![Coronary artery atherectomy reduces plaque shear strains: An … · 2015-08-31 · related biological destabilization of atherosclerotic plaques [2]. The prospective evaluation of](https://static.fdocuments.in/doc/165x107/5f3bd5dc7a1ed97f8c0c69e1/coronary-artery-atherectomy-reduces-plaque-shear-strains-an-2015-08-31-related.jpg)
Relation of matrix-metalloproteinase 3 found in coronary lesion samples retrieved by directional...
6
Relation of Matrix-Metalloproteinase 3 Found in Coronary Lesion Samples Retrieved by Directional Coronary Atherectomy to Intravascular Ultrasound Observations on Coronary Remodeling Paul Schoenhagen, MD, D. Geoffrey Vince, PhD, Khaled M. Ziada, MD, Samir R. Kapadia, MD, Michael A. Lauer, MD, Timothy D. Crowe, BS, Steven E. Nissen, MD, and E. Murat Tuzcu, MD We investigated the relation between the presence of matrix-metalloproteinases (MMPs) and direction of re- modeling in the coronary lesions of 35 patients. Positive arterial remodeling describes a compensatory expan- sion of the external elastic membrane (EEM) area of atherosclerotic lesions. An association between positive remodeling and unstable clinical presentation has been previously described. However, the pathophysiology of the remodeling process is not completely understood. Preinterventional intravascular ultrasound images and directional atherectomy (DCA) samples were analyzed. The remodeling ratio was calculated as the EEM area at the lesion site divided by the EEM area at the proximal reference. Positive, intermediate, and negative remod- eling were defined as ratios of >1.05, 0.95 to 1.05, and <0.95, respectively. The histologic samples were immu- nostained for MMP-1, -2, -3, and -9. Positive, interme- diate, and negative remodeling was present in 15, 7, and 13 lesions, respectively. Mild and intense cell-asso- ciated staining for MMP-1 was found in 21 (68%) and 10 (32%) patients, respectively. Staining for MMP-3 was mild in 20 patients (67%) and intense in 10 patients (33%). Immunostaining for MMP-2 and -9 was mild in all samples. Intense staining for MMP-3 was significantly more common in lesions with positive than negative and/or intermediate remodeling (58% vs 17%; p 0.04; p 0.053 after adjustment for gender). Thus, in this in vivo intravascular ultrasound and histologic study, increased cell-associated MMP-3 staining was associated with positive arterial remodeling. 2002 by Excerpta Medica, Inc. (Am J Cardiol 2002;89:1354 –1359) R ecently, we and others demonstrated a strong association between positive remodeling and un- stable clinical presentation in patients with coronary artery disease. 1–3 Because both matrix-metalloprotein- ase (MMP) activity and positive remodeling are asso- ciated with plaque instability, 4,5 we hypothesized that MMPs might play a role in the pathophysiology of coronary remodeling. Accordingly, we investigated the relation between MMP staining and direction of remodeling in human coronary lesions. We performed in vivo intravascular ultrasound and subsequently used directional atherectomy (DCA) to obtain histo- logic specimens of the imaged lesion site. The inten- sity of staining for various MMPs was compared with the direction and extent of coronary remodeling as assessed by intravascular ultrasound. METHODS Patient population: The study population consisted of 35 patients who had DCA performed for a single epicar- dial lesion in a native vessel in 1994. Clinical data including age, gender, presence or absence of risk factors for coronary disease (diabetes mellitus types 1 and 2, hypertension, total cholesterol, smoking history, and family history), and angina severity were available from an interventional database. Clinical presentation was de- fined as stable or unstable. In the stable group, only those patients with stable angina and unchanged symptoms for 2 months were included. The unstable group included patients with unstable angina and Braunwald class IIB or IIIB symptoms. Coronary intravascular ultrasound imaging: Intra- vascular ultrasound imaging was performed using standard techniques as previously reported. 