Regulation of renal ammoniagenesis in metabolic acidosis · dehydrogenase pathway, are located in...
13
Kidney international, Vol. 40 (1991), pp. 961—9 73 NEPHROLOGY FORUM Regulation of renal ammoniagenesis in metabolic acidosis Principal discussant: ANTON C. SCHOOLWERTH Medical College of Virginia, Richmond, Virginia Patient 1. A 22-year-old diabetic male came to the Emergency Room of the Medical College of Virginia Hospitals with an infected toe, polyuria, weight loss, and shortness of breath for several days. Diabetes mellitus had been diagnosed 9 years earlier. The patient had had 3 previous episodes of diabetic ketoacidosis, the most recent 2 years previously. He had recently been managed with 32 Units of NPH and 6 units of regular insulin in the morning, and 12 units of NPH in the evening. Because of a "busy schedule," however, he had not taken his evening insulin for at least 6 days. Approximately 2 weeks prior to presentation, he had noted a blister on his right great toe after wearing a new pair of shoes. Over the past week the toe had become redder and warmer and had exuded a yellow discharge. Although he had monitored his blood sugar levels in the past, he had not done so for more than one month. Despite a good appetite, he had lost 8 pounds over the previous 2 weeks. On physical examination, the patient was a young, thin white male with rapid, deep respirations. His supine blood pressure was 110/70 mm Hg, dropping to 96/60mm Hg on standing. The pulse was 116 beats/mm; respiratory rate, 28/mm; temperature, 38°C; and weight, 65 kg. There were several microaneurysms in the right optic fundus, the neck veins were flat at 30°, and the lungs were clear. Cardiac examination disclosed a grade Il/VI systolic murmur. Mild epigastric tenderness was present, as was a swollen, warm, tender right great toe with purulent discharge. Laboratory studies revealed: plasma sodium, 138 mEq/liter; potas- sium, 5.4 mEq/liter; chloride, 100 mEq/liter; total carbon dioxide, 12 mM/liter; glucose, 450 mg/dl; urea nitrogen, 30 mg/dl; and serum creatinine, 3.1 mg/dl. Serum ketones were present at 1:8 dilution. An arterial blood gas sample disclosed: pH, 7.20; pCO2, 26 mm Hg; p02, Presentation of the Forum is made possible by grants from Pfizer, Incorporated; Sandoz, Incorporated; Marion Merrell Dow incorpo- rated; Merck Sharp & Dohme International; and Amgen Incorporated. © 1991 by the International Society of Nephrology 112 mm Hg; and calculated bicarbonate, 9.9 mEq/liter. Urinalysis revealed pH 5.0, no protein, > 200 mg/dl glucose, and 4+ ketones; microscopic examination disclosed 1—2 white blood cells/high-power field and occasional hyaline and granular casts. The hemoglobin was 13.2 gldl; hematocrit, 40.6%; and white blood cell count, 7500/mm3. A 24-hour urine collection begun 12 hours after admission contained 186 mEq ammonium. The patient was admitted and treated with intravenous sodium chloride, insulin, potassium, antibiotics, and local care to the toe. With correction of the hyperglycemia, extracellular volume depletion, and metabolic acidosis, his clinical condition improved; the ketonemia cleared, and the infected toe gradually healed. A regimen of split-dose NPH and regular insulin was restarted and he received additional diabetic teaching. He was discharged with followup by the Diabetes Clinic. Patient 2. A 25-year-old male prison inmate was brought to the Emergency Room of the Medical College of Virginia Hospitals because of malaise, fatigue, and chest discomfort over several weeks. He was sent to the hospital when laboratory studies at the prison infirmary revealed severe anemia, hyperkalemia, acidosis, and azotemia. He had experienced transient gross hematuria at age 12 and sickle cell anemia was diagnosed at that time. During his childhood he had had only rare episodes of pain, usually involving his shoulders, knees, and abdomen, but he had not required transfusions or hospitalization. Gross hematuria had not recurred and he had had few symptoms over the previous 5 years, with the exception of several episodes of priapism. Four months prior to admission, he developed lateral malleolar ulcers, which were treated with local care and intermittent antibiotic therapy. Following incarceration, he had a positive skin test for tuberculosis; rifampin therapy was initiated. A urinalysis disclosed microhematuria and pyuria, and ciprofloxacin was added to his regimen; he received these medications up to the time of admission. He denied illicit drug use, a history of hypertension, or urinary symptoms, with the exception of nocturia and possible polyuria for several months. On physical examination, the patient was an alert, young black male in no acute distress. His supine blood pressure was 150/70 mm Hg; pulse, 86 beats/mm, without postural change; and weight, 64 kg. The conjunctivae were pale, the lungs were clear, a grade Ill/VI systolic murmur and S4 gallop were present, and there was no edema. A healing malleolar ulcer was present on the right leg. Laboratory studies revealed: plasma sodium, 136 mEq/liter; potas- sium, 6.9 mEq/liter; chloride, 119 mEq/liter; total carbon dioxide, 8 mM/liter; urea nitrogen, 57 mg/dl; serum creatinine, 4.4 mg/dl; calcium, 8.4 mg/dl; and phosphorus, 7.3 mg/dl. The hemoglobin was 3.7 g/dl; hematocrit, 11.5%; and white blood cell count, 12,500 mm3 with 6% eosinophils. Many sickled red blood cells, moderate ovalocytes, How- ell-Jolly bodies, and nucleated red blood cells were present on blood smear. An arterial blood gas evaluation disclosed: pH, 7.23; pCO2, 21 mm Hg; pO2' 99 mm Hg; and calculated bicarbonate, 8 mEq/liter. An electrocardiogram demonstrated sinus bradycardia and symmetrically peaked T-waves. Urinalysis revealed: pH, 5.0; protein, 30 mg/dl; 10—15 white blood cells and 3—6 red blood cells/high-power field. A Hansen's stain of the urinary sediment disclosed rare eosinophils. Measurement of chemistry values on a random sample of urine obtained shortly after admission demonstrated: sodium, 66 mEq/liter; potassium, 10 mEq/ liter; chloride, 53 mEq/liter; and creatinine, 77 mg/dl. Negative studies included Urine culture for routine pathogens and acid-fast bacilli, and Editors JORDAN J. COHEN JOHN T. HARRINOTON NICOLAOS E. MADIAS Managing Editor CHERYL J. ZUSMAN State University of New York at Stony Brook and Tufts University School of Medicine Case presentations
Transcript of Regulation of renal ammoniagenesis in metabolic acidosis · dehydrogenase pathway, are located in...

Kidney international, Vol. 40 (1991), pp. 961—9 73
NEPHROLOGY FORUM
Regulation of renal ammoniagenesis in metabolic acidosis
Principal discussant: ANTON C. SCHOOLWERTH
Medical College of Virginia, Richmond, Virginia
Patient 1. A 22-year-old diabetic male came to the Emergency Roomof the Medical College of Virginia Hospitals with an infected toe,polyuria, weight loss, and shortness of breath for several days.
Diabetes mellitus had been diagnosed 9 years earlier. The patient hadhad 3 previous episodes of diabetic ketoacidosis, the most recent 2years previously. He had recently been managed with 32 Units of NPHand 6 units of regular insulin in the morning, and 12 units of NPH in theevening. Because of a "busy schedule," however, he had not taken hisevening insulin for at least 6 days. Approximately 2 weeks prior topresentation, he had noted a blister on his right great toe after wearinga new pair of shoes. Over the past week the toe had become redder andwarmer and had exuded a yellow discharge. Although he had monitoredhis blood sugar levels in the past, he had not done so for more than onemonth. Despite a good appetite, he had lost 8 pounds over the previous2 weeks.
On physical examination, the patient was a young, thin white malewith rapid, deep respirations. His supine blood pressure was 110/70 mmHg, dropping to 96/60mm Hg on standing. The pulse was 116 beats/mm;respiratory rate, 28/mm; temperature, 38°C; and weight, 65 kg. Therewere several microaneurysms in the right optic fundus, the neck veinswere flat at 30°, and the lungs were clear. Cardiac examination discloseda grade Il/VI systolic murmur. Mild epigastric tenderness was present,as was a swollen, warm, tender right great toe with purulent discharge.
Laboratory studies revealed: plasma sodium, 138 mEq/liter; potas-sium, 5.4 mEq/liter; chloride, 100 mEq/liter; total carbon dioxide, 12mM/liter; glucose, 450 mg/dl; urea nitrogen, 30 mg/dl; and serumcreatinine, 3.1 mg/dl. Serum ketones were present at 1:8 dilution. Anarterial blood gas sample disclosed: pH, 7.20; pCO2, 26 mm Hg; p02,
Presentation of the Forum is made possible by grants from Pfizer,Incorporated; Sandoz, Incorporated; Marion Merrell Dow incorpo-rated; Merck Sharp & Dohme International; and Amgen Incorporated.
© 1991 by the International Society of Nephrology
112 mm Hg; and calculated bicarbonate, 9.9 mEq/liter. Urinalysisrevealed pH 5.0, no protein, > 200 mg/dl glucose, and 4+ ketones;microscopic examination disclosed 1—2 white blood cells/high-powerfield and occasional hyaline and granular casts. The hemoglobin was13.2 gldl; hematocrit, 40.6%; and white blood cell count, 7500/mm3. A24-hour urine collection begun 12 hours after admission contained 186mEq ammonium.
The patient was admitted and treated with intravenous sodiumchloride, insulin, potassium, antibiotics, and local care to the toe. Withcorrection of the hyperglycemia, extracellular volume depletion, andmetabolic acidosis, his clinical condition improved; the ketonemiacleared, and the infected toe gradually healed. A regimen of split-doseNPH and regular insulin was restarted and he received additionaldiabetic teaching. He was discharged with followup by the DiabetesClinic.
Patient 2. A 25-year-old male prison inmate was brought to theEmergency Room of the Medical College of Virginia Hospitals becauseof malaise, fatigue, and chest discomfort over several weeks. He wassent to the hospital when laboratory studies at the prison infirmaryrevealed severe anemia, hyperkalemia, acidosis, and azotemia.
He had experienced transient gross hematuria at age 12 and sickle cellanemia was diagnosed at that time. During his childhood he had hadonly rare episodes of pain, usually involving his shoulders, knees, andabdomen, but he had not required transfusions or hospitalization. Grosshematuria had not recurred and he had had few symptoms over theprevious 5 years, with the exception of several episodes of priapism.Four months prior to admission, he developed lateral malleolar ulcers,which were treated with local care and intermittent antibiotic therapy.Following incarceration, he had a positive skin test for tuberculosis;rifampin therapy was initiated. A urinalysis disclosed microhematuriaand pyuria, and ciprofloxacin was added to his regimen; he receivedthese medications up to the time of admission. He denied illicit druguse, a history of hypertension, or urinary symptoms, with the exceptionof nocturia and possible polyuria for several months.
On physical examination, the patient was an alert, young black malein no acute distress. His supine blood pressure was 150/70 mm Hg;pulse, 86 beats/mm, without postural change; and weight, 64 kg. Theconjunctivae were pale, the lungs were clear, a grade Ill/VI systolicmurmur and S4 gallop were present, and there was no edema. A healingmalleolar ulcer was present on the right leg.
