
Recurrent Auricular Keloids during Pregnancy - e APS · Recurrent Auricular Keloids during...
3
70 Recurrent Auricular Keloids during Pregnancy Hyung-Do Kim, So-Min Hwang, Kwang-Ryeol Lim, Yong-Hui Jung, Sung-Min Ahn, Jennifer Kim Song Department of Plastic and Reconstructive Surgery, Good Moonhwa Hospital, Busan, Korea Correspondence: So-Min Hwang Department of Plastic and Reconstructive Surgery, Good Moonhwa Hospital, 119 Beomil-ro, Dong-gu, Busan 601-803, Korea Tel: +82-51-630-0199, Fax: +82-51-630-0145 E-mail: [email protected] No potential conflict of interest relevant to this article was reported. Received: 11 May 2012 • Revised: 5 Oct 2012 • Accepted: 6 Oct 2012 pISSN: 2234-6163 • eISSN: 2234-6171 http://dx.doi.org/10.5999/aps.2013.40.1.70 • Arch Plast Surg 2013;40:70-72 Copyright 2013 The Korean Society of Plastic and Reconstructive Surgeons This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. A keloid is one of the most frustrating clinical problems in wound healing. Keloids form following dermal injury and exhibit exuberant and indefinite growth of collagen. Many theories have been pro- pounded in trying to explain some of the vagaries of keloids. From one of the theories, keloid scars may develop at any age; patients between 10 and 30 years of age (reproductive age) are the most affected population, and there may be a hormonal influence because keloid scars tend to grow during puberty and pregnancy, and resolve during menopause [1]. In our experience, pregnancy-related recurrent keloids have arisen from the ear, despite the patient’s successful completion of our treatment. e case presented here illustrates the possible connection between keloid formation and hormonal changes during pregnancy. A 27-year-old pregnant female visited our clinic due to progressive growth of her leſt auricular keloid. ree years prior to the visit, she had developed a scar on her leſt auricle aſter treatment for acute inflam- mation caused by an ear piercing procedure at a non- medical institute. She showed no other particular medical history. She also reported that the lesions appeared and became larger aſter the first trimester of pregnancy (Fig. 1). On physical examination, the leſt auricle showed a keloid of nearly circular appearance, approximately 2.2 cm in diameter, with a mean thick- ness of about 1.5 cm, extending from the superior pole of the auricle down to the middle ear. e skin surface of the keloid was irregular and showed dis- persed minute superficial ulcer with itching sensation. Because of pregnancy, we waited to perform a core extirpation of the keloid until 6 months aſter delivery. Compression on the auricle was performed post- operatively in combination with the application of scar care ointment. Even aſter 1 month, the clinical result remained obviously acceptable where the core extirpation had been performed. Two years later, the patient returned with a huge enlargement of the leſt auricular keloid. Similar to the previous keloid, it appeared and became bigger (2.2 × 1.7 cm) simultaneously with child bearing. She remembered that the keloid started to enlarge rapidly in her first trimester of her second pregnancy, with mild itching and redness. She was asked to return aſter her delivery (Fig. 2). Fig. 1. Preoperative photo showing a keloid after the first pregnancy. Fig. 2. Preoperative photo showing a keloid after the second pregnancy. Images
Transcript of Recurrent Auricular Keloids during Pregnancy - e APS · Recurrent Auricular Keloids during...
70
Recurrent Auricular Keloids during PregnancyHyung-Do Kim, So-Min Hwang, Kwang-Ryeol Lim, Yong-Hui Jung, Sung-Min Ahn, Jennifer Kim SongDepartment of Plastic and Reconstructive Surgery, Good Moonhwa Hospital, Busan, Korea
Correspondence: So-Min HwangDepartment of Plastic and Reconstructive Surgery, Good Moonhwa Hospital, 119 Beomil-ro, Dong-gu, Busan 601-803, KoreaTel: +82-51-630-0199, Fax: +82-51-630-0145E-mail: [email protected]
No potential conflict of interest relevant to this article was reported.
