherif-Zahar, B., Le Van Kim, C., Raynal, V., vanHuffel, V. & Cartron, J.-P. (1991) Genetic basis of the RhD-positive and RhD-negative blood group polymorphism asdetermined by southern analysis.Blood, 78, 2747–2752.
Cooper, D.N. & Krawczak, M. (1993)Human Gene Mutation.Bios Scientific Publishers, Oxford.
Cossu, G., Angius, A., Gelfi, C. & Righetti, P.G. (1996) Rh D/dgenotyping by quantitative polymerase chain reaction andcapillary zone electrophoresis.Electrophoresis, 17, 1911–1915.
298 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

Daniels, G., Green, C. & Smart, E. (1997) Differences betweenRhD-negative Africans and RhD-negative Europeans(Letter).Lancet, 350,862–863.
Dildy, G.A., Jackson, G.M. & Ward, K. (1996) Determinationof fetal RhD status from uncultured amniocytes.Obstetricsand Gynecology, 88, 207–210.
Eshleman, J.R., Shakin-Eshleman, S.H., Church, A., Kant, J.A.& Spitalnik, S.L. (1995) DNA typing of the human MN andSs blood group antigens in amniotic fluid and followingmassive transfusion.American Journal of Clinical Pathol-ogy, 103,353–357.
Faas, B.H.W. (1998)Rhesus blood group antigens: from post-natal phenotyping to prenatal genotyping. PhD Thesis, Uni-versiteit van Amsterdam, pp. 175–189.
Faas, B.H.W., Becker, E.A.M., Wildoer, P., Ligthart, P.C., Over-beeke,M.A.M.,Zondervan,H.A.,vondemBorne,A.E.G.K.&van der Schoot, C.E. (1997a) Molecular background of VSand weak C expression in blacks.Transfusion, 37, 38–44.
Faas, B.H.W., Beckers, E.A.M., Simsek, S., Overbeeke,M.A.M., Pepper, R., van Rhenen, D.J., von dem Borne,A.E.G.K. & van der Schoot, C.E. (1996) Involvement ofSer103 of the Rh polypeptides in G epitope formation.Transfusion, 36, 506–511.
Faas, B.H.W., Christiaens, G.C.M.L., Maaskant-van Wijk,P.A., Ligthart, P.C., Overbeeke, M.A.M., van Rhenen, D.J.,von dem Borne, A.E.G.K. & van der Schoot, C.E. (1997b)Prenatal genotyping of Rh and Kell antigens on amnioticfluid DNA (Abstract).Transfusion, 37, 100S.
Faas, B.H.W., Ligthart, P.C., Lomas-Francis, C., Overbeeke,M.A., von dem Borne, A.E. & van der Schoot, C.E. (1997c)Involvement of Gly96 in the formation of the Rh26 epitope.Transfusion, 37, 1123–1130.
Faas, B.H.W., Simsek, S., Bleeker, P.M.M., Overbeeke,M.A.M., Cuijpers, H.T.M., von dem Borne, A.E.G.K. &van der Schoot, C.E. (1995) Rh E/e genotyping by allele-specific primer amplification.Blood, 85, 829–832.
Ferguson-Smith, M.A., Zheng, Y.L. & Carter, N.P. (1994)Simultaneous immunophenotyping and FISH on fetal cellsfrom maternal blood.Annals of the New York Academy ofScience, 731,73–79.
Fischer, G.F., Fae, I., Petrasek, M. & Moser, S. (1995) Acombination of two distinct in vitro amplification proceduresfor DNA typing of HLA-DRB and -DQB 1 alleles.VoxSanguinis, 69, 328–335.
Fischer, S.G. & Lerman, L.S. (1983) DNA fragments differingby single base-pair substitutions separated in denaturing gra-dient gels: correspondence with melting theory.Proceedingsof the National Academy of Sciences USA, 80, 1579–1583.
Flegel, W.A. (1997)Haufigkeit sporadischer nicht-funktionalerAllele und ihre Bedeutung fu¨r die Genotypisierung amBeispiel des Polymorphismus im FUT1-Blutgruppengen.Habilitationsschrift, Universita¨t Ulm. <www.uni-ulm.de/,wflegel/HABIL>.