6 Briefly, a 30-MHz 3.5Fr monorail ultrasound catheter (Boston Scientific, Scimed Inc., Maple Grove, Minnesota) in- terfaced with a scanner (Hewlett-Packard, Andover, Massachusetts) was employed. After coronary angiog- raphy, anticoagulation with heparin, and intracoronary administration of nitroglycerin, the ultrasound cathe- ter was inserted over a guidewire distal to the target lesion site. The ultrasound catheter was then with- drawn manually during continuous image recording on 1/2-inch super-VHS videotape. From the Departments of Cardiology and Biomedical Engineering, The Cleveland Clinic Foundation, Cleveland, Ohio; Department of Cardi- ology, University of Washington, Seattle, Washington; and Depart- ment of Cardiology, Michigan State University, Kalamazoo, Michi- gan. Dr. Schoenhagen is supported by a postdoctoral fellowship award from the Ohio Valley Regional Affiliate of the American Heart Association, St. Petersburg, Florida. Manuscript received November 9, 2001; revised manuscript received and accepted February 18, 2002. Address for reprints: E. Murat Tuzcu, MD, The Cleveland Clinic Foundation, F 25, 9500 Euclid Ave., Cleveland, Ohio 44195. E-mail: [email protected]. 1354 ©2002 by Excerpta Medica, Inc. All rights reserved. 0002-9149/02/$–see front matter The American Journal of Cardiology Vol. 89 June 15, 2002 PII S0002-9149(02)02346-9
-
Upload
paul-schoenhagen -
Category
Documents
-
view
214 -
download
2
Transcript of Relation of matrix-metalloproteinase 3 found in coronary lesion samples retrieved by directional...

Relation of Matrix-Metalloproteinase 3Found in Coronary Lesion SamplesRetrieved by Directional Coronary
Atherectomy to Intravascular UltrasoundObservations on Coronary Remodeling
Paul Schoenhagen, MD, D. Geoffrey Vince, PhD, Khaled M. Ziada, MD,Samir R. Kapadia, MD, Michael A. Lauer, MD, Timothy D. Crowe, BS,
Steven E. Nissen, MD, and E. Murat Tuzcu, MD
We investigated the relation between the presence ofmatrix-metalloproteinases (MMPs) and direction of re-modeling in the coronary lesions of 35 patients. Positivearterial remodeling describes a compensatory expan-sion of the external elastic membrane (EEM) area ofatherosclerotic lesions. An association between positiveremodeling and unstable clinical presentation has beenpreviously described. However, the pathophysiology ofthe remodeling process is not completely understood.Preinterventional intravascular ultrasound images anddirectional atherectomy (DCA) samples were analyzed.The remodeling ratio was calculated as the EEM area atthe lesion site divided by the EEM area at the proximalreference. Positive, intermediate, and negative remod-eling were defined as ratios of >1.05, 0.95 to 1.05, and<0.95, respectively. The histologic samples were immu-
nostained for MMP-1, -2, -3, and -9. Positive, interme-diate, and negative remodeling was present in 15, 7,and 13 lesions, respectively. Mild and intense cell-asso-ciated staining for MMP-1 was found in 21 (68%) and 10(32%) patients, respectively. Staining for MMP-3 wasmild in 20 patients (67%) and intense in 10 patients(33%). Immunostaining for MMP-2 and -9 was mild in allsamples. Intense staining for MMP-3 was significantlymore common in lesions with positive than negativeand/or intermediate remodeling (58% vs 17%; p �0.04; p � 0.053 after adjustment for gender). Thus, inthis in vivo intravascular ultrasound and histologicstudy, increased cell-associated MMP-3 staining wasassociated with positive arterial remodeling. �2002by Excerpta Medica, Inc.
(Am J Cardiol 2002;89:1354–1359)
Recently, we and others demonstrated a strongassociation between positive remodeling and un-
stable clinical presentation in patients with coronaryartery disease.1–3Because both matrix-metalloprotein-ase (MMP) activity and positive remodeling are asso-ciated with plaque instability,4,5 we hypothesized thatMMPs might play a role in the pathophysiology ofcoronary remodeling. Accordingly, we investigatedthe relation between MMP staining and direction ofremodeling in human coronary lesions. We performedin vivo intravascular ultrasound and subsequentlyused directional atherectomy (DCA) to obtain histo-logic specimens of the imaged lesion site. The inten-sity of staining for various MMPs was compared withthe direction and extent of coronary remodeling asassessed by intravascular ultrasound.
