REVIEW Open Access Social wanting dysfunction in autism ...reinforcement-based learning principles,...
20
REVIEW Open Access Social ‘wanting’ dysfunction in autism: neurobiological underpinnings and treatment implications Gregor Kohls * , Coralie Chevallier, Vanessa Troiani and Robert T Schultz Abstract Most behavioral training regimens in autism spectrum disorders (ASD) rely on reward-based reinforcement strategies. Although proven to significantly increase both cognitive and social outcomes and successfully reduce aberrant behaviors, this approach fails to benefit a substantial number of affected individuals. Given the enormous amount of clinical and financial resources devoted to behavioral interventions, there is a surprisingly large gap in our knowledge of the basic reward mechanisms of learning in ASD. Understanding the mechanisms for reward responsiveness and reinforcement-based learning is urgently needed to better inform modifications that might improve current treatments. The fundamental goal of this review is to present a fine-grained literature analysis of reward function in ASD with reference to a validated neurobiological model of reward: the ‘wanting’/’liking’ framework. Despite some inconsistencies within the available literature, the evaluation across three converging sets of neurobiological data (neuroimaging, electrophysiological recordings, and neurochemical measures) reveals good evidence for disrupted reward-seeking tendencies in ASD, particularly in social contexts. This is most likely caused by dysfunction of the dopaminergic–oxytocinergic ‘wanting’ circuitry, including the ventral striatum, amygdala, and ventromedial prefrontal cortex. Such a conclusion is consistent with predictions derived from diagnostic criteria concerning the core social phenotype of ASD, which emphasize difficulties with spontaneous self-initiated seeking of social encounters (that is, social motivation). Existing studies suggest that social ‘wanting’ tendencies vary considerably between individuals with ASD, and that the degree of social motivation is both malleable and predictive of intervention response. Although the topic of reward responsiveness in ASD is very new, with much research still needed, the current data clearly point towards problems with incentive-based motivation and learning, with clear and important implications for treatment. Given the reliance of behavioral interventions on reinforcement-based learning principles, we believe that a systematic focus on the integrity of the reward system in ASD promises to yield many important clues, both to the underlying mechanisms causing ASD and to enhancing the efficacy of existing and new interventions. Keywords: Autism spectrum disorders, Reward, Social motivation, Ventral striatum, Ventromedial prefrontal cortex, Amygdala, Dopamine, Oxytocin, Opioids, Treatment * Correspondence: [email protected] Center for Autism Research, The Children's Hospital of Philadelphia, 3535 Market Street, 8th floor, Suite 860 Philadelphia , PA 19104, USA © 2012 Kohls et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 http://www.jneurodevdisorders.com/content/4/1/10
Transcript of REVIEW Open Access Social wanting dysfunction in autism ...reinforcement-based learning principles,...

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10http://www.jneurodevdisorders.com/content/4/1/10
REVIEW Open Access
Social ‘wanting’ dysfunction in autism:neurobiological underpinnings andtreatment implicationsGregor Kohls*, Coralie Chevallier, Vanessa Troiani and Robert T Schultz
Abstract
Most behavioral training regimens in autism spectrum disorders (ASD) rely on reward-based reinforcementstrategies. Although proven to significantly increase both cognitive and social outcomes and successfully reduceaberrant behaviors, this approach fails to benefit a substantial number of affected individuals. Given the enormousamount of clinical and financial resources devoted to behavioral interventions, there is a surprisingly large gap inour knowledge of the basic reward mechanisms of learning in ASD. Understanding the mechanisms for rewardresponsiveness and reinforcement-based learning is urgently needed to better inform modifications that mightimprove current treatments. The fundamental goal of this review is to present a fine-grained literature analysis ofreward function in ASD with reference to a validated neurobiological model of reward: the ‘wanting’/’liking’framework. Despite some inconsistencies within the available literature, the evaluation across three converging setsof neurobiological data (neuroimaging, electrophysiological recordings, and neurochemical measures) reveals goodevidence for disrupted reward-seeking tendencies in ASD, particularly in social contexts. This is most likely causedby dysfunction of the dopaminergic–oxytocinergic ‘wanting’ circuitry, including the ventral striatum, amygdala, andventromedial prefrontal cortex. Such a conclusion is consistent with predictions derived from diagnostic criteriaconcerning the core social phenotype of ASD, which emphasize difficulties with spontaneous self-initiated seekingof social encounters (that is, social motivation). Existing studies suggest that social ‘wanting’ tendencies varyconsiderably between individuals with ASD, and that the degree of social motivation is both malleable andpredictive of intervention response. Although the topic of reward responsiveness in ASD is very new, with muchresearch still needed, the current data clearly point towards problems with incentive-based motivation and learning,with clear and important implications for treatment. Given the reliance of behavioral interventions onreinforcement-based learning principles, we believe that a systematic focus on the integrity of the reward system inASD promises to yield many important clues, both to the underlying mechanisms causing ASD and to enhancingthe efficacy of existing and new interventions.
Keywords: Autism spectrum disorders, Reward, Social motivation, Ventral striatum, Ventromedial prefrontal cortex,Amygdala, Dopamine, Oxytocin, Opioids, Treatment
* Correspondence: [email protected] for Autism Research, The Children's Hospital of Philadelphia, 3535Market Street, 8th floor, Suite 860 Philadelphia , PA 19104, USA
© 2012 Kohls et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 2 of 20http://www.jneurodevdisorders.com/content/4/1/10
ReviewIntroductionAutism is currently defined by impairments in socialinteractions, communication and restricted interests andbehaviors [1]. The core social and communicativeimpairments (which will probably be collapsed into onecategory in the forthcoming fifth edition of the Diagnosticand Statistical Manual of Mental Disorders) can be concep-tualized as a set of related skill deficits (including social reci-procity, social perception and memory, joint attention, andperspective-taking). These deficits conspire to make it diffi-cult for people with autism to develop and maintain socialrelationships [2]. Considering the symptoms of autismspectrum disorders (ASD) as developmental failure to ac-quire adequate social-communication skills brings intofocus the learning processes that underlie ASD. Such skill-based focus has concrete implications for treatment. Cur-rently, there are no FDA-approved medications to treat thecore social and communicative skill impairments of ASD.In fact, it is probably naive to expect that a medication is byitself able to remediate a skill deficit, but it clearly mighthave a role in potentiating or facilitating social skill learning.At present, most interventions targeting social-
communicative skill defects and other behavioral problemsin ASD rely on the principles of applied behavior analysis(ABA), especially operant techniques, where desired beha-viors are reinforced using a variety of rewards (for ex-ample, verbal praise, candy, or stickers). Accumulatingevidence from over 40 years of research indicates thatthese reinforcement-based interventions significantly in-crease both cognitive and social outcomes, and success-fully reduce aberrant behaviors [3]. Although it is wellestablished and has proven efficacious at the group level,this approach fails to benefit a substantial number of indi-viduals on the autistic spectrum [4-6]. It is not yet under-stood how and why behavioral approaches work well forsome people with ASD but not for others. As well asfactors such as lack of treatment fidelity, inadequate choiceof reinforcers, and absent generalization effects, rewardresponsiveness might be a significant moderator of inter-vention outcome in the context of behavior-analysis treat-ment programs. Reward responsiveness most likelymediates skill learning during these types of interventions[4]. Thus, the variable treatment response rate of indivi-duals with ASD might indicate that reward systems aremore efficient in those for whom behavioral interventionsare most effective than in those who profit only minimallyor not at all. Given the enormous amount of clinical andfinancial resources devoted to reinforcement-based inter-ventions, there is a surprisingly large gap in our knowledgeconcerning the basic reward mechanisms in ASD. Under-standing the mechanisms for reward-based learning isurgently needed to better elucidate and inform modifica-tions to the current standard of care.
The aim of this paper was to review the biologicalsubstrates of reward processing in ASD, including neu-roimaging data, electrophysiological recordings, andneurochemical measures. Because current ASD researchlacks a clear reference to any validated neurobiologicalmodel of reward, we introduce a well-established frame-work of reward responsiveness formulated by Berridgeand colleagues: the ‘wanting’/’liking’ model [7,8]. Withreference to this model, we summarize what is currentlyknown concerning the neural correlates underlying re-ward responsiveness in ASD, with a special emphasis onsocial reward versus other reward types. In this context, wediscuss how the available data may not only inform thebasic mechanisms of reward-based treatments in ASD, butalso variability in treatment response. Ultimately, suchknowledge could facilitate early diagnosis and future inter-vention approaches with potentially greater treatment bene-fits for a larger percentage of individuals with ASD. Finally,we highlight several limitations in the current ASD rewardliterature that probably contribute to discrepant studyfindings and that should be resolved in future research.
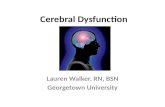
A heuristic of reward responsiveness: the ‘wanting’/’liking’modelThe concepts of reward ‘wanting’ and reward ‘liking’Most people associate reward with something pleasantthat they like, such as a piece of chocolate. However,hedonic feelings are only one feature of reward. Researchhas indeed shown that reward is not a unitary construct,but is actually comprised of different components, whichcan be dissociated both psychologically and neurobiolo-gically [8]. One component is ‘liking’, which is related tothe pleasurable effect of reward consumption. The othercomponent is ‘wanting’ (also called ‘incentive salience’),which corresponds to the motivational aspect of reward;it is the anticipatory drive. Both reward components in-clude conscious and unconscious levels of processing.On a temporal dimension, the processing of reward can besubdivided into two successive phases, with an appetitiveanticipation or ‘wanting’ period usually preceding a rewardconsumption or ‘liking’ response (Figure 1). Typically,rewards that are ‘liked’ are also ‘wanted’. Based on learningexperiences, previously neutral stimuli usually acquirereward value either through the occurrence of hedonic sen-sations of ‘liking’ an unconditioned stimulus (UCS) whenconsuming it (for example, the actual taste of chocolate) orthrough associations of a conditioned stimulus (CS) thatpredicts a reward (for example, picture of a chocolate bar).After learning, ‘wanting’ is easily triggered by encounterswith an incentive CS or with a reward itself (for example,UCS). Incentive CS themselves become strongly salient,and function as motivational ‘magnets’ attracting attention,because they take on incentive properties similar to thereward they predict. This can even turn a previously

Figure 1 A simplified view of the time course of reward processing and its underlying neural correlates (after Berridge and Kringelbach[7]). Temporally, the processing of reward can be subdivided into two successive phases, with a ‘wanting’ period usually preceding a ‘liking’response, each with a discrete neural basis. Although rewards that are ‘liked’ are typically also ‘wanted’, it seems that these two aspects of rewardare dissociable both psychologically and neurobiologically. Rewarding situations are characterized by an anticipation phase or the ‘wanting’ of areward, which often results in a phase of reward consumption or ‘liking’, with some rewards causing a peak level of subjective pleasantness (forexample, a lottery win, job promotion, encounter with an old friend, favorite meal or music, sexual orgasm, drug high). Many rewarding episodesare followed by a period of satiation for the specific reward experienced. To our knowledge, there are currently no data available to suggest thatthe ‘wanting’/’liking’ model would apply differently to social and non-social types of reward. However, some rewards lack satiation effects or resultin only short periods of satiation (for example, money). In general, physiological or drive states (for example, satiation, deprivation, stress, anxiety)strongly modulate an individual’s responsiveness to reward. Both reward ‘wanting’ and reward ‘liking’ have been associated with discrete (and toa specific extent with some overlapping) neural correlates. Whereas ‘wanting’ is mainly driven by phasic dopaminergic neural firing in the ventralstriatum (including the nucleus accumbens), ‘liking’ is largely influenced by the opioid system, and recruits the ventromedial prefrontal cortex(vmPFC). As summarized in this paper, there is good evidence to suggest that reward ‘wanting’ is disrupted in ASD, particularly in the socialdomain, whereas the available data for reward ‘liking’ are inconclusive (see below for details).
Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 3 of 20http://www.jneurodevdisorders.com/content/4/1/10
neutral stimulus into an instrumental conditioned reinfor-cer for which people will work to obtain and ‘consume’(for example, money). Humans possess a general intrinsicmotivation system, which regulates approach behaviors to-wards pleasant stimuli and avoidance of threatening andstressful events. The power of this ‘wanting’ system variesfrom individual to individual, because of natural biologicaldifferences in reward responsiveness and learned differencesin the value of different rewards.Many rewarding episodes are followed by a period of
satiation for the specific reward that was consumed. Toour knowledge, there are no data available to suggestthat the ‘wanting’/’liking’ model would apply differentlyto social and non-social types of reward. However, somerewards lack satiation effects or result in only short periodsof satiation (for example, money). In general, physiologicalor drive states (for example, satiation, deprivation) stronglymodulate an individual’s reward ‘wanting’ and ‘liking’responses. For instance, food cues (for example, smell) arevery potent in eliciting desire for food when a person ishungry, but are less salient when they have recently eaten ameal. As noted above, both reward ‘wanting’ and ‘liking’have been associated with some distinct (and to a specificextent with some overlapping and interrelated) neural sub-strates, which are reviewed next.
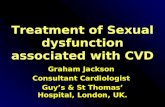
The neurobiological substrates of ‘wanting’ versus ‘liking’The neural circuit mediating reward-related behavior is acomplex network comprising, among others, the midbrain(including the ventral tegmental area (VTA) and the sub-stantia nigra (SN)), the amygdala, the ventral striatum (in-cluding the nucleus accumbens (NAcc)), and theventromedial prefrontal cortex (including the medial orbito-frontal cortex (OFC) and the ventral portion of the anteriorcingulate cortex (ACC)) [9] (Figure 2). Although severalbrain structures contribute to the reward circuitry, thecentral hub within this functional network is the ventralstriatum (VS) [10]. The VS receives major afferent inputfrom the OFC, the ACC, and the medial temporal lobe, in-cluding the amygdala. In addition, strong reciprocal fiberprojections exist between the VS and midbrain regions.Although mostly based on anatomical research in non-human primates, recent developments in human brainimaging, such as functional connectivity measures anddiffusion tensor imaging (DTI), confirm the complexinformation transfer within this frontolimbic networkunderlying reward processing [11].Dopamine is the neurotransmitter predominately asso-
ciated with reward processing [12]. Most dopaminergicneurons within the core reward circuitry, particularly inthe VS, show short bursts of phasic activation in