Flegel, W.A., Gassner, C., Mu¨ller, T.H., Schonitzer, D., Schun-ter, F. & Wagner, F.F. (1998) The molecular basis of weak D(Abstract).Vox Sanguinis, 74 (Suppl. 1), 55.
Flegel, W.A., Hillesheim, B. & Wagner, F.F. (1996) RHDcategory VII is caused by a single molecular event(Abstract).Transfusion Clinique et Biologique, 3, 33s.
Flegel, W.A. & Wagner, F.F. (1996) The frequency of RHDprotein variants in Caucasians (Abstract).Transfusion Clin-ique et Biologique, 3, 10s.
Flegel, W.A. & Wagner, F.F. (1998)Rhesus Immunisierungs-register (RIR) [The Rhesus Immunization Surveillance].DRK-Blutspendedienst Baden-Wu¨rttemberg, Ulm.<www.uni-ulm.de/,wflegel/RH/RIR>.
Fukumori, Y., Hori, Y., Ohnoki, S., Nagao, N., Shibata, H.,Okubo, Y. & Yamaguchi, H. (1997) Further analysis of Del(D-elute) using polymerase chain reaction (PCR) with RHDgene-specific primers.Transfusion Medicine, 7, 227–231.
Ganshirt-Ahlert, D., Borjesson-Stoll, R., Burschyk, M., Dohr,A., Garritsen, H.S., Helmer, E., Miny, P., Velasco, M.,Walde, C., Patterson, D., Teng, N., Bhat, N.M., Bieber,M.M. & Holzgreve, W. (1993) Detection of fetal trisomies21 and 18 from maternal blood using triple gradient andmagnetic cell sorting.American Journal of ReproductiveImmunology, 30, 194–201.
Gassner, C., Mu¨ller, T.H., Wagner, F.F., Flegel, W.A. &Schonitzer, D. (1997a) Rhesus C typing by polymerasechain reaction using sequence specific primers: realisationof ’medium resolutionRH-DNA-typing’ (Abstract).Transfu-sion, 37S, 101S.
Gassner, C., Schmarda, A., Kilga-Nogler, S., Jenny-Feld-kircher, B., Rainer, E., Mu¨ller, T.H., Wagner, F.F., Flegel,W.A. & Schonitzer, D. (1997b) RhesusD/CE typing bypolymerase chain reaction using sequence-specific primers.Transfusion, 37, 1020–1026.
Gassner, C., Schmarda, A., Nussbaumer, W. & Scho¨nitzer, D.(1996) ABO glycosyltransferase genotyping by polymerase-chain reaction using sequence-specific primers.Blood, 88,1852–1856.
Geifman-Holtzman, O., Bernstein, I.M., Berry, S.M., Bianchi,D.W. & Holtzman, E.J. (1996a) Rapid molecular determina-tion of fetal rhesus E type.Prenatal Diagnosis, 16,489–493.
Geifman-Holtzman, O., Bernstein, I.M., Berry, S.M., Holtz-man, E.J., Vadnais, T.J., DeMaria, M.A. & Bianchi, D.W.(1996b) Fetal RhD genotyping in fetal cells flow sorted frommaternal blood.American Journal of Obstetrics and Gyne-cology, 174,818–822.
Hamlington, J., Cunningham, J., Mason, G., Mueller, R. &Miller, D. (1997) Prenatal detection of rhesus D genotype(Letter).Lancet, 349,540.
Heid, C.A., Stevens, J., Livak, K.J. & Williams, P.M. (1996)Real time quantitative PCR.Genome Research, 6, 986–994.
Hengstschlager, M., Holzl, G., Ulm, B. & Bernaschek, G.(1997) Raising the sensitivity of fetal RhD typing and sexdetermination from maternal blood (Letter).Journal ofMedical Genetics, 34, 350–351.
Hessner, M.J., McFarland, J.G. & Endean, D.J. (1996)Genotyping of KEL1 and KEL2 of the human Kell bloodgroup system by the polymerase chain reaction withsequence-specific primers.Transfusion, 36, 495–499.
Rh phenotype prediction by DNA typing299
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

Huang, C.H. (1996) Alteration ofRH gene structure andexpression in human dCCee and DCw- red blood cells:phenotypic homozygosity versus genotypic heterozygosity.Blood, 88, 2326–2333.
