REQUIRED CLERKSHIP CURRICULUM COMMITTEE - depts.washington.edu 031510.pdf · and receive feedback...
19
REQUIRED CLERKSHIP CURRICULUM COMMITTEE Date: March 15, 2010 Time: 4:30 – 5:30 P.M. A325 Conference Room Dr. Eric Kraus, Chair Conference Phone Number: 1-800-503-2899 access code 8305023 Committee website: https://staff.washington.edu/angwick/Curriculum/RCC.htm Webcast: http://uwsom.na4.acrobat.com/curriculum-committee/ . AGENDA 1. Approval of Minutes ATT A 2. Surgical Clerkship Review Dr. Tatum ATT B 3. New Clerkship Site Aplication a. MEDRCK 601 Clinical Clerkship at Northwest Hospital Dr. Paauw ATT C 4. Student Update Medical Student Reps 5. Oversight Committee Update Dr. Marshall 6. Academic Affairs Update 7. Colleges Update Dr. Goldstein 8. Student Affairs Update Dr. Eveland 9. Technology Update Michael Campion 2009-10 Committee meeting & clerkship review schedule 04/19/10 430pm Family Medicine review Dr. Greer 05/17/10 430-530pm 06/21/10 430-530pm Pediatrics review Dr. Bennett Suggested Agenda topics for 2009-10 • Clerkship availability • Timing of Capstone/final clerkships and residency start date • Scheduling of Boards. Students seem to want to start their rotations later so that they can prepare for boards. Discuss how to deal with the large number of students dropping required clerkships in June. • Medical student charting is a nightmare. We started the discussion and decided we need documentation and ORCA specialists to attend a meeting. The main goal is to make student note writing educational even though it can’t be used for billing. • What do we do when we fail a student, what do we do when a student fails a test – upper campus deadlines to make up work – 10 days.
Transcript of REQUIRED CLERKSHIP CURRICULUM COMMITTEE - depts.washington.edu 031510.pdf · and receive feedback...

REQUIRED CLERKSHIP CURRICULUM COMMITTEE Date: March 15, 2010 Time: 4:30 – 5:30 P.M.
A325 Conference Room Dr. Eric Kraus, Chair
Conference Phone Number: 1-800-503-2899 access code 8305023
Committee website: https://staff.washington.edu/angwick/Curriculum/RCC.htm Webcast: http://uwsom.na4.acrobat.com/curriculum-committee/.
AGENDA
1. Approval of Minutes ATT A
2. Surgical Clerkship Review Dr. Tatum ATT B
3. New Clerkship Site Aplication
a. MEDRCK 601 Clinical Clerkship at Northwest Hospital Dr. Paauw ATT C
4. Student Update Medical Student Reps
5. Oversight Committee Update Dr. Marshall
6. Academic Affairs Update
7. Colleges Update Dr. Goldstein
8. Student Affairs Update Dr. Eveland
9. Technology Update Michael Campion
2009-10 Committee meeting & clerkship review schedule 04/19/10 430pm Family Medicine review Dr. Greer 05/17/10 430-530pm 06/21/10 430-530pm Pediatrics review Dr. Bennett Suggested Agenda topics for 2009-10 • Clerkship availability • Timing of Capstone/final clerkships and residency start date • Scheduling of Boards. Students seem to want to start their rotations later so that they can prepare for boards. Discuss how to deal
with the large number of students dropping required clerkships in June. • Medical student charting is a nightmare. We started the discussion and decided we need documentation and ORCA specialists to
attend a meeting. The main goal is to make student note writing educational even though it can’t be used for billing. • What do we do when we fail a student, what do we do when a student fails a test – upper campus deadlines to make up work – 10
days.

Minutes
Required Clerkship Curriculum Committee February 22, 2010
Dr. Eric Kraus, Chair Members in Attendance___________________________________________________________________ MS3 Kristina Bajema Dr. Curt Bennett Michael Campion Dr. Jan Carline MS3 Sarah Chisolm Linda Clark Dr. Heidi Combs
Kellie Engle Dr. Jay Erickson Dr. Pete Eveland Dr. Erika Goldstein Dr. Tom Greer Dr. Ross Hays Dr. Rich Hillman
Dr. Eric Kraus Dr. Susan Marshall Dr. Tom McNalley Dr. Vicki Mendiratta Dr. Tom Nighswander Dr. Tom Norris Dr. Doug Paauw
Sandy Pomerinke Dr. Doug Schaad Dr. Sue Stern Judi Sullivan Dr. Roger Tatum
Members Unable to Attend_________________________________________________________________ Dr. David Acosta Dr. Suzanne Allen Dr. Rachel Beda Dr. Thomas Benedetti Michelle Divine
Deb Dolph MS3 Tiffany Erwin Dr. Deb Harper MS4 Jared Kirkham, Connie Lamb
Dr. John McCarthy Peg Pattee Carla Salldin MS3 Alex Salskov MS4 Laura Stoll
Dr. Jared Strote MS3 Sara Van Nortwick Marj Wenrich Angie Wick MS3 Tara Whitaker
January 11, 2010 minutes were reviewed and approved with a correction to attendance list. Policy for Grade Appeal – Dr. Kraus There is a need for policy regarding the time frame for a student to appeal a grade and for the final decision to be made. There is a policy statement in the Student Handbook that refers to all four years of medical school. It was decided that a separate policy for the clerkship years was needed as the grading is quite different. Please note that a student will have the opportunity to appeal all comments in their records along with their final grades. The student will have 6-8 weeks in which to make a formal appeal to a grade. A second key issue is the order in which students can make an appeal. It was agreed that students should write out their appeal first and bring it to the clerkship director who will then have a proposed 21 days in which to research the issue. If the student appeals the clerkship director’s decision, there is a second level of appeal to the department chair who will have 21 days to make a decision and has the final say. The clerkship director will facilitate communication between the preceptor and student. Because students, site directors, or chairs may be unavailable within the time stated, all deadlines are expected but not required. Dr. Goldstein will examine the Student Handbook for changes that may need to be made to the current policy for first and second year courses. Dr. Kraus will make updates to the document. It was approved and will be sent to the Curriculum Oversight Committee. Dr. Tatum will take this to the next Elective Clerkship Committee meeting for discussion. Policy for Planned Delay in Grade Reporting - Dr. Kraus After a brief review of the background, Dr. Kraus reported that Connie had gone to Upper campus registrar for approval of the new policy as we wanted to create the new denotation “In Progress”. The registrar’s office recommended using the term “incomplete;” and will allow us to define the grade “incomplete” for the Required Clerkships any way we want. It is recommended that departments put a link on their websites to the Student Handbook for most current policy statements. The policy was approved with the recommended changes and will go to the Curriculum Oversight Committee. *Note-Agenda item for Sept. meeting: Verify that the above policies have been placed in the Student Handbook. New Clerkship Site Application – Dr. McNalley and Dr. Farber CONJ 675 P-Chronic Care/PALLIATIVE CARE – GHHH Tacoma: This is an outpatient–based patient care experience. Students will have experiences with home care and hospice. This site application was approved.
Page 1 Attachment A Required Clerkship Committee March 15, 2010