Figure 2 The neural circuitry of reward ‘wanting’ versus reward‘liking’. The neural circuitry of reward ‘wanting’ comprises theventral striatum (VS; blue), while that for reward ‘liking’ comprises theventromedial prefrontal cortex, including the orbitofrontal cortex(OFC) and the dorsal and ventral anterior cingulate cortex (dACC,vACC) (green), which closely interacts with the amygdala(AMY=orange) and the midbrain, including the ventral tegmental area(VTA; purple). This complex network interfaces with motor-related areasand other higher cognitive associative cortices (not shown here) totranslate basic reward information into appropriate goal-directedaction plans to achieve a desired reward.
Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 4 of 20http://www.jneurodevdisorders.com/content/4/1/10
response to reward and, after learning, in response toconditioned cues that signal a potential reward [13].Although dopamine had long been thought to mediate ‘lik-ing’, recent evidence indicates that dopamine is neither ne-cessary nor sufficient for generating ‘liking’ responses, butplays a more important role in the motivational component(‘wanting’) of reward [8]. More specifically, it has been sug-gested that the amount of phasic dopaminergic neuronalfiring encodes the incentive salience of appetitive environ-mental stimuli, and that such firing typically precedes motorbehavior to seek out, approach, and consume a reward. Ani-mal research using in vivo neurochemical methods indicatesthat phasic dopamine signals in the VS, potentially influ-enced by input from the midbrain, amygdala, and ventro-medial prefrontal cortex (vmPFC), underlie non-social andsocial reward-seeking behaviors, including eating, drinking,reproduction, and other species-specific interactions [14].By contrast, the hedonic effect of reward is primarily asso-ciated with the opioid and endocannabinoid system [15,16].Recent research aims to disentangle the spatiotemporal
localization of both these reward-related components inthe human brain using functional magnetic resonanceimaging (fMRI) [17], although early fMRI studies primarilyfocused on money. Cued anticipation of monetary gainshas been consistently found to recruit the VS, includingthe NAcc, with greater VS activity for more salient incen-tives (for example, $1 versus $5; [18]). Similarly, animalresearch suggests that cue-triggered VS activations pre-cede reward consumption (for example, winning money)and primarily reflect reward ‘wanting’ . This finding has
been replicated with other appetitive stimuli such as bio-logical and social rewards [19,20], suggesting that theVS, particularly the NAcc, functions as a general, modality-independent mediator of reward ‘wanting’.Reward ‘liking’, by contrast, has been primarily asso-
ciated with activations in vmPFC, particularly the medialOFC and the ventral ACC [21]. Using prototypical fMRIparadigms designed to investigate differential brainresponsiveness to reward consumption versus anticipa-tion [18,22,23], the vmPFC has been repeatedly found tobe activated during the processing of pleasant outcomes,including monetary and social rewards [24]. Insight intothe neural basis of reward ‘liking’ has also been gainedusing pleasant-tasting food rewards. Diminished activityin the OFC has been found after a specific food item hasbeen eaten to satiety, thereby decreasing its hedonicvalue and subjective pleasantness [25,26]. More specific-ally, a medial–lateral hedonic gradient has been indenti-fied within the OFC, which tracks the reward value ofdifferent reinforcers with regard to its valence [27]. MedialOFC activity is related to the positive value of reinforcers(for example, winning money), whereas the lateral OFC isassociated with evaluating the unpleasant aspects ofreinforcement (for example, losing money). This medial–lateral gradient interacts with a second hedonic gradientalong the posterior–anterior axis, which represents sec-ondary reinforcers (such as money), more anteriorly in theOFC than primary reinforcers (such as odors, food, touch,sexual pleasure, or drugs) [15,28,29].The ‘wanting’/’liking’ circuitry also interfaces with
category-specific brain areas, allowing informationabout the type of reward to influence the circuit [21];for example, social rewards such as affirmative smilesrecruit reward structures and ‘social brain’ pathways[30]. This complex network interacts closely withmotor-related areas and other higher cognitive associa-tive cortices to translate basic reward information intoappropriate goal-directed action plans to achieve thedesired reward [9].
Relevance to research into autism spectrum disordersAlthough the human fMRI literature is arguably morecomplex than the simple VS (‘wanting’) versus vmPFC(‘liking’) dichotomy described above [31], this frameworkprovides a useful heuristic model to evaluate rewardresponsiveness in individuals with ASD. To date, little isknown about reward function in ASD, and conflictingevidence comes from intervention programs versusexperimental research.On the one hand, behavior analytic intervention pro-
grams, which place reward-based reinforcement at theheart of their treatment system, have been repeatedlyfound to improve socially appropriate behavior and cog-nitive skills while diminishing dysfunctional activities

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 5 of 20http://www.jneurodevdisorders.com/content/4/1/10
[32]. Reward-based interventions draw on a variety ofreinforcers (food, tokens, sensory stimulation, toys, idio-syncratic preferred objects, praise [33]), which act as keylevers for learning. For instance, when a positive reinforcerfollows a desired behavior, the future frequency of thatbehavior is enhanced under similar conditions. By con-trast, when positive punishment (for example, disapproval)follows an undesired behavior, the future frequency of thatbehavior is decreased under similar conditions. On theother hand, evidence from behavioral experiments sug-gests that individuals with ASD have diminished respon-siveness to reward. Stimulus–reward association learninghas been repeatedly highlighted as an area of difficulty forchildren with ASD [34,35], and variability in reward-learning skills has been identified as an important pre-dictor of social-communication abilities [36]. Interestingly,the deficit in reward learning (and its link to social skills)seems to persist through to adulthood, as evidenced byimpairments in the rapid formation of reward–stimulusassociations and its correlation with clinical symptoms ofsocial dysfunction [37-39].Furthermore, both intervention research and behavioral
investigations have suggested that individuals with ASDmight be characterized by particularly low responsivenessto social rewards such as facial expressions (for example,smile), spoken language (for example, praise), and gestures(for example, the thumbs-up gesture) [40,41]. In fact, inbehavioral treatment programs, young children with ASDprofit less from the use of social rewards than from non-social reinforcers [42,43], and several experimental studieshave confirmed that, relative to typically developingchildren (TDC), the performance of children with ASD isonly minimally affected by social reinforcement [44-47].To date, the paradoxical finding of efficacious treatments
rooted in reinforcement strategies in combination withweaker reward systems in ASD has received little attentionin the field. This highlights a gap in our understanding ofthe underlying cognitive and biological processes that con-tribute to treatment response. In particular, a potentiallyimportant limitation of current experimental and interven-tion research in ASD is that it tends to construe reward asa unitary phenomenon, lacking a clear reference to anyvalidated neurobiological model of reward; however, a crit-ical examination of reward function in ASD requires amore fine-grained analytic approach. For instance, lowerresponsiveness to social reward as evident at the behav-ioral level could be the result of diminished ‘wanting’or ‘liking’, or both. More specifically, reward ‘liking’usually triggers and directs reward ‘wanting’ so that theextent to which a reward is wanted typically depends onthe degree to which it has been liked [7]. However, in somepsychiatric disorders, such as addiction, schizophrenia, anddepression, ‘wanting’ and ‘liking’ can become uncoupled asa result of circumscribed neurobiological dysfunctions [48].
For example, a disruption in dopamine function mightcause diminished ‘wanting’ and approach behavior to obtaina specific rewarding stimulus, even if the ‘liking’ response tothat particular reward is preserved. In the case of schizo-phrenia, anhedonia (the reduced capacity to experiencepleasure or ‘liking’), has long been considered to be a car-dinal symptom of patients with this disorder [49]. However,recent studies using a range of pleasant stimuli, includingpositive words, faces, sounds, film clips, erotic pictures, andsweet drinks, have highlighted that the ability to experiencepleasure is generally intact in individuals with schizophre-nia, whereas the capacity to pursue and achieve a pleasur-able goal (that is, the ‘wanting’ component of reward), issignificantly disrupted [50]. Several authoritative reviewsthus concluded that anhedonia (diminished ‘liking’) is a lessprominent feature of schizophrenia than avolition(diminished ‘wanting’) [49,51-53].This example clearly illustrates that consulting the
‘wanting’/’liking’ model is particularly helpful to identifywhich aspect of reward function is compromised or pre-served in different psychopathologies. Such informationmight facilitate efforts at early identification and couldhave important implications for prevention and interven-tion programs. In the case of ASD, an improved under-standing of distinct reward functions and their respectivedisruption may help to isolate discrete reward subpro-cesses (‘wanting’ versus ‘liking’) and their associated bio-logical substrates (VS versus vmPFC) as treatmenttargets.Given that there are currently no objective behavioral
markers of ‘liking’ and ‘wanting’, it is necessary to drawon neurobiological measures. Three sets of data areconsidered in this review: 1) functional neuroimagingsignals, 2) electrophysiological recordings, and 3) neuro-chemical data. Several preliminary predictions can bemade with respect to the ‘wanting’/’liking’ model. If‘wanting’ is compromised in ASD we would expect tosee 1) aberrant brain responses in the VS, 2) atypicalevent-related brain potentials (ERPs) and EEG patternsassociated with the anticipatory aspect of reward, and(3) disrupted dopamine function. On the other hand, if‘liking’ is negatively affected, we would predict 1) aber-rant brain activation in the vmPFC, 2) atypical ERP andEEG responses related to reward outcome processing, and3) disrupted opioid function. Considering the core socialphenotype of ASD (for example, ‘lack of spontaneousseeking to share enjoyment, interests, or achievements withother people’ [1]), it can be speculated that both ‘wanting’and ‘liking’ of social reward is compromised in this dis-order, with the most pronounced disruptions to beexpected for social reward ‘wanting’ (that is, social moti-vation). In the following sections, we evaluate the extent towhich the proposed predictions are supported by the avail-able data.

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 6 of 20http://www.jneurodevdisorders.com/content/4/1/10
Reward responsiveness at the neurobiological level in ASDFunctional magnetic resonance imagingAlthough the involvement of the mesocorticolimbicreward circuitry in the psychopathology of ASD has beendiscussed in the literature for many years [40,41,54-58],only recently has research begun to systematically evaluatepotential malfunctions within this circuitry. In the followingsection, we review the handful of studies that used fMRI tocompare the blood oxygen level-dependent (BOLD) signalin response to different types of reward in children andadults with ASD relative to typically developing controls.There are complex sets of data reported across the differentstudies, but in this paper, we focus exclusively on the VSand the vmPFC as the neural substrates of reward ‘wantingand ‘liking’ respectively. Further, because the amygdalaforms a unique microcircuitry with the VS and the vmPFCto promote reward-seeking behaviors [59], and has beenrepeatedly suggested to be dysfunctional in ASD [41], wealso review the amygdala-related findings in more detail.
The ventral striatum and reward ‘wanting’The available data suggest that ‘wanting’ (the motivationaldrive to achieve reward) is compromised in ASD. Four outof five published fMRI studies reported diminished VSactivation in individuals with ASD compared with TDCwhen processing either social or monetary reward versusnon-reward [30,60-62]. In two studies, Dichter and collea-gues compared neural activation in samples of adults withand without ASD during a delayed anticipation task withtwo different reward contingencies. First, they tested brainresponses to money and typical autism-specific objects ofinterest (for example, trains, cars, plastic bricks) and founddecreased VS activation in ASD during periods of moneyanticipation and outcome, whereas VS activity was presentfor typical autism-specific objects of interest [60]. In a fol-low-up study applying the same paradigm but with a focuson social (for example, faces) versus monetary reward,adults with ASD again showed lower brain activation inthe VS during money anticipation, but did not reveal VShypoactivation for face rewards [61]. An early study bySchmitz and colleagues applied a monetarily rewardedsustained attention task to adults with and without ASD,but did not report VS activation in either group [63].Scott-Van Zeeland and colleagues [62] were the first tocompare BOLD responses to both monetary and social re-ward (for example, smiling face combined with verbalpraise) in children with and without ASD performing animplicit learning task. In this study, the ASD group dis-played diminished activation in the VS for social reward,but not for monetary reward. In addition, VS activation tosocial reward predicted social capacities (as measured bythe Social Responsiveness Scale) within the TDC group,but not the ASD group. Kohls et al. [30] also tested chil-dren with and without ASD, and investigated BOLD
responses to social and monetary reward in the context ofan incentive go/no-go paradigm. Similar to the stimuli byScott-Van Zeeland and colleagues [62], approving faces thatwere contingent on accurate task performance were usedas social reinforcers. Despite normal reward responsivenessat the behavioral level, participants with ASD showedhypoactivation in the VS under monetary reward condi-tions that required an active response to obtain a reward.Contrary to the authors’ predictions and to the results ofthe previous study [62], significantly reduced VS responsesduring social reward processing were not seen, but thesefindings are consistent with results from Dichter et al. [61].Taken together, blunted VS activity is a replicated
phenomenon in children and adults with ASD, andmight represent a neurobiological marker for diminishedincentive salience (‘wanting’) related to social and/ormonetary reward. Compromised ‘wanting’ possibly dis-rupts the tendency in ASD to self-initiate goal-directedactions to seek out specific environmental rewards (forexample, social incentives), whereas motivational tenden-cies towards strongly preferred idiosyncratic rewardsseem to be preserved; typical autism-specific objects ofinterest led to normal VS activation suggestive of intact‘wanting’ for this type of incentive. However, it should beacknowledged that the reviewed data provide a some-what inconsistent picture about the specificity of VS dis-ruption to social versus monetary reward. It is beyondthe scope of this paper to speculate upon the diversesubject- and method-related factors that might have con-tributed to these inconsistencies (for a thorough discus-sion, see Kohls et al. [30]). Importantly, however,although monetary reinforcers have predominantly beenoperationalized and used as non-social stimuli, money isimbued with social connotations and exerts a substantialinfluence on pro-social behavior [64-66]. In this regard,aberrant VS responses to monetary incentives would notnecessarily be at odds with the autism social phenotype.In addition, different potencies of social reward havebeen applied across studies, which could explain the dis-crepant results with respect to this type of reward. A pic-ture of a smiling face paired with verbal praise was usedas social reinforcement by Scott-Van Zeeland et al.,whereas Dichter et al. and Kohls et al. chose static facerewards without praise. It seems likely that the combin-ation of facial rewards with praise may represent a stron-ger social incentive with correspondingly greater rewardsystem responsiveness, primarily in TDC, making itmore probably that activation differences are detectedbetween individuals with and without ASD within theVS. Future research should address these issues.
The ventromedial prefrontal cortex and reward ‘liking’Regarding the vmPFC as the mediator of reward valuationor ‘liking’, the available imaging data are rather mixed. For

