Record card keeping, why bother, what can we learn, how do ...€¦ · Kingdom throughout the...
66
Are you practising legally? David Cartwright Chair, Derby/Notts local professional network Member, GOC hearing panel Chair, National Eye Health Week Non Exec Director, Nottingham Univ’ Hospital Suffolk LOC June 2015
Transcript of Record card keeping, why bother, what can we learn, how do ...€¦ · Kingdom throughout the...

Are you practising legally?
David Cartwright
Chair, Derby/Notts local professional network
Member, GOC hearing panel
Chair, National Eye Health Week
Non Exec Director, Nottingham Univ’ Hospital
Suffolk LOC June 2015

Objectives this evening
Understand the optical legal issues, that may affect
you.
Review the issues and risks that frequently arise.
Are there obvious learnings and actions to reduce
the risks?
Review illustrative examples.
Q&A.
Suffolk LOC June 2015

GOC professional conduct competencies
“The ability to comply with the legal, ethical and
professional aspects of practice”
2.2.3 Is able to work within the law and within the codes and
guidelines set by the regulator and the profession.
- Demonstrates knowledge of the advice and guidance set by the respective
professional body and standards set by their local PCT.
- Demonstrates knowledge of the code of conduct set down by the General
Optical Council.
- Demonstrates a knowledge of the relevant law relating to their role e.g.
Opticians Act, GOS benefits, fees and charges, Medicines Act
2.2.4 Creates and keeps full, clear, accurate and
contemporaneous records
Suffolk LOC June 2015

The regulation, codes & guidance
Civil action
Criminal, in our case The Opticians Act 1989 and subsequent
amendments
Codes of conduct for individual and business registrants
College & Association of British Dispensing Opticians
guidelines
Suffolk LOC June 2015

Other regulation
Contract law
NHS regulations
Data protection
Freedom of information
Insurances; employers liability, public insurance
Health and safety
Disability discrimination
(Refer to “Quality in Optometry”)
Suffolk LOC June 2015

Civil Action
Generally covers areas as contracts, negligence, family
matters, employment, probate and land law.
The patient has to show that we are negligent and there has
been damage as a result.
Usually taken out of our hands
Sometimes best to accept to avoid long legal process
Suffolk LOC June 2015

Opticians Act
Four main functions of GOC
Setting standards for optical education and
training, performance and conduct
Approve qualifications
Maintain the register
Investigate and act where registrants fitness to
practice, train or carry on business is impaired.
Suffolk LOC June 2015

Restrictions on sight tests, fitting CLs
The Act states only a registered optometrist or
medical practitioner can;
Test sight.
“duty to perform an examination of the external eye, an
intraocular examination and such additional examinations
that appear necessary”
“give a written statement re referral and the Rx”
Fit CLs
“must have a Rx from sight test less than 2 years old”
“give a signed specification, with expiry date”
Suffolk LOC June 2015

Restrictions on sale of appliances
Optical appliances, (spectacles and contact lenses),
can only be sold unless by or under the supervision
of a registrant. Exemptions are;
Unregistered dispensing to anyone over 16, not registered.
The seller must have a signed dated Rx within 2 years,
verify the Rx with a focimeter and that the OCs align with
the PD.
Ready mades.
Contact lenses, under general direction of a registrant.
Suffolk LOC June 2015

Titles
It is an offence under the Act for an individual
to take or use the titles of ophthalmic optician,
dispensing optician, optometrist, registered
optometrist or imply registration, when they
are not registered.
Suffolk LOC June 2015

GOC individual code of conduct
Suffolk LOC June 2015
As a registered optometrist, dispensing optician, or person undertaking
training as an optometrist or dispensing optician, you must:
1. Make the care of the patient your first and continuing concern;
2. Treat every patient politely and considerately;
3. Respect patients' dignity and privacy;
4. Listen to patients and respect their views;
5. Give patients information in a way they can understand and make them aware of
the options available
6. Maintain adequate patients' records;
7. Respect the rights of patients to be fully involved in decisions about their care;
8. Keep professional knowledge and skills up to date;
9. Recognise, and act within, the limits of your professional competence;
10. Be honest and trustworthy;

GOC individual code of conduct
Suffolk LOC June 2015
11. Ensure that financial and commercial practices do not compromise patient safety;
12. Respect and protect confidential information;
13. Make sure that personal beliefs do not prejudice patient care;
14. Act quickly to protect patients from risk where there is good reason to believe that
you, or a colleague, may not be fit to practise, fit to undertake training, or in the case
of a business registrant fit to carry on business as an optometrist, dispensing optician
or both
15. Never abuse your professional position;
16. Work with colleagues in the ways that best serve patients' interests;
17. Register with and maintain registration with the GOC;
18. Be covered by adequate and appropriate insurance for practice in the United
Kingdom throughout the period of your registration2;
19. Ensure your conduct, whether or not connected to your professional practice,
does not damage public confidence in you or your profession.

