Rectal cancer: Extent of disease and radiotherapeutic effects by computed tomography
6
Corqxrtrri.-r,d Radio/. Vol. 7. No. 4. pp. 209-214, 1983 0730-4862/U $3.00 +O.OO Printed in the U.S.A. All rights reserved Copyright 0 Pergamon Press Ltd RECTAL CANCER: EXTENT OF DISEASE AND RADIOTHERAPEUTIC EFFECTS BY COMPUTED TOMOGRAPHY MIRIAM SPERBER’, GERALD J. MARKS’, MOHAMMED MOHIUDDIN~ and ESMOND MAPP’ ‘Department of Radiology, ‘Department of Surgery and 3Department of Radiation Therapy, Thomas Jefferson University Hospital, Philadelphia, PA 19107. U.S.A. Abstract-The CT scans of 54 patients with carcinoma of the rectum were studied in an attempt to assess the value of computed tomography in the initial evaluation and therapeutic management of these patients. Thirty-five of the examined patients received full dose preoperative radiation therapy for sphincter preserva- tion purposes, and had two or more computed tomography studies to delineate the progression of the disease and the response to radiotherapy. In 70”4 of these patients, changes in tumor size were demon- strated. Various aspects in the CT diagnosis of the primary or recurrent tumor extent. distant metastatic spread or involvement of surrounding tissues are discussed. Rectum, computed tomography Rectal neoplasm, radiotherapy Rectal cancer, computed tomography INTRODUCTION In patients with carcinoma of the rectum, despite the capability of the clinical examination, endos- copy and conventional radiology techniques, preoperative staging and evaluation are often unsatis- factory. Certain rectal cancers do not require radical surgical treatment. In others, marked palliative and occasional curative results are obtained by radiation therapy or by combining irradiation with surgical measures. The difficult pivotal element of proper patient selection for these various treat- ment modalities remains an accurate preoperative staging, as well as early recognition of recurrency or post-irradiation changes. In the continuous quest for improved methods of pretherapeutic evaluation, several reports have tried over the past few years to define the role of computed tomography (CT) in the diagnosis of pelvic abnormalities [l, 3, 5, lo]. The present study, based on the investigation of 89 CT examinations of 54 patients with cancer of the rectum was undertaken in an effort to further assess the value of CT in the preoperative diagnosis and staging of rectal cancer, as well as to evaluate its use in the assessment of progression of the disease or response to therapy. METHODS AND MATERIALS Fifty-four patients with carcinoma of the rectum underwent CT scanning at our institution between November 1980 and April 1981. No selection was made when including the patients in this retrospective study. There were 29 men and 25 women, aged from 35 to 87 years. Thirty-five of them had two or more CT examinations. All studies were performed on a commercially available Pfizer 0200-FS scanner with a scanning time capability of 19 sec. Approximately 1 hr prior to scanning the patients ingested 1200 to 1600 ml of 15 : 1 mixture of water to Gastrografin and were injected 100 cc of Conray 60 intravenously, half an hour before scanning. In addition, the patients were given a contrast enema with 400 to 800 ml of a mixture of water and Gastrografin, as well as an intravenous injection of 15: 1 Glucagon (0.5 to 1 mg) to limit bowel peristalsis, immediately prior to scanning. Where possible, a tampon was inserted in the vagina in order to define this region by means of its low density. CT scanning was performed during suspended respiration, and 13-mm thick sections were taken at 1.5-cm intervals through the liver, mid and lower abdomen and through the pelvis. Images were obtained at varying window widths and levels. When necessary, suspicious areas were rescanned. 209
Transcript of Rectal cancer: Extent of disease and radiotherapeutic effects by computed tomography

Corqxrtrri.-r,d Radio/. Vol. 7. No. 4. pp. 209-214, 1983 0730-4862/U $3.00 +O.OO Printed in the U.S.A. All rights reserved Copyright 0 Pergamon Press Ltd
RECTAL CANCER: EXTENT OF DISEASE AND RADIOTHERAPEUTIC EFFECTS BY
COMPUTED TOMOGRAPHY
MIRIAM SPERBER’, GERALD J. MARKS’, MOHAMMED MOHIUDDIN~ and ESMOND MAPP’
‘Department of Radiology, ‘Department of Surgery and 3Department of Radiation Therapy, Thomas Jefferson University Hospital, Philadelphia, PA 19107. U.S.A.