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 7 of 20http://www.jneurodevdisorders.com/content/4/1/10
the vmPFC (including rostral–ventral ACC and medialOFC), two studies reported stronger activation [62,63] andtwo reported lower activation [30,61] in ASD comparedwith TDC in response to monetary reward. In Schmitz’sstudy [63], ventral ACC activity correlated positively withsocial symptom severity (ADI-R), suggesting a possiblelink between atypical reward consumption and social func-tioning. Another study showed diminished activation inthe vmPFC under social reward conditions [30], which isin contrast to data from Dichter et al. [61] and Scott-VanZeeland et al. [62]. Lastly, one investigation found greateractivation in the vmPFC in response to autism-specificobjects of interest in individuals with ASD relative to typicalcontrol participants [60].In summary, the current ASD imaging literature pre-
sents no clear pattern of results with respect to possibledifferences from controls for reward consumption or‘liking’. Interestingly, however, enhanced activation inthe vmPFC in response to high autism-interest objectssuggests that the hedonic value of such objects is greaterin individuals with ASD than in TDC. This idea is in linewith literature showing that certain classes of objectsand topics, which often constitute circumscribed interests,are perceived as pleasurable by many affected individuals[67], and the use of such items in behavior-analysis inter-vention programs has been found to be therapeuticallyeffective [68,69]. However, on a day-to-day basis, thesestrongly ‘liked’ circumscribed interests are likely to inter-fere with social functioning.
The amygdala as a salience detectorThe amygdala is thought to influence and amplify theperception of emotionally and motivationally potentstimuli at very early stages in their processing. It tracksrelevant positive and negative events in the environmentand contributes to appropriate adaptation of behavior(for example, approach or avoidance reactions [70]).Additionally, amygdala function is crucial for making anassociation between a specific stimulus (for example, faceof an unknown person) and the affective experiencesintrinsically associated with this stimulus (for example,pleasant social interaction with this person), linking ini-tially neutral environmental stimuli with motivationalsignificance [71].The amygdala has been repeatedly linked to the social
deficits present in ASD [41,56]. For instance, in an inter-esting fMRI study, Grelotti and colleagues [72] foundweaker amygdala activation for faces than for cartooncharacters (for example, Digimon ‘Digital Monsters’) inan autistic boy with a strong preoccupation with thesecharacters, whereas a matched typical control boyshowed the expected opposite neural activation pattern.The strong amygdala engagement with the cartoon char-acters seemed to reflect the exaggerated motivational
salience tagged to this idiosyncratic interest relative tofaces. Put another way, decreased amygdala activationfor faces might reflect a lack of proper appetitive valueassigned to this class of stimuli [41,73].The study by Dichter and colleagues [61] on reward
processing revealed hyperactivation in the amygdala inadult participants with ASD while they were anticipatingsocial reward. This activation correlated positively withsocial symptom severity (Autism Diagnostic ObservationSchedule-Generic ADOS-G). By contrast, Kohls and co-authors [30] found hypoactivation in this brain areaunder social reward conditions in children with the dis-order. Both studies used very similar experimental taskdesigns with comparable reward contingencies. Theinconsistent finding might be due to the different agesstudied in the two papers, as other data suggest thatthere could be an abnormal developmental trajectory ofamygdala reactivity to social incentives in ASD [74,75].Systematic research is clearly needed to address this ideaand its implications for the development of aberrant so-cially motivated behavior in ASD.
SynopsisIn summary, the vmPFC–VS–amygdala circuitry seemsto be dysfunctional in ASD, and to form, at least par-tially, the basis for atypical reward responsiveness inindividuals with ASD. Preliminary evidence indicates thatthe motivational component of reward (the ‘wanting’)might be particularly compromised in individuals withASD. This is reflected in blunted VS activity, which,however, seems to be dependent on the incentive at stake(that is, low versus high autism-interest rewards).Dysfunction within the vmPFC–VS–amygdala system,
such as an insufficient communication between theamygdala and/or the vmPFC to the VS, has been pro-posed to underlie aberrant motivation to seek out detri-mental substances at the expense of ‘natural’ rewards inother psychopathologies (for example, addiction [76,77]).It can therefore be hypothesized that an atypical pattern ofbrain activity within this circuitry in individuals with ASDmay trigger strong seeking of salient, autism-specificrewards at the cost of neglecting other essential environ-mental rewards, including social rewards. In fact, severalrecent imaging studies on resting-state functional con-nectivity and DTI confirm disruptive neural activationdynamics in ASD within the vmPFC–VS–amygdala cir-cuitry [78-81]. These findings are also in line with theidea of ASD as a neurofunctional disconnection syn-drome [82-84], most likely mediated by complex geneticfactors (for example, synaptic cell adhesion plasticity[85]), which affect efficient information transfer withinthe mesocorticolimbic reward circuitry and may causeaberrant motivation, that is, affect ‘wanting’ tendencies.

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 8 of 20http://www.jneurodevdisorders.com/content/4/1/10
Event-related brain potentials and resting-state EEGDespite the fine spatial resolution of functional MRI, onemajor limitation is its restricted temporal precision. Forinstance, the BOLD signal in the VS evoked by reward-predicting cues has been shown to rise at 2 seconds, topeak between 4 and 6 seconds, and to fall back to base-line after 10 to 12 seconds [86]. In contrast to the rela-tive slowness of the brain’s BOLD response as measuredby fMRI, electrophysiological recordings such as electro-encephalography (EEG) and ERP provide measures withexquisite real-time temporal resolution on the scale ofmilliseconds [87]. Thus, EEG and ERP might be specific-ally suited to address the question about the extent towhich temporal phase of reward processing might becompromised in ASD (reward anticipation/’wanting’versus reward consumption/‘liking’). In the next section,we summarize the current knowledge with regard toelectrophysiological correlates underlying reward respon-siveness in individuals with ASD relative to controls.
Event-related brain potentials components related to‘wanting’ and ‘liking’Two ERP components are especially relevant to the‘wanting’/’liking’ framework: the feedback-related nega-tivity (FRN) and the P3 component. Although these twoERP correlates are associated with well-described func-tional roles in the cognitive neuroscience literature (FRNwith external reward monitoring; P3 with selective atten-tion allocation), both have been repeatedly described asindirect neural indices of reward responsiveness. The P3and the FRN can be elicited by reward-predicting cuesand reward outcome. However, research and theory sug-gests that the P3 is more closely related to reward-seekingbehaviors (‘wanting’) and the FRN to reward consumption(‘liking’ or ’disliking’) [88,89].The P3 is a positive ERP component with a maximum
deflection at parietocentral electrodes (for example, Pz),whereas the FRN is a negative deflection, which has itslargest amplitudes at frontocentral sites (for example,FCz). Each component peaks around 300 ms after theonset of a critical stimulus. However, whereas the P3 hasbeen found to be sensitive to reward magnitude (that is,larger amplitudes for high versus low reward) and rewardvalence (that is, larger amplitudes for reward gain versusloss), the FRN is modulated almost exclusively by rewardvalence, with more negative waveforms in response tonon-reward outcome relative to reward gain [90]. More-over, both components are influenced by an individual’stask engagement, so that larger amplitudes result fromactive goal-directed responding to achieve a reward com-pared with the passive receipt of a reward [91]. Althoughmost normative studies have focused on the effect ofmonetary reward on these components, more recently,two reports showed that social rewards (for example,
affirmative faces) elicited robust P3 and FRN responsescomparable with those evoked by monetary rewards[92,93]. Additionally, different personality dimensions,including reward dependence, seem to determine the ex-tent to which both waveforms are modulated by rewardin the normal population [94,95].According to the locus coeruleus norepinephrine (LC-
NE) P3 hypothesis, the P3 component reflects a short,phasic signal of the widely distributed and synchronouslyactive LC-NE system, which closely interacts with the re-ward circuitry (for example, vmPFC, amygdala) to evaluatethe salience of an incoming stimulus and, as a result, tooptimize active reward-seeking (‘wanting’) behaviors [89].By contrast, the FRN can be understood as a general mani-festation of a reward-monitoring system that recognizes dis-crepancies of outcome expectancies during rewardconsumption, for example, if a ‘liked’ reward is expected butnot delivered, it elicits a ‘disliking’ signal, which is reflectedin a negative ERP response. Such a mechanism enables anindividual to adjust their behavior adequately so that the re-ward benefit can be maximized in the future. The vmPFC(that is, ACC) and the striatum have both been suggestedas potential sources for the scalp-recorded FRN response[96-98]; however, the involvement of the striatum is lesslikely [99].
Feedback-related negativity, P3, and reward responsivenessThe field of ASD has a long and rich tradition of usingERP measures to acquire detailed real-time informationabout the dynamics and integrity of neural processes inthe brain of individuals with ASD [100]. However, re-search has just started to evaluate the clinical utility ofthe P3 and the FRN as potential markers for abnormalreward responsiveness in ASD. In the following sections,we present recent relevant findings and interpret themin the framework of reward anticipation (’wanting’)versus reward consumption (’liking’).Groen and colleagues [101] investigated ERP responses
in a mildly impaired group of children with pervasivedevelopmental disorder not otherwise specified (PDD-NOS) while they performed a reinforcement-based learn-ing task with performance feedback (winning or losingpoints). There was a robust P3 effect in response to feed-back outcome. A P3 related to feedback anticipation wasnot reported. The participants with PDD-NOS did notdiffer from a TDC group in their outcome-evoked P3,suggesting that feedback processing was intact in this pa-tient group. Interestingly, however, during the anticipa-tion of positive feedback, the PDD-NOS group displayedan atypical stimulus-preceding negativity (SPN), an ERPcomponent that is thought to index reward anticipation,similar to the P3 [102].Larson and colleagues [103] used a gambling task to
specifically elicit the FRN and P3 in response to

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 9 of 20http://www.jneurodevdisorders.com/content/4/1/10
monetary gain versus loss in children with and withoutASD. Reward anticipation was not assessed in this study.Similar to the findings by Groen [101], the ERPs evokedby reward outcome did not differ between the experi-mental groups. The authors concluded that the neuralresponse to concrete, external feedback, that is, monet-ary gain (‘liking’) and loss (‘disliking’), is intact in ASD,reflected in normal FRN and P3 effects.It should be noted that both Groen and Larson only used
one type of incentive in their studies, points and money re-spectively, which leaves unclear the extent to which theirfindings may also be relevant for other fundamental typesof appetitive stimuli such as social rewards. Kohls and col-leagues [92] were the first to compare the effect of social(that is, affirmative faces) and monetary incentives on ERPresponses in children with ASD versus TDC. They adopteda cued go/no-go paradigm from the animal literature,which has been widely used to assess reward anticipation(initiated by cue signals) followed by goal-directed behavior(for example, button press or inhibitory response) and apotential rewarding outcome [104]. The authors focusedon the P3 as the ERP component of interest; the task de-sign was not suited to evoke the FRN. Consistent with thefindings of Groen et al. [102] and Larson et al. [103], theoutcome-related P3 did not differentiate between ASD andTDC participants. However, whereas the TDC group exhib-ited an increased P3 in response to cues that signaled a po-tential social or monetary reward, relative to non-reward,the ASD group did not show this enhancement effect, andeven showed diminished P3 activity in response to cues thattriggered a phase of social reward anticipation. Moreover,P3 activity elicited by incentive cues in both social andmonetary reward conditions correlated negatively with so-cial symptom severity (ADOS-G), suggesting that childrenwith ASD who had stronger social deficits had weakermodulation of the go-cue P3 when reward was at stake.Based on the LC-NE P3 theory, the authors concluded thatthe ERP data indicate an attenuated state of motivated at-tention allocation, particularly towards signals that triggeractive reward-seeking (‘wanting’) behavior in individualswith ASD [105].Although it is premature to draw conclusions from only
three ERP reports, the evidence suggests that outcome-related neural responses are less impaired in ASD (reflectiveof relatively intact ‘liking’) than are brain potentials relatedto the anticipatory period preceding reward consumption(reflective of disrupted ‘wanting’), based on the incentivesused to date. This neural dysfunction involves both socialand non-social (for example, monetary) reward, with amore pronounced deficit for social incentives.
Frontal alpha power asymmetriesThe strength of reward approach tendencies can beassessed across the age spectrum with active- and
resting-state EEG by calculating hemispheric alphapower asymmetries over the frontal cortex [106]. Indivi-duals with greater frontal alpha activity on the left rela-tive to the right hemisphere display more reward-seekingbehaviors than do individuals with greater activity on theright side. The left vmPFC has been suggested as thepotential source for stronger left-sided alpha-band activity[107]. Owing to the relatively limited spatial resolution ofEEG source localization techniques, it is not yet clear towhat extent other reward structures contribute to thescalp-recorded alpha asymmetries. Because of its involve-ment in reward ‘wanting’, one likely candidate is the dopa-minergic VS [108,109].With regard to autism, Sutton and colleagues [110]
were the first to investigate the relationship betweenresting-state frontal alpha asymmetry and symptom se-verity expression in ASD. Children with ASD whoshowed left frontal EEG asymmetry were reported bytheir parents to have fewer symptoms of social impair-ment compared with children with right frontal asym-metry; however, the former was accompanied by greaterlevels of social anxiety and stress. These findings suggestthat children with ASD with left frontal asymmetrymight be more motivated to participate in social interac-tions, possibly because of stronger ‘wanting’ tendencies.A stronger inclination to seek out social interactionsmay make the appearance of social impairments lesssevere, resulting in reduced reports of symptoms,whereas, the motivation to interact with others, coupledwith an underdeveloped behavioral repertoire to do so,might result in heightened levels of social stress and anx-iety [111]. Interestingly, the left asymmetry subgroup ofchildren with ASD has a great resemblance to the ‘ac-tive-but-odd’ clinical subtype described by Wing andGould [112], whereas the right asymmetry group is moreconsistent with the ‘passive’ or ‘aloof ’ subtypes [111].Dawson and colleagues [113] first noted differences infrontal alpha power in children with ASD classified as‘active-but-odd’ versus ‘passive’. This was replicated re-cently by Burnette and colleagues [114], who also foundthat left frontal alpha asymmetry during resting state wasassociated with later age of onset of ASD-specific symp-toms based on parental report. This could indicate thatgreater social interest (‘wanting’) may obscure socialsymptom presentation in young children, resulting indelayed identification.In a first attempt to measure frontal alpha activity during
an active task, Kylliäinen and colleagues [115] recentlyreported relatively greater left-sided frontal alpha activityin TDC during viewing of faces with direct eye gaze,reflective of motivational social approach [116], a patternthat was absent in children with ASD. By contrast, nogroup differences were detected in frontal alpha responsesto non-social control stimuli, such as automobiles. The