METHODSPatient population: The study population consisted of
35 patients who had DCA performed for a single epicar-dial lesion in a native vessel in 1994. Clinical dataincluding age, gender, presence or absence of risk factorsfor coronary disease (diabetes mellitus types 1 and 2,hypertension, total cholesterol, smoking history, andfamily history), and angina severity were available froman interventional database. Clinical presentation was de-fined as stable or unstable. In the stable group, only thosepatients with stable angina and unchanged symptoms for�2 months were included. The unstable group includedpatients with unstable angina and Braunwald class IIB orIIIB symptoms.
Coronary intravascular ultrasound imaging: Intra-vascular ultrasound imaging was performed usingstandard techniques as previously reported.6 Briefly, a30-MHz 3.5Fr monorail ultrasound catheter (BostonScientific, Scimed Inc., Maple Grove, Minnesota) in-terfaced with a scanner (Hewlett-Packard, Andover,Massachusetts) was employed. After coronary angiog-raphy, anticoagulation with heparin, and intracoronaryadministration of nitroglycerin, the ultrasound cathe-ter was inserted over a guidewire distal to the targetlesion site. The ultrasound catheter was then with-drawn manually during continuous image recordingon 1/2-inch super-VHS videotape.
From the Departments of Cardiology and Biomedical Engineering, TheCleveland Clinic Foundation, Cleveland, Ohio; Department of Cardi-ology, University of Washington, Seattle, Washington; and Depart-ment of Cardiology, Michigan State University, Kalamazoo, Michi-gan. Dr. Schoenhagen is supported by a postdoctoral fellowshipaward from the Ohio Valley Regional Affiliate of the American HeartAssociation, St. Petersburg, Florida. Manuscript received November9, 2001; revised manuscript received and accepted February 18,2002.
Address for reprints: E. Murat Tuzcu, MD, The Cleveland ClinicFoundation, F 25, 9500 Euclid Ave., Cleveland, Ohio 44195.E-mail: [email protected].
1354 ©2002 by Excerpta Medica, Inc. All rights reserved. 0002-9149/02/$–see front matterThe American Journal of Cardiology Vol. 89 June 15, 2002 PII S0002-9149(02)02346-9

Image analysis: A single operator who was blindedto the histologic results analyzed the intravascularultrasound images. The target lesion was selected asthe site with the smallest luminal diameter (MLD) inthe segment where DCA was performed. A pullbackafter DCA confirmed that the tissue was retrievedfrom this segment. The proximal reference segmentwas chosen as the least diseased site proximal to thetarget lesion without any intervening side branch.Short segments of videotape were digitized at 30frames/s into a 640 � 480-pixel, 8-bit gray scaleimage matrix for analysis.
Ultrasound measurements and calculations: At eachselected site, the lumen and external elastic membrane(EEM) areas were traced manually using the intimalleading edge boundary and the leading edge of theadventitia, respectively. The plaque & media area wascalculated as the difference between EEM and lumenarea. Percent stenosis was calculated as:
Stenosis �%� � �plaque area/EEM area� � 100.
Ultrasound definitions of remodeling: The remodel-ing ratio was defined as the ratio of the EEM area at thelesion site to the EEM area at the proximal reference site(Figure 1). Three remodeling categories were defined, aspreviously reported.1,7 Positive remodeling was definedas a remodeling ratio �1.05, intermediate remodeling asa ratio between 0.95 and 1.05, and negative remodelingas a ratio �0.95. The negative and intermediate groupswere combined for purposes of analysis.
Histology: The DCA tissue samples were placed intissue fixative (Histochoice, Amresco, Solon, Ohio) im-mediately after the interventional procedure and fixed for
12 hours. The tissue was then pro-cessed and paraffin embedded ac-cording to standard laboratory proce-dures. Sections were cut from theseparaffin blocks at 4 �m at the time ofanalysis, collected onto electrostati-cally charged slides, and baked at 60°C for 60 minutes.
