
RARE DISORDERS OF IRON METABOLISM - Enerca · RARE DISORDERS OF IRON METABOLISM ... Key regulator...
30
RARE DISORDERS OF IRON METABOLISM Clara Camaschella Vita-Salute University and San Raffaele Scientific Institute Milano, Italy Madrid, 3rd European Symposium on rare anemias November 19, 2010
Transcript of RARE DISORDERS OF IRON METABOLISM - Enerca · RARE DISORDERS OF IRON METABOLISM ... Key regulator...
RARE DISORDERS OF IRON METABOLISM
Clara CamaschellaVita-Salute University and San Raffaele Scientific Institute
Milano, Italy
Madrid, 3rd European Symposium on rare anemiasNovember 19, 2010
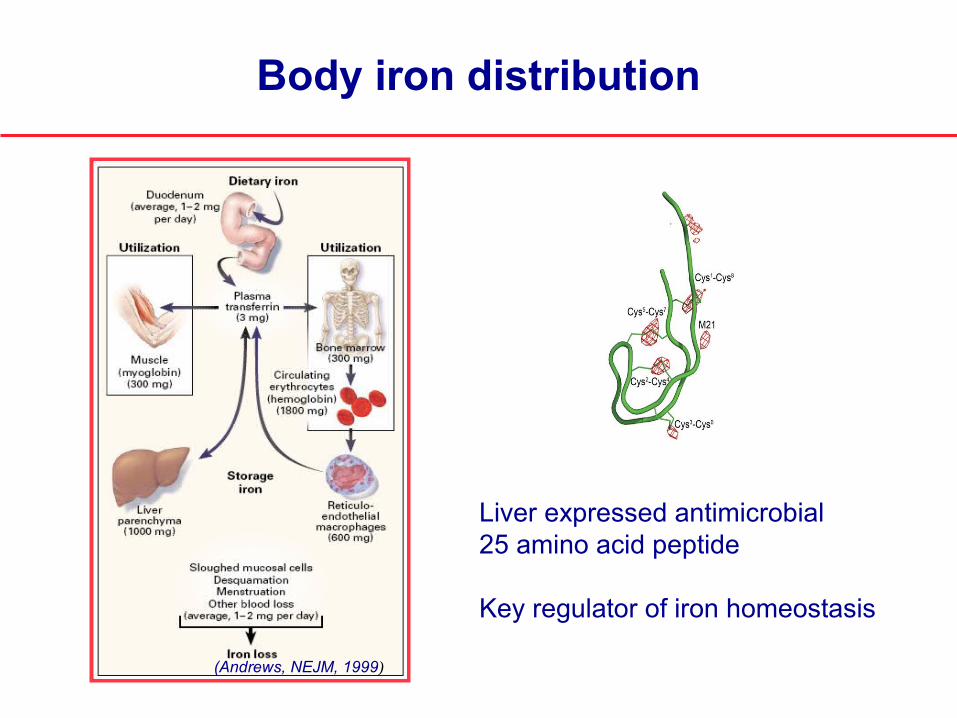
Body iron distribution
(Andrews, NEJM, 1999)
Liver expressed antimicrobial 25 amino acid peptide
Key regulator of iron homeostasis
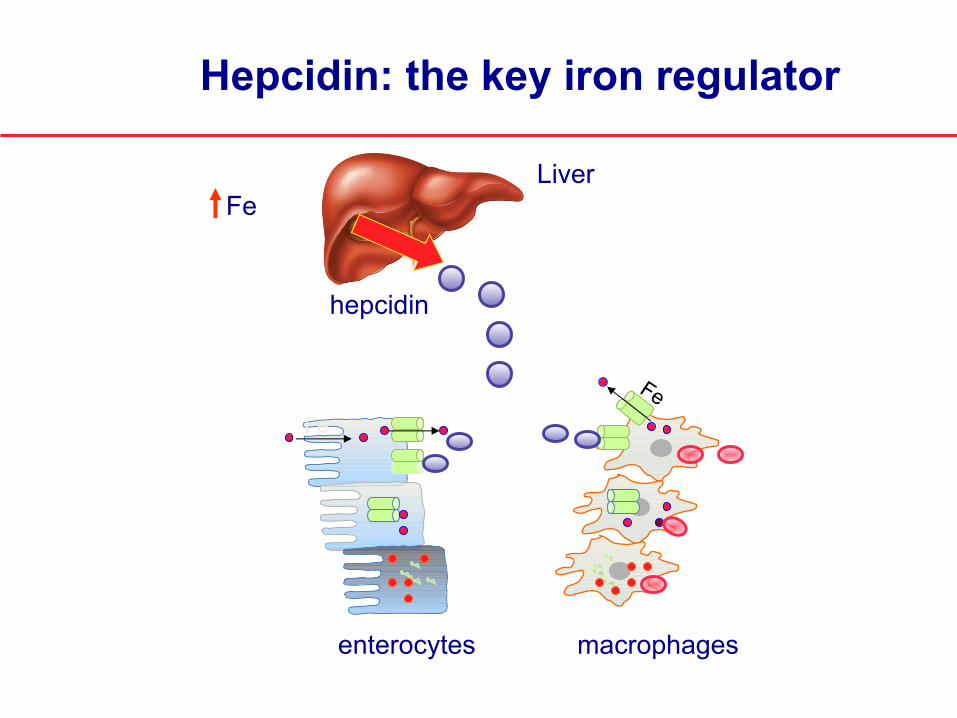
Hepcidin: the key iron regulator
hepcidin
Fe
Liver
macrophagesenterocytes
Fe
Fe
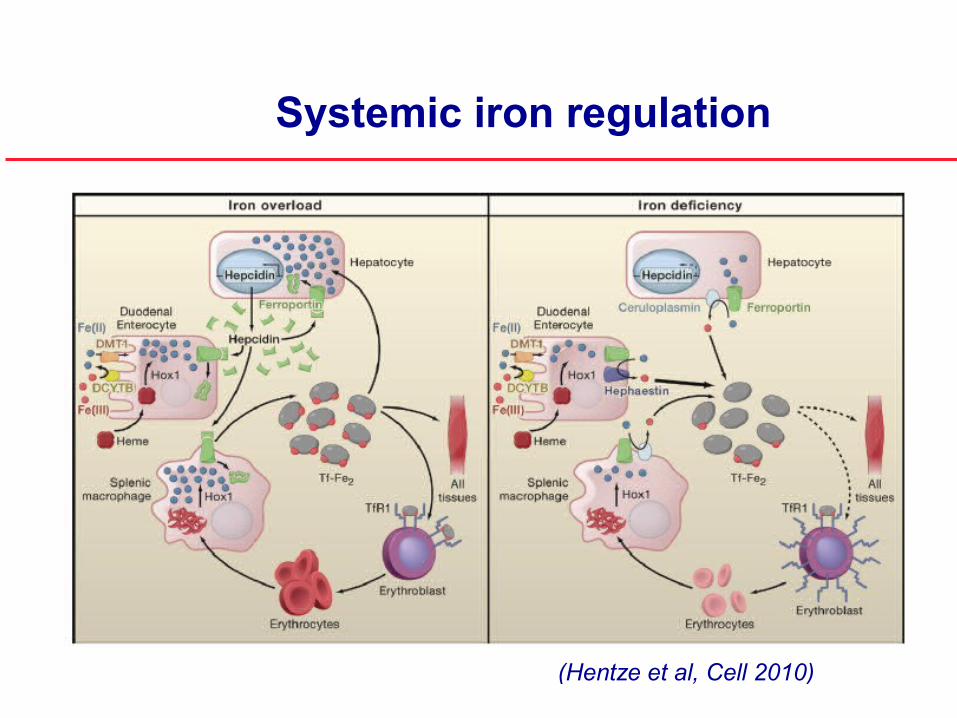
Systemic iron regulation
(Hentze et al, Cell 2010)
Disorders of hepcidin deficiency
Genetic disordersHereditary hemochromatosis type 1,2,3
(Hemochromatosis type 4 may be due to ferroportin mutations that are hepcidin-resistant)
Acquired disorderssecondary iron overload in iron loading anemias
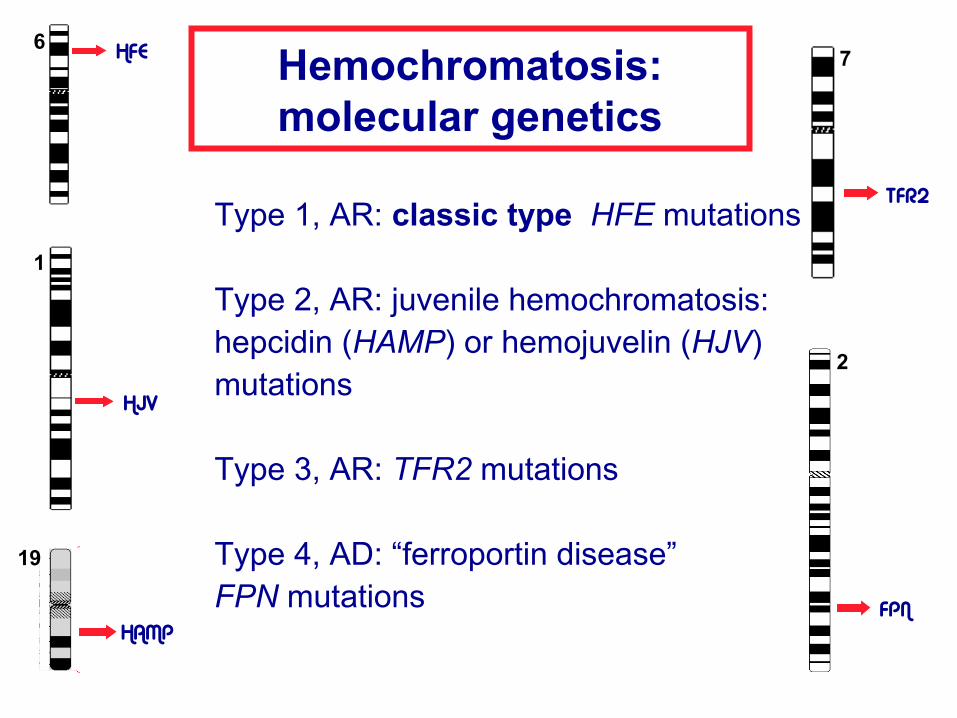
Hemochromatosis:molecular genetics
Type 1, AR: classic type HFE mutations
Type 2, AR: juvenile hemochromatosis: hepcidin (HAMP) or hemojuvelin (HJV)
mutations
Type 3, AR: TFR2 mutations
Type 4, AD: “ferroportin disease” FPN mutations
HFE
HJV
HAMP
TFR2
FPN
6
1
19
2
7

Hemochromatosis: pathogenesis
The genetic defect causes inappropriately high intestinal iron absorption and macrophage iron recycling leading to:
increased transferrin saturation increased serum ferritin iron accumulation in parenchymal organs iron toxicity and organ failure
skinskin
jointsjointspancreaspancreas
heartheartDietary ironDietary iron
pituitary
liverliver
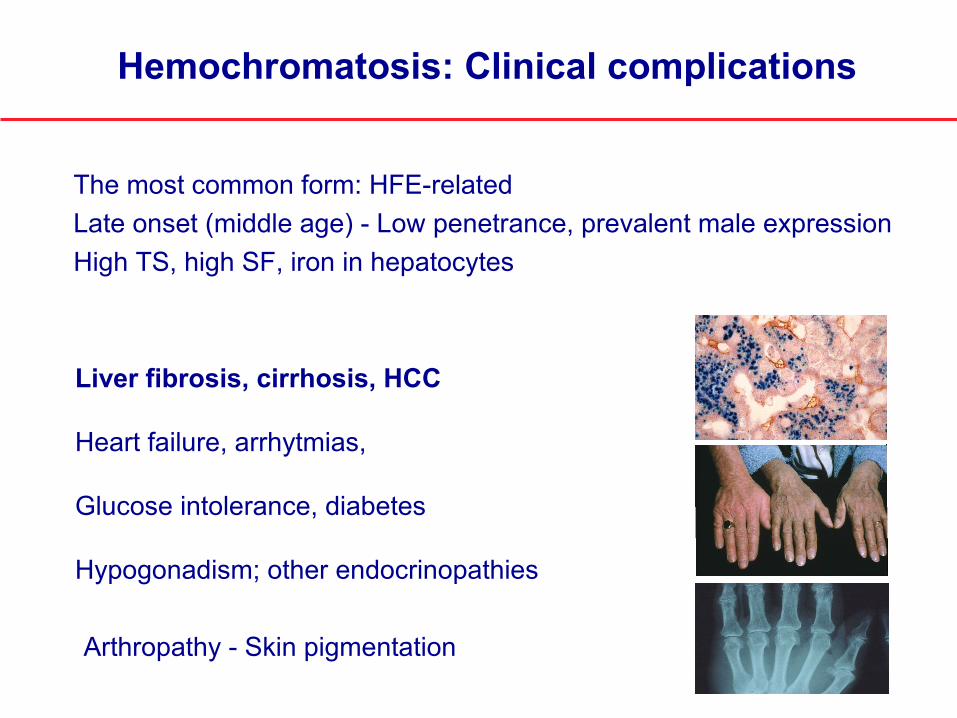
Hemochromatosis: Clinical complications
The most common form: HFE-relatedLate onset (middle age) - Low penetrance, prevalent male expressionHigh TS, high SF, iron in hepatocytes
Liver fibrosis, cirrhosis, HCC
Heart failure, arrhytmias,
Glucose intolerance, diabetes
Hypogonadism; other endocrinopathies
Arthropathy - Skin pigmentation
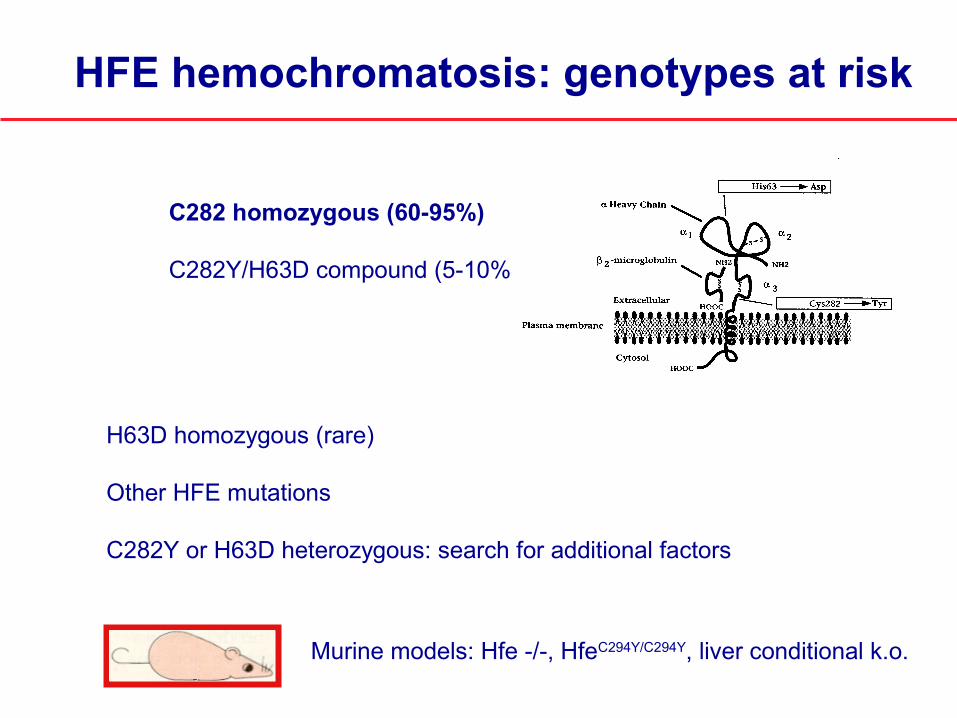
HFE hemochromatosis: genotypes at risk
C282 homozygous (60-95%)
C282Y/H63D compound (5-10%)
H63D homozygous (rare)
Other HFE mutations
C282Y or H63D heterozygous: search for additional factors
Murine models: Hfe -/-, HfeC294Y/C294Y, liver conditional k.o.
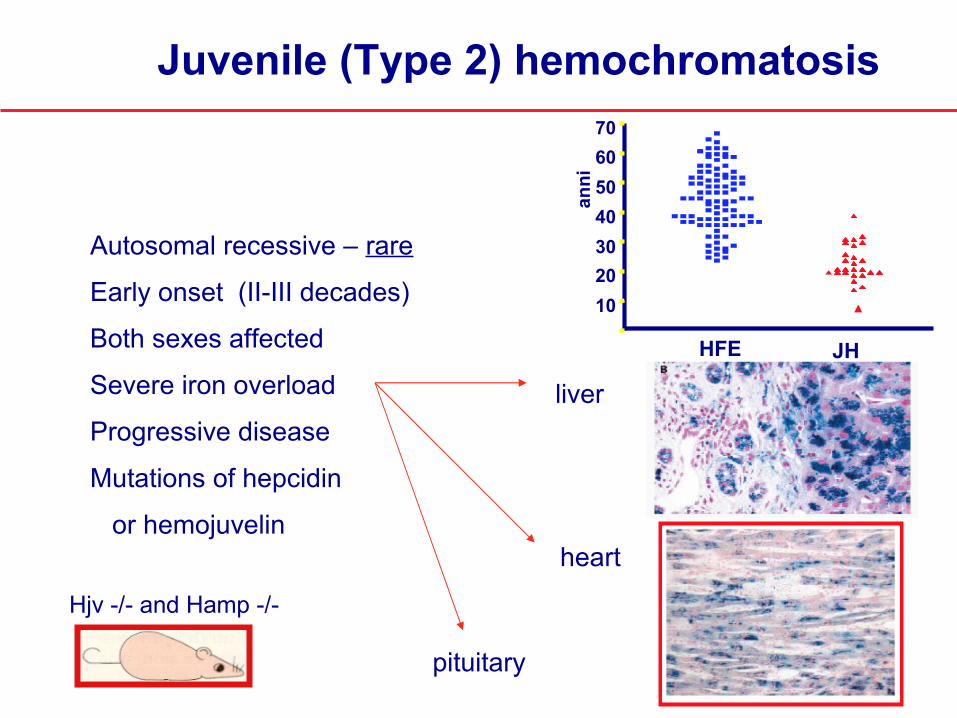
Autosomal recessive – rare
Early onset (II-III decades)
Both sexes affected
Severe iron overload
Progressive disease
Mutations of hepcidin
or hemojuvelin
Juvenile (Type 2) hemochromatosis
liver
heart
pituitary
10203040506070
HFE JH
anni
Hjv -/- and Hamp -/-

TFR2- (Type 3) hemochromatosis
Autosomal recessive, rare
High transferrin saturation, Iron in hepatocytes
Clinical complications as in HFE-disorder
Early onset but not severe
Responsive to phlebotomy
(Camaschella et al, Nat Genet 2000)
Tfr2 Y245X/ Y245X
Wild type
Fleming et al, PNAS 2002

(Ganz et al. Blood 2008;112:4292-4297)
Hepcidin dosage by ELISA in hemochromatosis
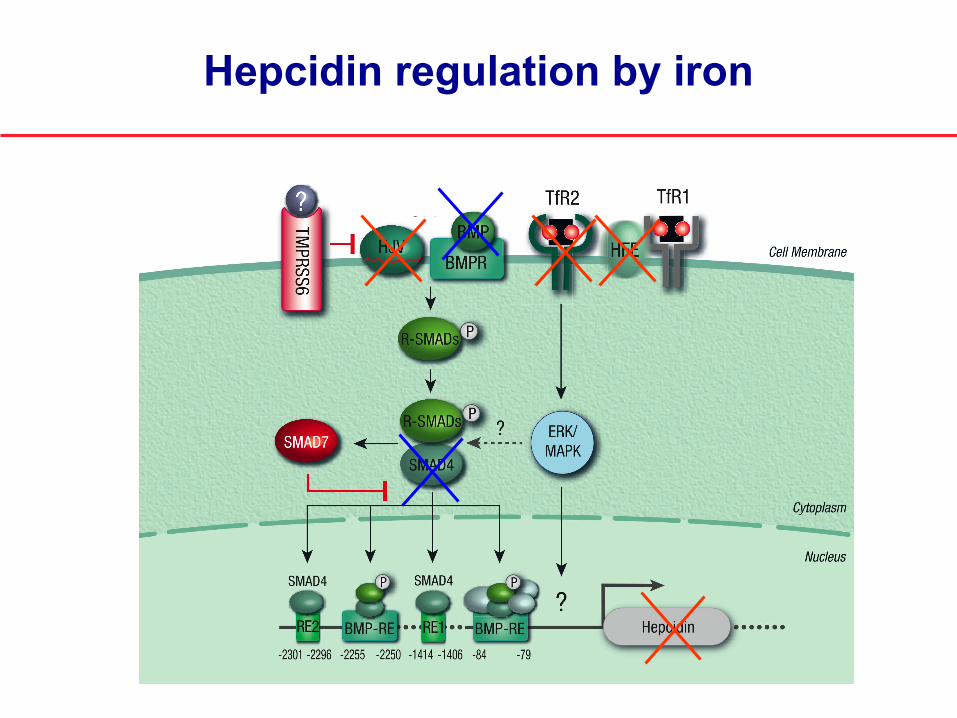
Hepcidin regulation by iron
Type 4 Hemochromatosis
Heterogeneous condition due to heterozygous mutations of the iroexporter ferroportin - Autosomal dominant
Type ANormal transferrin saturation, high serum ferritinMacrophage iron loadingMild anemia or phlebotomy intoleranceMutant ferroportin protein do not reach the plasma membrane
Type B High transferrin saturation, high serum ferritin Hepatocyte iron loading. Mutant ferroportin protein are hepcidin-resistant (e.g. C326S)
Disorders of hepcidin deficiency
Genetic disordersHereditary hemochromatosis type 1,2,3
(Hemochromatosis type 4 may be due to ferroportin mutations that are hepcidin-resistant)
Acquired disorderssecondary iron overload in iron loading anemias

Defective hepcidin activation: iron loading anemias (thalassaemia)
Tf sat % 33 79 95
Ferritin ng/ml 178 627 2,748
Hb g/dL 14.6 8.8 11.3
sTfR 1.4 47 12
(Orita el al Haematologica 2007 and Nemeth, personal comunication)
Hep
cidi
n (n
g/m
g cr
eat)
normal TI TM
10
100
1,000

Hepcidin inhibition in erythropoiesis expansion
Disorders of Hepcidin excess
Acquired disordersAnemia of chronic diseases (ACD)
Genetic disordersIron refractory iron deficiency anemia (IRIDA)
Inappropriate high hepcidin: IRIDA
IRIDA = iron refractory iron deficiency anemiaAutosomal recessive disorder due to TMPRSS6(matriptase 2) mutations Moderate anemia, severe microcytosis
(Finberg et al, Nat Genet 2008, Sem Hematol 2009)
Extremely low iron and transferrin saturationNormal serum ferritinHigh serum (and urinary) hepcidin levelsRefractory to oral and partially refractory to iv iron
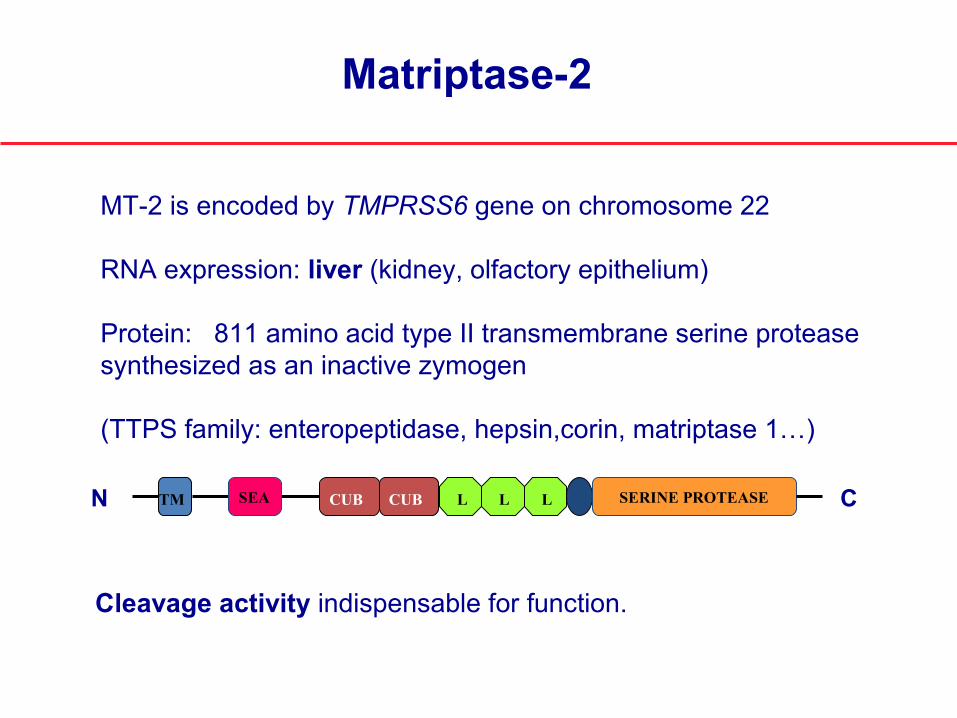
Matriptase-2
CN TM CUB LCUB LL SERINE PROTEASESEA
MT-2 is encoded by TMPRSS6 gene on chromosome 22
RNA expression: liver (kidney, olfactory epithelium)
Protein: 811 amino acid type II transmembrane serine protease synthesized as an inactive zymogen
(TTPS family: enteropeptidase, hepsin,corin, matriptase 1…)
Cleavage activity indispensable for function.

Y141
CL1
66fs
I212
T
Q22
9fs
W24
7fs
R27
1Q
C51
0S
S561
XS5
70fs
E486
D
S304
L
A118
D
Y335
XY3
93X
G44
2RE4
61fs
D52
1NE5
22K
Mas
kR
599X
A605
fsK
636f
s
P686
fs
R77
4C
Mutations associated with IRIDA
L674
F
(Silvestri et al Blood 2009De Falco et al, Hum Mut 2010)

↓HEPC
SMADs
BMP
BMPR
m-HJV
TMPRSS6
↑ serum iron
normalerythropoiesis
↑HEPC
SMADs
BMP
BMPR
m-HJV
TMPRSS6
↓ serum iron
IRIDA
Model of hepcidin regulation by matriptase-2
(Silvestri et al Cell Met 2008)

Mean±SDHb g/dl (at presentation)
7.7±1.3
Hb g/dl (at diagnosis)
9.21±1.8
MCV fl 55.47±7.6Transferrin saturation %
5.03±2.3
Ferritin ng/ml 126±82Serum hepcidin nM 257±157*Urin. hepcidin ng/mg creat
4113±3089*
IRIDA: hematological data (32 published cases)

IL-1liverIL-6
hepcidin
Hepcidin in inflammation
LPS
Reduced iron absorptionReduced iron recyclingIron retention in macrophagesIron restricted erythropoiesis(ACD)

(Ganz, T. et al. Blood 2008;112:4292-4297)
Hepcidin dosage by ELISA in inflammation
Recent reports of increased hepcidin in patients series of Hodgkin diseases, RA, Multiple Myeloma….
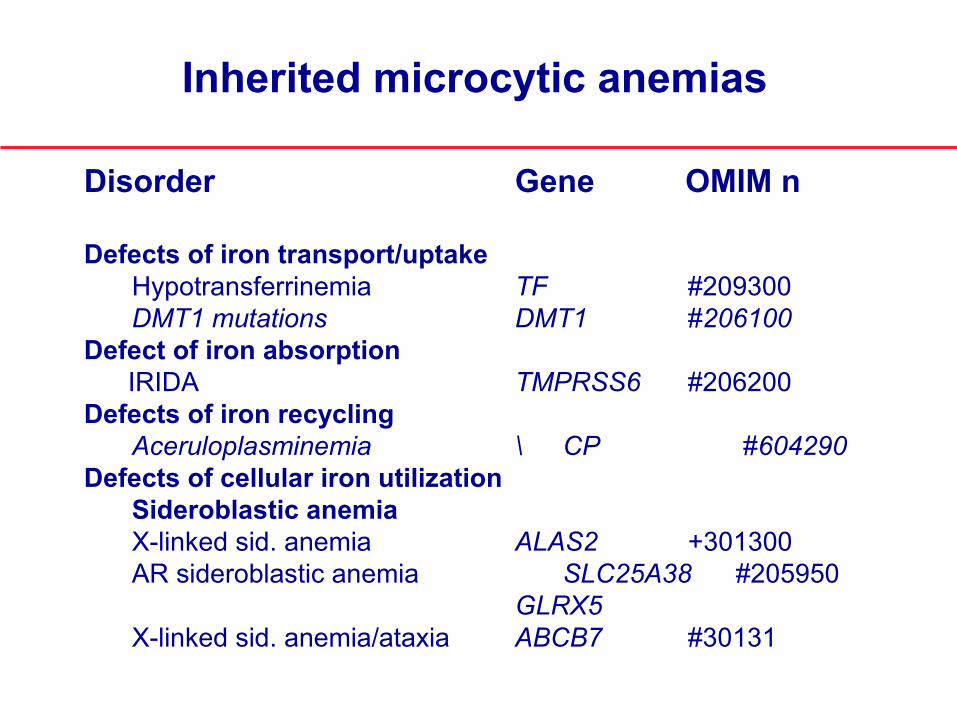
Disorder Gene OMIM n
Defects of iron transport/uptake Hypotransferrinemia TF #209300DMT1 mutations DMT1 #206100
Defect of iron absorption IRIDA TMPRSS6 #206200 Defects of iron recycling
Aceruloplasminemia \ CP #604290Defects of cellular iron utilization
Sideroblastic anemiaX-linked sid. anemia ALAS2 +301300AR sideroblastic anemia SLC25A38 #205950
GLRX5X-linked sid. anemia/ataxia ABCB7 #30131
Inherited microcytic anemias
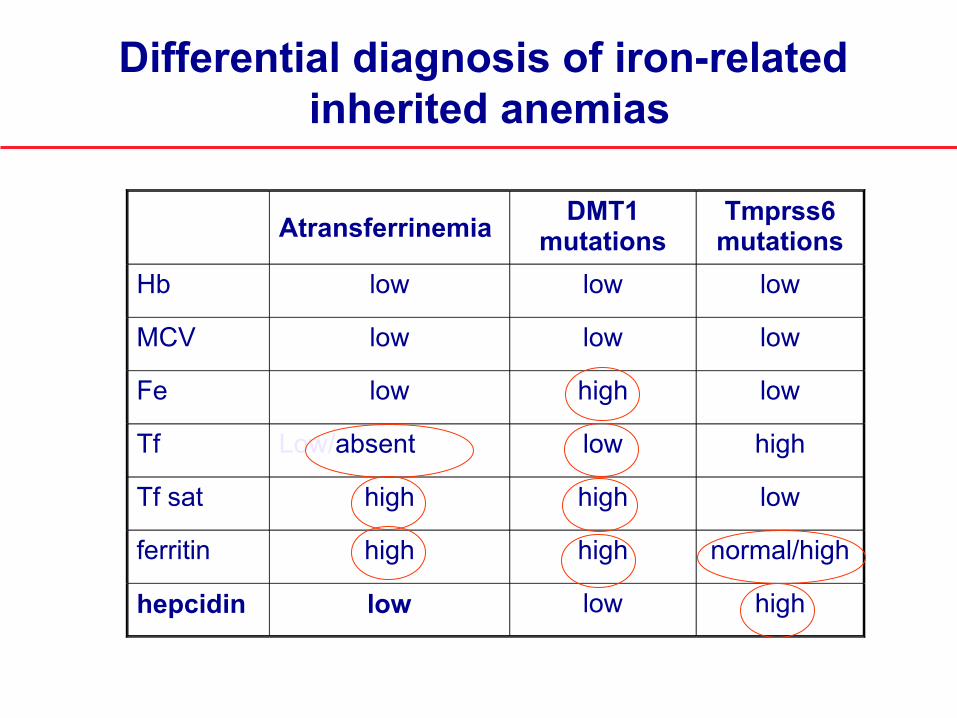
Atransferrinemia DMT1 mutations
Tmprss6 mutations
Hb low low low
MCV low low low
Fe low high low
Tf Low/absent low high
Tf sat high high low
ferritin high high normal/high
hepcidin low low high
Differential diagnosis of iron-related inherited anemias

How to suspect genetic iron-related anemias
Family history
Microcytic anemia since childhood (or birth)
Atypical iron parameters
Serum ferritin not consistent with transferrin saturation
Lack of response to oral iron, hihg hepcidin levels(IRIDA)
E-RARE project on microcytic anemias (ERARE-115, HMA-IRON)
•Dr. Carole Beaumont (France)
•Dr. Clara Camaschella (Italy)
•Dr. Martina Muckenthaler (Germany)
•Dr. Mayka Sanchez (Spain)

Acknowledgments
CEINGE & University of NaplesAchille IolasconGina De Falco
University of BresciaPaolo Arosio
University of VeronaDomenico Girelli
Laura SilvestriAlessia PaganiAntonella Nai
Vita-Salute University and San Raffaele Scientific Institute
E-rare Call 2009















![Molecular insights into the regulation of iron metabolism ... · The likely importance of hepcidin in iron homeostasis was first noted by Pigeon et al. [8], who observed that levels](https://static.fdocuments.in/doc/165x107/5f292a27856aba42a04f1452/molecular-insights-into-the-regulation-of-iron-metabolism-the-likely-importance.jpg)

