
Respiratory disorder and periodontitis
62
-
Upload
dr-vartika-srivastava -
Category
Health & Medicine
-
view
156 -
download
4
Transcript of Respiratory disorder and periodontitis


Presented by:Dr. Vartika Srivastava
PG II yr

Introduction
Human Respiratory System
Defence Mechanism Of Respiratory System
Respiratory Diseases -------- 1.Bacterial Pneumonia 2.Chronic Obstructive Pulmonary Diseases
Basis Of Relating Periodontal Disease With Respiratory Disorders
Oral Bacterial As Etiologic Agents Of Respiratory Infection
Dental Plaque As A Reservoir Of Respiratory Pathogens
Potential Mechanisms Of Action Of Oral Bacteria In The Pathogenesis Of Respiratory Infection
Prevention Of Oral Colonization By Potential Respiratory Pathogens
Conclusion
References

Introduction
??????????

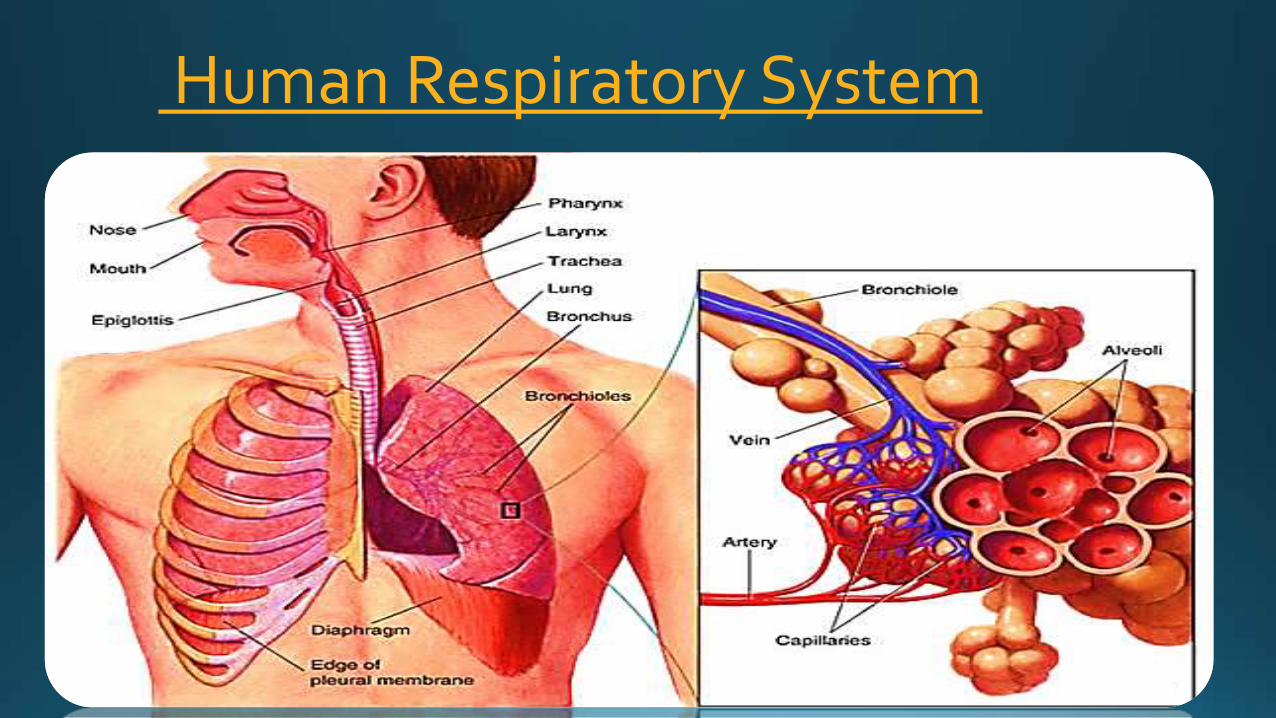
Human Respiratory System

Defence Mechanism Of Respiratory System
•
•

•
•

Role of lungs in defence mechanism :

Leukocytes Macrophages Mast cellsNatural
killer cells Dentritic
cells

Respiratory Diseases
Bacterial Pneumonia
Chronic Obstructive Pulmonary
Disease (COPD)
Bacterial pneumonia


-

Clinical features:
-
-
-
-
-
-

Chronic Obstructive Pulmonary Disease (COPD)
• Chronic bronchitis


• Incidence

Etiology:
••••

Clinical features:

Emphysema
Etiology:
Clinical features:

Basis Of Relating Periodontal Disease With Respiratory Disorders



Oral Bacterial As Etiologic Agents Of Respiratory Infection

Porphyromonas gingivalis, Bacteroides gracilus,Bacteriodies oralis, Bacteroies buccae, Eikenellacorrodens, Fusobacterium nucleatum, Fusobacteriumnecrophourm, Actinobacillus actinomycetemocomitans,Paptostreptococci, Clostridum, & Actinomyces.
• Viridans streptococci


Oral bacteria may also have a role in the exacerbations of COPD.
Nelson S et al. (1986) found that oral anaerobes such as P.gingivalis can cause marked inflammation when instilled into the lungs of laboratory animals.
Torres A et al.(1996) found Virdans streptococci to be the cause of pneumonia in 4% of COPD patients.
Grollier G et al. (1996) found a relationship b/w the systemic humoral response to Prevotella species (bacteria associated with periodontal disease) and ventilator-associated pneumonia in hospitalized patients.

Dental Plaque as a Reservoir of Respiratory Pathogens

Scannapieco FA et al.(1996,1998)

Fourrier F et al. (1998) conducted a prospective study of 57 consecutive patients admitted to a MICU during a 3-month period & assessed the colonization of dental plaque by respiratory pathogens.
The amount of dental plaque on the teeth of in patients increased over time, as did the proportion of respiratory pathogens in their dental plaque.
A high concordance was found b/w respiratory colonization of dental plaque by pathogens & the presence of the same pathogens in tracheal aspirate cultures, & b/w salivary & dental plaque cultures.


Oral status and COPD
Scannapieco FA et al.(1998)

POTENTIAL MECHANISMS OF ACTION OF ORAL BACTERIA IN
THE PATHOGENESIS OF
RESPIRATORY INFECTION

1)Aspiration of oral pathogens.
2) Periodontal disease-associated enzymes in saliva maymodify mucosal surfaces to promote adhesion &colonization by respiratory pathogens.
3) Periodontal disease-associated enzymes may destroysalivary pellicles on pathogenic bacteria.
4) Cytokines originating from periodontal tissues may alterrespiratory epithelium to promote infection by respiratorypathogens

Aspiration of oral pathogens
Chronic mechanical aspiration of small amounts of saliva & oral particulate matter takes place in all human beings.
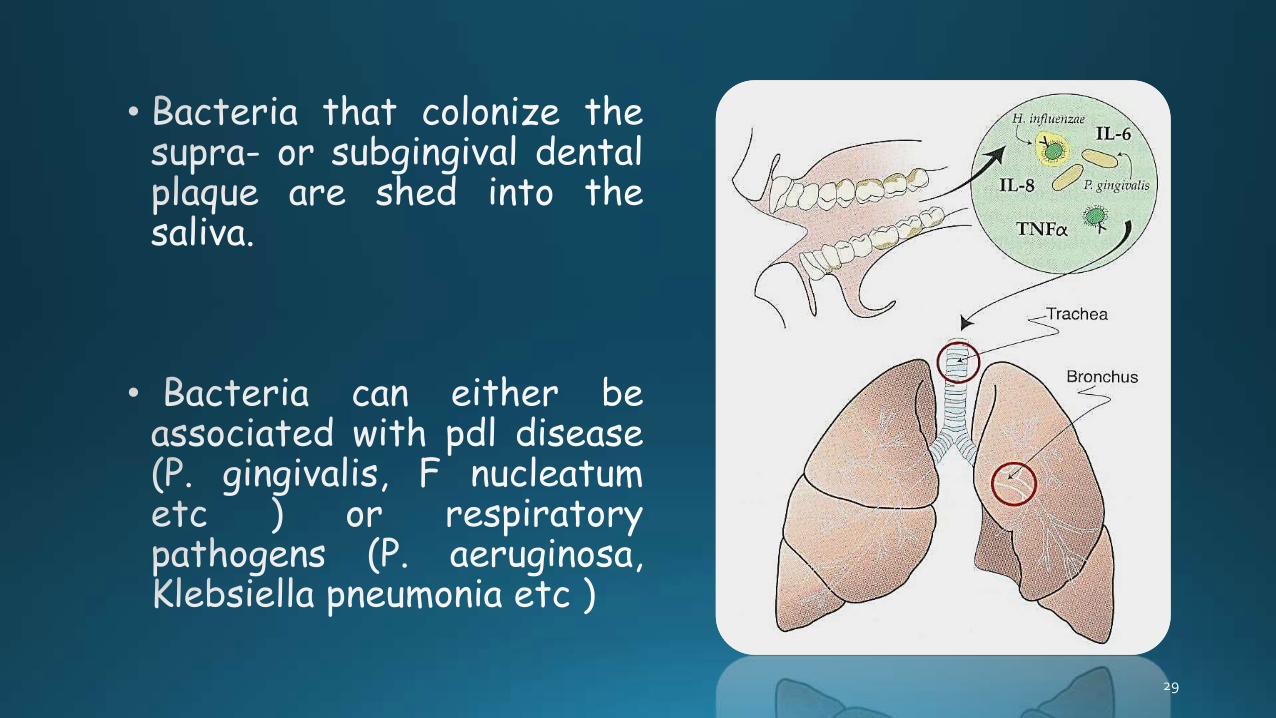
The most common aspirate is the patient's own saliva. If saliva also contains high counts of bacteria, these are also aspirated.
The aspiration of oral contents is probably one of the most important links b/w oral & periodontal disease & respiratory infection.
The bacterial content of saliva is varied, & high counts of many species of bacteria in saliva give rise to the suspicion that direct transfer of bacteria from the mouth to the airways is occurring.