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 10 of 20http://www.jneurodevdisorders.com/content/4/1/10
authors concluded that social attention as expressed bydirect eye contact may not be socially rewarding for chil-dren with ASD, and thus, does not properly activate theirapproach-related brain mechanisms. Interestingly, the datadid not support the assumption of greater aversion-relatedphysiological responses to direct eye gaze in ASD relativeto controls that have been made in previous reports[117,118]. However, it should be noted that left frontalalpha asymmetries have not been linked exclusively toreward seeking in the social domain. Stronger responsive-ness to monetary incentives also correlates with larger leftfrontal alpha power in typical individuals [107], indicatingthat EEG asymmetries reflect more general motivationtendencies rather than specifically social ones. With regardto ASD, further studies are warranted that assess, for in-stance, frontal alpha activity in response to stimuli of highautism-specific interest to test the extent to which anexaggerated reward value of this type of stimuli contri-butes to the presentation of the autism social phenotype(for example, interference with socially motivatedapproach behaviors).
SynopsisIn summary, electrophysiological studies in ASD showatypical results related to the anticipatory (or ‘wanting’)aspect of rewarding events, especially in the social do-main, which may affect social orienting and approach.However, the degree to which this impairment reflectsan intrinsic versus a learned process (or a combinationof both), and its specificity to social stimuli (versus, forexample, autism-specific objects of interest), is as yet un-resolved. The literature suggests that stronger socialinterest can potentially overshadow symptom expressionin young children with ASD, preventing early diagnosis.Therefore, information about social motivation profilesacquired through either behavioral and/or electrophysio-logical measures (for example, frontal alpha asymmetry)is crucial to facilitate efforts at early identification. More-over, future inquiries will reveal the extent to which EEGinvestigations can assist in determining which childrenwith ASD are likely to be treatment responders andwhich might require special or modified treatmentefforts.
Neurotransmitters and neuropeptidesAlthough multiple reward-related neurotransmitters andneuropeptides have been implicated as atypical in ASD,we focus here on dopamine, opioid, and oxytocin (dys)function, because of their potential effect on reward‘wanting’ and ‘liking’ [56]. Dopamine and endogenousopioids are well-known neurochemicals with circum-scribed roles in motivational behavior such as reward-seeking versus consumption, respectively [119], whereasthe peptide oxytocin has only recently become
established as a facilitator of reward signaling and learning,particularly in social contexts [120]. Thus, all three mole-cules provide independent contributions to rewardingeffects, as described below.
The dopaminergic ‘wanting’ systemDopamine mediates a variety of behaviors and functions,including selective attention, learning, motor functioning,hormone release, and goal-directed motivated behaviors[121]. In this context, dopamine primarily encodes the in-centive value (or the ‘wanting’) of reward. It is released inresponse to contextual cues predictive of reward, initiatinga phase of reward anticipation and approach. Animalresearch shows that dopamine antagonists or agonistsinjected into the VTA and VS impair or facilitate, respect-ively, reward approach behaviors, but not reward con-sumption [119]. In humans, drug-induced activity in theVS is linked to feelings of craving and ‘wanting’, but not tofeelings of euphoria or pleasure [122].Dysfunction in the dopamine system in ASD has been
suggested, based on the beneficial effects of dopaminereceptor antagonists (for example, antipsychotic drugssuch as risperidone) in treating certain symptoms com-monly exhibited by affected individuals, such as stereoty-pies, aggression, hyperactivity, and self-injury [123].Because such symptoms can be induced in animals byincreasing the dopamine level, it has been inferred thatASD might be associated with mesocorticolimbic dopa-minergic overactivity. However, conflicting results havebeen found in studies measuring peripheral (for example,blood, urine) or central (for example, cerebrospinal fluid(CSF)) levels of dopamine and its metabolites, with somestudies reporting atypical dopamine turnover in patients[121]. Evidence is also scarce and inconclusive with re-gard to dopamine-related neuroimaging using positronemission tomography (PET) or single photon emissioncomputed tomography (SPECT) in individuals withASD. For instance, Ernst and colleagues [124] foundreduced dopamine metabolism in the vmPFC, but not inthe VS, in children with ASD compared with controls.However, follow-up studies could not confirm this earlyfinding, and reported either enhanced dopamine bind-ings in the vmPFC [125], in the VS [126,127], or in bothbrain areas [128], or did not find any abnormalities inASD [129]. It should be noted that urine, blood, CSF andbaseline PET/SPECT measurements usually assess stable,tonic dopamine levels, whereas the beneficial effects ofantipsychotic drugs stem from blocking phasic dopaminerelease, which only minimally contributes to these toniclevels [130]. This raises the possibility of a dysfunction inthe phasic rather than the tonic dopamine metabolism inASD, which would be more consistent with the neuroi-maging and electrophysiological findings of atypical re-ward ‘wanting’. Indeed, reward-predicting signals and

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 11 of 20http://www.jneurodevdisorders.com/content/4/1/10
behaviorally important events (for example, novel stimuli)elicit brief, phasic, bursts of dopamine impulses, which lastless than 500 ms, and prompt reward anticipation [12]. Re-search provides evidence that specific subpopulations ofdopaminergic cells within the VS respond differently de-pending on reinforcer type. It has been shown that somestriatal cell groups encode primary reinforcers (for ex-ample, water, food, sexual intercourse), whereas others arethought to be ‘idle’ and modifiable through reward-basedlearning (for example, drug conditioning [131]). The ideathat dopaminergic cell activity tracks different rewardtypes is intriguing, because it might offer a simplistic, al-though plausible, explanation as to why some incentives(for example, objects of circumscribed interest) inducegoal-directed approach behavior in individuals with ASD,whereas others (for example, social reward) do not. Such‘selective’ impairment could be thought of as geneticallydriven [132,133], or acquired through aberrant learningexperiences, or both. Because single-cell recordings aremostly limited to animal research, the use of mousemodels of ASD could be a fruitful approach to test themerits of this idea [134].
The opioid ‘liking’ systemBehavioral effects of opiate administration include symp-toms such as insensitivity to pain, social withdrawal,motor hyperactivity, repetitive and stereotyped behaviors,and hypersensitivity to sensory stimulation. This overlapwith ASD symptoms has led to the idea of an opioid dys-function in autism [135-140]. Endogenous opioids (oropiates, such as beta-endorphins or enkephalins) arepeptides that act as neuromodulators in the CNS anddock at receptors activated by morphine, an alkaloidextracted from opium, and related substances [141].Thus, the euphoric and narcotic effects elicited by mor-phine are thought to be shared by endogenous opioids pro-duced by the body. A large body of evidence from animaland human research suggests a role of endogenous opioidsin pleasant social and non-social behaviors, including sexualactivity, social interactions, play, grooming, and food intake.In humans, endogenous opioids increase subjective feelingsof interpersonal warmth, euphoria, and calmness, but de-crease incentive motivation. It has been proposed that en-dogenous opioids induce pleasure and bring consummatorybehaviors to a satisfying conclusion [119,142,143]. This‘liking’ role is emphasized by the fact that the vmPFC, abrain area that is explicitly associated with reward ‘liking’,contains a particularly high density of opioid receptors [15].The data on the possible role of opioid dysfunction in
ASD has been conflicting, with opioid measurementsfrom urine, blood plasma and CSF being reported asdecreased, increased or normal [121]. Some authorsargue that there might be subtle alterations in opioidfunctioning in ASD (for example, increased C-terminally
directed beta-endorphin protein immunoreactivity, butnormal N-terminally directed activity), whereas otherssuggest that such aberrant opioid levels are not specificto ASD [56]. Moreover, because of the putative role ofendogenous opioids in the regulation of social behavior,several investigations have examined the effect of opioidreceptor antagonists (for example, naltrexone) on symp-tom expression in ASD. Despite some modest effects onmaladaptive behaviors, for example, irritability, hyper-activity, self-injury, most controlled studies suggest thatthe efficacy of this treatment is limited, especially withregard to the social symptoms of ASD [144]. Takentogether, there is no consistent evidence that atypicalopioid functioning is a determining factor for the corephenotype of ASD. Considering that endogenous opioidsmediate the hedonic aspect of reward, this conclusion isin line with the neurophysiological findings that reward‘liking’ is less compromised than ‘wanting’ in affectedindividuals.
The oxytocin system as neuromodulator of ‘wanting’ and‘liking’Several lines of inquiry suggest that social cognition andbehavior are regulated by a combination of dopamine,opioids and the hormone oxytocin [145,146]. Oxytocin isa nine amino-acid peptide, which is synthesized in theparaventricular and supraoptic nucleus of the hypothal-amus, and released into the bloodstream by the posteriorpituitary with wide distribution in the central nervous sys-tem [147,148]. Oxytocin is best known for its contributionto numerous social functions in humans and animals, in-cluding social recognition, species-specific interactions,attachment, and other pro-social behavior [120,149-151].Cumulative evidence is consistent with the view that oxy-tocin enhances the motivation for social interactionsthrough a complex functional system. This involvesincreased social attention and memory and reduced socialstress and social anxiety, which in combination promotethe ability and willingness of an individual to repeatedlytake risks in approach, cooperative, and trusting behaviors[152]. Oxytocin exerts its effects on social motivationthrough a variety of neurochemicals among which dopa-mine and opioids are key players. Both dopamine (‘wanting’)and opioids (‘liking’) mediate social encounters and eventu-ally the formation of pleasant social rewards and memoriesassociated with such occurrences. In turn, this increases thelikelihood of an individual to seek out these stimuli in thefuture [119].External contextual cues predictive of potential social
reward (for example, face or voice of the caregiver) serveas incentive signals that elicit a dopamine-related antici-patory phase of ‘wanting’. Oxytocin is thought to en-hance the perceptual salience of such signals, whichfacilitates their interpretation and influences affiliative

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 12 of 20http://www.jneurodevdisorders.com/content/4/1/10
approach behavior. Physiological evidence suggests thatoxytocin neurons in the hypothalamus may directly pro-ject to the VS, activating dopamine release and influen-cing locomotor behavior [153,154]. As the affiliativeperson is reached, the exchange of reward (for example,pleasant touch, approval) triggers opioid release, whichpromotes a state of pleasure and ‘liking’. During thisconsummatory phase of ‘liking’, oxytocin has the poten-tial to increase opioid release in the brain by up to 300%[155]. In fact, it has been shown that brain areas that areinnervated by dopamine and opioids including the VS,the VTA and the prefrontal cortex, contain a high dens-ity of oxytocin receptors, making these regions veryreceptive to changes in central levels of oxytocin[119,156]. Moreover, human imaging demonstrates thatintranasally administered oxytocin acts directly on brainprocesses by modulating social and reward circuitries[157-163]. As a result of the neurochemical interplaybetween the oxytocin , dopamine, and opioid systems,social encounters and contextual stimuli associated withthese encounters (for example, face of the caregiver) aretagged with positive reward value, an essential prerequisitefor socially motivated approach behaviors (for example,orienting towards the caregiver).Evidence is emerging that the oxytocin system is altered
in ASD [164], which might be a contributing factor toatypical reward functioning in affected individuals. Dawsonand colleagues [40], drawing upon the work of Insel andcolleagues [165], proposed a model suggesting that socialreward deficits in ASD could result from alterations inoxytocin activity in the context of social interactions, whichnegatively influence the dopaminergic reward system, andprevent linking of social stimuli with their proper rewardvalue. In fact, two studies have found lower average levelsof blood plasma concentrations of oxytocin in individualswith ASD relative to controls [166,167], a decrease thatcould stem from inefficient or incomplete conversion ofoxytocin from its precursor prohormone [168,169].Genetic associations between ASD and the oxytocin re-ceptor gene, and with the closely related vasopressingene, have also been reported [170]. As discussed byInsel et al. [165], abnormalities in the oxytocin neuralpathway could account for many features of ASD, in-cluding early onset, predominance in males, geneticloading, and neuroanatomical abnormalities. In fact,postmortem brain analyses were found to have a specificdecrease in oxytocin mRNA in the temporal cortex inASD, which was associated with hypermethylation [171].The reduced expression of oxytocin receptors in thetemporal lobe of persons with ASD is interesting in lightof extensive evidence suggesting that the temporal lobe,including the amygdala, has a special role in social percep-tual and reward processes [41,70]. The most promisingdata suggestive of an oxytocin deficiency related to the
development of ASD come from pioneering studies on thetherapeutic effects of intravenous and intranasal oxytocinin individuals with this disorder. These initial studiesfound that oxytocin , relative to placebo, reduces repetitivestereotypic behaviors [172], improves the recognition andmemory of social–emotional information [173,174], andincreases cooperative behaviors, trust, and attention tosocially informative stimuli (for example, eyes) [166]. Con-sidering the role of oxytocin within the ‘wanting’/’liking’framework, the positive therapeutic effects on social func-tioning in ASD may be partially mediated by enhanced so-cially motivated attention and drive (‘wanting’) towardsimportant social encounters and affiliation (for example,social stimuli or interactions [120,146]). The extent towhich this enhancement of social responsiveness is indeeda direct consequence of oxytocin-induced dopamine in-volvement remains to be determined [175,176]. Innovativeresearch is needed to elucidate the interaction betweenoxytocin and dopamine as well as between oxytocin andopioid systems to guide both theory (for example, neuro-biological basis of social motivation deficits in ASD) andspecifically tailored therapeutic approaches for manipulatingthe underlying neural circuitries (see also the Discussionsection).
SynopsisIn summary, whereas the opioid ‘liking’ system lacksconsistent evidence of involvement, both the dopamine-mediated ‘wanting’ system and particularly the oxytocinsystem are promising candidates for contribution toatypical reward-related behaviors in ASD. Given theclose interaction between dopaminergic and oxytocinmechanisms in driving socially motivated behaviors, anyimbalance within the physiological interplay of these twomechanisms has the potential to disrupt social ‘wanting’tendencies such as seeking out of social activities or friend-ships. Based on the evidence reviewed in this section, itcan be hypothesized that the administration of oxytocin asa pharmacological adjunct to social reinforcement learningprocedures may help tag social stimuli with incentive valueby stimulating social brain and reward circuitries, and thuspotentiating social reward-based ‘wanting’ [177]. We elab-orate on this idea below.
DiscussionThe fundamental aim of this paper was to present afine-grained analysis of reward responsiveness in ASDembedded in the ‘wanting’/’liking’ framework [7,8,178].The evaluation across three converging sets of neurobio-logical data, including functional neuroimaging responses,electrophysiological recordings, and neurochemical mea-sures, revealed disrupted social reward ‘wanting’ capacitiesin individuals with ASD, most likely caused by dysfunctionof the dopaminergic–oxytocinergic ‘wanting’ circuitry,

