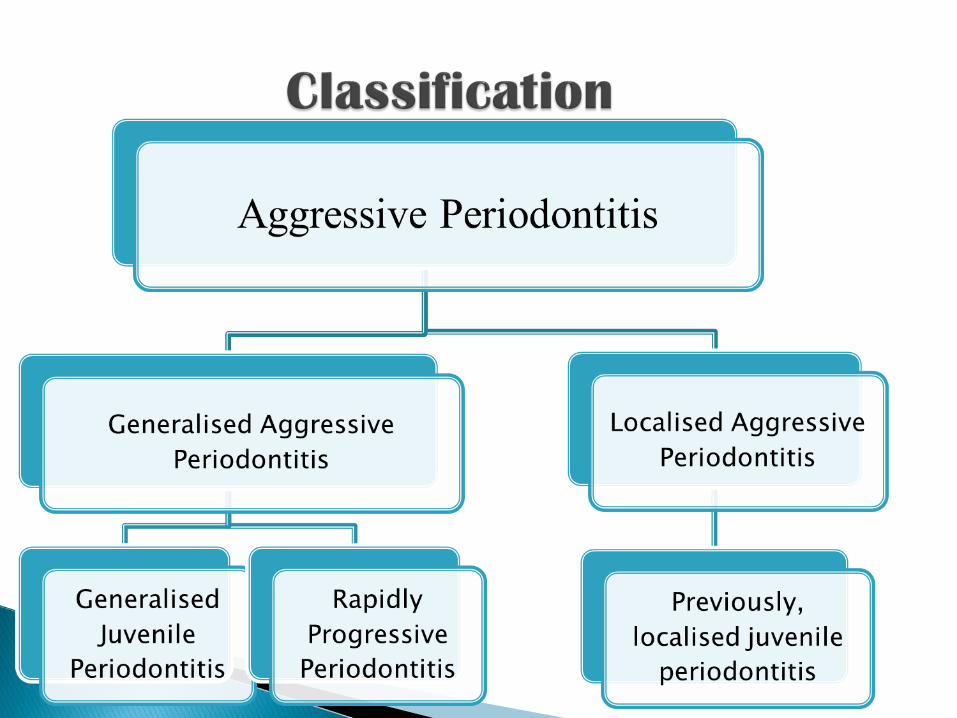
Aggressive periodontitis
25
Kingshuk Mazumder
-
Upload
kingshuk-mazumder -
Category
Health & Medicine
-
view
111 -
download
13
Transcript of Aggressive periodontitis
Kingshuk Mazumder
Periodontitis is defined as an inflammatory disease of the supporting tissues of teeth, caused by specific micro organisms, resulting in progressive destruction of PDL and alveolar bone, with increased depth formation, and recession of teeth.
Generally affects systemically healthy individuals, less than 30 years of age.
Universally distinguished from chronic periodontitis, by:
1. Age of onset,2. Rapid rate of disease progression,3. The nature and composition of the associated subgingival
microflora,4. Alterations in the host’s immune response, and5. A familial aggregation of diseased individuals.6. In addition, there is a racial predilection of the disease among
African Americans.
Age of onset is, at around puberty.
Clinically characterized as having “localized first molar/incisor presentation, with inter-proximal attachment loss, on at least two permanent teeth, one of which is a first molar and involving no more than 2 teeth, other than first molars and incisors.”
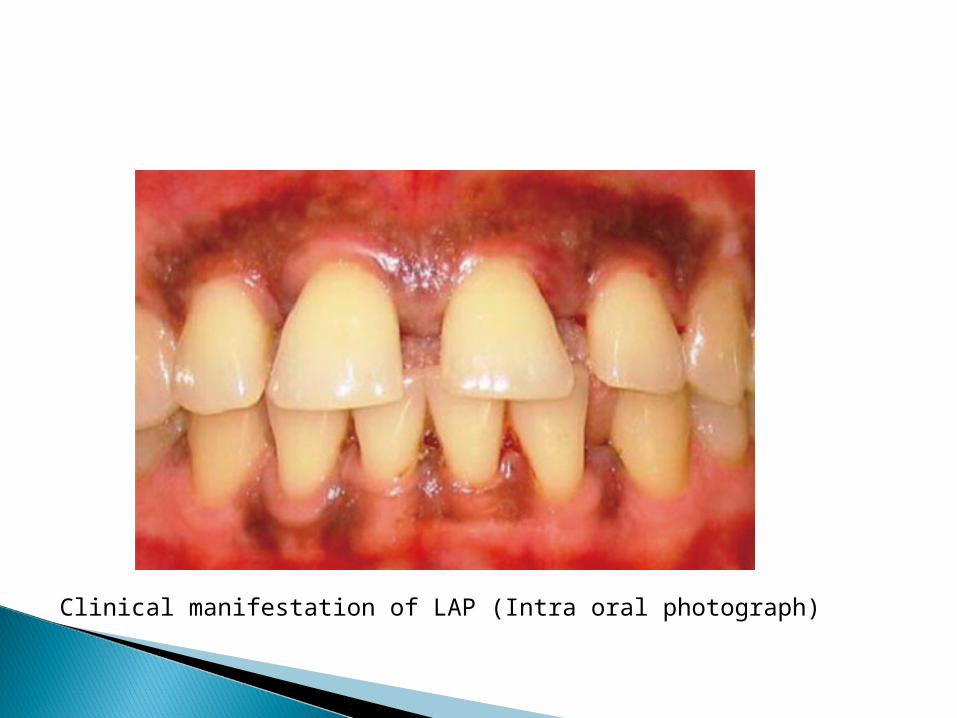
Clinical manifestation of LAP (Intra oral photograph)
A striking clinical feature of LAP, is the lack of clinical inflammation, despite the presence of deep periodontal pockets, and advanced bone loss.
