Response of the human peritoneal mesothelial cell to injury: An in vitro model of peritoneal wound...
10
Response of the human peritoneal mesothelial cell to injury: An in vitro model of peritoneal wound healing SUSAN YUNG and MALCOLM DAVIES Institute of Nephrology, University of Wales College of Medicine, Royal Infirmary, Cardiff, Wales United Kingdom Response of the human peritoneal mesothelial cell to injury: An in vitro model of peritoneal wound healing. Background. The denudation of the peritoneal mesothelium and damage to the underlying interstitium is a frequent finding in patients receiving continuous ambulatory peritoneal dialysis as a treatment for end-stage renal failure. The response of the me- sothelium to injury from repeated episodes of infection or from exposure to dialysis fluids has not been extensively studied. The present study describes a simple and reproducible method with which to investigate the response of human mesothelial cells to injury. Methods. The model of peritoneal injury consists of mechani- cally wounding a monolayer of human peritoneal mesothelial cells with a glass probe and following the repopulation of the denuded area by time-lapse photomicroscopy. In addition immunohisto- chemistry was used to follow the response of marker proteins for stress fibers and focal adhesions as well as macromolecules associated with the extracellular matrix. Results. Under serum-free conditions the wound (0.58 6 0.094 mm; mean 6 SD; N 5 20) closed within 72 6 5 hours (N 5 8). This rate of healing was enhanced by fetal calf serum, by human serum (10%) and by undiluted spent non-infected dialysate. The repair process over the first 48 hours was the result of cell migration, was independent of cell proliferation and involved the de novo syn- thesis of several different extracellular matrix components. An early event in the healing process was the rapid reorganization of intracellular stress fibers together with the formation of associated focal adhesions in cells at the wound edge. Conclusion. This in vitro model should prove invaluable in characterizing the process of wound healing within the peritoneal cavity, thus allowing a better understanding of the response to infection as well as any effect of dialysis fluids in this pattern of cell behavior. The peritoneal membrane has a complex ultrastructure and is composed of a mesothelial cell monolayer, a distinct but discontinuous basement membrane and an interstitial matrix containing capillary networks [1]. Recent studies from our and other laboratories have focused on the mesothelial cell and its role in the peritoneal response to infection as well as its importance in maintaining peritoneal homeostasis [2–9]. In addition, studies focusing on the effects of dialysis fluids on mesothelial cells have high- lighted defects in the biocompatibility of these fluids and the susceptibility of the mesothelial monolayer to injury [10 –13]. The introduction of a reliable and reproducible method to study human peritoneal mesothelial cells (HPMC) in vitro has provided some evidence that these cells respond directly to biological and chemical insults by the synthesis and secretion of biologically active molecules including IL-1, IL-6 and IL-8 [2, 3, 14, 15], and the vasoactive prostaglandins PGE 2 and PGI 2 [16]. Recent findings also suggest that these cells may respond to injury by the synthesis of significantly increased amounts of proteoglycans and hyaluronan [8, 9, 17, 18]. It has also been shown that following periods of infection areas of the mesothelial surface become denuded of cells [19]. The mechanisms by which peritoneal mesothelial cells respond to such injury are poorly understood and there is considerable debate as to the origin of the cells that colonize the exposed surface of the peritoneum. In addi- tion, the factors that control repopulation of the peritoneal surface are unknown. Mechanical injury of cultured cells has served as a useful in vitro system for studying the response of a number of different cell types to injury [20 –26]. To gain some insight into the response of the mesothelium to injury we have developed a model system for studying the response of confluent HPMC after mechanical wounding. Our results demonstrate that the reorganization of the cytoskeleton and cell migration are early responses, and that this is accompanied by the synthesis of major components of the mesothelial basement membrane. METHODS All chemicals, unless otherwise stated, were obtained from Sigma-Aldrich Ltd Chemical Company (Poole, UK). Tissue culture plastics were purchased from Becton Dick- inson (UK) Ltd. Key words: peritoneal injury, end-stage renal failure, infection, dialysate, cell behavior. © 1998 by the International Society of Nephrology Kidney International, Vol. 54 (1998), pp. 2160 –2169 2160
Transcript of Response of the human peritoneal mesothelial cell to injury: An in vitro model of peritoneal wound...

Response of the human peritoneal mesothelial cell to injury: Anin vitro model of peritoneal wound healing
SUSAN YUNG and MALCOLM DAVIES
Institute of Nephrology, University of Wales College of Medicine, Royal Infirmary, Cardiff, Wales United Kingdom
Response of the human peritoneal mesothelial cell to injury: Anin vitro model of peritoneal wound healing.
Background. The denudation of the peritoneal mesotheliumand damage to the underlying interstitium is a frequent finding inpatients receiving continuous ambulatory peritoneal dialysis as atreatment for end-stage renal failure. The response of the me-sothelium to injury from repeated episodes of infection or fromexposure to dialysis fluids has not been extensively studied. Thepresent study describes a simple and reproducible method withwhich to investigate the response of human mesothelial cells toinjury.
Methods. The model of peritoneal injury consists of mechani-cally wounding a monolayer of human peritoneal mesothelial cellswith a glass probe and following the repopulation of the denudedarea by time-lapse photomicroscopy. In addition immunohisto-chemistry was used to follow the response of marker proteins forstress fibers and focal adhesions as well as macromoleculesassociated with the extracellular matrix.
Results. Under serum-free conditions the wound (0.58 6 0.094mm; mean 6 SD; N 5 20) closed within 72 6 5 hours (N 5 8). Thisrate of healing was enhanced by fetal calf serum, by human serum(10%) and by undiluted spent non-infected dialysate. The repairprocess over the first 48 hours was the result of cell migration, wasindependent of cell proliferation and involved the de novo syn-thesis of several different extracellular matrix components. Anearly event in the healing process was the rapid reorganization ofintracellular stress fibers together with the formation of associatedfocal adhesions in cells at the wound edge.
Conclusion. This in vitro model should prove invaluable incharacterizing the process of wound healing within the peritonealcavity, thus allowing a better understanding of the response toinfection as well as any effect of dialysis fluids in this pattern ofcell behavior.