Immunohistochemical staining proce-dure: Paraffin was removed from thebaked tissue sections in 3 changes ofxylene, and the tissue hydratedthrough graded alcohols before rins-ing in phosphate-buffered saline. Im-munohistochemical staining was per-formed using a Jung Histostainer(Leica, Illinois), with processing oc-curring at 30° C. The first stage of theprocedure involved the application of1% hydrogen peroxide solution inmethanol for 5 minutes to removeany endogenous peroxidase presentin the tissue section. A blocking so-lution comprising a 1:10 dilution ofnormal rabbit serum (Dako, Carpin-teria, California) in phosphate-buff-ered saline was then added for 10minutes before application of the pri-mary antibody. Eight antibodies were
selected for staining: antimacrophage (HAM56); anti–T-lymphocyte (CD43/DF-T1); antismooth muscle actin(SMA/1A4); anti–HLA-DR-� (TAL-1B5); anti-MMP-1(41 to 1ES); anti–MMP-2 (42 to 5D11); anti–MMP-3(56 to 2A4); and anti–MMP-9 (55 to 2A4). The anti-MMP antibodies were obtained from ICN Biochemical(Costa Mesa, California), and the remaining antibodiesfrom Dako Corporation. Incubation occurred at 30°C for60 minutes, and a 1:200 dilution of biotinylated rabbitantimouse polyclonal antibody (Dako) was added for afurther 30 minutes. The antibody was labeled using anElite avidin/biotin/peroxidase complex (Vector Labora-tories, Burlingame, California) that was applied for 30minutes. The final stage comprised the addition of 3,3-diaminobenzidine as a chromogen (DABKit, VectorLaboratories). Between each step, the slides were rinsedtwice for 2 minutes in phosphate-buffered saline. Fol-lowing staining, the sections were rinsed in distilledwater, counterstained with hematoxylin, dehydrated,
FIGURE 1. Longitudinal section through a vessel segment with apositively remodeled lesion. White arrows, proximal referenceand lesion sites.
FIGURE 2. Postmortem human coronary artery specimen with positive immunostainingfor MMP-3 (A) and smooth muscle actin (B) (magnification � 40). Negative control forMMP staining (C), positive control for MMP-3 (D), and MMP-1 (E) in human tissue ofinvasive breast carcinoma (magnification �200, reduced 33%).
CORONARY ARTERY DISEASE/METALLOPROTEINASES AND REMODELING 1355

cleared in xylene, and a coverslip placed on the section.Figure 2 shows examples of positive and negative con-trols for MMP staining.
Qualitative evaluation of MMP immunostaining: Thetissue sections were independently reviewed by 2 ofthe investigators who were blinded to the remodelingstatus. The pattern of staining in each individual sec-tion was evaluated qualitatively by assessing the esti-mated percentage of cells with cell-associated stainingand the intensity of staining. Based on these criteria,staining was graded as mild versus intense. The stain-ing pattern was analyzed in several different areas of1 section from each sample. The interobserver agree-ment was 93% (� � 0.85). The assessment was re-
peated after 4 weeks. The intraob-server agreement was 96% (� �0.93)
Tissue quantification of cell surfacemarkers: Cell quantification was per-formed using an image analysis soft-ware custom engineered in the Depart-ment of Biomedical Engineering.8 Thestained tissue sections were capturedinto 2,048 � 2,048 pixel images, at256 gray levels, using an Eikonix78/99 digital scanner (Kodak, Roches-ter, New York). Each image was dis-played on a Gould IP9527 image pro-cessor and atherectomy specimens out-lined manually. A computer-assistedthresholding algorithm (Castleman,Digital Image Processing, Prentice-Hall, Inc., Upper Saddle River, NewJersey) was used to create a binaryimage where 0 represented no stainingand 1 positive staining, and a histo-gram was computed for each piece oftissue. The histograms for all tissuesections of individual slides weresummed, and the percent positive areawas computed by dividing the totalnumber of positive pixels on an imageby the total number of pixels withinthe outlined specimen.
Statistical analysis: Continuousdata were described as mean � SD.Continuous variables were comparedusing the unpaired t test. Categoricalvariables were compared using Fish-er’s exact test. A p value �0.05 wasconsidered statistically significant. Theassociation between MMP stainingand direction of remodeling was alsotested after adjustment for gender byuse of a logistic regression model.
