Respiratory Physiology Ventilation Gas exchange Oxygen uptake & utilization & removal of...
55
Respiratory Physiology Ventilation Gas exchange Oxygen uptake & utilization & removal of carbondioxide
-
Upload
thomas-allen -
Category
Documents
-
view
218 -
download
0
Transcript of Respiratory Physiology Ventilation Gas exchange Oxygen uptake & utilization & removal of...

Respiratory Physiology
VentilationGas exchange
Oxygen uptake & utilization & removal of carbondioxide
From this study you should be able to:Describe the need to breath as a part of a metabolic process
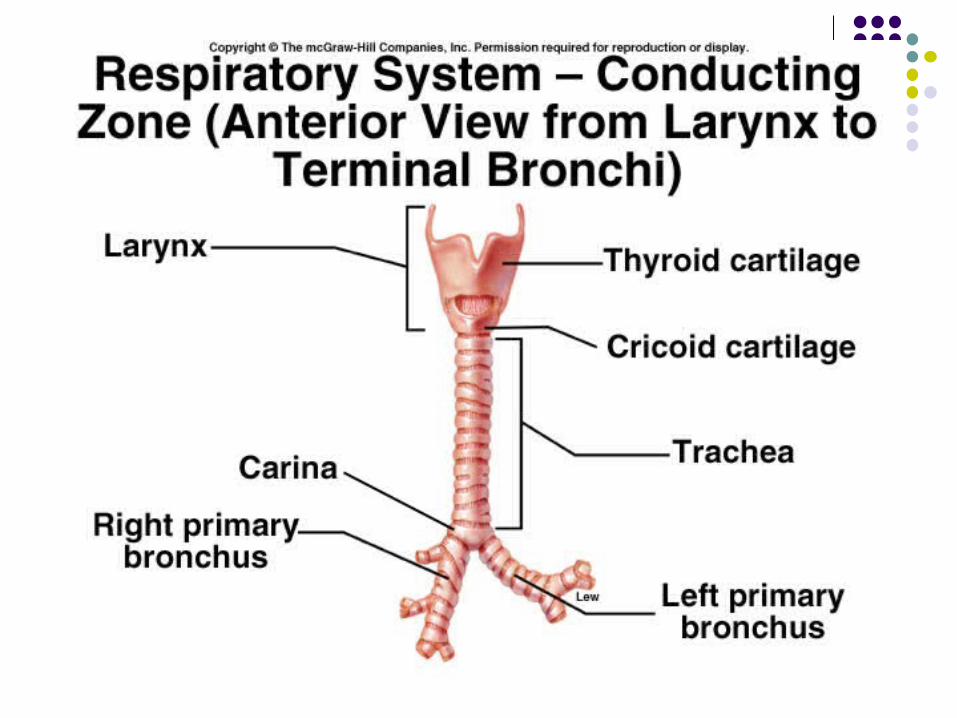
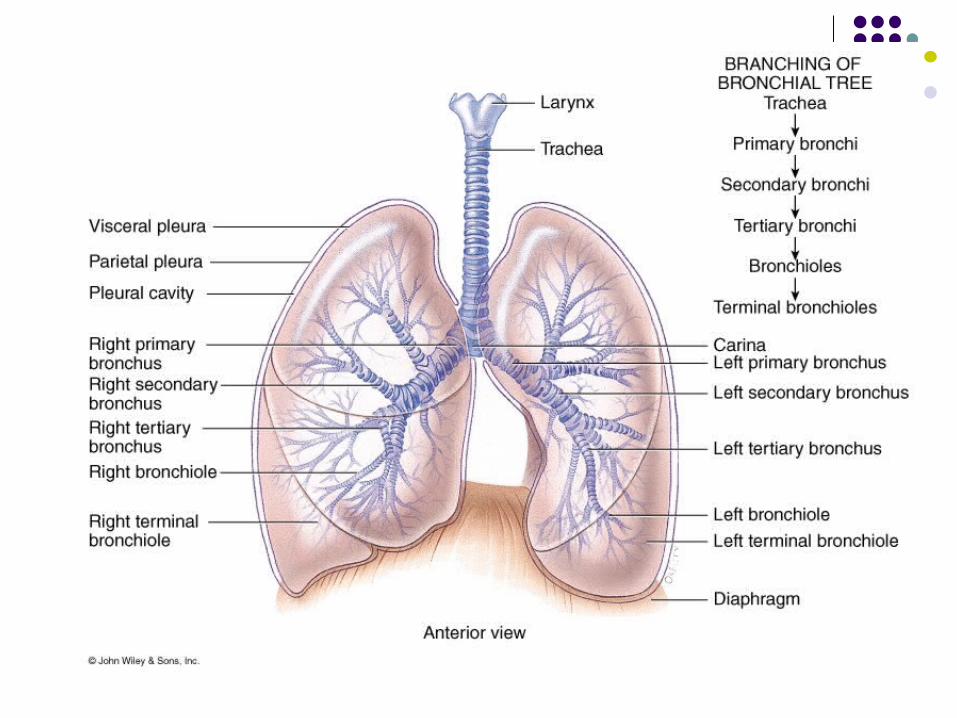
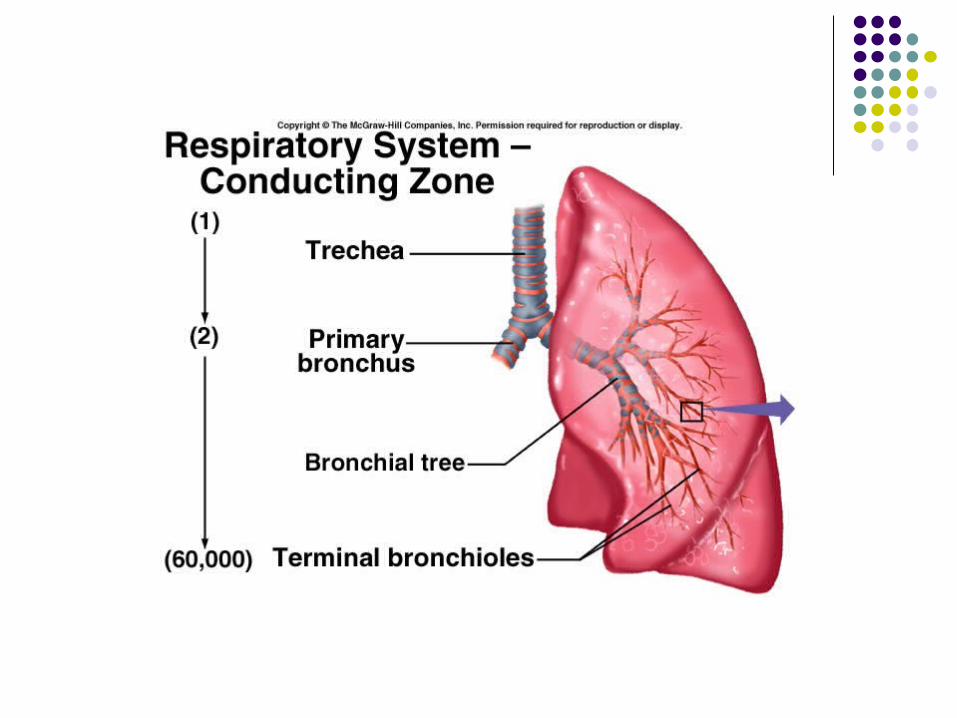
Describe the function of the respiratory conducting zone
Describe pulmonary ventilation
Briefly explain how surface tension arises & is stabilized
Define lung volumes & lung capacities
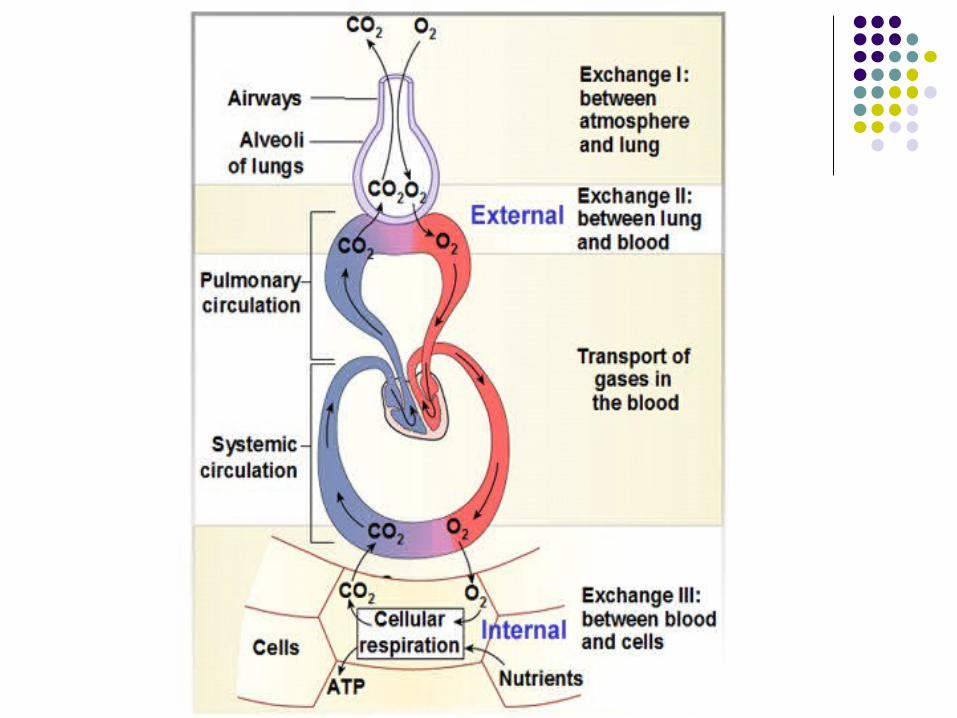
Explain gas movement during external & internal respiration
Briefly describe neurological control of breathing with description of the stimulation of central chemoreceptor
State the role of Haemoglobin in gas movement
Explain how O2 & CO2 are carried in the blood
The Need to Breath The Primary function of the respiratory system is to supply oxygen
to the tissues of the body and to remove carbondioxide and to regulate acid base balance
Oxygen helps us to release energy from food we eat
Every cell in the body needs energy
Glucose + Oxygen = Energy + Carbondioxide + water + Heat (ATP)
From the atmosphere
Waste products of
energy production
Dealing with waste products
Carbondioxide + water
CO2 plus H2O= COO + HHO
H2 CO3
A weak acid substance
CARBONIC ACID
RespirationVentilation:
Breathing.