The peritoneal membrane has a complex ultrastructureand is composed of a mesothelial cell monolayer, a distinctbut discontinuous basement membrane and an interstitialmatrix containing capillary networks [1]. Recent studiesfrom our and other laboratories have focused on themesothelial cell and its role in the peritoneal response to
infection as well as its importance in maintaining peritonealhomeostasis [2–9]. In addition, studies focusing on theeffects of dialysis fluids on mesothelial cells have high-lighted defects in the biocompatibility of these fluids andthe susceptibility of the mesothelial monolayer to injury[10–13]. The introduction of a reliable and reproduciblemethod to study human peritoneal mesothelial cells(HPMC) in vitro has provided some evidence that thesecells respond directly to biological and chemical insults bythe synthesis and secretion of biologically active moleculesincluding IL-1, IL-6 and IL-8 [2, 3, 14, 15], and thevasoactive prostaglandins PGE2 and PGI2 [16]. Recentfindings also suggest that these cells may respond to injuryby the synthesis of significantly increased amounts ofproteoglycans and hyaluronan [8, 9, 17, 18].
It has also been shown that following periods of infectionareas of the mesothelial surface become denuded of cells[19]. The mechanisms by which peritoneal mesothelial cellsrespond to such injury are poorly understood and there isconsiderable debate as to the origin of the cells thatcolonize the exposed surface of the peritoneum. In addi-tion, the factors that control repopulation of the peritonealsurface are unknown.
Mechanical injury of cultured cells has served as a usefulin vitro system for studying the response of a number ofdifferent cell types to injury [20–26]. To gain some insightinto the response of the mesothelium to injury we havedeveloped a model system for studying the response ofconfluent HPMC after mechanical wounding. Our resultsdemonstrate that the reorganization of the cytoskeletonand cell migration are early responses, and that this isaccompanied by the synthesis of major components of themesothelial basement membrane.
METHODS
All chemicals, unless otherwise stated, were obtainedfrom Sigma-Aldrich Ltd Chemical Company (Poole, UK).Tissue culture plastics were purchased from Becton Dick-inson (UK) Ltd.
Key words: peritoneal injury, end-stage renal failure, infection, dialysate,cell behavior.
© 1998 by the International Society of Nephrology
Kidney International, Vol. 54 (1998), pp. 2160–2169
2160

Isolation and culture of human peritoneal mesothelial cells
Human peritoneal mesothelial cells (HPMC) were iso-lated by enzymatic disaggregation of omentum obtainedwith consent from non-uremic patients undergoing abdom-inal surgery. Cells were isolated and cultured essentially asreported by us previously [8, 16]. The cells were maintainedand propagated in Medium 199 (Life Technologies Ltd,Paisley, Scotland, UK) containing 10% fetal calf serum(FCS; Life Technologies Ltd) and supplemented withpenicillin 100 U/ml, streptomycin 100 mg/ml, glutamine 2mM, insulin 5 mg/ml, transferrin 5 mg/ml, and hydrocorti-sone 0.4 mg/ml. Confluent cells were split at a ratio of 1:3and all experiments performed with cells of the secondpassage.
Wounding experiments
Cells were grown to confluence in 35 mm dishes (BectonDickinson UK Ltd), and growth arrested by incubatingthem for 72 hours in serum free Medium 199. Under theseconditions the cells remained viable in a nonproliferatingstate. The quiescent monolayer was injured by scrapingwith a sterile glass rod. The monolayer was washed twicewith PBS and then incubated with serum free Medium-199alone or Medium 199 containing varying concentrations ofFCS, decomplemented human serum (HS) or pooled non-infected peritoneal dialysate prepared from overnight dwellsamples from six different patients. Control cells weretreated in an identical manner but without injury.
Time-lapsed cinemicrography
The closure of the denuded area (that is, wound) wasmonitored using an Axiovert 135 inverted microscope fittedwith an M heating stage and incubator (Zeiss, Oberkochen,Germany). With this arrangement the cultures were main-tained in a 5% CO2 humidified atmosphere at 37°C for theduration of the experiment. A video camera (C5985;Hamamatsu Inc, Japan) was attached to the microscopeand images of the wounded area captured as a digitalisedsequence every 15 minutes using image analysis (Biovision,Improvision, Coventry, UK). The rate of motility of thecells (mm/hr) entering the wound was calculated for eachhour after injury from six separate points along the originalmargin of the wound. Each experiment was repeated threetimes using cell lines established from omentum obtainedfrom different patients.
Immunocytochemical staining for stress fibers, focaladhesions and extracellular matrix components
For immunocytochemical studies, the cells were plated onglass coverslips (Fisher Scientific, Loughborough, UK) placedin 24-flat bottomed well tissue culture plates (Becton Dickin-son UK Ltd), grown to confluence and then growth arrestedfor 72 hours. The monolayers were injured as describedabove, the cells washed with PBS and the cultures continued
in either serum-free Medium 199 or Medium 199 containing10% FCS. At five minutes, 30 minutes, one hour, three hours,and every three hours thereafter, the cells were fixed witheither freshly prepared 3.5% paraformaldehyde in PBS(detection of focal adhesion and stress fibers) or cold acetone:methanol (1:1 by volume; localization of fibronectin, laminin,perlecan and collagens) for five minutes at room temperature.Autofluorescence of any aldehyde groups present wasquenched with 0.1 M ammonium chloride for 10 minutes atroom temperature. The cells were then washed three timeswith PBS. Each cover slip was then incubated in primaryantisera or the appropriate non-immune serum. The followingprimary antibodies (diluted in PBS) were incubated forone hour at 37°C; vinculin (1:50; Sigma-Aldrich Ltd), paxillin(1:50; Zymed, San Francisco, CA, USA), a-actinin (1:100;Sigma-Aldrich Ltd), collagen type III (1:50, Southern Bio-Technology, Birmingham, AL, USA), collagen type I(1:500; Sigma-Aldrich Ltd) collagen type IV (1:50; kindlyprovided by Dr. John Couchman, University of Alabama atBirmingham, USA), collagen V (I:50; Southern Biotechnolo-gy), laminin (1:50; Dr. John Couchman), fibronectin (1:50;Dr. John Couchman), and perlecan (1:100; Dr. John Hassall,Shriner’s Hospital, Tampa, FL, USA). After washing withPBS, secondary antibodies (conjugated with FITC) wereapplied for one hour at 37°C in a darkened humidifiedchamber. Controls included omitting the primary antibodyand substituting the primary antibody with an irrelevantantibody of the same Ig class. Finally, the preparations werewashed thoroughly with PBS, mounted in Vectashield (VectorLaboratories, Peterborough, UK) and immunofluorescenceviewed with an Axiovert 135 microscope and photographedon Ilford HP-5 film. F-actin was also visualized with fluores-cein-labeled phalloidin (Sigma-Aldrich Ltd) [27].