RESULTSPatients: The study group consisted
of 35 patients (69% men). Mean agewas 61 � 11 years (range 43 to 82).The risk factor profile showed serumtotal cholesterol �200 mg/dl in 31%,
diabetes mellitus (type 1 or 2) in 29%, a positive familyhistory of coronary disease in 17%, systemic hyperten-sion in 51%, and history of smoking in 63%. Clinicalpresentation included unstable angina in 25 patients(71%) and stable angina in 10 patients (29%).
Ultrasound characteristics of lesion and referencesite: The lesion was located in the left anterior de-scending artery in 22 patients (63%), the left circum-flex artery in 2 patients (6%), and the right coronaryartery in 11 patients (31%). All lesions were located inrelatively large proximal coronary segments. The per-cent of EEM area occupied by atheroma was 46.0 �8.9% at the proximal reference and 86.1 � 3.1% at thelesion site.
TABLE 1 Clinical and Demographic Characteristics
Positive RemodelingNegative/Intermediate
Remodeling p Value(n � 15) (n � 20)
Age (yrs) 62 � 11 60 � 11 0.6Men 7 (47%) 17 (85%) 0.03Diabetes mellitus 4 (27%) 6 (30%) �0.9Systemic hypertension 10 (67%) 8 (40%) 0.2Total cholesterol �200 mg/dl 6 (40%) 5 (25%) 0.5Cigarette smoker 9 (60%) 13 (65%) �0.9Family history of CAD 3 (20%) 3 (15%) �0.9Coronary narrowings
Left anterior descending 10 (67%) 12 (60%)Left circumflex 1 (7%) 1 (5%) 0.1Right coronary artery 4 (27%) 7 (35%)
Clinical presentationUnstable angina 11 (73%) 14 (70%) �0.9Stable angina 4 (27%) 6 (30%)
CAD � coronary artery disease.
TABLE 2 Intravascular Ultrasound Measurements at Target and Reference Site
PositiveRemodeling
Negative/IntermediateRemodeling p Value
Adjustedp Value*
Proximal referenceEEM area (mm2) 15.4 � 4.4 19.7 � 4.5 0.009 0.04Lumen area (mm2) 8.3 � 2.7 10.6 � 3.1 0.03 0.1Plaque area (mm2) 7.0 � 2.6 9.1 � 2.6 0.03 0.06% stenosis 45.4 � 9.1 46.4 � 9.0 0.8 0.5
Culprit lesionEEM area (mm2) 18.0 � 5.0 17.6 � 5.2 0.8 0.6Lumen area (mm2) 2.2 � 0.5 2.6 � 1.0 0.2 0.1Plaque area (mm2) 15.8 � 4.8 15.0 � 4.4 0.6 0.3% stenosis 87.3 � 2.6 85.1 � 3.2 0.04 0.02Remodeling ratio 1.18 � 0.11 0.89 � 0.12 0.0001 0.0009
*Adjusted for gender using logistic regression.
TABLE 3 MMP Staining in Positive and Negative and/or Intermediate Groups
PositiveRemodeling
Negative/IntermediateRemodeling p Value
Adjustedp Value*
MMP-1 n � 13 n � 18Mild 9 (69%) 12 (67%) �0.9 0.9Intense 4 (31%) 6 (33%)
MMP-3 n � 12 n � 18Mild 5 (42%) 15 (83%) 0.04 0.053Intense 7 (58%) 3 (17%)
*p Value after adjustment for gender with logistic regression.
1356 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 89 JUNE 15, 2002

Remodeling calculations: The remodeling ratio forthe entire group was 1.01 � 0.19 (0.7 to 1.4). Fifteenlesions (43%) met the predefined criteria for positiveremodeling, 7 lesions (20%) showed intermediate re-modeling, and 13 lesions (37%) exhibited negativeremodeling. The remodeling ratio was 1.18 � 0.11(1.06 to 1.40), 1.01 � 0.04 (0.97 to 1.05), and 0.83 �0.10 (0.65 to 0.94) in the positive, intermediate, andnegative remodeling groups, respectively. In the groupcombining negative and intermediate remodeled le-sions (n � 20) the mean remodeling ratio was 0.89 �0.12 (0.65 to 1.05).
Orientation of the DCA samples: All samples in-cluded material from the intima and media but notfrom the adventitia.