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 13 of 20http://www.jneurodevdisorders.com/content/4/1/10
including the VS, amygdala, and ventromedial prefrontalcortex. This is in line with predictions derived fromcurrent (and forthcoming) diagnostic criteria concerningthe core social phenotype of ASD, which emphasize diffi-culties with spontaneous self-initiated seeking of socialencounters [1]. Reduced social–motivational drive andinterest has also been found in infants at genetic risk forASD, who are later diagnosed with the disorder [179-181].By contrast, empirical evidence for compromised reward‘liking’, including social reward, is inconclusive, and at thispoint, not strongly supported by data on hand [54]. How-ever, the literature is still very new, with few studies, eachof which varies in what could be important details of theirmethodology. Hence, it would be premature to try to drawfirm conclusions. Much more research is needed to eluci-date the nuances (for example, developmental trajectories,heterogeneity) of reward ‘wanting’ versus ‘liking’ in ASD.Moreover, what still needs to be determined empirically isthe extent to which a deficient dopaminergic–oxytocinergic‘wanting’ circuitry in fact affects motivational actions, socialfunctioning and development in affected individuals.
Social motivation theory of ASDIt should be acknowledged that disrupted social engage-ment certainly falls short of explaining the full picture ofthe ASD phenotype, including non-social weaknessesand strengths [2]. However, on the basis of the evidencesummarized in this paper and by others [2,40,41,54,56],it seems to be crucial to elucidate the brain–behaviorunderpinnings of aberrant social motivation, a core deficitin ASD, and its diversity among affected individuals. Suchknowledge should advance our understanding of the etio-logical and phenotypic complexities of the autismspectrum, but may also lead to an understanding of theunique risk and protective factors that can be specificallytargeted by intervention and prevention researchers [182].This will help create tailored treatment programs that canoptimize functional outcome and, thus positively influencethe developmental course of an affected individual or anindividual with a genetic risk for the disorder.By integrating behavioral observations and biological
findings, the social motivation theory of ASD posits thatASD can be construed as an extreme case of reduced socialinterest. This reduction fundamentally alters how indivi-duals with ASD attend to and interact with the world,depriving them of crucial social perceptual and social cogni-tive learning opportunities [2,4,40,41,54,183]). The theoryassumes that the social motivation impairment is attribut-able, at least partially, to dysfunction of the dopaminergic–oxytocinergic vmPFC–VS–amygdala brain network [2,40].Consistent with the expression of the core social phenotype[1] and in line with evidence reviewed in this paper, it ismost likely that the lack of social-seeking tendencies in indi-viduals with ASD is caused by an inability of the ‘wanting’
circuit to activate motivational behaviors, particularly in so-cial contexts. We extend this idea by hypothesizing thatdiminished activation associated with social ‘wanting’ mayadditionally be affected by exaggerated brain receptivity fornon-social objects of high autism salience [60,72,184]. Suchcircumscribed stimuli may indeed have greater than normalincentive valence for individuals with ASD (for yet unclearreasons), and thus potentially further absorb resourcestypically dedicated to social interests and attention [184].An alternative, but not mutually exclusive explanation
is that social anxiety, as opposed to diminished socialmotivation, contributes to social avoidance behaviors inASD [185]. The unpredictable nature inherent in socialencounters might be particularly challenging for indivi-duals with ASD [186], and could promote symptoms ofanxiety and withdrawal. In fact, unpredictability hasrecently been reported to elicit anxiety-like behavior inhumans and mice, reflected in amygdala involvement atthe brain level [70,187]. Further inquiries are clearlyneeded to clarify the extent to which social anxiety, rela-tive to low social motivation, is implicated in the coresocial phenotype of ASD.
Implications for treatmentA weak social ‘wanting’ circuitry suggests that particularlystrong social cues, in combination with other strategies toboost attention and engagement [2], might be necessaryfor individuals with ASD to help them establish motiv-ational salience and initiate desired behaviors [4,42]. Theinitial behavioral modification programs attempted tocreate responsiveness to social stimuli through operant con-ditioning using already powerful reinforcers (for example,food [43,188,189]), but this approach only showed limitedgeneralization effects to daily social function [42]. Laterprograms focusing on the functional (that is, contextual)analysis of problem behaviors were more successful inaddressing core deficits [3,5,6,32,42,190-196]. Not surpris-ingly, diminished motivational tendencies, in particularreduced self-initiated social encounters, have been identifiedas a pivotal area of intervention in ASD [42,197]. The litera-ture reviewed in this paper clearly supports this approachby highlighting that impaired social motivation is mostlikely caused by functional disruptions in the ‘wanting’circuitry.A number of intervention-related factors that promote
successful treatment outcome in ASD, in terms of socialand cognitive gains, have been defined (for example, ini-tiation of intervention before the age of 4 years, intensedelivery of h more than 20 hours/week for at least 2 years,incorporation of reinforcement principles; [182]). How-ever, the percentage of affected children who actuallyprofit from behavioral treatment, let alone reach optimaloutcome (recovery), differs widely between studies, rangingfrom 3% to 50% [4]. Most recently, child characteristics that

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 14 of 20http://www.jneurodevdisorders.com/content/4/1/10
are predictive of response to intervention have beendescribed. Besides intellectual and language abilities, severalstudies suggest that individual differences in the degree ofsocial motivation tendency are associated with treatmentefficacy [182]. Young children with ASD who displaystronger social approach (‘wanting’) and fewer avoidancebehaviors at treatment onset are more responsive to earlyintensive behavioral interventions than are passive andavoidant children [198-202]. It seems that children withgreater inherent social interest engage more actively andconstructively in the intervention procedures, whichresults in greater benefits. However, Koegel and colleagues[198] found that children with few social-seeking attemptsand initially poor treatment outcome were able to learnsocial self-initiations (for example, seeking adults for helpand attention), which then led to favorable interventioneffects (for example, having best friends, going to birthdayparties and sleepovers, talking to friends on the phone).Similar findings were reported by Kasari et al. [203]. Takentogether, impaired social motivation, a core deficit withconsiderable variation among individuals with ASD, ismalleable, and its successful treatment contributes to betterfunctional outcome.If our conclusion about a biobehavioral imbalance of
diminished social ‘wanting’ and excessive seeking of ASD-specific stimuli is correct, it argues in favor of capitalizingon the latter to improve the former. This idea is not new,as there have been several small-scale behavioral interven-tion studies reporting that the use of child-preferredobjects and activities to promote social initiations indeedincreases this type of behavior in ASD [42,204-206].Because many children with ASD show circumscribedinterests in mechanical systems [207], we foresee that newtechnologies, including computers (for example, videogames), internet platforms, or robots, also have the po-tential, if used thoughtfully, to become therapeuticallymeaningful [208,209].Moreover, given the possible involvement of the
dopaminergic–oxytocinergic circuitry in social motivationdeficits, oxytocin pharmacotherapy seems to be a promisingtreatment approach for ASD [120]. Intriguingly, animalmodels show that oxytocin can exert therapeutic effects viabinding to the vasopressin receptor V1a in the absence offunctional oxytocin receptors [210]. Therefore, adminis-tering oxytocin (for example, in the form of a nasalspray), or other substances that enhance central oxytocinturnover might be effective in ASD even in the presence ofa disrupted oxytocin system [164]. However, most recentliterature reviews conclude that oxytocin pharmacotherapyalone will probably have only limited long-term beneficialeffects on pro-social functioning [120,149,152,164]. Com-bining oxytocin with a structured social-skills trainingregimen, as part of ABA [42] or computerized gaming, hasthe potential to be a more effective treatment for social
motivation impairments and other skill deficits in ASD[177,211]. Ultimately, it is hoped that such combinationtreatments will result in optimal outcome for a largerpercentage of individuals with ASD than traditionalbehavior-only approaches.
Obstacles and recommendations for future researchOne significant obstacle in the field concerns the tremen-dous phenotypic heterogeneity of ASD, with important con-sequences for intervention outcome. There is shockinglylittle research on that topic to date. Besides pre-treatmentvariables such as the degree of social motivation capacities,other subject characteristics have been described that canpotentially impair reward sensitivity, and thus may con-tribute to treatment failure in ASD. For instance, co-mor-bid traits, such as depression, anxiety, or inattention/hyperactivity, are often associated with ASD [212], and areknown to affect general reward processing [213,214] andintervention response [215]. Moreover, research indicatesthat sleep deficit, a problem commonly exhibited byindividuals with ASD [216], alters reward receptivity,particularly to social rewards [217-219]. Lastly, individualdifferences in temperament and achievement/intrinsic mo-tivation tendencies have been documented in ASD[220,221], and can result in differential responsiveness toreward [222,223]. Taken together, these findingsemphasize the need for rigorous assessments and optimalmanagement of such factors to increase the likelihood ofoptimal outcome. However, laboratory-based measuresthat accurately quantify reward responsiveness and mo-tivational tendencies in ASD are lacking, and have yet tobe developed. Additionally, a goal for future research isto identify neurobiological ‘traits’ for example, [224] andgenetic moderators [225,226] that are predictive of treat-ment response. This will allow determination of whichtreatment option works well for a specific subset of indi-viduals with ASD but not for others.A second obstacle relates to methodological shortcomings
in experimental research on reward responsiveness. For in-stance, there is a lack of research into biological rewardssuch as food items, despite these being a most commonlyused reinforcer during intervention. Furthermore, physio-logical or drive states have been neglected, although inter-vention researchers have shown that individuals with ASDrespond at higher rates to social rewards under conditionsof social deprivation than during social satiation, for ex-ample [227]. Lastly, many reward stimuli used in experi-mental tasks lack ecological validity. For instance, staticimages of smiling people and coins have been used as socialand monetary rewards respectively [61,62,92]. Taken to-gether, the field needs an innovative line of experimentalresearch that systematically assesses responsiveness todifferent types of treatment-relevant reinforcers underdifferent physiological states at both the behavioral and

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 15 of 20http://www.jneurodevdisorders.com/content/4/1/10
the brain level. In this context, more ecologically validstimulus sets and experimental paradigms are necessary tofully understand the extent to which there is any domainspecificity to the reward dysfunction in ASD, which wouldbe most consistent with the core autism phenotype. Ultim-ately, enhanced characterization of these processes willcontribute to our understanding of the biobehavioral het-erogeneity of ASD and allow for the development ofbetter, more personalized treatments.
ConclusionThe intent of this review was to spark interest in thispromising area of research and to move discussion of so-cial motivation and reward-based learning more into themainstream of the autism research community. Giventhe prominent role that behavioral interventions play inthe lives of families affected by ASD, and that theseinterventions can be ineffective in a large percentage ofcases, its seems imperative that new research agendas in-clude the study of reward mechanisms, supported byefforts of both cognitive science and cognitive neuroscience.Firm conclusions about the relative importance of ‘wanting’and ‘liking’ components of reward in ASD are not yet pos-sible, owing to the paucity of studies. However, the datapublished to date indicate the importance of social motiv-ation (‘wanting’) and of the forces that propel social strivingas crucial to understanding and treating autism. We expectthat the next decade of systematic research will elucidatewith greater detail the basis of these deficits, and that thisknowledge will be translated into more effective treatments.
AbbreviationsABA: Applied behavior analysis; ACC: Anterior cingulate cortex; ADI-R: Autismdiagnostic interview-revised; ADOS-G: Autism Diagnostic ObservationSchedule-Generic; ASD: Autism Spectrum Disorder; BOLD: Blood oxygenlevel-dependent; CSF: Cerebrospinal fluid; CS: Conditioned stimulus;DTI: Diffusion tensor imaging; EEG: Electroencephalography; ERP: Event-related potential; fMRI: Functional magnetic resonance imaging;FRN: Feedback-related negativity; LC-NE: Locus coeruleus norepinephrine;NAcc: Nucleus accumbens; OFC: Orbitofrontal cortex; PET: Positron emissiontomography; PDD-NOS: Pervasive developmental disorder not otherwisespecified; SPECT: Single photon emission computed tomography;SN: Substantia nigra; TDC: Typically developing children/controls;UCS: Unconditioned stimulus; vmPFC: Ventromedial prefrontal cortex;VS: Ventral striatum; VTA: Ventral tegmental area.
Competing interestsThe authors declare that they have no competing interests.
AcknowledgmentsThis work was supported by the National Institute of Health NIMHR01MH073084 (RTS), by the Robert Wood Johnson Foundation (number66727 to RTS, and GK); by the Pennsylvania Department of Health SAP(numbers 4100042728 to RTS and CC, and 4100047863 to RTS), and by aNational Science Foundation Graduate Fellowship (to VT). We would like tothank Judith Miller, Benjamin Yerys, Jim Connell and Katja Spreckelmeyer forfruitful discussions on several ideas presented in this paper. We are alsograteful to the two anonymous reviewers for their helpful comments on aprevious version of the manuscript.
Authors’ contributionsGK drafted the manuscript; GK, CC and RTS contributed to the theoreticalapproach presented in the manuscript; and VT prepared the illustrations. Allauthors contributed to writing the manuscript. All authors read andapproved the final manuscript.
Received: 6 March 2012 Accepted: 25 April 2012Published: 17 May 2012
References1. Association AP: Diagnostic and Statistical Manual of Mental Disorders DSM-IV-
TR Fourth Edition. 4th edition. Washington: American Psychiatric Association;2000.
2. Chevallier C, Kohls G, Troiani V, Brodkin ES, Schultz RT: The socialmotivation theory of autism. Trends Cogn Sci 2012, 16:231–239.
3. Virués-Ortega J: Applied behavior analytic intervention for autism in earlychildhood: meta-analysis, meta-regression and dose–response meta-analysis of multiple outcomes. Clin Psychol Rev 2010, 30:387–399.
4. Helt M, Kelley E, Kinsbourne M, Pandey J, Boorstein H, Herbert M, Fein D:Can children with autism recover? If so, How? Neuropsychol Rev 2008,18:339–366.
5. Vismara LA, Rogers SJ: Behavioral treatments in autism spectrum disorder:what do we know?. Annu Rev Clin Psychol 2010, 6:447–468.
6. Warren Z, McPheeters ML, Sathe N, Foss-Feig JH, Glasser A, Veenstra-VanderWeele J: A systematic review of early intensive intervention forautism spectrum disorders. Pediatrics 2011, 127:e1303–e1311.
7. Berridge KC, Robinson TE, Aldridge JW: Dissecting components of reward:“liking”, “wanting”, and learning. Curr Opin Pharmacol 2009, 9:65–73.
8. Berridge KC, Robinson TE: Parsing Reward. Trends Neurosci 2003, 26:507–513.9. Haber SN, Knutson B: The reward circuit: linking primate anatomy and
human imaging. Neuropsychopharmacology 2010, 35:4–26.10. Sesack SR, Grace AA: Cortico-Basal Ganglia reward network: microcircuitry.
Neuropsychopharmacology 2010, 35:27–47.11. Camara E, Rodriguez-Fornells A, Münte TF: Functional connectivity of
reward processing in the brain. Front Hum Neurosci 2008, 2:19.12. Schultz W: Multiple dopamine functions at different time courses. Annu
Rev Neurosci 2007, 30:259–288.13. Schultz W: Predictive reward signal of dopamine neurons. J Neurophysiol
1998, 80:1–27.14. Robinson DL, Zitzman DL, Williams SK: Mesolimbic dopamine transients in
motivated behaviors: focus on maternal behavior. Front. Psychiatry 2011, 2:23.15. Berridge KC, Kringelbach ML: Building a neuroscience of pleasure and
well-being. Psychology of Well-Being. Theory, Research and Practice 2011, 1:3.16. van Hell H, Jager G, Bossong M, Brouwer A, Jansma J, Zuurman L, van
Gerven J, Kahn R, Ramsey N: Involvement of the endocannabinoid systemin reward processing in the human brain. Psychopharmacology 2012,219:981–990.
17. O’Doherty JP: Reward representations and reward-related learning in thehuman brain: insights from neuroimaging. Curr Opin Neurobiol 2004,14:769–776.
18. Knutson B, Taylor J, Kaufman M, Peterson R, Glover G: Distributed neuralrepresentation of expected value. J Neurosci 2005, 25:4806–4812.
19. Clithero JA, Reeck C, Carter RM, Smith DV, Huettel SA: Nucleus accumbensmediates relative motivation for rewards in the absence of choice.Neuroscience: Frontiers in Human 2011, 5:2011.
20. Spreckelmeyer KN, Krach S, Kohls G, Rademacher L, Irmak A, Konrad K,Kircher T, Gründer G: Anticipation of monetary and social rewarddifferently activates mesolimbic brain structures in men and women. SocCogn Affect Neurosci 2009, 4:158–165.
21. Grabenhorst F, Rolls ET: Value, pleasure and choice in the ventralprefrontal cortex. Trends Cogn Sci 2011, 15:56–67.
22. Knutson B, Adams CM, Fong GW, Hommer D: Anticipation of increasingmonetary reward selectively recruits nucleus accumbens. J Neurosci 2001,21:RC159.
23. Knutson B, Westdorp A, Kaiser E, Hommer D: FMRI visualization of brainactivity during a monetary incentive delay task. Neuroimage 2000,12:20–27.
24. Rademacher L, Krach S, Kohls G, Irmak A, Gründer G, Spreckelmeyer KN:Dissociation of neural networks for anticipation and consumption ofmonetary and social rewards. Neuroimage 2010, 49:3276–3285.