Laboratory studies revealed: plasma sodium, 136 mEq/liter; potas-sium, 6.9 mEq/liter; chloride, 119 mEq/liter; total carbon dioxide, 8mM/liter; urea nitrogen, 57 mg/dl; serum creatinine, 4.4 mg/dl; calcium,8.4 mg/dl; and phosphorus, 7.3 mg/dl. The hemoglobin was 3.7 g/dl;hematocrit, 11.5%; and white blood cell count, 12,500 mm3 with 6%eosinophils. Many sickled red blood cells, moderate ovalocytes, How-ell-Jolly bodies, and nucleated red blood cells were present on bloodsmear. An arterial blood gas evaluation disclosed: pH, 7.23; pCO2, 21mm Hg; pO2' 99 mm Hg; and calculated bicarbonate, 8 mEq/liter. Anelectrocardiogram demonstrated sinus bradycardia and symmetricallypeaked T-waves. Urinalysis revealed: pH, 5.0; protein, 30 mg/dl; 10—15white blood cells and 3—6 red blood cells/high-power field. A Hansen'sstain of the urinary sediment disclosed rare eosinophils. Measurementof chemistry values on a random sample of urine obtained shortly afteradmission demonstrated: sodium, 66 mEq/liter; potassium, 10 mEq/liter; chloride, 53 mEq/liter; and creatinine, 77 mg/dl. Negative studiesincluded Urine culture for routine pathogens and acid-fast bacilli, and
EditorsJORDAN J. COHENJOHN T. HARRINOTONNICOLAOS E. MADIAS
Managing EditorCHERYL J. ZUSMAN
State University of New York at Stony Brookand
Tufts University School of Medicine
Case presentations

962 Nephrology Forum: Regulation of renal ammoniagenesis
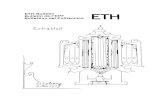
Fig 1. Intramitochondrial pathways for renalglutamine metabolism. Abbreviated termsenclosed in boxes refer to the enzymesglutaminase (PDG), glutamate dehydrogenase(GDH), glutamate oxaloacetate transaminase(GOT), a-ketoglutarate dehydrogenase(aKGDH), and succinate dehydrogenase(SDH). Transporters are denoted by ovals onthe membrane (clockwise beginning at left):the glutamine transporter, dicarboxylatecarrier, the glutamate/aspartate antiporter, andthe glutamate/hydroxyl carrier. + =stimulation; — = inhibition. Dark arrows referto sites activated at acid medium pH.(Modified from Ref. 52).
serum HIV antibody titer. A renal ultrasound disclosed 11 cm kidneyswithout hydronephrosis.
The patient was treated with nebulized albuterol, intravenous glucoseand insulin, sodium bicarbonate, and four units of packed red bloodcells. A protein- and potassium-restricted diet, oral sodium bicarbon-ate, aluminum hydroxide, nifedipine, and clonidine were prescribed.With this regimen, both his clinical status and his laboratory valuesimproved. Nine days after admission, laboratory values were: plasmasodium, 141 mEq/liter; potassium, 5.2 mEq/liter; chloride, Ill mEq/liter; total carbon dioxide, 16 mM/liter; urea nitrogen, 36 mg/dl; andserum creatinine, 3.4 mg/dl. A 24-hour urine collection contained 0.63 gprotein, 1115 mg creatinine, and 34.7 mEq ammonium. Creatinineclearance was 23 mI/mm. Repeated urine sediment examinations dis-closed 3—b white blood cells, 5-.-l0 red blood cells, and occasionalgranular casts/high-power field. The patient declined further diagnosticstudies and was discharged with followup in the Renal Clinic.
Discussion
DR. ANTON C. SCHOOLWERTH (Chairman, Division ofNephrology, Medical College of Virginia Hospitals, and Pro-fessor of Medicine and Physiology, Virginia CommonwealthUniversity, Richmond, Virginia): Despite recent controversy, itis generally accepted that the kidney plays a primary role inmaintaining acid-base homeostasis [1, 2J. The kidney can syn-thesize bicarbonate; this process is closely linked to the metab-olism of glutamine, the primary precursor of ammonium. Bothammonium excretion and the metabolism within the renalcortex of the carbon skeleton of glutamine, in the form ofcr-ketoglutarate (aKG), are necessary for net bicarbonate syn-thesis [1, 3]. The escape of ammonium by renal excretion,rather than its addition to renal venous blood, is critical inpreventing ammonium incorporation into urea by the liver,because ureagenesis, which is a bicarbonate-consuming pro-cess, would counteract bicarbonate synthesis by the kidney [1,3, 4, 5]. The metabolism of the glutamine carbon skeleton,either to glucose or to carbon dioxide and water, is critical,because two hydrogen ions are consumed per one glutamineutilized [1, 3]. A great deal of work has been directed atunderstanding the regulation of renal ammoniagenesis becauseof the kidney's remarkable ability to increase ammonium syn-thesis substantially in response to metabolic acidosis. Studies in
this area have focused on the relationship between the biochem-istry of glutamine metabolism and the transport of metabolitesinto and out of renal cortical mitochondria, where most of thekey enzymes related to glutamine metabolism are located [6, 7].
In this presentation I will emphasize the current status of ourunderstanding of the stimulation of ammonium formation inresponse to metabolic acidosis. In addition, I will review recentdata suggesting that the increased rate of ammonium synthesisper nephron might contribute to nephron destruction in exper-imental renal disease. Finally, I will mention briefly recentobservations suggesting that altered animonium synthesis andhandling underlie the pathogenesis of distal renal tubular aci-dosis. The relative contributions of the kidney and liver to themaintenance of acid-base homeostasis have been addressedelsewhere [4, 8—12], and I will not discuss these issues here.
The problems that remain to be resolved include the follow-ing: (1) the details of the pathways of renal glutamine metabo-lism; (2) the specific site(s) at which augmented rates of renalammoniagensis are regulated in acute and chronic metabolicacidosis; and (3) factors that modulate ammonium synthesis.Although several pathways exist by which glutamine might bemetabolized to yield ammonium in renal cortex, the pathwayinvolving the enzymes glutaminase and glutamate dehydroge-nase is generally accepted as the predominant one [1, 13].Glutamine is deamidated by phosphate-dependent glutaminase(PDG) to yield ammonium and glutamate. Oxidative deamina-tion of the resulting glutamate by glutamate dehydrogenase(GDH) then yields ammonium and a-ketoglutarate. These twoenzymes, which together comprise the glutaminase/glutamatedehydrogenase pathway, are located in the mitochondrial ma-trix space (Fig, 1) and are found in distal and proximal convo-luted tubules (PCT) in the rat [14, 15]. However, in chronicmetabolic acidosis, both enzyme activities increase substan-tially (5- to 20-fold) only in the S1 and S2 segments of PCT [14,15]. These findings correlate well with measurements of ammo-nium production by microdissected nephron segments fromcontrol and acidotic rats incubated in vitro with glutamine [16,17].

Nephrology Forum: Regulation of renal ammoniagenesis 963
Other pathways of glutamine metabolism, studied most ex-tensively in the rat, do not appear to have a significant physio-logic role in ammoniagenesis. For example, y-glutamyl trans-peptidase, although capable of forming ammonium fromglutamine, is unlikely to be important. Located in the brush-border membrane of the S3 segment of the PCT, this enzymehas its active site exposed to the luminal surface [18]. Glu-tamine is removed almost completely from glomerular filtrate inthe early PCT segments (S1 and S2), however, so no substrate isavailable (to the enzyme) for ammonium formation unlessglutamine is secreted into the lumen in this or more proximalPCT segments. Such secretion seems unlikely. Additional path-ways, including the cytosolic glutaminase II pathway and thepurine nucleotide cycle, probably do not contribute substan-tially to renal ammonium formation either [1, 2, 19—211.
Some issues with regard to pathways of ammonium formationremain unresolved. For example, it has not been demonstratedconclusively that the rat kidney extracts glutamine under phys-iologic conditions [22, 23]. Thus, although glutamine extractionincreases markedly in metabolic acidosis [22, 23], the precursorfor ammonium formation under basal conditions remains to beclarified. The source of increased synthesis of ammonium byhuman kidney in acute metabolic acidosis also has not beenidentified. Tizianello and coworkers found no change in renalglutamine extraction under these conditions and raised the ques-tion of whether other sources of ammonium are significant [24].
More controversial than the arguments regarding the path-way of ammonium formation is the site of regulation of glu-tamine metabolism both in acute and chronic metabolic acido-sis. I believe, however, that arguments regarding this issue aremore apparent than real. If one accepts that regulation is likelyto be different in acute, as opposed to chronic, acidosis, thatsignificant species differences exist, and that numerous poten-tial sites of control are present, there actually might be consid-erable agreement in this area. Although many investigatorshave advanced hypotheses focusing on one specific site ofregulation, it is probable, as Pitts suggested, that several sitesact in concert to control the accelerated rate of glutaminemetabolism in metabolic acidosis [25]. I believe that a lack ofappreciation of species differences and a tendency to extrapo-late results from one species to another have confounded a fullunderstanding of the regulation of renal ammoniagenesis. Atpresent, it seems likely that several control sites exist and thatthe relative importance of these control sites varies in differentspecies, as I will discuss later.
Finally, the mechanisms by which several factors, includingions and hormones, modulate renal ammonium productionrequire clarification, as reviewed by Tannen and Sahai [13].Later I will discuss some of these factors, which include potas-sium, calcium, cyclic nucleotides, angiotensin II, catecholamines,parathyroid hormone, insulin, and growth hormone.
Acute metabolic acidosis: In discussing metabolic acidosis(both acute and chronic), I will separate my comments on dataobtained in the rat from those obtained in the dog, becausesubstantial species differences have been demonstrated. In therat, an acute acid load results in marked changes in renalcortical metabolite levels [26, 27]. The most consistent of thesechanges is a decrease in aKG content of as much as 50% [261.Subsequent experiments, based on findings in other tissues [28],have demonstrated that increased hydrogen ion activity acti-
yates renal cortical a-ketoglutarate dehydrogenase (aKGDH)[29—31]. Lowry and Ross first showed that increased hydrogenion activity decreases the Km of the enzyme for aKG [29].These findings, subsequently confirmed in our laboratory [32,33], explain the observation of increased aKG oxidation andcalculated flux through SKGDH by intact renal cortical mito-chondria at acid pH [30, 31]. The result of an increase inhydrogen ion activity on aKGDH is a decrease in mitochondrialmatrix aKG content with a consequent increase in glutamatedeamination and ammonium formation by GDH [31, 34]. De-creased matrix aKG can accelerate glutamate deaminationeither by decreasing the reverse reaction (that is, aKG amina-tion) of GDH or by relieving competitive inhibition by aKG onglutamate deamination [32]. Indeed, in-vitro studies indicatethat accelerated GDH flux is the first event leading to increasedammonium synthesis in the presence of acidification of themedium [31, 34]. Thus, with the exception of data recentlyreported by Bogusky and Dietrich [35], the results from severallaboratories indicate that acute acidosis in the rat acceleratesflux through aKGDH with a resultant increase in ammoniumformation by the GDH reaction (Fig. 1) [20, 30, 31]. Thesefindings imply that glutamate deamination precedes increasedflux through PDG in acute acidosis, as suggested 20 years agoby Preuss and Weiss [36]. However, Preuss postulated thatGDH flux was increased in acidosis by a more oxidized mito-chondrial redox state [37], for which no direct evidence isavailable. Although the precise timing of subsequent PDGactivation remains to be elucidated, it is likely that withcontinued increase in GDH flux, matrix glutamate levels de-crease. Glutamate is a well-recognized end-product inhibitor ofrenal PDG [38]; this change therefore might account for PDGactivation via an allosteric effect.
