
Anesthetic Record Positioning Your Patient Recovering Your Patient.
Recommended Practices for Positioningthe Patient in the Perioperative Practice Setting
The following recommended practices for positioning the patient in the perioperative practicesetting were developed hy the AORN Recommended Practices Committee and have been
approved by the AORN Board of Directors. Theywere presented as proposed recommendations forcomments by members and others. They are effective January 1, 2008.
These recommended practices are intended asachievable recommendations representing what isbelieved to be an optimal level of practice. Policiesand procedures will reflect variations in practicesettings and/or clinical situations that determinethe degree to which the recommended practicescan be implemented.
AORN recognizes the various settings in whichperioperative registered nurses practice. These recommended practices are intended as guidelinesadaptable to various practice settings. These practice settings include traditional operating rooms,ambulatory surgery centers, physicians' offices,cardiac catheterization laboratories, endoscopysuites, radiology departments, and all other areaswhere surgery may be performed.
References to nursing interventions (I) used in thePerioperative Nursing Data Set (PNDS) are noted inparentheses when a recommended practice corresponds to a PNDS intervention.' The reader isreferred to the PNDS for further explanation ofnursing diagnoses, interventions, and outcomes.
PurposeThese recommended practices provide guidelinesfor positioning the patient in the perioperative setting. They are not intended to cover aspects of perioperative patient care addressed in other recommended practices. Prevention of positioning injuryrequires anticipation of the positioning equipmentnecessary based on the patient's identified needsand the planned operative or invasive procedure,application of the principles of body mechanicsand ergonomics, ongoing assessment throughoutthe perioperative period, and coordination with theentire perioperative team.' Attention should begiven to patient comfort and safety, as well as toassessing circulatory, respiratory, integumentary,musculoskeletal, and neurological structures.Working as a member of the team, the perioperative registered nurse can minimize the risk of perioperative complications related to positioning.
2009 Perioperative Standards and Recommended PracticesLast revised: November 2007. © AORN, Inc. All rights reserved.
Recommendation I
Personnel who purchase positioning equipmentshould make decisions based on the health careorganization's patient population, current researchfindings, and the equipment design safety featuresrequired to minimize risks to patients and personnel.
The technology used to create mattresses,padding, and other positioning equipment continues to evolve, and it is important for perioperativeregistered nurses to be aware of products and current research to support their product selection.
The primary safety feature consideration forpositioning equipment is that it redistribute pressure, especially at bony prominences on thepatient's body. The National Pressure Ulcer Advisory Panel Support Surface Standards Initiativedefines a support surface as "a specialized devicefor pressure redistribution designed for management of tissue loads, micro-climate, and/or othertherapeutic functions (ie, any mattresses, integratedbed system, mattress replacement, overlay, or seatcushion, or seat cushion overlay).1!2
Although physiologic blood and lymphatic flowrates vary among individuals, capillary pressures mayincrease to as much as 150 mm Hg during prolonged, unrelieved pressure without position change.'
The traditional procedure bed mattress usually isconstructed of one to two inches of foam coveredwith a vinyl or nylon fabric. Research studies havefound that foam overlays or replacement pads, whichrepresent most OR and procedure bed mattresses, donot have effective pressure-reduction capabilities.'Studies comparing the pressure-reducing abilities ofstandard foam procedure bed mattresses to gel mattresses (ie, visco-elastic polymer) have found gel mattresses to be more effective."; One research studyreported that polyether mattresses generate a lowercapillary interface pressure when the patient was inthe supine position than gel mattresses or foam mattresses: Another study found that foam and gel mattresses are effective for preventing skin changes, butvisco-elastic overlays are effective for preventing bothskin changes and pressure sore formation.'
Clinical support surfaces (ie, padding) functiondifferently for persons of different height andweigh!.' A performance improvement studyreported that supplemental padding on the procedure bed mattress or the use of other positioning
Patient care.
RP: Positioning the Patient
devices may not reduce capillary interface pressurefor all body types or for all areas of bony prominences even in patients with the same body type."
Postoperative use of alternating pressure mattresses has been found to minimize the incidenceof pressure ulcers. Intraoperative use of this technology may be limited due to concerns aboutpatient movement, electrical safety, and asepsis.'
There are studies reporting a reduction in thepostoperative incidence of pressure ulcers whenpressure-relieving overlays are used on procedurebed mattresses and in the postoperative period;however, use of mattress overlays intraoperativelymay not minimize this risk." It is difficult, therefore,to draw firm conclusions about the most effectivemeans of intraoperative pressure relief. Future studies of pressure-relieving surfaces are needed andmust address methodological deficiencies associated with many of the available studies. Examples ofcurrent study limitations include the following:
• Trials that do not clearly reflect whether areduction in risk for skin changes is due tointraoperative or postoperative pressure reliefor whether application of the trial is necessaryin both settings to achieve a risk reduction. '"
• Studies that do not include information gathered on the postoperative skin care of thepatient make it difficult to assess the clinicalsignificance of the studies' findings.'"
• Cross comparisons of study resu Its often arenot effective because of variations of selection criteria. In addition, limited sample sizes,interrater reliability, and contradictory findings further contribute to weak scientific support for recommendations on how to predictand prevent pressure ulcers resulting fromintraoperative procedure bed mattresses. n
• Studies that measure only interface pressure(ie, the pressure on different parts of thepatient's body that are in contact with thesupport surface) have serious limitations. Theprocess that leads to the development of apressure ulcer involves the complex interplayof several factors.;o
The most frequent predictors of perioperativepressure ulcers have been found to be
• increasing age of the patient,• a patient diagnosed with diabetes or vascular
disease, and• vascular procedures.ll
• Patient Care
La. Personnel selecting procedure bed mattressesand positioning equipment for purchase anduse should make decisions based on criteriathat include, but are not limited to,- ability to hold the patient in the desired
position;- available in a variety of sizes and shapes;- suitable for the patient population and
anticipated position requirements;- ability to support maximum weight
requirements;- durable material and design (eg, main
tains resilience under constant use);- evidence that it is able to disperse skin
interface pressure;- resistance to moisture;- low risk for moisture retention;- radiolucent, if necessary;- fi re retardant;- nonallergenic;- promotes air circulation;- low risk of harboring bacteria (eg, replace-
ments may be needed when soiled);- easy to use and store; and- cost effective. 3,4,7,12
One study found the viscoelastic mattressoverlay appears to offer the most benefit forolder patient populations; patients whohave more serious or chronic health problems, where there is a prevalence of vascular disease; or in situations where surgicalprocedures extend beyond two-and- onehalf hours.'
l.a.1. Positioning equipment for obese patientsshould include, but is not limited to,• lateral transfer devices or patient lifts
to move obese patients from stretcherprocedure bed to the OR procedurebed;" and
• stretchers and beds in the postanesthesia care unit (PACU) that are ableto accommodate at least a 3D-degreeelevation of the patient's upper bodyand head to avoid respiratory distress.Whether or not a facility has a bariatric
surgery program, it is necessary to accommodate the unique needs of the obesepatient population. Patient demographics,baseline utilization requirements, andpeek census requirements may help to
2009 Per;operative Standards and Recommended Practices
RP: Positioning the Patient
La.2.
IILc. Proper working condition of positioning andtransporting equipment should be verifiedbefore use. (PNDS: 1122, 1138)
Creating a culture of safety includesdesigning a work environment that minimizesfactors that contribute to errors or injuries."
IILd. Potential hazards associated with the use ofpositioning and transporting equipmentshould be identified, and safe practices
ILa.1. When a procedure is scheduled, theavailability of special equipment shouldbe verified.
ILb. The perioperative registered nurse shouldconfirm that the room is set up appropriately for the planned procedure before thepatient arrives. (PNDS: 185, 130, 1138)
Compromises in patient safety may resultwhen the room arrangement is not specificto the planned procedure and its laterality."
Positioning and transporting equipment should beperiodically inspected and maintained in properlyfunctioning condition.
Properly functioning equipment contributes topatient safety and assists in providing adequateexposure of the surgical site. Patients and health careworkers are at risk for injury if equipment is not usedaccording to manufacturers' specifications.
liLa. Scheduled preventive maintenance and repairshould be performed on all equipment usedfor patient transport. (pNDS: 1138)
Preventive mai ntenance and repai r promote proper functioning and decrease therisk for injury to patients and personnel.
IILb. Surfaces of positioning and transportingequipment should be smooth and intact.(PNDS: 1122, 1138)
Loss of equipment surface integrity canresult in bacterial growth. Surfaces that holdmoisture or wrinkle contribute to skinbreakdown.
Recommendation III
The correct patient position and relatedequipment should be verified during thetime out period. 18
ILb.1 .
determine whether caseloads justifypurchasing rather than leasing specialbariatric equipment. Upgrading existingequipment with bariatric accessoriesmay be a viable option rather thanreplacing equipment in its entirety."
The manufacturer should be consultedfor both weight capacity and articulation abilities of the procedure bed.
Many procedure beds are designed tosafely support a 500-pound patient, butmaximum weight for special functioningcapabilities is an important consideration. Heavy-duty procedure beds areavailable that lift, articulate, and supportpatients weighing 800 to 1000 Ibs."
Lb. Procedure bed mattresses and positioningequipment should be evaluated accordingAORN's "Recommended practices for product selection in the perioperative practicesetting."16
The patient's position should provide optimumexposure for the procedure while providing accessto IV lines and monitoring devices. The nursedetermines the equipment to be used based on theplanned procedure, surgeon's preference, andpatient condition. Assessment of surgical casecharacteristics (eg, procedure length, surgicalapproach, use of radiological equipment) helpsdetermine positioning equipment and modifications in positioning needed to safely accommodatea patient's physical needs.
ILa. The perioperative registered nurse shouldreview the surgery schedule before thepatient's arrival, preferably before the day ofsurgery, to identify potential conflicts inavailability of positioning equipment.(PNDS: 185, 130, 1138)
Compromises in patient safety may resultwhen proper equipment is not available.
Recommendation II
During the planning phase of patient care, theperioperative registered nurse should anticipatethe positioning equipment needed for the specificoperative or invasive procedure.
2009 Perioperative Standards and Recommended Practices Patient Care •
RP: Positioning the Patient
should be established in accordance withAORN's "Recommended practices for a safeenvironment of care.'"'' (PNDS: 1122, 1138)
Recommendation IV
During the preoperative assessment, the perioperative registered nurse should identify uniquepatient considerations that require additional precautions for procedure-specific positioning.
Assessing patients for pressure ulcer development risk factors serves as a key step to preventingthem. Patients who are immobile, as is requiredduring operative procedures, are at increased risk.'