Identification of proliferation using bromodeoxyuridineincorporation into cells
A modification of the immunocytochemical method de-scribed by Magaud et al [28] was used to evaluate prolifer-ation. Cells were wounded as described above, cultured inbromodeoxyuridine (BrdU) at a final concentration of 1025
M and at different time intervals were fixed in acetone:methanol (1:1) for 90 seconds. The incorporation of BrdUinto the DNA of cells entering the S-phase of the cell cyclewas then assessed. Following fixation, cells were washedwith Tris-buffered saline, pH 7.6 (TBS) for five minutes,incubated with 95% (vol/vol) formamide in 0.15 M triso-dium citrate for 45 minutes at 70°C to denature doublestranded DNA and washed with TBS. The cells were thenblocked by incubating with bovine serum albumin (1% inTBS) for 30 minutes at 37°C, after which time the coverslipswere transferred to a humidified chamber. Anti-BrdU(diluted 1:1000 in TBS; Sigma-Aldrich Ltd) was added, thecells further incubated for 30 minutes at room temperature,washed again in TBS for five minutes and then incubatedwith anti-mouse immunoglobulins (DAKO Ltd, Ely, UK;
Yung and Davies: A model of peritoneal mesothelium repair 2161

diluted 1:25) for 30 minutes at room temperature in ahumidified chamber. Cells were washed in TBS, incubatedwith alkaline phosphatase-anti-alkaline phosphatase com-plex for 30 minutes and re-washed with TBS for fiveminutes. The incorporation of BrdU into the nuclei of
HPMC was monitored by staining with FAST RED for 20minutes according to the manufacturer’s instructions. Thecells were then rinsed gently with water, mounted inaqueous mounting medium (Glycergel; DAKO Ltd) andviewed by light microscopy.
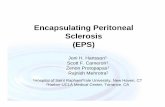
Fig. 1. Response of human peritoneal mesothelial cells to injury. Phase contrast microscopy of a typical experiment over a 72 hour time period of cellcultured in serum-free medium. Bar 5 100 mm.
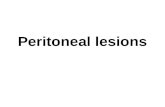
Fig. 2. Phase contrast microscopy of human peritoneal mesothelial cells migrating into the denuded area of the scratch-wound to show the extensionof lamellipodia at the leading edge of the wound at (a) time zero, (b) one hour and (c) three hours. The black line represents the initial wound (bar 5100 mm).
Yung and Davies: A model of peritoneal mesothelium repair2162

RESULTS
HPMC (104/cm2) were plated on 35 mm dishes andgrown to confluence over five days when they adopted anon-overlapping monolayer of flat polygonal appearancecharacteristic of epithelial cells (Figs. 1 and 2). Immuno-histochemical staining with vimentin and cytokeratin con-firmed the homogenous nature of the cultures and theabsence of macrophages and fibroblasts (data not shown).
Time course of wound repopulation
To examine the response of mesothelial cells to mechan-ical injury, monolayers were growth arrested in serum-freemedium and manually wounded by a single scratch alongthe diameter of the culture dish with a sterile glass rod. Thisprocedure left an area (that is, wound) in the monolayer,devoid of cells (Figs. 1 and 2) and any underlying extracel-lular matrix (Fig. 5). The mean width of a series of woundsmeasured from light photomicrographs at time zero was0.58 6 0.094 mm (mean 6 SD; N 5 20). The progress of atypical experiment over 72 hours as well the first threehours is included in Figures 1 and 2, respectively. Initiallythe cells at the wound edge rounded up but quicklyregained their epithelial-like appearance (Figs. 1b and 2b).
In serum-free conditions, two populations of HPMC basedon phase-contrast microscopy were observed. The cellsinitially moved as a monolayer of flat polygonal shapedcells towards the denuded area with those at the leadingedge having a more flattened appearance (Fig. 2 b, c).Moreover, these cells exhibited lamellipodia (Fig. 2 b, c).Ten hours after the initial injury some of the cells from theleading edge detached from the advancing monolayer andmigrated independently of the wound (Fig. 1 c, d). These‘pioneer’ cells showed a more elongated appearance com-pared to the cells within the monolayer and appeared tomigrate in a random manner within the wounded area. Thewounded area was repopulated after 72 6 5 hours (N 5 8)with the original morphology fully restored (Fig. 1f).
Role of proliferation in wound repair
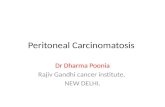
To further investigate the response of the monolayer tomechanical wounding we incubated the cells with BrdU andused immunocytochemical staining to detect its incorpora-tion into cellular DNA. Since BrdU is only introduced intothe S (synthetic) phase of the cell cycle, the method offersan accurate estimation of cell proliferation. Figure 3A
Fig. 3. Immunostaining of human peritoneal mesothelial cells with mouse anti-bromodeoxyuridine to demonstrate the proliferative activity in cells inresponse to wounding. (A) Control cells; (B) cells at the edge of the wound at six hours; (C) cells away from the wound at six hours; (D) cells in therestored monolayer at 72 hours (bar 5 100 mm).
Yung and Davies: A model of peritoneal mesothelium repair 2163

demonstrates that quiescent confluent mesothelial cellsprior to injury take up little BrdU. Moreover, there was noincreased staining at the margins of the wound or within
the unaffected layer during the initial 24 hours of therecovery of the monolayer. After this time the number ofcells staining positively for BrdU increased between two- to
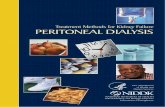
Fig. 4. Staining of 3.5% paraformaldehyde fixed human peritoneal mesothelial cells with fluorescein-labeled phalloidin (panels a, e, i, m) andmonoclonal antibodies to a-actinin (b, f, j, n), vinculin (c, g, k, o) and paxillin (d, h, l, p); a-d, cells fixed prior to wounding; e-h, one hour post wounding;i-l, 12 hours post-wounding; m-p, 72 hours post-wounding. The arrow in panels e to h indicate stress fibers and focal adhesions at the leading edge ofthe wound. The arrowhead in panels i-l indicate the enhance focal adhesion components during cell migration (bar 5 30 mm).