Abstract-The CT scans of 54 patients with carcinoma of the rectum were studied in an attempt to assess the value of computed tomography in the initial evaluation and therapeutic management of these patients. Thirty-five of the examined patients received full dose preoperative radiation therapy for sphincter preserva- tion purposes, and had two or more computed tomography studies to delineate the progression of the disease and the response to radiotherapy. In 70”4 of these patients, changes in tumor size were demon- strated. Various aspects in the CT diagnosis of the primary or recurrent tumor extent. distant metastatic spread or involvement of surrounding tissues are discussed.
Rectum, computed tomography Rectal neoplasm, radiotherapy Rectal cancer, computed tomography
INTRODUCTION
In patients with carcinoma of the rectum, despite the capability of the clinical examination, endos- copy and conventional radiology techniques, preoperative staging and evaluation are often unsatis- factory.
Certain rectal cancers do not require radical surgical treatment. In others, marked palliative and occasional curative results are obtained by radiation therapy or by combining irradiation with surgical measures. The difficult pivotal element of proper patient selection for these various treat- ment modalities remains an accurate preoperative staging, as well as early recognition of recurrency or post-irradiation changes.
In the continuous quest for improved methods of pretherapeutic evaluation, several reports have tried over the past few years to define the role of computed tomography (CT) in the diagnosis of pelvic abnormalities [l, 3, 5, lo].
The present study, based on the investigation of 89 CT examinations of 54 patients with cancer of the rectum was undertaken in an effort to further assess the value of CT in the preoperative diagnosis and staging of rectal cancer, as well as to evaluate its use in the assessment of progression of the disease or response to therapy.
METHODS AND MATERIALS
Fifty-four patients with carcinoma of the rectum underwent CT scanning at our institution between November 1980 and April 1981. No selection was made when including the patients in this retrospective study. There were 29 men and 25 women, aged from 35 to 87 years. Thirty-five of them had two or more CT examinations.
All studies were performed on a commercially available Pfizer 0200-FS scanner with a scanning time capability of 19 sec. Approximately 1 hr prior to scanning the patients ingested 1200 to 1600 ml of 15 : 1 mixture of water to Gastrografin and were injected 100 cc of Conray 60 intravenously, half an hour before scanning. In addition, the patients were given a contrast enema with 400 to 800 ml of a mixture of water and Gastrografin, as well as an intravenous injection of 15: 1 Glucagon (0.5 to 1 mg) to limit bowel peristalsis, immediately prior to scanning. Where possible, a tampon was inserted in the vagina in order to define this region by means of its low density.
CT scanning was performed during suspended respiration, and 13-mm thick sections were taken at 1.5-cm intervals through the liver, mid and lower abdomen and through the pelvis. Images were obtained at varying window widths and levels. When necessary, suspicious areas were rescanned.
209

(a) (b)
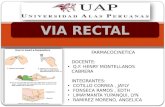
Fig I. (a) Adenocarcinoma demonstrated by soft tissue density projecting into the lumen of the rectum in the right antero-lateral wall. in a 54-yr-old man. There is no extension of tumor mass outside the lateral wall and fat planes appear to be preserved. (b) Postradiation CT scans of tumor seen in Fig. la. Repeat scan revealed concentric rectal wall thickening secondary to radiation. Diagnosed as submucosal fibrosis without
local defect or tumor.
RESULTS
Clinical appraisal of carcinoma of the rectum is based on careful digital examination, endoscopy and barium enema studies. As options of treatment include local surgical excision, extensive resection, or a combination of radiotherapy and surgery, the ability to accurately stage the cancer has a direct impact upon selecting the most adequate mode of primary treatment.