Huang, C.H. (1997a) Human DVI category erythrocytes: corre-lation of the phenotype with a novel hybrid RhD-CE-D genebut not an internally deleted RhD gene.Blood, 89, 1834–1839.
Huang, C.H. (1997b) Molecular insights into the Rh proteinfamily and associated antigens.Current Opinion in Hema-tology, 4, 94–103.
Huang, C.H., Chen, Y. & Reid, M. (1997) Human DIIIa
erythrocytes: RhD protein is associated with multiple dis-persed amino acid variations.American Journal of Hematol-ogy, 55, 139–145.
Hyland, C.A., Cherif-Zahar, B., Cowley, N., Raynal, V.,Parkes, J., Saul, A. & Cartron, J.P. (1998) A novel singlemissense mutation identified along the RH50 gene in acomposite heterozygous Rhnull blood donor of the regulatortype.Blood, 91, 1458–1463.
Hyland, C.A., Wolter, L.C. & Saul, A. (1994) Three unrelatedRh D gene polymorphisms identified among blood donorswith Rhesus CCee (r0r0) phenotypes.Blood, 84, 321–324.
Hyland, C.A., Wolter, L.C. & Saul, A. (1995) Identification andanalysis of RH genes: application of PCR and RFLP typingtests.Transfusion Medicine Reviews, 9, 289–301.
Ikemoto, S., Iwamoto, S., Tsuchida, S., Goto, K., Oyamada, T.& Kajii, E. (1996) Molecular genetic basis of red cellmarkers and its forensic application.Forensic Science Inter-national, 80, 147–161.
Issitt, P.D. & Telen, M.J. (1996) D, weak D (Du), and partial D:the molecular story unfolds.Transfusion, 36, 97–100.
Jones, J. (1995) Identification of two new D variants, DHMi andDHMii using monoclonal anti-D.Vox Sanguinis, 69, 236–241.
Jones, J.W., Finning, K.M., Mattock, R., Voak, D., Scott, M.L.& Avent, N.D. (1997) The serological profile and molecularbasis of a new partial D phenotype, DHR.Vox Sanguinis, 73,252–256.
Jones, J., Scott, M.L. & Voak, D. (1995) Monoclonal anti-Dspecificity and Rh D structure: criteria for selection ofmonoclonal anti-D reagents for routine typing of patientsand donors.Transfusion Medicine, 5, 171–184.
Joyce, P. & Tavare, S. (1995) The distribution of rare alleles.Journal of Mathematical Biology, 33, 602–618.
Kalinina, O., Lebedeva, I., Brown, J. & Silver, J. (1997)Nanoliter scale PCR with TaqMan detection.Nucleic AcidsResearch, 25, 1999–2004.
Kemp, T.J., Poulter, M. & Carritt, B. (1996) A recombinationhot spot in the Rh genes revealed by analysis of unrelateddonors with the rare d – phenotype.American Journal ofHuman Genetics, 59, 1066–1073.
Langley, C.H., Voelker, R.A., Leigh Brown, A.J., Ohnishi, S.,Dickson, B. & Montgomery, E. (1981) Null allele frequen-cies at allozyme loci in natural populations of Drosophilamelanogaster.Genetics, 99, 151–156.
Le Van Kim, C., Mouro, I., Brossard, Y., Chavinie, J., Cartron,J.-P. & Colin, Y. (1994) PCR-based determination of Rhcand RhE status of fetuses at risk for Rhc and RhE haemolyticdisease.British Journal of Haematology, 88, 193–195.
Le Van Kim, C., Mouro, I., Cherif-Zahar, B., Raynal, V.,Cherrier, C., Cartron, J.-P. & Colin, Y. (1992) Molecularcloning and primary structure of the human blood group RhDpolypeptide. Proceedings of the National Academy ofSciences USA, 89, 10925–10929.
Lee, S., Bennett, P.R., Overton, T., Warwick, R., Wu, X. &Redman, C.M. (1996) Prenatal diagnosis of Kell blood groupgenotypes: KEL1 and KEL2.American Journal of Obstetricsand Gynecology, 175,455–459.