Table 1. Percentage of cells staining positive for BrdU
Time after injuryhr
Distance away from wound edge (mm)
0–150 151–300 301–450 451–600
Pre-wounding 8.41 6 2.78 7.43 6 2.89 7.78 6 2.70 7.65 6 5.401.0 6.14 6 3.11 6.94 6 3.03 7.29 6 3.84 6.87 6 3.283.0 11.34 6 7.02 6.26 6 0.67 7.00 6 4.22 13.31 6 4.49
12.0 8.47 6 1.01 4.44 6 3.11 7.15 6 3.72 9.06 6 1.9824.0 20.09 6 5.48 17.42 6 5.63 23.39 6 7.99 12.42 6 7.9036.0 15.42 6 6.48 11.30 6 3.11 17.11 6 4.92 13.40 6 3.6348.0 21.55 6 5.22 20.35 6 2.47 21.17 6 7.07 21.28 6 1.9260.0 16.03 6 6.50 18.28 6 8.28 23.48 6 4.00 19.37 6 2.5672.0 17.64 6 3.36 21.95 6 7.16 25.10 6 11.13 21.22 6 10.7396.0 11.64 6 3.36 10.95 6 7.16 12.10 6 11.13 10.22 6 10.73
Data represents the average of four separate determinations.
Yung and Davies: A model of peritoneal mesothelium repair2164

threefold with time (Fig. 3B and Table 1). By five days themonolayer was re-established and the staining for BrdUreverted back to that observed prior to wounding (Table 1).
Response of the cytoskeleton elements to injury
An early response of many cells to extracellular stimuli isthe reorganization of their actin filaments (stress fibers)and focal adhesions. Interactions of these cellular elementswith extracellular matrix are important in defining cellshape and cell movement [29]. To determine the responseof the cytoskeletal elements of HPMC to mechanicalwounding, the localization of F-actin (phalloidin), a-acti-nin, vinculin, and paxillin were followed by immunofluores-cence [30, 31]. HPMC that had reached confluence inserum-free conditions exhibited very few stress fibers andfocal adhesions (Fig. 4 a-d). The cells, however, did show apunctate distribution of actin (Fig. 4 a, b). This pattern ofstaining resembles the pattern of actin staining reported forserum-starved Swiss 3T3 cells [32, 33]. Within one hour ofinjuring the monolayer this staining pattern for cytoskeletalelements was considerably changed. The actin fibers be-came organized to show a thick cable of F-actin thatappeared continuous from cell to cell along the leadingedge of the wound (Fig. 4. e, f). Vinculin and paxillin werealso prominently concentrated along the extreme edge, butwith a slightly patchy distribution rather than the unifor-
mity shown by F-actin (Fig. 4 g, h). This organization of thecytoskeletal components appeared to be restricted to theleading edge. Very few actin fibers were observed through-out the cytoplasm. Vinculin and paxillin, however, wereobserved in cells away from the wound edge, suggestingthat these cells formed focal adhesions or focal contacts(Fig. 4 g, h). This pattern of immunostaining was main-tained for up to 10 hours. In this phase of wound repairthere was no sign of actin thickening (data not shown).Between 10 to 12 hours when individual HPMC detachedfrom the injured monolayer the staining pattern for phal-loidin and a-actinin changed again. The F-actin fibersbecame thicker and highly organized throughout the cellcytoplasm (Fig. 4 i, j). In addition prominent teardrop-shaped focal adhesions were established (Fig. 4 k, l) thatremained until the closure of the wound. As the monolayerwas re-established (t 5 72 hr), the actin filaments becamefiner and were again predominantly localized at the periph-ery of the cell (Fig. 4 m, n). At this time the staining forvinculin and paxillin was reduced (Fig. 4 o, p). Ninety-sixhours after wounding the F-actin reverted back to a disor-ganized form (data not shown).
Extracellular matrix in response to injury
The procedure used to wound the cells also removed themajority of the underlying extracellular matrix (ECM; Fig. 5).
Fig. 5. Immunostaining of acetone:methanol fixed human peritoneal mesothelial cells with polyclonal antibodies to collagen IV, laminin, fibronectinand perlecan. Fixed cells were stained (i) prior to injury (panels a-d), (ii) after 12 hours (e-h), and (iii) after wound closure (i-l). Bar 5 30 mm.
Yung and Davies: A model of peritoneal mesothelium repair 2165

The various proteins of the ECM have a major influence oncell migration by virtue of their involvement in cell attachmentto, and detachment from organized matrix [34]. We thereforeinvestigated whether collagen type IV, laminin, fibronectinand basement membrane heparan sulphate proteoglycan(perlecan) were involved in the migration of the mesothelialcells into the wound. These experiments were carried out oncells grown and injured on cover slips in the absence of serum.At various times after wounding the monolayer, the coverslipswere fixed and extracellular matrix proteins visualized byimmunohistochemistry. Figure 5 shows the results of theseexperiments before injury (Fig. 5 a-d), 12 hours after injury(Fig. 5 e-h) and after 72 hours (Fig. 5 i-l). While no stainingwas observed in areas devoid of cells, the cells in or enteringthe wound stained positively for each matrix protein exam-ined. After 72 hours, at which time the wound had fullyrepopulated, a well defined matrix made up of collagen typeIV, laminin, fibronectin and perlecan was evident in the areamaking up the wound (Fig. 5. a-l). These experiments indicatethat the cells migrating into the wound were also accompaniedby the de novo synthesis of a number of different matrixcomponents. Inspection of the immunohistochemical stainingafter wound closure showed no signs of excess matrix depo-sition in the repopulated area. Staining for collagens I, III andV also showed similar patterns as those described above (datanot shown).