Student Update – Sarah Chisholm Overall things are going well. E*value is working pretty well. There is frustration regarding lack of preparation for the fourth year, the lack of guidance regarding signing up and ranking their preferences for next year, and if there be enough places for them to go. Some students find the forms difficult. There are problems with students waiting until the end and the more desirable sites are taken. The committee is reminded that e*Value is new and that this is a transitional year. Also, students think that they would benefit from more effective career counseling. Dr. Eveland is working on expanding the counseling opportunities and career advisors from each department. Curriculum Oversight Update – Dr. Marshall Angie Wick will be out on leave for four to six weeks. Please contact Shalley Lane, Marcie Buckner, or Sandy Pomerinke for questions. Academic Affairs Update – Dr. Norris Thank you all for your work preparing for the LCME visit. There will be an LCME preparation visit following this meeting. Colleges Update – Dr. Goldstein All is well Student Affairs Update – Dr. Eveland Submission date for rank order list is this Wednesday. Technology Update – Michael Campion Scheduling process for next year is almost completed and will be released by the end of March or early April. Clerkship directors are asked to take a last look at time slots in their clerkships for sites available. Third year students usually get the information before the directors. Sub-I information will be released later. There is a need to find out what the process and time frame will be for changes to be made by the students. *Please note: LCME Required Clerkship Interview, Group 1: Monday, March 8, 3:45 – 5:00 p.m., Turner Conerence Room LCME Required Clerkship Interview, Group 2: Monday, March 8, 3:45 – 5:00 p.m., A-325 2009-2010 Committee meeting & clerkship review schedule 3/15/10 430-530 pm Surgery Review, Dr. Tatum 4/19/10 430-530 pm Family Medicine Review, Dr. Greer 5/17/10 430-530 pm 6/21/10 430-530 pm Pediatrics Review, Dr. Bennett
Page 2 Attachment A Required Clerkship Committee March 15, 2010

University of Washington School of Medicine Required Clerkship in Surgery Review, 2008-2010
I. What is the link to your website? http://depts.washington.edu/surgstus/ II. What, if any, changes were made to the clerkship this year? New sites added? Surgery has changed our grading policy and grade distribution (detailed below) New site (for 2010-2011 AY): Caldwell/Meridian Idaho Practice Group: Advanced Surgery of Idaho Site Director: Ronald Cornwell, MD III. How many total student slots are available total and per block? Total number for AY 2010-2011 = 234 SuA = 25 SuB = 26 FaA = 31 FaB =30 WiA = 31 WiB = 30 SpA = 31 SpB = 30 IV. Core goals and objectives. Describe the method used to educate the faculty and residents. Are students meeting the goals and objectives? Please discuss any changes. Core Objectives (unchanged since previous review):
1. In patients with surgical problems, demonstrate a method of focused evaluation, including the approach to workup and preparation of patients for anesthesia and surgical intervention Curriculum: Students will regularly evaluate patients together with residents and attendings in the clinic, in the ER, and on the wards (as consults). Benchmark: Students will be expected to perform initial patient evaluation (prior to evaluation by resident or attending) in each of these settings on a weekly (at minimum) basis; each student is required to complete 4 detailed patient write-ups, including thorough history and physical as well as a focused discussion of the patient’s disease process and management. Test: Student write-ups are turned in to whichever attending is responsible for the patient; the write-up is reviewed by the attending, who is required to grade it and is expected to discuss it directly with the student for one-on-one feedback.
2. Identify what constitutes appropriate surgical referral by recognition of which problems are clearly surgical, potentially surgical, and those which do not require surgical intervention Curriculum: Students will regularly discuss evaluations with residents and attendings and receive feedback and guidance concerning differential diagnosis, triage, and care plans. Benchmark: All students are expected to discuss patients and cases on a regular basis with their resident/attending team as part of the patient-evaluation process, as in item 1. Test: The clinical grade includes evaluation of students’ problem-solving ability and knowledge as it applies to patients whom they have evaluated.
3. Perform a thorough abdominal exam in the presence of a faculty preceptor, evaluating for pain and tenderness, abdominal distension, abdominal masses, hernias, and bruits
Page 1 Attachment B Required Clerkship Committee March 15, 2010