In most cases, the amount of plaque on the affected teeth is minimal, which seems inconsistent with the amount of periodontal destruction exhibited.
It often contains elevated levels of Aggregatibacter actinomycetemcomitans, and in some patients, Porphyromonas gingivalis.
LAP progresses rapidly. Rate of bone loss is 3 to 4 times faster than Chronic Periodontitis.
Other clinical features of LAP are:
1. Distolabial migration of maxillary incisors, with concomitant diastema formation.
2. Increasing mobility of the maxillary and mandibular incisors and first molars.
3. Sensitivity of denuded root surfaces to thermal and tactile stimulation.
4. Deep dull radiating during mastication, (probably caused by irritation of the supporting structures by mobile teeth and food impaction).
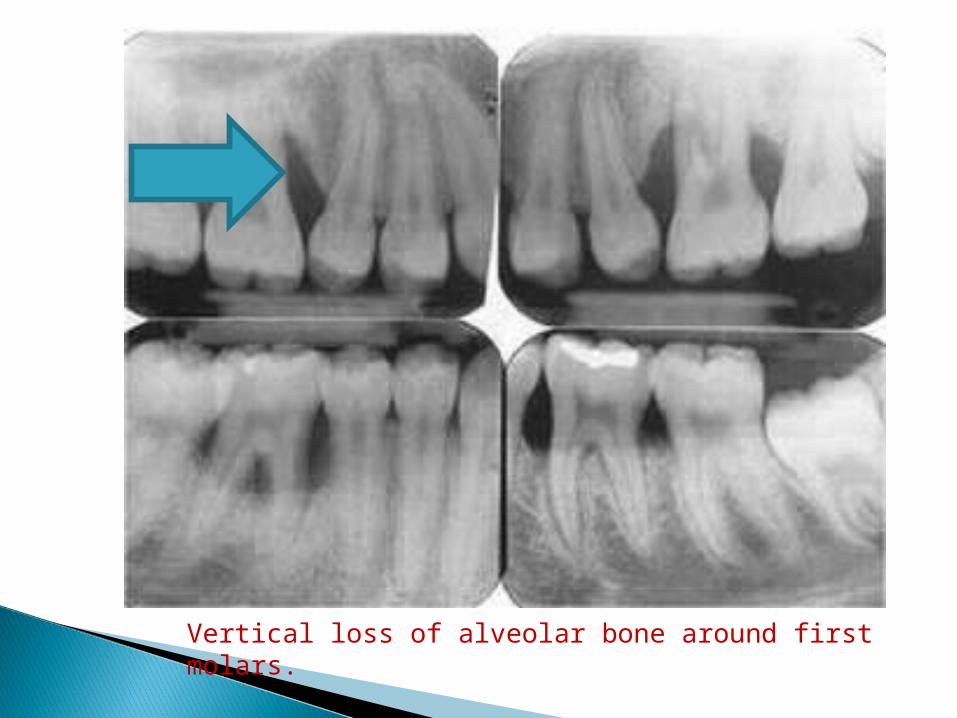
Vertical loss of alveolar bone around first molars.

Vertical loss of alveolar bone
Usually affects individuals under 30 years, but patients may also be affected.
In contrast to LAP, individuals affected by GAP produce poor antibody response to the pathogens present.
“Generalised interproximal attachment loss affecting at least 3 permanent teeth, other than the first molars and incisors.”
The destruction occurs episodically, with periods of advanced destruction, followed by stages of quiescence, of variable length.
As in LAP, patients in GAP often have small amounts of bacterial plaque associated with the affected teeth.
Quantitatively, the amount of plaque seems inconsistent with the amount of periodontal destruction.
Qualitatively, P. gingivalis, A. actinomycetemcomitans, and Tannerella forsythia, are more frequently detected in the plaque that is present.
Two types of gingival tissue responses are found in GAP:-
1. One is severely acutely inflamed tissue, often proliferating, ulcerated and fiery red. Marked by spontaneous bleeding.
2. In other cases, the gingival tissue may appear pink, free of inflammation and occasionally with some degree of stippling (usually stippling is absent).
However, despite the apparently mild clinical appearance, deep pockets can be demonstrated by probing.