Gas exchange: Occurs between air and blood in the lungs. Occurs between blood and tissues.
Oxygen (02 ) utilization: Cellular respiration and removal of
carbondioxide
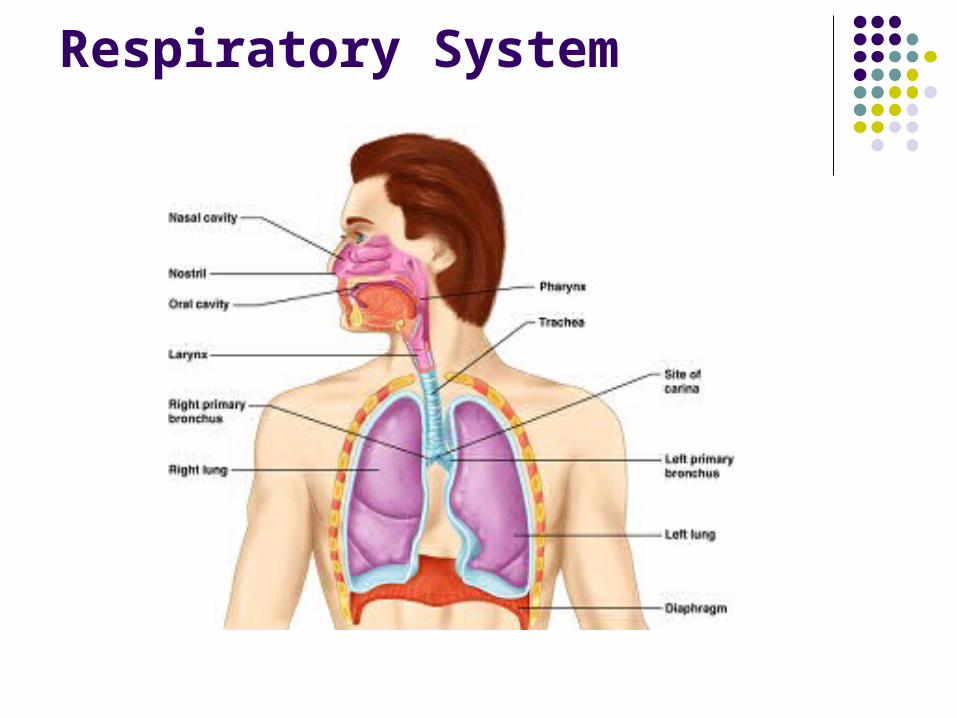
Respiratory System
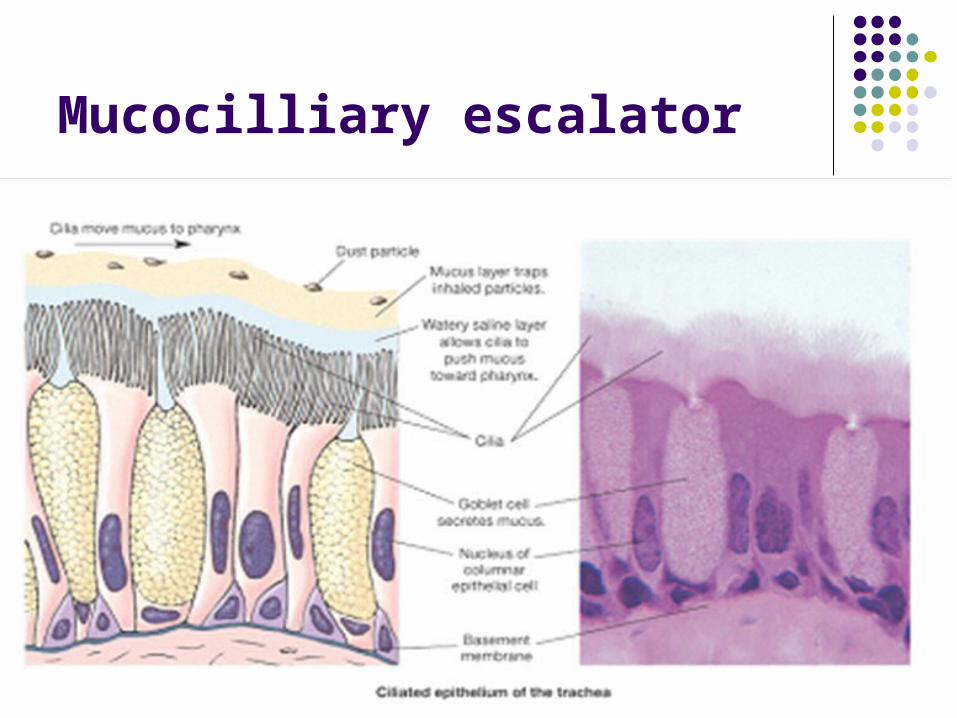
Mucocilliary escalator
Mucocilliary escalator Covers most of the trachea, bronchi,
bronchioles and nose- consists of goblet cells and ciliated columnar epithelium
There is synchronous regular beating of cilia of the mucous membrane
Wafts mucous and adhered particles (dust, bacteria etc) up towards the larynx
Mucous is then expectorated or swallowed. Involved in non-specific immunity What happens in people who smoke?

The Pleura2 layers- Visceral & Parietal.
Intrapleural space
-a film of fluid-secreted by the pleura & NO AIR
The lungs remain in contact with the chest wall –allowing them to move with the thoracic cavity
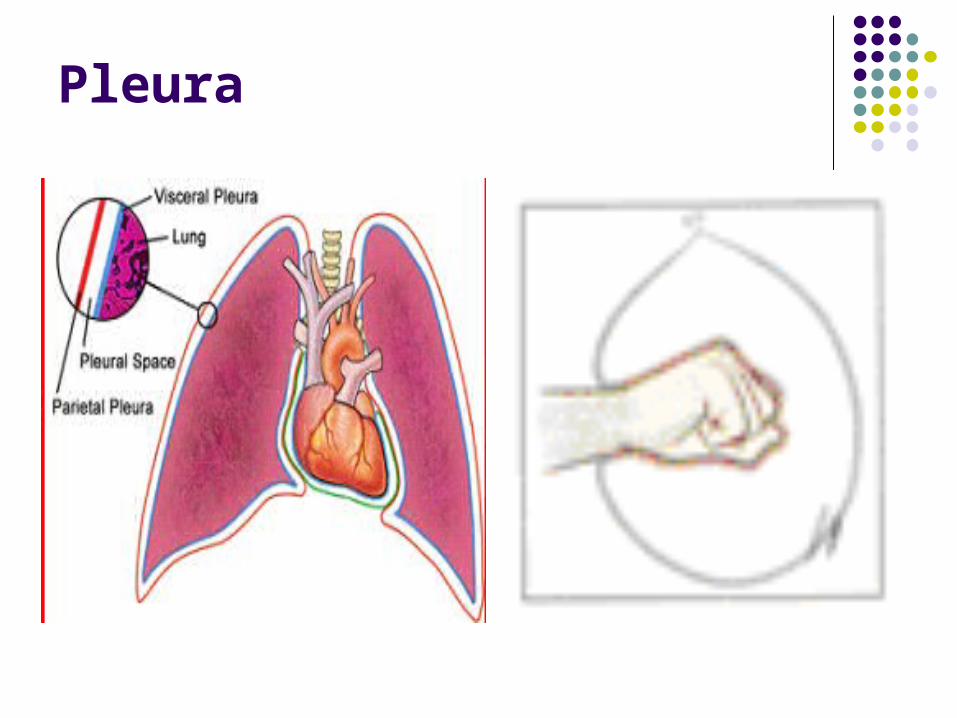
Pleura
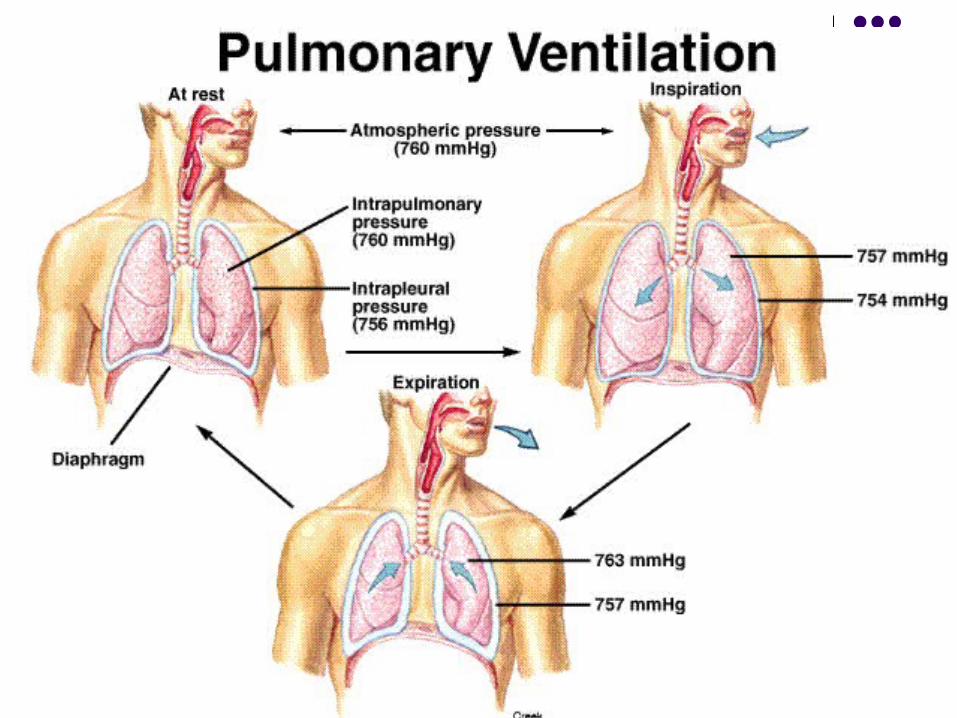
Pulmonary Ventilation:Inspiration and expiration
anim0075.exe
Quiet Inspiration - Process
Contract your diaphragm, to achieve vertical expansion of your lungs.