Curriculum: Students will directly observe multiple abdominal exams performed by residents and attendings during initial patient evaluations. Benchmark: Each student is required to complete one thorough abdominal exam mini-CEX in the presence of an attending or chief resident. Test: Abdominal exam mini-CEX cards, signed by the reviewing attending or chief resident, are turned in to the clerkship coordinator.
4. Identify the important factors in the diagnosis, workup, and management of specific surgical problems in the following categories:
a. Acute abdomen b. Bowel obstruction c. GI hemorrhage d. Hepatobiliary and pancreatic disease e. Endocrine disease (thyroid, parathyroid, and adrenal) f. Breast disease g. Vascular disease (carotid, aortic, and peripheral vascular) h. Cardiac and thoracic disease i. Trauma, burns, and surgical critical care j. Pediatric surgery k. Plastic surgery
Curriculum: A lecture series is given throughout the clerkship covering each of the above topics, which the students are required to attend Benchmark: Students are expected to attend each of the lectures, and are asked to maintain a log indicating that they have directly participated in the care of a patient in each category (performing an H&P in clinic, performing and ER evaluation, or consult evaluation, directly caring for a patient on the wards, or scrubbing into the case in the operating room). Because different clerkship sites have varied offerings in terms of case experience, web-based case scenarios will be offered for each category. Students will be expected to complete the case scenarios by the last week of their clerkship for those categories in which they have not been involved in direct patient care. Test: Student case logs will be submitted online by the end of the clerkship to the clerkship coordinator, indicating that they have either participated in the care of a patient in each category, or completed the relevant web-based case scenario.
5. Perform some basic surgical techniques, particularly basic suturing skills and general wound management Curriculum: Students will attend a wound closure skills lab early in the clerkship, in which they will learn suturing and knot-tying techniques. Opportunities to further develop these techniques will be an integral part of their operating room experience. Additionally, wound management skills will be learned through activities on the wards and in clinic. Benchmark: Students are required to attend the wound closure lab (or to practice independent instruction with an on-line tutorial and supplied suture/knot tying board at WWAMI sites), as well as to participate in cases in the OR. Test: Assessment of technical skills is a component of the clinical grade for the clerkship.
Page 2 Attachment B Required Clerkship Committee March 15, 2010

6. Evaluate and critique surgical literature
Curriculum: Self study, with attending feedback. Benchmark: Students will each choose one article from the recent surgical literature (published within the previous 3 years), and write a one-page review consisting of a summary of the content and relevance of the article as well as an evaluation of the methodology and validity of the findings and conclusions. Test: The review is to be turned in to an attending from the service on which the student is rotating for grading. It is expected that the student will meet one-on-one with that attending to discuss the review and the grade.
V. Desired goals and objectives. Please discuss any changes. We do not have separate desired or suggested goals and objectives in a formal fashion. VI. Absentee and work hours policy. Verify that it is on the website and describe the method used to educate the faculty and residents. Discuss the call schedule for students. The policies are on the website, and faculty and residents receive periodic (at least once/year) emails reminding them of student work hour restrictions. These rules are enforced on an as-needed basis via direct communication from the clerkship director to the site director for the relevant site. Call is no more frequent than one in four at any site, with the exception of certain WWAMI sites where a student may be on at-home call corresponding to the call schedule of a particular attending with whom they are working. VII. Didactics. How are non‐Seattle WWAMI students educated (video lectures, webcasting, other)? Include information about student orientation. Our live orientation is an approximately 90-minute lecture given by the clerkship director in Seattle, and webcast (audio and slides) simultaneously to all WWAMI sites using Adobe Connect. This enables real-time interaction for all students beginning the clerkship. The lectures are given in Seattle for all of the four Seattle sites and exist in a recorded, on-line format for students at WWAMI sites. We are currently in the process of recording updated versions of these lectures using the Adobe Connect format. VIII. Clinical CEX(s). How are they taught, completed and remediated if needed? A discussion of the Abdominal Exam (the Surgery Mini-CEX) is given during the orientation, including tips and pointers specific to surgical patients and problems. The students are instructed to perform a thorough abdominal exam in the presence of one of their attendings, using a checklist for guidance, during a clinic day within the first two weeks of the clerkship. Once this has been satisfactorily completed, the checklist is signed off by the attending preceptor and submitted centrally to the clerkship coordinator. IX. Bioethical component to the clerkship. A mini-lecture on the principles and particulars of informed consent is given during the orientation day. Students are then instructed to observe the formal informed consent process as performed by their attending preceptors throughout the course of their clerkship, which each has numerous opportunities to do.
Page 3 Attachment B Required Clerkship Committee March 15, 2010
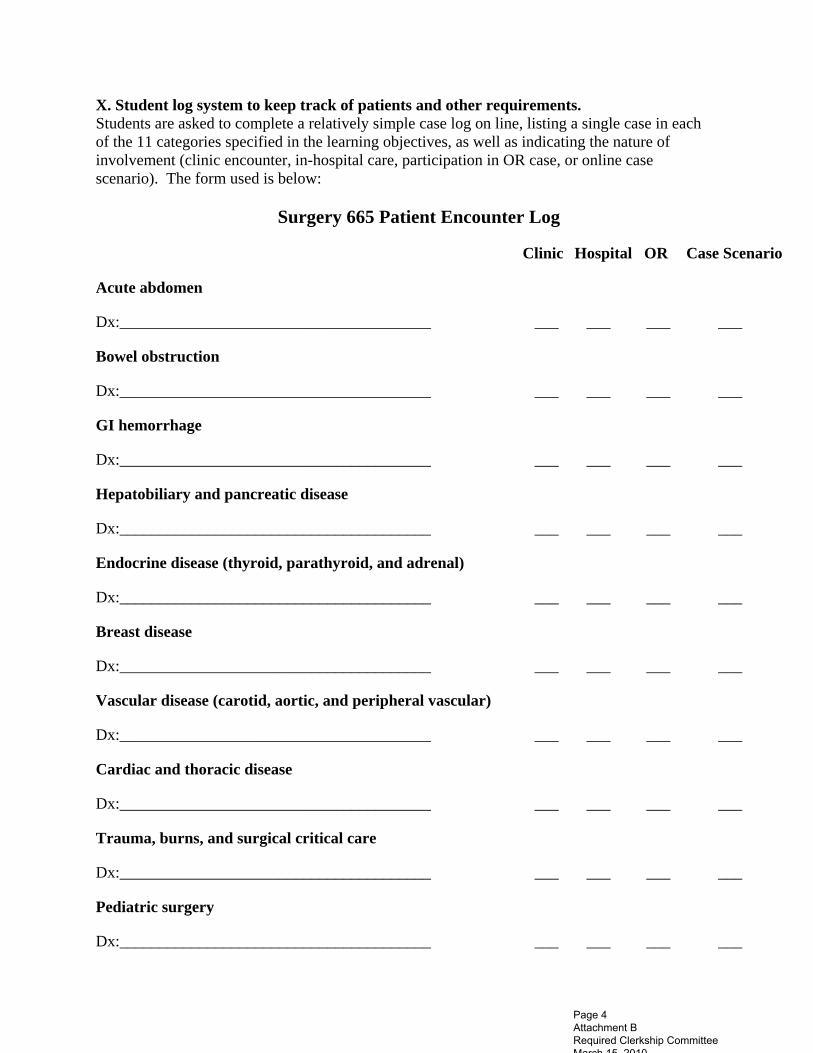
X. Student log system to keep track of patients and other requirements. Students are asked to complete a relatively simple case log on line, listing a single case in each of the 11 categories specified in the learning objectives, as well as indicating the nature of involvement (clinic encounter, in-hospital care, participation in OR case, or online case scenario). The form used is below:
Surgery 665 Patient Encounter Log
Clinic Hospital OR Case Scenario
Acute abdomen
Dx:_______________________________________ ___ ___ ___ ___
Bowel obstruction
Dx:_______________________________________ ___ ___ ___ ___
GI hemorrhage
Dx:_______________________________________ ___ ___ ___ ___
Hepatobiliary and pancreatic disease
Dx:_______________________________________ ___ ___ ___ ___
Endocrine disease (thyroid, parathyroid, and adrenal)
Dx:_______________________________________ ___ ___ ___ ___
Breast disease
Dx:_______________________________________ ___ ___ ___ ___
Vascular disease (carotid, aortic, and peripheral vascular)
Dx:_______________________________________ ___ ___ ___ ___
Cardiac and thoracic disease
Dx:_______________________________________ ___ ___ ___ ___
Trauma, burns, and surgical critical care
Dx:_______________________________________ ___ ___ ___ ___
Pediatric surgery
Dx:_______________________________________ ___ ___ ___ ___
Page 4 Attachment B Required Clerkship Committee March 15, 2010