These data suggest that an early event in acute acidosis isactivation of aKGDH consequent to an increase in hydrogenion activity. Because aKGDH is a mitochondrial enzyme, itshould respond in situ to altered hydrogen ion activity withinthe matrix space. The significance of the findings with thesolubilized enzyme and intact mitochondria [29, 31, 33] couldnot be interpreted until further data were available that wouldallow one to estimate the change in mitochrondrial matrix pH(PHm) in intact PCT in response to altered extracellular fluid(ECF) pH. As predicted by Mitchell's chemiosmotic hypothesis[39], the mitochondrial matrix space is likely alkaline withrespect to the extramitochondrial medium; the latter shouldsimulate the cytosolic space. This prediction was confirmedexperimentally in isolated mitochondria from several tissues [7,8, 40] by the calculation of steady-state PHm from the distribu-tion of the labeled organic anion 5,5-dimethyloxazolidine-2,4-dione (DM0). This method, suitable for estimating steady-statePHm values, assumes that: (1) the un-ionized DM0 speciesreadily permeates the inner mitochondrial membrane, and (2)the distribution of the anionic species is determined by theprevailing pH in the intra- and extramitochondrial spaces [41].Using this DM0 method, we studied rat kidneys in bicarbonate-free media and found pH to be 7.9 at medium pH 7.3; the pHgradient (pH) was approximately 0.6 pH units [31]. An obser-vation first made by Simpson and Hager and not yet explainedis that the pH is approximately 0.2 pH units lower whendetermined in bicarbonate-buffered media [42, 43]. Neverthe-less, regardless of the buffer sytem utilized, these in-vitro

964 Nephrology Forum: Regulation of renal ammoniagenesis
PHea pH1 PHm APHm
Non-HC03 (7)b 7.03 O.01'7.41 0.017.70 0.01
6.89 0.037.08 0.027.30 0.03
7.65 0.037.96 0.088.37 0.03
0.78 0.090.88 0.091.15 0,03
HC03 (12) 7.04 0.017.44 0.017.73 0.01
6.91 0.027.10 0.037.28 0,02
7.51 0.087.78 0.068.08 0.08
0.62 0.030.68 0.080.79 0.05
studies with isolated mitochondria indicate that the matrixspace is more alkaline than the medium, which suggests thatP1m is more alkaline than the cytosolic pH in situ. Thesestudies also indicated that medium acidification in vitro causedPHm to decrease only slightly with a resultant increase in thepH [31, 43].
To obtain additional data regarding the change in PHm thatoccurs in situ in response to a decrease in ECF pH, we adapteda technique used in isolated hepatocytes [441 to estimatesimultaneously changes in cytosolic and mitochondrial matrixpH in suspensions of intact rat proximal tubules as a function ofaltered pH of the medium [4511. These experiments were per-formed with the fluorescent probe 2' ,7'-biscarboxyethyl-5(6)carboxyfluorescein (BCECF) to estimate intracellular pH[461. Using BCECF in combination with radiolabeled DM0,which distributes across both the plasma and mitochondrialmembranes, one can calculate matrix pH if the percentage ofPCT occupied by the matrix space is known; the latter wasdetermined by us [45] and others [47] to be approximately 20%.Using this technique, we estimated steady-state cytosolic pH(pH1) and PHm at different ECF pH (pHe) values [45]. The data,obtained with bicarbonate-buffered media and summarized inTable 1 and Figure 2, indicate a linear relationship between PHeand pH1 as well as between pH1 and PHm. We observed nodifference in pH1 in the absence of bicarbonate as buffer;however, as in isolated mitochondria, we found pHm to beapproximately 0.2 pH units lower in the presence of bicarbon-ate as compared with its absence [45]. These findings indicatethat the acceleration in aKGDH flux that occurs in intactproximal nephron segments in acute metabolic acidosis mightsimply reflect the ability of these segments to respond to adecrease in PTe and thus cause a decrease in PHm. However,the decreases in pHm, although related linearly to those in thepH and pH1, are relatively small. It remains uncertain whetherthis change in PHm can fully explain the activation of aKGDHor whether the concentration of other ions, such as Ca2, whichis also known to activate aKGDH [29, 48—SO], changes in thematrix space in acute acidosis and contributes to this activation.
The effects of a change in pH,, on pH1 and P11m in the rat arequite different from those in the dog [51, 52], as shown in Figure3. At all levels of pH,,, we found that pH, was higher in proximal
I I I I I6.6 6.8 7.0 7.2 7.4 7.6
pH,
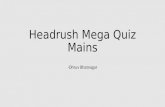
Fig. 2. Relationship of cytosolic pH (pH,) and the medium pH (pJ1)(top panel) and of mitochondrial matrix pH (pH,,,) and pH1 in ratpro..mal tubules. Symbols indicate that tubules were incubated innonbicarbonate (non HCO31- or bicarbonate (HCO3 i-buffered media.(Modified from Ref. 45).
nephron segments obtained from dog than in those obtainedfrom rat [51, 52]. Moreover, in contrast to the rat, PHm appearsto be well buffered in dog and remained unchanged (PHmapproximately 7.9) over the PF1e range 7.0—7.7. Thus, nodecrease in pHm, which could account for activation ofaKGDH, apparently occurs with acidification of PH,, in the dog.Although it is not entirely certain that ammonium production isincreased in acute metabolic acidosis in the dog in vivo [26, 53],this uncertainty might relate to the decrease in GFR and renalblood flow accompanying an acute intravenous infusion ofhydrochloric acid. These hemodynamic changes might lowerrenal glutamine delivery and offset any increase in glutaminemetabolism such that calculated total-kidney ammonium forma-tion is similar in acute metabolic acidosis compared with thecontrol situation [53]. Other data, obtained in in-vitro studies inour laboratory, do suggest a pH effect on glutamine metabolismin canine renal tubules and indicate substantial differences inmitochondrial response to pH changes in the dog compared
Table 1. Effect of medium pH changes on cytosolic andmitochondrial pH and the pH gradient across the inner
mitochondrial membrane
a Cytosolic pH (pH,) and mitochondrial pH (pH,,,) were determined atdifferent medium pH (PHe) values in intact rat renal cortical tubules.
b Number of experiments is shown in parentheses. Experiments wereperformed with nonbicarbonate (non-HCO3i- or bicarbonate(HC03)-buffered media. The non-HC03 buffer used was HEPES.
C The results (modified from Ref. 45) are expressed as mean 5EM.
7.6 - • nonHCO3
0 HCO
6.8 07!2747!67!8pH
0.
EI0.
8.4
8.2
8.0
7.8 -
7.6 -
7.4 -
• nonHCO3 •o HCoç
.

Nephrology Forum: Regulation of renal ammoniagenesis 965
a
• Dog
.2tI7.2
7.0.6.8- I
7.0 7.2 7.4 7.6 7.8pH
8.2 -• Dogo Rat
8.0 -
7.8-a
7.6
7.4
6.8 7.0 7.2 7.4 7.6pH
PHe
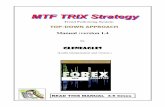
Fig. 3. Effect of changes in pH on pH1, pH,,,, and the pH gradientacross the mitochondrial membrane (zpH) in proximal tubules from ratand dog renal cortex. (Modified from Ref. 52).
with the rat [51, 52]. Although tubules from canine renal cortexrespond to acidification of the medium with an increase inammonium synthesis from glutamine, this increase appears to
0NH4 PDG GDH
Fig. 4. Ammonium (NH4) production by proximal tubules (top panel)and isolated mitochondria (bottom panel) from control and chronicallyacidotic dogs. In the top panel, the effect of medium pH (pH) wasevaluated. In the bottom panel, the contribution of flux throughglutaminase (PDG) and glutamate dehydrogenase (GDH) to NH4formation is shown. k, significantly greater than control, P < .05.Substrate = 1 mM glutamine. (Modified from Ref. 51.)
be almost entirely due to augmented flux of PDG, not GDH(Fig. 4) [51, 52].
An abundance of additional data indicates the complexitysurrounding glutamine and glutamate metabolism in rat renalcortex. These data have emphasized the close relationshipbetween transport of metabolites across the inner mitochondrialmembrane and flux through enzymes located within the matrixspace [8, 54]. As Figure 2 shows, several transporters regulateglutamate transport across the inner mitochondrial membrane.
7.6
E0C',C)E0EC
20 —
15 —
C)E
10 —
E0EC
5—
7.0 7.4 7.7
pH,,
1.0
0.8
Control
Acidosis
*
I
0.4
0.2
7.0 7.2 7.4 7.6 7.8

966 Nephrology Forum: Regulation of renal ammoniagenesis
These transporters, also found in mitochondria from extrarenaltissues, include the so-called glutamate hydroxyl transporterand the glutamate/aspartate antiporter [7, 54]. I would like toreview briefly the characteristics of these transporters. Theelectroneutral glutamate hydroxyl carrier is believed to trans-port glutamate with H; glutamate entering mitochondria onthis carrier is functionally linked to metabolism by GDH. Thistransporter is relatively inactive in kidney with a max (3nmol . min . mg protein') one order of magnitude lowerthan in liver [55, 56]. Moreover, in contrast to liver, the activityof this transporter is not stimulated when the medium isacidified [55, 56]. In fact, data indicate that an insufficientamount of glutamate enters renal mitochondria on the glutamatehydroxyl carrier to result in substantial glutamate deaminationby GDH [55, 57, 58]. Only glutamate formed from glutaminewithin the matrix space can be deaminated to a significantdegree under physiologic conditions [58]. Although glutamateuptake on this carrier is very slow in the kidney, the glutamatehydroxyl transporter might exert some effect on matrix gluta-mate content and hence GDH flux, since efflux of glutamatefrom the matrix space on this carrier is pH sensitive [59].Studies from our laboratory have demonstrated that effiux ofglutamate on this transporter, which obeys first-order kineticswith respect to glutamate concentration, is decreased in anacidic medium [591. The decrease in glutamate effiux underthese conditions could contribute to accelerated GDH flux; theresultant increase in matrix glutamate concentration (coupledwith a decrease in cKG) would increase the matrix ratio ofglutamate:aKG and drive the GDH reaction in the direction ofincreased glutamate deamination [31].
The other glutamate transporter is an electrogenic glutamate!aspartate countertransporter [60]. Glutamate, entering mito-chondria in exchange for aspartate, is transaminated by mito-chondrial aspartate aminotrnsferase (GOT) in a reaction thatproduces no ammonium. But because aKG is one of theproducts of the GOT reaction, this carrier can influence ammo-nium formation. Increased glutamate/aspartate carrier activitywith the resultant increased flux through GOT can reduceammonium formation consequent to aKG inhibition of GDHflux. Support for this concept comes from studies utilizingtransaminase inhibitors. For example, in the presence of ami-nooxyacetate, an inhibitor of GOT, ammonium formation byGDH increases in isolated rat mitochondria [61]. This effect ofaminooxyacetate is due to a decrease in aKG formation [61].Although the response of the glutamate!aspartate carrier toacute acidosis in situ is not known, its activity is likely reducedand, together with a stimulation of aKGDH flux, this transportsystem probably contributes to the observed stimulation inGDH flux.