Contract your Intercostal Muscles, to increase thoracic volume laterally.
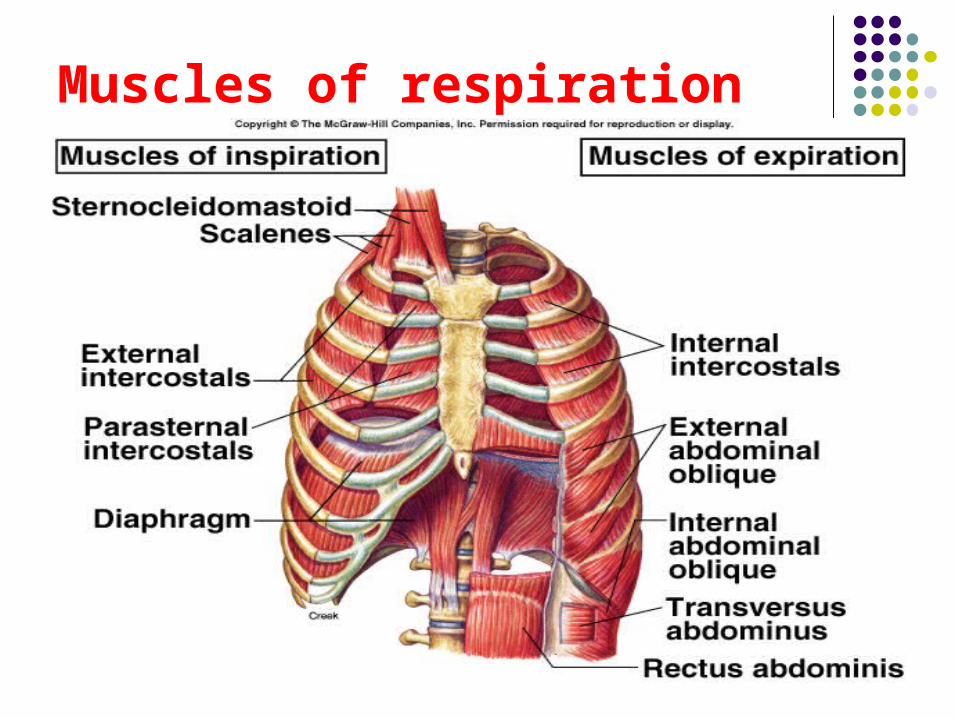
Muscles of respiration
% of gases in inspired air
Oxygen-- 20-21 Carbondioxide – 0.04 Nitrogen - 78 Inert gases – 1% Water vapour - variable
% of expired air
Oxygen – 16 Carbondioxide- 4 Nitrogen = 78 Inert gases – 1 Water vapour – more on expiration
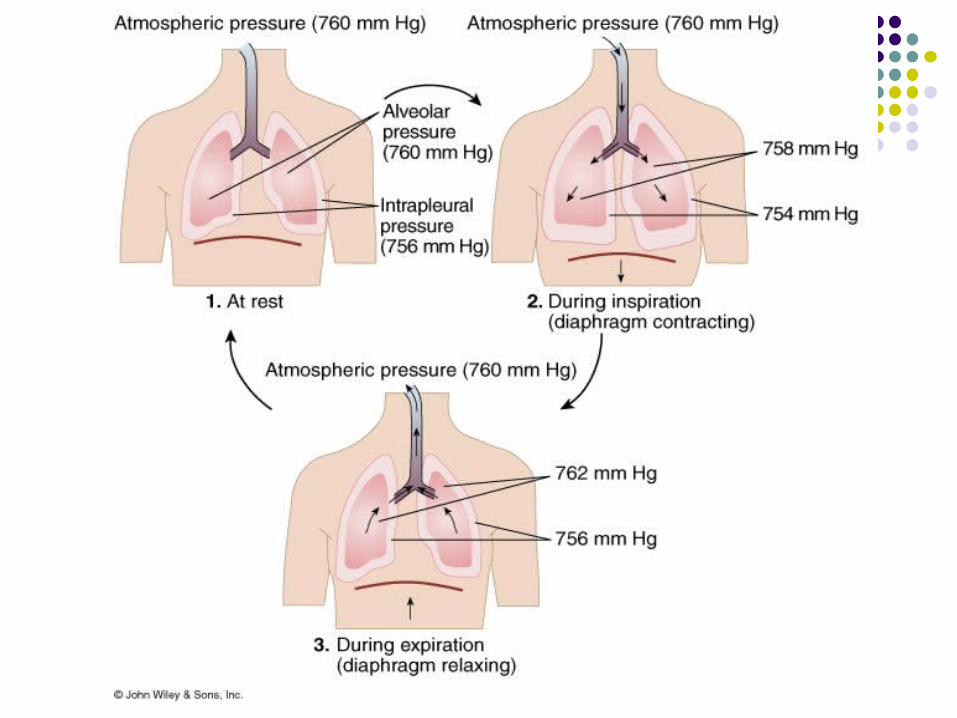
Pressure changes on Quiet InspirationAtmospheric pressure (at sea level) = 760 mmHg
The chest expands (actively)
Intrapulmonary press 757 mmHg so
air moves into the lungs
Pulmonary pressure rises by + 3 mm Hg.

Expiration Hold your breath-
After stretching the lungs (by contracting both diaphragm and thoracic muscles), the diaphragm and thoracic muscles relax & the thorax and lungs recoil
The decrease in lung volume raises the pressure inside to above 763mmHg This is greater than atmospheric pressure- so air moves out of the lungs.
Are your respiratory muscles getting tired?

Recap
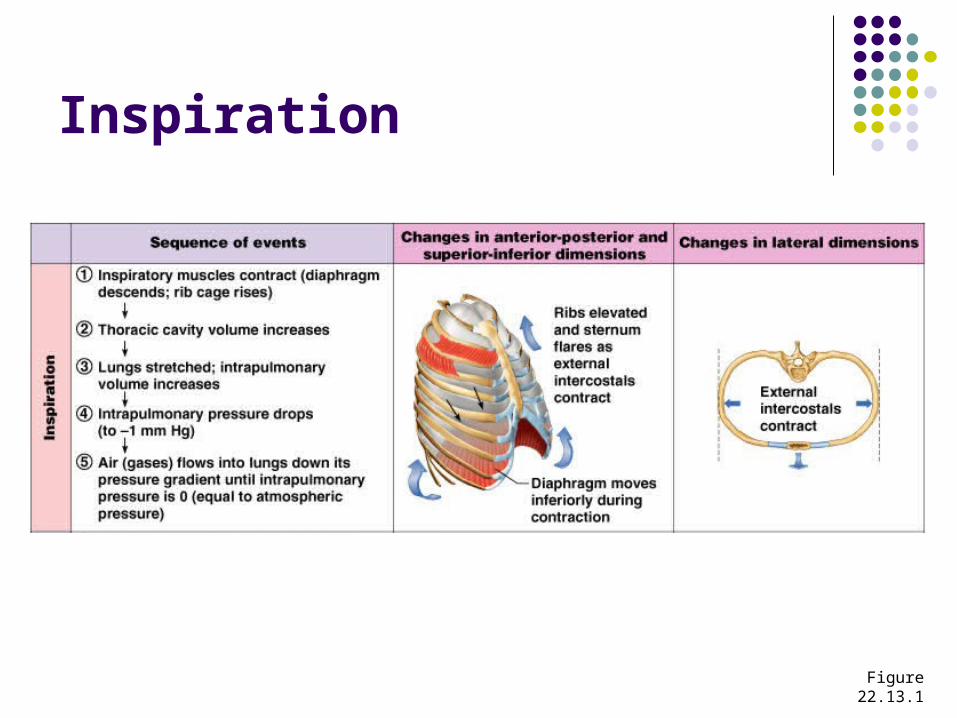
Inspiration
Figure 22.13.1
Expiration
Inspiratory muscles relax and the rib cage descends due to gravity
Thoracic cavity volume decreases Elastic lungs recoil passively and intrapulmonary
volume decreases Intrapulmonary pressure rises above
atmospheric pressure (+1 mm Hg) Gases flow out of the lungs down the pressure
gradient until intrapulmonary pressure is 0
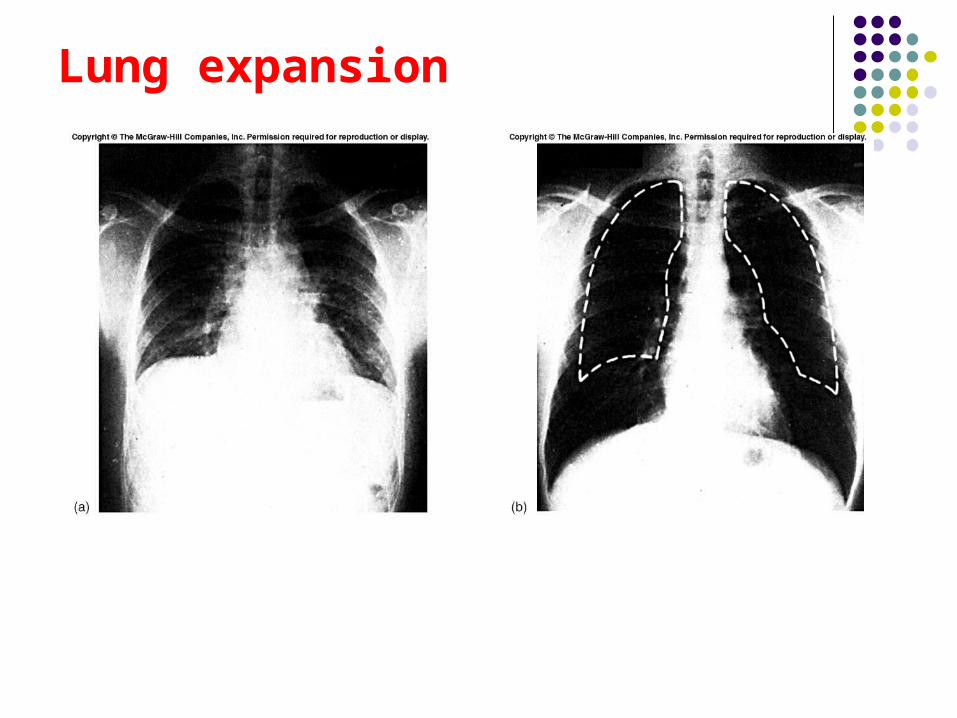
Lung expansion
BOYLE’S LAW.