Additional precautions may be necessary whenpositioning special patient populations (eg, neonatal, elderly, malnourished, morbidly obese patients;patients with chronic diseases; patients with existing pressure ulcers) to reduce the risk for integumentary, respiratory, or cardiovascular compromises, and nerve impairment,12,21 For example:
• Obesity adversely affects most body systems. 22 Routine skin condition assessmentsmay be difficult because of the patient's size,lack of landmarks, and chronic conditions."Traditional foam positioning products mayprove ineffective, due to compression resulting from the patient's weight. "."
• Patients with vascular disease may have existing tissue ischemia and often have additionalrisk factors (eg, age, nutritional deficits, obesity, diabetes). Patients with vascular diseasewho are hypertensive may react unexpectedlyto a reduction in blood pressure that is considered normotensive for many patients, butwhich results in loss of blood flow throughstenotic vessels.24
• Patients who smoke often experience vasoconstriction, another mechanism that contributes to pressure ulcer formation.24
IV.a. Patient needs should be assessed by a registered nurse before transport to determinethe required equipment and the skill leveland number of transport personnel needed.(PNDS: 164)
Advance preparation for transport may berequired for obese patients or other patientswith special needs."
• Patient Care
IVb. The preoperative nursing assessment shouldinclude questions to determine patient tolerance to the planned operative position.(PNDS: 115, 160, 164, 166, 1127, 1144, 1148)
IVb.1. The perioperative registered nurseshould take additional precautions todecrease the risk for pressure ulcers inpatients who• are more than 70 years of age;• require vascular procedures or any
procedure lasting longer than fourhours;
• are thin, small in stature, or who havepoor preoperative nutritional status;
• are diabetic or have vascular disease;and
• have a preoperative Braden Scalescore that is less than 20."Studies report that the duration of a
procedure is a significant predictor ofpressure ulcer development. One studyreported that intraoperative pressureulcers increased when the procedure timeextended beyond three hours. Cardiac,general, thoracic, orthopedic, and vascular procedures were reported to be themost common types of procedures associated with pressure ulcer formation."
IVb.2. Preoperative assessment should includeevaluation of both patient and intraoperative factors.• Patient assessment should include,
but is not limited to,• age;• height;• weight;• body mass index (BMI);• skin condition;• presence of jewelry;• nutritional status;• allergies (eg, latex);• preexisting conditions (eg, vascular,
respiratory, circulatory, neurological,immune system suppression);
• laboratory results;• physical or mobility limitation (eg,
range of motion);• presence of prosthetics or correc
tive devices;
2009 Perioperative Standards and Recommended Practices
• presence of implanted devices (eg,pacemakers, orthopedic implants);
• presence of external devices (eg,catheters, drains, orthopedicimmobilizers);
• presence of peripheral pulses;• perception of pain;• level of consciousness; and• psychosocial and cultura[ consid
erations. 1,12
• Intraoperative assessment factorsshould include, but are not limited to,• anesthesia care provider's access
to patient;• estimated length of procedure;
and• desired procedural position.
IV.c. Special procedure beds and accessoriesdesigned to meet unique patient needsshould be used. (PNDS: [30, 164, 1122)
When assessing a patient's body weightand condition it is important to assess morethan just their BM!. Patients of the same BM[(a relative ratio of height and weight) canhave significantly different body composition that affects positioning needs and theirrisk for pressure ulcer development; therefore, procedure bed and positioning devicerequirements may be quite different.
The perioperative nursing assessmentshould include the length and weightcapacity of the procedure bed.
lV.d. Perioperative registered nurses should participate in their health care organization'sfall-reduction program by including anassessment of the patient's risk for fal[ing.(PNDS: [64)
Patients may be prone to fa[1s before theyenter the operating room, during transfer tothe procedure bed, and when attempting tosit up or transfer to a recliner in the PACU.'"Patients may be at a higher risk for fa[ling ifthe fol[owing conditions are present:- history of a fall during the past three
months;- use of certain medications (eg, psychotrop
ies, antidepressants, benzodiazepines, cardiovascular agents, antihypertensives,diuretics, anticoagulants, antihistamines,
2009 Perioperative Standards and Recommended Practices
RP: Positioning the Patient
bowel preparation medications, medications related to treating nocturia);"
- confusion or depression;- function or mobility problems (ie, gait),- age, and- dizziness. 27,28
The top three risk factors for predicting fallsinclude a previous fall, medications used, andgait." Age ranks fourth as a risk factor, however, it is not a good predictor of falls becausestudies show a wide range of age groupsexperience fa[ls. One study reported a highpercentage of injuries due to falls occurring inthe 20- t024-year-o[d age group.'"
IV.d.l. Regardless of age, patients who havepoor vision, postural hypotension, or analtered mental status should be considered to be at a high risk for falling."
Recommendation V
Perioperative personnel should use proper bodymechanics when transporting, moving, lifting, orpositioning patients.
The incidence of work-related back injuries innursing is among the highest of any professionworldwide.'" Manua[ lifting and other patient-hand[ing tasks are high-risk activities that can result inmusculoskeleta[ disorders." Most injuries are dueto overexertion when lifting patients; tasks thatrequire staff members to twist or bend forward; andhigh-risk tasks performed on a horizontal plane(eg, [ateral transfer from bed to stretcher, repositioning patient in bed)."'"
Biomechanical studies have demonstrated thathealth care personnel are at risk for injury, despitethe use of proper body mechanics, if patienthandling tasks are beyond reasonable limits andthe caregiver's capabilities." The combination offrequency, duration, and the stress of performinghigh-risk tasks that push the limits of human capabi[ities (eg, heavy loads; sustained, awkward positions; bending and twisting; reaching fatigue orstress; force; standing for long periods of time) predisposes nurses to musculoskeletal disorders."
V.a. An adequate number of personnel shouldbe available to ensure patient and personnelsafety when transporting the patient. (PNDS:130, 177)
Patient Care •
RP: Positioning the Patient
Procedure beds can be very heavy and difficult to move, even without the presence of apatient. When a procedure bed is moved witha patient on it, the risk of injury is increasedfor both the worker and the patient.B
V.b. The perioperative registered nurse shouldidentify high-risk tasks and implementergonomic solutions to eliminate or reduceoccupational risks for injury.
Transferring, lifting, and handling patientshave been identified as the most frequentprecipitating trigger of back and shoulderproblems for nurses." Nurses are oftenrequired to use the weaker muscles of thearms and shoulders as the primary liftingmuscles, rather than the stronger muscles ofthe legs, because lifting, turning, or repositioning patients is often performed on a horizontal plane, such as a bed or stretcher.'"
Experts do not always agree on the safestmethods for lifting or assisting dependentpatients. One research center recommendsthe use of a roller or mechanical liftingequipment to reduce the risk of strain whenmoving a patient who is unable to moveindependently. The same center studiednurses' behaviors regarding use of liftingequipment and identified the following reasons for continued manual lifting:- devices were purchased in insufficient
quantities,- lifts were stored in inconvenient loca
tions, and- equipment was not maintained ade
quately."
V.c. All perioperative personnel should be educated in the principles of body mechanicsand ergonomics.
The majority of musculoskeletal disordersreported by nurses working in the privatesector are back injuries that require timeaway from work. Several studies report thatnurses complain of chronic back pain, areunable to do their work because of injuriesto shoulder and neck, or are planning toleave the profession because of their concern for personal safety in the health careenvironment,1J
• Patient Care
Recommendation VI
Potential hazards associated with patient transportand transfer activities should be identified, andsafe practices should be established.
Preoperative patient observation and assessmentby a perioperative registered nurse allows for identification of potential problems during transportand transfer activities that can be prevented by theimplementation of appropriate precautions.
Vl.a. When selecting the appropriate transportvehicle, design features to be consideredshould include, but are not limited to,- locking devices on wheels;- protective devices (eg, safety straps, side
rails, cribs rails high enough to prevent astanding child from falling out);
- stable, adjustable IV poles or stands;- holding devices for oxygen tanks;- positioning capabilities;- controls that are easy to operate and
within reach of the operator;- maneuverability;- sufficient size;- removable head and foot boards;- mattress-stabilizing devices;- easily cleanable surfaces; and- a rack or shelf to hold monitoring equip-
ment. (PNDS: 1138)Equipment safety design features help
reduce the risk of injury to patients and personnel during transport.
Vl.b. The patient should be attended during transport and transfer by personnel deemedappropriate by the perioperative registerednurse or as determined by the anesthesiacare provider or surgeon. (PNDS: 1138)
Vl.c. Safety measures to be implemented duringtransport and transfer activities shouldinclude, but are not limited to,- presence of locking wheels on the trans
port vehicle and the patient's bed duringtransfer activities;
- side rai Is that can be elevated;- use of safety straps;- hanging and securing IV containers away
from the patient's head;
2009 Per;operative Standards and Recommended Practices
- ensuring that the patient's head, arms,and legs are protected;
- ensuring that one staff member remains atthe head of the patient transport vehicle;
- pushing the transport vehicle with thepatient's feet first and avoiding rapidmovement through hallways or whenturning corners;
- maintaining the integrity and function ofIV infusions, indwelling catheters, tubes,drainage systems, and monitoring equipment; and
- obtaining appropriately skilled assistancepersonnel and specific instructions for thepatient with special needs. (PNDS: 1138)Locking wheels, raising side rails, and
securing safety straps reduce the risk ofpatient falls. Maintaining proximity to thepatient's head provides access to thepatient's airway in the event of respiratorydistress or vomiting. Rapid movements cancause patient disorientation, nausea andvomiting, and dizziness.
Recommendation VII
Positioning equipment should be used in a safemanner and according to manufacturers' writteninstructions.
To reduce the risk of injury, it is important to follow manufacturers' written instructions regardingweight limits in flat, articulated, and reverse orientation positions for each type of procedure bed. Oneresearcher reviewed 16 perioperative incidentreports and found that 63% involved patients whowere above the specified weight limit for the positioning equipment used for back surgery. [n all of thereports, it was noted that a staff member notified thesurgeon of the problem before the beginning of thesurgery, but the equipment was used anywaybecause a[temative equipment was not available."
Vll.a. The perioperative registered nurse shouldverify that the positioning equipment to beused has been designed specifically for surgical procedure positioning. (PNDS: 1122)
The goal of using positioning equipmentis to use equipment that is designed toredistribute pressure and that decreases therisk for positioning injuries.