MMP immunostaining: Cell-associated staining forMMP-1 was mild in 21 patients (68%) and intense in10 patients (32%). Staining for MMP-3 was mild in 20
patients (67%) and intense in 10 patients (33%). Im-munostaining for MMP-2 and -9 was mild in allsamples. MMP presence was associated with macro-phages and smooth muscle cells.
Tissue quantification: Cells staining for anti–T-lym-phocyte (CD43), antimacrophage (HAM 56), anti-smooth muscle actin (SMA), and anti–HLA-DR-�were quantified. For the entire group the averagestained area per sample was 0.46 � 0.73% (0% to2.69%) for CD43, 8.76 � 9.39% (0.13% to 45.09%)for HAM 56, 32.6 � 14.55% (9.48% to 59.28%) for�-actin, and 15.04 � 10.49% (2.23% to 43.55%) forHLA-DR-�.
Comparisons between remodeling groups: Demo-graphic and intravascular ultrasound characteristics ofthe groups with positive and negative and/or interme-diate remodeling are shown in Tables 1 and 2. Clinicalpresentation did not differ between the 2 groups.
Other than gender, there were no sig-nificant differences in the frequencyof conventional risk factors for cor-onary artery disease.
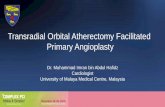
MMP immunostaining: The histo-logic results for the positive and neg-ative and/or intermediate remodelinggroups are shown in Table 3. Intensecell-associated staining for MMP-3was significantly more common inlesions with positive arterial remod-eling than in lesions with negativeand/or intermediate remodeling(58% vs 17%, p � 0.04) (Figures 3to 5). After adjustment for the differ-ences in gender, this difference hadborderline significance (p � 0.053).
There was no relation betweenMMP-3 immunostaining and clinicalpresentation. Intense staining forMMP-3 was found in 7 lesions(33%) related to unstable presenta-tion and 3 lesions (33%) related tostable presentation (p �0.9). No dif-ference in the quantity of positivestaining for cell surface markers was
found between the positive and negative and/or inter-mediate-remodeling group (p �0.1 for all).
DISCUSSIONUsing intravascular ultrasound, we have previously
shown that positive arterial remodeling of coronaryatherosclerotic lesions is associated with an unstableclinical presentation.1 To further elucidate the natureof this relation, we performed the present investiga-tion to determine the histologic characteristics of pos-itively remodeled plaques. Using intravascular ultra-sound guidance, we obtained atherosclerotic plaquesamples from 35 patients using a DCA device. Thisprocedure enabled confirmation of the site from whichthe specimen had been obtained and permitted mea-surements of the extent of remodeling at the target sitebefore intervention.
Despite a relatively small sample size, there were
FIGURE 3. Frequency of mild and intense staining for MMP-3 ineach remodeling group. Intense staining for MMP-3 was morecommon in positive remodeled lesions and mild MMP-3 stainingwas more common in negative and/or intermediate remodeledlesions.
FIGURE 4. Example of the association of positive remodeling and intense MMP-3staining. (A) and (D) show an intravascular ultrasound image of the proximal refer-ence; (B) and (E) show an image of the lesion site. (C) and (F) show a correspondinghistologic section with intense MMP-3 staining (magnification �200, reduced 37%).
CORONARY ARTERY DISEASE/METALLOPROTEINASES AND REMODELING 1357

significant differences in MMP-3 presence in patientswith positive versus negative and/or intermediate re-modeling. We found that increased cell-associatedMMP-3 was associated with positive arterial remod-eling. MMP-1, -2, and -9 were not different betweenlesions with positive and negative and/or intermediateremodeling. The quantity of inflammatory and inter-stitial cells was not different between the groups withpositive and negative and/or intermediate remodeling,indicating that the differences in MMP-3 presence arenot merely related to the quantity of inflammatorycells.