Adam and Simpson postulated a major role for the transportof glutamine across the inner mitochondrial membrane as arate-controlling step in glutamine metabolism in acidosis [62].They incubated rat and dog renal cortical mitochondria withradiolabeled glutamine in the presence of rotenone, whichinhibited glutamate metabolism, and demonstrated increaseduptake of glutamine and its conversion to glutamate when thepH of the medium was decreased from 7.4 to 7.0 [62—64].Although rotenone prevents glutamate metabolism, it does notinhibit PDG. Thus, these studies [62, 631 and those by others[65—67] could not unequivocally distinguish activation of glu-
tamine transport from its deamidation by PDG. Recently,Sastrasinh and Sastrasinh attempted to clarify this issue bystudying the transport of labeled glutamine in submitochondrialparticles (SMP), which are largely free of contaminating PDG[68, 69]. Using SMP, these investigators demonstrated a higherrate of glutamine uptake at medium pH 7.0 compared with 7.4;these findings are compatible with an activation of the glu-tamine transporter in acute acidosis. Sastrasinh and Sastrasinhsuggested that a decrease in the pH of the medium reduced theKm of the transporter for glutamine [69]. Although these dataindicate a role for accelerated glutamine transport across theinner membrane of dog and rat renal mitochondria in acuteacidosis, further studies are needed to clarify and fully charac-terize the kinetics of this transporter. The data from Simpsonand colleagues suggest that the glutamine transporter is partic-ularly important in the augmented rate of ammoniagenesis inchronic metabolic acidosis [7, 62, 63, see later]. No studies areavailable to assess this carrier in human kidneys.
One additional site of potential regulation is the succinatedehydrogenase (SDH) step (see Fig. 1). As described initially inhepatic [701 and more recently in renal mitochondria [71], theactivity of this enzyme is inhibited competitively by bicarbon-ate ions with a K3 of approximately 12 mM. If this effect ispresent in situ, a decrease in bicarbonate content in the matrixspace could activate SDH and complement the effect of de-creased pH on aKGDH, thereby resulting in an increase inammonium production by GDH. Improved understanding ofthis regulatory site will require data on the prevailing range ofmatrix bicarbonate concentrations under both control and aci-dotic conditions. However, this bicarbonate-sensitive site ofregulation could explain the observation made by Rodriguez-Nichols et al that ammonium synthesis is not increased inchronic respiratory acidosis [72]. Ammonium production andexcretion are increased acutely in respiratory acidosis, presum-ably in response to a decrease in intracellular pH. With persis-tence of hypercapnea, this leads to an increase in bicarbonatecontent in extracellular fluid and the matrix space in renalmitochondria. The increase in matrix bicarbonate, by inhibitingsDH, could in turn prevent a sustained increase in glutaminemetabolism (brought about by an acid pH) from occurring.
In summary, data indicate that in the rat, ammonium forma-tion is accelerated in acute acidosis primarily by an increase influx through GDH, consequent to a decrease in matrix aKGcontent; glutamine transport also might be increased underthese conditions. In the dog, acidification of P1e leads to amodest increase in ammonium synthesis, at least in vitro, dueprimarily to an increase in glutamine transport and deamidationby PDG. Further studies are needed, particularly in the dog, tounravel the factors that contribute to the increased rate ofglutamine metabolism in acute acidosis. In addition, furtherinformation is needed to characterize the mechanisms of in-creased ammonium production in acute acidosis in humankidneys.
Chronic metabolic acidosis. That increase in ammoniumexcretion observed in chronic metabolic acidosis is associatedwith activation of PDG and GDH in rat renal cortex has beenrecognized for almost 40 years [731. Since then, we havelearned that the increase in enzyme activity occurs exclusivelyin the early segments of PCT [14, 15]. Studies both with isolatedrat renal mitochondria [57, 74] and isolated tubules [75] have

Nephrology Forum: Regulation of renal ammoniagenesis 967
indicated that augmented flux through both PDG and GDHaccounts for the increased ammonium synthesized in chronicmetabolic acidosis. The mechanisms and precise stimulus ac-counting for the augmented flux rates have not been determinedunequivocally. Evidence supports an increase in glutaminetransport in chronic metabolic acidosis [62—64] secondary to anincrease in ''max of the transporter. An increase in Vmaxsuggests an increase in the number of transport sites, in turndue to an increase in synthesis, reduction in turnover, orunmasking of carrier molecules on the inner mitochondrialmembrane [7]. However, recent data using SMP from acidoticrats demonstrated a slight decrease from control in Km forglutamine but no increase from control in Vmax of glutaminetransport [68]; thus, the mechanism of an increased rate ofglutamine transport in metabolic acidosis remains to be clari-fied. Since an increase in GDH flux accounts for as much as50% of the rise in ammonium formation [74], other factors suchas accelerated aKGDH flux could be critical in chronic acido-sis, as in acute metabolic acidosis [29—31].
In the rat, renal glucose production is also accelerated inresponse to metabolic acidosis. Goodman et al suggested 25years ago that stimulation of gluconeogenesis might regulateglutamine metabolism [76]. They proposed that the key gluco-neogenic enzyme, phosphoenolpyruvate carboxykinase(PEPCK), was induced early in acidosis and led to an increasein glucose formation; as a result of the increased rate of glucosesynthesis, renal cortical glutamate content decreased withsubsequent activation of PDG [77]. Although more recent datahave demonstrated that an increase in glucose synthesis is nota necessary step for augmented ammoniagenesis, gene expres-sion of PEPCK as well as PDG have been studied in response toacidification [78—83]. Curthoys and associates have demon-strated an increase in messenger RNA for PDG and PEPCK,changes that precede the increase in assayable enzyme activityin rat PCT and in cultured LLC-PK1 F cells [78—80, 83].Because the message for both enzymes increased in response toacidification of the medium, the data suggest that the inductionof mRNAs for these enzymes might be mediated by a commonsignal transduction mechanism [80]. The data also indicateseparate regulation of gene expression of both enzymes by Wand bicarbonate. Further studies are necessary to characterizethe mechanisms by which acidosis affects gene expression in ratrenal cortex.
One of the major differences between rat and dog is thatchronic metabolic acidosis in the dog accelerates the rate ofrenal ammonium excretion without an evident increase in PDGor GDH enzyme activities [841. These observations, made morethan 30 years ago, suggest that these enzymes are not inducedin the canine kidney, and that the stimulation of ammoniagene-sis cannot be ascribed to an increased amount of PDG andGDH. Indeed, Halperin and coworkers have suggested that anexcess of both enzymes is present in renal cortex in the rat andthe dog [2]; one can presume that factors other than the amountof enzyme are of greater importance in leading to an augmentedrate of glutamine metabolism in acidosis. As far as I am aware,no studies have been published evaluating the effect of meta-bolic acidosis on the message for PDG and GDH and themechanism(s) regulating ammonium synthesis in dog renalcortex. This evaluation is important because the dog modelmost closely approximates the systems likely to exist in human
kidney [85]. The data on canine renal ammoniagenesis havebeen reviewed by Vinay et al [53], who have performed most ofthe critical experiments. Their data, which involve studiesperformed in vivo, suggest activation in metabolic acidosis ofthe mitochondrial glutaminase/glutamate dehydrogenase path-way [53]. However, recent in-vitro studies with isolated mito-chondria from acidotic canine renal cortex have demonstratedthat an increase in PDG, but not GDH, flux accounts for theincreased ammonium production [51, 52].
One additional difference has been noted between dog andrat. The rat proximal tubule, but not that of the dog or thehuman, contains the enzyme glutamine synthetase (GS), whichcatalyzes the formation of glutamine from glutamate and am-monium [85]. The function of this enzyme in the rodent kidneyis not clear, although it possibly is more critical for the smallerspecies if substantial glutamine losses are to be prevented,especially under physiologic conditions.
Although Tannen and Sahai have addressed other modulatingfactors of renal ammoniagenesis [13], 1 would like to mentionbriefly some additional points. Recently, interest has beenrekindled in evaluating the role of Ca2 in affecting both renalgluconeogenesis and ammoniagenesis, particularly with thedemonstration by Denton and McCormack that submicromolarconcentrations of Ca2 stimulate the activity of aKGDH,pyruvate dehydrogenase, and isocitrate dehydrogenase [50, 86].Estimates indicate that changes in mitochondrial free Ca2 arelikely to be in a range that could regulate the activity of theseenzymes in situ [87, 88]. It will be of interest to determinematrix-free Ca2 alterations as a function of acid-base distur-bances; for example, in metabolic acidosis, an increase couldoccur. These studies might shed light on the different behaviorof rat and dog renal cortex in response to acute acidosis. Inaddition, studies are needed to determine whether the hormonalstimulation of gluconeogenesis and ammoniagenesis is medi-ated by increases in cytosolic and mitochondrial free Ca2tReports from several laboratories have indicated that angioten-sin II, a-adrenergic agonists, parathyroid hormone, and dopa-mine stimulate both of these metabolic processes, whereasinsulin stimulates ammonium but inhibits glucose production[89—94]. Furthermore, we have noted a relationship between thehormonal stimulation of ammoniagenesis and the activity of theluminal Na/H exchanger in PCT [94]. Specifically, stimula-tion of metabolism by hormones that activate the Na/Hexchanger (angiotensin II, a-agonists) may do so by a differentmechanism than hormones that inhibit the exchanger (parathy-roid hormone, dopamine) [95]. Moreover, in the case of theformer agents, stimulation of Na/H exchange might benecessary to achieve maximal metabolic stimulation, as thestimulation of ammoniagenesis by angiotensin II and a1-ago-nists, but not parathyroid hormone and dopamine, is preventedby the specific inhibitor of luminal Na/H exchange, ethyliso-propyl amiloride [95]. Further work defining this interactionalso might provide more information about the subcellularmessenger systems that modulate hormonal effects of ammo-niagenesis.
The classic studies by Bricker and associates demonstratedan adaptive increase in ammonium excretion per nephron in theremnant canine kidney [96]. This report prompted Simpson tosuggest that similar changes are likely to occur in humans [97].These findings were extended to studies in the remnant rat

968 NephrologyForum: Regulation of renal am,noniagenesis
kidney [98, 99], which also provided evidence for increasedin-vitro ammonium production per gram and per cell in theremaining tissue [98]. More recently, Harris et al have sug-gested that hypermetabolism occurs in the remnant rat kidney[100]. This adaptive response may prevent severe metabolicacidosis from occurring early in the course of progressive renaldisease, even though progressive reduction in renal mass ulti-mately limits ammonium production and results in the well-recognized metabolic acidosis of chronic renal failure. Nath andcolleagues have suggested that the adaptive increase in ammo-niagenesis per nephron could have adverse consequences [101],In an elegant series of experiments, they demonstrated thatammonia can activate the alternate complement pathway byamidation and that this activation could lead to tissue injury inthe form of tubulointerstitial disease [101]. In these studies,they demonstrated that suppressing ammonium formation bysodium bicarbonate feeding reduced the degree of tubulo-interstitial damage in rats following subtotal nephrectomy. Thesame group proposed that hypermetabolism is deleterious be-cause of the formation of reactive oxygen species [102]. Al-though these are attractive hypotheses, further work is neces-sary to confirm their relevance and validity to the situation invivo. For example, Buerkert et al have estimated that theconcentration of ammonium in renal cortex of the remnant ratkidney is twofold higher than in controls [103]: whether theselevels are sufficient to explain an activation of the complementpathway in renal tissue in vivo has not been confirmed. Theissue is made even more interesting by the recent observationby Golchini and coworkers that ammonium chloride induceshypertrophy in cultured proximal tubule cells [104].
