Reducing Readmissions Cheryl Ruble, MS, RN, CNS Montana Regional Meetings Glendive Medical Center...
94
Reducing Readmissions Cheryl Ruble, MS, RN, CNS Montana Regional Meetings Glendive Medical Center Glendive, MT
-
Upload
junior-stewart -
Category
Documents
-
view
214 -
download
0
Transcript of Reducing Readmissions Cheryl Ruble, MS, RN, CNS Montana Regional Meetings Glendive Medical Center...
Reducing Readmissions
Cheryl Ruble, MS, RN, CNSMontana Regional Meetings
Glendive Medical CenterGlendive, MT
Your Improvement Opportunity
• Do you know what your readmission rates are? Overall? For specific clinical conditions?
• Compared to other hospitals in your area, state, national? Should you compare to others or just yourself?
• What’s possible?
Aim Statement
• Reduce overall readmissions by 20% from the 2010 baseline by December 31, 2012
• By end of 2013, reduce readmissions for heart failure by 30%.
Outcome Measure
All cause readmissions within 30 days
Process Measure
All cause readmission can include:
• DC phone calls• Risk Assessment
completed• Med-Rec completed on DC• Percent of patients with
complete, customized after care plan
• Percent patients with completed DC education
Outcome Measure
Heart failure patients – readmission within 30 days, all cause

Readmission Reduction Drivers

Reduce readmissions by 20% by 12/31/2013
Identify high risk patients
Risk assessment & stratification
Enhanced admission assessment
Multi-disciplinary care team to coordinate care
Self-management skills
Patient/Caregiver knowledge of medications, symptoms, self-care strategies
Identify and address patients’ health literacy and activation levels
Use of teach-back to validate understanding
Coordination of information along the
care continuum
Create a patient-centered record
Timely communication with members of the care team who are not hospital based
Medication reconciliation at admission, change in level of care, and at discharge
Adequate follow-up and community resources
Coordination with physician/other care provider to facilitate resources and follow-up needs
Post-discharge calls and visits
Integrate organizations and Consider medical home capabilities. Coordinate with skilled nursing facilities.
Determine community resources for vulnerable populations
AIM Primary Driver Secondary Driver

Driver: Identify high risk patients

Risk Stratify: Identify High Risk Patients and Communicate to all Providers
High Risk Patients
• Patient has been admitted two or more times in the past year
• Patient is unable to teach-back, or the patient or family caregiver has low degree of confidence to carry out self-care at home
Nielsen GA, Rutherford P, Taylor J. How-to Guide: Creating an Ideal Transition Home. Cambridge, MA: Institute for Healthcare Improvement; 2009. Available at http://www.ihi.org.

Risk Assessment
• Use a validated readmission risk assessment tool
• Select an easy to implement risk assessment

Assessing Patient Risk
Project Red Risk Factors• Depressive symptoms • Limited health literacy • Frequent hospital
admissions • Unstable housing • Substance abuse
http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/PDFs/TARGET.pdf

Risk Stratification
• Low risk – normal process
• Moderate risk – enhanced hospital process
• High risk – enhanced hospital process + community intervention

Assessing Patient Risk
Project BOOST 8P Screening Tool– Problem medications– Psychological– Principal diagnosis– Polypharmacy– Poor health literacy– Patient support– Prior hospitalization– Palliative care
http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/PDFs/TARGET_screen_v22.pdf