Suffolk LOC June 2015
“Not a checklist, it is up to
each clinician to exercise
their professional judgement,
however the is a common law
duty to practice to the same
standard as a reasonably
competent optometrist”.

Suffolk LOC June 2015

Fitness to practice
The grounds upon which fitness to practise of a
registered optometrist or dispensing optician are
impaired may be;
Misconduct
Deficient professional performance
A conviction/caution for an criminal offence
Adverse physical or mental health or a finding by another
health/regulatory body
Suffolk LOC June 2015

Fitness to practice
Process
Following receipt of an allegation it is referred to
a case worker.
Decision to reject or refer to FTP committee.
Civil standard, “balance of probability.”
Decide if facts are proven and whether they
amount to misconduct, deficient professional
performance or physical/mental health.
Suffolk LOC June 2015

GOC sanctions
There are a number of sanctions possible
The registrants name can be erased, (except in health
cases)
The registrant can be suspended for up to twelve months
The registration is subject to conditions for up to three
years.
In addition to the directions, the FTP committee have the
power to impose a financial penalty, up to £50,000. (except
in health case).
Suffolk LOC June 2015

Issues?
There are some issues that frequently come up
Supervision
Indemnity
Personal behaviours
Record card completion
Five eye exam themes
Suffolk LOC June 2015

Supervision
Children will always be treated more
seriously by GOC
The supervisor is on the premises, able to
intervene if necessary.
Supervisor and supervisee are aware of their
role.
The practice should have some form of
standard operating procedure in place.
Suffolk LOC June 2015

Indemnity
A requirement of registration, protecting the
patient, practitioner and practice.
Claims made and claims occurring
Remember when changing mode of employment
to make sure that you are covered
Suffolk LOC June 2015

Personal behaviours
Custodial sentence
Dishonesty is viewed very dimly and will be
reported to GOC
– Cash for cash
– Theft of vouchers and money
– Fraudulent with NHS
Drugs
Suffolk LOC June 2015

Records
To provide a continuity of care
– Between colleagues
– To monitor progression and trends
– Provide repeat prescriptions
To show your thought processes
– You did the appropriate tests
– You considered differential diagnosis
– You gave reasonable advice
To protect ourselves
– GOC and GOS regulations require it
– Records show you acted reasonably and is your main defence in litigation
Suffolk LOC June 2015
We have a duty to keep contemporaneous and legible records

What should we record?
Suffolk LOC June 2015
Not good enough today

Any other record card issues?
Business owns the records
Transfer of records to other practices
– Copy the originals & retain the original records on file
Patient has legal access
– Data protection act 1984 and 1998
– The person or someone authorised
– Written request, fee payment, 21/40 days.
– More sensible to check identity, copy and offer
explanation
Suffolk LOC June 2015

What “paperwork” should be kept
Everything !
– Records, eye exams and dispensing
– Referrals
– Notes
NHS, 7 years
AOP, 10 years
Children up to 25yr of age.
Suffolk LOC June 2015

Common complaint themes wrt
record cards
Review previous records
Dilation
Match tests conducted, decisions and advice
given to finding, history/symptoms
Communication of findings with patient
Speed of referral
Suffolk LOC June 2015

Suffolk LOC June 2015
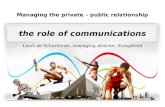
Px. Mrs BJ Date. 0000 Optom. AS DoB. 29.3.34 (75) Last visit. 3 years
S/H. LE itchy and injected 4-5 days, yellow discharge
GH, med. Good, no med POH/FH Mother glaucoma Occ/Hob
E Eye SL, RE mild staining
LE bact conj
Lens
Vessels R+L A/V 2/3
Disc R+L CD 0.4 deep
Macula Macs healthy, R and L
Periphery Healthy R and L
Fields. Few points missed LE.
Ton Perkins R 16 L15
Vision R 6/9 L 6/9
OMB D N
Motility Pupils
Current Rx As previous card
Add
Obj
Subj R +0.75/-0.75x115 6/5 L +1.25/-0.50x65 6/5
Add +2.25
Final Rx, as found
Advice.
See GP re’ bacterial conjunctivitis.
Repeat fields in 3/12
No need to change specs.
Mrs BJ, first visit, FH glaucoma, routine exam, suspect field to be repeated