Normal oral flora , including , A. actinomycetemcomitans &anaerobes such as P.gingivalis and Fusobacterium spp., canbe aspirated into the lower airways to cause pneumonia.
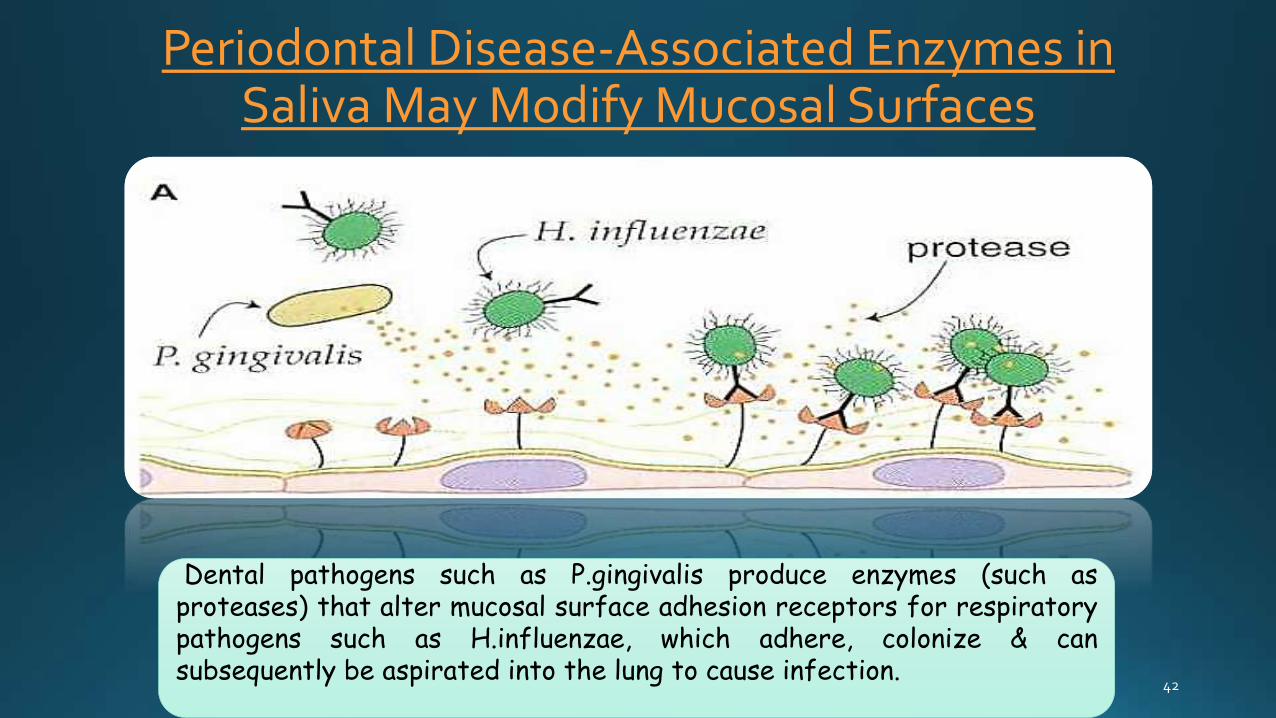
Periodontal Disease-Associated Enzymes in Saliva May Modify Mucosal Surfaces
Dental pathogens such as P.gingivalis produce enzymes (such asproteases) that alter mucosal surface adhesion receptors for respiratorypathogens such as H.influenzae, which adhere, colonize & cansubsequently be aspirated into the lung to cause infection.