Driver: Self-Management Skills
Patient self management as goal
Primary Driver: Self Management Skills
• Assess patient / caregiver knowledge: of medications, symptoms, self-care strategies
• Health literacy: Identify and address patient’s health literacy and activation level; use culturally appropriate training materials and clear written instructions using health literacy concepts
• Teach-back: Use teach-back to validate understanding; use patient-centered, culturally sensitive educational tools
Medication Reconciliation
•Medication reconciliation– Perform at a minimum on admission & discharge– List given to patient/care giver clearly identifies– For high risk patients, work with home health or other ambulatory providers
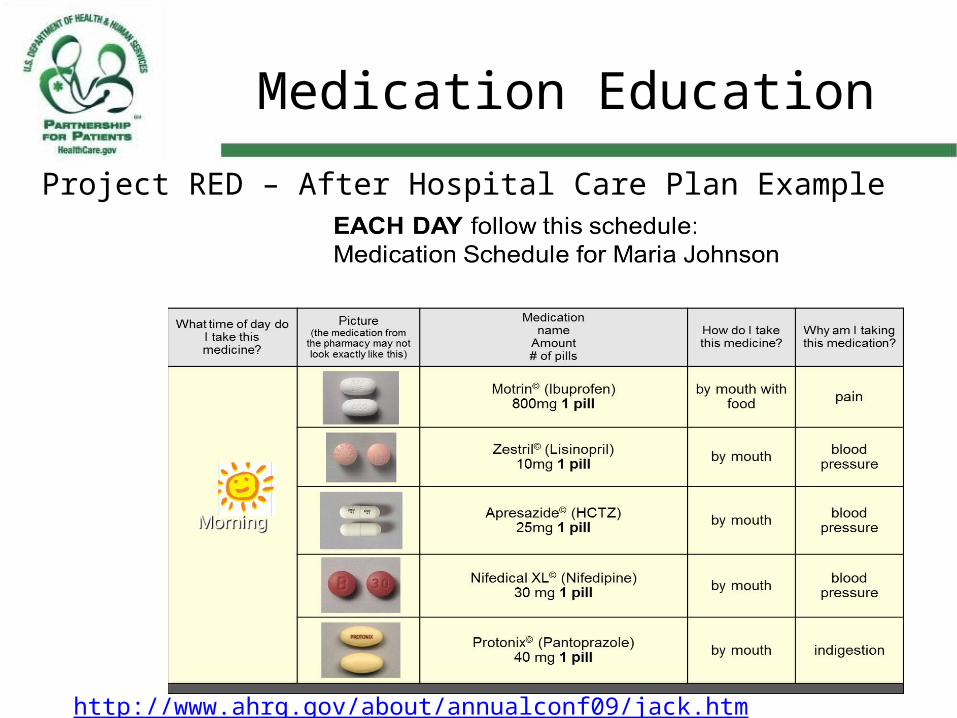
Medication Education
Project RED – After Hospital Care Plan Example
http://www.ahrq.gov/about/annualconf09/jack.htm
Assess Health Literacy
Health literacy measurement tool, available in English and Spanish, from AHRQ
Red Flags for Low Literacy in Patients
• Frequently missed appointments• Incomplete registration forms• Non-compliance with meds• Unable to name meds, explain
purpose or dosing• Identifies pills by looking at
them, not reading label• Unable to give coherent,
sequential history• Ask few questions• Lack of follow through on tests
or referrals

Strategies to Improve Patient Understanding
• Focus on “need to know” & “need to do”
• Use ‘Teach Back’• Demonstrate/draw
pictures• Use clearly written
education materials– 5th grade level or below
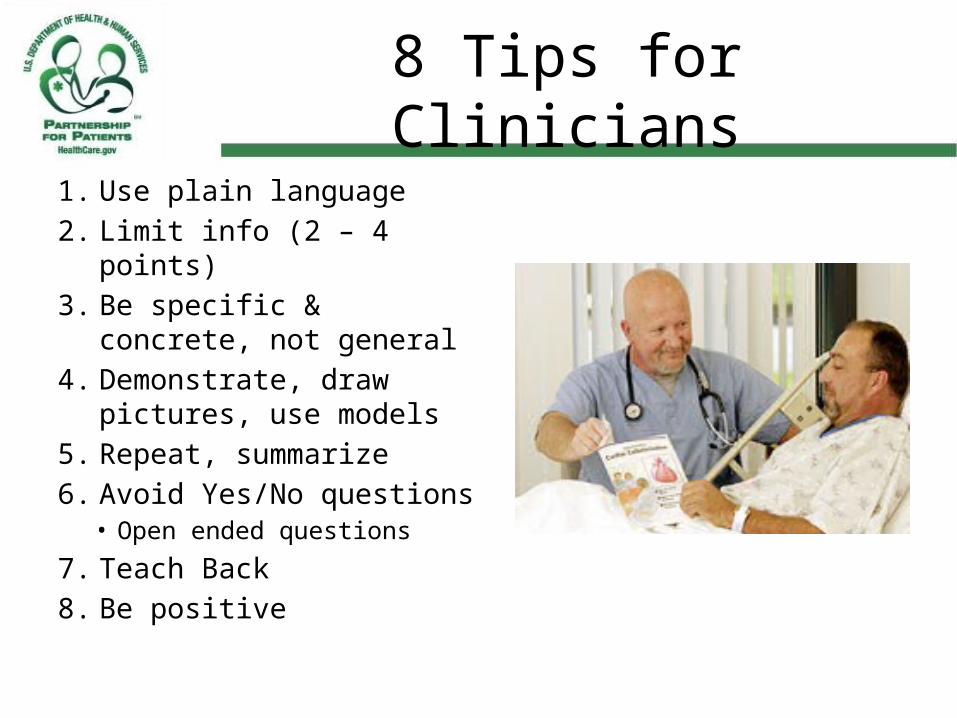
8 Tips for Clinicians
1. Use plain language2. Limit info (2 – 4 points)3. Be specific & concrete,
not general4. Demonstrate, draw
pictures, use models5. Repeat, summarize6. Avoid Yes/No questions
• Open ended questions
7. Teach Back8. Be positive
Teach Back is….
• Asking patients to repeat in their own words what they need to know or do, in a non-shaming way.
• Not a test of the patient, but of how well YOU explained a concept.
• A chance to check for understanding and, if necessary, re-teach.
Teach Back Is…
• Ensuring agreement & understanding– Critical to achieving
adherence
• Associated with improved patient engagement in their own care
“I want to make sure I explained it correctly. Can you tell me in your own words how you understand the plan?”
Teach Back Examples
• “I want to be sure I explained everything clearly. Can you please explain it back to me so I can be sure I did?”
• “What will you tell your husband about the changes we made to your blood pressure medicine?”
• “We’ve gone over a lot of information about getting more exercise in your day. In your own words tell me some of the ways you can get more exercise. How will you make it work at home?”