A morphologic change in the size and contour of the rectum may indicate the presence of rectal cancer (Fig. la). In the case of a sessile lesion, asymmetric wall thickening is observed and extention beyond the muscularis is defined by irregular or ill-defined margins. In the more advanced stages of the disease, perirectal masses can be seen replacing the normal perirectal fat (Fig. 2).
Mesenteric extension may be identified by masses or linear streak-like densities with lymphatic involvement. The involved lymph nodes appear larger than their 1 to 1.5 cm size. Invasion of the iliopsoas muscles may be seen unilaterally or bilaterally. In some cases, a pelvic mass is demon- strated as a round density, often presenting a central area of low attenuation and extending into adjacent organs such as the bladder or the ovary.
The CT scans included in our study were compared with the clinical findings, barium enema studies, and when possible with subsequent pathology specimens. For a better evaluation of the results, patients included into the survey were categorized in one of four groups, based on the indication for the initial study (Table 1).
Group I
Forty patients, presenting with a diversity of complaints including changes in bowel habits,
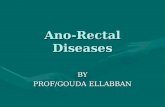
Fig. 2. lnvasiv’e adenocarcinoma of rectosigmoid, presenting as a mass which extends into perirectal area and bladder base. causing almost complete obstruction.

Rectal cancer and CT
Table 1. Classification of patients
211
No. of Group Indication for CT scan patients*
I II
III IV
Preoperative staging 40 Response to radiotherapy 35 Local recurrence 14 Distant metastases 10
* Multiple indications cause overlapping mto more than one classification.
bloody stools and abdominal pains and subsequently diagnosed as having a rectal mass, were included in the first group of our study and were scanned in an attempt to stage their disease by computed tomography.
Abnormalities on CT scans paralleled in most of the cases the pathological findings, demon- strating the ability of computed tomography to identify the size, shape and orientation of the rectum, with accurate location of tumoral masses, as well as pathology in the adjacent organs (lymph nodes, bladder, prostate, seminal vesicles, uterus, vagina and small bowel).
In 40% of the patients with stage B cancer computed tomography demonstrated lesions larger than clinically expected, the same as tumor extension into surrounding tissues in 52% of the patients with stage C cancer. In both groups, more than 60% of the patients had a change in their clinical management following the CT findings. The method did fail to diagnose two of our five cases with stage A cancer, most likely because of the small size of the tumor.
Group I1
Thirty-five patients received full dose preoperative radiation therapy for sphincter preservation purposes and had two or more CT studies in order to delineate the progression of the disease and the response to radiotherapy.
The amount of radiation received by these patients (4500 rad) was divided in 25 fractions over a period of approx 5 weeks. Post radiation responses and normal tissue effect in adjacent structures were monitored by consecutives CT scans.
In 70% of these patients, changes in tumor size were demonstrated, ranging from 40% regression to complete disappearance of local disease.
Most tumors have an attenuation value similar to other soft tissues (35 to 54 Ho), but in some instances it is difficult to distinguish a tumor from granulation tissue or postradiation fibrosis based on density measurements only. Recognition of tumor changes has to be based on the morphology of the mass and its relation to adjacent structures (muscles, viscera, lymph nodes).
CT has helped significantly in the evaluation and the surgical-radiotherapeutic management of these patients. Figure lb represents a repeat CT scan in a patient included in this study group and whose initial scan is shown in Fig. la. After a course of radiation therapy (4500rad) in 4$ weeks, only a concentric rectal wall thickening is visible, possible secondary to radiation, but no localized defect. The patient underwent combined abdomino-transsacral proctocolectomy and coloproctos- tomy. At the time of the operation a definite mass could not be palpated. An area of induration in the posterior wall of the rectum probably corresponded with the site of the previously treated cancer.