THE RELATIONSHIP BETWEEN
THE PRESSURE AND VOLUME OF GASES
IS GIVEN BY BOYLE’S LAW.
IT STATES THAT WHEN THE
TEMPERATURE IS CONSTANT, THE
PRESSURE OF A GAS VARIES
INVERSELY WITH ITS VOLUME
PRINCIPLE 1Boyle’s Law
Changes in intrapulmonary pressure occur as a result of changes in lung volume.(Pressure of gas is inversely proportional to its volume).
Increase in lung volume decreases intrapulmonary
(alveolar) pressure. Air goes in.
Decrease in lung volume, raises intrapulmonary pressure above atmosphere. Air goes out.
animation
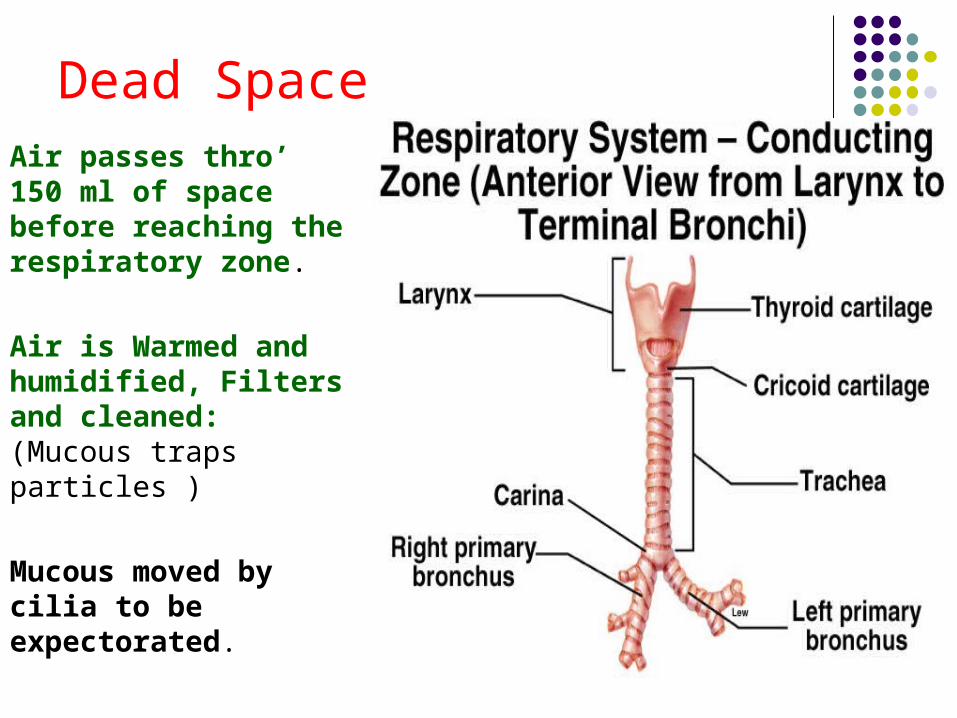
Dead SpaceAir passes thro’ 150 ml of space before reaching the respiratory zone.
Air is Warmed and humidified, Filters and cleaned: (Mucous traps particles )
Mucous moved by cilia to be expectorated.
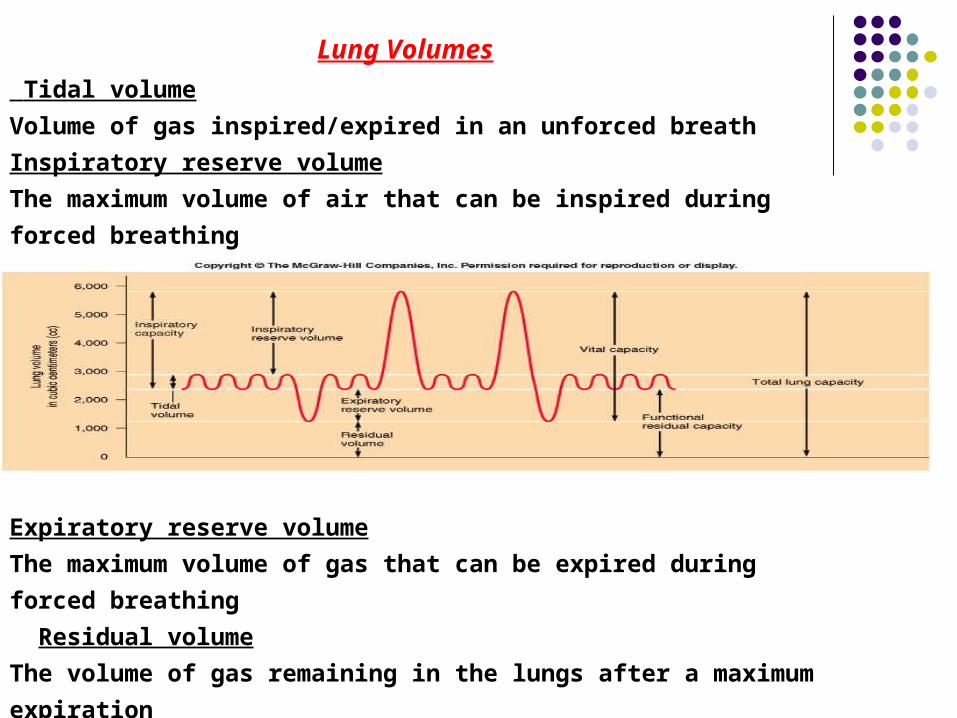
Lung Volumes
Tidal volume
Volume of gas inspired/expired in an unforced breath
Inspiratory reserve volume
The maximum volume of air that can be inspired during
forced breathing
Expiratory reserve volume
The maximum volume of gas that can be expired during
forced breathing
Residual volume
The volume of gas remaining in the lungs after a maximum
expiration
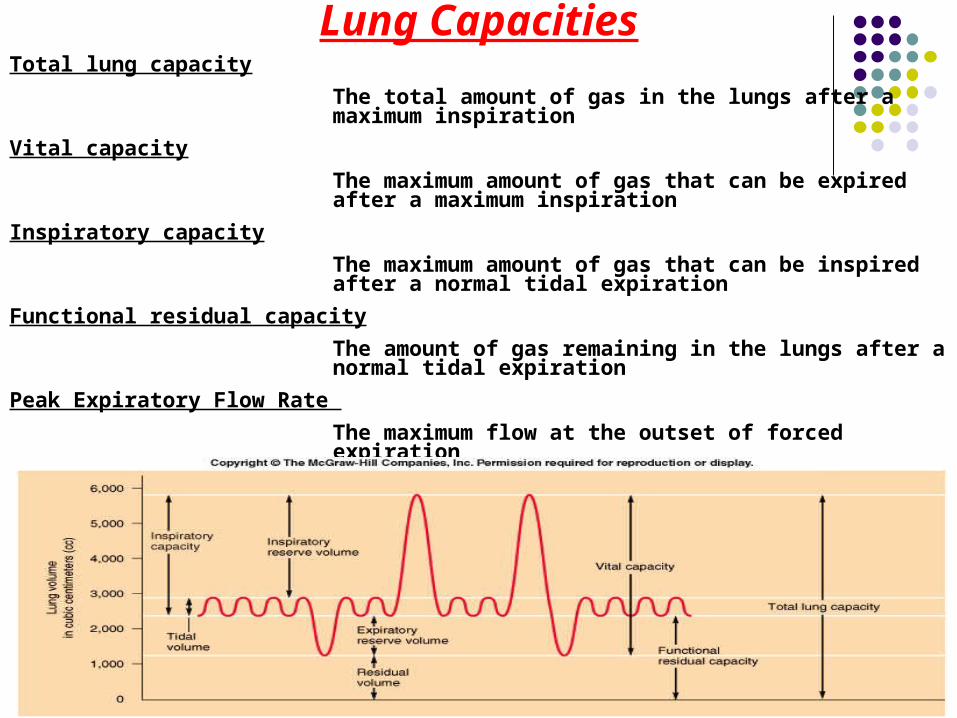
Lung CapacitiesTotal lung capacity
The total amount of gas in the lungs after a maximum inspiration
Vital capacity
The maximum amount of gas that can be expired after a maximum inspiration
Inspiratory capacity
The maximum amount of gas that can be inspired after a normal tidal expiration
Functional residual capacity
The amount of gas remaining in the lungs after a normal tidal expiration
Peak Expiratory Flow Rate
The maximum flow at the outset of forced expiration
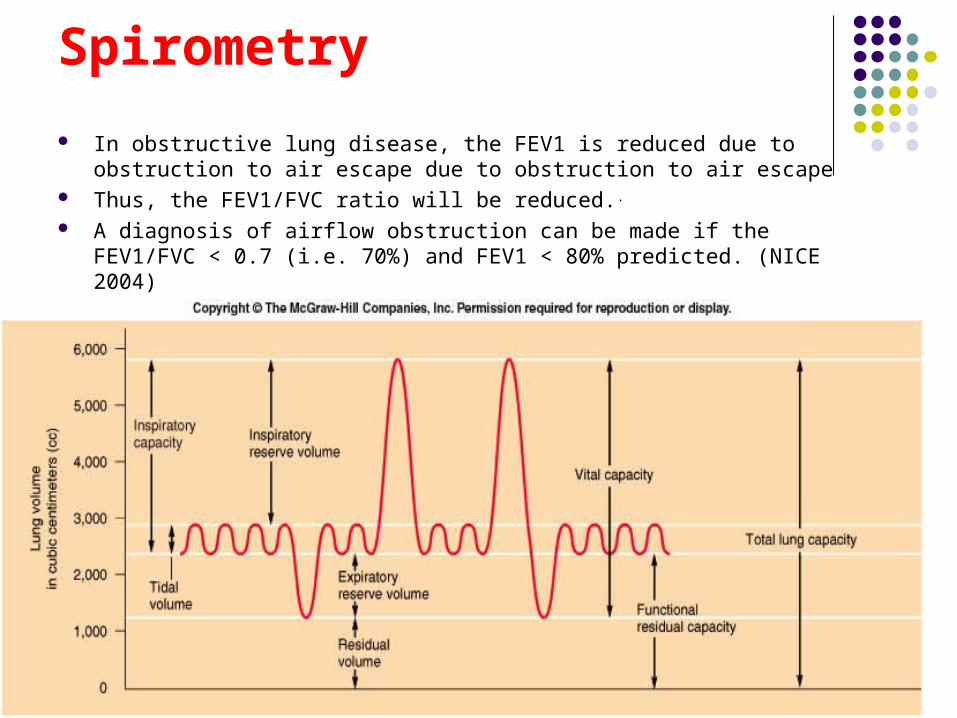
Spirometry
In obstructive lung disease, the FEV1 is reduced due to obstruction to air escape due to obstruction to air escape
Thus, the FEV1/FVC ratio will be reduced.. A diagnosis of airflow obstruction can be made if the FEV1/FVC < 0.7 (i.e.