Teach Back Examples
• “Can you tell me how you take each medicine?”
• “When do you take these medicines?”
• “Home much or how many do you take?”
“Show me how many pills you would take in 1 day.”
Teach-back
• Teach-Back guide from Medicare Quality Improvement Organizations National Coordinating Center for the Integrating Care for Populations and Communities Aim (ICPCA)
• Train clinical staff, use “I” statements

ASTHMA ZONESKnow your zone: Green, Yellow, or Red
Green Zone: All Clear No cough, wheeze, or shortness of breath Sleeping through the night Can do usual activities Don’t need quick-relief (rescue) medicine most
daysor Peak Flow:______________ as instructed
Green Zone Means Your symptoms are under control Continue taking your medications as ordered Continue activity as tolerated Keep all doctor appointments
Yellow Zone: Caution Cough, wheeze, or shortness of breath, chest
tightness Waking at night due to asthma symptoms Can do some but no all usual activities Using more quick-relief (rescue) medicine more
frequently No improvement in your symptoms after
medications were startedor Peak Flow:______________
Yellow Zone Means: Warning Your symptoms may mean that you need a
change in your medications Call your doctor_____________________ number_____________________ Call your Home Care Nurse 24 hour
number___________________________Tell your home care nurse if you call or see your doctor
Red Zone: Medical Alert Very short of breath, ribs show Quick-relief (rescue) medicine has not helped• If you have trouble walking or talking• Your lips or fingernails are blue• You are feeling faintor Peak Flow:______________
Red Zone Means: Emergency This indicates that you need to be seen by a
doctor right away- NOW!
Call 911 or go to the nearest emergency room