Effects of serum and dialysis fluid on woundrepopulation
In the peritoneum the mesothelium is exposed to manyof the components of serum. Since the results from theabove experiments were undertaken in serum-free mediumthe response of wounded cells to FCS, heat-inactivatedhuman serum, as well as a pooled preparation of undiluted
spent non-infected dialysis fluid was investigated. Therewas a dose-dependent effect of FCS on the kinetics ofwound re-population. Maximum rate of wound closureoccurred at 10% FCS (Fig. 6) and was not increased in thepresence of 20% (data not shown). Human serum (10%vol/vol) was as effective as FCS. Non-infected peritonealfluid also enhanced the migration of the cells into thewound at a similar rate to that achieved with 5% FCS.
DISCUSSION
There is accumulating evidence that the human perito-neal mesothelium is damaged or injured during CAPD asthe result of persistent infection or the prolonged exposureto dialysis fluids. The present study has described a simpleand reproducible model with which to investigate theresponse of HPMC to injury. The model consists of amonolayer of HPMC that is mechanically wounded. Re-population of the wound can then be followed temporallyby time-lapse photomicroscopy, and planimetry. Since thebasic experimental conditions employed a homogenouspopulation of cells devoid of macrophages or fibroblastsand was undertaken in conditions lacking serum, the modelprovides information on the direct response of HPMC toinjury.
The healing of the human mesothelium after denudationin vivo is believed to involve mesothelial cells advancingcentripetally from the wound margin [35]. Since re-epithe-lization is rapid, and the closure time independent of theinitial area affected, it has been argued that other mecha-nisms must be involved [36–38]. Thus, in addition tomigration three other proposals for the origin of the newlyformed mesothelium have been suggested. The first is thatperitoneal mesothelial cells exfoliate from the intact peri-toneum, adhere to the injured area and proliferate to form
Fig. 6. Effects of fetal calf serum (FCS;0 to 10%), heat-inactivated human serumand a pooled non-infected dialysate(N 5 6) from patients receiving CAPD, onthe rate of migration of human peritonealmesothelial cells after wounding.Experiments were performed in triplicateusing cells derived from omentum obtainedfrom four different patients. Results areexpressed as mean 6 SD (N 5 4).
Yung and Davies: A model of peritoneal mesothelium repair2166

a new mesothelial layer [39–41]. This has been questionedby Raftery [42, 43], who found very little evidence for freemesothelial cells in the peritoneum in an experimentalmodel of peritoneal wounding, and furthermore indicatedthat those cells present were either injured or dying. Thesecond proposal is that the regeneration of the mesothelialsurface involves the differentiation of the macrophages orhistiocytes into mesothelial cells at the site of the wound[44]. Evidence for this is based on the morphologicalcharacteristics of the cellular content and the cytochemicalstaining of lysosomal acid hydrolases. It requires confirma-tion using the many specific cell surface markers nowavailable for the positive identification of macrophages andtheir distinction from mesenchymal cells. Clearly, macro-phages are involved in tissue repair, but this is probablythrough their ability to release cytokines and proteolyticenzymes that facilitate tissue remodeling [45]. The thirdproposal is that new mesothelium arises as the result ofmetaplasia of fibroblasts present in submesothelial tissuebordering the wound [43, 46, 47].
The present study demonstrates that the repair of amesothelial wound in vitro is complete after approximately72 hours and that the process can take place in the absenceof serum or added cytokines. This also occurred in theabsence of proliferation at the leading edge, since theimmunocytochemical studies with BrdU did not reveal achange in the proportion of cells synthesizing DNA ateither the wound edge or in the unaffected cells at any onetime over and above controls. The closure of the wound isthe result of cell migration but the process is accompaniedby an overall increase in proliferation. These proliferatingcells are distributed evenly through the wound model. Thisconclusion is in agreement with the general response ofother epithelial cells to injury in vitro [24, 48–50]. Thus, theresults of this study give some support to one of theproposals advanced for peritoneal repair in vivo. Further-more, since our studies were undertaken with a homoge-neous population of HPMC, the results also demonstratethat other cell-types need not necessarily be involved inmesothelial wound healing, although their involvement isnot excluded.
The scrape-wounding of a defined area of the mesothe-lial monolayer also removed the underlying extracellularmatrix. Since cell migration depends on adhesion of cells totheir substratum via cell surface receptors, the repopulationrequires the cells to deposit additional matrix proteins. By12 hours there was a clear appearance of new matrixassociated with the migrating cells, suggesting that thesecells actively lay down their own matrix. It is likely that theyexpress appropriate adherence molecules to achieve suffi-cient traction for cell movement. Under the conditions ofthe experiment it was not possible to ascertain from theimmunohistochemical staining if matrix synthesis was con-fined to migrating cells alone, or if the wounding alsoinitiated de novo synthesis by cells at or away from the
wound. Furthermore, we do not have any information onthe kinetics of the synthesis of the different ECM proteinsby the cells in response to mechanical injury. The findingthat fibronectin is one of the matrix proteins synthesized islikely to be important, since this glycoprotein has multiplefunctions in wound healing in vivo and in vitro, and alsoplays a critical role in cell adhesion and movement [51, 52].In addition fibronectin promotes the reorganization ofstress fibers and focal adhesions [53].
The study also shows that scrape wounding of confluentHPMC in the absence of serum initiates a number of otherevents, including the organization of stress fibers within thecells and the development of focal adhesions. This isaccompanied by cell migration, which ultimately bringsabout the closure of the denuded area. These observationstherefore raise questions about the nature of the stimulusor cellular signals associated with the repair process. Theyalso raise the question of how the cells at the leading edgecommunicate with cells distant from the wound to initiateproliferation. The growth and migration of mammaliancells is tightly regulated by both growth inhibitory andstimulatory signals. Thus, one of the consequences ofmechanical injury could be the loss of inhibitory signalsmediated by the removal or modification of cell surfaceproteins such as contactinhibin [54, 55] or cell surfaceheparan sulphate glycosaminoglycans, which are known tomodulate the biological activity of many different growthfactors [56, 57]. A more likely effect of injury is the releaseof agents that invoke a positive signal, which in turninitiates events that lead to either cell migration and cellproliferation. Recent studies with mammary epithelial andarterial endothelial cells showed an immediate but tran-sient elevation in intracellular calcium ([Ca21]i) metabo-lism upon mechanical injury [22]. Interestingly, the Ca21
response was not limited to the cells at the wound edge, butextended into the monolayer for a distance up to 12 cells,indicating the response was caused by the release of asoluble factor that diffused from the wound and acted viacell surface receptors. The nature of the released factor wasnot investigated, but one can speculate on the release ofgrowth factors or nucleotides. Thus, from similar woundhealing studies membrane disruption initiates the releaseof growth factors such as FGF, TGF-b, and EGF that act inan autocrine fashion to effect re-epithelialization of thewound [49]. In addition injured cells release adenosinenucleotides that in turn stimulate repair by promotingmigration of the unaffected cells into the denuded area[24]. Other molecules identified in the early stages of injuryin vitro include the receptor for hyaluronan-mediated mo-tility, referred to as RHAMM [21], matrix metalloprotein-ases [25, 58], hepatocyte growth factor [59], and platelet-derived growth factor (PDGF).