Plastic surgery
Dx:_______________________________________ ___ ___ ___ ___
XI. Mid‐clerkship feedback process. Students are expected to receive mid-clerkship feedback by the end of the third week of the clerkship from the site director or from another faculty preceptor with whom they have worked. All site directors are aware of this requirement and are periodically reminded through e-mail or in some cases direct phone or face-to-face communication. The students are also all instructed during the orientation to remind their site directors near the mid-way point if they have not yet received this formal feedback. XII. Summative evaluation process. This takes slightly different forms at different sites, but all sites use the standard required clerkship evaluation form through E-Value for reporting of the final clinical grade. Sites generally follow one of two models: 1) evaluations and feedback are discussed by all of the attendings and residents who have worked with the student at a meeting at the end of the student’s clerkship, and then the site director distills this into scores and comments as well as a final clinical grade for the E-Value reporting form; or 2) each faculty member who has worked with a student will fill out a paper version of the evaluation form, and then the site director will distill this into a final clinical evaluation and grade to be entered into E-Value. XIII. Final exam. The final examination has remained unchanged since it was re-written in summer of 2005. This consists of 100 multiple choice questions; there are actually 4 versions of the exam, each of which contains a core of 75 questions which are the same, together with 25 questions (balanced for general level of difficulty) which are different on each version. We are planning to write a newer exam, more closely based on the lecture series, for the upcoming academic year 2010-2011. XIV. Grading policy. How many students received honors, high pass, pass, and fail? Were fail grades based on knowledge deficiencies or professionalism? How was the fail grade remediated? Because of the concern that relatively few students were achieving a grade of Honors in the last 5 years (ranging from 11 to 15% of each class), we decided to change the grading system for the current academic year in an effort to increase the number of students achieving the highest grade (the national average for the percentage of students receiving the highest grade in surgery is 23%). The previous system required a student to achieve both a clinical honors grade as well as an honors grade on the examination in order to achieve honors for the clerkship. The examination was graded on a curve, with a raw score of the mean + 1 SD representing honors. Currently, our system is based on a point scale, with 100-point possible total. Sixty of these points come from the numerical portion of clinical evaluation, with each of 12 indices being assigned the 1-5 points as detailed on the evaluation form; hence, scores theoretically may range from 12 to 60 for the clinical grade. The exam grade makes up the remainder, and points are
Page 5 Attachment B Required Clerkship Committee March 15, 2010