Changes in vascular architecture are mediatedthrough modulation of the extracellular matrix.9,10
The extracellular matrix of the vessel wall is a com-plex system of acellular substances, providing theconnective tissue scaffolding for cellular elements.The MMPs, a group of enzymes with the capability todegrade components of the extracellular matrix, havea particular prominent role in the continuous produc-tion and degradation of matrix components.11–13
The results of our and other studies suggest that thedegradation of extracellular matrix by MMP-3 may con-tribute to the expansion of the coronary vessel wall,which is characteristic of positive remodeling.14 In re-cent histologic studies, the relation between inflamma-tion, MMP and remodeling has been examined in fem-oral and coronary arteries.15–17 A relation between vesselexpansion and MMPs has also been described in abdom-inal aortic aneurysms.18–22 Aneurysm formation appearsto be initiated by an inflammatory response within theaortic wall, resulting in ongoing matrix destruction andeventual vessel expansion.23 Extensive inflammation anddestruction of musculoelastic vessel wall elements hasalso been found in dilated or ectatic human coronaryarteries.24–26
The use of clinical, interventional methods allows
simultaneous imaging and histologicexamination of coronary atheroscer-otic plaques in vivo but has method-ologic limitations.27 DCA cuts are di-rected at vessel areas with largeplaque burden and may not reliablyreflect focal processes such as theMMP expression in the plaque shoul-der of ruptured plaques. Immunocy-tochemistry provides information re-garding MMP presence, rather thanenzymatic activity.28 Our studygroup showed differences in genderdistribution between the remodelinggroups, and we cannot exclude thepossibility that the imbalances ingender, or other uncontrolled vari-ables, are in part responsible for thedifferences in MMP staining.
The association between in-creased MMP-3 staining and posi-tive arterial remodeling suggests apathophysiologic role of MMP-3 inthe remodeling process of coronaryarteries. Further studies are needed
to elucidate these complex interactions.
Acknowledgment: We want to thank Misty Garciafor her invaluable contribution in the processing andstaining of the tissue samples.
1. Schoenhagen P, Ziada KM, Kapadia SR, Crowe TD, Nissen SE, Tuzcu EM.Extent and direction of arterial remodeling in stable and unstable coronarysyndromes. Circulation 2000;101:598–603.2. Smits PC, Pasterkamp G, de Jaegere PPT, de Feyter PJ, Borst C. Angioscopiccomplex lesions are predominantly compensatory enlarged: an angioscopic andintracoronary ultrasound study. Cardiovasc Res 1999;41:458–464.3. Schoenhagen P, Vince DG, Ziada KM, Tsutsui H, Jeremias A, Crowe TD,Nissen SE, Tuzcu EM. Association of arterial expansion (expansive remodeling)of bifurcation lesions determined by intravascular ultrasonography with unstableclinical presentation. Am J Cardiol 2001;88:785–787.4. Galis ZS, Sukhova GK, Lark MW, Libby P. Increased expression of matrixmetalloproteinases and matrix degrading activity in vulnerable regions of humanatherosclerotic plaques. J Clin Invest 1994;94:2493–2503.5. Henney AM, Wakeley PR, Davies MJ, Foster K, Hembry R, Murphy G,Humphries S. Localization of stromelysin gene expression in atheroscleroticplaques by in situ hybridization. Proc Natl Acad Sci USA 1991;88:8154–8158.6. Tuzcu EM, Hobbs RE, Rincon G, Bott-Silverman C, De Franco AC, RobinsonK, McCarthy PM, Stewart RW, Guyer S, Nissen SE. Occult and frequenttransmission of atherosclerotic coronary disease with cardiac transplantation.Circulation 1995;91:1706–1713.7. Pasterkamp G, Borst C, Gussenhoven EJ, Mali WP, Post MJ, The SH, ReekersJA, van den Berg FG. Remodeling of de novo atherosclerotic lesions in femoralarteries: impact on mechanism of balloon angioplasty. J Am Coll Cardiol 1995;26:422–428.8. Vince DG, Demirkaya O, Cothren RM, Cothren RM, Cornhill JF, Tubbs RR.Quantitative analysis of inflammatory cells in aortic atherosclerosis of youngadults. Cardiovasc Pathol 1996;5:3–10.9. Gibbons GH, Dzau VJ. The emerging concept of vascular remodeling. N EnglJ Med 1994;330:20:1431–1438.10. Dzau VJ, Gibbons GH. Vascular remodeling. Mechanisms and implications.J Cardiovasc Pharmacol 1993;21(suppl):S1–5.11. Nagase H, Woessner JF. Matrix metalloproteinases. J Biol Chem 1999;274:21491–21494.12. Ye S, Humphries S, Henney A. Implication in vascular matrix remodelingduring atherogenesis. Clin Sci 1998;94:103–110.13. Dollery CM, McEwan JR, Henney AM. Matrix metalloproteinases andcardiovascular disease. Circ Res 1995;77:863–868.14. Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Com-pensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med1987;316:1371–1375.
