Renal Physiology 1
9
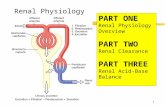
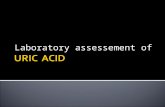
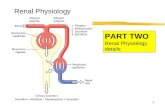
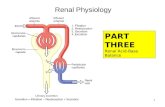
1 | Page Mar Mariano PHYSIO B 1.1 RENAL PHYSIOLOGY PT. 1 [DR. VILA] FEU-NRMF INSTITUTE OF MEDICINE 11.03.14 – 11.04.14 [1MD-D] Kidneys o Part of the urinary system o Formation of urine o Excretion of waste products, specifically water-soluble waste products o A small portion of water-soluble waste products is excreted via the skin as sweat, but majority is excreted by the kidneys as urine Function: o Excretion of metabolic waste products o Regulate water and electrolyte balance o Regulate body fluid osmolality and blood pressure *Body fluid: specifically extracellular fluid (ECF) ECF as: 1. Intravascular fluid – within blood vessels 2. Interstitial fluid – space bet. blood vessels and cells 3. Transcellular fluid – space other than intravascular and interstitium (ex.) CSF, perilymph, endolymph, peritoneal, pericardial, etc. *Vascular Physio Review* Increase fluid intake increase BV increase VR increase EDV increase SV increase CO increase BP BP= CO x TPR CO= HR x SV SV= EDV – ESV o Regulate arterial BP o Regulate acid-base balance o 3 systems maintaining acid-base balance: Blood, respiratory and renal o Normal blood pH: 7.35 – 7.45 (slightly basic) o Regulate gluconeogenesis Physiologic Anatomy: Renal hilum – where blood vessels, nerves and lymph enter, where ureter exits 2 layers: o Outer cortex o Inner medulla (landmark: renal pyramids) Apex (renal papilla) of renal pyramids drains into minor calyx major calyx renal pelvis ureter Blood supply: Renal artery Segmental artery Interlobar artery Arcuate artery Interlobular artery Afferent arteriole Glomerular capillay Peritubular capillary Vasa Recta (Cortical nephron) (Juxtamedullary nephron) *True capillary – peritubular capillary
-
Upload
anny-alvrz -
Category
Documents
-
view
236 -
download
6
description
you probably won't understand this. But this is a transcribed note
Transcript of Renal Physiology 1
1 | P a g eMar Mariano PHYSIO B 1.1 RENAL PHYSIOLOGY PT. 1 [DR. VILA] FEU-NRMF INSTITUTE OF MEDICINE 11.03.14 11.04.14 [1MD-D] Kidneys oPart of the urinary system oFormation of urine oExcretionofwasteproducts,specifically water-soluble waste products oAsmallportionofwater-solublewaste productsisexcretedviatheskinassweat, butmajorityisexcretedbythekidneysas urine Function: oExcretion of metabolic waste products oRegulate water and electrolyte balance oRegulatebodyfluidosmolalityandblood pressure *Body fluid: specifically extracellular fluid (ECF) ECF as: 1.Intravascular fluid within blood vessels 2.Interstitialfluidspacebet.bloodvessels and cells 3.Transcellularfluidspaceotherthan intravascularandinterstitium(ex.)CSF, perilymph,endolymph,peritoneal, pericardial, etc. *Vascular Physio Review* IncreasefluidintakeincreaseBVincreaseVR increaseEDVincreaseSVincreaseCO increase BP BP= CO x TPR CO= HR x SV SV= EDV ESV oRegulate arterial BP oRegulate acid-base balance o3systemsmaintainingacid-base balance:Blood,respiratoryand renal oNormalbloodpH:7.357.45 (slightly basic) oRegulate gluconeogenesis Physiologic Anatomy: Renalhilumwherebloodvessels,nervesand lymph enter, where ureter exits 2 layers: oOuter cortex oInner medulla (landmark: renal pyramids) Apex(renalpapilla)ofrenalpyramidsdrainsinto minor calyx major calyx renal pelvis ureter Blood supply: Renal artery Segmental artery Interlobar artery Arcuate artery Interlobular artery Afferent arteriole Glomerular capillay Peritubular capillaryVasa Recta (Cortical nephron) (Juxtamedullary nephron) *True capillary peritubular capillary 2 | P a g eMar Mariano Blood Supply: Starlings forces: 1.Capillary Hydrostatic Pressure 2.CapillaryOsmoticPressureofPlasma Protein Pressure 3.Interstitium/tissue HP 4.Interstitium/ tissue OPPP oHydrostatic Pressure drive away fluid oOsmoticPressureofPlasmaProteins attractsfluid(contributedlargelyby proteins) Forces favoring filtration: ocHP & iOPP Forces favoring reabsorption: ocOPP & iHP Glomerular capillary: oHigh pressure capillary bed o60mmHg oFavors filtration Peritubular capillary / vasa recta oLower pressure o13mmHg oFavors reabsorption Renal Blood Flow: oAbout22%ofthecardiacoutput (1100mL/min) Structural & Functional unit of the kidney: Nephron: o1 million per kidney oAfter 40 years old, there will be a decrement of 10% per 10 years Types of nephron: 1.Cortical outer-cortex and mid-cortex oShorter loop of Henle oMore numerous oSupplied by