calculated by multiplying the number of questions correct on the exam by 0.4, for a total of 0 to 40 points. Grades are then assigned according to the following point scale:
Honors = 84 or above High pass = 78-83 Pass = 63-77 Fail = 62 or below
Below are the grade distributions for the old system and the new system (first 2 quarters only): AY 2008-2009 Grade Distribution: Honors: 11% High Pass: 40% Pass: 50% Fail: 0% AY 2009-2010 Grade Distribution (new system)*: Honors: 30% High Pass: 24% Pass: 44% Fail: 0% *one grade is still pending an examination re-take at the time that these statistics were compiled When a student has initially received a fail grade based on the new point scale, as has happened twice thus far, it is typically primarily because of the examination score. Thus, they are given an opportunity to take a re-examination, consisting of 50 of the core questions from the original examination, and the score on this exam is then used to determine whether or not the student will receive a passing grade on the clerkship by factoring it into the point scheme outlined above. In the past 2 years, no student has received a failing grade based upon clinical performance, and no student has received a final grade of fail in the clerkship requiring them to repeat the clerkship. XV. Common item scores from the clerkship evaluation and USMLE Step 2 performance. (Provided by the department of Medical Education and Biomedical Informatics) AY 2008-2009
Site N
Clarity of
Goals Object
ives
Quality of
Faculty Teach
Quality of Resident
Teach
Quality of Formal Teach
Quality of
Resources
Observation of Skills
Fairness of
Evaluation
Mini-CEX
Quality
Clerkship as a Whole
Clerkship Contributio
n to Education
% Received Mid Rotation
Feedback
Billings 8 4.8 5.4 4.0 4.6 5.6 4.5 4.4 5.1 5.4 75
Boise 8 4.5 5.4 5.5 4.9 3.6 4.8 4.2 3.1 5.1 5.1 88
BoiseVA 6 4.7 5.3 5.3 5.0 5.0 5.2 5.4 3.5 5.2 5.2 67
Page 6 Attachment B Required Clerkship Committee March 15, 2010
Casper 6 3.8 4.5 4.0 3.2 4.7 3.8 3.2 4.7 4.7 33
Fairbanks 11
4.1 4.5 3.4 3.5 4.5 3.4 3.3 4.0 4.4 64
HMC 34
4.2 4.8 4.5 5.0 4.5 3.5 3.6 3.2 4.7 4.9 18
Madigan 12
4.1 4.8 5.3 4.9 3.7 4.2 4.4 3.3 4.8 5.2 83
Missoula 3 4.7 5.3 4.0 5.7 4.7 4.0 5.0 5.3 0
Spokane 12
4.6 5.5 6.0 5.5 4.4 5.2 4.4 3.2 5.3 5.3 42
UWMC 34
4.1 4.6 4.3 4.6 4.3 3.9 3.9 3.0 4.0 4.5 88
VAMC 24
4.9 5.4 5.2 5.3 4.8 4.9 4.7 3.9 5.2 5.5 96
Virginia Mason
14
4.1 4.9 4.8 4.9 4.2 4.5 4.3 3.4 4.8 4.8 57
TOTAL 172
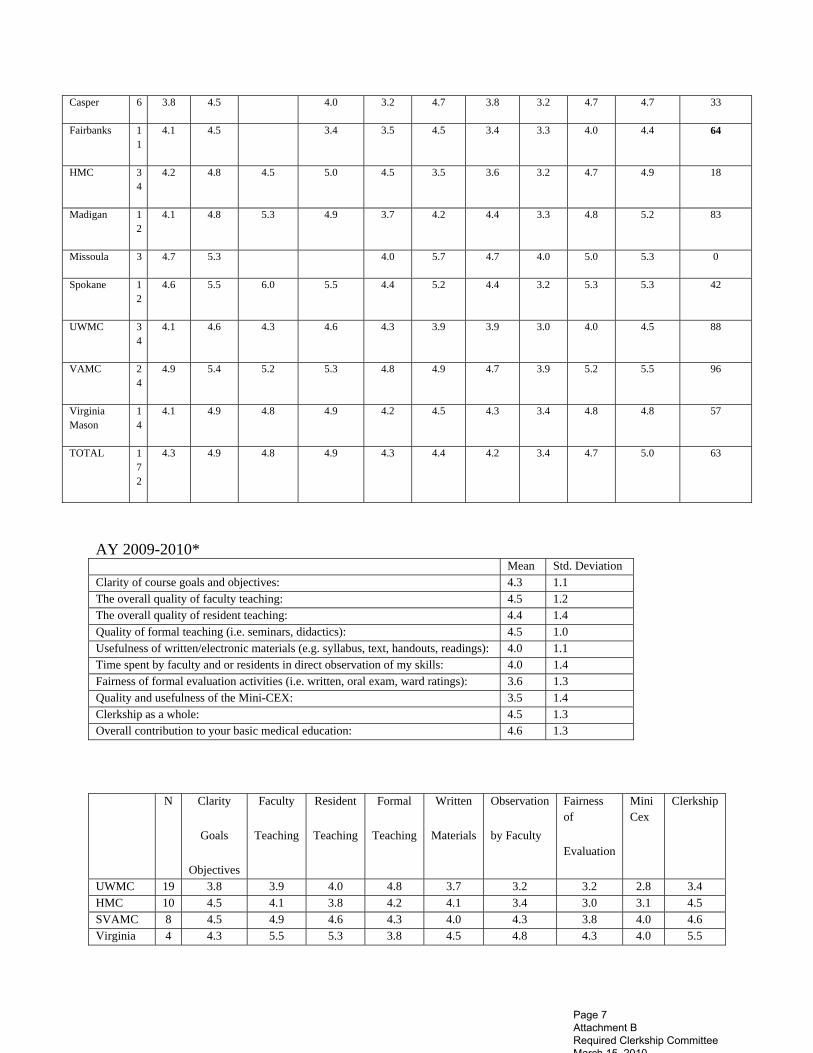
4.3 4.9 4.8 4.9 4.3 4.4 4.2 3.4 4.7 5.0 63
AY 2009-2010* Mean Std. Deviation Clarity of course goals and objectives: 4.3 1.1 The overall quality of faculty teaching: 4.5 1.2 The overall quality of resident teaching: 4.4 1.4 Quality of formal teaching (i.e. seminars, didactics): 4.5 1.0 Usefulness of written/electronic materials (e.g. syllabus, text, handouts, readings): 4.0 1.1 Time spent by faculty and or residents in direct observation of my skills: 4.0 1.4 Fairness of formal evaluation activities (i.e. written, oral exam, ward ratings): 3.6 1.3 Quality and usefulness of the Mini-CEX: 3.5 1.4 Clerkship as a whole: 4.5 1.3 Overall contribution to your basic medical education: 4.6 1.3
N Clarity
Goals
Objectives
Faculty
Teaching
Resident
Teaching
Formal
Teaching
Written
Materials
Observation
by Faculty
Fairness of
Evaluation
Mini Cex
Clerkship
UWMC 19 3.8 3.9 4.0 4.8 3.7 3.2 3.2 2.8 3.4 HMC 10 4.5 4.1 3.8 4.2 4.1 3.4 3.0 3.1 4.5 SVAMC 8 4.5 4.9 4.6 4.3 4.0 4.3 3.8 4.0 4.6 Virginia 4 4.3 5.5 5.3 3.8 4.5 4.8 4.3 4.0 5.5
Page 7 Attachment B Required Clerkship Committee March 15, 2010

