Rene Ekpini E
21
Virtual elimination of mother- to-chilfd transmission of HIV: progress, remaining challenges, opportunities and way forward Rene Ekpini E Senior Adviser UNICEF, New York
description
Virtual elimination of mother-to-chilfd transmission of HIV: progress, remaining challenges, opportunities and way forward. Rene Ekpini E. Senior Adviser UNICEF, New York. Expenditure in HIV care and treatment, prevention and PMTCT in selected countries. Source: UNAIDS 2008 Global Report. - PowerPoint PPT Presentation
Transcript of Rene Ekpini E

Virtual elimination of mother-to-chilfd transmission of HIV:
progress, remaining challenges, opportunities and way forward
Rene Ekpini ESenior Adviser
UNICEF, New York

0 20,0
00
40,0
00
60,0
00
80,0
00
100,0
00
120,0
00
140,0
00
160,0
00
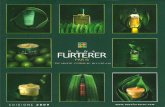
Botswana
Mozambique
Haiti
Cote d'Ivoire
Rwanda
PMTCT Total prevention Care & Treatment
Expenditure in HIV care and treatment, prevention and PMTCT in selected
countries
Source: UNAIDS 2008 Global Report
Source: UNAIDS 2008 Global Report

Remaining challenges-1
• Lack of translation of political commitment into
catalytic
actions with accountability mechanisms at the
country
level between central and sub-national authorities
and
health management structures
• Donor-driven programmes with limited national
ownership, parallel funding, M&E and PSM systems
with
concentration in limited urban settings
• Weak health systems with low access to and
uptake of
services, the use of less efficacious interventions
(e.g. Sd-
NVP) and poor continuum of care for mothers and
children
• Lack of translation of political commitment into
catalytic
actions with accountability mechanisms at the
country
level between central and sub-national authorities
and
health management structures
• Donor-driven programmes with limited national
ownership, parallel funding, M&E and PSM systems
with
concentration in limited urban settings
• Weak health systems with low access to and
uptake of
services, the use of less efficacious interventions
(e.g. Sd-
NVP) and poor continuum of care for mothers and
children

0
20
40
60
80
100
120
Countries
Perc
enta
ge
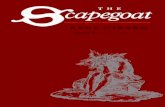
ANC HIV T&C
The gap between antenatal care The gap between antenatal care coverage and HIV testing and counseling coverage and HIV testing and counseling
in the context of PMTCT in selected in the context of PMTCT in selected countries – 2007countries – 2007

Building up PMTCT on weak health systems in resource-limited settings
9196
6874
60.5
43.4
0
20
40
60
80
100
120
Malawi Zambia
1+ visit 4+ visits Births with skilled attendant
Sources: 1- ANC coverage: Antenatal care in developing countries-Promise, achievements and missed opportunities – An analysis of trends, level and differentials, 1990-2001 updates 2- Skilled attendant at birth 2006
Coverage of antenatal care and skilled attendant at birth
50
65
32
47
1721
1216
0
10
20
30
40
50
60
70
Malawi Zambia
HIV T&C ARV for PMTCTInfant ARV for PMTCT CTP for infant by 2 months
Coverage of PMTCT services

8
2.2
25 25
19.5
17.2
0
5
10
15
20
25
30
Sd-NVP AZT/ Sd-NVP
tran
smis
sion
ra
te (
%)
In PMTCT programme Outside PMTCT pg All
Current system performance (KZN province)
Attend ANC clinic 92%
Counseled and tested for HIV, CD4 75%
Get ARVs (pre- and perinatal) 50%
Adapted from Pierre Baker & Nigel RollinsAdapted from Pierre Baker & Nigel Rollins

8
2.2
25 25
11.1
6.1
0
5
10
15
20
25
30
Sd-NVP AZT/ Sd-NVP
tra
nsm
issi
on
ra
te (
%)
In PMTCT programme Outside PMTCT pg All
95% efficiency of the system (KZN province)
Attend ANC clinic 92%
Counseled and tested for HIV, CD4 95%
Get ARVs (pre- and perinatal) 95%

0
10
20
30
40
50
60
70
80
90
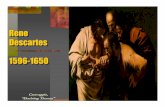
nutritionduring
pregnancy
Familyplanning
Preventionof STIs
Measurefoetal
heart rate
Partographever filled
in
Checkuterine
retraction
Perc
enta
ge
Before PMTCT After PMTCT
Individual counsellingIndividual counselling
Quality of antenatal and delivery care before and after the implementation of
PMTCT; Cote d’Ivoire
Therese Delvaux et al.Therese Delvaux et al.