Case 4
Suffolk LOC June 2015

Suffolk LOC June 2015
Px. Mrs BJ Optom. YF
S/H. Reading less easy with specs
GH, med. POH/FH Occ/Hob
E Eye
Lens
Vessels
Disc
FN
Macula
Periphery
Fields. ………………….
Ton Perkins R 14 L16
Vision R L
OMB D N
Motility Pupils
Current Rx As previous card
Add
Obj
Subj R +0.75/-0.75x110 6/6 L +1.00/-0.50x70 6/9
Add +2.50
Final Rx, as found
Advice.
Varifocals
Mrs BJ, 2nd visit, 6 months later

Suffolk LOC June 2015
Px. Mrs BJ Optom. YF
S/H. ? Vision changed, reading difficult? After light is switched off-scattered pricks of light
GH, med. POH/FH Occ/Hob
E Eye
Lens
Vessels
Disc
FN
Macula
Periphery
Fields.
Ton Perkins R 15 L17
Vision R L
OMB D N
Motility Pupils
Current Rx As previous card
Add
Obj
Subj R +1.00/-0.50x105 6/6 just L +1.50/-1.00x80 6/12
Add +2.50
Final Rx, as found
Advice.
Distance and reading specs
Watch LE
Mrs BJ, 3rd visit, 18 months later

Suffolk LOC June 2015
Px. Mrs BJ Optom. YF
S/H. Specs seem fine
GH, med. POH/FH Occ/Hob
E Eye
Lens
Vessels
Disc a
FN
Macula
Periphery
Fields.
Ton Perkins R 14 L15
Vision R L
OMB D N
Motility Pupils
Current Rx As previous card
Add
Obj
Subj R +0.75/-0.75x105 6/6 just L +1.25/-0.50x80 6/12
Add +2.25
Final Rx, as found
Advice.
Talked of varifocals
Mrs BJ, 4th visit, 2 years later

Suffolk LOC June 2015
Px. Mrs BJ Optom. AS
S/H. Pain over R eye since grand daughter poked in 2/52 ago.
GH, med. Good, no med POH/FH Mother glaucoma
E Eye Slight media haze
Vessels
Disc 0.5 deep cupping.
Suspicious LE
Macula Macs healthy, R and L
Periphery Healthy R and L
Fields. Dense arcuate scotoma LE
Ton Perkins R 14 L14
Vision R 6/9 L 6/12
OMB D N
Motility Pupils
Current Rx As previous card
Add
Obj
Subj R +1.00/-0.75x115 6/6 L +1.00/-0.75x80 6/12
Final Rx,
Advice.
Refer to GP.
(NTG confirmed by hospital)
Mrs BJ, 5th visit, 3 years later

Suffolk LOC June 2015

Patient, Mrs BJ
Next contact from patient is to inform the
practice that glaucoma has been diagnosed
Asks practice why it was not identified
Expert witness would suggest monitoring of
condition should have occurred
Compensation paid
Suffolk LOC June 2015

Suffolk LOC June 2015
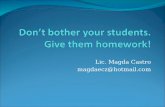
Px. Mr CJ Date. 0000 DoB. 7.2.46 (70) Last visit. 4yrs Optom. FP
S/H. Patient notices near vision is worse
GH, med. Good, no med POH/FH Lazy RE` as a child Occ/Hob Retired
E Eye NAD
Lens
Vessels
Disc
NAD
Macula
Periphery
Fields.
Ton R 21 L21
Vision R 6/12 L 6/6
OMB D RSOT N
Motility Pupils
Current Rx As previous card
Add
Obj
Subj R +3.00 6/12 L +3.00/-0.50x65 6/6
Add +2.25 N5
Final Rx,
Advice.
1st readers
24mths
Mr CJ, first visit, “lazy RE as a child”