Mason Madigan 5 4.0 5.6 5.6 5.5 3.0 5.0 3.8 3.8 5.6 Billings 3 4.7 5.3 . 4.0 5.0 5.3 4.0 5.0 5.7 Boise 3 5.3 6.0 . 5.7 5.0 6.0 5.3 5.0 6.0 Casper 2 4.5 3.5 . 4.0 5.0 2.5 4.5 4.5 4.0 Fairbanks 4 4.5 4.3 . 3.0 4.0 4.3 3.0 2.7 4.5 Missoula 3 4.3 4.3 . 4.0 4.3 4.7 3.7 4.3 5.0 Spokane 4 4.5 4.8 4.0 5.0 4.0 4.3 4.0 2.5 4.8 TOTAL 65 4.3 4.5 4.4 4.5 4.0 4.0 3.6 3.5 4.5
Siten2 Clerkship
Contribution
% Receiving
Mid-Clerk
Evaluation
% Compliance
Work Hours
UWMC 3.6 79 79 HMC 4.4 10 20 SVAMC 4.8 100 88 Virginia Mason 5.5 50 100 Madigan 5.4 80 100 Billings 5.3 100 100 Boise 6.0 67 100 Casper 4.0 0 100 Fairbanks 4.8 25 100 Missoula 5.3 33 100 Spokane 4.8 25 100 TOTAL 4.6 58 80
These items rated on a scale of 1 to 5 but no scale values included in the questionnaire
Site Numeric Wound Closure Lab
Site Orientation
ParticipationIn Care
ConferencesSeminars
FeedbackTime
% Yes Site
Selection
% Yes Web
Site UWMC 4.1 3.7 3.4 3.3 3.4 31.6 100.0 HMC 4.6 3.7 3.5 3.7 3.3 100.0 100.0 SVAMC 4.1 3.5 4.4 3.8 4.4 87.5 100.0 Virginia Mason 4.3 3.0 3.8 4.0 4.3 100.0 100.0 Madigan 4.5 2.8 4.2 4.4 4.6 80.0 80.0 Billings . 3.0 4.3 4.0 3.7 100.0 100.0 Boise 5.0 4.3 4.7 4.7 4.3 100.0 100.0 Casper 4.0 4.0 3.5 4.0 3.0 100.0 100.0 Fairbanks 4.0 3.3 2.8 3.0 3.3 75.0 75.0 Missoula 3.0 4.3 3.7 3.0 4.0 100.0 100.0 Spokane 4.0 3.3 3.3 4.5 3.0 100.0 100.0 TOTAL 4.3 3.5 3.7 3.7 3.7 75.4 96.9
XVI. What aspects of the clerkship were particularly successful?
Page 8 Attachment B Required Clerkship Committee March 15, 2010

The orientation works particularly well, as it is live and given simultaneously to all 11 sites. This allows me to address any patterns of difficulties or questions from the students from the previous clerkships with the new group, as well as to ensure that all students are aware of the expectations of the clerkship and informed of the various policies, such as work hours, and mid-clerkship feedback. The newer WWAMI expansion sites in Montana, Wyoming, and at Madigan have all been well received by the students, and we are observing an increasing number of students, including those who have rotated at these sites, expressing an interest in pursuing a career in surgery. XVII. What challenges did/does the clerkship face? Currently, accommodating the class expansion is the greatest challenge. Other challenges include maintaining standards and quality across the widely spread sites; encouraging certain faculty to complete evaluations in a timely manner; and limiting work hours at particularly busy sites such as HMC. XVIII. When was the last retreat? When is the next retreat planned? The Department of Surgery has yearly retreats, although these do not necessarily focus on surgical student education; the last of these was in August 2009. An additional retreat focused on student education is unfortunately not feasible at this time. XIX. Which sites were visited during the year? Spokane, WA—February 2008 Boise, ID—December 2008 Billings, MT—May 2009 Fairbanks, AK—July 2009 Others have been monitored and maintained via periodic telephone conversation with the individual site directors XX. What changes are planned for the clerkship? How do you communicate the changes?
1. Write a new examination 2. Recruit at least one more clerkship site in the Seattle area 3. Increase faculty and resident development for teaching skills
Page 9 Attachment B Required Clerkship Committee March 15, 2010