Table 2. CT staging accuracy compared to other preoperative methods
CT stage compared to other methods Stage at More Not Total surgery Same advanced diagnosed patients
A 3 0 2 5 B 6 4 0 10 C 1 10 0 17 D 5 3 0 8

212
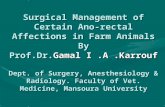
Fig. 3. Recurrent rectal mass extending presacrally with invasion of seminal vesicles and posterior bladder wall in a ho-yr-old man. 1 yr after combined abdominoperineal resection for rectal cancer.
Group III
CT was used in 14 patients who had undergone surgery for adenocarcinoma of the rectum, in an attempt to discover recurrent disease. One half of these patients had clinical and radiological evidence of recurrence and the CT scans were performed to determine the exact location and degree of tumor spread. The other half of the patients were scanned immediately after surgery in search for persistent disease.
An increasing number of reports reveal a marked palliative and occasional curative value of radiation in early detected rectosigmoid tumor recurrences [Z, 31. Even when pelvic recurrence is obvious, demonstrating the exact site and extent of the disease may be impossible by conventional techniques.
The postoperative pelvis can be remarkably difficult to evaluate, particularly in patients who have had an abdominoperineal resection. CT, however, was able to demonstrate a recurrent tumor mass and accurately delineate its extent in 10 of the 14 patients in this group (Fig. 3).
Group IV
While intra-abdominal organs and structures, e.g. adrenal glands or retroperitoneal lymph nodes, are inadequately visualized by other methods, CT facilitates visualization of these structures and pathology in these areas is easily defined. Secondary deposits, for example, in the liver or in the lungs can be demonstrated quite early.
In five of the eight patients included in the fourth group of our study, CT demonstrated the exact extent of clinically suggested metastatic disease. In the other three, more extensive pathology was discovered, including clinically unsuspected lung metastatic deposits, a mass in the right para-aortic region obstructing the inferior vena cava (Fig. 4) or bilateral hydronephrosis. Other abnormalities such as ascites, invasion of the iliopsoas muscles and an abdominal wall mass were demonstrated as well.
Fig. 4. A large metastatic lesion in the portal area causing obstruction of the inferior vcna cava. in a 67-yr-old woman presenting with lymphedema 11 months after surgery for rectal cancer.

Rectal cancer and CT 213
DISCUSSION
Although a number of diagnostic procedures are available for the initial diagnosis of the primary rectosigmoid carcinoma, it appears that CT provides a better delineation of the presenting rectal tumor and its extension into surrounding tissues, the same as it offers a more accurate and complete picture of multiple abnormalities.
While performing CT scanning special attention should be paid to the technique. The use of intravenous, oral and rectal contrast media is recommended, since the evaluation of pelvic pathol- ogy is made difficult by the similar attenuation values of pelvic organs, tumor masses, bowel loops or postoperative fibrotic changes. A great number of patients will prove to have disease outside the pelvis. Both pelvis and abdomen should be examined in such patients.
We find CT to be useful in the preoperative staging of patients with cancer of the rectum, with abnormalities in most of the cases, paralleling the pathological specifications and findings at surgery. Sequential studies have been used and proved to be helpful in monitoring radiotherapy effects, seeking in addition to tumor changes, early recognition of radiation morbidity due to treatment or local recurrence.
Despite radical surgery, cancer of the rectum still has a low survival rate [7]. As radiotherapy has been found to reduce tumor size and improve the chances of operability and survival [2,3,9], the routine use of CT in the initial evaluation of rectal cancer, in the treatment choice and in the follow-up of these patients appears to be justified.
SUMMARY
A review was made of 89 (CT) examinations of the pelvis and abdomen in 54 patients with carcinoma of the rectum obtained for evaluation of initial extent of disease or location of possible recurrence. CT demonstrated tumoral masses larger than clinically expected in 40”/, of the patients, tumor extension to surrounding tissues in 52’4, distant metastases in 3”j,, and evidence of disease in 10 of the 14 patients scanned for pelvic recurrence. The study indicates that computed tomography is effective for the diagnosis and initial evaluation of rectal carcinoma and supports the routine use of this method for surgical and radiotherapeutic planning.