Suffolk LOC June 2015
Px. Mr CJ Optom. FP
S/H. Routine exam
GH, med. Good, no med POH/FH Lazy RE` as a child Occ/Hob Retired
E Eye NAD
Lens
Vessels
Disc
NAD
Macula
Periphery
Fields.
Ton R 19 L20
Vision R L
OMB D N
Motility Pupils
Current Rx As previous card
Add
Obj
Subj R +3.00 6/24 L +3.00/-0.50x65 6/6
Add +2.25 N5
Final Rx,
Advice.
New glasses
24mths
Mr CJ, second visit, 2 years later

Suffolk LOC June 2015
Px. Mr CJ Optom. FP
S/H. Reading poor
GH, med. Good, no med POH/FH Lazy RE` as a child Occ/Hob Retired
E Eye NAD
Lens
Vessels
Disc
NAD
Macula
Periphery
Fields.
Ton R 23 L23
Vision R L
OMB D N
Motility Pupils
Current Rx As previous card
Add
Obj
Subj R +3.25 6/36 L +3.50/-0.25x 6/6
Add +2.25 N5
Final Rx,
Advice.
Change reading
2yrs
Mr CJ, third visit, 3 years later

Patient, Mr CJ
Next contact from patient is to inform the
practice that glaucoma has been diagnosed
Asks practice why it was not identified
Expert witness suggests that the trend in
decreasing RE VA should have been noted.
Compensation paid
Suffolk LOC June 2015

Learning points
Must review and compare old records
Were previous records referred to?
– No recognition of previous S/H
– VA slightly decreasing
– Was there any monitoring of a condition?
Suffolk LOC June 2015

When should we take records?
Eye examination
Contact lens consultation
On the phone
At the reception
Dispensing
Contemporaneous
Suffolk LOC June 2015

Suffolk LOC June 2015
Detail
-Not a lot of it….however

Suffolk LOC June 2015
When we next see the
record the missing areas
are complete
Learning
Don’t add afterwards!

Common complaint themes wrt
record cards
Review previous records
Dilation
Match tests conducted, decisions and advice
given to finding, history/symptoms
Communication of findings with patient
Speed of referral
Suffolk LOC June 2015

Suffolk LOC June 2015
-Patient “floaters in LE
for last 10 days”
- Myopic, -4 DS
- No dilation, no further
Qs re’ flashes,
- description of
periphery “normal”

Suffolk LOC June 2015
-Patient seen 6 days later
-Increase in flashes floaters
-Definite problem
-Referred to hospital
The patient complained to
GOC

Learning points
If there is an obvious condition that the symptoms
describe, we to make sure we have completed
appropriate tests to rule out that condition.
Need to have better description of structure
Dilate, (and use indirect), high myopes or if S/H
point toward retinal problem
Suffolk LOC June 2015

Common complaint themes wrt
record cards
Review previous records
Dilation
Match tests conducted, decisions and advice
given to finding, history/symptoms
Communication of findings with patient
Speed of referral
Suffolk LOC June 2015

Suffolk LOC June 2015
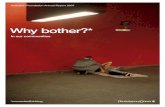
Px. SD Date. 0000 Age 4 Last visit. First Optom. MP
S/H. School referral-?squint. DV, seems OK
GH, med. Good, no med POH/FH no FH refractive Occ/Hob School
E Eye NAD
Lens Clear
Vessels Normal
Disc 0.2
Colour Healthy
Macula Slight foveal reflex
Periphery NAD
Fields.
Ton
Colour Ishihara OK
Vision R 6/6 L 6/7.5
OMB D ortho N ortho
Motility Full Pupils aaa
Current Rx
Obj R +0.50DS L +1.00/-0.50x70
0.5% cyclo instilled
Subj R +0.50 conc poor L +1.25DS conc poor
Final Rx,
Advice.
No Rx required, see 12/12
Master SD, 1st visit visit,

Suffolk LOC June 2015
Px. SD Optom. DT
S/H. Mother “LE lazy”
GH, good. Med r POH/FH r Occ/Hob School
E Eye All clear
Lens
Vessels
Disc 0.2
Colour Pink
Macula
Periphery
Fields.
Ton
Colour Ishihara OK
Vision R 6/6 L 6/12-
OMB D N
Motility Full Pupils aaa
Current Rx
Obj R Plano L +0.50DS
0.5% cyclo instilled
Subj R Plano 6/6 L +0.50DS 6/12
Final Rx,
Advice.
No Rx required, 6/12
Master SD, 2nd visit, 3 years later