New Clerkship Site Provisional Approval Application January 2009 1
REQUIRED CLERKSHIP SITE APPLICATION
Clerkship Site: CURRICULUM OFFICE ONLY City, State
Seattle, Washington
REQ COM. Approval Date:
Oversight Approval Date:
Responsible Department: FCAA Approval Date:
MEDICINE Date affiliation approved:
Clinics Involved in the Clerkship WWAMI DEAN APPROVAL:
Complete corresponding section for each clinic. Name:
B-1: Date:
B-2: CLERKSHIP DIRECTOR APPROVAL:
B-3: Name: Doug Paauw MD
B-4: Date: February 17, 2010
Hospitals Involved in the Clerkship Clerkship Information
Northwest Hospital Site Director: Laura Quinnan, MD
Site Visit Date: 2/9/2010
Site Visit Performed by: Doug Paauw, Jenny Wright, Tom Norris
Clerkship # Title: MEDRCK 601 P-Clinical Clerkship (Northwest Hospital)
Surgery Selective Approval Do you want this course reviewed to meet Surgery Selective Requirements?
Yes No Prerequisites: Completion of basic curriculum. Third and Fourth Year Medical Students
Rotation Information (completed by Department): Length of Clerkship: Fixed Variable 12 weeks # Credits 24 Number of Students per rotation: 2SU A 2SU B 2 SP C 2AU A 2 AU B 2 AU C
2 WI A 2WI B 2WI C 2SP A 2SP B 2SP C
Additional Information:
Housing/Transportation (for REQUIRED clerkships): Housing Provided: Yes No Transportation: Type of housing provided: Type of transportation available:
Not applicable
Suitable for family housing? Yes No If Other please explain:
INSTRUCTIONS: Save this application to your computer. Move from section to section by using the tab key. The Department must submit the application electronically for approval through the committee process. Please indicate Clerkship Director/WWAMI Dean and approval dates in the approval section below, prior to submitting application. Press F1 for Help Hints.
Page 1 Attachment C Required Clerkship Committee March 15, 2010
New Clerkship Site Provisional Approval Application January 2009 2
Number of bedrooms: Section B -1: MAIN CLINIC PRACTICE STAFFING COMPOSITION
Name of Clinic: Northwest Hospital Physician (Site Coordinator): Laura Quinnan MD
Address: 1550 115th St. Phone: 206-368-1500
City/State/Zip: Seattle WA 98133 Email: [email protected]
Phone: 206-368-1500 Status of UW faculty appointment: PENDING
Fax: TBA
Administrative Contact: TBA Additional Info. Administrative Contact Phone Number:
Administrative email address:
MD’s/DO’s List only those who will spend significant teaching time.
Sp
eci
alt
y
(Ab
bre
via
te)
Bo
ard
C
ert
ifie
d/
B
oard
Eli
gib
le
Does this physician provide hospital
care?
UW Faculty Appointment
Name
Laura Quinnan, MDMain Contact/Site Coordinator IM Board Certified Yes PENDING
Santiago Neme, MD IM Board Certified Yes PENDING
Maria D'Souza, MD IM Board Certified Yes PENDING
Michael Fujimoto, MD IM Board Certified Yes PENDING
Jacob Fleet, MD IM Board Certified Yes PENDING
Eduardo Margo, MD IM Board Certified Yes PENDING
Hong Zhou, MD IM Board Certified Yes PENDING
Mid-Level Practitioners on site: (ARNP, PA, etc.)
Specialty/Credentials
Other On-Site Health Professionals (Mental Health, Nutritionist, Health Educator, Etc.)
Specialty/Credentials
If no other clinics move to Section C
Page 2 Attachment C Required Clerkship Committee March 15, 2010

New Clerkship Site Provisional Approval Application January 2009 3
Section B -2: MAIN CLINIC PRACTICE STAFFING COMPOSITION
Name of Clinic: Northwest Hospital continued. Physician (Site Coordinator):
Address: Phone:
City/State/Zip: Email:
Phone: Status of UW faculty appointment:
Fax:
Administrative Contact: Additional Info.
Administrative Contact Phone Number:
Administrative email address:
MD’s/DO’s List only those who will spend significant teaching time.
Sp
eci
alt
y
(Ab
bre
via
te)
Bo
ard
C
ert
ifie
d/
B
oard
Eli
gib
le
Does this physician provide hospital
care?
UW Faculty Appointment
Name
Main Contact/Site Coordinator
Tinsley Coble, MD IM Board Certified Yes PENDING
Nguyen Lan Nguyen, MD IM Board Certified Yes PENDING
Robert Kalus, MD IM Board Certified Yes CLINICAL FACULTY
Mid-Level Practitioners on site: (ARNP, PA, etc.)
Specialty/Credentials
Other On-Site Health Professionals (Mental Health, Nutritionist, Health Educator, Etc.)
Specialty/Credentials
If no other clinics move to Section C
Page 3 Attachment C Required Clerkship Committee March 15, 2010

New Clerkship Site Provisional Approval Application January 2009 4
Section C-1 CLINIC/HOSPITAL FACILITY INFORMATION
Hospital/Clinic Name:
Sett
ing
of
Care
# S
taff
ed
B
ed
s
Occ
up
an
cy
Rate
Avera
ge
len
gth
of
stay
# o
f A
nn
ual
Ad
mis
sio
ns
# A
nn
ual
ER
Vis
its
# A
nn
ual
Ou
tpati
en
t V
isit
s
Dis
tan
ce
fro
m C
lin
ic
Est
. #
p
ati
en
ts a
t on
e t
ime
for
pra
ctic
e
as
wh
ole
Northwest Hospital Both 238 57% 4 10171 38,000 428,000 70
Section C-2 CLINIC/HOSPITAL LEARNING RESOURCES AVAILABLE TO STUDENTS
Facilities: Hospital/Clinic
Name:
Is the practice a
formal residency program
site?
Specify residency training program
Does your practice train residents?
Can site accommodate both students
and residents?
Adequate computer
station and High speed
internet available to
student?
Adequate Library facilities
available to student?
Tel
econfe
renci
ng a
vaila
ble
?
Study rooms available to
student?
Adequate call rooms,
shower/changing area, and
lockers available to students?
Didactic lectures/grand rounds available for students
Northwest Hospital No No Yes Yes Yes No Yes No Call Yes
List didactic, lecture, and grand rounds facilities available at each facility: Students will come to the University of Washington for Grand Rounds, core clerkship lecture series and small group didactics two half days a week. At Northwest Hospital, Grand Rounds and a stroke conference is held monthy. Weekly hospitalist team meetings for case presentations will be available to students. Section D: Description of the student program (Describe how student might spend his/her time during the average day/week.) Office/Clinic Experiences: N/a Hospital Experience: Admitting patients to the hospital with a hospitalist medicine attending and care of hospitalized patients for at least 8 half days a week. Emergency Department Experience: Admit patients from the Emergency Department to the hospital wards. If you have chosen to have this clerkship reviewed as a Surgery Selective option, please specify how the clerkship meets the requirements: N/a On-Call Responsibilities (frequency, where, home or in-house call, etc): No overnight call. Community visits: N/a
Page 4 Attachment C Required Clerkship Committee March 15, 2010