Received: 11 May 2012 • Revised: 5 Oct 2012 • Accepted: 6 Oct 2012pISSN: 2234-6163 • eISSN: 2234-6171http://dx.doi.org/10.5999/aps.2013.40.1.70 • Arch Plast Surg 2013;40:70-72
Copyright 2013 The Korean Society of Plastic and Reconstructive SurgeonsThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
A keloid is one of the most frustrating clinical problems in wound healing. Keloids form following dermal injury and exhibit exuberant and indefinite growth of collagen. Many theories have been pro- pounded in trying to explain some of the vagaries of keloids. From one of the theories, keloid scars may develop at any age; patients between 10 and 30 years of age (reproductive age) are the most affected population, and there may be a hormonal influence because keloid scars tend to grow during puberty and pregnancy, and resolve during menopause [1]. In our experience, pregnancy-related recurrent keloids have arisen from the ear, despite the patient’s successful
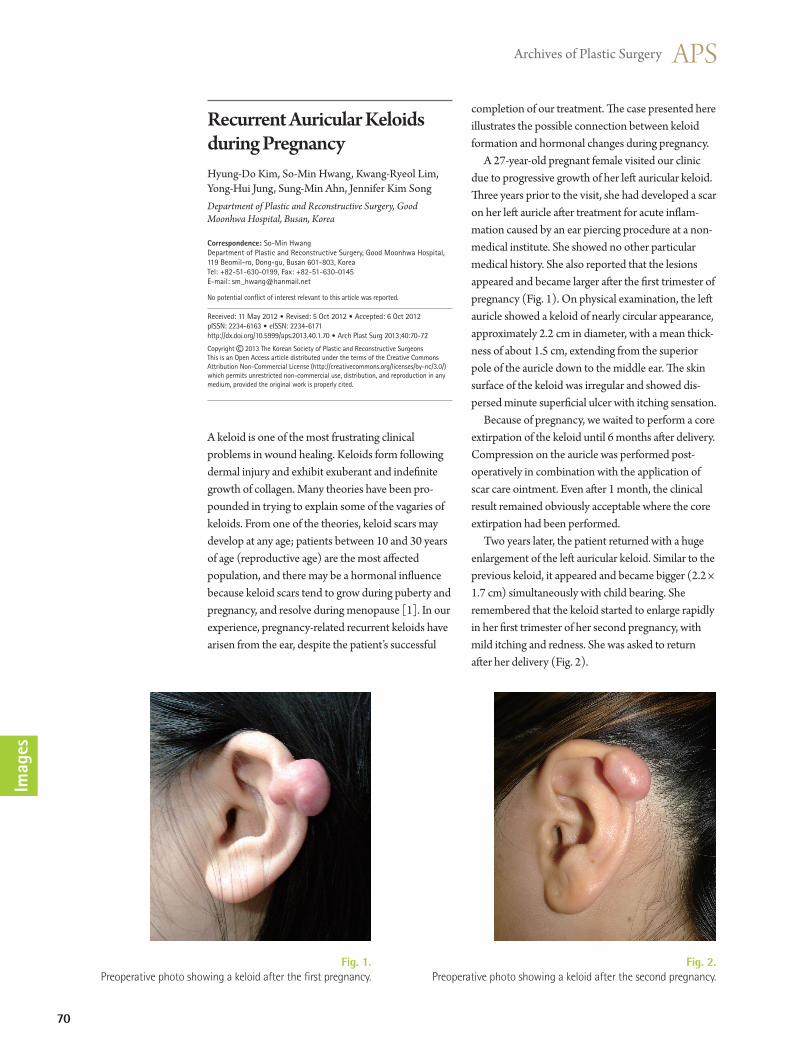
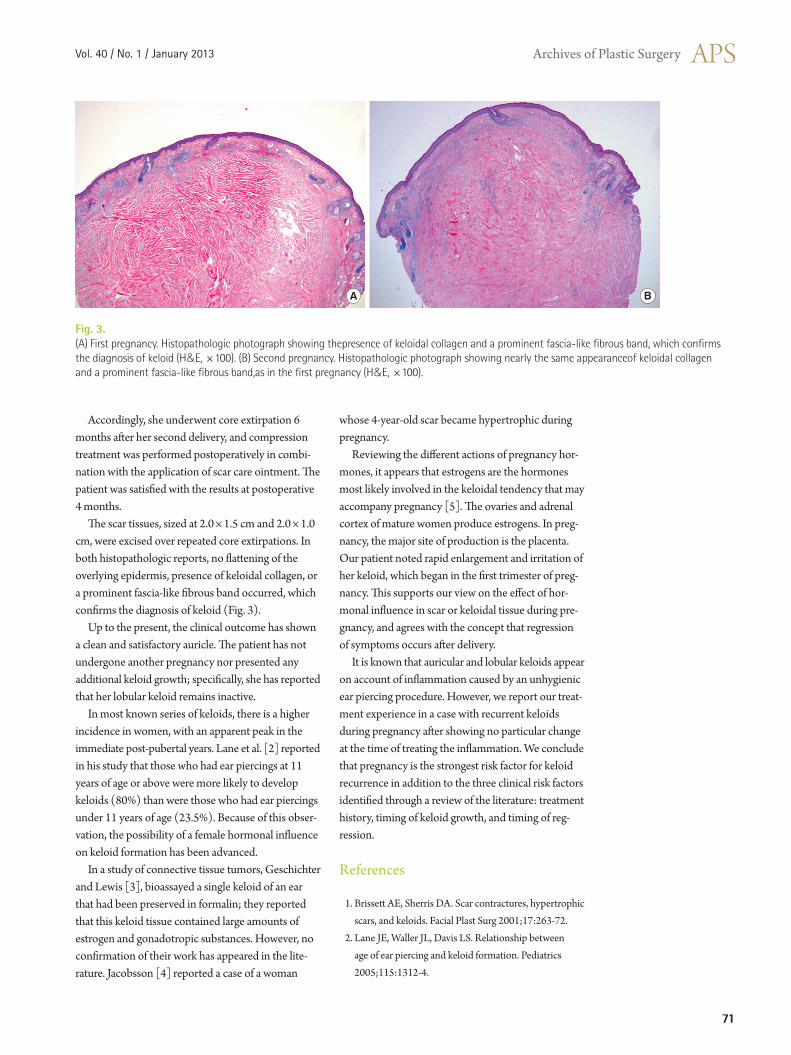
completion of our treatment. The case presented here illustrates the possible connection between keloid formation and hormonal changes during pregnancy. A 27-year-old pregnant female visited our clinic due to progressive growth of her left auricular keloid. Three years prior to the visit, she had developed a scar on her left auricle after treatment for acute inflam- mation caused by an ear piercing procedure at a non-medical institute. She showed no other particular medical history. She also reported that the lesions appeared and became larger after the first trimester of pregnancy (Fig. 1). On physical examination, the left auricle showed a keloid of nearly circular appearance, approximately 2.2 cm in diameter, with a mean thick- ness of about 1.5 cm, extending from the superior pole of the auricle down to the middle ear. The skin surface of the keloid was irregular and showed dis- persed minute superficial ulcer with itching sensation. Because of pregnancy, we waited to perform a core extirpation of the keloid until 6 months after delivery. Compression on the auricle was performed post- operatively in combination with the application of scar care ointment. Even after 1 month, the clinical result remained obviously acceptable where the core extirpation had been performed. Two years later, the patient returned with a huge enlargement of the left auricular keloid. Similar to the previous keloid, it appeared and became bigger (2.2 × 1.7 cm) simultaneously with child bearing. She remembered that the keloid started to enlarge rapidly in her first trimester of her second pregnancy, with mild itching and redness. She was asked to return after her delivery (Fig. 2).
Fig. 1. Preoperative photo showing a keloid after the first pregnancy.
Fig. 2. Preoperative photo showing a keloid after the second pregnancy.