COPD ZONESKnow your zone: Green, Yellow, or Red
Green Zone: All Clear Able to do usual activities No new symptoms No chest pain Your usual medications are controlling your symptoms
Green Zone Means Your symptoms are under control Continue taking your mediations as ordered Continue activity as tolerated Use pursed lip breathing as instructed Keep all doctor appointments
Yellow Zone: Caution If you have any of the following signs and symptoms: Increased cough and/or discolored sputum production Increased in shortness of breath with usual activity level Increase in the amount of quick relief medications used Change in usual energy level: increase in either fatigue
or restlessness
Yellow Zone Means: Warning Your symptoms may indicate that you need an adjustment of
your medications Call your doctor_____________________ number_____________________• You should consult or see your doctor within 24-48 hours Call your Home Care Nurse 24 hour
number___________________________Tell your home care nurse if you call or see your doctor
RED ZONE: MEDICAL ALERT Severe or unusual shortness of breath: shortness of
breath at rest Unrelieved chest pain Wheezing or chest tightness at rest Need to sit in chair to sleep if you don’t normally New or increased confusion
RED ZONE Means: Emergency This indicates that you need to be evaluated by a
doctor right away – NOW!
Go to the nearest emergency room or call 911
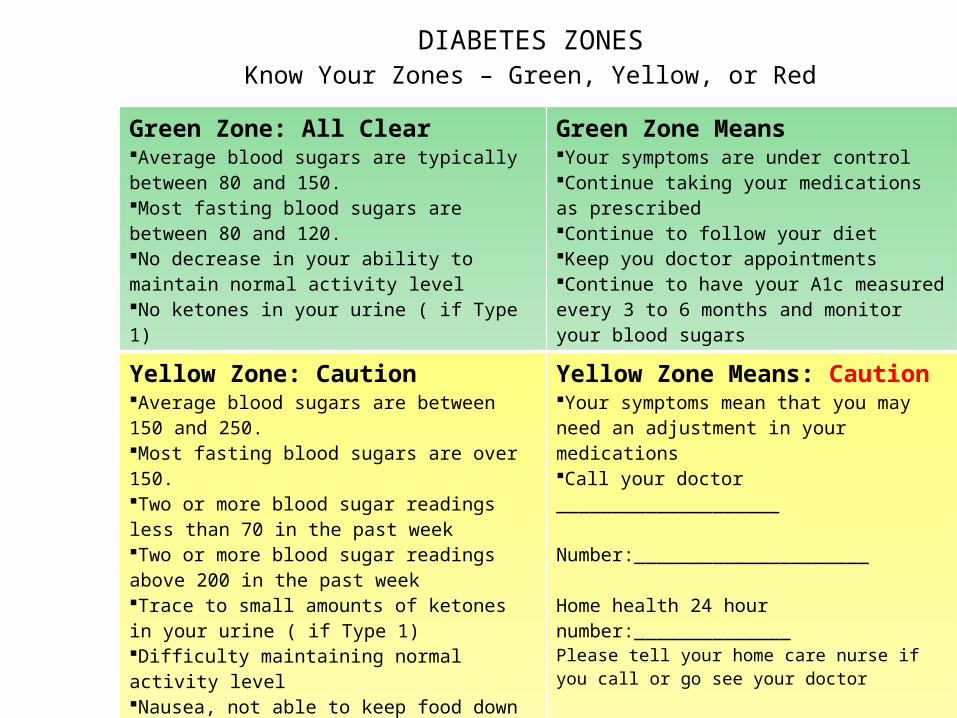
DIABETES ZONESKnow Your Zones – Green, Yellow, or Red
Green Zone: All ClearAverage blood sugars are typically between 80 and 150.Most fasting blood sugars are between 80 and 120.No decrease in your ability to maintain normal activity levelNo ketones in your urine ( if Type 1)
Green Zone MeansYour symptoms are under controlContinue taking your medications as prescribedContinue to follow your dietKeep you doctor appointmentsContinue to have your A1c measured every 3 to 6 months and monitor your blood sugars
Yellow Zone: CautionAverage blood sugars are between 150 and 250.Most fasting blood sugars are over 150.Two or more blood sugar readings less than 70 in the past week Two or more blood sugar readings above 200 in the past weekTrace to small amounts of ketones in your urine ( if Type 1)Difficulty maintaining normal activity levelNausea, not able to keep food down or eat normally
Yellow Zone Means: CautionYour symptoms mean that you may need an adjustment in your medicationsCall your doctor ____________________ Number:_____________________ Home health 24 hour number:______________Please tell your home care nurse if you call or go see your doctor
RED ZONE: Medical AlertAverage blood sugars are above 250.Most fasting blood sugars are over 200Two or more events in the past week when blood sugar was less than 60.You are unable to stay awake even during the dayIndividual is not responsive, has passed out
RED ZONE MEANS: EmergencyThis indicates that you need to be evaluated by a doctor right away – NOW!Name:_________________________Number:_______________________Call 911: if individual is unresponsive

PNEUMONIA ZONESKnow your zone: Green, Yellow, or Red
Green Zone: All Clear Having slight to no shortness of breath Temperature below 100 Slight cough No chest pain You are able to drink liquids and eat normally
Green Zone Means Your infection is being treated The medications are working that helps fight the infection Increase your activities slowly; it may take several weeks
before you feel normal. Make sure to go to your doctor as directed
Yellow Zone: Caution Fever over 101 Have an increase in shortness of breath Have an increase in coughing Your sputum changes color You are not taking in liquids Feeling more tired than when you were in the hospital
Yellow Zone Means: Warning You may need to adjust your medications Call your doctor to discuss your symptoms
Doctor: ___________________________Phone: _________________________
Call your Home Care Nurse 24 hour number___________________________
RED ZONE: MEDICAL ALERT Very difficult time breathing Your breathing does not get any better if you sit or lay
down Having chest pain Feeling more confused or having trouble thinking Coughing up blood
RED ZONE Means: Emergency You need to be seen by a doctor NOW! Call 911 or go to the nearest Emergency
room.