Legler, T.J., Kohler, M., Mayr, W.R., Panzer, S., Ohto, H. &Fischer, G.F. (1996) Genotyping of the human plateletantigen systems 1 through 5 by multiplex polymerase chainreaction and ligation-based typing.Transfusion, 36, 426–431.
Lighten, A.D., Overton, T.G., Sepulveda, W., Warwick, R.M.,Fisk, N.M. & Bennett, P.R. (1995) Accuracy of prenataldetermination of RhD type status by polymerase chainreaction with amniotic cells.American Journal of Obstetricsand Gynecology, 173,1182–1185.
Lin, Z., Cui, X. & Li, H. (1996) Multiplex genotype determina-tion at a large number of gene loci.Proceedings of theNational Academy of Sciences USA, 93, 2582–2587.
Liu, W., Jones, J.W., Scott, M.L., Voak, D. & Avent, N.D.(1996) Molecular analysis of twoD-variants, DHMi and DHMii
(Abstract).Transfusion Medicine, 6 (Suppl. 2), 21.Lo, Y.M., Bowell, P.J., Selinger, M., Mackenzie, I.Z., Cham-
berlain, P., Gillmer, M.D., Elliott, P., Pratt, G., Littlewood,T.J. & Fleming, K.A. (1994a) Prenatal determination of fetalRhesus D status by DNA amplification of peripheral blood ofRhesus-negative mothers.Annals of the New York Academyof Science, 731,229–236.
Lo, Y.-M.D., Bowell, P.J., Selinger, M., Mackenzie, I.Z.,Chamberlain, P., Gillmer, M.D.G., Littlewood, T.J., Flem-ing, K.A. & Wainscoat, J.S. (1993) Prenatal determination offetal RhD status by analysis of peripheral blood of rhesusnegative mothers.Lancet, 341,1147–1148.
Lo, Y.M., Noakes, L., Bowell, P.J., Fleming, K.A. & Wains-coat, J.S. (1994b) Detection of fetal RhD sequence fromperipheral blood of sensitized RhD-negative pregnantwomen.British Journal of Haematology, 87, 658–660.
Lomas, C., Gra¨ssmann, W., Ford, D., Watt, J., Gooch, A., Jones,J., Beolet, M., Stern, D., Wallace, M. & Tippett, P. (1994)FPTT is a low-incidence Rh antigen associated with a ’new’partial Rh D phenotype, DFR.Transfusion, 34, 612–616.
Lomas, C., Tippett, P., Thompson, K.M., Melamed, M.D. &Hughes-Jones, N.C. (1989) Demonstration of seven epitopeson the Rh antigen D using human monoclonal anti-D anti-bodies and red cells from D categories.Vox Sanguinis, 57,261–264.
Maas, J.H., Legler, T.J., Lynen, R., Blaschke, V., Ohto, H. &Kohler, M. (1997) [Rh-D genotyping for exon 2, 5 and 7 ofGerman and Japanese blood donors with sequence specific
300 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

polymerase chain reaction].Beitrage zur Infusionstherapieund Transfusionsmedizin, 34, 203–209.
Maaskant van Wijk, P.A., Beckers, E.A.M., van Rhenen, D.J.,Mouro, I., Colin, Y., Cartron, J.-P., Faas, B.H.W., van derSchoot, C.E., Apoil, P.A., von Blancher, A. & von demBorne, A.E.G. (1997a) Evidence that the RHD (VI) deletiongenotype does not exist.Blood, 90, 1709–1711.
Maaskant van Wijk, P.A., Faas, B.H.W., de Ruijter, J.A.M., vonOverbeeke, M.A.M., von dem Borne, A.E.G.K. & van Rhenen,D.J. (1997b)RHDgenotyping by multiplex PCR analysis of allRHD specific exons (Abstract).Transfusion, 37, 1S.
Maaskant van Wijk, P.A., Faas, B.H.W., de Ruijter, J.A.M., vonOverbeeke, M.A.M., dem Borne, A.E.G.K., van Rhenen, D.J.& van der Schoot, C.E. (1998) Genotyping of RHD bymultiplex polymerase chain reaction analysis of allRHD-specific exons.Transfusion, 38, in press.