Imag
es
Vol. 40 / No. 1 / January 2013
71
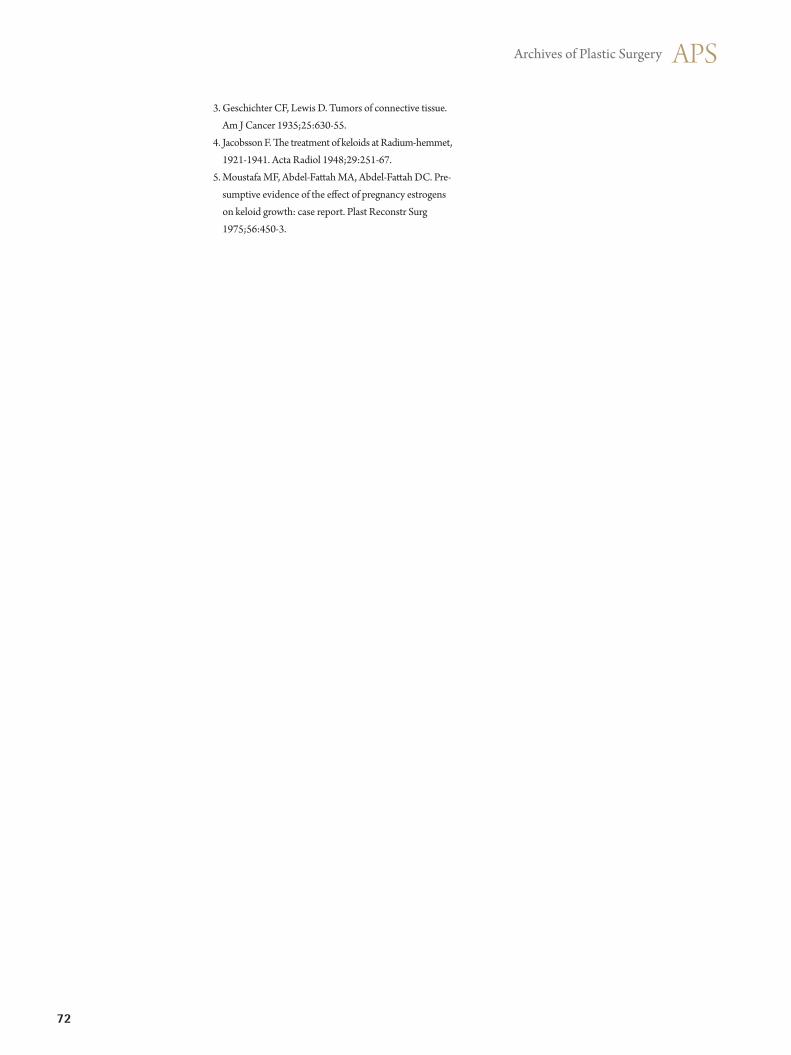
Accordingly, she underwent core extirpation 6 months after her second delivery, and compression treatment was performed postoperatively in combi- nation with the application of scar care ointment. The patient was satisfied with the results at postoperative 4 months. The scar tissues, sized at 2.0 × 1.5 cm and 2.0 × 1.0 cm, were excised over repeated core extirpations. In both histopathologic reports, no flattening of the overlying epidermis, presence of keloidal collagen, or a prominent fascia-like fibrous band occurred, which confirms the diagnosis of keloid (Fig. 3). Up to the present, the clinical outcome has shown a clean and satisfactory auricle. The patient has not undergone another pregnancy nor presented any additional keloid growth; specifically, she has reported that her lobular keloid remains inactive. In most known series of keloids, there is a higher incidence in women, with an apparent peak in the immediate post-pubertal years. Lane et al. [2] reported in his study that those who had ear piercings at 11 years of age or above were more likely to develop keloids (80%) than were those who had ear piercings under 11 years of age (23.5%). Because of this obser- vation, the possibility of a female hormonal influence on keloid formation has been advanced. In a study of connective tissue tumors, Geschichter and Lewis [3], bioassayed a single keloid of an ear that had been preserved in formalin; they reported that this keloid tissue contained large amounts of estrogen and gonadotropic substances. However, no confirmation of their work has appeared in the lite- rature. Jacobsson [4] reported a case of a woman
whose 4-year-old scar became hypertrophic during pregnancy. Reviewing the different actions of pregnancy hor- mones, it appears that estrogens are the hormones most likely involved in the keloidal tendency that may accompany pregnancy [5]. The ovaries and adrenal cortex of mature women produce estrogens. In preg- nancy, the major site of production is the placenta. Our patient noted rapid enlargement and irritation of her keloid, which began in the first trimester of preg- nancy. This supports our view on the effect of hor- monal influence in scar or keloidal tissue during pre- gnancy, and agrees with the concept that regression of symptoms occurs after delivery. It is known that auricular and lobular keloids appear on account of inflammation caused by an unhygienic ear piercing procedure. However, we report our treat- ment experience in a case with recurrent keloids during pregnancy after showing no particular change at the time of treating the inflammation. We conclude that pregnancy is the strongest risk factor for keloid recurrence in addition to the three clinical risk factors identified through a review of the literature: treatment history, timing of keloid growth, and timing of reg- ression. References
1. Brissett AE, Sherris DA. Scar contractures, hypertrophic scars, and keloids. Facial Plast Surg 2001;17:263-72.
2. Lane JE, Waller JL, Davis LS. Relationship between age of ear piercing and keloid formation. Pediatrics 2005;115:1312-4.