The movement of cells requires the reorganization of thecytoskeleton, the assembly of focal adhesions and theisoforms of integrins. Our studies clearly demonstrate that
Yung and Davies: A model of peritoneal mesothelium repair 2167

in response to scrape wounding of mesothelial cells actin ispolymerized and assembled into stress fibers. Simulta-neously there is an increase in the staining of vinculin andpaxillin suggesting that new focal adhesions or focal con-tacts are formed. However, whether these componentproteins of focal adhesions are associated with the end ofactin stress fibers requires further investigation. The for-mation of cytoskeleton elements are regulated by theGTP-binding proteins that belong to the rho-subfamily,members of the Ras superfamily of small GTPases [re-viewed in 30]. When serum-starved fibroblasts, which havevery few stress fibers and associated focal adhesions, aretreated with FCS or lysophosphatidic acid (LPA), a con-stituent of serum, stress fibers and aggregation of vinculinand talin into focal adhesion are induced within twominutes [27, 32]. PDGF, EGF and insulin also induce asimilar effect but over a longer time period of 5 to 10minutes. To explain this time delay, Ridley and Hall arguedthat serum and LPA directly stimulate the rho-dependentsignaling pathway, whereas PDGF, EGF and insulin, ini-tially activate rac, which in turn stimulates membraneruffling formation and rho activation [27, 32]. The peptidesTGF-b, TNF-a and prothrombin do not directly induce anydetectable changes in actin filaments. These findings give aclue as to a possible mechanism to explain the response ofHPMC to injury. In preliminary experiments we have alsoobserved that LPA induced the rapid assembly of actinstress fibers and the clustering of vinculin and paxillin toform focal adhesions in cultured HPMC (data not shown).In the current experiments we showed that scratch injury toHPMC is also accompanied by reorganization of stressfibers and the appearance of focal contacts, but that thisresponse was relatively slow. These results argue againstLPA as a possible factor to explain the response of HPMCto mechanical injury. A role for LPA, however, could beimportant in the response of the mesothelium to injury invivo, since our results show that non-infected peritonealfluid, like serum, increases the rate of wound healing. LPAis an abundant constituent of serum and therefore a likelyconstituent of spent dialysis fluid. In addition, LPA can beproduced through extracellular phospholipase A2 acting onmicrovesicles shed from cells [60]. Experiments to furtherinvestigate a possible involvement of LPA cytokines orgrowth factors in our model are in progress.
In conclusion, we have shown that HPMC in serum-freeculture conditions can be used as a model to follow theresponse of these cells to injury. The finding that therecovery from injury is influenced by serum and peritonealfluid from patients on CAPD indicates a potential clinicalimportance for the model. The model, however, has anumber of limitations that need to be addressed in futureexperiments aimed at understanding the response of theperitoneum to the toxic effect of dialysis fluids or peritoni-tis. In particular, there is need to consider that the perito-neum also consists of a cellular basement membrane and an
interstitial matrix in addition to HPMC. In vivo it is notclear whether denudation of the peritoneum is also accom-panied by loss of or damage to the underlying basementmembrane and the effect this would have on the repairprocess. Thus, future experiments will be designed toinvestigate the effect of both types of extracellular matrixon the response of the HPMC to injury.
Reprint requests to Dr. Malcolm Davies, Institute of Nephrology, Universityof Wales College of Medicine, Royal Infirmary, Cardiff, CF2 1SZ, Wales,United Kingdom.E-mail: [email protected]
APPENDIX
Abbreviations used in this article are: BrdU, bromodeoxyuridine;[Ca21]i, intracellular calcium; ECM, extracellular matrix; EGF, epidermalgrowth factor; FCS, fetal calf serum; GTP, guanosine 59-triphosphate;HPMC, human peritoneal mesothelial cells; HS, human serum; IL,interleukin; LPA, lysophosphatidic acid; PDGF, platelet-derived growthfactor; PG, prostaglandin; RHAMM, receptor for hyaluronan-mediatedmotility; TBS, Tris buffered saline; TGF-b, transforming growth factorbeta.