Resources
• HRET’s Preventable Readmissions http://hret-hen.org/preventable-readmissions
• State Action on Avoidable Rehospitalizations (STAAR) Initiative, http://www.ihi.org/IHI/Programs/StrategicInitiatives/STateActiononAvoidableRehospitalizationsSTAAR.htm
• Project RED (Re-Engineered DC) http://www.bu.edu/fammed/projectred/index.htlm Brian Jack, MD
• Project BOOST (Better Outcomes for Older adults through Safe Transitions) http://www.hospitalmedicine.org/ResourceRoomRedesign/RR_CareTransitions/CT_Home.cfm Mark Williams, MD, FHM
Resources
• Transitional Care Model http://www.transitionalcare.info Mary D. Naylor, PhD, RN, FAAN
• Patient Activation Measure http://www.insigniahealth.com/solutions/patient-activation-measure
• INTERACT II http://www.interact2.net/• Hospital 2 Home sponsored by the American College of
Cardiology and the Institute for Healthcare Improvement http://www.h2hquality.org/

Finding and Reducing ADEsCheryl Ruble, MS, RN, CNS
Montana Regional Meetings – Barrett Memorial Hospital
Dillion, MT

What is an ADE?

What is an ADE?
• Any injury resulting from medical care involving medication use.
AHRQ
But be careful…..
• The occurrence of an ADE does not necessarily indicate an error or poor quality of care
AHRQ

What is a Medication Error?

What is a Medication Error?
• Any error occurring in the medication use process
ISMP
So how is an ADE and a Med Error Different?
Well what is An ADR?
WHO:“Any response to a drug which is noxious and unintended, and which occurs at doses normally used in man for prophylaxis, diagnosis, or therapy of disease, or for the modification of physiological function.”
• All ADRs are ADEs• All ADEs are not necessarily ADRs
ADRsAll ADEs

So how is an ADE and a Med Error Different?
Adverse Drug Event
Medication Error
Med ErrorADE BOTH

Why do we care?
• Harm and Death>770,000 patients per year
• CostsUp to $5.6M per hospital annuallyUp to $32,000 per patient
AHRQ

So what is an ADE again?
• Any injury resulting from medical care involving medication use.
AHRQ

What do they look like?

What do they look like?

How do we find them?

How do we find them?
• Voluntary reports• Triggers• RCA’s• Electronic data
mining from EMR’s

Voluntary Reports
• Does it work?• Why?• Why not?
The key…
• Make it SAFE• Make it EASY• Make it MEANINGFUL
Triggers
• Does it work?• Why?• Why not?
CLUES

How Did We Get Started?
• RRT’s & ICU nursing staff tipped us off • All RRT’s reviewed by the Critical Care CNS• Large portion were respiratory in nature and required
transfer to ICU• Causative factor – over use of sedatives & analgesics
in post-op patients
• Of note – these were not found in occurrence reports
What Did We Test?
• Revision of work flow & assessment of patient readiness for discharge from PACU to floor.
• ICU, PACU, and ortho unit nurses involved

What’s Our Data Show?
• We virtually eliminated RRTs due to over sedation/ analgesic use post recovery.
• It became a rare event.

What Did We Learn?
• Communication between departments is crucial
• Not about the who but how – at first there was finger pointing between department staff
• Led us to think what about other rescue meds?

Rescue Meds
Other Triggers

Key Tips
• Always involve staff to identify the problem, design a solution, test and implement.
• Use what you have – – RRT forms/audits, – automated medication dispensing reports – use of rescue
meds– Use other reports such as blood product usage
• Consider unanticipated pulls from your automated medication dispensing

RCA’s
• Does it work?• Why?• Why not?
Mining EMR’s
• Does it work?• Why?• Why not?
Lab & Pharmacy Data
• How do you get it?• Does it work?• Why?• Why not?