Do altered proximal tubular glutamine metabolism and am-monium formation play a role in the pathogenesis of distal renaltubular acidosis? Recently, two new hypotheses have beendeveloped to explain this condition [105, 106]. Donnelly andassociates have suggested that distal renal tubular acidosis isthe consequence of a decreased pH, in the PCT [105]. Stimu-lated ammonium formation secondary to acidification of theproximal tubular cell may lead to toxicity in the medulla due tohigh ammonia content, as well as to nephrolithiasis and neph-rocalcinosis from the decreased urinary citrate excretion [106].Kurtz et al have postulated that some forms of distal renaltubular acidosis can occur secondary to altered permeability toammonia and/or NH4 in the collecting duct [104]. Theyproposed that ammonium enters the renal venous circulation,rather than the tubular fluid and urine; as a result of thesubsequent incorporation of this ammonium into urea by theliver, the consumption of bicarbonate would be increased [105].Further work is necessary to test the validity of these hypoth-eses. However, both theses emphasize the point made recentlyby Halperin et al that a reduction in urine ammonium excretionis the key feature of distal renal tubular acidosis [107].
In this review I have attempted to summarize our currentunderstanding of the renal regulation of ammonium formation.Although considerable progress has been made over the last 40years, key issues remain unresolved and require further inves-tigation. This challenge is complicated by substantial speciesdifferences and by the likelihood that controlling factors aredifferent in acute, as opposed to chronic, acidosis. The appli-cation of contemporary techniques of molecular biology to this
problem should provide important new insights into the effectsof acidosis on the genetic regulation of ammonium metabolism.
Questions and answers
Da. NTCOLAOS E. MADIAS (Chief, Division of Nephrology,New England Medical Center, Boston, Massachusetts): I'd liketo ask you to briefly address the issue of potassium's effect onammonium generation and also the possibility that increasedammonium production might have a role in the pathogenesis ofthe nephropathy of potassium depletion.
DR. SCHOOLWERTH: Potassium depletion has been clearlyshown to stimulate renal ammonium production [108]. Althoughthe signal responsible for stimulating and maintaining increasedammonium generation has not been elucidated, the suggestionthat intracellular acidosis in the kidney occurs as a consequenceof potassium depletion is supported by some, but not all, data[109, 110]. Regardless of the mechanism, several clinical con-sequences have been postulated. For example, renal ammo-nium production, with diversion into the systemic circulation,might contribute to the development of hepatic coma in patientswith liver disease and potassium depletion [111]. RecentlyTolins et al have suggested that the pathogenesis of hypokale-mic nephropathy involves activation of the alternate comple-ment pathway by increased renal cortical ammonia levels withsubsequent development of tubulointerstitial disease [112].
DR. JOHN T. HARRINGTON (Chief of Medicine, Newton-Wellesley Hospital, Newton, Massachusetts): You referred tostudies on the kinetics of alpha ketoglutarate at specific pHs of7.4 and pH 6.8, I believe. Have you or others done studies atother pHs to determine whether the relationship is a stepfunction or a graded function?
DR. SCHOOLWERTH: Lowry and Ross studied the kinetics ofrenal aKGDH over the range 7.7 to 6.8 [29]. They demonstrateda reduction in the Km of the enzyme for aKG with each 0.3 pHunit decrease, suggesting that the relationship is a graded one.This finding is compatible with our observations on the effect ofpH on cKG oxidation by intact renal mitochondria.
DR. HARRTNGTON: My second question is more complicated,but it is based on my being a believer in the 'non-homeostatic"control of systemic pH [113, 114]. More than 20 years ago,studies from the Renal Laboratory here at the New EnglandMedical Center showed that the administration of ADH andwater to dogs in a steady state of chronic HCI acidosis raisedserum bicarbonate to normal and increased renal net acidexcretion sufficiently to account for that rise [115]. My questionis: Are there enzymatic studies comparable to yours in the kindof experimental setting I described?
DR. SCHOOLWERTH: Do you mean when water excretion wasdecreased?
DR. HARRINCTON: In effect, the animals developed SIADH.Later studies disclosed increased aldosterone excretion in thepresence of volume expansion [1161.
DR. SCHOOLWERTH: I am not aware of any enzymatic studiesthat would explain these observations. However, the experi-mental maneuvers performed in the studies you described werecomplex. No specific data on ammonium production and excre-tion were given, although it is likely that ammonium productionwas stimulated. It should be noted that following vasopressinadministration, the dogs became hypokalemic [115]. Thus thehypokalemia, resulting from vasopressin administration, could

Nephrology Forum: Regulation of renal ammoniagenesis 969
have increased ammonium production beyond that occurring inthe stable state of metabolic acidosis. Despite volume expan-sion and hypokalemia, aldosterone secretion and excretionwere increased, as you pointed out; this increase might contrib-ute to an increased diversion of ammonium into the urine [1161.Recently, Halperin and Chen, using a different protocol, dem-onstrated that hypotonic volume expansion in chronically aci-dotic dogs markedly increased urine flow rate; this increase alsocould contribute to the increased diversion of generated ammo-nium into the urine [1171. In the dogs with a serum sodiumconcentration of 126 mmol/liter, but without hypokalemia, therate of renal ammonium generation was not increased duringhyponatremia. Thus, I would speculate that the major factorproducing increased net acid excretion in the original studies byLowance et a! was hypokalemia, and that the increased urineflow rate and aldosterone secretion resulted in an increased rateof ammonium production and excretion.
DR. MADIAS: The study that Dr. Harrington referred toshowed that administration of vasopressin during restriction ofwater intake (thus preventing fluid retention) did not increaserenal acid excretion or plasma bicarbonate concentration. Hy-potonic volume expansion was required for the renal correctionof the metabolic acidosis.
DR. SCHOOLWERTH: Vasopressin administration in acidoticdogs that are water restricted resulted in little further change inserum potassium concentration [115]. In addition, althoughthese data were not provided, it is likely that urine flow rate wasless than that in the animals allowed unrestricted water intake.Finally, aldosterone secretion did not increase with administra-tion of vasopressin during water restriction [1161. The mecha-nism for increased aldosterone secretion remains obscure.
DR. ANDREW S. LEVEY (Division of Nephrology, New En-gland Medical Center): One might speculate that the increasedGFR and renal blood flow associated with water retentionincreases glutamine delivery to the kidney.
DR. SCHOOLWERTFJ: Was GFR measured?DR. MADIAS: No, but you can assume that GFR was in-
creased under these circumstances.DR. SCHOOLWERTH: I agree. Lemieux and associates clearly
demonstrated in the early 1970s that ammonium excretionparallels GFR and renal blood flow in acidotic dogs [118].
DR. MADIAs: I should like to counter your statement thatrespiratory acidosis does not stimulate renal ammoniagenesis.At least in the dog, Gougoux and colleagues have shown that inthe presence of stability of renal hemodynamics, renal ammonia-genesis adapts promptly and markedly in response to hypercap-nia. Indeed, under such circumstances, renal ammonia productionwas comparable to that observed in dogs with chronic metabolicacidosis [119]. Moreover, studies from our laboratory have shownthat during the maintenance phase of respiratory acidosis in thedog, urinary NH4 excretion remains significantly elevated ascompared with the baseline; however, net acid excretion does notdiffer from control because of accompanying bicarbonaturia and adecrease in titratable acidity [120].
DR. SCHOOLWERTH: Did you measure ammonium productionor just excretion?
DR. MAmAS: Ammonium production was measured duringthe studies of acute hypercapnia by Gougoux and colleagues[119]. In our studies of chronic hypercapnia, only urinaryammonium excretion was measured [120]. However, the ele-
vated ammonium excretion during the maintenance phase ofchronic hypercapnia was accompanied by an increased urinepH as compared with baseline [120].
DR. SCHOOLWERTH: There is no question that ammoniumproduction and excretion increase in acute respiratory acidosis.The increased glutamine metabolism and ammonium excretion,together with H secretion, lead to the generation of increasingamounts of bicarbonate ions and the well-recognized rise inextracellular fluid bicarbonate content in chronic respiratoryacidosis. I merely suggested that the increased bicarbonateconcentration, by inhibiting succinate dehydrogenase, mightoffset the stimulatory effect of acidemia on glutamine metabo-lism such that in the steady state of chronic respiratory acido-sis, ammonium production is not increased. This explanation iscompatible with the data obtained in rat kidney by Rodriguez-Nichols and Tannen [721 and the finding that renal tissue aKGis decreased in chronic metabolic acidosis and acute, but notchronic, respiratory acidosis [121]. The substantial increase inammonium excretion observed in your studies might suggestthat the situation differs in the dog and rat [120]. Alternatively,Tannen has suggested that an adaptive increase in distal, butnot proximal, proton transport occurs in chronic respiratoryacidosis [1221.
DR. RONALD PERRONE (Division of Nephrology, New En-gland Medical Center): Could you comment on the pathophys-iology of hyperkalemic renal tubular acidosis, in particular,whether you believe this is a disorder of ammoniagenesis versusa disorder of proton pumping?
DR. SCHOOLWERTH: Hyperkalemia reduces ammonium ex-cretion [123, 124]. The decreased ammonium excretion likelyreflects the ability of the elevated potassium concentration todecrease ammonium production [125]. Studies in chronicallyhyperkalemic rats recently confirmed a significant reduction inwhole-kidney ammonium production and excretion [126]. How-ever, chronic hyperkalemia had no effect on net ammoniumsecretion or absolute ammonium delivery out of the proximaltubule; thus reduced ammonium excretion probably is due tosome other abnormality, such as reduced ammonium transportinto collecting ducts in the medulla [1261. With regard tohyperkalemic RTA, a decrease in both ammonium productionand ammonium entry and altered proton pumping are likely toexist. I know of no evidence suggesting a reciprocal relationshipbetween ammonium and titratable acid excretion under thesecircumstances. In fact, I would expect titratable acid excretionalso to be reduced in situations in which proton pumping isimpaired.
DR. MAmAs: You mentioned that in acute metabolic acidosisin the rat, the renal cortical aKG level is decreased and theactivity of aKGDH is increased, presumably in response to theacidification of body fluids. Yet, in the chronic phase of metabolicacidosis, renal ammonium production is higher than acutely,despite higher systemic and renal pH values. My question is, hasthe activity of the aKGDH enzyme been looked at in chronicmetabolic acidosis as compared with the acute phase?
DR. SCHOOLWERTH: I am unaware of any data demonstratingan increased activity of renal aKGDH in chronic metabolicacidosis. Freeze-clamp studies of renal cortex from chronicallyacidotic rats and dogs have shown that tissue aKG and gluta-mate levels remain decreased [26]. These changes might reflectevents earlier in metabolic acidosis, but these alterations also

970 Nephrologv Forum: Regulation of renal ammoniagenesis
might "deinhibit" both PDG and GDH, resulting in an evengreater stimulation in ammonium production than in acutemetabolic acidosis. As I mentioned previously, the regulation ofthe augmented rate of ammoniagenesis in chronic metabolicacidosis likely involves factors other than those occurring inacute acidosis. For example, the enzymes PDG and GDH areinduced in the rat but not in the dog.