Woods DE et al.(1981) showed that Trypsin treatment of epithelial cells from non-colonized patients in vitro resulted in increased adhesion by respiratory pathogens, suggesting a mucosal alteration, perhaps the loss of fibronectin from the epithelial cell surface, promoted respiratory pathogens adhesion.
A direct relationship has been found b/w the ability of saliva to degrade fibronectin & oral hygiene status by Gibbons RJ & Etherden I (1986) , subjects practicing meticulous oral hygiene (dental hygiene students) had very low levels of salivary fibronectin degrading enzymes. In contrast, saliva samples collected from laboratory workers having less than ideal oral hygiene had higher amounts of enzyme activity.

Destruction of Protective Salivary Pellicles by Oral Bacteria
P.gingivalis produce enzymes that degrade the salivary molecules thatnormally form pellicle on the pathogens which prevents them fromadhering to mucosal surfaces.

Salivary Cytokines May Alter Respiratory Epithelium



Darveau et al. (1998) showed that IL-8 is secreted bygingival epithelial cells in response to components of thenormal oral flora. In contrast, P. gingivalis stronglyinhibited IL-8 accumulation from gingival epithelial cells.Inhibition was associated with a decrease in mRNA forIL-8.

PREVENTION OF ORAL COLONIZATION BY POTENTIAL RESPIRATORY PATHOGENS
Because of the key role that oropharayngeal bacteriacolonization plays in the pathogenesis of bacterialpneumonia, several methods have been proposed to reduceor eliminate colonization in susceptible patients, such asthose on mechanical ventilation..
Selective digestive decontamination (SDD)
Antibiotics topically applied to the surfaces of thegastrointestinal tract, including the oral cavity to reducethe carriage of pathogenic bacteria and thus preventrespiratory infection. For E.g.:- the use of lozengescontaining polymyxin B, tobramycin, and amphotericin Bdiminish oral colonization by gram –ve bacilli

Pugin J et al (1991) focused on the elimination oforopharyngeal colonization by pathogens & thesubsequent development of pneumonia.
They used topical oropharyngeal antibiotics (versustopical placebo) in mechanically ventilated patients.
Oropharyngeal colonization by aerobic gram –vebacilli and S. aureus and also pneumonia rates weresignificantly reduced in the treated populationversus the placebo group.

Chlorhexidine• Inhibit dental plaque formation, gingivitis, & oral mucosal
ulcerations.
• It also inhibits the production of proteases by subgingivalbacteria, by inhibiting protease activity, chlorhexidine may diminish the potential of these enzymes to process oral surfaces to expose “cryptitopes” that may act as receptors for bacterial adhesions.

Balbuena L et al. (1998) - chlorhexidine has been shown to reduce plaque & salivary levels of bacteria by upto 85%.
Nilsson G et al (1989) - chlorhexidine gluconate reduce transfer of group B streptococci from mother to infant during parturition

In epidemiological terminology, smoking is referred to as a confounder factor.
Smoking is most strongly associated with lung cancer, followed by COPD, CHD and stroke.
Periodontitis mimics this pattern step by step: periodontitis is most strongly associated with lung cancer, followed by COPD, CHD and stroke.
In nut shell Periodontitis may cause systemic diseases only in the presence of smoking; or, periodontitis may worsen the ill effects of smoking on systemic health.

Peter K P et al in 2013 suggested that poor periodontal health is associated with obstructive lung
disease.
Study included 500 individuals consisting of 102 patients (case group) having COPD and 399 individuals
as controls.
Individuals in case group had significantly higher CAL, PD and OHI

Souto R et al in August 2014 investigated the prevalence of P. aeruginosa and Acinetobacter spp. in
subgingival biofilm and saliva of subjects with periodontal disease or health.
P. aeruginosa and Acinetobacter spp. are important pathogens associated with late nosocomial pneumonia in
hospitalized and institutionalized individuals.
He concluded that Poor oral hygiene, smoking and the presence of P. aeruginosa are strongly associated with
periodontitis.

Zhou X et al in JUNE 2014 did a study to evaluate the direct effects
of periodontal therapy in Chronic Obstructive Pulmonary Disease (COPD) patients with
chronic periodontitis (CP).
Preliminary results from this pilot trial suggest that periodontal therapy in COPD
patients with CP may improve lung function and decrease the frequency of COPD
exacerbation.
CONCLUSION
References Periodontal Medicine Rose, Genco, Mealey & Cohen.
Davidson’s Principles and Practice of Medicine. 21st edition.
J Periodontal 1999 ; 70 :793-802.
Braz J Microbiol 2014 Aug 29;45(2):495-501
J Clin Periodontol 2014 Jun;41(6):564-72
J Periodontol 2013 Dec;84(12):1717-23
Ann. Periodontal 2000; 6: 66-70,78-90.
J Periodontal 1996; 67: 1114-1122.
Ann. Periodontal 2003; 8 :54-69.
Ann. Periodontal 1998; 3 : 251-275



