REFERENCES
I. H. Brizel et al., Radiotherapeutic applications of pelvic computed tomography, J. Conlput. assisf. Tomogr. 3. 453 (1979). 2. C. E. Dukes, The classification of cancer of the rectum, J. Pathol. Boer. 35. 323 (1932). 3. L. Gunderson and A. Cohen, Residual, inoperable or recurrent colorectal cancer-interaction of surgery and radiotherapy,
Am. J. Surg. 139, 518 (1980). 4. L. Gunderson, Radiation therapy of colorectal cancer. In Digestioe Cancer, N. Thatcher. Ed., pp. 29-38. Proc. Int. Cancer
Cong. (1979). 5. J. E. Husband, et al. The use of computed tomography in recurrent rectal tumors, Radioloqv 134, 677 (1980). 6. B. Mayer and J. Zornoza, Computed tomography of colon carcinoma. .4/n. J. Radio!. 135.43 (1980). 7. M. Mohiuddin and R. R. Dobelbower, A selective sandwich technique of adiuvant radiotherapy in the treatment of rectal
cancer, Dis. Colon Rrctum 22 l-4 (1979). . .
8. R. C. Newland and P. H. Chapius. The relationship of survival to staging and grading of colorectal carcinoma. Cancer 47, 1424 (1981).
9. W. D. Rider and N. V. Hawkins, Radiation for the cure of rectal cancer, I!lt. J. Rad. OncoL. 4, 114 (1978). IO. J. Tirnado and M. A. Amendoba, Computed tomography of the perineum, Am. J. Radio/. 136. 475 (1981).
About the Author-MIRIAM SPERBER received the M.D. in 1972 from the Tel-Aviv University Medical School, Israel. In 1979, after completing residency program in Israel Diagnostic Radiology. Dr Sperber worked in London, England at the Royal Free and the University College Hospitals, being active in the field of Computed Tomography. Since November 1980, Dr Miriam Sperber joined the faculty of the Department of Radiology at Thomas Jefferson University Hospital, Philadelphia, PA. Here she initiated research projects evaluating the use of CT in conditions such as occupational lung diseases, abdominal malignancies, diffuse pulmonary disorders and others. Currently, Dr Sperber is editing a book covering multiple diagnostic aspects in pulmonary diseases with Computed Tomography.
About the Author-GERALD J. MARKS is Professor of Surgery at the Jefferson Medical College, Thomas Jefferson University Hospital; Consultant in Colorectal Surgery at the VA Hospitals in Coatesville, PA. Wilmington, DE, San Juan. PR; and Pennsvlvania Hosuital. Philadelnhia. Dr Marks is also President of the Societyof American Gastrointestinal Endoxopic Surgeons and Assdciate Editor of Diseases of the Colon and Rectum as well as Pennsylvania Medicine.

214 MIRIAM SPERBER rr (II.
About the Author-MOHAMMED MOHIUDDIN graduated from Osmania Medical College, India in 1968. He completed a residency program in Radiation Therapy at the Royal Marsden Hospital in London, England in 1975. Dr Mohiuddin is presently Professor and Chief, Clinical Division at the Department of Radiation Therapy and Nuclear Medicine, Thomas Jefferson University Hospital, Philadelphia, PA and Co-Chairman of the Subcommittee on Gastrointestinal Malignancies, Radiation Therapy Oncology Group. He is also Principal Investigator, for the Radiation Therapy Oncology Group.
About the Author-EsMoxD M. MAPP received his M.D. from Howard University College of Medicine in Washington, DC in 1958. He did an internship at the District of Columbia General Hospital Washington, DC followed by a 3-year residency in the Department of Radiology at the Graduate Hospital of the University of Pennsylvania, Philadelphia. Since 1977, Dr Mapp has been a member of the faculty of Thomas Jefferson University Hospital in the Department of Radiology.