DR. MADIAs: What is the importance of the basolateralmechanism for the entry of glutamine in the proximal tubulecell? Some data suggest adaptation of this transporter in chronicmetabolic acidosis in the dog [1271.
DR. SCHOOLWERTH: The study you refer to revealed analmost twofold increase in the max for glutamine uptake inrenal basolateral vesicles from dogs with metabolic acidosis[127]. Earlier, Silverman et al had obtained evidence in vivothat the unidirectional basolateral uptake of glutamine was notincreased in chronically acidotic as compared with normaldogs; the data suggested no adaptation of this transporter [128].The data further suggested that under normal acid-base condi-tions, bidirectional transport of glutamine occurred across thebasolateral membrane, but with increased oxidation of glu-tamine in metabolic acidosis, the cell served as a "sink" andaccounted for increased extraction. I do not believe that theplasma membrane transport of glutamine across either theluminal or basolateral membrane is a rate-limiting factor in themetabolism of glutamine by renal proximal tubules.
Da. HARRINGTON: I'm interested in what happens to theenzymes in the reverse side, that is, in chronic metabolicalkalosis. Are these enzymes turned off as one might expect?Specifically, what happens to alpha ketoglutarate?
DR. SCHOOLWERTH: Several laboratories have demonstrateda decrease in rat renal PDG activity in chronic metabolicalkalosis [14, 129]. Seyama and associates found no decrease inGDH activity after feeding of sodium bicarbonate to rats [130].On increasing pH, the activity of aKGDH decreases because ofa decreased affinity of the enzyme for its substrate aKG [291;however, I am not aware of any measurements of the activity ofthe enzyme in renal cortex from chronically alkalotic animals.
DR. HARRINGTON: The data you've discussed have beenobtained in rats and dogs. Are there new ways of looking athumans to find out the answers to any of these questions? I'minterested in both in-vitro and in-vivo studies and techniques.
DR. SCHOOLWERTH: In-vivo studies performed by Tizianelloand collaborators have demonstrated an increase in ammoniumproduction both in acute and chronic metabolic acidosis [24,131]. Although glutamine extraction and ammonium productionwere measured, it is difficult to identify the metabolic pathwaysinvolved from these in-vivo studies. With increasing success inculturing human proximal renal tubular cells, it is likely thatadditional information will be forthcoming [132]. For example,studies have evaluated the effect of pH in the medium onglutamine metabolism in cultured human cortical cells. Thesestudies with radiolabeled nitrogen demonstrated an increase inglutamate deamination following a decrease in pH [133]. Al-though there is always a concern about dedifferentiation of cellsin culture, future studies should provide insight into the molec-ular mechanisms regulating increased glutamine metabolismwith both acute and chronic reductions in medium pH.
DR. LEVEY: Other than urine pH, what are the factors thatregulate the proportion of ammonium that is excreted in the
urine and that is returned in the renal venous blood? What arethe effects of metabolic acidosis on these factors?
DR. SCHOOLWERTH: Other than pH, urine flow rate affectsthe proportion of ammonium that is excreted, at least in urine thatis only weakly acid or mildly alkaline. In addition, a relationshipbetween potassium concentration and ammonium excretion hasbeen demonstrated; thus, potassium loading leads to a reductionin ammonium excretion, whereas potassium depletion increasesurinary ammonium excretion [134]. Currently there is a great dealof interest in evaluating ammonia and ammonium transport indifferent nephron segments; new studies should clarify the mech-anisms of regulation of ammonium excretion [see 135, 136]. Thecomplex mechanisms for the transport of ammonia and ammo-nium also might interrelate with ammonium production. Forexample, Nagami and Kurokawa have shown that an increasedluminal flow rate leads to an increase in ammonium productionfrom glutamine in proximal tubules [1371. The factors that affectammonium excretion likely pertain in metabolic acidosis. It shouldbe emphasized that the same factors that stimulate ammoniumproduction are likely to result in increased ammonium excretion.
DR. MADIAS: Does phosphate play a role in regulating theactivity of phosphate-dependent glutaminase?
DR. SCHOOLWERTH: Glutaminase is activated by phosphate,among other anions. The maximum activation of renal PDGoccurs at high phosphate concentrations, considerably in ex-cess of those thought to occur in vivo. To my knowledge, datahave not demonstrated an alteration in cytosolic or mitochon-drial phosphate concentrations as a function of acid-base dis-turbances; thus no data suggest that phosphate is an importantregulator of the enzyme in situ. However, Yu et al havedemonstrated a stimulation of ammonium production and ex-cretion by inorganic phosphorus in rabbit kidney, and thisresponse might be unique to this species [138].
DR. MADIAS: Do we understand the nature of the adaptationof ammoniagenesis in the remnant kidney?
DR. SCFIOOLWERTH: An adaptive increase in ammoniumproduction and excretion per remaining nephron occurs inremnant dog and rat kidneys [6, 8]. In our studies, we evaluatedthe adaptive increase in ammonium excretion and production inthe remnant kidney of rats fed 6% and 40% casein diets.Adaptive increases in total ammonium excretion and ammo-nium excretion per nephron were observed in the animals fedthe 40% protein, but not the 6% protein, diets. In-vitro studiesin these animals demonstrated increased ammonium productionfrom both glutamine and glutamate in animals with the highprotein intake. The increase was present when measured pergram of tissue weight, per milligram of protein, or per mg ofDNA; total-kidney DNA did not change in the remnant, sothese studies were consistent with an increase in ammoniumproduction per cell. We also assessed enzyme activity andfound an increased activity of PDG in remnant renal cortexfrom rats fed both the low- and high-protein diet. However, weobserved an increase in GDH activity only in the animals given40%, but not 6%, protein [8]. This increase occurred without ademonstrable change in systemic acid-base value, thus lendingsupport to the hypothesis that the stimulation in metabolism isrelated to increased hemodynamics, specifically an increase insodium load and sodium reabsorption per nephron [139]. Fur-ther work is needed to clarify the mechanisms of the adaptiveincrease in ammonium production per nephron [9].

Nephrology Forum: Regulation of renal ammoniagenesis 971
DR. MADIAS: Has there been any further progress in thecharacterization of the renal ammoniagenic factor reported byAlleyne and colleagues in the plasma of rats with acute meta-bolic acidosis [140]?
DR. SCHOOLWERTH: I am unaware of any studies furthercharacterizing the factor described by Alleyne and colleagues.
Reprint requests to Dr. A. Schoolwerth, Division of Nephrology,Virginia Commonwealth University, Box 160, Richmond, Virginia23298-0160, USA
Acknowledgments
The work presented in this Forum was supported in part by NationalInstitutes of Health grant DK 36822.
References
I. TANNEN RL: Ammonia metabolism. Am J Physiol 235:F265—F277, 1978
2. HALPERIN ML, GOLDSTEIN MB, STINEBAUGH BJ, JUNGAS L:Biochemistry and physiology of ammonium excretion, in TheKidney: Physiology and Pathophysiology, edited by SELDIN DW,GIEBISCH G, New York, Raven, 1985, pp 1471—1490
3. BROSNAN JT, LOWRY M, VINAY P, Gouooux A, HALI'ERIN ML:Renal ammonium production-une vue canadienne. Can J PhysiolPharmacol 65:489—498, 1987
4. OLIVERJ, BOURKE E: Adaptations in urea ammonium excretion inmetabolic acidosis in the rat: a reinterpretation. Clin Sci Mo! Med48:515—520, 1975
5. GUDER WG, HAUSSSINGER D, GEROK W: Renal and hepaticnitrogen metabolism in systemic acid base regulation. J Clin ChemClin Biochem 25:457—466, 1987
6. HALPERIN ML, JUNGAS RL: The metabolic production and renaldisposal of hydrogen ions. Kidney mt 24:709—713, 1983
7. SIMPSON DP: Mitochondrial transport functions and renal metab-olism. Kidney mt 23:785—793, 1983
8. SCHOOLWERTH AC, LANOUE KF: Transport of metabolic sub-strates in renal mitochondria. Annu Rev Physiol 47:143—171, 1985
9. ATKINSON DE, BOURKE E: The role of ureagenesis in pH homeo-stasis. Trends Biochem Sci 9:297—300, 1984
10. ATKINSON DE, BOURKE E: Metabolic aspects of the regulation ofsystemic pH. Am J Physiol 252:F947—F956, 1987
11. HAUSSINGER D, GEROK W, SIES H: Hepatic role in pH regulation:role of the intercellular glutamine cycle. Trends Biochem Sci9:300—302, 1984
12. HALPERIN ML, JUNGAS RL, CHEEMA-DHADLI S, BROSNAN iT:Disposal of the daily acid load: an integrated function of the liver,lungs, and kidneys. Trends Biochem Sci 12:197—199, 1987
13. TANNEN RL, SAHAI A: Biochemical pathways and modulators ofrenal ammoniagenesis. Miner Electrolyte Metab 16:249—258, 1990
14. CURTHOYS NP, LOWRY OH: The distribution of glutaminaseisoenzymes in the various structures of the nephron in normal,acidotic, and alkalotic rat kidney. J Biol Chem 248:162—168, 1973
15. WRIGHT PW, KNEPPER MA: Distribution of ammoniagenic en-zymes in renal cortical and medullary tubule segments. Proc Fifthmt Workshop Ammoniagenesis, Tsumagoi, Japan, July 11—14,1990, p 12
16. GooD DW, BURG MB: Ammonia production by individual seg-ments of the rat nephron. J Clin Invest 73:602—610, 1984
17. NONOGUCHI H, TAKEHARA Y, ENDOU H: Intra- and inter-nephronheterogeneity of ammoniagenesis in rats: effects of chronic meta-bolic acidosis and potassium depletion. Pflugers Arch 407:245—251, 1986