MacGeoch, C., Mitchell, C.J., Carritt, B., Avent, N.D., Ridg-well, K., Tanner, M.J. & Spurr, N.K. (1992) Assignment ofthe chromosomal locus of the human 30-kDal Rh (rhesus)blood group-antigen-related protein (Rh30A) to chromosomeregion 1p36.13–-p34.Cytogenetics and Cellular Genetics,59, 261–263.
Mallinson, G., Soo, K.S. & Anstee, D.J. (1995) The molecularbasis of the Fy (a) and Fy (b) antigens (Abstract).TransfusionMedicine, 5, 45.
Morris, T., Robertson, B. & Gallagher, M. (1996) Rapid reversetranscription-PCR detection of hepatitis C virus RNA inserum by using the TaqMan fluorogenic detection system.Journal of Clinical Microbiology, 34, 2933–2936.
Mouro, I., Le Van Kim, C., Rouillac, C., van Rhenen, D.J., LePennec, P.Y., Bailly, P., Cartron, J.-P. & Colin, Y. (1994)Rearrangements of the blood group RhD gene associatedwith the DVI category phenotype.Blood, 83, 1129–1135.
Muller, T.H., Doscher, A. & Schunter, F. (1997a) Genotypingof the human platelet antigen-1 by ELISA detection of allele-specific amplicons.Vox Sanguinis, 73, 185–188.
Muller, T.H., Gassner, C., Gran, S., Wagner, F.F., Flegel, W.A.& Schunter, F. (1997b) Semiautomated Rhesus DNA-typingby multiplex PCR: 4 reactions with 15 sequence-specificprimer pairs (Abstract).Transfusion, 37, 19S.
Ohnishi, S., Brown, A.J.L., Voelker, R.A. & Langley, C.H.(1982) Estimation of genetic variability in natural popula-tions of Drosophila simulans by two-demensional and starchgel electrophoresis.Genetics, 100,127–136.
Okuda, H., Kawano, M., Iwamoto, S., Tanaka, M., Seno, T.,Okubo, Y. & Kajii, E. (1997) TheRHD gene is highlydetectable in RhD-negative Japanese donors.Journal ofClinical Investigation, 100,373–379.
Olives, B., Merriman, M., Bailly, P., Bain, S., Barnett, A.,Todd, J., Cartron, J.P. & Merriman, T. (1997) The molecularbasis of the Kidd blood group polymorphism and its lack ofassociation with type 1 diabetes susceptibility.Human Mole-cular Genetics, 6, 1017–1020.
Pope, J., Navarrete, C., Warwick, R. & Contreras, M. (1995)Multiplex PCR analysis of RhD gene.Lancet, 346,375–376.
Poulter, M., Kemp, T.J. & Carritt, B. (1996) DNA-based
Rhesus typing: simultaneous determination of RHC andRHD status using the polymerase chain reaction.Vox San-guinis, 7, 164–168.
Reubinoff, B.E., Avner, R., Rojansky, N., Manny, N., Fried-mann, A., Laufer, N. & Mitrani-Rosenbaum, S. (1996) RhDgenotype determination by single sperm cell analysis.Amer-ican Journal of Obstetrics and Gynecology, 174,1300–1305.
Rose, N.C., Hurwitz, C., Silberstein, L., Andovalu, R. &Stoerker, J. (1997) Prenatal analysis of rhesus CcDEeblood groups by heteroduplex generator.American Journalof Obstetrics and Gynecology, 176,1084–1089.
Rossiter, J.P., Blakemore, K.J., Kickler, T.S., Kasch, L.M.,Khouzami, A.N., Pressman, E.K., Sciscione, A.C. & Kaza-zian, H.H. (1994) The use of polymerase chain reaction todetermine fetal RhD status.American Journal of Obstetricsand Gynecology, 171,1047–1051.
Roubinet, F., Apoil, P.A. & Blancher, A. (1996) Frequency ofpartial D phenotypes in the south western region of France.Transfusion Clinique et Biologique, 3, 247–255.
Rouger, P. & Muller, J.-Y. (1996) Third International Work-shop and Symposium on Monoclonal Antibodies againstHuman Red Cells and Related Antigens: Section RH.Trans-fusion Clinique et Biologique, 3, 329–541.