Fig. 3. (A) First pregnancy. Histopathologic photograph showing thepresence of keloidal collagen and a prominent fascia-like fibrous band, which confirms the diagnosis of keloid (H&E, ×100). (B) Second pregnancy. Histopathologic photograph showing nearly the same appearanceof keloidal collagen and a prominent fascia-like fibrous band,as in the first pregnancy (H&E, ×100).
A B
72
Fig. 1. Preoperative photograph of case 1. The defect size was 17×12 cm. Both
the testes and anal sphincter were exposed.
3. Geschichter CF, Lewis D. Tumors of connective tissue. Am J Cancer 1935;25:630-55.
4. Jacobsson F. The treatment of keloids at Radium-hemmet, 1921-1941. Acta Radiol 1948;29:251-67.
5. Moustafa MF, Abdel-Fattah MA, Abdel-Fattah DC. Pre- sumptive evidence of the effect of pregnancy estrogens on keloid growth: case report. Plast Reconstr Surg 1975;56:450-3.
There are many reasons for skin defects of the peri- neoscrotal area. These defects can result from severe
Reconstruction of a Perineoscrotal Defect Using Bilateral Medial Thigh Fasciocutaneous FlapsJihoon Yang, Sung Hoon Ko, Suk Joon Oh, Sung Won JungDepartment of Plastic and Reconstructive Surgery, Hallym University Sacred Heart Hospital, Hallym University Medical Center, Anyang, Korea
Correspondence: Sung Hoon Ko Department of Plastic and Reconstructive Surgery, Hallym University Sacred Heart Hospital, Hallym University Medical Center, 22 Gwanpyeong-ro 170beon-gil, Donan-gu, Anyang 431-070, Korea Tel: +82-31-380-3781, Fax: +82-31-380-5980E-mail: [email protected]
No potential conflict of interest relevant to this article was reported.
Received: 31 Aug 2012 • Revised: 6 Oct 2012 • Accepted: 7 Oct 2012pISSN: 2234-6163 • eISSN: 2234-6171http://dx.doi.org/10.5999/aps.2013.40.1.72 • Arch Plast Surg 2013;40:72-74
Copyright 2013 The Korean Society of Plastic and Reconstructive SurgeonsThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
infection with gangrene and loss of the covering skin. Traumatic avulsions of the scrotal and penile skin are commonly caused by clothing being caught in revolv- ing machinery, automobile versus pedestrian accidents, falls, rare bull-horn avulsion injuries, the excision of scrotal skin diseases and genital burns [1]. Pressure sores of the ischial region have been treated with muscles and skin of the medial part of the thigh. Hirshowitz and Peretz [2] introduced superomedial thigh flaps in the reconstruction of the scrotum and vulva in 1982. We present two cases using medial thigh fasciocutaneous flaps in the reconstruction of wide skin defects of the perineoscrotal area. The operations were performed under general anesthesia and in the lithotomy position. We first used a Doppler sonogram to mark the external pudendal, superficial femoral, and medial circumflex femoral arteries at the area 5 cm lateral to the pubic tubercle. Then, a triangular flap was designed. A line was drawn extending from the pubic tubercle to the insertion area of the semiten- dinosus tendon. The anterior border of the flap may lie a centimeter or so anterior to this line. A triangular flap 9 cm in width can be safely elevated distally 20 cm along that border [3]. Dissection begins distally to identify the deep fascia, which must be included with the flap. To preserve the main pedicles, surgeons must not dissect near a line 5 cm lateral to pubic tubercle. After avoiding the loss of septocutaneous perforators in the dissection, the flap, including the fascia, was raised from the distal aspect, advanced cephalad and rotated medially toward the inguinal canal using the pedicles of the three arteries as a pivot point. Superficial subcutaneous tissues and veins may be included in the pedicle if they do not prevent flap mobilization [4]. Then, the distal end of the flap was rotated toward the anus, and the posterior end of the flap was rotated toward the penis. After
Imag
es







![fibrilacion auricular[1]](https://static.fdocuments.in/doc/165x107/577d2baa1a28ab4e1eab09b6/fibrilacion-auricular1.jpg)