18. CURTHOYS NP: Role of y-glutamyltranspeptidase in the renal metab-olism of glutathione. Miner Electrolyte Metab 9:236—245, 1983
19. COOPER AJL, MEISTER A: Isolation and properties of a newglutamine transaminase from rat kidney. J Biol Chem 249:2554—2561, 1974
20. NISSIM I, YUDKOFF M, SEGAL S: Metabolism of glutamine andglutamate by rat renal tubules. Study with '5N and gas chroma-tography-mass spectrometry. J Biol Chem 260:13955—13967, 1985
21. STRZELECKI T, ROGULSKI J, ANGIELSKI S: The purine nucleotidecycle and ammonia formation from glutamine by rat kidney slices.Biochem J 212:705—711, 1983
22. SQUIRES EJ, HALL DE, BROSNAN JT: Arteriovenous differencesfor amino acids and lactate across kidneys of normal and acidoticrats. Biochem J 160:125—128, 1976
23. HUGHEY RP, RANKIN BB, CURTHOYS NP: Acute acidosis andrenal arteriovenous differences of glutamine in normal and adre-nalectomized rats. Am J Physiol 238:Fl99—F204, 1980
24. TIZIANELLO A, DEFERRARI G, GARIBOTTO G, RABAUDO C, Ac-
QUARONE N, GHIGGERI GM: Renal ammoniagenesis in an earlystage of metabolic acidosis in man. J Clin Invest 69:240-250,1982
25. PITTS RF: Control of renal production of ammonia. Kidney Int1:297—305, 1972
26. VINAY P, ALLIGNET E, PICHETTE C, WATFORD M, LEMIEUX G,GouGoux A: Changes in renal metabolite profile and ammonia-genesis during acute and chronic metabolic acidosis in dog and rat.Kidney Int 17:312—325, 1980
27. TANNEN RL, SASTRASJNH S: Response of ammonia metabolism toacute acidosis. Kidney Int 25:1—10, 1984
28. MCCORMACK JG, DENTON RM: The effects of calcium and ade-nine nucleotides on the activity of pig heart 2-oxoglutarate dehy-drogenase complex. Biochem J 180:533—544, 1979
29. LOWRY M, Ross BD: Activation of oxoglutarate dehydrogenase inthe kidney in response to acute acidosis. Biochem J 190:771—780,1980
30. TANNEN RL, KUNIN AS: Effect of pH on metabolism of a-keto-
glutarate by renal cortical mitochondria. Am J Physiol 240:F120—F126, 1981
31. SCHOOLWERTH AC, LANOUE KF: Control of ammoniagenesis bya-ketoglutarate in rat kidney mitochondria. Am J Physiol 244:F399—F408, 1983
32. SCHOOLWERTH AC, STRZELECKI T, LANOUE KF, HOOVER Wi:Effect of pH and a-ketoglutarate on mitochondnal ammoniaproduction. Contrib Nephrol 31:127—133, 1982
33. SCHOOLWERTH AC, STRZELECKI T, GESEK FA: Regulation of ratkidney mitochondrial metabolism in acute acidosis. Am J KidneyDis 14:303—306, 1989
34. SCHOOLWERTH AC, LANOUE KF: Effects of 2-oxoglutarate andglutamate on glutamine metabolism by rat kidney mitochondna, inGlutamine Metabolism in Mammalian Tissues, edited by HAUSS-INGER D, SIE5 H, Heidelberg, Springer, 1984, pp 178—186
35. BOGUSKY RT, DIETRICH RL: Effect of acute metabolic acidosis onammonia metabolism in kidney. Am J Physiol 256:F321—F328,1989
36. PREUSS HG, WEISS FR: Rate-limiting factor in rat kidney sliceammoniagenesis. Am J Physiol 221:458—464, 1971
37. PREUSS HG: Regulation of renal ammoniagenesis during acidosis:the pyridine nucleotide hypothesis revisited. Life Sci 27:2293—2302, 1980
38. SHAPIRO RA, MOREHOUSE RF, CURTHOYS NP: Inhibition by
glutamate of phosphate-dependent glutaminase of rat kidney.Biochem J 207:561—566, 1982
39. MITCHELL P: Chemiosmotic Coupling in Oxidation and Photosyn-thetic Phospho,ylation, Res Rep 66/1, Bodwin, Cornwall, En-
gland, Glynn Res Ltd, 196640. MITCHELL P, MOYLEJ: Estimation of membrane potential and pH
difference across the cristal membrane of rat liver mitochondria.Eur J Biochem 7:471—484, 1969
41. ROTTENBERG H: The measurement of membrane potential and pHin cells, organelles, and vesicles. Methods Enzymol 55:547—569,
1979
42. SIMPSON DP, HAGER SR: pH and bicarbonate effects on mito-chondrial anion accumulation. Possible mechanism for changes inrenal metabolite levels in acute acid-base disturbances. J ClinInvest 63:704—712, 1979
43. HAGER SR, SIMPSON DP: Influence of bicarbonate buffer systemon pH gradient in rabbit renal cortex mitochondria. MolecularPhysiol 2:203—211, 1982
44. STRZELECKI T, THOMAS JA, KOCH CD, LANOUE KF: The effectof hormones on proton compartmentation in hepatocytes. J BidChem 259:4122—4129, 1984

972 Nephrology Forum: Regulation of renal ammoniagenesis
45. SCHOOLWERTH AC, GESEK FA, CULPEPPER RM: Proton compart-mentation in rat renal cortical tubules. Am J Physiol 256:F986—F993, 1989
46. RINK TJ, TSIEN RY, POZZAN T: Cytoplasmic pH and free Mg2 inlymphocytes. J Cell Biol 95:189—196, 1982
47. PFALLER WW, RITTINGER M: Quantitative morphology of the ratkidney. ml j Biochem 12:17—22, 1980
48. LAWLIS YB, ROCHE TE: Regulation of bovine kidney a-ketoglu-tarate dehydrogenase complex by calcium ion and adenine nude-otides. Effects on S05 for s-ketoglutarate. Biochemistry 20:2512—2518, 1981
49. TULLISON P, GOLDSTEIN L: Allosteric regulation of renal a-keto-glutarate dehydrogenase. Contrib Nephrol 31:122—126, 1982
50. MCCORMACK JG, BROMIDGE ES, DAWES NJ: Characterization ofthe effects of Ca2 on the intramitochondrial Ca2-sensitive de-hydrogenases within intact rat-kidney mitochondria. BiochimBiophys Acta 934:282—292, 1988
51. SCHOOLWERTH AC, SMITH BC: Ammoniagenesis and protoncompartmentation in dog kidney cortex. Contrib Nephrol 63:71—76, 1988
52. SCHOOLWERTH AC, GESEK FA: Intramitochondrial pH and am-monium production in rat and dog kidney cortex. Miner Electro-lyte Metab 16:264—269, 1990
53. VINAY P, LEMIEUX G, GouGoux A, HALPERIN ML: Regulationof glutamine metabolism in dog kidney in vivo. Kidney hit29:68—79, 1986
54. LANOUE KF, SCHOOLWERTH AC: Metabolite transport in mam-malian mitochondria, in Bioenergetics, New Comprehensive Bio-chemistry (vol 9), edited by ERNSTER L, Amsterdam, Elsevier,1984, pp 221—268
55. SCHOOLWERTH AC, LANOUE KF, HOOVER WJ: Glutamate trans-port in rat kidney mitochondria. J Biol Chem 258:1735—1739, 1983
56, LANOUE KF, SCHOOLWERTH AC, PEASE AJ: Ammonia formationin isolated rat liver mitochondria, J Biol Chem 258:1726—1734,1983
57. KUNIN AS, TANNEN RL: Regulation of glutamate metabolism byrenal cortical mitochondria. Am J Physiol 237:F55—F62, 1979
58. SCHOOLWERTH AC, LANOUE KF: The role of microcompartmen-tation i the regulation of glutamate metabolism by rat kidneymitochondria. J Biol Chem 255:3403—3411, 1980
59. SCHOOLWERTH AC, LANOUE KF, HOOVER Wi: Effect of pH onglutamate efflux from rat kidney mitochondria. Am J Physiol245:F266—F27l, 1984
60. LANOLJE KF, TISCHLER ME: Electrogenic characteristics of themitochondrial glutamate-aspartate antiporter. J Biol Chem 249:7522—7528, 1974
61. SCHOOLWERTH AC, HOOVER WJ, DANIEL CH, LANOUE KF:Effect of aminooxyacetate and a-ketoglutarate on glutamatedeãmination by rat kidney mitochondria. list J Biochem 12:145—149, 1980
62. ADAM W, SIMPSON DP: Glutamine transport in rat kidney mito-chondria in metabolic acidosis. J Clin Invest 54:165—174, 1974
63. SIMPSON DP, ADAM W: Glutamine transport and metabolism bymitochondria from dog renal cortex. J Biol Chem 250:8148—8158,1975
64. SIMPSON DP: Modulation of glutamine transport and metabolismin mitochondria from dog renal cortex. Influence of pH andbicarbonate. J Biol Chem 255:7123—7128, 1980
65. GOLDSTEIN L: Glutamine transport by mitochondria isolated fromnormal and acidotic rats. Am J Physiol 229:1027—1033, 1975
66. BROSNAN JT, HALL B: The transport and metabolism of glutainineby kidney-cortex mitochondria from normal and acidotic rats.Biochem J 164:331—337, 1977
67. CURTHOYS NP, SHAPIRO RA: Effect of metabolic acidosis and ofphosphate on the presence of glutamine within the matrix space ofrat renal mitochondria during glutamine transport. J Biol Chem253:63—68, 1978
68. SASTRASINH S, SASTRASINH M: Glutamine transport in submito-chondrial particles. Am J Physiol 257:F1050—Fl058, 1989
69. SASTRASINH M, SASTRASINH S: Effect of acute pH change onmitochondrial glutamine transport. Am J Physiol 259:F863—F866,1990
70. WANDERS RJA, MEIJER AJ, GROEN AK, TAGER JM: Bicarbonate
and the pathway of glutamate oxidation in isolated rat-livermitochondria. Eur J Biochem 133:245—254, 1983
71. SCADUTO RC Ja, SCHOOLWERTH AC: Effect of bicarbonate onglutamine and glutamate metabolism by rat kidney cortex mito-chondria. Am J Physiol 249:F573—F581, 1985
72. RODRIGUEZ-NICHOLS F, LAUGHREY FE, TANNEN RL: Responseof renal NH3 production to chronic respiratory acidosis. Am JPhysiol 247:F896—F903, 1984
73. RECTOR RC JR. SELDIN DW, COPENHAVER JH: The mechanism ofammonia excretion during ammonium chloride acidosis. J ClinInvest 34:20—26, 1954
74. SCHOOLWERTH AC, NAZAR BL, LANOUE KF: Glutamate dehy-drogenase activation and ammonia formation by rat kidney mito-chondria. J Biol Chem 253:6177—6183, 1978
75. Nissnt I, YUDKOFF M, SEGAL S: Metabolism of glutamine andglutamate by rat renal tubules. Study with 15N and gas chroma-tography-mass spectrometry. J Biol Chem 260:13955—13967, 1985
76. GOODMAN AD, Fuisz RE, CAHILL GF: Renal gluconeogenesis in
acidosis, alkalosis, and potassium deficiency: its possible role inregulation of renal ammonia production. J Clin Invest 45:612—619,1966
77, ALLEYNE GAO, SCULLARD GH: Renal metabolic response toacid-base changes. 1. Enzymatic control of animoniagenesis in therat. J Clin Invest 48:364—370, 1969
78. TONG J, SHAPIRO RA, CURTHOYS NP: Changes in the levels oftranslatable glutaminase mRNA during onset and recovery frommetabolic acidosis. Biochem J 26:2773—2777, 1987
79. SHAPIRO RA, BANNER C, HWANG J, WENTHOLD RJ, CURTHOYSNP: Regulation of renal glutaminase gene expression duringmetabolic acidosis. Contrib Nephrol 63:141—146, 1988
80. KAISER PS, HWANG JJ, CURTHOYS NP: Effect of acidosis onphosphoenolpyruvate carboxykinase (PCK) and glutaminase (GA)mRNAs in rat kidney and in LLC-PK-F cells. Fifth Int WorkshopAmmoniagenesis, Tsumagoi, Japan, July 11—14, 1990, p