2009 Per;operative Standards and Recommended Practices
RP: Positioning the Patient
The number of pads, blankets, and warming blankets beneath the patient has beenimplicated as a risk factor for pressure ulcerdevelopment.4,11,26,32,33
- Foam pads may not be effective aspadding devices because they quicklycompress under heavy body areas."'" Insome situations, however, foam can bean effective pressure-reducing materialequal to that of gel or visco-elastic.Convoluted foam mattress overlays (eg,egg crate mattresses) may be more effectivein redistributing pressure if they are madeof thick, dense foam that resists compression. The effectiveness of this type of mattress overlay depends on the weight of thepatient and may not provide adequatepressure reduction in obese patients.Pillows, blankets, and molded-foamdevices may produce only a minimumamount of pressure redistribution and areless effective during long procedures.Towe[s and sheet rolls do not reducepressure and may contribute to frictioninjuries.]
Vll.b. The perioperative registered nurse shouldselect a surface that is able to reduce excessive pressure on the patient's bony prominences. (PNDS: 111, [122)
Pressure against the skin above 32 mm Hginterieres with tissue petfusion.36,37 Firm, stabledevices may help hold the patient in positionbut may not help redistribute pressure. If careis not taken to minimize pressure pointscaused by positioning equipment, the positioning equipment may not adequatelydecrease the potential for injury and may actually increase the potential for pressure injury.
Vll.b.lo Rolled sheets and towels should not beused beneath the procedure bed mattress or an overlay. When using positioning equipment such as a uterine displacing wedge or chest rolls, thepositioning devices should be placedunderneath the patient and not beneaththe mattress or overlay.
When rolled towels, sheets, or otherpositioning equipment are placedbeneath the mattress or the overlay,
Patient Care •
RP: Positioning the Patient
they may negate the pressure-reducingeffect of the mattress or overlay. n
VILe. Patients should not be transported in procedure beds unless the manufacturer's writteninstructions state that the bed is safe to useas a transportation device. (PNDS: 1122)
Procedure bed designs vary. Unlocking thebed may make it unstable. Moving an occupied procedure bed is not recommendedbecause the risk of injury increases for boththe worker and the patient.B There are someprocedure beds, however, that are designedfor patient transport. It is important to consultthe manufacturers' written instructions todetermine if unlocking and moving a patientoccupied procedure bed is recommended.
Recommendation VIII
The perioperative registered nurse should activelyparticipate in safely positioning the patient underthe direction of and in collaboration with the surgeon and anesthesia provider.
The physiologic effects of anesthesia increasethe patient's vulnerabi[ity to the effects of pressure.Patients may have preexisting conditions that limitthe positions they can assume and may influencethe positions they can to[erate."
VilLa. The perioperative registered nurse shouldprovide for patient dignity and privacy during transport, transfer, and positioning.(PNDS: 1100, [102, [150)
Maintaining patient privacy is essential topreserving the trust developed in the nursepatient relationship. The perioperative registered nurse is responsible for developing acaring environment that promotes the we[lbeing of patients. Perioperative registerednurses should provide care that recognizesthe importance of each patient's values,beliefs, and health practices and is culturallyrelevant to a diverse patient popu[ation."
VIILa.1. The perioperative registered nurseshould implement actions that include,but are not limited to, the following:• Restrict OR patient care area access
to designated authorized personnelonly.
• Patient Care
• Keep doors to patient care areasclosed.
• Limit traffic coming into OR procedure rooms.
• Expose only the areas of the patient'sbody needed to provide care oraccess to the surgical site during theplanned procedure.
• Provide auditory privacy for patientand staff member conversations during transport and transfer.
• Provide care without prejudicialbehavior.:w
VIILb. Patient jewelry and body piercing accessories should be removed before positioningor transferring to the procedure bed if it willcause potential injury or interfere with thesurgical site. (PNDS: 1138)
Patients positioned on jewelry may besubject to pressure injuries.;' Patient jewelrycan become entangled in bedding or caughton equipment while moving the patient andcause injuries due to accidental removal.
VIILc. Movement or positioning of the patientshould be coordinated with the surgicalteam. (PNDS: 196, [77)
Sliding or pulling the patient can result inshearing forces and/or friction on the patient'sskin. Shearing can occur when the patient'sskin remains stationary and underlying tissues shift or move, as might occur when thepatient is pulled or dragged without supportto the skeletal system or while using a drawsheet. Friction occurs when skin surfaces rubover a rough stationary surface:,,40
VIILe.l. Specific patient needs should be communicated to the peri operative teambefore initiating transfer or positioningthe patient.
VIILe.2. Attention should be given to protectingthe patient's airway at all times duringpatient transfer and positioning.
VIILe.3. Before and during transfer or positioning,perioperative team members shouldcommunicate with each other regardingsecuring tubes, drains, and catheters;take actions to support these devices andprevent dislodging; and confirm that the
2009 Perioperalive Standards and Recommended Practices
devices have maintained patency aftertransfer, positioning, or repositioning.
Indwelling catheters, tubes, or cannulas may be dislodged without propersupport.
VIlLcA. The peri operative registered nurseshould actively participate in monitoring the patient's body alignment andconfirming that the patient's legs are notcrossed during transfer and positioning.
Maintaining the patient's correctbody alignment and supporting his orher extremities and joints decreases thepotential for injury during transfer andposition ing. 12
VIILc.5. When on the procedure bed, the patientshould be attended by surgical teammembers at all times.
A lack of clear communication aboutwho should be watching the patientafter the safety straps are removed orbefore the patient is transferred hasbeen reported as a contributing factorfor patient falls in the operating room.'"
VIILd. The number of personnel and requiredequipment should be adequate to safelyposition the patient. (PNDS: 164, 1138)
Inadequate numbers of personnel and/orequipment can result in patient or personnelinjury.
VilLe. The perioperative registered nurse shouldactively participate in monitoring the patient'stissue integrity based on sound physiologicprinciples. (PNDS: 115, 142, 164, 196, 1145)
VIII.f. The perioperative registered nurse shouldimplement general positioning safety measuresincluding, but not limited to, the following:- Positioning equipment should be used to
protect, support, and maintain thepatient's position.
- Padding should be used to protect thepatient's bony prominences.
- The patient's arms should be positionedto protect them from nerve injury."'"
- The location of the patient's fingersshould be confirmed to ensure they arein a position that is clear of procedurebed breaks or other hazards.
2009 Perioperative Standards and Recommended Practkes
RP: Positioning the Patient
- Safety restraints should be applied carefully to avoid nerve compression injuryand compromised blood flow."
- The patient's body should be protectedfrom coming in contact with metal portions of the procedure bed.
- The patient's heels should be elevated offthe underlying surface when possible."
- The patient's head and upper body shouldbe in alignment with the hips. Thepatient's legs should be parallel and theankles uncrossed to reduce pressure toocciput, scapulae, thoracic vertebrae, olecrandn processes (ie, elbows), sacrum/coccyx, calcaneae (ie, heel),12,'14 andischial tuberosities."'"
- The patient's head should be in a neutralposition and placed on a headrest.
- A pillow may be placed under the backof the patient's knees to relieve pressureon the lower back."
- If the patient is pregnant, a wedge shouldbe inserted under the patient's right sideto displace the uterus to the left and prevent supine hypotensive syndrome,caused by the gravid uterus compressingthe aorta and vena cava.46
- If patient is attached to a robot, cautionshould be used before moving either thepatient or the robot. (PNDS: 177, 192, 196,1139)
VIII.f.1. Unless necessary for surgical reasons, thepatient's arms should not be tucked at hisor her sides when in the supine position.If there are surgical reasons to secure thepatient's arms at his or her side with theuse of a draw sheet, the draw sheetshould extend above the elbows andshould be tucked between the patientand the procedure bed's mattress."'"
When a patient's arms are tuckedtightly at his or her side with sheets, itmay add unnecessary pressure on thetucked arms and may lead to tissueinjury and ischemia. It may also causeinterference with physiologic monitoring (eg, blood pressure monitoring, arterial catheter monitoring) and result inan inability to resuscitate during anemergency due to unrecognized IV
Patient Care •
RP: Positioning the Patient
infiltration in the tucked arm. There isalso an increased risk for the patient todevelop compartment syndrome in theupper extremity."'
VIII.f.2. Direct pressure on the eye should beavoided to reduce the risk of centralretinal artery occlusion and other oculardamage, including corneal abrasion.
Patients who are at increased risk fordevelopment of postoperative visualloss are those that are undergoing procedures that are prolonged (ie, > 6.5hrs), have substantial blood loss (ie, >44.7% of estimated blood volume), orwho are in a prone position.48
• Patients at risk for ocular injury shouldbe positioned so that their heads arelevel with or higher than their hearts,when possible. In addition, their headsshould be maintained in a neutral forward position without significant neckflexion, extension, lateral flexion, orrotation, when possible. The use of ahorseshoe headrest may increase therisk of ocular compression.
• The eyes of patients in the proneposition should be assessed regularly.
• The surgeon may consider using aseries of staged spine procedures forhigh-risk patients.
Vlll.g. Peri operative team members should implement measures to reduce the risk of nerveinjuries when positioning the patient'sextremities. (PNDS: 138, 1144)- Patients who undergo general anesthesia
are at an increased risk for nerve injuryresulting from patient positioning."
- Trauma may result from compression orstretching of nerves, with the most frequent injuries involving the ulnar nerveand brachial plexus. Why some of theseinjuries occur is unknown. 12,41,42,49,SO,51
- The saphenous, sciatic, and peronealnerves are vulnerable when the patient isin the lithotomy position. The peronealnerve is also at risk with the patient in thelateral position."
- Injury to the pudendal nerve may resultfrom inadequate padding or incorrect
• Patient Care
placement of the positioning post, whenusing a fracture table. 37,52,53
Vlll.g.l. To minimize the risk of nerve injury,safety measures should include, but arenot limited to, the following:• Padded arm boards should be attached
to the procedure bed at less than a 90degree angle for supine patients.37"ll,4'1.-~O
• The patient's palms should be facingup and the fingers should beextended when his or her arms areplaced on arm boards,37,41,SO
• When the patient's arms are placedat the side of the body, they shouldbe in a neutral position (ie, elbowsslightly flexed, wrist in neutral position, palms facing inward).37,41,50
• Patient shoulder abduction and lateralrotation should kept be to a minimum.'"
• Patient extremities should be prevented from dropping below procedure bed level.
• The patient's head should be placed ina neutral position, if not contraindicated by the surgical procedure or thepatient's physical limitations."
• Adequate padding is required for thesaphenous, sciatic, and peronealnerves, especially when the patient isin a lithotomy or lateral position."
• A well-padded perineal post shouldbe placed against the perineumbetween the genitalia and the uninjured leg when a patient is positioned on a fracture table.37,52,5J
VlIl.h. Peri operative team members should implement measures to reduce the risk of injurieswhen positioning the patient in the supineposition. (PNDS: 13, 111, 177, 196, 1122)
The supine position may be modified intoa sitting or semi-sitting position for access tothe shoulder, posterior cervical spine, or posterior or lateral head. While there is betterlung excursion and diaphragmatic activity inthese positions, there is increased risk for poorvenous return from the lower extremities andpooling of blood in the patient's pelvis."- When using only a draw sheet without a
lateral transfer device for a lateral patient
2009 Perioperative Standards and Recommended Practices
----------
transfer in the supine position, the careprovider exerts a pull force up to 72.6%of the patient's weight."