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 16 of 20http://www.jneurodevdisorders.com/content/4/1/10
25. Kringelbach ML, O’Doherty J, Rolls ET, Andrews C: Activation of the humanorbitofrontal cortex to a liquid food stimulus is correlated with itssubjective pleasantness. Cereb Cortex 2003, 13:1064–1071.
26. O’Doherty J, Rolls ET, Francis S, Bowtell R, McGlone F, Kobal G, Renner B,Ahne G: Sensory-specific satiety-related olfactory activation of the humanorbitofrontal cortex. Neuroreport 2000, 11:399–403.
27. Kringelbach ML, Rolls ET: The functional neuroanatomy of the humanorbitofrontal cortex: evidence from neuroimaging and neuropsychology.Prog Neurobiol 2004, 72:341–372.
28. Sescousse G, Redouté J, Dreher J-C: The architecture of reward value codingin the human orbitofrontal cortex. J Neurosci 2010, 30:13095–13104.
29. Smith DV, Hayden BY, Truong T-K, Song AW, Platt ML, Huettel SA: Distinctvalue signals in anterior and posterior ventromedial prefrontal cortex.J Neurosci 2010, 30:2490–2495.
30. Kohls G, Schulte-Rüther M, Nehrkorn B, Müller K, Fink GR, Kamp-Becker I,Herpertz-Dahlmann B, Schultz RT, Konrad K: Reward System Dysfunction inAutism Spectrum Disorders. Soc Cogn Affect Neurosci 2012, in press.
31. Liu X, Hairston J, Schrier M, Fan J: Common and distinct networks underlyingreward valence and processing stages: a meta-analysis of functionalneuroimaging studies. Neurosci Biobehav Rev 2011, 35:1219–1236.
32. Matson JL, Benavidez DA, Compton LS, Paclawskyj T, Baglio C: Behavioraltreatment of autistic persons: a review of research from 1980 to thepresent. Res Dev Disabil 1996, 17:433–465.
33. Northup J, Vollmer TR, Serrett K: Publication trends in 25 years of thejournal of applied behavior analysis. J Appl Behav Anal 1993, 26:527–537.
34. Dawson G, Osterling J, Rinaldi J, Carver L, McPartland J: Brief report:recognition memory and stimulus-reward associations: indirect supportfor the role of ventromedial prefrontal dysfunction in autism. J AutismDev Disord 2001, 31:337–341.
35. Dawson G, Meltzoff AN, Osterling J, Rinaldi J: Neuropsychologicalcorrelates of early symptoms of autism. Child Dev 1998, 69:1276–1285.
36. Munson J, Faja S, Meltzoff A, Abbott R, Dawson G: Neurocognitivepredictors of social and communicative developmental trajectories inpreschoolers with autism spectrum disorders. J Int Neuropsychol Soc 2008,14:956–966.
37. Zalla T, Sav A-M, Leboyer M: Stimulus-reward association and reversallearning in individuals with asperger syndrome. Research in AutismSpectrum Disorders 2009, 3:913–923.
38. Solomon M, Smith AC, Frank MJ, Ly S, Carter CS: Probabilisticreinforcement learning in adults with autism spectrum disorders. AutismRes 2011, 4:109–120.
39. Solomon M, Frank MJ, Smith AC, Ly S, Carter CS: Transitive inference inadults with autism spectrum disorders. Cogn Affect Behav Neurosci 2011,11:437–449.
40. Dawson G, Webb SJ, Wijsman E, Schellenberg G, Estes A, Munson J, Faja S:Neurocognitive and electrophysiological evidence of altered faceprocessing in parents of children with autism: implications for a modelof abnormal development of social brain circuitry in autism. DevPsychopathol 2005, 17:679–697.
41. Schultz RT: Developmental deficits in social perception in autism: therole of the amygdala and fusiform face area. Int J Dev Neurosci 2005,23:125–141.
42. Koegel RL, Koegel LK, McNerney EK: Pivotal areas in intervention forautism. J Clin Child Psychol 2001, 30:19–32.
43. Margolies PJ: Behavioral approaches to the treatment of early infantileautism: a review. Psychol Bull 1977, 84:249–264.
44. Garretson HB, Fein D, Waterhouse L: Sustained attention in children withautism. J Autism Dev Disord 1990, 20:101–114.
45. Geurts HM, Luman M, van Meel CS: What’s in a game: the effect of socialmotivation on interference control in boys with ADHD and autismspectrum disorders. J Child Psychol Psychiatry 2008, 49:848–857.
46. Freitag G: An experimental study of the social responsiveness of childrenwith autistic behaviors. J Exp Child Psychol 1970, 9:436–453.
47. Demurie E, Roeyers H, Baeyens D, Sonugan Barke E: Common alterations insensitivity to type but not amount of reward in ADHD and autismspectrum disorders. Journal of Child Psychology and Psychiatry 2011,52:1164–1173.
48. Der-Avakian A, Markou A: The neurobiology of anhedonia and otherreward-related deficits. Trends Neurosci 2012, 35:68–77.
49. Foussias G, Remington G: Negative symptoms in schizophrenia: avolitionand occam’s razor. Schizophr Bull 2010, 36:359–369.
50. Cohen AS, Minor KS: Emotional experience in patients with schizophreniarevisited: meta-analysis of laboratory studies. Schizophr Bull 2010, 36:143–150.
51. Dowd EC, Barch DM: Anhedonia and emotional experience inschizophrenia: neural and behavioral indicators. Biol Psychiatry 2010,67:902–911.
52. Messinger JW, Trémeau F, Antonius D, Mendelsohn E, Prudent V, StanfordAD, Malaspina D: Avolition and expressive deficits capture negativesymptom phenomenology: Implications for DSM-5 and schizophreniaresearch. Clin Psychol Rev 2011, 31:161–168.
53. Wolf DH: Anhedonia in schizophrenia. Curr Psychiatry Rep 2006, 8:322–328.54. Mundy P: Joint attention and social-emotional approach behavior in
children with autism. Dev Psychopathol 1995, 7:63–82.55. Mundy P: Annotation: the neural basis of social impairments in autism:
the role of the dorsal medial-frontal cortex and anterior cingulatesystem. J. Child Psychol. Psychiatry Allied Discip. 2003, 44:793–809.
56. Neuhaus E, Beauchaine TP, Bernier R: Neurobiological correlates of socialfunctioning in autism. Clin Psychol Rev 2010, 30:733–748.
57. Waterhouse L, Fein D, Modahl C: Neurofunctional mechanisms in autism.Psychol Rev 1996, 103:457–489.
58. Bachevalier J, Loveland KA: The orbitofrontal-amygdala circuit and self-regulation of social–emotional behavior in autism. Neurosci Biobehav Rev2006, 30:97–117.
59. Ishikawa A, Ambroggi F, Nicola SM, Fields HL: Contributions of theamygdala and medial prefrontal cortex to incentive cue responding.Neuroscience 2008, 155:573–584.
60. Dichter GS, Felder JN, Green SR, Rittenberg AM, Sasson NJ, Bodfish JW:Reward circuitry function in autism spectrum disorders. Soc Cogn AffectNeurosci 2012, 7:160–172.
61. Dichter GS, Richey JA, Rittenberg AM, Sabatino A, Bodfish JW: Rewardcircuitry function in autism during face anticipation and outcomes.J Autism Dev Disord 2012, 42:147–160.
62. Scott-Van Zeeland AA, Dapretto M, Ghahremani DG, Poldrack RA,Bookheimer SY: Reward processing in autism. Autism Res 2010, 3:53–67.
63. Schmitz N, Rubia K, van Amelsvoort T, Daly E, Smith A, Murphy DGM: Neuralcorrelates of reward in autism. Br J Psychiatry 2008, 192:19–24.
64. Vohs KD, Mead NL, Goode MR: The psychological consequences ofmoney. Science 2006, 314:1154–1156.
65. Zhou X, Vohs KD, Baumeister RF: The symbolic power of money:reminders of money alter social distress and physical pain. Psychol Sci2009, 20:700–706.
66. Warneken F, Tomasello M: Extrinsic rewards undermine altruistictendencies in 20-month-olds. Dev Psychol 2008, 44:1785–1788.
67. Mercier C, Mottron L, Belleville S: A psychosocial study on restrictedinterests in high functioning persons with pervasive developmentaldisorders. Autism 2000, 4:406–425.
68. Boyd BA, Conroy MA, Mancil GR, Nakao T, Alter PJ: Effects of circumscribedinterests on the social behaviors of children with autism spectrumdisorders. J Autism Dev Disord 2007, 37:1550–1561.
69. Charlop-Christy MH, Haymes LK: Using objects of obsession as tokenreinforcers for children with autism. J Autism Dev Disord 1998, 28:189–198.
70. Adolphs R: What does the amygdala contribute to social cognition?. AnnN Y Acad Sci 2010, 1191:42–61.
71. Murray EA: The amygdala, reward and emotion. Trends Cogn Sci 2007,11:489–497.
72. Grelotti DJ, Klin AJ, Gauthier I, Skudlarski P, Cohen DJ, Gore JC, Volkmar FR,Schultz RT: fMRI activation of the fusiform gyrus and amygdala tocartoon characters but not to faces in a boy with autism.Neuropsychologia 2005, 43:373–385.
73. Grelotti DJ, Gauthier I, Schultz RT: Social interest and the development ofcortical face specialization: what autism teaches us about faceprocessing. Dev Psychobiol 2002, 40:213–225.
74. Tottenham N, Sheridan MA: A review of adversity, the amygdala and thehippocampus: a consideration of developmental timing. Front HumNeurosci 2010, 3:68.
75. Schumann CM, Bauman MD, Amaral DG: Abnormal structure or function ofthe amygdala is a common component of neurodevelopmentaldisorders. Neuropsychologia 2011, 49:745–759.
76. Kalivas PW: The neural basis of addiction: a pathology of motivation andchoice. Am J Psychiatry 2005, 162:1403–1413.
77. Volkow ND, Wang G-J, Fowler JS, Tomasi D: Addiction circuitry in thehuman brain. Annu Rev Pharmacol Toxicol 2012, 52:321–336.