What do we do with them when we find them?
• Aggregate• Analyze• Look for system
defects• Fix the system
• We are about what and how not who

Reduce harm from ADEs due to high-alert
medications (HAMs)
Awareness, Readiness &
Education
Use the ISMP Assessment tool to
assess capacity
Create awareness of HAMs
Assess clinical knowledge
Standardize Care Processes
Implement quarterly ISMP action agenda
Develop standard order sets
Allow nurses to administer rescue drugs per protocol
Sequence implementation by
drug class
AIM Primary Driver Secondary Drivers

Reduce harm from ADEs due to high-alert medications (HAMs)
Avoid errors during care transitions
Implement effective med rec processes
Where appropriate, create outpt clinics
for HAM f/up
Use flow sheets that follow pt through care
New insulin orders from parenteral to
enteral
Decision Support
Include pharmacist on rounds
Use alerts for dosage limits
Monitor overlapping meds given to a patient
Use alerts to avoid multiple
narcotics/sedatives
Double checks by pharmacy and
nursing
AIM Primary Driver Secondary Drivers
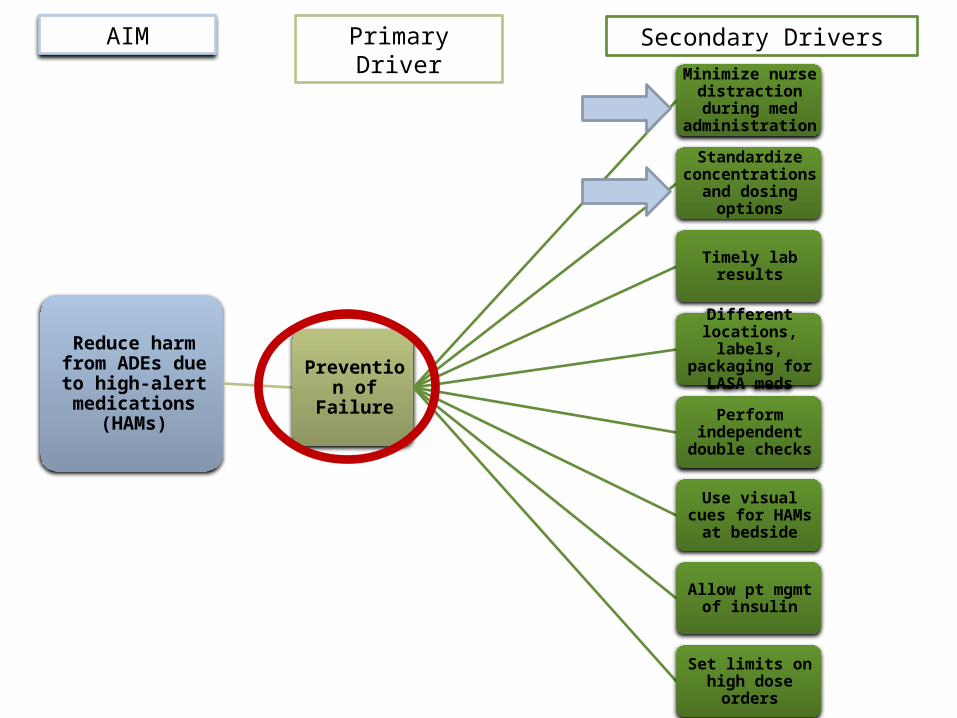
Reduce harm from ADEs due to high-alert medications
(HAMs)
Prevention of Failure
Minimize nurse distraction during
med administration
Standardize concentrations and
dosing options
Timely lab results
Different locations, labels, packaging for
LASA meds
Perform independent double
checks
Use visual cues for HAMs at bedside
Allow pt mgmt of insulin
Set limits on high dose orders
AIM Primary Driver Secondary Drivers