70%) and FEV1 < 80% predicted. (NICE 2004)
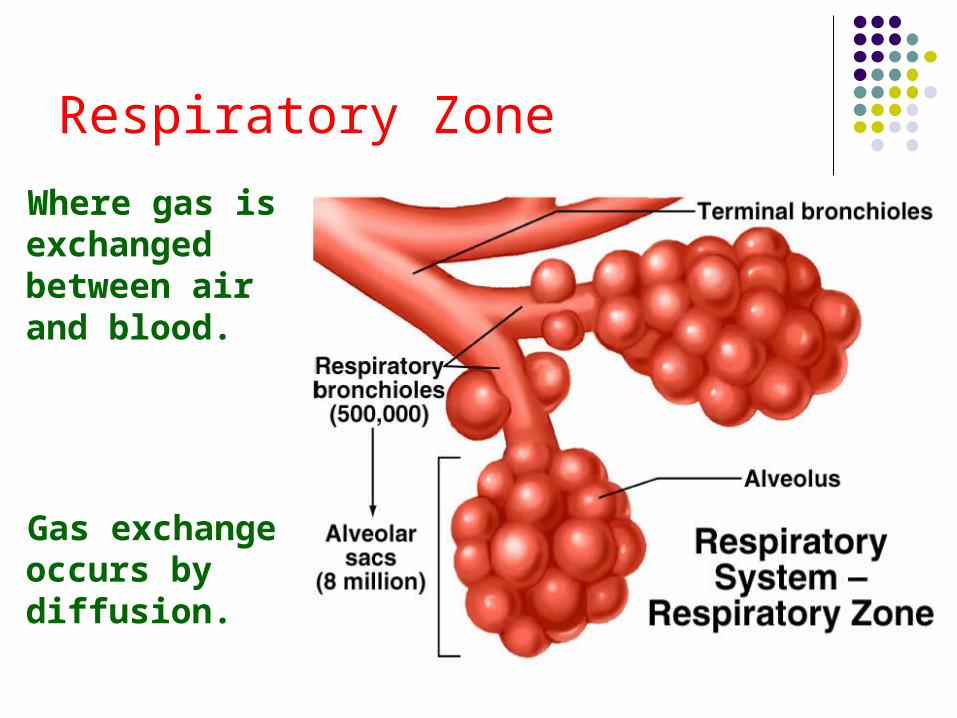
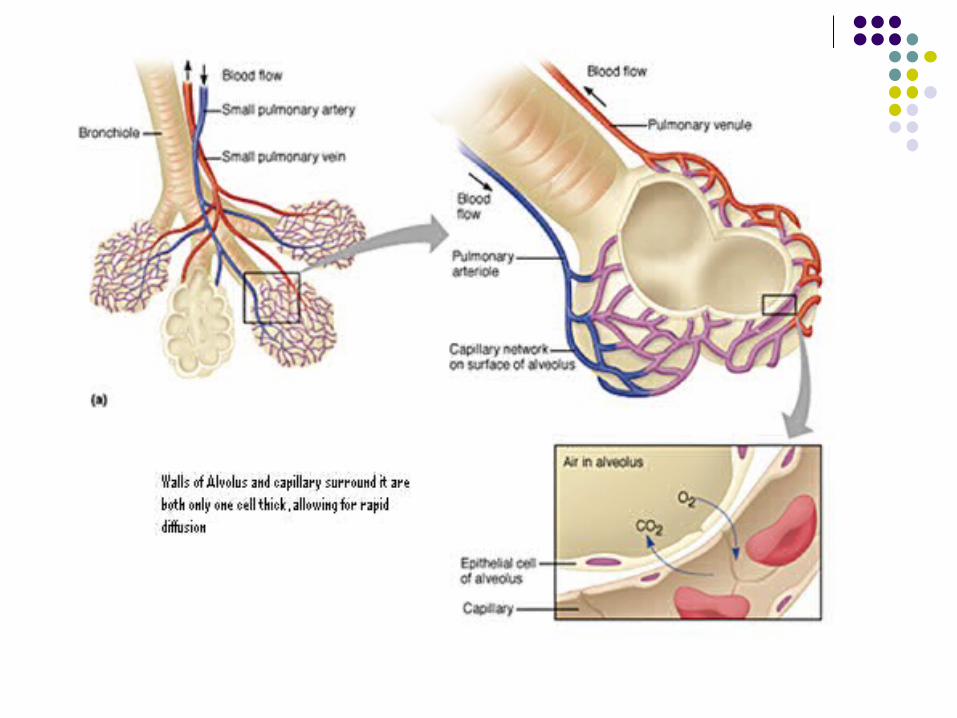
Respiratory Zone
Where gas is exchanged between air and blood.
Gas exchange occurs by diffusion.
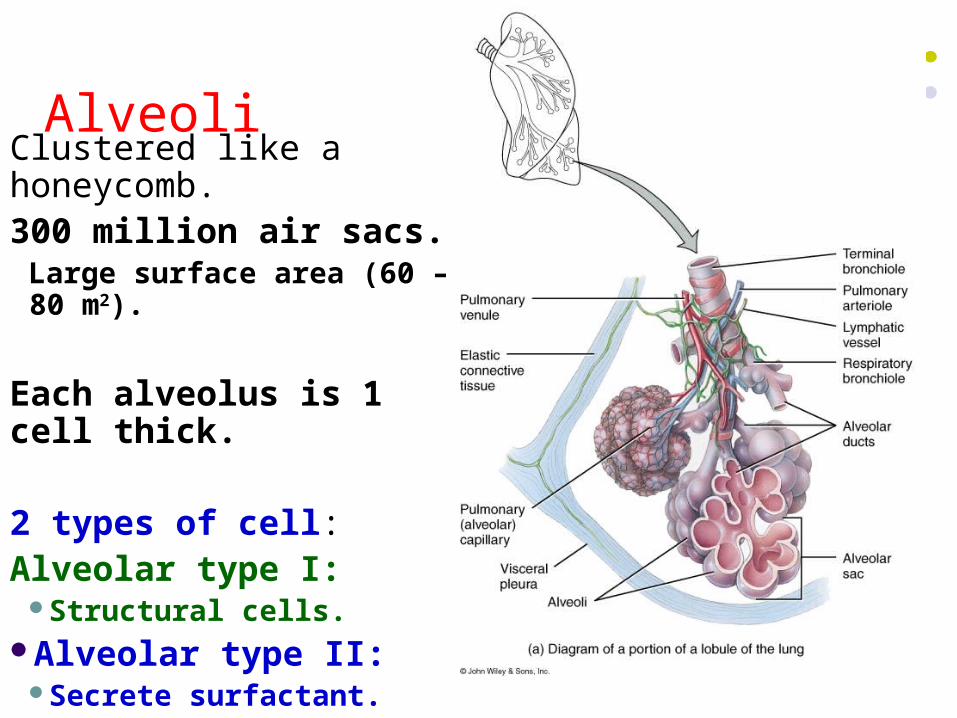
AlveoliClustered like a honeycomb.300 million air sacs.