Rouillac, C., Colin, Y., Hughes-Jones, N.C., Beolet, M.,D’Ambrosio, A.-M., Cartron, J.-P. & Le Van Kim, C.(1995a) Transcript analysis of D category phenotypes pre-dicts hybrid Rh D-CE-D proteins associated with alterationof D epitopes.Blood, 85, 2937–2944.
Rouillac, C., Gane, P., Cartron, J.-P., Le Pennec, P.Y. & Colin,Y. (1996) Molecular basis of the altered antigenic expressionof RhD in weak D (Du) and RhC/e in RN phenotypes.Blood,87, 4853–4861.
Rouillac, C., Le Van Kim, C., Beolet, M., Cartron, J.-P. &Colin, Y. (1995b) Leu110Pro substitution in the RhD poly-peptide is responsible for the DVII category blood groupphenotype.American Journal of Hematology, 49, 87–88.
Rouillac, C., Le Van Kim, C., Blancher, A., Roubinet, F.,Cartron, J.-P. & Colin, Y. (1995c) Lack of G blood groupantigen in DIIIb erythrocytes is associated with segmentalDNA exchange betweenRH genes.British Journal of Hae-matology, 89, 424–426.
Salmon, C., Cartron, J.-P. & Rouger, P. (1984)The HumanBlood Groups. Masson, New York.
Scott, M.L., Voak, D., Jones, J.W., Liu, W., Avent, N.D.,Hughes-Jones, N. & Sonneborn, H.-H. (1997) A model forRhD – the relationship of 30 serologically defined epitopesto predicted structure.Biotest Bulletin, 5, 459–466.
Sekizawa, A., Watanabe, A., Kimura, T., Saito, H., Yanaihara,T. & Sato, T. (1996) Prenatal diagnosis of the fetal RhDblood type using a single fetal nucleated erythrocyte frommaternal blood.Obstetrics and Gynecology, 87, 501–505.
Simsek, S., Faas, B.H.W., Bleeker, P.M.M., Overbeeke,M.A.M., Cuijpers, H.T.M., van der Schoot, C.E. & vondem Borne, A.E.G.K. (1995) Rapid Rh D genotyping bypolymerase chain reaction-based amplification of DNA.Blood, 85, 2975–2980.
Rh phenotype prediction by DNA typing301
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302

Simsek, S., Bleeker, P.M.M. & von dem Borne, A.E.G. (1994)Prenatal determination of fetal RhD type (Letter).NewEngland Journal of Medicine, 330,795–796.
Sonneborn, H.-H. & Voak, D. (1997) A review of 50 years ofthe Rh blood group system.Biotest Bulletin, 5, 389–552.
Spence, W.C., Maddalena, A., Demers, D.B. & Bick, D.P.(1995a) Molecular analysis of the RhD genotype in fetuses atrisk for RhD hemolytic disease.Obstetrics and Gynecology,85, 296–298.
Spence, W.C., Maddalena, A., Demers, D.B. & Bick, D.P.(1997) Prenatal determination of genotypes Kell and Cellanoin at-risk pregnancies.Journal of Reproductive Medicine, 42,353–357.
Spence, W.C., Potter, P., Maddalena, A., Demers, D.B. & Bick,D.P. (1995b) DNA-based prenatal determination of the RhEegenotype.Obstetrics and Gynecology, 86, 670–672.
Steers, F., Wallace, M., Johnson, P., Carritt, B. & Daniels, G.(1996) Denaturing gradient gel electrophoresis: a novelmethod for determining Rh phenotype from genomic DNA.British Journal of Haematology, 94, 417–421.
Stoerker, J., Hurwitz, C., Rose, N.C., Silberstein, L.E. &Highsmith, W.E. (1996) Heteroduplex generator in analysisof Rh blood group alleles.Clinical Chemistry, 42,356–360.
Tanaka, M., Seno, T., Shibata, H., Okubo, Y., Okuda, H., Kajii,E. & Utsumi, R. (1997) Genotyping for RhC/c and RhE/e byPCR using allele-specific oligonucleotide primers.JapaneseJournal of Legal Medicine, 51, 32–38.
Tippett, P., Lomas-Francis, C. & Wallace, M. (1996) The Rhantigen D: partial D antigens and associated low incidenceantigens.Vox Sanguinis, 70, 123–131.
Tippett, P. & Sanger, R. (1962) Observations on subdivisions ofRh antigen D.Vox Sanguinis, 7, 9–13.