Reduce harm from ADEs due to high-alert medications
(HAMs)
Prevention of Failure -
Continued
Prepackages Heparin infusion
Reduce the number of heparin
concentrations
Use of LMWH versus unfractionated
heparin
Automatic nutrition consults for pts on
warfarin
Use of table drug-to-drug conversion
doses
Use fall prevention programs
Use dosing limits
Prepackages Heparin infusion
AIM Primary Driver Secondary Drivers
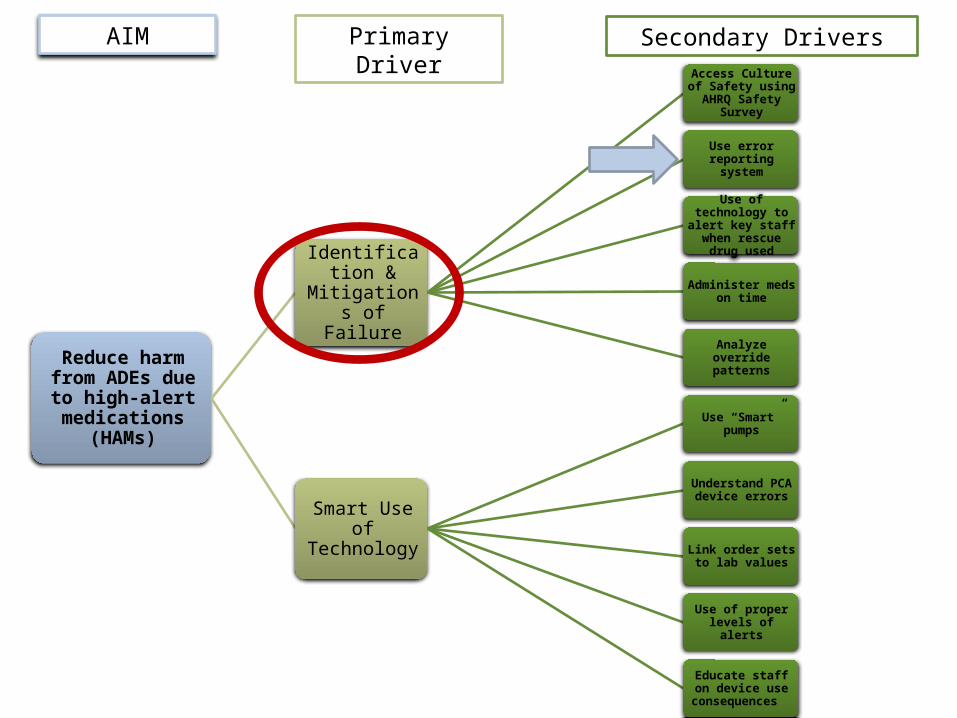
Reduce harm from ADEs due to high-alert medications
(HAMs)
Identification & Mitigations of
Failure
Access Culture of Safety using AHRQ
Safety Survey
Use error reporting system
Use of technology to alert key staff when
rescue drug used
Administer meds on time
Analyze override patterns
Smart Use of Technology
Use “Smart” pumps
Understand PCA device errors
Link order sets to lab values
Use of proper levels of alerts
Educate staff on device use
consequences
AIM Primary Driver Secondary Drivers
Awareness, Readiness, Education, Standard Care Processes
• Getting Started: – Is the organization
ready?– Does the organization
have the capacity?– Is the organization
willing?
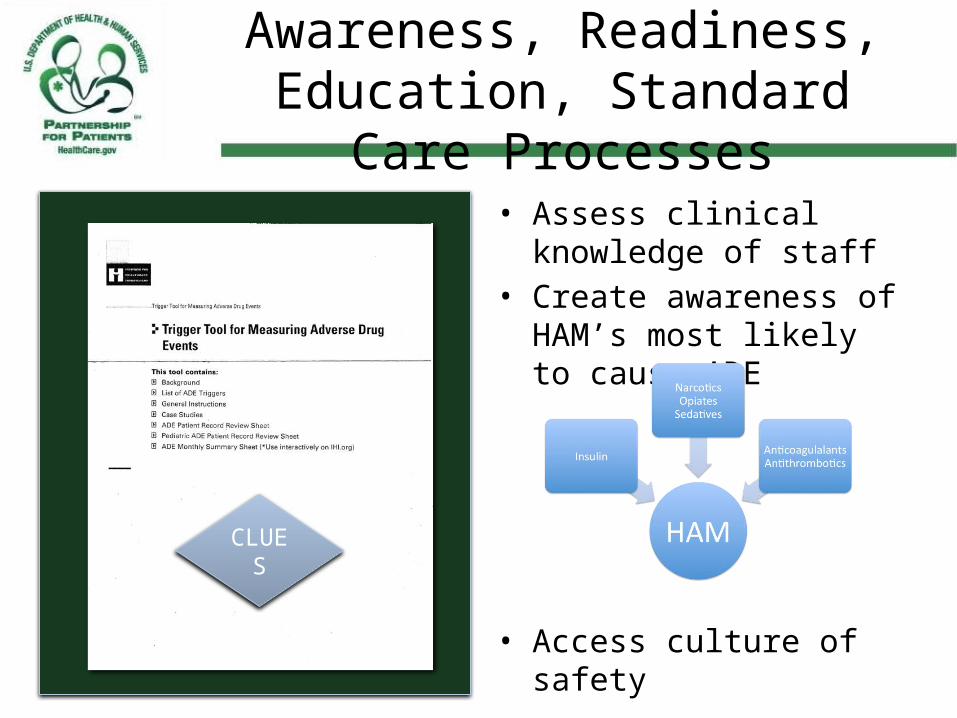
Awareness, Readiness, Education, Standard Care Processes
• Assess clinical knowledge of staff
• Create awareness of HAM’s most likely to cause ADE
• Access culture of safety
CLUES
Driver: Standardize the Care Process
“If you can’t describe your process, you don’t have one.” W. Edwards Deming
“Every system is perfectly designed to get the results it gets.”Paul Batalden, Dartmouth
“Standardize what is standardizable and no more”Brent James, MD, Intermountain Health
“Quality is the absence of unexplained variation.”David Nash, MD, Editor, American Journal of Medical Quality
Protocols
• Standard order sets for high priority HAMs– Start with the drug class
with greatest opportunity
• Nurse administered rescue drugs
• Allow for “opt out”• Make it easy to use
What does it have to do with readmissions?
• In one study 1 of 8 readmissions was due to an ADE
• Note…if we eliminated those we would be 60% of the way to our goal of a 20% reduction in readmissions
• Causes:– Failure to monitor– Drug- Drug interactions
Guharoy, 2007