FIGURE 5. Example of the association of negative remodeling and mild MMP-3 stain-ing. (A) and (D) show an intravascular ultrasound image of the proximal reference; (B)and (E) show an image of the lesion site. (C) and (F) show a corresponding histologicsection with mild MMP-staining (magnification �200, reduced 37%).
1358 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 89 JUNE 15, 2002

15. Pasterkamp G, Schoneveld AH, van der Wal AC, Haudenschild CC, ClarijsRJ, Becker AE, Hillen B, Borst C. Relation of arterial geometry to luminalnarrowing and histologic markers for plaque vulnerability: the remodeling para-dox. J Am Coll Cardiol 1998;32:655–662.16. Pasterkamp G, Schoneveld AH, Hijnen DJ, de Kleijn DP, Teepen H, van derWal AC, Borst C. Atherosclerotic arterial remodeling and the localization ofmacrophages and matrix metalloproteases 1, 2 and 9 in the human coronaryartery. Atherosclerosis 2000;150:245–253.17. Brown DL, Hibbs MS, Kearney M, Loushin C, Isner JM. Identification of92-kD gelatinase in human coronary atherosclerotic lesions. Circulation 1995;91:2125–2131.18. Freestone T, Turner RJ, Coady A, Higman DJ, Greenhalgh RM, Powell JT.Inflammation and matrix metalloproteinases in the enlarging abdominal aorticaneuryms. Arterioscler Thromb Vasc Biol 1995;15:1145–1151.19. Newman KM, Ogata Y, Malon AM, Irizarry E, Gandhi RH, Nagase H, TilsonMD. Identification of matrix metalloproteinase 3 (stromelysin-1) and 9 (gelati-nase B) in abdominal aortic aneurysm. Arterioscler Thromb 1994;14:1315–1320.20. McMillan WD, Tamarina NA, Cipollone M, Johnson DA, Parker MA, PearceWH. Size matters. The relationship between MMP-9 expression and aorticdiameter. Circulation 1997;96:2228–2232.21. McMillan WD, Patterson BK, Keen RR, Shively VP, Cipollone M, PearceWH. In situ localization and quantification of mRNA for 92-kD type IV colla-
genase and its inhibitor in aneurysmal, occlusive, and normal aorta. ArteriosclerThromb Vasc Biol 1995;15:1139–1144.22. Elmore JR, Keister BF, Franklin DP, Youkey JR, Carey DJ. Expression ofmatrix metalloproteinases and TIMP’s in human abdominal aortic aneurysms.Ann Vasc Surg 1998;12:221–228.23. Koch AE, Haines GK, Rizzo RJ, Radosevich JA, Pope RM, Robinson PG,Pearce WH. Human abdominal aortic aneurysms. Am J Pathol 1990;137:1199–1213.24. Hartnell GG, Parnell BM, Pridie RB. Coronary artery ectasia. Its prevalenceand clinical significance in 4993 patients. Br Heart J 1985;54:392–395.25. Swanton RH, Lea Thomas M, Coltart DJ, Jenkins BS, Webb-Peploe MM,Williams BT. Coronary artery ectasia—a variant of occlusive coronary arterio-sclerosis. Br Heart J 1978;40:393–400.26. Berkoff HA, Rowe GG. Atherosclerotic ulcerative disease and associatedaneurysms of the coronary arteries. Am Heart J 1975;90:2:153–158.27. Alfonso F, Macaya C, Goicolea J, Hernandez R, Banuelos C, Iniguez A,Zamorano J, Zarco P. Angiographic changes (Dotter effect) produced by intra-vascular ultrasound imaging before coronary angioplasty. Am Heart J 1994;128:244–251.28. Galis ZS, Sukhova GK, Libby P. Microscopic localization of active proteaseby in situ zymography: detection of matrix metalloproteinase activity in vasculartissue. FASEB J 1995;9:974–980.
CORONARY ARTERY DISEASE/METALLOPROTEINASES AND REMODELING 1359