81. MAPES RE, WATFORD M: Acid-base regulation of renal geneexpression: a role for cAMP? Contrib Nephrol 63:147—155, 1988
82. MAPES RE, WATFORD M: Effects of metabolic acidosis anddiabetes on the abundance of specific renal mRNAs. mt i Bio-chem 21:297—305, 1989
83. SCHOOLWERTH AC, BETCHER SL, CURTHOYS NP: Renal metab-olism, in Contemporary Nephrology, edited by KLAHR S. MASSRYS, New York, Plenum, 1989, pp 81—112
84. RECTOR FC JR, ORLOFI' J: The effect of the administration ofsodium bicarbonate and ammonium chloride on the excretion andproduction of ammonia. The absence of alterations in the activityof renal ammonia-producing enzymes in the dog. J Clin Itivest38:366—372, 1959
85. LEMIEUX G, BAVEREL G, VINAY P, WADOUX P: Glutaminesynthetase and glutamyltransferase in the kidney of man, dog, andrat. Am JPhysiol23l:1068—1073, 1976
86. MCCORMACK JG, HALESTRAP AP, DENTON RM: Role of calcium
ions in regulation of mammalian intramitochondrial metabolism.Physiol Rev 70:391—425, 1990
87. LEFURGEY A, INGRAM P, MANDEL U: Heterogeneity of calcium
compartmentation: electron probe analysis of renal tubules. JMembrBiol 94:191—196, 1986
88. SOMLYO AP, BOND M, SOMLYO AV: Calcium content of tnito-chondria and endoplasmie reticulum in liver frozen rapidly in vivo.Nature (Lond) 314:622—625, 1985
89. KLAHR S, NAWAR T, SCHOOLWERTHAC: Effects of catechol-amineS on ammoniagenesis and gluconeogenesis by renal cortex invitro. Biochim Biophys Ada 304:161—168, 1973
90. CHOBANIAN MC, HAMMERMAN MR: Insulin stimulates ammonia-genesis in canine renal proximal tubular segments. Am J Physiol253:Fll7l—Fl 177, 1987
91. CHOBANIAN MC, HAMMERMAN MR: Parathyroid hormone stim-ulates ammoniagenesis in canine renal proximal tubular segments.Am J Physiol 255:F847—F852, 1988
92. CHOBANIAN MC, JULIN CH, 000DFRIEND TL: Angiotensin Hstimulates ammoniagenesis in canine renal proximal tubular seg-ments. Kidney list 35:443, 1989
93. CHOBANIAN MC: Hormonal control of renal ammonium metabo-lism: a review. Am J Kidney Dis 14:248—252, 1989

Nephrology Forum: Regulation of renal ammoniagenesis 973
94. GESEK FA, MISHKIND MT. SCHOOLWERTH AC: Hormonal regu-lation of renal ammonium and glucose production are modulatedby Na/H exchange. Contrib Nephrol, in press
95. GESEK FA, SCHOOLWERTH AC: Hormonal interactions with theproximal Na/H exchanger. Am J Physiol 258:F514—F521, 1990
96. DORI-IOUT-MEES Li, MACHADO M, SLATOPOLSKY E, KLAHR S,BRICKER NS: The functional adaptation of the diseased kidney.III. Ammonium excretion. J Clin Invest 45:289—296, 1966
97. Srau'soi'i PD: Control of hydrogen ion homeostasis and renalacidosis. Medicine 50:503—541, 1971
98. SCHOOLWERTH AC, SANDLER RS, HOFFMAN PM, KLAHR S: Theeffects of nephron reduction and dietary protein content on renalammoniagenesis in the rat. Kidney mt 7:397—404, 1975
99. MACLEAN AJ, HAYSLETT JP Adaptive changes in ammoniaexcretion in renal insufficiency. Kidney mt 7:595—606, 1980
100. HARRIS DCH, CHAN L, SCHRIER RW: Remnant kidney hyperme-tabolism and progression of chronic renal failure. Am J Physiol254:F267—F276, 1988
101. NATH KA, HOSTETTER MK, HOSTETTER TH: Pathophysiology ofchronic tubulo-interstitial disease in rats. Interactions of dietaryacid load, ammonia, and complement component C3. J Clin Invest76:667—675, 1985
102. NATH KA, CROAT AJ, HOSTETTER TH: 02 consumption andoxidant stress in the surviving nephrons. Am J Physiol 258:F1354—F1362, 1990
103. BUERKERT J, MARTIN D, TRIGG D, SIMON E: Effect of reducedrenal mass on ammonium handling and net acid formation by thesuperficial and juxtamedullary nephron of the rat. Evidence forimpaired entrapment rather than decreased production of ammo-nium in the acidosis of uremia. J Clin Invest 71:1661—1675, 1983
104. GOLCHINI K, NORMAN i, BOHMAN R, KURTZ I: Induction ofhypertrophy in cultured proximal tubule cells by extracellularNH4CI. J Clin Invest 84:1767—1779, 1989
105. KURTZ I, D.ss PD, CRAMER S: The importance of renal ammoniametabolism to whole body acid-base balance: a reanalysis of thepathophysiology of renal tubular acidosis. Miner ElectrolyteMetab 16:331—340, 1990
106. DONNELLY S, VASUVATTAKUL S, HALI'ERIN ML: Is distal renaltubular acidosis (RTA) a proximal cell disease? JAm Soc Nephrol1:318, 1990
107. HALPERIN ML, RICHARDSON RMA, BEAR RA, MAGNER P0,KAMEL K, ETHIER J: Urine ammonium: the key to the diagnosisof distal renal tubular acidosis. Nephron 50:1-4, 1988
108. TANNEN RL: Relationship of renal ammonia production andpotassium homeostasis. Kidney mt 11:453—465, 1977
109. ADAM WR, KORETSKY AP, WEINER MW: 31P-NMR in vivomeasurement of renal intracellular pH: effect of acidosis and Kdepletion in rats. Am J Physiol 251 :F904—F910, t986
110. SCHOOLWERTH AC, CULPEPPER RM: Measurement of intracellu-lar pH in suspensions of renal tubules from potassium-depletedrats. Miner Electrolyte Metab 16:191—196, 1990
ill. GABUZDA Gi, HALL PW: Relation of potassium depletion to renalammonium metabolism and hepatic coma. Medicine 45:481—490,1966
112. T0LIN5 iP, HOSTETTER MK, HOSTETTER TH: Hypokalemicnephropathy in the rat. Role of ammonia in chronic tubular injury.J Clin Invest 79: 1447—1458, 1987
113. DESOUSA RC, HARRINGTON JT, RICANATI ES, SHELKROT iW,SCHWARTZ WB: Renal regulation of acid-base equilibrium duringchronic administration of mineral acid. J Clin Invest 53:465—476,1974
114. SCI-IWARTZ WB, COHEN ii: The nature of the renal response tochronic disorders of acid-base equilibrium. Am J Med 64:417—428,1968
115. LOWANCE C, GARFINKLE HB, MATTERN WD, SCHWARTZ WB:The effect of chronic hypotonic volume expansion on the renalregulation of acid-base equilibrium. J Clin Inest 51:2928—2940, 1972
116, COHEN Ji, HULTER HN, SMITHLINE N, MELBY JC, SCHWARTZWB: The critical role of the adrenal gland in the renal regulation ofacid-base equilibrium during hypotonic expansion. J Clin Invest58: 1201—1208, 1976
117. HALPERIN ML, CHEN CB: Influence of acute hyponatremia onrenal ammoniagenesis in dogs with chronic metabolic acidosis.Am J Physiol 258:F328—F332, 1990
118. LEMIEUX G, VINAY P, CARTIER P: Renal hemodynamics andammoniagenesis. Characteristics of the antiluminal site for glu-tamine extraction. J Clin Invest 53:884—894, 1974
119. Gouooux A, VINAY P, CARDOSO M, DUPLAIN M, LEMIEUX G:Immediate adaptation of the dog kidney to acute hypercapnea. AmJ Physiol 243:F227—F234, 1982
120. ADROGUE HG, MADIAS NE: Renal acifidication during chronic
hypercapnea in the conscious dog. Pflugers Arch 406:520—528, 1986121. TRIVEDI B, TANNEN RL: Effect of respiratory acidosis on intra-
cellular pH of the proximal tubule. Am J Physiol 250:Fl039—F1045, 1986
122. TANNEN RL, HAMID B: Adaptive changes in renal acidification inresponse to chronic respiratory acidosis. Am J Physiol 248:F492—F499, 1985
123. HULTER HN, ILNICKI LP, HARBOTTLE A, SEBASTIAN A: Impairedrenal H secretion and NH3 production in mineralocorticoid-
deficient glucocorticoid-replete dogs. Am J Physiol 232:F136-F146, 1977
124. HULTER HN, ToTo RD, ILNICKI LP, SEBASTIAN A: Chronichyperkalemic renal tubular acidosis induced by KCI loading. Am JPhysiol 244:F255—F264, 1983
125. SASTRASINH S, TANNEN RL: Effect of potassium on renal NH3
production. Am J Physiol 244: F383—F39l, 1983126. DUBOSE TD, GooD DW: Effects of chronic hyperkalemia on renal
production and proximal tubule transport of ammonium in rats.Am J Physiol 260:F680—F687, 1991
127. WINDUS DW, COHN DE, KLAHR S, HAMMERMAN MR: Glutaminetransport in renal basolateral vesicles from dogs with metabolicacidosis. Am J Physiol 246:F78—F86, 1984
128. SILVERMAN M, VINAY F, SI-IINOBU L, Goucioux A, LEMIEUX G:Luminal and antiluminal transport of glutamine in dog kidney:effect of metabolic acidosis. Kidney mt 20:359—365, 1981
129. DAVIES BMA, YUDKIN J: Studies in biochemical adaptation. Theorigin of urinary ammonia as indicated by the effect of chronicacidosis and alkalosis on some renal enzymes in the rat. BiochemJ52:407—4l2, 1952
130. SEYAMA 5, SAEKI T, KATUNUMA N: Comparison of propertiesand inducibility of glutamate dehydrogenases in rat kidney and
liver. J Biochem 73:39—45, 1973131. TIZIANELLO A, DEFERRARI G, GARIBOTTAG, GURRERI 0: Effects
of chronic renal insufficiency and metabolic acidosis on glutaminemetabolism in man. Clin Sc! Mo! Med 55:391—397, 1978
132. DETRISAC Ci, SENS MA, GARVIN Ai, SPICER SS, SENS DA:Tissue culture of human kidney epithelial cells of proximal tubule
origin. Kidney Int 25:383—390, 1984133. NIS5IM 1, STATES B: Ammoniagenesis by cultured human renal
cortical epithelial cells: study with '5N. Am J Physiol 256:F187—Fl96, 1989
134. TANNEN RL: Effect of potassium on renal acidification andacid-base homeostasis. Semin Nephrol 7:263—273, 1987
135. HAMM LL, SIMON EE: Roles and mechanisms of urinary bufferexcretion. Am J Physiol 253:F595—F605, 1987
136. KNEPPER MA, PACKER R, GOOD DW: Ammonium transport in thekidney. Physiol Rev 69:179—249, 1989
137. NAGAMI GT, KUROKAWA K: Regulation of ammonia productionby mouse proximal tubules perfused in vitro. Effect of luminalperfusion. J Clin Invest 75:844—849, 1985
138. Yu HL, CIAMMARCO R, GOLDSTEIN MB, STINEBAUGH BJ, HAL-PERIN ML: Stimulation of ammonia production and excretion inthe rabbit by inorganic phosphate. Study of control mechanisms.J Clin Invest 58:557—564, 1976
139. HALPERIN ML, VINAY P, GouGoux A, PICHETTE C, JUNGA5 RL:Regulation of the maximum rate of renal ammoniagenesis in theacidotic dog. Am J Physiol 248:F607—F6l5, 1985
140. ALLEYNE GAO, BARNSWELL J, MCFARLANE-ANDERSON N, AL-EXANDER JE: Renal ammoniagenic factor in the plasma of ratswith acute metabolic acidosis. Am J Physiol 241 (Renal FluidElectrolyte Physiol lO):Fl 12—Fl 16, 1981