Avoid Errors During Care Transitions

How can we prevent discharge related ADE’s that lead to
readmissions?

How?• Get the meds right!• Monitor meds• Minimize drug-drug
interactions• Reconciliation• Did the patient really
get the outpatient rx’s filled:– PA’s approved– affordable

What matters most?
• Checking out the patient 24-28 hours post discharge to see that they are completely reconciled…that all issues related to med rec are resolved
The Pill Mill
Dr. Suess’ You’re Only Old Once! A Book for Obsolete Children

How do we do that?
• Call them• Visit them• Have them visit
you

Driver: Prevention of Failure
• Medication errors are the most frequent cause of ADEs
• It goes beyond the mind numbing recitation of the 5 rights – right med, right patient, right dose, right time, right route
• System design in crucial! Set the clinician up for success!





NOT DISTURB
MED ERROR
REDUCTION ZONE
DO NOT D
ISTURB
DO NOT DISTURB
Driver: Identification & Mitigation of Failure
• Prompt identification and actions to reduce harm
• Understanding failure and taking broad system view is crucial
• Opportunities for learning and system re-dsign

Culture of SafetyDo you have a non-punitive environment?


Aoccdrnig to rschearch at Cmabrigde Uinervtisy, it deosn’t mttaer in what oredr the ltteers in a word are, the olny iprmoetnt tihng is that the frist and lsat ltteer be at the rghit pclae. The rset can be a total mses and you can still raed it wouthit a porbelm. This is bcuseae the huamn mnid deos not raed ervey lteter by istlef, but the word as a wlohe.
Amzanig huh?
The Human Mind

Resources
• 2011 Institute for Safe Medication Practices (ISMP) Medication Safety Self Assessment® for Hospitals http://ismp.org/selfassessments/Hospital/2011/pdfs.asp
• Institute for Healthcare Improvement High-Alert Medication Safety (Improvement Map)
• http://app.ihi.org/imap/tool/#Process=b8541097-7456-4aab-a885-38c31950e6bf• http://www.cshp.org/uploads/file/Shared%20Resources/2012/guideline_anticoag
ulants_2.21.12.pdf• Federico, Preventing Harm from High-Alert Medications, The Joint Commission
Journal on Quality and Patient Safety, 33(9), 537-542• Agency for Healthcare Research and Quality Hospital Survey on Patient Safety
Culture http://www.ahrq.gov/qual/patientsafetyculture/hospsurvindex.htm• Miller et al, Bar code Medication Administration Technology: Charcterization of
High-Alert Medication Triggers and Clinician Workarounds, The Annals of Pharmacotherapy 2011 Feb Vol 45, 162-168