peritubular capillary 2.Juxtamedullary oLonger and straighter loop of Henle oSupplied by vasa recta oConcentrates urine Nephronfromrenalcorpuscle(glomerulus+ Bowmans capsule) to distal tubule Urineferoustubuleconnectingtubulesand collecting tubuless Urge to urinate: 150mL (for a normal 70kg person) Urinary/micturition reflex: 700mL or 1L 3 | P a g eMar Mariano Filtration barrier: 1.Basement membrane oLamina densa: central dense layer oLaminararainternaandexterna proteoglycanswhichcontributeto the membranes negative charge 2.Glomerular endothelium ofenestrated,withfixednegative chargesthatinhibitpassageof plasma proteins 3.Layerofepithelialcells(podocytes) surrounding the glomerulus Glomerular capillary: oFenestrated capillary without diaphragm oSizeselectivedoesnotallowlarge molecules to pass through oShapeselectivebasallaminaisusually electronegative,thereforedoesnotallow negative substances to pass through oShape selective Net Glomerular Filtration ColloidosmoticpressureinBowmansspaceis absentorzero,supposedly,becauseproteinisnot filteredbytheglomerulus.Remember,protein largelycontributestoosmoticpressure.Since walang protein na-filter, walang osmotic pressure. Colloid osmotic pressure is high in efferent arteriole and peritubular capillaries. Why?Sincehindina-filtersiprotein,pupuntasiya ngayonsaefferentarterioleatperitubular capillaries,whichthencontributestoahigher osmotic pressure, favoring reabsorption. Reabsorption= cOPPP + iHP = 13mmHg + 37mmHg = 50mmHg Filtration= cHP + iOPPP =60mmHG +0mmHg(zero pressure because no proteins were filtered) Net filtration pressure= Filtration Reabsorption = 60mmHg 50mmHg = +10mmHg (if positive value= filtration; negative value= reabsorption) Intraglomerular mesangial cells: oContractile in response to angiotensin oPhagocytic 4 | P a g eMar Mariano JG Apparatus: 1.Macula densa: oDetermine Na content in the filtrate oFound near distal tubule oColumnar cells 2.JG cells: oSecrete renin oModifiedtunicamediaofthe afferent arteriole 3.Lacis cells: oProduce erythropoietin oMainlyserveascommunication between macula densa and JG cells According to Doc Vila: **Truelocationofmaculadensa:Thickascending limbofLoopofHenleANDthebeginningofthe distal tubule. **MostoftheJGcellsarelocatednearafferent arteriole.However,somearealsolocatednear efferent arteriole. Urine Formation: Plasmafilteredbyglomerulusfiltered substancesmoveintoBowmanscapsulepass through the tubules for reabsorption secretion of ofothersubstancesfromperitubularcapillariesto tubules excretion Therefore: Excretion = Filtration Reabsorption + Secretion Waste Materials: Urea: from amino acids Creatinine: from muscle degradation Uric Acid: from nucleic acids Bilirubin: from hemoglobin Renal Clearance: Therenalclearance(C)ofasubstance(s)isthe volume of plasma required to supply the amount of substanceexcretedintheurineduringagiven period of time. =
5 | P a g eMar Mariano oPrincipleofclearance:Whatistakenin should be equal to what is given out. oSource of input for the kidney: Renal artery oOutput:Maygointotheurineoritmay remain the plasma. Why? Notallsubstancesarefilteredsoitgoesto theefferentarteriolesandperitubular capillaries or into the urine. A.Substanceisfreelyfilteredbyglomerular capillaries,neitherreabsorbednor secreted. Excretion rate = Filtration rate (Ex: Waste products like creatinine) B.Subtanceisfreelyfiltered,andpartially reabsorbed. Excretion= Filtration Reabsorption (Ex: electrolytes like Na and Cl) C.Substanceisfreelyfilteredandcompletely reabsorbed.Therefore,nosubstanceis excreted. (Ex: Glucose and amino acids) D.Substanceisfreelyfiltered,notreabsorbed andpartiallysecretion.(Ex:Organicacids and bases) Glomerular Filtration Rate (GFR) =
GFR =125mL/min 7500mL/min 180L/day =
=
ThegoldstandardformeasuringtheGFRisinulin, becauseit is freely filtered, and neither reabsorbed norsecreted.However,inulinisnotproducedby the body and has to be introduced to the subject via IV infusion. TheroutinesubstanceusedtodetermineGFRis creatinine,becauseitisnaturallyproducedbythe body.Creatinineisfreelyfiltered,butitispartially secreted (20%). For a substance to be used as a measure for GFR: oMust be freely filtered oNot reasbsorbed nor secreted oNot metabolized or synthesized by the body (especially the kidneys) oDoes not alter filtration rate Filtration Fraction =