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 17 of 20http://www.jneurodevdisorders.com/content/4/1/10
78. Assaf M, Jagannathan K, Calhoun VD, Miller L, Stevens MC, Sahl R, O’BoyleJG, Schultz RT, Pearlson GD: Abnormal functional connectivity of defaultmode sub-networks in autism spectrum disorder patients. Neuroimage2010, 53:247–256.
79. Di Martino A, Kelly C, Grzadzinski R, Zuo X-N, Mennes M, Mairena MA, LordC, Castellanos FX, Milham MP: Aberrant striatal functional connectivity inchildren with autism. Biol Psychiatry 2011, 69:847–856.
80. Lai M-C, Lombardo MV, Chakrabarti B, Sadek SA, Pasco G, Wheelwright SJ,Bullmore ET, Baron-Cohen S, Suckling J: A shift to randomness of brainoscillations in people with autism. Biol Psychiatry 2010, 68:1092–1099.
81. Langen M, Leemans A, Johnston P, Ecker C, Daly E, Murphy CM, Dell’ AcquaF, Durston S, Murphy DGM: Fronto-striatal circuitry and inhibitory controlin autism: findings from diffusion tensor imaging tractography. Cortex2012, 48:183–193.
82. Just MA, Cherkassky VL, Keller TA, Minshew NJ: Cortical activation andsynchronization during sentence comprehension in high-functioningautism: evidence of underconnectivity. Brain: A Journal of Neurology 2004,127:1811–1821.
83. Schipul SE, Keller TA, Just MA: Inter-regional brain communication and itsdisturbance in autism. Front Syst Neurosci 2011, 5:10.
84. Geschwind DH, Levitt P: Autism spectrum disorders: developmentaldisconnection syndromes. Curr Opin Neurobiol 2007, 17:103–111.
85. Betancur C, Sakurai T, Buxbaum JD: The emerging role of synaptic cell-adhesionpathways in the pathogenesis of autism spectrum disorders. Trends Neurosci2009, 32:402–412.
86. Knutson B, Greer SM: Anticipatory affect: neural correlates andconsequences for choice. Phil. Trans. R. Soc. B 2008, 363:3771–3786.
87. Banaschewski T, Brandeis D: Annotation: what electrical brain activity tells usabout brain function that other techniques cannot tell us – a child psychiatricperspective. Journal of Child Psychology and Psychiatry 2007, 48:415–435.
88. Holroyd CB, Coles MGH: The neural basis of human error processing:reinforcement learning, dopamine, and the error-related negativity.Psychol Rev 2002, 109:679–709.
89. Nieuwenhuis S, Aston-Jones G, Cohen JD: Decision making, the p3, and thelocus coeruleus–norepinephrine system. Psychol Bull 2005, 131:510–532.
90. Wu Y, Zhou X: The P300 and reward valence, magnitude, and expectancyin outcome evaluation. Brain Res 2009, 1286:114–122.
91. Yeung N, Holroyd CB, Cohen JD: ERP correlates of feedback and rewardprocessing in the presence and absence of response choice. Cereb Cortex2005, 15:535–544.
92. Kohls G, Peltzer J, Schulte-Rüther M, Kamp-Becker I, Remschmidt H,Herpertz-Dahlmann B, Konrad K: Atypical brain responses to reward cuesin autism as revealed by event-related potentials. J Autism Dev Disord2011, 41:1523–1533.
93. Pfabigan DM, Bauer H, Lamm C: All about the money – externalperformance monitoring is affected by monetary, but not by sociallyconveyed feedback cues in more antisocial individuals. Front HumNeurosci 2011, 5:100.
94. Lange S, Leue A, Beauducel A: Behavioral approach and rewardprocessing: results on feedback-related negativity and P3 component.Biol Psychol 2012, 89:416–425.
95. Van den Berg I, Franken IHA, Muris P: Individual differences in sensitivity toreward. Journal of Psychophysiology 2011, 25:81–86.
96. Carlson JM, Foti D, Mujica-Parodi LR, Harmon-Jones E, Hajcak G: Ventral striataland medial prefrontal bold activation is correlated with reward-relatedelectrocortical activity: a combined erp and fmri study. Neuroimage 2011,57:1608–1616.
97. Foti D, Weinberg A, Dien J, Hajcak G: Event-related potential activity in thebasal ganglia differentiates rewards from nonrewards: temporospatialprincipal components analysis and source localization of the feedbacknegativity. Hum Brain Mapp 2011, 32:2207–2216.
98. Martin LE, Potts GF, Burton PC, Montague PR: Electrophysiological andhemodynamic responses to reward prediction violation. NeuroReport: ForRapid Communication of Neuroscience Research 2009, 20:1140–1143.
99. Cohen MX, Cavanagh JF, Slagter HA: Event-related potential activity in thebasal ganglia differentiates rewards from nonrewards: temporospatialprincipal components analysis and source localization of the feedbacknegativity: commentary. Hum Brain Mapp 2011, 32:2270–2271.
100. Jeste SS, Nelson CA: Event related potentials in the understanding ofautism spectrum disorders: an analytical review. J Autism Dev Disord 2008,39:495–510.
101. Groen Y, Wijers AA, Mulder LJM, Waggeveld B, Minderaa RB, Althaus M:Error and feedback processing in children with ADHD and children withAutistic Spectrum Disorder: an EEG event-related potential study. ClinNeurophysiol 2008, 119:2476–2493.
102. Brunia CHM, Hackley SA, van Boxtel GJM, Kotani Y, Ohgami Y: Waiting toperceive: reward or punishment? Clin Neurophysiol 2011, 122:858–868.
103. Larson MJ, South M, Krauskopf E, Clawson A, Crowley MJ: Feedback andreward processing in high-functioning autism. Psychiatry Res 2011,187:198–203.
104. Schultz W, Apicella P, Scarnati E, Ljungberg T: Neuronal activity in monkeyventral striatum related to the expectation of reward. J Neurosci 1992,12:4595–4610.
105. Hoeksma MR, Kemner C, Verbaten MN, van Engeland H: Processingcapacity in children and adolescents with pervasive developmentaldisorders. J Autism Dev Disord 2004, 34:341–354.
106. Fox NA: If it’s not left, it’s right: electroencephalograph asymmetry andthe development of emotion. Am Psychol 1991, 46:863–872.
107. Pizzagalli DA, Sherwood RJ, Henriques JB, Davidson RJ: Frontal brainasymmetry and reward responsiveness. A Source-Localization Study.Psychological Science 2005, 16:805–813.
108. Allen JJB, Cohen MX: Deconstructing the “resting” state: exploring thetemporal dynamics of frontal alpha asymmetry as an endophenotype fordepression. Front Hum Neurosci 2010, 4:232.
109. Tomer R, Goldstein RZ, Wang G-J, Wong C, Volkow ND: Incentivemotivation is associated with striatal dopamine asymmetry. Biol Psychol2008, 77:98–101.
110. Sutton SK, Burnette CP, Mundy PC, Meyer J, Vaughan A, Sanders C, Yale M:Resting cortical brain activity and social behavior in higher functioningchildren with autism. Journal of Child Psychology and Psychiatry 2005,46:211–222.
111. Mundy PC, Henderson HA, Inge AP, Coman DC: The modifier model ofautism and social development in higher functioning children. Research &Practice for Persons with Severe Disabilities 2007, 32:124–139.
112. Wing L, Gould J: Severe impairments of social interaction and associatedabnormalities in children: Epidemiology and classification. J Autism DevDisord 1979, 9:11–29.
113. Dawson G, Klinger LG, Panagiotides H, Lewy A, Castelloe P: Subgroups ofautistic children based on social behavior display distinct patterns ofbrain activity. J Abnorm Child Psychol 1995, 23:569–583.
114. Burnette CP, Henderson HA, Inge AP, Zahka NE, Schwartz CB, Mundy PC:Anterior EEG asymmetry and the modifier model of autism. J Autism DevDisord 2011, 41:1113–1124.
115. Kylliäinen A, Wallace S, Coutanche MN, Leppänen JM, Cusack J, Bailey AJ,Hietanen JK: Affective-motivational brain responses to direct gaze inchildren with autism spectrum disorder. Journal of Child Psychology andPsychiatry 2012, in press.
116. Kampe KKW, Frith CD, Dolan RJ, Frith U: Reward value of attractivenessand gaze. Nature 2001, 413:589–590.
117. Dalton KM, Nacewicz BM, Johnstone T, Schaefer HS, Gernsbacher MA,Goldsmith HH, Alexander AL, Davidson RJ: Gaze fixation and the neuralcircuitry of face processing in autism. Nat Neurosci 2005, 8:519–526.
118. Senju A, Johnson MH: Atypical eye contact in autism: models,mechanisms and development. Neurosci Biobehav Rev 2009, 33:1204–1214.
119. Depue RA, Morrone-Strupinsky JV: A neurobehavioral model of affiliativebonding: implications for conceptualizing a human trait of affiliation.Behav Brain Sci 2005, 28:313–395.
120. Bartz JA, Zaki J, Bolger N, Ochsner KN: Social effects of oxytocin inhumans: context and person matter. Trends Cogn Sci 2011, 15:301–309.
121. Lam KSL, Aman MG, Arnold LE: Neurochemical correlates of autisticdisorder: a review of the literature. Res Dev Disabil 2006, 27:254–289.
122. Breiter HC, Gollub RL, Weisskoff RM, Kennedy DN, Makris N, Berke JD,Goodman JM, Kantor HL, Gastfriend DR, Riorden JP, Mathew RT, Rosen BR,Hyman SE: Acute effects of cocaine on human brain activity andemotion. Neuron 1997, 19:591–611.
123. McPheeters ML, Warren Z, Sathe N, Bruzek JL, Krishnaswami S, JeromeRN, Veenstra-VanderWeele J: A systematic review of medical treatmentsfor children with autism spectrum disorders. Pediatrics 2011, 127:e1312–e1321.
124. Ernst M, Zametkin A, Matochik J, Pascualvaca D, Cohen R: Low medialprefrontal dopaminergic activity in autistic children. Lancet 1997,350:638.

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 18 of 20http://www.jneurodevdisorders.com/content/4/1/10
125. Nakamura K, Sekine Y, Ouchi Y, Tsujii M, Yoshikawa E, Futatsubashi M,Tsuchiya KJ, Sugihara G, Iwata Y, Suzuki K, Matsuzaki H, Suda S, SugiyamaT, Takei N, Mori N: Brain serotonin and dopamine transporter bindingsin adults with high-functioning autism. Arch Gen Psychiatry 2010,67:59–68.
126. Fernell E, Watanabe Y, Adolfsson I, Tani Y, Bergström M, Hartvig P, Lilja A,von Knorring AL, Gillberg C, Langstrom B: Possible effects oftetrahydrobiopterin treatment in six children with autism - clinical andpositron emission tomography data: a pilot study. Dev Med Child Neurol1997, 39:313–318.
127. Makkonen I, Riikonen R, Kuikka JT, Kokki H, Bressler JP, Marshall C, KaufmannWE: Brain derived neurotrophic factor and serotonin transporter bindingas markers of clinical response to fluoxetine therapy in children withautism. Journal of Pediatric Neurology 2011, 9:1–8.
128. Nieminen-von Wendt TS, Metsähonkala L, Kulomäki TA, Aalto S, Autti TH,Vanhala R, Bergman J, Hietala JA, von Wendt LO: Increased presynapticdopamine function in Asperger syndrome. Neuroreport 2004, 15:757–76.
129. Makkonen I, Riikonen R, Kokki H, Airaksinen MM, Kuikka JT: Serotonin anddopamine transporter binding in children with autism determined bySPECT. Dev Med Child Neurol 2008, 50:593–597.
130. Grace AA: Phasic versus tonic dopamine release and the modulation ofdopamine system responsivity: a hypothesis for the etiology ofschizophrenia. Neuroscience 1991, 41:1–24.
131. Grigson PS: Like drugs for chocolate: separate rewards modulated bycommon mechanisms? Physiol Behav 2002, 76:389–395.
132. Hettinger JA, Liu X, Schwartz CE, Michaelis RC, Holden JJA: A DRD1haplotype is associated with risk for autism spectrum disorders inmale-only affected sib-pair families. Am J Med Genet B NeuropsychiatrGenet 2008, 147B:628–636.
133. Robinson PD, Schutz CK, Macciardi F, White BN, Holden JJA: Geneticallydetermined low maternal serum dopamine beta-hydroxylase levels andthe etiology of autism spectrum disorders. Am J Med Genet 2001,100:30–36.
134. Bishop SL, Lahvis GP: The autism diagnosis in translation: shared affect inchildren and mouse models of ASD. Autism Res 2011, 4:317–335.
135. Chamberlain RS, Herman BH: A novel biochemical model linkingdysfunctions in brain melatonin, proopiomelanocortin peptides, andserotonin in autism. Biol Psychiatry 1990, 28:773–793.
136. Kalat JW: Speculations on similarities between autism and opiateaddiction. J Autism Child Schizophr 1978, 8:477–479.
137. Panksepp J: A neurochemical theory of autism. Trends Neurosci 1979,2:174–177.
138. Sahley TL, Panksepp J: Brain opioids and autism: an updated analysis ofpossible linkages. J Autism Dev Disord 1987, 17:201–216.
139. Sandman CA: Various endogenous opioids and autistic behavior: aresponse to Gillberg. J Autism Dev Disord 1992, 22:132–133.
140. Sher L: Autistic disorder and the endogenous opioid system. MedicalHypotheses 1997, 48:413–414.
141. van Ree JM, Gerrits MAFM, Vanderschuren LJMJ: Opioids, reward andaddiction: an encounter of biology, psychology, and medicine. PharmacolRev 1999, 51:341–396.
142. Trezza V, Baarendse PJJ, Vanderschuren LJMJ: The pleasures of play:pharmacological insights into social reward mechanisms. TrendsPharmacol Sci 2010, 31:463–469.
143. Machin AJ, Dunbar RIM: The brain opioid theory of social attachment: areview of the evidence. Behaviour 2011, 148:987–1025.
144. ElChaar GM, Maisch NM, Augusto LMG, Wehring HJ: Efficacy and safety ofnaltrexone use in pediatric patients with autistic disorder. AnnPharmacother 2006, 40:1086–1095.
145. Campbell A: Oxytocin and human social behavior. Pers Soc Psychol Rev2010, 14:281–295.
146. Gordon I, Martin C, Feldman R, Leckman JF: Oxytocin and socialmotivation. Developmental Cognitive Neuroscience 2011, 1:471–493.
147. Gimpl G, Fahrenholz F: The oxytocin receptor system: structure, function,and regulation. Physiol Rev 2001, 81:629–683.
148. Landgraf R, Neumann ID: Vasopressin and oxytocin release within thebrain: a dynamic concept of multiple and variable modes ofneuropeptide communication. Front Neuroendocrinol 2004, 25:150–176.
149. Striepens N, Kendrick KM, Maier W, Hurlemann R: Prosocial effects ofoxytocin and clinical evidence for its therapeutic potential. FrontNeuroendocrinol 2011, 32:426–450.
150. MacDonald K, MacDonald TM: The peptide that binds: a systematic reviewof oxycotin and its prosocial effects in humans. Harv Rev Psychiatry 2010,18:1–21.
151. Insel TR: The challenge of translation in social neuroscience: a review ofoxytocin, vasopressin, and affiliative behavior. Neuron 2010, 65:768–779.
152. Meyer-Lindenberg A, Domes G, Kirsch P, Heinrichs M: Oxytocin andvasopressin in the human brain: social neuropeptides for translationalmedicine. Nat Rev Neurosci 2011, 12:524–538.
153. Kovàcs GL, Sarnyai Z, Babarczi E, Szabó G, Telegdy G: The role ofoxytocin-dopamine interactions in cocaine-induced locomotorhyperactivity. Neuropharmacology 1990, 29:365–368.
154. Pfister HP, Muir JL: Influence of exogeneously administered oxytocin oncentral noradrenaline, dopamine and serotonin levels followingpsychological stress in nulliparous female rats (rattus norvegicus). Int JNeurosci 1989, 45:221–229.
155. Csiffáry A, Ruttner Z, Tóth Z, Palkovits M: Oxytocin nerve fibers innervatebeta-endorphin neurons in the arcuate nucleus of the rat hypothalamus.Neuroendocrinology 1992, 56:429–435.
156. Strathearn L, Fonagy P, Amico J, Montague PR: Adult attachment predictsmaternal brain and oxytocin response to infant Cues.Neuropsychopharmacology 2009, 34:2655–2666.
157. Baumgartner T, Heinrichs M, Vonlanthen A, Fischbacher U, Fehr E: Oxytocinshapes the neural circuitry of trust and trust adaptation in humans.Neuron 2008, 58:639–650.
158. Domes G, Heinrichs M, Gläscher J, Büchel C, Braus DF, Herpertz SC: Oxytocinattenuates amygdala responses to emotional faces regardless of valence.Biol Psychiatry 2007, 62:1187–1190.
159. Gamer M, Zurowski B, Büchel C: Different amygdala subregions mediatevalence-related and attentional effects of oxytocin in humans. PNAS 2010,107:9400–9405.
160. Kirsch P, Esslinger C, Chen Q, Mier D, Lis S, Siddhanti S, Gruppe H, Mattay VS,Gallhofer B, Meyer-Lindenberg A: Oxytocin modulates neural circuitry forsocial cognition and fear in humans. J Neurosci 2005, 25:11489–11493.
161. Petrovic P, Kalisch R, Singer T, Dolan RJ: Oxytocin attenuates affectiveevaluations of conditioned faces and amygdala activity. J Neurosci 2008,28:6607–6615.
162. Riem MME, Bakermans-Kranenburg MJ, Pieper S, Tops M, Boksem MAS,Vermeiren RRJM, van IJzendoorn MH, Rombouts SARB: Oxytocin modulatesamygdala, insula, and inferior frontal gyrus responses to infant crying: arandomized controlled trial. Biol Psychiatry 2011, 70:291–297.
163. Rilling JK, DeMarco AC, Hackett PD, Thompson R, Ditzen B, Patel R, PagnoniG: Effects of intranasal oxytocin and vasopressin on cooperative behaviorand associated brain activity in men. Psychoneuroendocrinology 2012,37:447–461.
164. Modi ME, Young LJ: The oxytocin system in drug discovery for autism:animal models and novel therapeutic strategies. Horm Behav 2012,61:340–350.
165. Insel TR, O’Brien DJ, Leckman JF: Oxytocin, vasopressin, and autism: isthere a connection?. Biol Psychiatry 1999, 45:145–157.
166. Andari E, Duhamel J-R, Zalla T, Herbrecht E, Leboyer M, Sirigu A: Promotingsocial behavior with oxytocin in high-functioning autism spectrumdisorders. PNAS 2010, 107:4389–4394.
167. Modahl C, Green L, Fein D, Morris M, Waterhouse L, Feinstein C, LevinH: Plasma oxytocin levels in autistic children. Biol Psychiatry 1998,43:270–277.
168. Green L, Fein D, Modahl C, Feinstein C, Waterhouse L, Morris M: Oxytocinand autistic disorder: alterations in peptide forms. Biol Psychiatry 2001,50:609–613.
169. Jansen LMC, Gispen-de Wied CC, Wiegant VM, Westenberg HGM, Lahuis BE,Engeland H: Autonomic and neuroendocrine responses to a psychosocialstressor in adults with autistic spectrum disorder. J Autism Dev Disord2006, 36:891–899.
170. Campbell DB, Datta D, Jones ST, Batey Lee E, Sutcliffe JS, Hammock EAD,Levitt P: Association of oxytocin receptor (OXTR) gene variants withmultiple phenotype domains of autism spectrum disorder. Journal ofNeurodevelopmental Disorders 2011, 1:12.
171. Gregory S, Connelly J, Towers A, Johnson J, Biscocho D, Markunas C, LintasC, Abramson R, Wright H, Ellis P: others: Genomic and epigenetic evidencefor oxytocin receptor deficiency in autism. BMC Med 2009, 7:62.
172. Hollander E, Novotny S, Hanratty M, Yaffe R, DeCaria CM, Aronowitz BR,Mosovich S: Oxytocin infusion reduces repetitive behaviors in adults