New Clerkship Site Provisional Approval Application January 2009 5
Professional Meetings/Seminars (CME, grand rounds, journal club, etc.): At Northwest Hospital: monthly grand rounds; monthly stroke conference;, weekly noon hospitalist team meetings for case presentations; occasional evening CME events; monthly chest, cancer, gyn-onc conferences Other Learning Experiences/Unique features of the practice: Frequent, close interactions with subspecialists; large geriatric patient population; open ICU; collegial hospital team; emphasis on quality initiatives/process improvement projects How will the students be evaluated throughout the rotation? Student performance in clinical clerkship evaluation form. Is the site capable of providing mid-clerkship feedback to every student during every rotation? YES NO Does the site have the capability of providing every student a timely evaluation in a secure and confidential environment within 15 days of rotation end date?
YES NO Outreach and Social Services Available at Clerkship Site: Social work services at the hosptial. Are there consultants who will also assist in student teaching? YES NO (If yes, please provide information below)
Consultants Name
Specialty/Credentials P
ract
icin
g
in t
he
Co
mm
un
ity
(yes/
no
)
Vis
itin
g
Co
nsu
ltan
ts
(y
es/
no
)
Availab
le
by
Tele
ph
on
e
On
ly
(yes/
no
)
Teresa Wagner, MD Pulmonary/Critical Care yes no no
James Gordon, MD Neurology yes no no
Section E: Objectives For REQUIRED CLERKSHIPS: Can the site meet the stated objectives of the core clerkship? YES NO If yes, please attach the Departmental core objectives for this clerkship. If no, please explain why. For ELECTIVE CLERKSHIPS: If this is a new Elective, please attach a list of the clerkship objectives. If this is a current Elective, please attach a list of the current core objectives for this elective. Will this site be able to meet these objectives?
YES NO Section F: Pathways Should this clerkship be considered for one of the following pathways YES NO If yes, which of the following Pathways: Global Health Pathway Indian Health Pathway Hispanic Health Pathway Underserved Pathway Please describe why this clerkship would meet the requirements for the pathway.
Page 5 Attachment C Required Clerkship Committee March 15, 2010

New Clerkship Site Provisional Approval Application January 2009 6
Attachments:
If this is the first rotation in this clerkship, please attach a short summary of the community, listing any unique features.
Please list course objectives here or attach them as a separate sheet. Course Objectives Outlined below are our learning objectives for the course. Each objective has three components: • Content: what we expect you to learn • Curriculum: the tools we hope you use to learn it • Evaluation: the tools we use to find out if you've learned it I. Core Topics Content The curriculum contains 12 core clinical topics, listed below. For each topic we expect you to see at least one patient with the topic, and hope you will develop the knowledge and judgment necessary to manage a patient presenting with this problem. The 12 topics are: 1. Chest pain 2. Dyspnea 3. GI bleed 4. Abdominal pain 5. Altered mental status 6. Preventive care 7. Fever 8. Hypertension 9. Diabetes 10. Electrolyte disorder 11. Kidney failure 12. Joint or back pain Curriculum We expect that over the clerkship you will see at least one patient with each of these common problems, and will track whether or not you have done so as the clerkship progresses. However, these are also covered in the online cases as another way to meet this requirement in the unusual circumstance you don't see them in real patients. Evaluation • Patient log data • Clinical grades • Multiple choice final exam
Page 6 Attachment C Required Clerkship Committee March 15, 2010

New Clerkship Site Provisional Approval Application January 2009 7
II. Core Clinical Skills Content There are specific skills we hope you learn as part of the clerkship. These include: 1. Gaining experience and confidence in history taking and physical examination. 2. Refining and condensing write-ups and oral presentations to be precise but efficient in communication about patients. 3. Learning to use laboratory tests, radiologic examinations and special procedures, (i.e., blood drawing, intravenous lines, arterial blood gases) to work up and treat patients' problems. 4. Learning to construct a differential diagnosis, and be able to support your diagnosis based on clinical findings. 5. In addition to general clinical skills, we have developed specific benchmarks for three skill sets which will be used for the mini-CEX and the senior OSCE. These skills are: • Chest examination • Cardiac examination • Oral case presentation Curriculum • Online exam benchmarks [see above] • Lectures • Direct patient care • Bedside teaching Evaluation • Mini-CEX • Clinical grades III. Professionalism We have high expectations of professionalism and will be evaluating you by the same standard we would apply for anyone engaged in direct patient care. In addition to basic expectations (for example, attendance) we ask that you engage in a reflection on some of the professional and ethical conflicts that arise on the inpatient service. These will be discussed at a dedicated session with a faculty facilitator during the clerkship. Curriculum • Facilitated discussion with faculty • Bedside/ward teaching Evaluation • Clinical grades
Page 7 Attachment C Required Clerkship Committee March 15, 2010