Some patients of GAP may have systemic manifestations, like: weight loss, mental depression, and general malaise.
As seen with LAP, cases of GAP may be arrested spontaneously or after therapy.
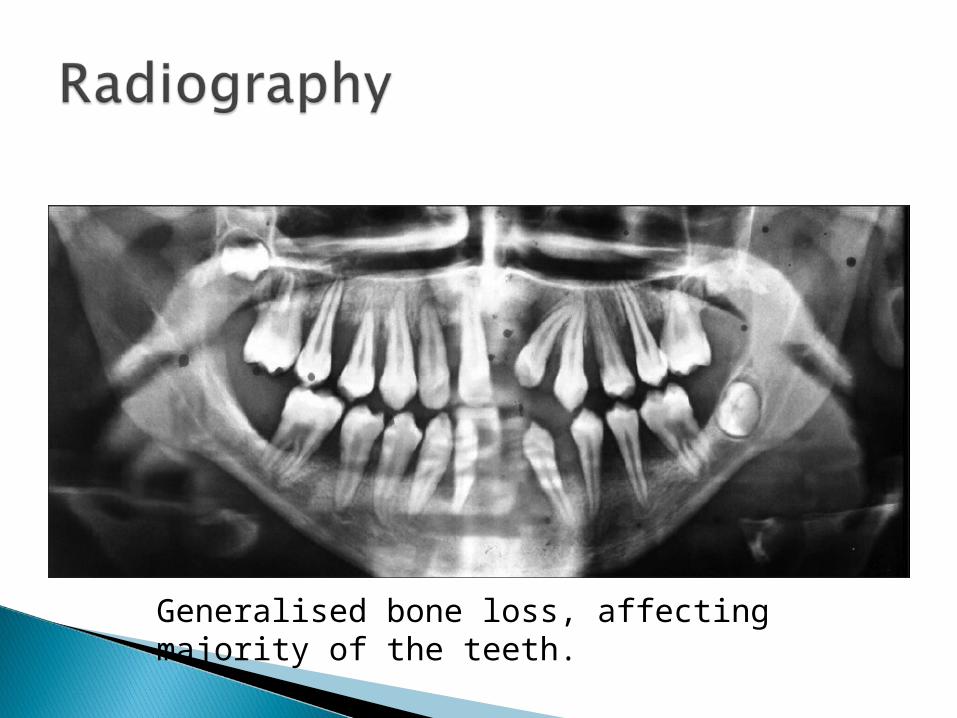
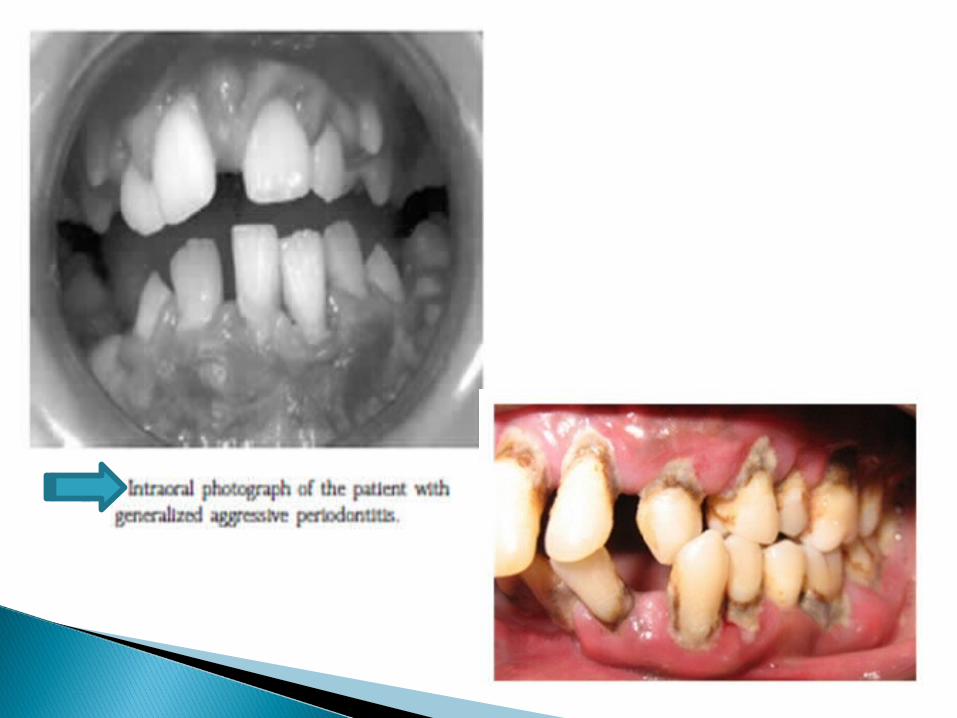
Generalised bone loss, affecting majority of the teeth.
Patients with GAP, who smoke have more affected teeth and more loss of clinical attachment than non smoking patients.
However, smoking may not have the same impact on young patients suffering from LAP.