Large surface area (60 – 80 m2).
Each alveolus is 1 cell thick.
2 types of cell:Alveolar type I:
Structural cells.Alveolar type II:
Secrete surfactant.
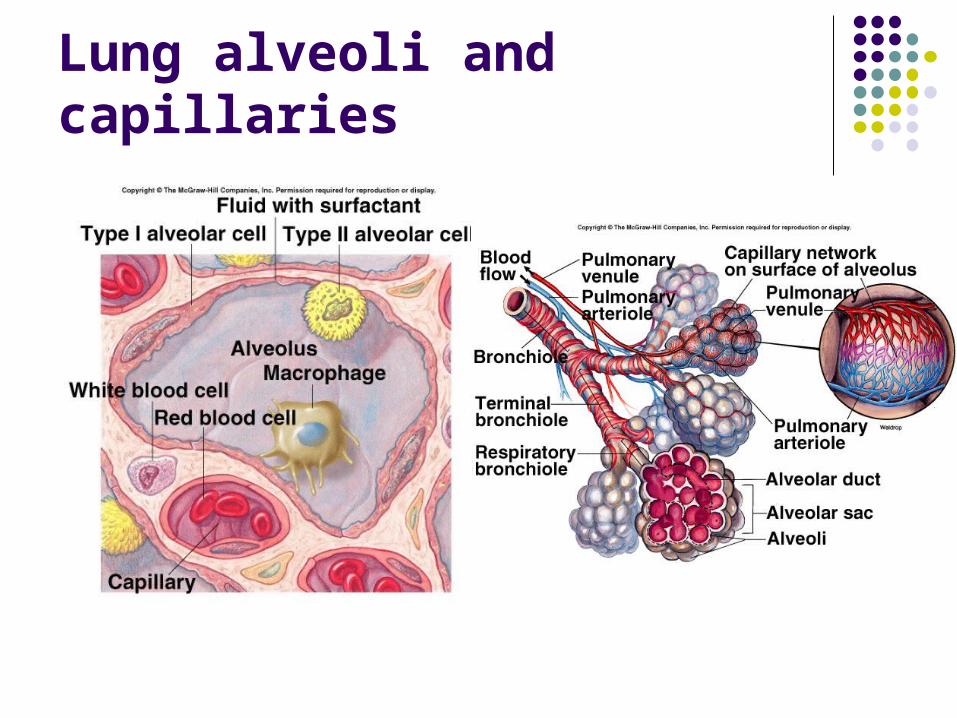
Lung alveoli and capillaries
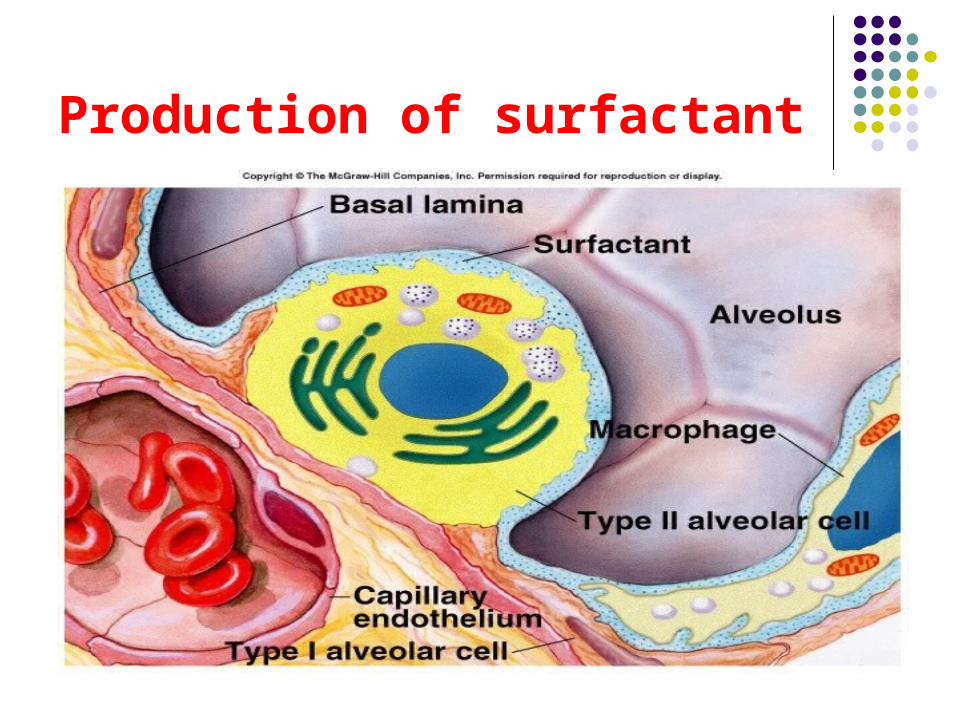
Production of surfactant
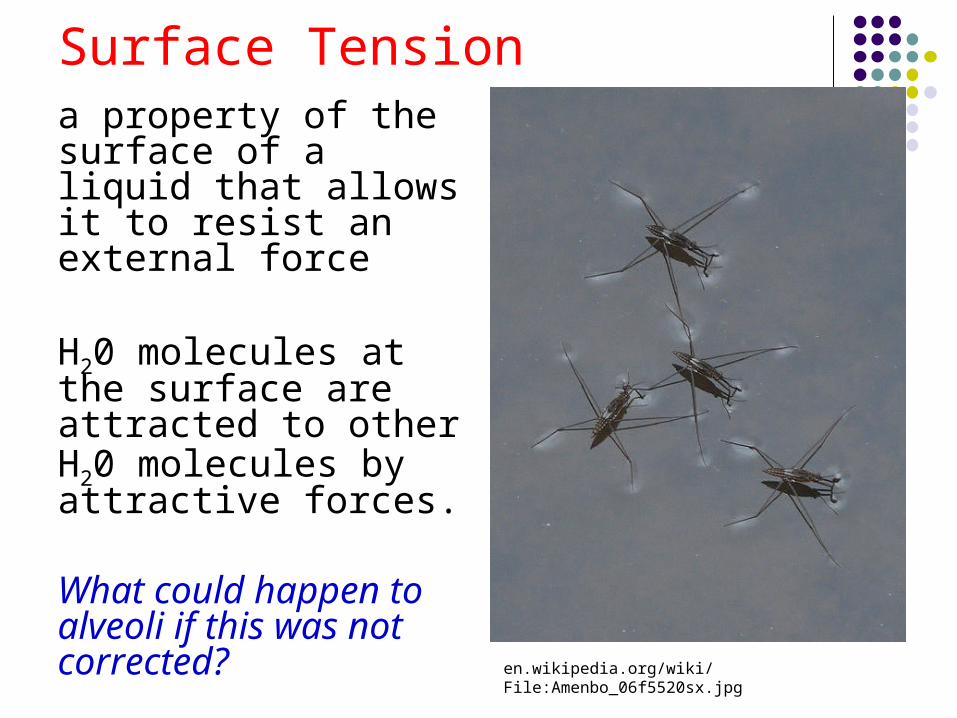
Surface Tensiona property of the surface of a liquid that allows it to resist an external force
H20 molecules at the surface are attracted to other H20 molecules by attractive forces.
What could happen to alveoli if this was not corrected?
en.wikipedia.org/wiki/File:Amenbo_06f5520sx.jpg
Surfactant- reduces surface tension
A phospholipid produced by alveolar type II cells.
Function: Lowers surface tension.
Think of a detergent
Reduces attractive forces between H20 molecules.
As alveoli radius decreases, surfactant’s ability to lower surface tension increases- so the alveolus does not collapse
Principle 2 Gases move from an area of high concentration to
an area of low concentration
This movement is termed diffusion ( a passive process)
Gas movement relies on concentration gradients
Diffusion of gases
If I set off a stink bomb in the lecture theatre, those unfortunate to be near the front (an area of high concentration) would smell it. After a while the gases would attempt to fill the whole lecture theatre- the gases would diffuse from an area of high concentration to an area of low concentration (e.g. the back of the lecture theatre) when this occurs the molecules would be so far apart that no one would smell it.
Principle 3
Gas Exchange: Dalton’s Law Total pressure of a gas mixture is = to the sum of
the pressures that each gas in the mixture would exert independently.