Suffolk LOC June 2015
Px; SD, 2nd visit card
Illegible comment

Suffolk LOC June 2015
Px. SD Last visit. 5 mths Optom. HP
S/H. School advised poor NV. C/o headache
GH, anaemic. Med iron POH/FH LE lazy, Occ/Hob School
E Eye All clear
Lens
Vessels
Disc 0.2
Colour Pale esp. LE
Macula
Periphery
Fields.
Ton
Colour Ishihara OK
Vision R 6/9- L HM
OMB D ortho N
Motility Pupils
Current Rx
Obj R +0.50 L +0.50DS
Subj R Plano 6/9- L Balance HM
Final Rx,
Advice.
Mother to take to surgery today.
Letter to GP requests an URGENT ophthalmology view
Master SD, 3rd visit,

Patient, Master SD
Outcome
- After referral, a catalogue of errors
- Delay in getting to hospital
- Wrong diagnosis.
- Eventual diagnosis, pituitary adenoma
Suffolk LOC June 2015

Learning
- If there is reduced VA we need to have a reason
- Should we follow up referral ?
Suffolk LOC June 2015

Advice and recommendations
Address the symptoms/history and anomalies. NB The most productive 1 minute you will have
Details of correction given
– When to be worn
– Adaptation
– Dispensing advice
Other action taken
– Referral/reports and what you have found *
– Advice given, e.g. if symptoms worsen to attend A&E
– Recommended re examination
– Leaflets
Suffolk LOC June 2015

Common complaint themes wrt
record cards
Review previous records
Dilation
Match tests conducted, decisions and advice
given to finding, history/symptoms
Communication of findings with patient
Speed of referral
Suffolk LOC June 2015

Suffolk LOC June 2015
Px. SD Date. 0000 Age 68 Last visit. 3 yrs Optom. OJ
S/H. DV poor for last 2 months
GH, med. Slight high BP, ?medication POH/FH None Occ/Hob Drives
E Eye Normal
Lens Early l.ops R+L
Vessels
Disc 0.2
Macula
Normal R+L
Periphery
Fields. Henson R 3.4 L 3.4
Ton R 14 L15 NCT, 12.30
Vision R L
OMB D ortho N
Motility Pupils aaa
Current Rx
+1.00/-0.50x90 6/12 +1.25/-0.50x80 6/12
N6 Add +2.25 N6
Obj +1.25/-0.75x90 +1.50/-0.50x85 6/12
Subj +1.50/-0.50x90 6/9 +1.75/-0.50x90 6/9
N5/40 Add +2.25 N5/40
Final Rx, As found
Advice. New bifocals. 2 yr reminder
Miss CA

Patient; Miss CA
The next contact from the patient is to
enquire why the optometrist did not find her
cataracts
The practice explains they found, but not
tell her
Patient asks for £2k for private operation
Suffolk LOC June 2015

Learning
Advice; fully inform patient.
Suffolk LOC June 2015

Common complaint themes wrt
record cards
Review previous records
Dilation
Match tests conducted, decisions and advice
given to finding, history/symptoms
Communication of findings with patient
Speed of referral
Suffolk LOC June 2015

Suffolk LOC June 2015
Px; AT
-Px feels visual field
reduced
-No flashing
-Early lens changes

Suffolk LOC June 2015
Fields show a marked
Right superior defect
Patient is referred

Suffolk LOC June 2015
What degree of urgency?
The letter says
“ophthalmological
opinion is requested”
Expert report recommends
dilation and urgent referral
Record AT

Learning
- Consider the degree of urgency and instruct the GP
accordingly
- Optometrists have the knowledge to decide how serious
the condition is and so how urgent.
Suffolk LOC June 2015

Finally….
- Code of conduct
- Have I addressed the key signs and symptoms and any
anomalous results?
- Take time at end of examination to consider what could go
wrong and have I addressed it?
Suffolk LOC June 2015

Questions
Suffolk LOC June 2015

What should we record; broad areas.
History and symptoms
Reason for visit, in patient own words
Visual tasks, including driving Y/N
Ocular health and history
Medical health and history
Family history
NB. show positive and negative findings
Vision and VA with current Rx
Refraction results and OMB
Ocular examination
Results of additional tests
Advice and recommendations
Referral/notification letters
Motility
Pupils
Tonometry
Fields
Suffolk LOC June 2015
Current spectacles
Vision, unaided
Objective refraction
Subjective
– Visual acuity (is it acceptable?)*
– +1 blur
– Pin hole
– OMB
Prescription advised