Impact of PMTCT on institutional deliveries in Rwanda – HIV-positive
women
69%
72%
80%
87%
89%
31%
28%
20%
13%
11%
0% 20% 40% 60% 80% 100%
2004 (N= 412)
2005 (N=499)
2006 (N=966)
2007 (N=1,053)
2008 (N=1,253)
At health facility Home
Bangendanye, L; Price, J.E.; Micomyiza E.; Shumbusho F.; Wesson Bangendanye, L; Price, J.E.; Micomyiza E.; Shumbusho F.; Wesson
In the general population 45% of women delivered at HF (IDHS 2007-08)
In the general population 45% of women delivered at HF (IDHS 2007-08)

Remaining challenges - 2
• Insufficient integration and linkages within
maternal,
newborn and child health services, and other sexual
and
reproductive health services, including family
planning
• Limited resources and operational guidance for
effective
implementation of primary prevention and
prevention of
unintended pregnancies among women living with
HIV in
the specific context of PMTCT
• Insufficient integration and linkages within
maternal,
newborn and child health services, and other sexual
and
reproductive health services, including family
planning
• Limited resources and operational guidance for
effective
implementation of primary prevention and
prevention of
unintended pregnancies among women living with
HIV in
the specific context of PMTCT

Preventing HIV infection in women
Preventing HIV infection in women
Preventing HIV infection in all women
(and their partners)
Preventing HIV infection in all women
(and their partners)
Preventing HIV infection in pregnant women(and their partners)
Preventing HIV infection in pregnant women(and their partners)
Within national multi-sectoral
prevention strategies
Specific interventions targeting
pregnant women
PMTCT as an opportunity to operationalize combination
prevention

• Provide HIV testing and counselling at family planning clinics (on-site or through referrals)
• Provide FP services with focus on condom-based dual protection at PMTCT sites, STIs clinics and ART centers
• Provide access to emergency contraception services and post-abortion care services
• Capacity-building of service providers in addressing SRH needs and rights of women living with HIV
Prevention of unintended pregnancies among women living with HIV

Remaining challenges-3
• Lack of operationalisation of community-based
interventions (lay counselors, peer support
groups, Mother2Mother) as integral components of
national scale-up strategies
• Poor data collection, reporting, analysis and use,
and
limited capacity for operation research to inform
policy formulation, advocacy and programming
• Lack of operationalisation of community-based
interventions (lay counselors, peer support
groups, Mother2Mother) as integral components of
national scale-up strategies
• Poor data collection, reporting, analysis and use,
and
limited capacity for operation research to inform
policy formulation, advocacy and programming

Opportunities
• Current momentum for health systems strengthening (IHP+, H4, etc)
• Current momentum for virtual elimination of mother-to-child transmission of HIV
⁃ UNAIDS joint programme: focus of all the UNAIDS cosponsors on PMTCT as a priority area by making the resources of the UN work for results at the country level
⁃ The Global Fund has declared PMTCT a priority: reprogramming existing grants to accelerate scale-up in 10 countries (Ethiopia, Kenya, Malawi, Mozambique, Nigeria, South Africa, Tanzania, Uganda, Zambia, and Zimbabwe)
⁃ PEPFAR’s second five-year authorization includes as target PMTCT coverage of 80%

Global strategic vision for virtual elimination of mother-to-child
transmission of HIV - 1
1.Strategic shift from HIV infection averted and HIV-free survival focus towards the overall goal of improved maternal and child health and survival for an HIV-free and AIDS-free generation
2. Increasing access and coverage by bringing services
closer to those in need through decentralization and
devolution to subnational authorities and subnational
health management structures

Global strategic vision for virtual elimination of mother-to-child
transmission of HIV - 2
3.Using implementation of PMTCT as an opportunity to strengthen health systems with special attention to MNCH services
4. Operationalising integration and linkages within
MNCH services, other SRH services including FP and
HIV care and treatment services to ensure better
continuum of care for women and children

Way forward -1 1. Alignment and harmonization among national programmes
(HIV/PMTCT, MNCH, Nutrition, SRH, …) and partners around population-based national scale up plans and sub-national operational plans to address programme fragmentation and parallel funding
2. Promoting and supporting decentralisation and devolution: operationalizing planning, financing and implementation of decentralised delivery of services using sub-national level as unit of planning, implementation and M&E and making resources available
3. Scaling up innovations as integral components of continuum of care for children and mothers (Point of care CD4; Mother-Baby-Packs; Rapid SMS) to accelerate expansion of services

Way forward - 2•
4.Making resources available and fostering sustainability through induction of changes in resource allocation including innovative approaches such as performance-based financing
5. Improvement of infrastructure and equipment, optimizing working conditions, and improve efficient delivery of services:
- Rehabilitation and equipment of ANC, delivery care, laboratory and pharmacy facilities
- Reorganization of service delivery mechanisms

Way forward - 3
4. Closing the gap between health facility-based approach and communities through partnering with individuals, families and communities, including PLWH and male partners in service provision, curbing stigma and discrimination and demand creation
6. Closing the knowledge gap through promotion of and support to impact evaluation and operational research to inform policies, advocacy, and programming

Ways forward - 4
7. Promoting and supporting access to the best available science for all in need by:
- Scaling up more efficacious ARV regimens for PMTCT
- Early diagnosis and ART for infants and children
- Redoubling our efforts for optimal and safe infant and young child feeding practices
8. Building national capacity in M&E (data collection, analysis and use), progress tracking, and operational research (including impact assessment) to inform advocacy, programming and scale up

Two Worlds, Two Realities, One Hope: Two Worlds, Two Realities, One Hope:
addressing inequity for social justice