Think of being in a crowded lift
Now think of Partial Pressure
43
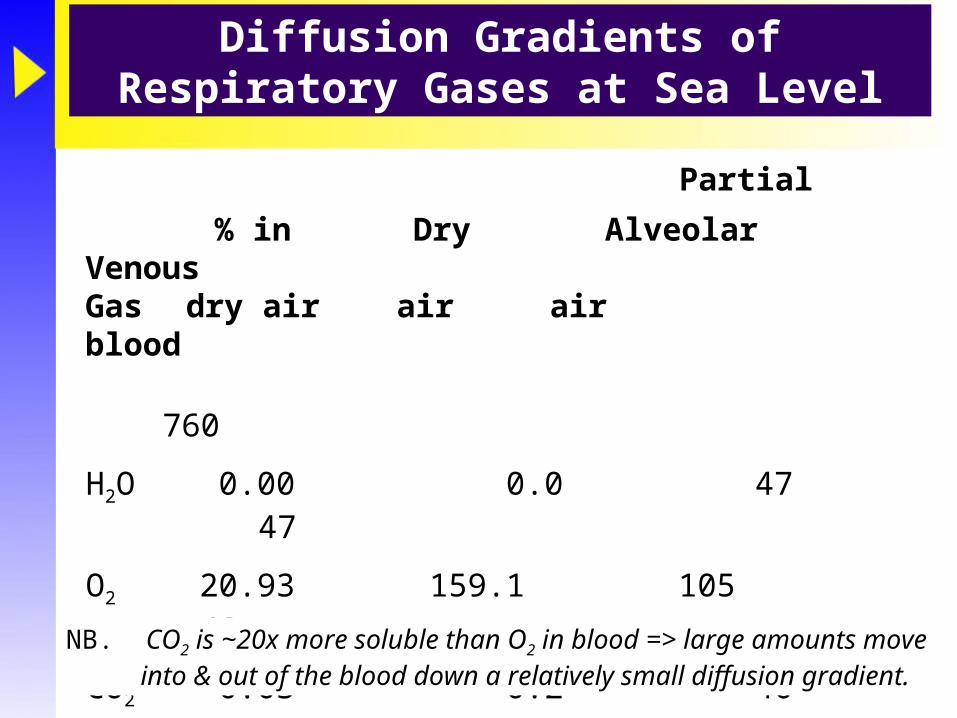
Diffusion Gradients of Respiratory Gases at Sea Level
Total 100.00 760.0 760 760
H2O 0.00 0.0 47 47
O2 20.93 159.1 105 40
CO2 0.03 0.2 40 46
N2 79.04 600.7 569 573
Partial pressure (mmHg)
% in Dry Alveolar VenousGas dry air air air blood
NB. CO2 is ~20x more soluble than O2 in blood => large amounts move into & out of the blood down a relatively small diffusion gradient.
44
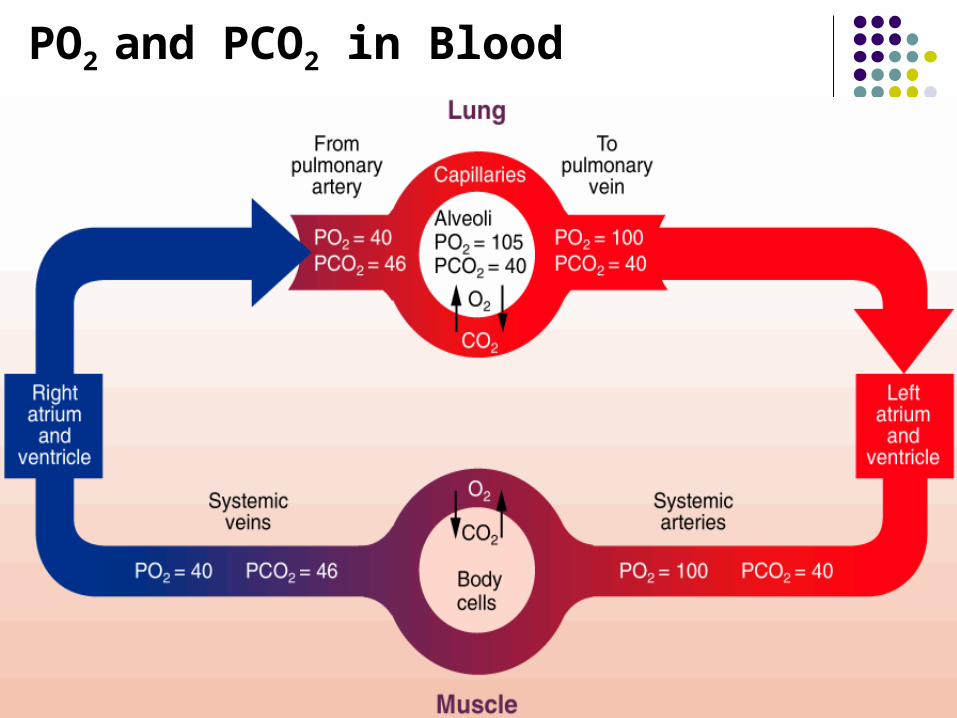
PO2 and PCO2 in Blood
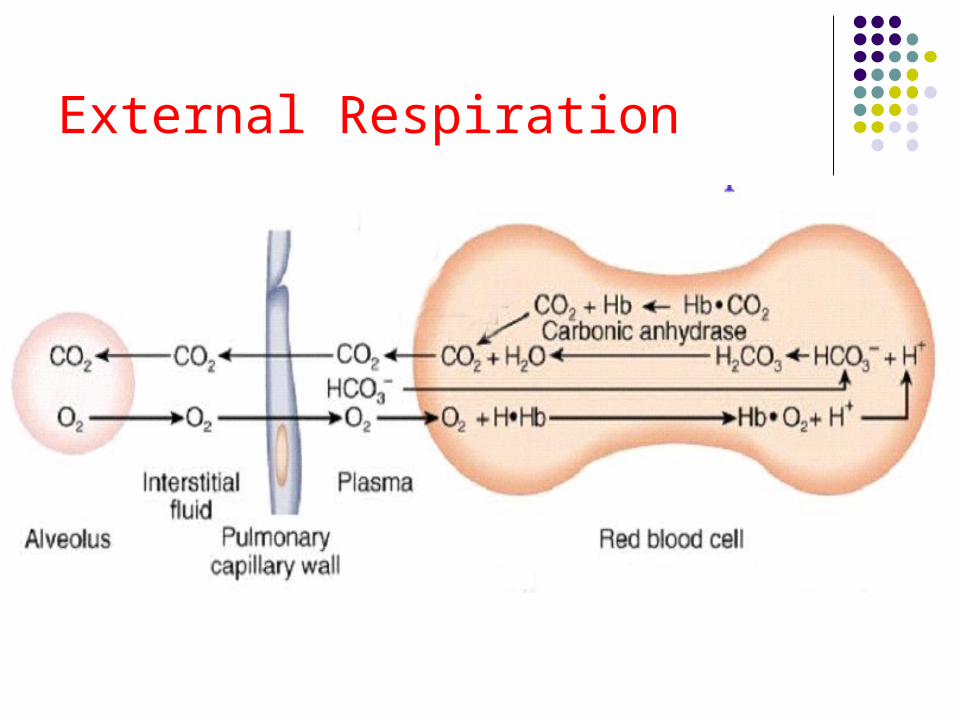
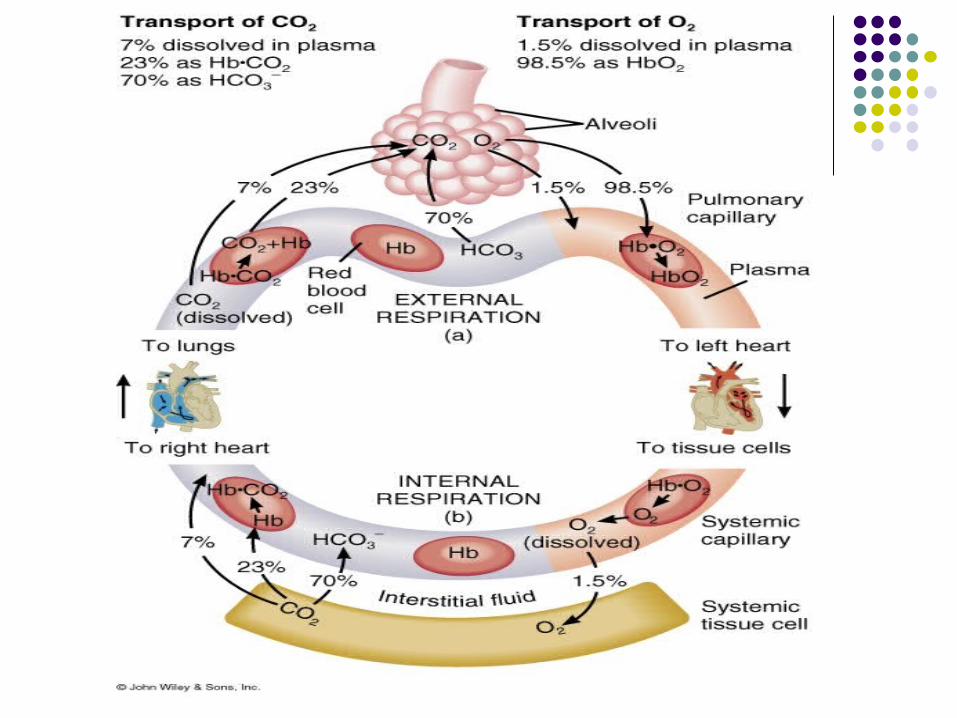
External Respiration
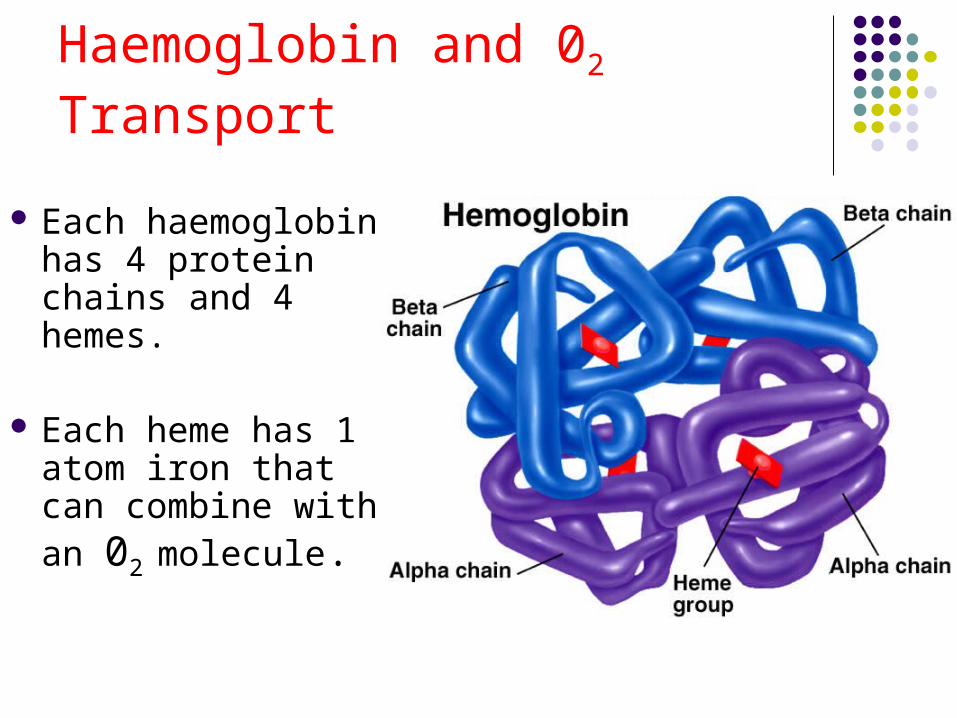
Haemoglobin and 02 Transport
Each haemoglobin has 4 protein chains and 4 hemes.