REFERENCES1. VERGER C: Peritoneal ultrastructure with special reference to chronic
renal failure alterations, in The Peritoneum and Peritoneal Access,edited by BENGMARK S, London, Wright, 1989, pp 14–23
2. TOPLEY N, JORRES A, LUTTMANN W, PETERSEN MM, LANG MJ,THIERAUSCH K-H, MULLER C, COLES GA, DAVIES M, WILLIAMS JD:Human peritoneal mesothelial cells synthesize IL-6: Induction byIL-1b and TNFa. Kidney Int 43:226–233, 1993
3. TOPLEY N, BROWN Z, JORRES A, WESTWICK J, DAVIES M, COLES G A,WILLIAMS JD: Human peritoneal mesothelial cells synthesize inter-leukin-8; Synergistic induction by interleukin-1b and tumor necrosisfactor-a. Am J Pathol 142:1876–1886, 1993
4. TOPLEY N, MACKENZIE R, JORRES A, COLES GA, DAVIES M, WIL-LIAMS JD: Cytokine networks in CAPD. Interaction of resident cellsduring inflammation in the peritoneal cavity. Perit Dial Int 13:1–4,1993
5. TOPLEY N, PETERSEN MM, MACKENZIE R, NEUBAUER A, STYLIANOUE, KAEVER V, DAVIES M, COLES GA, JORRES A, WILLIAMS JD:Human peritoneal mesothelial cells prostaglandin synthesis: Inductionof cyclooxygenase mRNA by peritoneal macrophage-derived cyto-kines. Kidney Int 46:900–908, 1994
6. BREBOROWICZ A, RODELA H, PAGIAMTZIS J, OREOPOULOS DG:Stimulation of mesothelial cells proliferation by endogenous growthfactor(s). Perit Dial Int 11:228–232, 1991
7. BREBOROWICZ A, RODELA H, OREOPOULOS DG: Toxicity of osmoticsolutes on human mesothelial cells in vitro. Kidney Int 41:1280–1285,1992
8. YUNG S, COLES, GA WILLIAMS, JD, DAVIES M: The source andpossible significance of hyaluronan in the peritoneal cavity. Kidney Int46:527–533, 1994
9. YUNG S, THOMAS, GJ, STYLIANOU E, COLES GA, WILLIAMS JD,DAVIES M: The source of peritoneal proteoglycans: Human peritonealmesothelial cells synthesise and secrete mainly small dermatan sul-phate proteoglycans. Am J Pathol 146:520–529, 1995
10. PERFUMO F, ALTIERI P, DEGL’INNOCENTI ML, GHIGGERI GM, CARIDIG, TRIVELLI A, GUSMANO R: Effects of peritoneal effluents onmesothelial cells in culture-cell proliferation and extracellular-matrixregulation. Nephrol Dial Transplant 11:1803–1809, 1996
11. WITOWSKI J, TOPLEY N, JORRES A, LIBEREK T, COLES G, WILLIAMSJD: Effect of lactate-buffered peritoneal dialysis fluids on humanperitoneal mesothelial cell interleukin-6 and prostaglandin synthesis.Kidney Int 47:282–293, 1995
12. GOTLOIB L, WAISBRUT V, SHOSTAK A, KUSHNIER R: Acute long-termchanges in imprints of mouse mesothelium exposed to glucose-enriched, lactate, buffered dialysis solutions. Nephron 70:466–477,1995
Yung and Davies: A model of peritoneal mesothelium repair2168

13. TOPLEY N, KAUR D, PETERSON MM, JORRES A, PASSLICK-DEETJEN J,COLES GA, WILLIAMS JD: Bio-compatibility of bicarbonate-bufferedperitoneal dialysis fluids: Influence on mesothelial cell and neutrophilfunction. Kidney Int 49:1447–1456, 1996
14. LANFRANCONE L, BORASCHI D, GHIARA P, FALINI B, GRIGNANI, F,PERI G, MANTOVANI A, PELICCI PG: Human peritoneal mesothelialcells produce many cytokines (Granulocyte colony-stimulating factor[CSF], Granulocyte-monocyte-CSF, macrophage-CSF, interleukin-1[IL-1], and IL-6) and are activated and stimulated to grow by IL-1.Blood 80:2835–2842, 1992
15. DOUVDEVANI A, RAPOPORT J, KONFORTY A, ARGOV S, OVNAT A,CHAIMOVITZ C: Human peritoneal mesothelial cells synthesize IL-1aand IL-1b. Kidney Int 46:993–1001, 1994
16. STYLIANOU E, JENNER LA, DAVIES M, COLES GA, WILLIAMS JD:Isolation, culture and characterization of human peritoneal mesothe-lial cells. Kidney Int 37:1563–1570, 1990
17. BREBOROWICZ A, KORYBALSKA K, GRZYBOWSKI A, WIECZOROWSKA-TOBIS K, MARTIS L, OREOPOULOS DG: Synthesis of hyaluronic acid byhuman peritoneal mesothelial cells: Effect of cytokines and dialysate.Perit Dial Int 16:374–378, 1996
18. YUNG S, COLES GA, DAVIES M: IL-1b, a major stimulator ofhyaluronan synthesis in vitro of human peritoneal mesothelial cells:Relevance to peritonitis. Kidney Int 50:1337–1343, 1996
19. DOBBIE JW, ZAKI MA: The ultrastructure of the parietal peritoneumin normal and uraemic man in patients on CAPD, in Frontiers inPeritoneal Dialysis, edited by MAHER JF, WINCHESTER JF, New York,Field Rich and Associates, Inc, 1986, pp 3–10
20. KINSELLA MG, WIGHT TN: Modulation of sulfated proteoglycansynthesis by bovine aortic endothelial cells during migration. J CellBiol 102:679–687, 1986
21. SAVANI RC, WANG C, YANG B, ZHANG M, KINSELLA MG, WIGHT TN,STERN R, NANCE WM, TURLEY EA: Migration of bovine smoothmuscle cells after wounding injury. The role of hyaluronan andRHAMM. J Cin Invest 95:1158–1168, 1995
22. SAMMAK PJ, HINMAN LE, TRAN PO, SJAASTAD MD, MACHEN TE:How do injured cells communicate with the surviving cell monolayer.J Cell Sci 110:465–475, 1997
23. ZAMBRUNO G, MARCHISIO PC, MARCOMI A, VASCHIERI C, MELCHIORIA, GIANNETTI A, DELUCA M: Transforming growth factor b1 modu-lates b1 and a5 integrin receptors and induces the de novo expressionof the aVb6 heterodimer in normal human keratinoctyes: Implicationfor wound healing. J Cell Biol 129:853–865, 1995
24. KARTHA S, TOBACK FG: Adenine nuceotides stimulate migration inwounded cultures of kidney epithelial cells. J Clin Invest 90:288–292,1992
25. BUISSON A-C, ZAHN J-M, POLETTE M, PIERROT D, BELLON G,PUCHELLE E, BIERBAULT P, TOURNIER J-M: Gelatinase B is involvedin the in vitro wound healing repair of human respiratory epithelium.J Cell Physiol 166:413–426, 1996