- When one care provider (eg, anesthesiacare provider) supports the patient's headand neck, the remaining mass of thepatient's body equals 91.6% of his or hertotal body mass." To accommodate thisbody mass, each caregiver can safelycontribute a pull force required to trans·fer up to 48 Ibs."
- When moving the patient into and out ofa sitting or modified sitting position, themass of a patient's body from the waistup, including the head, neck, and upperextremities, equals almost 69% of thepatient's total body weight."
VII!.h.l. A lateral transfer device (eg, friction·reducing sheets, slider board, air·assisted transfer device) should be usedfor supine.to·supine patient transfer.One caregiver and one anesthesia careprovider (who is managing the airway,head, and neck) should be assigned tosafely transfer a patient who weighs 52Ibs. Two caregivers plus the anesthesiacare provider should be assigned tosafely transfer a patient up to 104 Ibs.Three caregivers plus the anesthesiacare provider should be assigned tosafely transfer a patieot up to 157 Ibs.For patients who weigh more than 157Ibs, an appropriate mechanical liftingdevice (ie, mechanical lift with supinesling, mechanical lateral transfer device,or air·assisted lateral transfer device)should be used and a minimum of threeto four caregivers should be assigned. n
VII!.h.2. When moving the patient into and outof a sitting or modified sitting position,three caregivers should be assigned towork together to lift up to 67 Ibs (30kg). It is preferable to use mechanicaldevices and a minimum of three care·givers if the patient weighs more than68 Ibs."
VII!.i. The perioperative team should implementmeasures to reduce the risk of injuries when
2009 Perioperative Standards and Recommended Practices
RP: Positioning the Patient
positioning the patient in the prone posi·tion. (PNDS: 13, 111, [77, 196, 1122)
The prone position may be modified intothe jackknife position to provide exposureto sacral, rectal, and perineal areas, or modified into the knee·chest position to provideexposure for spinal procedures. ll ,J6
Respiratory function may be affected bythe ultimate positioning of the patient and ismitigated by many factors, including theangle of incline, external pressure on the ribcage, and whether the diaphragm is free tomove.
Respiratory function may be decreased asa result of mechanical restriction of the ribcage and diaphragm when the patient is in aprone position. 12,37
Ophthalmic complications, includingvision loss, have been reported in association with patients undergoing spinal surgeryin a prone position,Sf> There is an increasedrisk for direct compression to the orbit andcorneal abrasion when the patient is in aprone position. During spinal surgeries, thepatient may be turned to a prone positionusing a frame that causes the head to belower than the rest of the body. This cerebral·dependent position may lead to a decreasedvenous return from the head, which canlead to capi Ilary bed stasis and decreasedperfusion to the optic nerve and result inblindness."
When transferring a patient from a supineposition to a prone position, the most com·mon physiologic changes are related tohypotension."
V[[!.i.l. General safety considerations for theprone position should include, but arenot limited to, the following.• The patient's cervical neck alignment
should be maintained.• Protection for the patient's forehead,
eyes, and chin should be provided.• A padded headrest should be used to
provide airway access.• Chest rolls (ie, from clavicle to iliac
crest) shou Id be used to allow chestmovement and decrease abdominalpressure.
Patient Care •
RP: Positioning the Patient
• Breasts and male genitalia should bepositioned in a way that frees themfrom torsion or pressure.
• The patient's toes should be positioned to allow them to hang overthe end of the bed or to be elevatedoff the bed by placing padding underthe patient's shins so the shins arehigh enough to avoid pressure on thetips of the toes."
VIILi.2. When in the prone position, direct pressure on the patient's eyes and faceshould be avoided."
Although ocular injuries have beenreported with and without the use of aheadrest (eg, the head held with pins),the use of a horseshoe headrest mayincrease the risk of ocular compressionand perioperative central retinal arteryocclusion. 57
VIILi.3. Ideally, the patient's arms should beplaced down by his or her sides in theprone position. If this is not possible,each arm should be placed on an armboard with the arms abducted to lessthan 90 degrees, the elbows flexed, andthe palms facing downwards. To safelysecure the patient's arms at his or hersides, the palms of the hands should befacing in toward the thighs, the elbowsand hands should be protected withpadding, and the hands and wrists shouldbe kept in anatomical alignment."
Positioning the arms above thepatient's head can cause a stretch injuryto the lower trunks of the brachialplexus. 5o
VIILi.4. Four caregivers should be available fora supine-to-prone patient transfer. Oneanesthesia care provider should maintain the airway and support the patient'shead, while other members of the teamare responsible for the patient's trunkand extremities.
Two caregivers, plus the anesthesiacare provider, can safely transfer a patientweighing up to 48.5 Ibs (22.0 kg) fromthe supine to the prone position. Three
• Patient Care
caregivers, plus an anesthesia careprovider, can safely transfer a patientweighing up to 72.7 Ibs (33.0 kg). If thepatient's weight is greater than 73 Ibs, it isnecessary to use assistive technology anda minimum of three to four caregivers.n
VIILj. The perioperative team should implementmeasures to reduce the risk of injuries whenpositioning the patient in the Trendelenburg's and reverse Trendelenburg's positions. (PNDS: 13, 111, 177, 196, 1122)
When the patient is in Trendelenburg's position, excessive pressure on the clavicle cancompress the brachial plexus as it exits the thorax between the clavicle and the first rib. Morrell closed claims files revealed that brachialplexus injuries were related to the use ofshoulder braces and the head-down position."
Positioning a patient with a history ofheart failure secondary to increased venousreturn and increased pulmonary blood flowin a steep, head-down tilt may adverselyaffect heart function. Trendelenburg's positioncauses redistribution of the blood supply dueto increased venous return from the lowerextremities. To ventilate the patient's lungswhile in this position, the diaphragm mustpush against the displaced abdominal contents, which increases the risk for the alveolito collapse resulting in atelectasis."·"
Circulatory response changes can be rapidand dramatic when moving the patient into orout of Trendelenburg's position. During surgery, there is gravitational flow of blood awayfrom the surgical field, which can mask significant blood loss. The patient may be hypotensive as a result of hypovolemia when returnedfrom Trendelenburg's position to the supineposition. Cerebral blood flow may fall asvenous and intracranial pressure rises; therefore, patients with known or suspectedintracranial pathology should not be placedin Trendelenburg's position if it can beavoided.""" Trendelenburg's position can leadto visual loss related to decreased venousreturn from the head."
VIILj.l. Measures should be taken to preventpatient from sliding on the procedure bed.
2009 Perioperative Standards and Recommended Practices
Risk for shear injuries increase whenchanging the patient's position fromsupine to Trendelenburg's or reverseTrendelenburg's."
VII!.j.2. To prevent injury to the shoulders,brachial plexus, or feet in Trendelenberg'sor reverse Trendelenberg's positions,41,42,49,50• shoulder braces should be avoided,
and• a padded footboard should be used
for reverse Trendelenburg's position.
VII!.k. The perioperative team should implementmeasures to reduce the risk of injury topatients and caregivers associated with thelithotomy position. (PNDS: 13, 111, 177, 196,1122)- Some type of leg holder is used in all
lithotomy positions. Modifications of theposition include low, standard, high, andexaggerated positions dependi ng on howhigh the legs and pelvis need to be elevated for the procedure."'"'
- The length of time that a patient mayremain in the lithotomy position withoutrisk of injury is unknown and is related topatient condition.
- In the lithotomy position the patient'sheels are at risk for pressure ulcers at theheel support sites, particularly when thelegs are supported by the heel in thestandard, high, or exaggerated lithotomyposition for prolonged procedures."'
- Injury to the peroneal nerve on the lateralaspect of the knee is common and resultsfrom the fibular neck resting against thevertical post of the stirrup when thepatient is in the lithotomy position. Thisinjury can result in foot drop and lateral,lower-extremity paresthesia. 11,37,50,60
- Compartment syndrome, although infrequent, has been reported as a complication of surgical positioning, especially theIithotomy position. 37,62-64
There is increased risk for poor venousreturn from the lower extremities and pooling of blood in the patient's pelvis when thepatient is in a lithotomy position. At the endof the procedure, the patient's overall circulating blood volume may be depleted when
2009 Perioperative Standards and Recommended Practices
RP: Positioning the Patient
the patient's legs are lowered to the procedure bed due to the blood returning quicklyinto the patient's peripheral circulation. Respiratory compromises may occur due topulmonary congestion. There is increasedrisk for deep vein thrombus formation dueto the increased risk of blood pooling in thecalf muscles."
When positioning the patient into and outof the lithotomy position, the maximum loadfor a two-handed lift is 22.2 Ibs (1 D.l kg). Eachcomplete lower patient extremity (includingthigh, calf, and foot) weighs almost 16% ofthe patient's total body mass.B
VII!.k.l. General positioning considerations forpatients in the lithotomy position include,but are not limited to, the following:• Stirrups should be placed at an even
height.• The patient's buttocks should be even
with the lower break of the procedure bed and positioned in a mannerthat securely supports the sacrum onthe bed surface. Confirm properpositioning of the patient buttocksbefore surgery is initiated."
• The patient's legs should be movedslowly and simultaneously into the legholders to prevent lumbosacral strain.
• The patient's legs should be removedfrom stirrups slowly and broughttogether simultaneously before lowering the legs to the bed surfacewhen removing the patient from legholders, to prevent lumbosacralstrain. To maintain the patient'shemodynamic status, his or her legsshould be slowly returned to the bed,one at a time if possible."
• The patient's arms should be placedon padded arm boards, extended lessthan 9D degrees from the long axis ofthe procedure bed, with the patient'spalms up and gently secured."'"" Thearms should be tucked at the patient'ssides only if surgically necessary.When it is necessary to tuck the armsat the patient's side, the elbowsshould be padded and the palms
Patient Care •
RP: Positioning the Patient
should be facing in toward thepatient's body. The hands should beenclosed and secured with ina foamprotector.37
• The patient's fingers should be protected from injury when the foot ofthe procedure bed is repositioned."
• The patient's heels should be placedin the lowest position possible."'
• Support should be provided over thelargest surface area of the leg possible.'"
• The patient's legs should not restagainst the stirrup posts.""
• Scrubbed personnel should not leanagainst the patient's thighs.w.",
• The patient should be in the lithotomy position for the shortest timepossible."'
• Care should be exercised to avoidshearing when moving the patient tothe break in the procedure bed during repositioning.
VlIl.k.2. In prolonged procedures (ie, longerthan four hours), the perioperative teamshould consider repositioning thepatient in the lithotomy position as astrategy to reduce the risk of pressureinjury (eg, skin damage, nerve injury,compartment syndrome).60,62
One research review suggests thatperi operative team members removethe patient's legs from support structuresevery two hours, if the procedure isanticipated to last four hours or more."'Research does not identify how long thepatient's legs should be out of the stirrups before repositioning.
VlIl.k.3. The perioperative registered nurse shouldmonitor the patient at all times, especiallywhen the safety strap is removed.
Proper placement of the safety strap isdifficult in the lithotomy position. Theperioperative registered nurse may notbe able to place the safety strap lowacross the patient's pelvis withoutrestricting access to the surgical site. Useof a safety strap that is placed high or tootight across the abdomen increases the
• Patient Care
risk of restricting respiration or causingpressure injuries. The patient's legs mayseem to be secure in leg holders with hisor her arms tucked at the side. It isimportant to remember that there is stilla risk for the patient to shift on the procedure bed, especially when moving intoor out of Trendelenburg's position, whichis often used in conjunction with theIithotomy position.
Vlll.kA. When positioning the patient into andout of the lithotomy position, a minimumof two caregivers is needed to lift thelegs. Mechanical devices such as supportslings can be used to lift the legs to andfrom the lithotomy position."
Vill.I. The perioperative team should implementmeasures to reduce the risk of injury topatient and caregivers associated with the lateral position. (PNDS: 13, 111, 177, 196, 1122)
The patient in the lateral position is at riskof injury due to spinal misalignment and vulnerable pressure points on the dependentside, specifically the ear, acromion process,iliac crest, greater trochanter, lateral knee,and malleolus.'
In a lateral position, the patient is positioned on the nonoperative side. Thisdependent side is the reference point for documentation. For example, when documenting a right lateral position, the patient is lyingon his or her right side. This position providesexposure for a left-sided procedure (eg,upper chest or kidney procedure). Whendocumenting the left lateral position, thepatient is lying on the left side. The left lateralposition provides exposure for a surgical orinvasive procedure on the patient's right side.
One research study on interface pressuresfound that the highest pressures occurred inthe lateral position and that there was anincreased risk for the procedure bed mattressto become fully compressed under the weightof the patient's body and cause a "bottomingout" effect." Another study found an increasedrisk for ulceration when a solid object or positioning device (eg, "bean bag" product) isused to maintain patients in a specific position. The firm pressure of the positioning
2009 Perioperative Standards and Recommended Practices
device may compromise the circulatory system due to the tight restraint and because ofthe overall effect of gravity on the horizontalbody posture."
The lateral position increases the risk ofdamage to the common peroneal nerve ifthere is not padding to protect the nerve onthe dependent leg from being compressedbetween the fibula and the procedure bed.'"
VlIl.l.l. Safety considerations for the lateralposition should include, but are notlimited to, the following:• The patient's spinal alignment should
be maintained during turning.• The patient's dependent leg should
be flexed for support."• The patient's straight upper leg
should be padded and supportedwith pillows between the legs.
• Padding should be used under thepatient's dependent knee, ankle, andfoot.
• A headrest or pillow should beplaced under the patient's head tokeep the cervical and thoracic vertebrae aligned.
• The patient's dependent ear shouldassessed to ensure that it is notfolded, and the ear should be wellpadded."
• The patient's arm should be securedto prevent movement during the procedure.
V1I1.1.2. To safely position a patient weighing upto 76 Ib (ie, 34.5 kg) into and out of thelateral position, three caregivers shouldbe assigned; one caregiver (eg, the anesthesia care provider) should be assignedspecifically to support the patient's headand neck and maintain the patient's airway during the lateral transfer.
When positioning or repositioningthe anesthetized patient into and out ofthe lateral position, pushing and pullingforces can occur rather than liftingforces. Three caregivers plus an anesthesia care provider can safely position apatient weighing up to 115 Ibs (ie, 52.2kg). If the patient's weight exceeds 115
2009 Perioperative Standards and Recommended Practices
RP: Positioning the Patient
Ibs (ie, 52.2 kg), it is important to uselateral positioning devices."
VlIl.m. The perioperative team members shou Idimplement measures to reduce the risk ofinjury to patient and caregivers associatedwith the morbidly obese patient. (PNDS: 13,111,164,177,196,1122)
Morbid obesity is associated withpatients who have a BMI of greater than 40or who weigh 100 Ibs or more over theirrecommended weight. Patients who aremorbidly obese tend to have other healthconditions, such as type II diabetes, hypertension, atherosclerosis, arthritis of weightbearing joints, sleep apnea, alveolarhypoventilation, urinary stress incontinence,and gastroesophageal reflux disease. Morbidly obese patients are at increased risk forstroke and sudden death."
It is essential for peri operative teammembers to understand the pathophysiologyof obesity and the effects that various positions have on the obese patient's cardiopulmonary function.66
- Respiratory issues include• airway compromise due to a patient's
short, thick neck;• risk of difficult intubation;• increased risk for hypoxia;• increased risk for intra-abdominal
pressure on diaphragm; and• increased risk of aspiration.
- Circulatory issues include• increased cardiac output,• increased pulmonary artery pressure,
and• risk of inferior vena cava compression.
Vlll.m.l. Safety considerations for positioning themorbidly obese patient should include,but are not limited to, the following:• The procedure bed should be capable
of articulating and supporting patientsweighing 800 to 1000 Ibs (363.2 kg to454 kgY Specialized hydraulics shouldbe capable of lifting patients weighing800 to 1000 Ibs (363.2 kg to 454 kg)."
• Mattresses should provide sufficientsupport and padding and should not"bottom OUt.!!23
Patient Care •
RP: Positioning the Patient
o The width of the patient's legs determines whether the lower legs willremain on the procedure bed or mustbe supported by stirrups. Side attachments may be available on morerecent procedure bed models.
o The patient's size may cause difficulty in determining if arms are positioned at less than a gO-degree angle.Padded sleds/toboggans may be usedto contain the patient's arms at theside of the body if necessary, provided they can be used without causing excessive pressure on the arms.
o An extra wide, extra long safety strapshould be used for patients whoexceed the length limits for a regularsize safety strap. Sheets should notbe substituted for inadequately-sizedsafety straps. Two separate safetystraps may be necessary to decreasethe risk for the patient falling off theprocedure bed due to instability andweight load shifts. One safety strapshould be placed across the patient'sthighs and one over the patient'slower legs."
o When in the supine position, a rollor wedge should be placed under thepatient's right flank to relieve compression of vena cava.
o Patients may not be able to toleratethe supine position due to respiratoryor circulatory compromises; it maybe necessary to reposition the patientinto a sitting or lateral position."'
o When in the prone position, thepatient's upper chest and pelvisshould be adequately supported tofree the abdominal viscera to reducepressure on the diaphragm and inferior vena cava. 66
o Trendelenburg's position should beavoided because the added weight ofthe abdominal contents press againstthe diaphragm causing respiratorycompromise, and the increased bloodflowing from the lower extremities intocentral and pulmonary circulationcauses vascular congestion.
• Patient Care
• In reverse Trendelenburg's position,care should be taken when placingthe patient's feet against a paddedfootboard to ensure that his or herfeet are aligned and flat against theboard. This prevents rotation andincreased pressure on the ankle.
o The lithotomy position should beavoided, if possible, due to theweight of the patient's thighs pressingon his or her abdomen and raisingintra-abdominal pressure, thusincreasing the risk of circulatorycomplications.
o If the patient is placed in the lithotomy position, heavy-duty stirrupsshould be used, and the perioperative nurse should be aware of andinstitute measures to reduce risks forrespiratory, circulatory, and neurological complications.
o The lateral position may be preferredover the prone position as the bulk ofthe patient's panniculus can be displaced off the abdomen. The perioperative nurse should be aware, however, that a shift of the patient'spanniculus may increase the risk offalling or other injury due to unintentional change in position. 15
Recommendation IX
After positioning the patient, the perioperativeregistered nurse should assess the patient's bodyalignment, tissue perfusion, and skin integrity.
Respiratory function may be compromised afterpositioning the surgical patient depending on individual factors and patient position. n.v
Circulatory function is influenced by anestheticagents and surgical techniques that may result invasodi latation, hypertension, decreased cardiacoutput, and inhibition of normal compensatorymechanisms.37
Intraoperative skin injury occurs because of acombination of events:
• unrelieved pressure,• duration of the pressure, and• the individual patient's ability to withstand
the insult.
2009 Perioperative Standards and Recommended Practices
Several studies indicate that procedures over twoand-one-half to three hours significantly increase thepatient's risk for pressure ulcer formation.37
•611 External
skin pressure exceeding normal capillary interfacepressure (ie, 23 to 32 mm Hg) can cause capillaryocclusion that will restrict or block blood flow. Theresulting tissue ischemia leads to tissue breakdown.Both high pressure for a short duration and low pressure for extended duration are pressure injury riskfactors. Other extrinsic factors for skin injury includeshear forces and friction.3,4,7,34,64,68
IX.a. After the desired patient position is attained,the perioperative registered nurse shouldreassess the patient to include, but not belimited to, the following systems:- respiratory,- circulatory,- neurological, and- m uscu loskeletal/i ntegu mentaryY'
(PNDS: 138, 187, 196, 1128)Positions such as lithotomy and Trende
lenburg's can cause redistribution and congestion of the patient's blood supply."."
Circulatory responses to certain positionsor position changes can be rapid and dramatic.12,43
IX.b. The perioperative registered nurse shouldmonitor the patient for external pressurefrom surgical team members leaning againstthe patient's body. (PNDS: /77, /128)
Retractors, equipment, or instrumentsresting on the patient and members of theperioperative team resting or leaning on thepatient add to the risk of pressure injuriesthat cause nerve or tissue damage.37
,60
IX.b.l. The perioperative registered nurse shouldcommunicate with the surgical teamabout the position of surgical instruments, retractor frames, Mayo stands, orother items placed on or over the patientthroughout the procedure.".eo
IX.c. The perioperative registered nurse shouldreassess the patient's body alignment, placement of the safety strap, and the placementof all padding after repositioning or anymovement of the patient, procedure bed, orany equipment that attaches to the procedure bed." (PNDS: /11; 1128)
2009 Per;operative Standards and Recommended Practices
RP: Positioning the Patient
Changing the patient's POSition mayexpose or damage otherwise protected bodytissue. The safety strap may shift and applyincreased pressure when repositioning thepatient or adding extra padding.
Patient repositioning may increase therisk of pressure ulcer development due toshearing of tissue.24AO
An injury may result from adding ordeleting positioning equipment, adjustingthe procedure bed, or moving the patient onthe procedure bed."
In nonsurgical settings, patients who areidentified as being at risk for developing pressure injuries are turned or repositioned at leastonce every two hours. If a patient is chairbound preoperatively, it is optimal to repositionthe patient once every hour.' When patientsreceive anesthesia, they are even more vulnerable to the effects of pressure due to physiological changes." One study found that the incidence of occipital alopecia was significantlyreduced when the patient's head was repositioned at regular intervals during prolongedprocedures (ie, longer than four hours).'"
When a prolonged surgical procedure isexpected, a patient who is in the lithotomyposition may need to be repositioned everytwo hours to reduce the risk of pressureinjury and compartment syndrome.60,62,63
Patients who have a radial intra-arterialcatheter in place throughout the procedure mayhave their wrists in a hyperextended position forthe duration of the surgical procedure. Onestudy suggests that patients' wrists should bereturned to the neutral position following arterial catheter placement as a strategy to decreasethe risk of injury to the median nerve."
Literature searches demonstrate that it isdifficult to determine the effect of patient repositioning during a surgical procedure because,while position changes are documented, thesechanges are not normally identified as a strategy to prevent pressure injuries.71 ,7l
IX.c.l. The perioperative registered nurse shouldcommunicate with anesthesia personneland the surgeon when assessing the needfor repositioning the patient every twohours for prolonged procedures.
Patient Care •
RP: Positioning the Patient
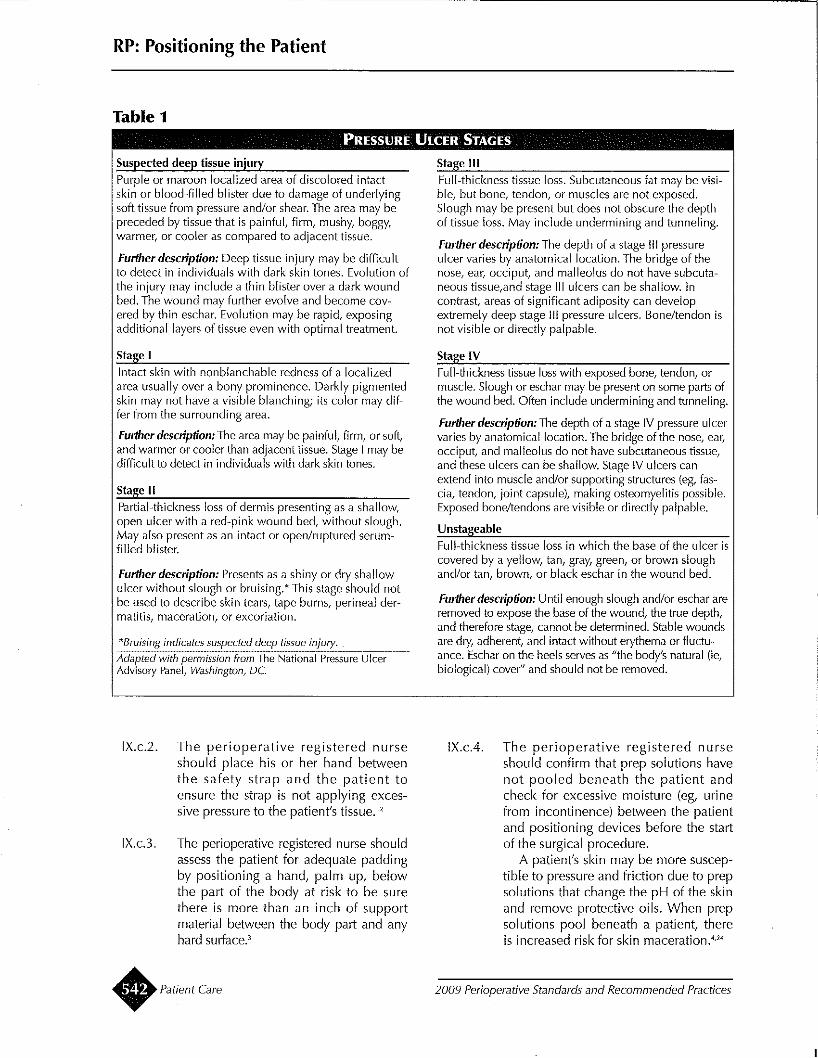
Table 1PRESSURE ULCER STAGES
Suspected deep tissue injuryPurple or maroon localized area of discolored intactskin or blood-filled blister due to damage of underlyingsoft tissue from pressure and/or shear. The area may bepreceded by tissue that is painful, firm, mushy, boggy,warmer, or cooler as compared to adjacent tissue.
Furlherdescription: Deep tissue injury may be difficultto detect in individuals with dark skin tones. Evolution ofthe injury may include a thin blister over a dark woundbed. The wound may further evolve and become covered by thin eschar. Evolution may be rapid, exposingadditional layers of tissue even with optimal treatment.
Stage IIntact skin with nonblanchable redness of a localizedarea usually over a bony prominence. Darkly pigmentedskin may not have a visible blanching; its color may differ from the surrounding area.
Further description: The area may be painful, firm, or soft,and warmer or cooler than adjacent tissue. Stage I may bedifficult to detect in individuals with dark skin tones.
Stage IIPartial-thickness loss of dermis presenting as a shallow,open ulcer with a red-pink wound bed, without slough.May also present as an intact or open/ruptured serumfilled blister.
Further description: Presents as a shiny or dry shallowulcer without slough or bruising.* This stage should notbe used to describe skin tears, tape burns, perineal dermatitis, maceration, or excoriation.
*Bruising indicates suspected deep tissue injury.-;A"daC-pc;le-cd:i'--w"Cith;-C-peC-rC:m-'is:'-sl:.c·o-'n-?li:':'o:'-m:'-T"h:.ce"N';'a~tiC:o-'na-'I';:pc're··ss"u·re~'U-;'lc·e·r·· ----Advisory Panel, Washington, DC
IX.c.2. The perioperative registered nurseshould place his or her hand betweenthe safety strap and the patient toensure the strap is not applying excessive pressure to the patient's tissue. 12
IX,c.3. The perioperative registered nurse shouldassess the patient for adequate paddingby positioning a hand, palm up, belowthe part of the body at risk to be surethere is more than an inch of supportmaterial between the body part and anyhard surface.;
• Patient Care
Stage IIIFull-thickness tissue loss. Subcutaneous fat may be visible, but bone, tendon, or muscles are not exposed.Slough may be present but does not obscure the depthof tissue loss. May include undermining and tunneling.
Further description: The depth of a stage III pressureulcer varies by anatomical location. The bridge of thenose, ear, occiput, and malleolus do not have subcutaneous tissue,and stage [II ulcers can be shallow. Incontrast, areas of significant adiposity can developextremely deep stage III pressure ulcers. Bone/tendon isnot visible or directly palpable.
Stage IVFull-thickness tissue loss with exposed bone, tendon, ormuscle. Slough or eschar may be present on some parts ofthe wound bed. Often include undermining and tunneling.
Further description: The depth of a stage IV pressure ulcervaries by anatomical location. The bridge of the nose, ear,occiput, and malleolus do not have subcutaneous tissue,and these ulcers can be shallow. Stage IV ulcers canextend into muscle and/or supporting structures (eg, fascia, tendon, joint capsule), making osteomyelitis possible.Exposed bone/tendons are visible or directly palpable.
UnstageableFull-thickness tissue loss in which the base of the ulcer iscovered by a yellow, tan, gray, green, or brown sloughand/or tan, brown, or black eschar in the wound bed.
Furtherdescription: Until enough slough and/or eschar areremoved to expose the base of the wound, the true depth,and therefore stage, cannot be determined. Stable woundsare dry! adherent! and intact without erythema or fluctuance. Eschar on the heels serves as "the body's natural (ie,biological) cover" and should not be removed.
IX.cA. The perioperative registered nurseshould confirm that prep solutions havenot pooled beneath the patient andcheck for excessive moisture (eg, urinefrom incontinence) between the patientand positioning devices before the startof the surgical procedure,
A patient's skin may be more susceptible to pressure and friction due to prepsolutions that change the pH of the skinand remove protective oils, When prepsolutions pool beneath a patient, thereis increased risk for skin maceration.4
,24
2009 Perioperative Standards and Recommended Practices
Recommendation X
The perioperative registered nurse should collaborate with the postoperative patient caregiver to identify patient injury due to intraoperative positioning.
The incidence of pressure ulcers occurring as aresult of surgery may be as high as 66%. Pressureulcers that originate in surgery may be assessedand documented as burns and may not appearuntil one to four days postoperatively. Operatingroom-acquired pressure injuries have a unique purple appearance initial[y. They tend to progress outward[y with origination at the muscle overlyingbony prominences, which explains why they maynot be detected when the initial skin assessment isdone in the operating room. Pressure injuries innonsurgical patients progress inward, gettingdeeper as the tissue injury advances' (Table 1).
Epithelialization may be delayed in patients whoare obese, which may cause poor postoperativewound healing and increased risk of infection."
X.a. Perioperative registered nurses should eva[uate the patient for signs and symptoms ofphysical injury related to intraoperative positioning. (PNDS: 144, 145, 146, 1146; [152)
Pressure ulcers are staged according tothe degree of tissue damage.,·n,,, Refer toTable 1 for assessment descriptors.
X.a." Perioperative registered nurses shouldidentify patients who are high risk forpostoperative injuries due to positioningand communicate areas of concern withpostoperative care provider. (PNDS: 164)
X.a.2. When the patient has been in the [ateralposition for an extended amount of timein the OR, the peri operative nurseshould alert the nurses caring for thepatient postoperatively to careful[yinspect the areas that are at high risk forpressure injuries. It is important tochange the patient's positions postoperatively to avoid recurring pressure onthose high risk areas.'
X,a.3. Patients who have been identified to beat-risk for development of postoperativevision loss should be assessed when thepatient becomes alert postoperatively.
2009 Perioperative Standards and Recommended Practices
RP: Positioning the Patient
The patient who has anemia preoperatively, who undergoes a prolongedprocedure, and who experiences substantia[ blood loss is identified as ahigh-risk patient for perioperative visionloss. Patient assessment, position modification, and staged procedures arestrategies identified to minimize the riskof this rare complication,56,58
The incidence of postoperative eyeinjury in nonocu[ar surgery is relativelyuncommon, but the risk may be greater inpatients whose surgery involves the face,head, or neck, and in patients whose surgery requires use of the latera[ position.The patient's age and length of procedureare also factors for ocular injury."
X.b. Perioperative registered nurses should establish open communications with postoperative care providers to obtain feedback aboutpostoperative injuries due to positioning.(PNDS: [38, 142)
X.b.1. When patients are discharged the sameday as the surgery, perioperative registered nurses should include an evaluation for signs and symptoms of injurydue to positioning in the postoperativephone call.
Recommendation XI
CompetencyPerioperative personnel should receive initial education, competency validation, and updated information on patient positioning, new positioningequipment and procedures, and ergonomic safety.
Competency verification serves as an indicatorthat personnel have a basic understanding ofpatient positioning, the risks of injury to patientand to staff members, and understand what may beimplemented as appropriate corrective actionwhen a process failure occurs.
Xl.a. The perioperative registered nurse should beeducated in, and demonstrate knowledgeabout, the physiologic effects and implications of positioning in relation to thepatient's assessed status and limitationsYz
Patient Care •
RP: Positioning the Patient
I(nowledge of anatomy and physiologyenhances the perioperative registered nurse'sappreciation of injury mechanisms associatedwith common intraoperative patient positions.12
Xl.b. Perioperative personnel should be familiarwith the proper function and use of positioning equipment.
Ongoing education of perioperative personnel will assist them in developing skillsthat will decrease the risk of patient injurydue to positioning.
XI.c. Perioperative personnel should receive education and competency validation in newpositioning equipment as they are introduced into the perioperative setti ng.
Xl.d. Members of the peri operative team whotransport patients should demonstrate competency in operating transport equipment.
Xl.e. Administrative personnel should periodically assess and document the competencyof personnel in safe patient positioning anduse of positioning equipment according tofacility and department policy. (PNDS: 11)
Recommendation XII
DocumentationPatient care and use of positioning devices shouldbe documented on the intraoperative record bythe registered nurse circulator.
Documenting nursing activities provides adescription of the perioperative nursing careadministered, status of patient outcomes upontransfer, and provides information for continuity ofpatient care. 76
Xll.a. Documentation should include, but not belimited to,- preoperative assessment including a
description of the patient's overall skincondition on arrival and discharge fromthe perioperative suite;
- type and location of positioning equipment;- name and titles of persons participating
in positioning the patient;- patient position and new position, if
repositioning becomes necessary; andpostoperative assessment for injuryrelated to position.""
• Patient Care
Xll.b. Photography used to document injuries dueto positioning should be consistent withhealth care organization's policies regardingmedical photography and videotaping.
Although the American Medical Directors Association's guidelines for pressureulcer prevention and treatment suggest photographs as a means to monitor the progressof wound care, risk management expertsand health care attorneys may adviseagainst photographs being included in thepatient's chart. If photography is used, highdefinition grid film may be recommendedfor accuracy. Digital images can be modified, resulting in questions about the accuracy and integrity of the image.'
Recommendation XIII
Policies and ProceduresPolicies and procedures related to positioning shouldbe developed, reviewed annually, revised as necessary, and readily available in the practice setting.
Policies and procedures establish authority,responsibility, and accountability. Policies alsoassist in the development of performance improvement activities. These recommended practicesshould be used to guide the development of policies and procedures within the individual perioperative practice setting.
Xlll.a. Policies and procedures for positioningshould include, but not be limited to,- assessment and evaluation criteria,- required documentation,- safety interventions,- positioning equipment care and mainte-
nance, and- ergonomic safety.
XlIl.b. Perioperative policies on positioning shouldbe consistent with the health care organization's risk-control plan for pressure ulcerprevention and management
Recommendation XIV
QualityA quality management program should be in placeto evaluate the outcomes of patient positioningpractices and to improve patient safety.
2009 Perioperative Standards and Recommended Practices
To evaluate the quality of patient care and formulate plans for corrective action, it is necessary tomaintain a system of evaluation. 77,78
XIV.a. Perioperative administration members shouldparticipate in developing and monitoring anorganization-wide risk control plan for pressure ulcer prevention and management.
XIVa.l. Pressure ulcer prevention and management risk-control plans should include,but not be limited to, the following:• a method for identifying patients at
risk for pressure ulcers;• a documentation system to follow
the progress of a wound;• prevention protocols that protect the
patient's skin integrity; and• education programs for caregivers,
patients, and family members.""
XIVb. Information about adverse patient outcomesand linear-miss incidentsfl associated withpositioning should be collected, analyzed,and used for performance improvement aspart of the institution-wide performanceimprovement program.
To demonstrate that all reasonable effortswere made to protect the patient's safety, itis considered a sound professional practiceto document information according to organizational policy when an event occurs. 5O
XIV.b.l. Following organizational policy, documentation of an event related to positioning should include, but not be limited to,• a description of what happened,• the date and time of the incident,• location of the incident,• witnesses,• corrective action to be implemented,
and• communications made regarding the
outcome.
XIV.b.2. Data on health care personnel injuriesrelated to positioning activities shouldbe collected, analyzed, and used forperformance improvement.
GlossaryBody mass index (BM/): The measure of a per
son's body fat based on height and weight thatapplies to both adult men and women.
2009 Pedoperative Standards and Recommended Practices
RP: Positioning the Patient
Braden scale: A widely used assessment tool forpredicting the development of pressure sores.
Capillary interface pressure: The amount ofpressure placed on the skin's resting surface over abony prominence.
Compartment syndrome: A pathologic conditioncaused by the progressive development of arterialcompression and consequent reduction of bloodsupply. Clinical manifestations include swelling,restriction of movement, vascular compromise, andsevere pain or lack of sensation.
Ergonomics: The science of fitting the demandsof work to the anatomical, physiological, and psychological capabilities of the worker to enhanceefficiency and well-being.
Friction: The act of rubbing one object (or tissuesurface) against another.
Morbid obesity: A person whose body massindex (BMI) is more than 40.
Procedure bed: A type of bed used in ORs orprocedure rooms that allow the surgical teamaccess to the patient and the ability to position thepatient for a surgical procedure through the use ofthe bed, its positions, and its attachments.
Positioning equipment/devices: Any device orpiece of equipment used for positioning the patientand/or providing maximum anatomic exposure.Devices include, but are not limited to,
• support devices for head, arms, chest, iliaccrests, and lumbar areasi
• pads in a variety of sizes and shapes for pressure points (eg, head, elbows, knees, ankles,heels, sacral areas);
• securing devices (eg, safety belts, tapes, kidney rests, vacuum-pack positioning devices);
• procedure beds equipment (eg, headrest!holders, overhead arm supports, stirrups,footboard); and
• specialty surgical beds (eg, fracture table,ophthalmology carts/stretchers, chairs). '"
Shearing: A sliding movement of skin and subcutaneous tissue that leaves the underlying musclestationary.
REFERENCES
1. Petersen C, ed. Perioperative Nursing Data Set. Rev2nd ed. Denver, CO: AORN, Inc; 2007:43-44, 64-66.
2. National Pressure Ulcer Advisory Panel SupportSurface Standards Initiative. Terms and definitions relatedto support surfaces. Ver. 01/29/07. http://invisib/ecaregiver. comldocslNPUAP_Standards.pdf. AccessedDecember 7, 2007.
Patient Care •
RP: Positioning the Patient
3. ECRI. Pressure ulcers. rlRC Risk Anaiysis.2006;3(Nursing 4):1-37.
4. Armstrong 0, Bortz P. An integrative review of pressure relief in surgical patients. AORN j. 2001 ;73:645,647-648,650-653.
5. Nixon J, McElvenny 0, Mason 5, Brown J, Bond S.A sequential randomised controlled trial comparing adry visco-elastic polymer pad and standard operatingprocedure bed mattress in the prevention of postoperative pressure sores. int} Nurs Stud. 1998;35:193-203.
6. Defloor T, De Schuijmer JD. Preventing pressureulcers: an evaluation of four operating-table bed mattresses. Applied Nursing Research. 2000;13:134-141.
7. Hoshowsky VM, Schramm CA. Intraoperative pressure sore prevention: an analysis of bedding materials.Res Nurs rlealth. 1994;17:333-339.
8. Shelton F, Lott Jw. Conducting and interpretinginterface pressure evaluations of clinical support surfaces. Geriatr Nurs. 2003;24:222-227.
9. King CA. Comparison of pressure relief propertiesof operating room surfaces. Perioperative NursingClinics. 2006;1 :261-265.
10. Cullum N, Mcinnes E, BellSyer SEM, Legood R.Support surfaces for pressure ulcer prevention. CochraneDatabase Syst Rev. 2007;(1 ):IDl 0300075320-1 00000000-01074.
11. Schultz A. Predicting and preventing pressureulcers in surgical patients. AORN j. 2005;81 :986-1 006.
12. McEwen DR. Intraoperative positioning of surgicalpatients. AORN j. 1996;63:1058-1063, 1066-1075, 10771082.
13. Petersen C, ed. AORN Guidance Statement: SafePatient Handling and Movement in the Perioperative Setting. Denver, CO: AORN, Inc; 2007:1-32.
14. Facility design, equipment, and supplies. In:Bariatric Services: Safety, Quality, and Technology Guide.Plymouth Meeting, PA: ECRI; 2004:77-110.
15. Dybec RS. Intraoperative positioning and care ofthe obese patient. Plastic Surgical Nursing. 2004;24:118122.
16. Recommended practices for product selection inperioperative practice settings. In: Standards, Recommended Practices, and Guidelines. Denver, CO: AORN,Inc; 2007:637-640.
17. AORN position statement on correct site surgery.In: Standards, Recommended Practices, and Guidelines.Denver, CO: AORN, Inc; 2007:371-374.
18. Joint Commission. Implementation expectations forthe universal protocol for preventing wrong site, wrongprocedure, and wrong person surgery, 2003. http://www.jointcommission.orgINRlrdonlyresIDEC4AB 16E052-4C04-AF8C-FEBA74A 732EA/OIup...guidelines.pdfAccessed May 3,2007.
19. AORN guidance statement: creating a patientsafety culture. In: Standards, Recommended Practices,and Guidelines. Denver, CO: AORN, Inc; 2007:305-310.
20. Recommended practices for a safe environmentof care. In: Standards, Recommended Practices, andGuidelines. Denver, CO: AORN, Inc; 2008:351-373.
• Patient Care
21. Keller C. The obese patient as a surgical risk.Semin Perioper Nurs. 1999;8:109-117.
22. Graling P, Elariny, H. Peri operative care of thepatient with morbid obesity. AORN }. 2003;77:801-819.
23. Bushard S. Trauma in patients who are morbidlyobese. AORN}. 2002;76:585-589.
24. Sieggreen M. OR-acquired pressure ulcers in vascular surgery patients. Adv Wound Care. 1998;11 :12.
25. Aronovitch SA. Intraoperatively acquired pressureulcer prevalence: a national study. journal of WOCN.1999/5;26:130-136.
26. Catalano, K. Update on the national patient safetygoals--changes for 2005. AORN}. 2005;81 :336-341.
27. Robey-Williams C, Rush I(L, Bendyk H, PattonLM, Chamberlain D, Sparks 1. Spartanburg Fall RiskAssessment Tool: a simple three-step process. AppliedNursing Research. 2007;20:86-93.
28. Beyea S. Preventing patient falls in perioperativesettings. [Patient Safety Firstl. AORN }. 2005; 81 :393395.
29. Nelson A, Fragala G, Menzel N. Myths and factsabout back injuries in nursing. Am j Nurs. 2003;103:3240.
30. Stetler CB, Burns M, Sander-Buscemi K, Morsi 0,Grunwald E. Use of evidence for prevention of workrelated musculoskeletal injuries. Orthop Nul's. 2003;22:32-41.
31. Chappy, S. Perioperative patient safety: a multisitequalitative analysis. AORN}. 2006; 83:871-897.
32. Sewchuk D, Padula C, Osborne E. Prevention andearly detection of pressure ulcers in patients undergoingcardiac surgery. AORN}. 2006; 84:75-96.
33. Feuchtinger J, de Sie R, Dassen T, Halfens R. A 4cm thermoactive viscoelastic foam pad on the operatingroom procedure bed to prevent pressure ulcer duringcardiac surgery.} Clin Nurs. 2006;15:162-167.
34. Ramsay J. Pressure ulcer risk factors in the operating room. Advances in Wound Care. 1998;11 :5-6.
35. Reddy M, Gill SS, Rochon PA. Preventing pressure ulcers: a systematic review. JAMA. 2006; 296: 974984.
36. Landis EM. Micro-injection studies of capillaryblood pressure in human skin. Heart. 1930;15:209-228.
37. O'Connell MP. Positioning impact on the surgicalpatient. Nurs Clin North Am. 2006;41 :173-192.
38. AORN explications for perioperative nursing. In:Standards, Recommended Practices, and Guidelines.Denver, CO: AORN, Inc; 2007;171-201.
39. Larkin BG. The ins and outs of body piercing.AORN}.2004;79:333-342.
40. Aronovitch SA, Wilber M, Slezak S, Martin T,Utter D. A comparative study of an alternating air mattress for the prevention of pressure ulcers in surgicalpatients. Ostomy Wound Management. 1999;45:34-40.
41. Practice advisory for the prevention of perioperative peripheral neuropathies: a report by the AmericanSociety of Anesthesiologists Task Force on Prevention ofPerioperative Peripheral Neuropathies. Anesthesiology.2000;92:1168-1182 .
2009 Perioperative Standards and Recommended Practices
42. Fritzlen T, I<remer M, Biddle C. The AANA Founda·tion Closed Malpractice Claims Study on nerve injuriesduring anesthesia care. AANA j. 2003;71 :347·352.
43. Ayello EA. Preventing pressure ulcers and skintears. In: Mezey M, Fulmer T, Abraham I, Zwicker OA,eds. Geriatric Nursing Protocols for Best Practice. 2nd.ed. New York, NY: Springer Publishing Company, Inc;2003:165·184.
44. Walsh J. AANA Journal course: update for nurseanesthetists-patient positioning. AANA j. 1994;62:289·298.
45. Lindgren M, Unosson M, Krantz AM, Ek AC. Pressure ulcer risk factors in patients undergoing surgery. JAdv Nul's. 2005;50:605·612.
46. Birnbach OJ, Browne 1M. Anesthesia for obstetrics. In: Miffer's Anesthesia, Volume Two. Miller RD, ed.6th ed. Philadelphia, PA: Elsevier; 2006: 2309.
47. Liau, DW. Injuries and liability related to peripheral catheters: a closed claims analysis. ASA Newsletter.june 2006. http://www.asahq.org/newsletter/2006/06/liau06_06.html. Accessed December 12, 2007.
48. Faust Rj, Cucchiara RF, Bechtel PS. Patient posi·tioninR"' In: Mifler/s Anesthesia, Volume One. Miller RO,ed. 6t ed. Philadelphia, PA: Elsevier; 2006:1155·1158.
49. Coppieters MW, Van de Velde M, Stappaerts I<H.Positioning in anesthes'lology: toward a better understanding of stretch-induced perioperative neuropathies.[Comment]. Anesthesiology. 2002;97:75·81.
50. Sawyer Rj, Richmond MN, Hickey jD, jarrratt jA.Peripheral nerve injuries associated with anaesthesia.[Comment]. Anaesthesia. 2000;55:980·991.
51. Cheney FW, Domino I<B, Caplan RA, Posner I(L.Nerve injury associated with anesthesia: a closed claimsanalysis. Anesthesiology. 1999;90:1062·1069.
52. France MP, Aurori BF. Pudendal nerve palsy following fracture procedure bed traction. ClinicalOrthopaedics & Related Research. 1992;276:272·276.
53. Toolan BC, I<oval Kj, I<ummer Fj, Goldsmith ME,Zuckerman JO. Effects of supine positioning and fracturepost placement on the perineal countertraction force inawake volunteers. JOrthop Trauma. 1995;9:164-170.
54. Lloyd JD, Baptiste A. Friction-reducing devices forlateral patient transfers: a biomechanical evaluation.American Association of Occupational Health Nurses.2006;54:113·119.
55. Chaffin DB, Andersson G, Martin BJ. Occupational Biomechanics. 3 rd ed. New York: J Wiley & Sons;1999:73.
56. American Society of Anesthesiologists Task Forceon Perioperative Blindness. Practice advisory for perioperative visual loss associated with spine surgery: a reportby the American Society of Anesthesiologists Task Forceon Peri operative Blindness. Anesthesiology. 2006;104:1319·1328.
57. Rupp·Montpetit 1<, Moody, ML. Visual loss as acomplication of non-ophthalmologic surgery: a, reviewof the literature. AANA journal. 2004;72:285·292.
58. Giarrizzo-Wilson S. Postoperative vision loss; cellular telephones; medical gas handling; roller latches.[Clinical Issues]. AORN j. 2006;84:107·108, 111·114.
2009 Perioperative Standards and Recommended Practices
RP: Positioning the Patient
59. Biddle C, Cannaday Mj. Surgical positions. theireffects on cardiovascular, respiratory systems. AORN J.1990;52:350·359.
60. Irvin W, Andersen W, Taylor P, Rice L. Minimizingthe risk of neurologic injury in gynecologic surgery.Ohstet Gynecol. 2004;103:374·382.
61. Roeder RA, Geddes LA, Corson N, Pell C, OtlewskiM, Kemeny A. Heel and calf capillary-support: pressure inlithotomy positions. AORN j. 2005;81 :821·830.
62. Wilde S. Compartment syndrome. the silent danger related to patient positioning and surgery. Br J Perioper Nul'S. 2004;14:546·550.
63. Raza A, Byrne D, Townell N. Lower limb (wellleg) compartment syndrome after urological pelvic surgery. jUral. 2004;171 :5·11.
64. Pfeffer SD, Halliwill jR, Warner MA. Effects oflithotomy position and external compression on lowerleg muscle compartment pressure. [Comment]. Anesthesiology. 2001 ;95:632·636.
65. Recommendations for facilities performingbariatric surgery. Bul! Am Col! Surg. 2000;85:20·23.
66 Brodsky jB. Positioning the morhidly obese patientfor anesthesia. Obesity Surg. 2002;12:751·758.
67. ECRI. Bariatric surgery. Operating Room RiskManagement. May 2005:14·17.
68. Schouchoff B. Pressure ulcer development in theoperating room. Crit Care Nul'S Q. 2002;25:76·82.
69. Lawson N, Mills NL, Oschner jL. Occipital alope·cia following cardiopulmonary bypass. J Thorac Cardiovase Surg. 1976;71 :342·347.
70. Chowet AL, Lopez jR, Brock·Utne jG, Jaffe RA.Wrist hyperextension leads to median nerve conductionblock: Implications for intra-arterial catheter placement.Anesthesiology. 2004;100:287·291.
71. Stotts, NA. Risk assessment of pressure ulcerdevelopment in surgical patients. Adv Skin Wound Care.1998;11 (suppl 3):7.
72. Price MC, Whitney jD, I<ing CA. Wound care.development of a risk assessment tool for intraoperativepressure ulcers. j WOCN. 2005;32:19·32.
73. Schoonhoven L, Defloor T, Grypdonck MH. Incidence of pressure ulcers due to surgery. J Clin Nurs.2002;11 :479-487.
74. National Pressure Ulcer Advisory PaneL Pressureulcer definition and stages. February 2007. http://www.npuap.org/pr2.htm. Accessed November 6, 2007.
75. Roth S, Thisted RA, Erickson jP, Black S, SchreiderBD. Eye injuries after nonocular surgery. a study of60,965 anesthetics from 1988 to 1992. Anesthesiology.1996;85:1020·1027.
76. Recommended practices for documentation of perioperative nursing care. In: Standards, Recommended Practices,and Guidelines. Denver, CO: AORN, Inc; 2007:511·514.
77. Dunn D. Incident reports: their purpose andscope. First in a two-part series. [Home Study Program].AORN j. 2003;78:45·46, 49·61,65·70.
78. Quality and performance improvement standardsfor perioperative nursing. In: Standards, RecommendedPractices, and Guidelines. Denver, CO: AORN, Inc;2007:437·446.
Patient Care •
RP: Positioning the Patient
79. Agency for Healthcare Research and Quality.Pressure Ulcers in Adults: Prediction and Prevention.Clinical PracUce Guideline Number 3, Pub No 92-0047(May 1992). http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.chapter.4409. Accessed November 6, 2007.
80. Liang BA. The adverse event of unaddressed medica!error: Identifying and filling the holes in the health-care andlegal systems. JI2w Med Ethics. 2001 ;29:346-368.
Originally published November 1990, AORN journal. Revised November 1995; published August1996, AORN journal.
Revised and reformatted; published January2001, AORN journal.
Revised 2007; published in Perioperative Standards and Recommended Practices, 2008 edition.
From the Editor
The AORN guidance document titled Safe Patient Handling and Movement in the Perioperative Setting is referenced extensively in these recommended practices. It can be ordered online from AORN's Perioperative Bookstore, http://www.aornbookstore.org, by searching forMAN-167 as the ISBN product code. To go directly to the productpage to place an order, type the following URL into your browser:
http://www.aornbookstore.org/product/product.asp?sku=MAN167
For assistance, call AORN Customer Service, 800-755-2676 ext. 1,and mention MAN-167.
• Patient Care 2009 Perioperative Standards and Recommended Practices













![X-Ray Patient Positioning Manual 080402[1]](https://static.fdocuments.in/doc/165x107/543016f6219acdf5478b5466/x-ray-patient-positioning-manual-0804021.jpg)