Each heme has 1 atom iron that can combine with an 02 molecule.
C02 transported in the blood:
HC03- (70%).
Dissolved C02 (10%).
Carbaminohemoglobin (20%).
CO2 is ~20x more soluble than O2 in blood. There for
large amounts of CO2 move into & out of the blood more easity
C02 Transport
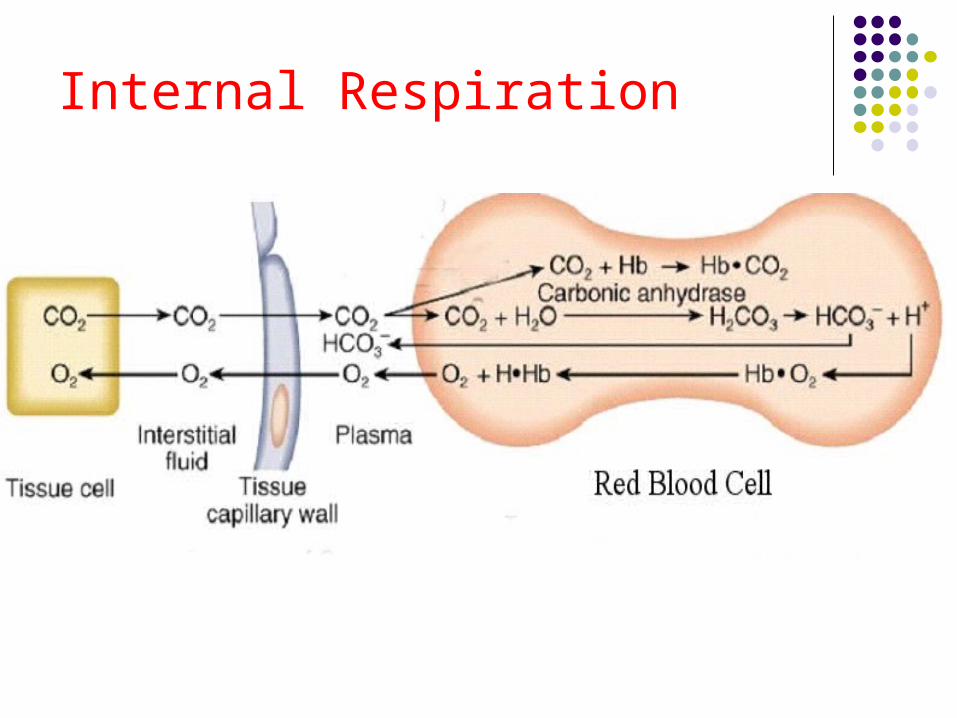
Internal Respiration
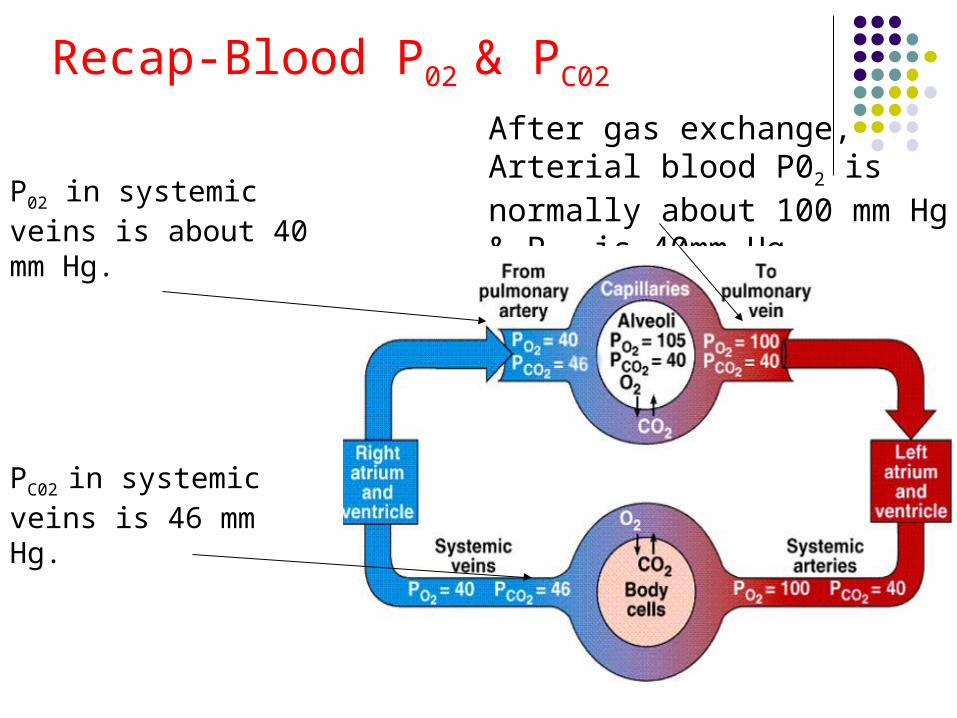
Recap-Blood P02 & PC02
P02 in systemic veins is about 40 mm Hg.
PC02 in systemic veins is 46 mm Hg.
After gas exchange, Arterial blood P02 is normally about 100 mm Hg & PC02 is 40mm Hg
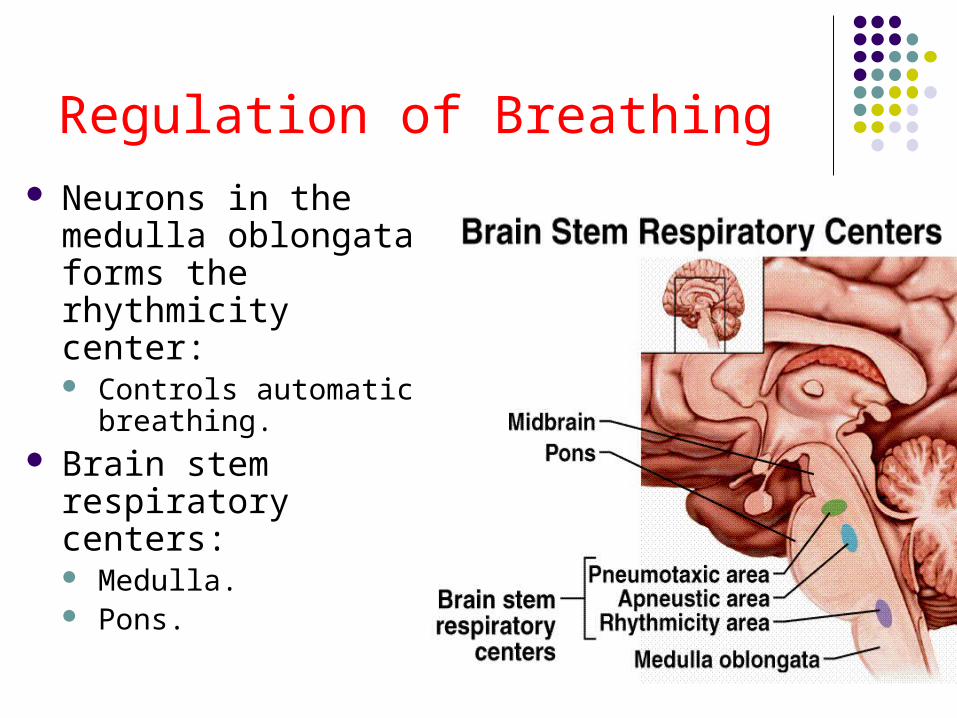
Regulation of Breathing Neurons in the medulla
oblongata forms the rhythmicity center: Controls automatic
breathing. Brain stem respiratory
centers: Medulla. Pons.

Chemoreceptor Control
C02 + H2O
H+ cannot cross the blood brain barrier.
C02 can cross the blood brain barrier and will form Carbonic acid & then H+
H+H2C03HC03
What is this?Bicarbonate
H+ is the trigger for the chemoreceptors
This is Carbonic acid
Clinical relevance point 1Haemoglobin production controlled by
erythropoietin.
(Produced re P02 delivery to kidneys).
Loading/unloading of gas on Hb depends on: Hb level & capacity in the blood Enzymes: ↑ 2,3 DPG - increases unloading of O2 Temp: ↑Heat increases unloading of O2 Acid/base: ↓pH increases unloading of O2
This enzyme is produced when Hb is low
Questions What are the three functions of the respiratory system? In order, list all of the components of the respiratory system What is the function of epiglottis? What is the function of the cilia in the trachea? What surrounds the trachea and helps to keep it open? What is the role of surfactant in the lungs? What is the composition of air in %. Which law governs movement of gases in out of the lungs? A) Boyles law
or b) process of diffusion Where are the chemo-receptors situated? How does the respiratory system respond to increase in CO2 in the blood? In what form, can carbondioxide be carried in the blood? – see slide no 49
for answer In what form can Oxygen be carried in the blood? – see slide no 49 for
answer What is the name of chemical produced by the kidneys which stimulates
production of Red Blood Cells from Red Marrow?