26. PAWAR P, KARTHA S, TOBACK FG: Differential gene expression inmigrating renal epithelial cells after wounding. J Cell Physiol 165:556–565, 1995
27. RIDLEY AJ, PATERSON HP, JOHNSTON CL, DIEKMAN D, HALL A: Thesmall GTP-binding protein rac regulates growth factor-induced mem-brane ruffing. Cell 70:401–410, 1992
28. MAGAUD J-P, CLARKE PJ, FFRENCH M, RIMOKH R, MASON DY:Double immunocytochemical labeling of cell and tissue samples withmonoclonal anti-bromodeoxyuridine. J Histochem Cytochem 37:1517–1527, 1989
29. BURRIDGE K, CHRZANOWSKA-WODNICKA M: Focal adhesions, con-tractility, and signaling. Ann Rev Cell Dev Biol 12:463–519, 1996
30. HALL A: Small GTPase-binding proteins and the regulation of theactin cytoskeleton. Ann Rev Cell Biol 10:31–54, 1994
31. WOODS A, COUCHMAN JR: Syndecan-4 heparan sulfate proteoglycanis a selectively enriched and widespread focal adhesion component.Mol Biol Cell 5:183–192, 1994
32. RIDLEY AJ, HALL A: The small GTP-binding protein rho regulates theassembly of focal adhesions and stress fibres in response to growthfactors. Cell 70:389–399, 1992
33. BARRY ST, CRITCHLEY DR: The RhoA-dependent assembly of focaladhesions in Swiss3T3 cells is associated with increased tyrosinephosphorylation and the recruitment of both 125FAK and proteinkinase-d to focal adhesions. J Cell Sci 107:2033–2045, 1994
34. NIEDBALA MJ, CRICKARD K, BERNAC RJ: Adhesion, growth andmorphology of human mesothelial cells on extracellular matrix. J CellSci 85:133–147, 1986
35. CUNNINGHAM RS: The physiology of the serous membranes. PhysiolRev 6:242–280, 1926
36. ELLIS H: The aetiology of postoperative abdominal adhesions. Anexperimental study. Br J Surg 50:10–14, 1962
37. ESKELAND G, KJAERHEIM A: Regeneration of parietal peritoneum inrats; 2. An electron microscopical study. Acta Path Microbiol Scan68:379–395, 1966
38. ESKELAND G: Regeneration of parietal peritoneum in rats 1. A lightmicroscopical study. Acta Path Microbiol Scan 68:355–378, 1966
39. JOHNSON FR, WHITTING HW: Repair of parietal peritoneum. BritJ Surg 49:653–660, 1962
40. CAMERON GR, HASSAN SM, DE SN: Repair of Glisson’s capsule aftertangential wounds in the liver. J Pathol Bacteriol 78:1–10, 1957
41. WATTERS WB, BUCK RC: Scanning electron microscopy of mesothe-lial regeneration in the rat. Lab Invest 26:604–609, 1972
42. RAFTERY AT: Regeneration of parietal and visceral peritoneum. Alight microscopical study. Br J Surg 60:293–299, 1973
43. RAFTERY AT: Regeneration of parietal and visceral peritoneum in theimmature animal: A light and electron microscopical study. Br J Surg60:969–975, 1973
44. RYAN GB, GROBETY J, MAJNO G: Mesothelial injury and recovery.Am J Pathol 71:93–113, 1973
45. RICHES DWH: Macrophages involvement in wound repair, remodel-ing, and fibrosis, in The Molecular and Cellular Biology of WoundRepair, edited by RAF CLARK, New York, Plenum Press, 1996, pp95–142
46. WILLIAMS DC: The peritoneum. A plea for a change in attitudetowards this membrane. Br J Surg 42:401–407, 1955
47. ELLIS H, HARRISON W, HUGH TB: The healing of the peritoneumunder normal and pathological conditions. Br J Surg 52:471–476, 1965
48. MCCORMACK SA, VIAR MJ, JOHNSON LR: Migration of IEC-6 cells: Amodel for mucosal healing. Am J Physiol 263:G426–G435, 1992
49. FABER-ELMAN AH, SOLOMON A, ABRAHAM JA, MARIKOVSKY M,SCHWARTZ M: Involvement of wound-associated factors in rat brainastrocyte migratory response to axonal injury in vitro stimulation.J Clin Invest 97:162–171, 1996
50. ZAHM JM, KAPLAN H, HERARD AL, DORIOT F, PIERROT M,SOMELETTE P, PUCHELLE E: Cell migration and proliferation duringthe in vitro wound repair of the respiratory epithelium. Cell MotilCytoskeleton 37:33–43, 1997
51. HYNES RO: Fibronectin, New York, Springer-Verlag, 199052. YAMADA KM, CLARK RAF: Provisional matrix, in The Molecular and
Cellular Biology of Wound Repair, edited by RAF CLARK, New York,Plenum Press, 1996, pp 51–93
53. WOODS A, COUCHMAN JR, JOHANSSON S, HOOK M: Adhesion andcytoskeletal organization of fibroblasts in response to fibronectinfragments. EMBO J 5:665–670, 1986
54. JOHNSON TC: Negative regulators of cell proliferation. Pharm Therap62:247–265, 1994
55. WIESER RJ, BAUMANN CE, OESCH F: Cell-contact mediated modula-tion of the sialylation of contactinhibin. Medizinische Welt 46:272–279,1995
56. BERNFIELD M, HINKES MT, GALLO RL: Developmental expression ofthe syndecans: Possible function and regulation. Development 119:205–212, 1993
57. DAVID G: Integral membrane heparan sulfate proteoglycans. FASEB7:1023–1030, 1993
58. JAMES TW, WAGNER R, WHITE LA, ZWOLAK RM, BRINCKERHOFF CE:Induction of collagenase and stromelysin gene expression by mechan-ical injury in a vascular smooth muscle-derived cell line. J Cell Physiol157:426–437, 1993
59. TAKAHASHI M, OTA S, SHIMADA T, HAMADA E, KAWABE T, OKUDAIRAT, MATSUMURA M, KANEKO N, TERANO A, NAKAMURA T, OMATA M:Hepatocyte growth factor is the most potent endogenous stimulant ofrabbit gastric epithelial cell proliferation and migration in primaryculture. J Clin Invest 95:1994–2003, 1995
60. FOURCADE O, SIMON MF, VIODE C, RUGANI N, LEBALLE F, RAGAB A,FOURNIE B, SARDA L, CHAP H: Secretory phospholipase A2 generatesthe novel lipid mediator lysophosphatidic acid in membrane mi-crovesicles shed from activated cells. Cell 80:919–927, 1995
Yung and Davies: A model of peritoneal mesothelium repair 2169