, where RPF = Renal Plasma Flow Although,nearlyalltheplasmathatentersthe kidneyspassesthroughtheglomerulus, approximately 10% does not. The portion of filtered plasma is termed filtration fraction. 6 | P a g eMar Mariano Factors affecting GFR: oFlow = volume / time oVelocity = distance / time Vasodilation = Increase flow; decrese velocity oIncreasediametertoaccommodatemore substance increase flow Vasoconstriction = Decrese flow, increase velocity oDecreasediametertoaccommodateless substance decrease flow If afferent arterioles VASODILATE: oMore flow oLess hydrostatic pressure oLess GFR If afferent arterioles VASOCONSTRICT: oLess flow oMore hydrostatic pressure oMore hydrostatic pressure If efferent arterioles VASODILATE: oMore flow oLess hydrostatic pressure oLess GFR If efferent arterioles VASOCONSTRICT: oLess flow oMore hydrostatic pressure oMore GFR BOTH afferent and efferent arterioles VASODILATE: oMore flow oSAME GFR
Renal Blood Flow: o22% of the CO (1,100mL/min) Based on Ficks Principle: =
Q= blood flow P= arterial pressure R= resistance to flow oVasodilate:increaseflow,decrease resistance oVasoconstrict: increase resistance, decrease flow = ClearancecanbeusedtoestimateRBF.Substance usedtomeasureRBFispara-aminohipuricacid (PAH).Itisfreelyfiltered,neithersecretednor reabsorbed and not metabolized by the body. =
=
Effective Renal Plasma Flow =
=
Extractionratioisthedifferencebetween subsancesinarteryandveinoversubstamcesin artery 7 | P a g eMar Mariano Autoregulation: oInherentmechanismofkidneyin maintainingRBFandGFRatarelatively constantleveloveranarterialpressure range between 80 170mmHg oAlsoinfluencedbynervousmechanism, hormones, autocoids and others. *CVS Review: Mean Arterial Pressure= Diastolic Pressure 1/3 Pulse Pressure = 80- 170mmHg Mechanisms: 1.Myogenic mechanism oPressure-sensitive oTendency of vascular smooth muscle to contract when pressure increases oWhen arterial pressure increases, and afferent arterioles is stretched, smooth mucscle contract oThe increase in resistance of the arteriole offsets the increase in pressure, therfore making the RBF and GFR constant, provided that P and R remain constant. oBased on Ficks Principle: =
2.Glomerulotubular Feedback oThe greater amount of substance being filtered will have a concomittant amount of substance being reabsorbed to maintain homeostasis oConstant proportion of substances 3.Tubuloglomerular Feedback oJG apparatus oWhen GFR increases and Na concentration also increases, which is detected by the macula densa 8 | P a g eMar Mariano oThiswillleadthemaculadensatodegrade ATP to adenosine oAdenosinewillcausevasoconstrictionof the AFFERENT arteriole due to the presence Adenosine 1 receptors oVasoconstriction will then decrease the GFR back to normal oWhenGFRdecreases,thereislowNa concentration,whichisdetectedbythe macula densa oMacula densa will then cause the JG cells to secrete renin oReninwillthenactivateangiotensinogento angiotensin I oAngiotensinIwillthenbeconvertedto angiotensin II by ACE in the lungs oAngiotensinIIwillthencause vasoconstriction of the EFFERENT arteriole, causing an increase of GFR back to normal 4.Nervous mechanism oExclusively Sympathetic NS oStrong activation of renal sympa: oVasoconstrict renal arterioles oDecrease RBF and GFR oModerate or mild activation: oLittle influence on RBF and GFR 5.Hormones and autocoids oNorepinephrine oEpinephrine(80%producedbyadrenal medulla) oEndothelin -oMost potent vasoconstrictor oReleased from damaged endothelial cells of the kidneys oNEandEpicanconstricttheafferentand efferentarteriolesbutonlyiftheyarein high amounts oAngiotensin II -oVasoconstrict EFFERENT arteriole oEndothelin-derived Nitric Oxide oVasodilate oIncreaseGFRbuteventually becomes stable oProstaglandin and Bradykinin -oVasodilate oIncreaseGFR,buteventually becomes stable Nerve Innervation oSympathetic NS oAct via beta receptors present in JG cells oJG cells secrete renin oReninwillcauseNareabsorption particularly in the proximal tubules oIncreaseNaIncreasefluidintake increase BV increase VR increase EDV increaseSVincreaseCOincrease BP Obligatoryreabsorptionisseenintheproximal tubules due to the presence of brush borders. Tubular Reabsorption 2 reabsorption pathways: oTranscellular:Luminalandbasolateral membrane oParacellular: via tight junctions Transport Limitation oTM Limited (Transport Maxima) oGlucose,SO4,PO4,aminoacids, lactate, malate and Vitamin C oActive transport oExhibits saturation oWhensaturated,rateoftransport remains constant 9 | P a g eMar Mariano oGradient-time Limited oNa, Cl and HCO3 oMostlypassive,butcanalsobe active transport oThegreatertheconcentration gradient,moresubstancesare transported oThelongerthetime,more substances are transported