Tippett, P. & Sanger, R. (1977) Further observations on sub-divisions of the Rh antigen D.Das Arztliche Laboratorium,23, 476–480.
Tonn, T., Westrup, D., Seidl, C., Kirchmaier, C.M. & Seifried,E. (1997) Sensitive determination of the RhD genotype inmixed samples using fluorescence-based polymerase chainreaction.Vox Sanguinis, 72, 177–181.
van den Veyver, I.B., Chong, S.S., Cota, J., Bennett, P.R., Fisk,N.M., Handyside, A.H., Cartron, J.P., Le Van Kim, C., Colin,Y. & Snabes, M.C. (1995) Single-cell analysis of the RhDblood type for use in preimplantation diagnosis in theprevention of severe hemolytic disease of the newborn.American Journal of Obstetrics and Gynecology, 172,533–540.
van den Veyver, I.B. & Moise, K.J. (1996) Fetal RhD typing bypolymerase chain reaction in pregnancies complicated by
rhesus alloimmunization.Obstetrics and Gynecology, 88,1061–1067.
van den Veyver, I.B., Subramanian, S.B., Hudson, K.M.,Werch, J., Moise, K.J. & Hughes, M.R. (1996) Prenataldiagnosis of the RhD fetal blood type on amniotic fluid bypolymerase chain reaction.Obstetrics and Gynecology, 87,419–422.
Wagner, F.F. & Flegel, W.A. (1997) Polymorphism of the hallele and the population frequency of sporadic nonfunc-tional alleles.Transfusion, 37, 284–290.
Wagner, F.F., Gassner, C., Mu¨ller, T.H., Scho¨nitzer, D.,Schunter, F. & Flegel, W.A. (1998a) Three molecular struc-tures cause Rhesus D category VI phenotypes with distinctimmunohematologic features.Blood, 91, 2157–2168.
Wagner, F.F., Gassner, C., Mu¨ller, T.H., Scho¨nitzer, D.,Schunter, F. & Flegel, W.A. (1998b) The molecular basisof weak D phenotypes.Blood, in press..
Wagner, F.F., Kasulke, D., Kerowgan, M. & Flegel, W.A.(1995) Frequencies of the blood groups ABO, Rhesus, Dcategory VI, Kell, and of clinically relevant high-frequencyantigens in South-Western Germany.Infusionstherapie undTransfusionsmedizin, 22, 285–290.
Wallace, M., Lomas-Francis, C., Beckers, E., Bruce, M.,Campbell, G., Chatfield, S., Nagao, N., Okubo, Y., Opalka,A., Overbeeke, M., Scott, M. & Voak, D. (1997) DBT: apartial D phenotype associated with the low-incidence anti-gen Rh32.Transfusion Medicine, 7, 233–238.
Wenk, R.E. & Chiafari, P.A. (1997) DNA typing of recipientblood after massive transfusion.Transfusion, 37, 1108–1110.
Wodicka, L., Dong, H., Mittmann, M., Ho, M.H. & Lockhart,D.J. (1997) Genome-wide expression monitoring in Sacchar-omyces cerevisiae.Nature Biotechnology, 15, 1359–1367.
Wolter, L.C., Hyland, C.A. & Saul, A. (1993) Rhesus Dgenotyping using polymerase chain reaction.Blood, 82,1682–1683.
Woo, T.H., Patel, B.K., Smythe, L.D., Norris, M.A., Symonds,M.L. & Dohnt, M.F. (1998) Identification of pathogenicLeptospira by TaqMan probe in a lightcycler.AnalyticalBiochemistry, 256,132–134.
Yankowitz, J., Li, S. & Murray, J.C. (1995) Polymerase chainreaction determination of RhD blood type: an evaluation ofaccuracy.Obstetrics and Gynecology, 86, 214–217.
Yankowitz, J., Li, S. & Weiner, C.P. (1997) Polymerase chainreaction determination of RhC, Rhc, and RhE blood types: anevaluation of accuracy and clinical utility.American Journalof Obstetrics and Gynecology, 176,1107–1111.
302 W. A. Flegelet al.
q 1998 Blackwell Science Ltd,Transfusion Medicine, 8, 281–302