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 19 of 20http://www.jneurodevdisorders.com/content/4/1/10
with autistic and Asperger’s disorders. Neuropsychopharmacology 2003,28:193–198.
173. Guastella AJ, Einfeld SL, Gray KM, Rinehart NJ, Tonge BJ, Lambert TJ, HickieIB: Intranasal oxytocin improves emotion recognition for youth withautism spectrum disorders. Biol Psychiatry 2010, 67:692–694.
174. Hollander E, Bartz J, Chaplin W, Phillips A, Sumner J, Soorya L, Anagnostou E,Wasserman S: Oxytocin increases retention of social cognition in autism.Biol Psychiatry 2007, 61:498–503.
175. Skuse DH, Gallagher L: Dopaminergic-neuropeptide interactions in thesocial brain. Trends Cogn Sci 2009, 13:27–35.
176. Melis MR, Melis T, Cocco C, Succu S, Sanna F, Pillolla G, Boi A, Ferri G,Argiolas A: Oxytocin injected into the ventral tegmental area inducespenile erection and increases extracellular dopamine in the nucleusaccumbens and paraventricular nucleus of the hypothalamus of malerats. Eur J Neurosci 2007, 26:1026–1035.
177. Hurlemann R, Patin A, Onur OA, Cohen MX, Baumgartner T, Metzler S,Dziobek I, Gallinat J, Wagner M, Maier W, Kendrick KM: Oxytocin enhancesamygdala-dependent, socially reinforced learning and emotionalempathy in humans. J Neurosci 2010, 30:4999–5007.
178. Robinson TE, Berridge KC: The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Res Rev 1993, 18:247–291.
179. Maestro S, Muratori F, Cavallaro MC, Pei F, Stern D, Golse B, Palacio-Espasa F:Attentional skills during the first 6 months of age in autism spectrumdisorder. J Am Acad Child Adolesc Psychiatry 2002, 41:1239–1245.
180. Zwaigenbaum L, Bryson S, Rogers T, Roberts W, Brian J, Szatmari P:Behavioral manifestations of autism in the first year of life. Int J DevNeurosci 2005, 23:143–152.
181. Bryson SE, Zwaigenbaum L, Brian J, Roberts W, Szatmari P, Rombough V,McDermott C: A prospective case series of high-risk infants whodeveloped autism. J Autism Dev Disord 2007, 37:12–24.
182. Dawson G: Early behavioral intervention, brain plasticity, and the preventionof autism spectrum disorder. Dev Psychopathol 2008, 20:775–803.
183. O’Connor K, Kirk I: Brief report: atypical social cognition and socialbehaviours in autism spectrum disorder: a different way of processingrather than an impairment. J Autism Dev Disord 2008, 38:1989–1997.
184. Sasson NJ, Turner-Brown LM, Holtzclaw TN, Lam KSL, Bodfish JW: Childrenwith autism demonstrate circumscribed attention during passive viewingof complex social and nonsocial picture arrays. Autism 2008, 1:31–42.
185. Wood JJ, Gadow KD: Exploring the nature and function of anxiety inyouth with autism spectrum disorders, exploring the nature andfunction of anxiety in youth with autism spectrum disorders. ClinicalPsychology: Science and Practice, Clinical Psychology: Science and Practice2010, 17:281–292.
186. Klin A, Lin DJ, Gorrindo P, Ramsay G, Jones W: Two-year-olds with autismorient to nonsocial contingencies rather than biological motion. Nature2009, 459:257.
187. Herry C, Bach DR, Esposito F, Di Salle F, Perrig WJ, Scheffler K, Lüthi A, SeifritzE: Processing of temporal unpredictability in human and animalamygdala. J Neurosci 2007, 27:5958–5966.
188. Lovaas OI, Freitag G, Kinder MI, Rubenstein BD, Schaeffer B, Simmons JQ:Establishment of social reinforcers in two schizophrenic children on thebasis of food. J Exp Child Psychol 1966, 4:109–125.
189. Lovaas OI, Schaeffer B, Simmons JQ: Building social behavior in autisticchildren by use of electric shock. Journal of Experimental Research inPersonality 1965, 1:99–109.
190. Kasari C, Lawton K: New directions in behavioral treatment of autismspectrum disorders. Curr Opin Neurol 2010, 23:137–143.
191. Howlin P, Magiati I, Charman T: Systematic review of early intensivebehavioral interventions for children with autism. Am J Intellect DevDisabil 2009, 114:23–41.
192. Seida JK, Ospina MB, Karkhaneh M, Hartling L, Smith V, Clark B: Systematicreviews of psychosocial interventions for autism: an umbrella review. DevMed Child Neurol 2009, 51:95–104.
193. Ospina MB, Krebs Seida J, Krebs Seida J, Clark B, Karkhaneh M, Hartling L,Tjosvold L, Vandermeer B, Smith V: Behavioural and developmentalinterventions for autism spectrum disorder: a clinical systematic review.PLoS One 2008, 3:e3755.
194. Reichow B, Wolery M: Comprehensive synthesis of early intensivebehavioral interventions for young children with autism based onthe ucla young autism project model. J Autism Dev Disord 2008,39:23–41.
195. Spreckley M, Boyd R: Efficacy of applied behavioral intervention inpreschool children with autism for improving cognitive, language, andadaptive behavior: a systematic review and meta-analysis. J Pediatr 2009,154:338–344.
196. Eldevik S, Hastings RP, Hughes JC, Jahr E, Eikeseth S, Cross S: Meta-analysisof early intensive behavioral intervention for children with autism. J ClinChild Adolesc Psychol 2009, 38:439–450.
197. Koegel RL, Mentis M: Motivation in childhood autism: can they or won’tthey?. Journal of Child Psychology and Psychiatry 1985, 26:185–191.
198. Koegel LK, Koegel RL, Shoshan Y, McNerney E: Pivotal responseintervention ii: preliminary long-term outcome data. Research and Practicefor Persons with Severe Disabilities 1999, 24:186–198.
199. Sallows GO, Graupner TD: Intensive behavioral treatment for children withautism: four-year outcome and predictors. Am J Ment Retard 2005,110:417–438.
200. Beglinger L, Smith T: Concurrent validity of social subtype and iq afterearly intensive behavioral intervention in children with autism: apreliminary investigation. J Autism Dev Disord 2005, 35:295–303.
201. Ingersoll B, Schreibman L, Stahmer A: Brief report: differential treatmentoutcomes for children with autistic spectrum disorder based on level ofpeer social avoidance. J Autism Dev Disord 2001, 31:343–349.
202. Sherer MR, Schreibman L: Individual behavioral profiles and predictors oftreatment effectiveness for children with autism. J Consult Clin Psychol2005, 73:525–538.
203. Kasari C, Freeman S, Paparella T: Joint attention and symbolic play in youngchildren with autism: a randomized controlled intervention study. Journal ofchild psychology and psychiatry and allied disciplines 2006, 47:611–620.
204. Gaylord-Ross RJ, Haring TG, Breen C, Pitts-Conway V: The training andgeneralization of social interaction skills with autistic youth. J Appl BehavAnal 1984, 17:229–247.
205. Koegel RL, Dyer K, Bell LK: The influence of child-preferred activities onautistic children’s social behavior. J Appl Behav Anal 1987, 20:243–252.
206. Vismara LA, Lyons GL: Using perseverative interests to elicit joint attentionbehaviors in young children with autism: theoretical and clinicalimplications for understanding motivation. Journal of Positive BehaviorInterventions 2007, 9:214–228.
207. Turner-Brown LM, Lam KSL, Holtzclaw TN, Dichter GS, Bodfish JW:Phenomenology and measurement of circumscribed interests in autismspectrum disorders. Autism 2011, 15:437–456.
208. Cumming TM: Using technology to create motivating social skills lessons.Intervention in School and Clinic 2010, 45:242–250.
209. Tanaka JW, Wolf JM, Klaiman C, Koenig K, Cockburn J, Herlihy L, Brown C, StahlS, Kaiser MD, Schultz RT: Using computerized games to teach facerecognition skills to children with autism spectrum disorder: the let’s face it!program. Journal of Child Psychology and Psychiatry 2010, 51:944–952.
210. Sala M, Braida D, Lentini D, Busnelli M, Bulgheroni E, Capurro V, Finardi A,Donzelli A, Pattini L, Rubino T, Parolaro D, Nishimori K, Parenti M, Chini B:Pharmacologic rescue of impaired cognitive flexibility, social deficits,increased aggression, and seizure susceptibility in oxytocin receptor nullmice: a neurobehavioral model of autism. Biol Psychiatry 2011, 69:875–882.
211. Modi ME, Young LJ: D-cycloserine facilitates socially reinforced learning inan animal model relevant to autism spectrum disorders. Biol Psychiatry2011, 70:298–304.
212. Levy SE, Mandell DS, Schultz RT: Autism. Lancet 2009, 374:1627–1638.213. Treadway MT, Zald DH: Reconsidering anhedonia in depression: lessons
from translational neuroscience. Neurosci Biobehav Rev 2011, 35:537–555.214. Luman M, Tripp G, Scheres A: Identifying the neurobiology of altered
reinforcement sensitivity in adhd: a review and research agenda. NeurosciBiobehav Rev 2010, 34:744–754.
215. Antshel KM, Polacek C, McMahon M, Dygert K, Spenceley L, Dygert L, MillerL, Faisal F: Comorbid ADHD and anxiety affect social skills groupintervention treatment efficacy in children with autism spectrumdisorders. J Dev Behav Pediatr 2011, 32(6):439–446. 32.
216. Cortesi F, Giannotti F, Ivanenko A, Johnson K: Sleep in children withautistic spectrum disorder. Sleep Med 2010, 11:659–664.
217. Libedinsky C, Smith DV, Teng CS, Namburi P, Chen VW, Huettel SA, CheeMWL: Sleep deprivation alters valuation signals in the ventromedialprefrontal cortex. Frontiers in Behavioral Neuroscience 2011, 5:70.
218. Gujar N, Yoo S-S, Hu P, Walker MP: Sleep deprivation amplifies reactivity ofbrain reward networks, biasing the appraisal of positive emotionalexperiences. J Neurosci 2011, 31:4466–4474.

Kohls et al. Journal of Neurodevelopmental Disorders 2012, 4:10 Page 20 of 20http://www.jneurodevdisorders.com/content/4/1/10
219. Holm SM, Forbes EE, Ryan ND, Phillips ML, Tarr JA, Dahl RE: Reward-relatedbrain function and sleep in pre/early pubertal and mid/late pubertaladolescents. J Adolesc Health 2009, 45:326–334.
220. Garon N, Bryson SE, Zwaigenbaum L, Smith IM, Brian J, Roberts W, SzatmariP: Temperament and its relationship to autistic symptoms in a high-riskinfant sib cohort. J Abnorm Child Psychol 2008, 37:59–78.
221. Joosten AV, Bundy AC, Einfeld SL: Intrinsic and extrinsic motivation forstereotypic and repetitive behavior. J Autism Dev Disord 2009, 39:521–531.
222. Yacubian J, Büchel C: The genetic basis of individual differences in rewardprocessing and the link to addictive behavior and social cognition.Neuroscience 2009, 164:55–71.
223. Murayama K, Matsumoto M, Izuma K, Matsumoto K: Neural basis of theundermining effect of monetary reward on intrinsic motivation. PNASProceedings of the National Academy of Sciences of the United States ofAmerica 2010, 107:20911–20916.
224. Forbes EE, Olino TM, Ryan ND, Birmaher B, Axelson D, Moyles DL, Dahl RE:Reward-related brain function as a predictor of treatment response inadolescents with major depressive disorder. Cogn Affect Behav Neurosci2010, 10:107–118.
225. van den Hoofdakker BJ, Nauta MH, Dijck-Brouwer DAJ, van der Veen-Mulders L,Sytema S, Emmelkamp PMG, Minderaa RB, Hoekstra PJ: Dopamine transportergene moderates response to behavioral parent training in children withADHD: a pilot study. Dev Psychol 2012, 48:567–574.
226. Belsky J, Pluess M: Beyond diathesis stress: differential susceptibility toenvironmental influences. Psychol Bull 2009, 135:885–908.
227. Vollmer TR, Iwata BA: Establishing operations and reinforcement effects.J Appl Behav Anal 1991, 24:279–291.
doi:10.1186/1866-1955-4-10Cite this article as: Kohls et al.: Social ‘wanting’ dysfunction in autism:neurobiological underpinnings and treatment implications. Journal ofNeurodevelopmental Disorders 2012 4:10.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit