Rapid Assay for Immunological Detection of Trichomonas vaginalis · withouttheaid ofvital stains...
5
Vol. 24, No. 4 JOURNAL OF CLINICAL MICROBIOLOGY, OCt. 1986, p. 551-555 0095-1137/86/100551-05$02.00/0 Copyright C 1986, American Society for Microbiology Rapid Assay for Immunological Detection of Trichomonas vaginalis ROBERT M. WATT,* ABRAHAM PHILIP, SUSAN M. WOS, AND GREGORY J. SAM Glasgow Research Laboratory, Biomedical Products Department, E. I. du Pont de Nemours and Company, Inc., Wilmington, Delaware 19898 Received 24 March 1986/Accepted 8 July 1986 Trichomoniasis is a common sexually transmitted disease with an estimated incidence of 4 million to 8 million cases a year in the United States. The most commonly used method of diagnosis is a direct microscopic observation (wet mount) of vaginal secretions and, although both rapid and inexpensive, the sensitivity of this technique is generally 50 to 70%. We developed an indirect enzyme-linked immunosorbent assay (ELISA) for the detection of Trichomonas vaginalis which is both rapid and sensitive (detection limit of approximately 100 trichomonads per ml). This assay, which employs affinity-purified rabbit anti-T. vaginalis antibodies in a "sandwich" configuration, is simple to perform and is neither interfered with nor appears to cross-react with other microorganisms which are common inhabitants of the urogenital tract. One hundred and seventy-seven consecutive unselected patients attending a clinic for sexually transmitted diseases were evaluated for trichomoniasis by a broth culture technique monitored for up to 7 days (and considered here to be the standard for positivity), the conventional wet mount method, a solid culture procedure, and the ELISA. Of these, 84 were positive by culture; 33 were positive by the wet mount; and despite the fact that the vaginal specimens were diluted 20-fold during the culture procedures prior to testing in the ELISA, 65 were positive by ELISA. In addition to exhibiting a sensitivity of 77%, the specificity of the ELISA was 100%. These results demonstrate that the ELISA is a significant improvement over the wet mount method for the diagnosis of trichomoniasis. Despite increased awareness of the frequency of Tricho- monas vaginalis infections worldwide, the most popular clinical diagnostic tool remains the wet mount or direct microscopic examination of specimens from patients. Under the best circumstances this technique is only 75% sensitive (25) and more commonly is only 50 to 70% sensitive (9, 27, 28). Despite the modest sensitivity of the wet mount method, the basic reasons for its widespread use are twofold: (i) it is an extremely fast, inexpensive procedure (although its level of sensitivity and specificity is highly dependent on the skill of the technician), and (ii) sequellae accompanying infection are generally regarded as relatively minor compared with other sexually transmitted diseases (24, 25). Recent observations, however, suggest that the diagnosis of trichomoniasis and its differentiation from other sexually transmitted diseases such as Chlamydia trachomatis may become increasingly important (15). Furthermore, respira- tory infections in adults, presumably caused by the related trichomonad T. tenax, may in part be due to T. vaginalis (12). Pharyngeal and respiratory infections in newborns born to mothers with vaginitis caused by T. vaginalis may repre- sent yet another important manifestation of trichomoniasis (22). In addition, an increased incidence of endometritis during pregnancy has been implicated with this infection (24). Thus, more sensitive diagnostic procedures may, in fact, need to be implemented. Several methods have been developed for the detection of the protozoan. These include in vitro culture of the organ- ism, direct microscopic examination of smears both with and without the aid of vital stains (11, 13, 28, 32), immunological staining of fixed specimens (5, 23), assays for antitrichomo- nad antibodies in either serum or vaginal secretions (2, 20, 21, 29, 30), and indirect immunofluorescence (16). In gen- eral, culture methods prove to be inconvenient due to the relatively slow generation time of the organism in vitro, the * Corresponding author. short shelf life of the culture medium, and the labor-intensive nature of the procedures. Moreover, the staining of speci- mens prior to microscopy does not provide significant in- creases in sensitivity (28), and serological methods suffer from the poor correlation between antibody titers and active infection (20, 21, 30). Thus, it appears likely that immuno- logical detection of trichomonad antigens will prove to be the most sensitive approach to the diagnosis of trichomoniasis. In this report we describe a sensitive enzyme-linked immunosorbent assay (ELISA) for the detection of T. vagi- nalis antigens present in vaginal secretions obtained from 177 consecutive, unselected female patients attending an inner-city clinic for sexually transmitted diseases. This as- say, which takes approximately 1 h to perform, is shown to be at least twice as sensitive as the wet mount procedure (compared with culture) and yielded no false-positive re- sults. MATERIALS AND METHODS Patient samples. Vaginal secretions were obtained from 177 consecutive, unselected female patients presenting to the City of Philadelphia Department of Health Sexually Transmitted Disease Clinic No. 1, using a sterile, nonabra- sive pipette. Wet mount examination was performed by standard methods. Briefly, the vaginal secretion was emul- sified into 1 to 2 drops of saline on a microscope slide, a cover slip was applied, and then the slide was examined at 400x magnification under a light microscope. A specimen was considered positive if motile trichomonads with an undulating membrane and flagella were seen. After a portion of the sample was prepared for direct microscopic examina- tion, approximately 0.1 ml of the specimen was diluted 20-fold in modified medium described by Diamond (8) and a fraction of the diluted specimen was stored at -70°C until tested in the immunoassay. Specimen dilution was a neces- sary prerequisite in obtaining sufficient sample volume for subsequent testing. Approximately 0.3 ml of the diluted specimen was inoculated into modified Diamond medium 551 on March 25, 2020 by guest http://jcm.asm.org/ Downloaded from
Transcript of Rapid Assay for Immunological Detection of Trichomonas vaginalis · withouttheaid ofvital stains...

Vol. 24, No. 4JOURNAL OF CLINICAL MICROBIOLOGY, OCt. 1986, p. 551-5550095-1137/86/100551-05$02.00/0Copyright C 1986, American Society for Microbiology
Rapid Assay for Immunological Detection of Trichomonas vaginalisROBERT M. WATT,* ABRAHAM PHILIP, SUSAN M. WOS, AND GREGORY J. SAM
Glasgow Research Laboratory, Biomedical Products Department, E. I. du Pont de Nemours and Company, Inc.,Wilmington, Delaware 19898
Received 24 March 1986/Accepted 8 July 1986
Trichomoniasis is a common sexually transmitted disease with an estimated incidence of 4 million to 8 millioncases a year in the United States. The most commonly used method of diagnosis is a direct microscopicobservation (wet mount) of vaginal secretions and, although both rapid and inexpensive, the sensitivity of thistechnique is generally 50 to 70%. We developed an indirect enzyme-linked immunosorbent assay (ELISA) forthe detection of Trichomonas vaginalis which is both rapid and sensitive (detection limit of approximately 100trichomonads per ml). This assay, which employs affinity-purified rabbit anti-T. vaginalis antibodies in a"sandwich" configuration, is simple to perform and is neither interfered with nor appears to cross-react withother microorganisms which are common inhabitants of the urogenital tract. One hundred and seventy-sevenconsecutive unselected patients attending a clinic for sexually transmitted diseases were evaluated fortrichomoniasis by a broth culture technique monitored for up to 7 days (and considered here to be the standardfor positivity), the conventional wet mount method, a solid culture procedure, and the ELISA. Of these, 84were positive by culture; 33 were positive by the wet mount; and despite the fact that the vaginal specimenswere diluted 20-fold during the culture procedures prior to testing in the ELISA, 65 were positive by ELISA.In addition to exhibiting a sensitivity of 77%, the specificity of the ELISA was 100%. These results demonstratethat the ELISA is a significant improvement over the wet mount method for the diagnosis of trichomoniasis.
Despite increased awareness of the frequency of Tricho-monas vaginalis infections worldwide, the most popularclinical diagnostic tool remains the wet mount or directmicroscopic examination of specimens from patients. Underthe best circumstances this technique is only 75% sensitive(25) and more commonly is only 50 to 70% sensitive (9, 27,28). Despite the modest sensitivity of the wet mount method,the basic reasons for its widespread use are twofold: (i) it isan extremely fast, inexpensive procedure (although its levelof sensitivity and specificity is highly dependent on the skillof the technician), and (ii) sequellae accompanying infectionare generally regarded as relatively minor compared withother sexually transmitted diseases (24, 25).Recent observations, however, suggest that the diagnosis
of trichomoniasis and its differentiation from other sexuallytransmitted diseases such as Chlamydia trachomatis maybecome increasingly important (15). Furthermore, respira-tory infections in adults, presumably caused by the relatedtrichomonad T. tenax, may in part be due to T. vaginalis(12). Pharyngeal and respiratory infections in newborns bornto mothers with vaginitis caused by T. vaginalis may repre-sent yet another important manifestation of trichomoniasis(22). In addition, an increased incidence of endometritisduring pregnancy has been implicated with this infection(24). Thus, more sensitive diagnostic procedures may, infact, need to be implemented.
Several methods have been developed for the detection ofthe protozoan. These include in vitro culture of the organ-ism, direct microscopic examination of smears both with andwithout the aid of vital stains (11, 13, 28, 32), immunologicalstaining of fixed specimens (5, 23), assays for antitrichomo-nad antibodies in either serum or vaginal secretions (2, 20,21, 29, 30), and indirect immunofluorescence (16). In gen-eral, culture methods prove to be inconvenient due to therelatively slow generation time of the organism in vitro, the
* Corresponding author.
short shelf life of the culture medium, and the labor-intensivenature of the procedures. Moreover, the staining of speci-mens prior to microscopy does not provide significant in-creases in sensitivity (28), and serological methods sufferfrom the poor correlation between antibody titers and activeinfection (20, 21, 30). Thus, it appears likely that immuno-logical detection of trichomonad antigens will prove to be themost sensitive approach to the diagnosis of trichomoniasis.
In this report we describe a sensitive enzyme-linkedimmunosorbent assay (ELISA) for the detection of T. vagi-nalis antigens present in vaginal secretions obtained from177 consecutive, unselected female patients attending aninner-city clinic for sexually transmitted diseases. This as-say, which takes approximately 1 h to perform, is shown tobe at least twice as sensitive as the wet mount procedure(compared with culture) and yielded no false-positive re-sults.
MATERIALS AND METHODSPatient samples. Vaginal secretions were obtained from
177 consecutive, unselected female patients presenting tothe City of Philadelphia Department of Health SexuallyTransmitted Disease Clinic No. 1, using a sterile, nonabra-sive pipette. Wet mount examination was performed bystandard methods. Briefly, the vaginal secretion was emul-sified into 1 to 2 drops of saline on a microscope slide, acover slip was applied, and then the slide was examined at400x magnification under a light microscope. A specimenwas considered positive if motile trichomonads with anundulating membrane and flagella were seen. After a portionof the sample was prepared for direct microscopic examina-tion, approximately 0.1 ml of the specimen was diluted20-fold in modified medium described by Diamond (8) and afraction of the diluted specimen was stored at -70°C untiltested in the immunoassay. Specimen dilution was a neces-sary prerequisite in obtaining sufficient sample volume forsubsequent testing. Approximately 0.3 ml of the dilutedspecimen was inoculated into modified Diamond medium
551
on March 25, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

552 WATT ET AL.
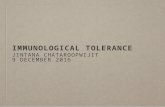
Step #1: Antigen Capture in the Presenceof Biotinylated Second Antibody.
Step #2: Wash and Add HRP-Streptavidin.
Step #3: Wash and Add ABTS °
/~~~~~~~
tAbl - \ ~~~B2
FIG. 1. Immunoassay strategy. The individualvaginalis antigen (Ag) immunoassay are outlined.performed by first incubating a sample putativel)protozoan in an antibody (Ab)-sensitized microtiterdiately adding biotinylated anti-T. vaginalis antitFollowing a 30-min incubation period, all wells iiplate were washed and horseradish peroxidase-coistreptavidin (Av-E) was added for 15 min (Step 2)plate was again washed and ABTS (0) was added,the A415 of the contents of each well was measuredresponses were delineated by quantitatively compar
generated in sample wells with a negative contriinspecting the plate visually, as described in the te
supplemented with nystatin, penicillin strel10% heat-inactivated horse serum. Culture anexaminations of patient specimens were comp
to 15 min after collection. Broth cultures wer37°C in an atmosphere of7% CO2 and scored texamination at 24, 48, and 72 h and at 7 dayrThe remaining sample volume was used in
procedure for the quantitation of viable T.details of this quantitation study have been dfully by Philip et al. (A. Philip, P. Carter-Rogers, J. Infect. Dis., in press), so only a tewill be provided here. Briefly, the solid medwas a modification of Diamond medium as diously by Ivey (14). Agar culture mediumprepared daily in 8.5-ml fractions, autoclaveheld at 48°C until use. As in the case with thehorse serum and antibiotics were added immethe introduction of the specimen. Liquefied ajinto plates (100 mm in diameter), and duplicatwere inoculated with each patient specimenwas negative for T. vaginalis by wet mount20-fold-diluted specimen was pipetted onto eatube of solid culture medium (held at 48°C)top of the inoculum, mixed, and allowed tcmount-positive samples were diluted an ad(
(1:400 final dilution) and processed in an identical fashion.Plates were placed in an anaerobic pouch (BBL Microbiol-ogy Systems, Cockeysville, Md.), heat-sealed, and incu-bated at 37°C for 5 days. At the end of this period colonies onboth plates were counted; the average was determined; andthe concentration of viable organisms, expressed asCFU/ml, in the specimen was calculated. Of the 84 broth-positive specimens obtained in this study, only 3 failed to
E grow on solid medium and, thus, they could not be quanti-, A,5 tated.
Antibody preparation. Antibodies to T. vaginalis wereelicited in rabbits by immunization with whole tricho-monads. Six adult female New Zealand White rabbits were
injected intradermally in multiple sites with a 1-ml inoculumcontaining 2.5 x 107 organisms emulsified in completeFreund adjuvant (Difco Laboratories, Detroit, Mich.). Theanimals received three injections within a 1-month period.The sera were pooled, and an immunoglobulin fraction was
prepared by ammonium sulfate precipitation. This crude0 immunoglobulin G (IgG) fraction was applied to a column of
\J7 sonicated T. vaginalis covalently coupled to CNBr-activatedSepharose CL-4B (Pharmacia Fine Chemicals, Piscataway,N.J.) (7). Specific antibodies were eluted from the columnwith 0.1 M acetic acid (pH 2.5) and immediately dialyzedagainst phosphate-buffered saline (PBS; 120 mM NaCl, 2.7mM KCI, 10 mM phosphate [pH 7.4]; Sigma Chemical Co.,St. Louis, Mo.). Purity of the antibody preparations was
steps of the T. verified by electrophoresis in sodium dodecyl sulfate-The assay was containing polyacrylamide gels (17), and the protein concen-
containing the tration of antibodies was determined by the procedure ofwell and imme- Lowry et al. (19).bodies (Step 1). Biotinylation of purified antibodies. Affinity-purified rabbitn the microtiter anti-T. vaginalis antibodies were biotinylated by reactionnjugated (HRP)- with N-hydroxysuccinimidobiotin (Pierce Chemical Co.,The microtiter Rockford, Ill.). Briefly, antibodies at a concentration of
Step 3). Positive approximately 1 mg/ml were first dialyzed against 0.1 M-ingthe color (y) sodium bicarbonate (pH 8.6) and then reacted with 30-foldol or by simply molar excess of N-hydroxysuccinimidobiotin (dissolved at 1xt. mg/ml in dimethyl sulfoxide) for 4 h at room temperature.
Free biotin was removed from the preparation by dialysis ofthe reaction mixture against PBS. Titers of biotinylated
ptomycin, and antibodies were then determined on T. vaginalis-sensitizedid microscopic polystyrene microtiter plates (Immulon 2; Dynatech Labo-oleted within 10 ratories, Inc., Alexandria, Va.) which were prepared byre incubated at incubating individual wells on the plates with 100 ,ul ofby microscopic sonicated trichomonads (10 pLg/ml) in PBS overnight at 4°C.s. Horseradish peroxidase-conjugated streptavidin (Bethesdaa solid culture Research Laboratories, Gaithersburg, Md.) was used tovaginalis. The detect bound biotinylated antibodies.lescribed more ELISA procedure. Polystyrene microtiter plates were
-Scott, and C. coated with affinity-purified rabbit anti-T. vaginalis antibod-rse description ies, blocked by incubation with 1% bovine serum albumin inlium employed PBS, and stored at 4°C until needed. Assay of the clinicalescribed previ- samples, depicted schematically in Fig. 1, involved the(pH 6.0) was addition of 50 ,ul of the diluted specimens to individual wellsd, cooled, and in microtiter plates, followed immediately by the addition ofbroth medium, 50 pl of biotinylated anti-T. vaginalis antibodies in 1%diately prior to bovine serum albumin in PBS. After a 30-min period ofgar was poured incubation at room temperature, the assay plates were
Le sets of plates washed nine times (three cycles of three washes per cycleIf the sample with an automatic plate washer) with PBS containing 0.05%0.5 ml of the Tween 20, and then 100 pul of horseradish peroxidase-
tch plate, and a conjugated streptavidin was pipetted into individual wells.was poured on Fifteen minutes later, following a second series of three
solidify. Wet wash cycles with PBS-Tween 20, 100 pL1 of 2,2'-azino-di(3-ditional 20-fold ethyl-benzthiazoline sulfonate) (ABTS; Kirkegaard and
J. CLIN. MICROBIOL.
on March 25, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

IMMUNOLOGICAL DETECTION OF T. VAGINALIS 553
Perry, Gaithersburg, Md.) was added to each well. After 10min the resulting green color produced was measured at 410nm in a microtiter plate reader. Results were also scored byan independent visual inspection of the plates before theabsorbance was measured.
All patient samples were run in duplicate, and a series ofT. vaginalis standard solutions was assayed in triplicate oneach of the five plates used to accommodate all 177 speci-mens. All samples with an absorbance equal to the meanplus 2 standard deviations of three negative controls run oneach plate were considered positive.
RESULTSDetection of T. vaginalis. A summary of the major findings
of this study are given in Table 1. Broth culture, monitoredfor the presence of motile trichomonads for up to 7 days,revealed that 84 (47.5%) of the 177 samples examined wereinfected with T. vaginalis. Approximately 37% (31 samples)of these trichomonad-containing specimens were correctlydiagnosed by the wet mount method, which was performedimmediately after sample collection. However, two speci-mens diagnosed as being positive for T. vaginalis could notbe confirmed by either broth or solid culture and weredeemed to be false-positive results. Thus, the specificity ofthe wet mount method in this setting was 97.8%. However,despite the fact that the samples were prediluted 20-fold withmodified Diamond medium prior to testing in the ELISA, theimmunoassay correctly identified 65 of the 84 positive sam-ples. Thus, the sensitivity of the assay with respect toculture was 77.4%; the specificity was 100%, as no false-positive results were observed.
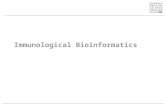
Assay response. The response of the 65 samples that werepositive for T. vaginalis antigen when assayed by ELISA ispresented in Fig. 2. A total of 58 of these samples displayedan optical density at 410 nm (OD410) greater than 0.2, while7 of the specimens yielded an OD410 assay response between0.1 and 0.2. This is significant when considering the assayresponse as a function of trichomonad concentration (insert,Fig. 2). The assay standard curve, which is given as themean response (+ standard deviation) of triplicate determi-nations on each of the five plates (or 15 determinations),shows that the overall assay response of the negative controlwas 0.091 + 0.008. Because ABTS appears colorless at anOD410 of <0.07 and only faintly blue-green at an OD410 of0.091, those seven samples with absorbance values between0.1 and 0.2 were easily discerned from the backgroundvalues with an ELISA plate reader and could be readilydistinguished by even a simple visual inspection.Comparison of the sensitivity of the ELISA with that of the
wet mount technique. The number of samples correctlyidentified by culture, the ELISA, and wet mount methodsplotted as a function of the level of trichomonads present inthe clinical specimen is shown in Fig. 3. The concentrationof organisms presented here represents undiluted, neat sam-ples. For the 81 broth culture-positive samples for whichquantitative culture data were obtained, several features of
TABLE 1. Detection of T. vaginalis in vaginal secretionsNo. correctly Sensitivity SpecificityMethod No. positive identifieda (%) (%)
Culture 84 84 100 100Wet mount 33 31 36.9 97.8ELISA 65 65b 77.4 100
a With respect to culture.b Samples for the ELISA were prediluted 1 to 20.
Assay Standard Curve
cnU1)
.0
,a)
Ez
.1-.2 .2-.3 .3-.4 .4-.5 .5-.6 .6-.7 .7-.8 .8-.9 .9-1.0 >1Assay Response (OD)
FIG. 2. Range of the measured absorbance values in positivesamples and assay response versus trichomonad concentration(insert). In total, 65 of the 177 clinical samples, prediluted 20-foldwith Diamond medium, were positive for T. vaginalis antigen whenassayed by ELISA. The range of assay responses observed for thesesamples is presented. The assay response as a function oftrichomonad concentration is given (insert). Data shown are themean response + standard deviation of triplicate determinations ofknown concentrations of organisms run on each of the five assayplates (or 15 determinations) employed; BKG is the backgroundobserved in the study.
the two assays are apparent. First, in general the wet mountis quite insensitive unless the sample contains on the order of100,000 trichomonads per ml, as only 2 of 40 (5%) of infectedspecimens were correctly diagnosed below that level. Sec-ond, despite the fact that the actual concentration of ELISA-positive samples was diluted 20-fold from that shown, theELISA correctly identified positive specimens in the 1,000-to 10,000-CFU/ml range in approximately 50% of the cases;above 10,000 CFU/ml, 58 of the 59 culture-positive sampleswere correctly identified (98.3%). These data suggest thatthe ELISA is capable of measuring trichomonads at levels atwhich the wet mount is demonstrably insensitive.
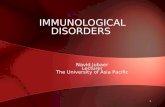
In total, 19 samples that were culture positive for T.vaginalis were not detected by the ELISA. Quantitativeculture data was available for 17 of these specimens, and thenumber of undetected samples as a function of the concen-tration of trichomonads in them is presented in Fig. 4. Theconcentration of organisms given is that in the undilutedsample, as shown in Fig. 3. With the exception of one samplecontaining >5,000 organisms per ml (i.e., 250 cells per ml asassayed), all the remaining specimens contained the organ-ism at concentrations after dilution below 250 cells per ml.
DISCUSSION
Many efforts to develop sensitive diagnostic tests fortrichomoniasis have been reported in recent years. Theseattempts followed the findings of Fouts and Krauss (9),whose work essentially invalidated the long-held view thatclinical symptoms were reliable indicators of trichomoniasis.
VOL. 24, 1986
on March 25, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

554 WATT ET AL.
-0 15 -
E
10-
1-2 2-3 3-4 4-5 5-6 6Log CFU/mL
FIG. 3. Detection of T. vaginalis antigens in 177 clinical speci-mens: a comparison of the sensitivity of broth culture, the wetmount procedure, and the ELISA as a function of trichomonadconcentration. The number of patients diagnosed as havingtrichomoniasis by the culture, ELISA, or wet mount techniques isplotted as a function of the quantitative number of organismspresent in the undiluted secretions, as described in the text. Of the65 ELISA-positive samples, 64 are represented here, one ELISA-positive sample could not be quantitated, as it did not grow in solidculture.
Using clinical presentation as the basis for diagnosis, theyreported that 88% of women with trichomoniasis wentundetected and an additional 29% of their patients weremisdiagnosed as having trichomoniasis.The sensitivity limitation of the wet mount, the most
prevalent method of diagnosis, is generally recognized.Various staining methods have been proposed (11, 13, 26,28, 32) in attempts to increase the sensitivity of microscopicexaminations of direct smears. These reports, however, areinconclusive. For example, one study (18) reported a four-fold increase in sensitivity (to approximately 80%) over wetmount when acridine orange staining followed by fluores-cence microscopy was used. Yet in a similar study, Green-wood and Kirk-Hillaire (11) observed little difference insensitivity between the wet mount technique and acridineorange staining. The primary utility of these methods lies inthe capability of deferring microscopic examination whichadversely effects the sensitivity and specificity of the wetmount due to the decreased motility of the protozoon.Another method often used is the visualization oftrichomonads on Papanicolaou smears. This method offers asensitivity of approximately 70% (28); however, the level ofsensitivity and specificity of this technique is also highlydependent on the skill of the cytologist.
Examination of sera or vaginal secretions for antibodies tothe parasite offers little promise of being of diagnostic utility(2, 20, 21, 29, 30), primarily because of the lack of correla-tion between the presence of antibodies and an activeinfection. Using indirect immunofluorescence microscopy,several investigators (20, 29) reported that while 80 to 90% ofpatients with trichomoniasis had circulating antibodies to the
protozoan, 13 to 17% of a control population of patients didalso. Their results in testing vaginal secretions for IgG or IgAantibodies to T. vaginalis were even less encouraging.
Currently, there are no reports in the literature in which anELISA is used for the detection of T. vaginalis antigens inclinical specimens. Here we have reported the developmentof a rapid, sensitive ELISA for the detection of T. vaginalisantigens in vaginal secretions. This assay was used todiagnose the presence of trichomonads in 177 clinical spec-imens, in which all of the samples were examined by wetmount and fractions of each specimen were cultured in abroth medium and microscopically examined up to 7 dayslater for the presence of T. vaginalis. Additionally, theconcentration of viable trichomonads in all but one positivesample was measured by a solid culture technique. Despitethe fact that fractions of individual samples were prediluted20-fold prior to testing in the ELISA, this procedure provedto be approximately twice as sensitive (77.4%) as the rou-tinely used wet mount (36.9%). Furthermore, the ELISAwas capable of detecting the protozoan at concentrations ofthe organism that were demonstrably below the level ofsensitivity of the wet mount. It is noteworthy that byextrapolating from the assay response as a function oftrichomonad concentration plotted in Fig. 2, we estimatethat 79 samples would have been correctly identified, if theyhad not been prediluted, yielding a sensitivity of about 94%.This figure is certainly only an approximation, as assayperformance on patient specimens was not observed to beabsolutely quantitative. Possible explanations for this phe-nomenon include fine differences in antigenicity from strainto strain and blocking effects due to the presence oftrichomonad-specific secretory IgA.Although several investigators have generated monoclonal
antibodies to T. vaginalis (6, 16), we utilized affinity-purifiedpolyclonal antibodies for several reasons. There is a currentlack of information concerning the antigenic relatedness ofvarious strains of T. vaginalis (4). No differences in antigeniccomposition were observed among several pathogenicstrains of T. vaginalis by sodium dodecyl sulfate-poly-acrylamide gel electrophoresis (1, 10; S. M. Wos and R. M.Watt, unpublished data) and fluorography (1), and commonreactivity with certain trichomonad antigens has been seenwhen patient sera is used to probe Western blots of solubil-
<100____ Viable T Vaginalis
100-500 Km
-j
U-
500-1000
1000-2500
2500-5004
> 5004
O
1 1I '0 1 2 3 4
# of Patients
FIG. 4. ELISA of 177 clinical specimens: a summary of thetrichomonad-positive samples undetected by the assay. Nineteensamples that were culture positive for T. vaginalis were not detectedby the ELISA. The undiluted levels of trichomonads in 17 of thesespecimens for which quantitative culture data were obtained areshown. Aside from one sample with >5,000 organisms per ml (i.e.,250 cells per ml as assayed), all the remaining samples contained<250 cells per ml.
J. CLIN. MICROBIOL.
on March 25, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

IMMUNOLOGICAL DETECTION OF T. VAGINALIS 555
ized trichomonads (10; S. M. Wos and R. M. Watt, submit-ted for publication). However, heterogeneity among theorganisms has been observed by several serologic-basedtechniques including ELISA (2, 3), indirect immunofluores-cence (16, 31, 33), and radioimmunoprecipitation (3). Al-though investigators are currently studying the antigeniccomposition of the organism with monoclonal antibodies (6,16), data from these reports indicate that obtaining a singlemonoclonal antibody which recognizes all isolates of theorganism could prove to be problematic. In addition, thetwo-site design of our assay requires antibodies with goodaffinity both bound to the solid phase and as detectors insolution in contrast to one-site assays developed for detect-ing the protozoan (e.g., immunofluorescence) (16). Thus, theuse of polyclonal antisera eliminates the possible need of a
second reagent. Finally, a sufficiently specific ELISA to theflagellated protozoan Giardia lamblia has been reported withpolyclonal antibodies (34), engendering confidence that an
analogous approach to another flagellate could prove fruit-ful. The data presented here indicate that an ELISA used forantigen detection is rapid, easy to perform, and providessuperior sensitivity over the wet mount method. The utilityof such a format would be a major step in diagnosingtrichomoniasis.
ACKNOWLEDGMENTS
We thank R. G. Charrar, H. Heineman, and M. Goldberg of theCity of Philadelphia, Department of Health, Sexually TransmittedDisease Clinic No. 1, for assistance in providing the patieht speci-mens. We also thank Christine A. Sieracki for excellent technicalassistance.
LITERATURE CITED1. Alderete, J. F. 1983. Antigen analysis of several pathogenic
strains of Trichlononas vaginalis. Infect. Immun. 39:1041-1047.2. Alderete, J. F. 1984. Enzyme linked immunosorbent assay for
detecting antibody to Trichomonas vaginalis: use of whole cellsand aqueous extract as antigen. Br. J. Vener. Dis. 60:164-170.
3. Alderete, J. F., L. Suprun-Brown, L. Kasmala, J. Smith, and M.Spence. 1985. Heterogeneity of Trichomonas vaginalis anddiscrimination among trichomonal isolates and subpopulationswith sera of patients and experimentally infected mice. Infect.Immun. 49:463-468.
4. Attilio de Carli, G. 1983. Antigenic comparison betweenTritrichomnonas sluis, T. foetius, Trichomnonas vaginalis, and T.gallinae by gel immunodiffusion. Rev. Microbiol. (Sao Paulo)14:122-128.
5. Bennett, B. D., J. Bailey, and W. A. Gardner. 1980. Immuno-cytochemical identification of trichomoniasis. Arch. Pathol.Lab. Med. 104:247-249.
6. Connelly, R. B., B. E. Torian, and H. H. Stibbs. 1985. Identifi-cation of a surface antigen of Tric/homonas vaginalis. Infect.Immun. 49:270-274.
7. Cuatrecasas, P., and C. B. Anfinsen. 1971. Affinity chromatog-raphy. Methods Enzymol. 2:345-378.
8. Diamond, L. S. 1957. The establishment of various tricho-monads of animals and man in axenic cultures. J. Parasitol.43:488-490.
9. Fouts, A. C., and S. J. Kraus. 1980. Tric/homnonas vaginalis:re-evaluation of its clinical presentation and laboratory diagno-sis. J. Infect. Dis. 141:137-143.
10. Garber, G. E., E. M. Proctor, and W. R. Bowie. 1986. Immu-nogenic proteins of Tric/hononas vaginalis as demonstrated bythe immunoblot technique. Infect. Immun. 51:250-253.
11. Greenwood, J. R., and K. Kirk-Hillaire. 1981. Evaluation ofacridine orange stain for detection of Trichomnonas vagingalis invaginal specimens. J. Clin. Microbiol. 14:699.
12. Hersh, S. M. 1985. Pulmonary trichomoniasis and Tric/hononastenax. J. Med. Microbiol. 20:1-10.
13. Hipp, S. S., M. W. Kirkwood, and H. A. Gaafar. 1980. Screen-ing for Trichotnonas vaginalis infection by use of acridineorange fluorescent microscopy. Sex. Transm. Dis. 6:235-238.
14. Ivey, M. H. 1961. Characteristics of clones of Tric/homonasvaginalis on solid medium. J. Parasitol. 28:363-379.
15. Judson, F. N. 1981. Epidemiology and control of nongonococcalurethritis and genital chlamydial infections: a review. Sex.Transm. Dis. 8:117-126.
16. Krieger, J. N., K. K. Holmes, M. R. Spence, M. F. Rein, W. M.McCormack, and M. R. Tam. 1985. Geographic variationamong isolates of Trichotnonas vaginalis: demonstration ofantigenic heterogeneity by using monoclonal antibodies and theindirect immunofluorescence technique. J. Infect. Dis. 152:979-984.
17. Laemmli, U. K. 1970. Cleavage of structural proteins during theassembly of the head of bacteriophage T4. Nature (London)227:680-685.
18. Levett, P. N. 1980. A comparison of five methods for thedetection of Trichoinonas laginalis in clinical specimens. Med.Lab. Sci. 37:85-88.
19. Lowry, 0. H., N. J. Rosebrough, A. L. Farr, and R. J. Randall.1951. Protein measurements with the Folin phenol reagent. J.Biol. Chem. 193:265-275.
20. Mason, P. R. 1979. Serodiagnosis of Trichoinonas vaginalisinfection by the indirect fluorescent antibody method. J. Clin.Pathol. 32:1211-1215.
21. Mathews, H. M., and G. R. Healy. 1983. Evaluation of twoserological tests for Trichotnonas va ginalis infection. J. Clin.Microbiol. 17:840-843.
22. McLaren, L. C., L. E. Davis, G. R. Healy, and C. G. James.1983. Isolation of Trichomnonas vaginalis from the respiratorytract of infants with respiratory disease. Pediatrics 71:888-890.
23. O'Hara, C. M., W. A. Gardner, and B. D. Bennett. 1980.Immunoperoxidase staining of Trichoinonas vaginalis in cyto-logic material. Acta Cytol. 24:448-451.
24. Rein, M. F., and T. A. Chapel. 1975. Trichomoniasis, candi-diasis, and the minor venereal diseases. Clin. Obstet. Gynecol.18:73-88.
25. Rein, M. F., and M. Muller. 1984. Trichotnonas vaginalis. p.525-536. In K. K. Holmes, P.-A. Mardh, P. F. Sparling, andP. J. Wiesner (ed.), Sexually transmitted diseases. McGraw-Hill, New York.
26. Ridge, A. G. 1982. A rapid method for detection of Trichomonasvaginalis. Med. Lab. Sci. 39:193-194.
27. Schmid, G. P., and S. A. Larsen. 1984. Finding the elusive T.vaginalis. Diag. Med. Nov-Dec:38-40.
28. Spence, M. R., D. H. Hollander, J. Smith, L. McCaig, D. Sewell,and M. Brockman. 1980. The clinical and laboratory diagnosis ofTric/hoinonas vaginalis infection. Sex. Transm. Dis. 7:168-171.
29. Street, D. A., D. Taylor-Robinson, J. P. Ackers, N. F. Hanna,and A. McMillan. 1982. Evaluation of an enzyme-linked immu-nosorbent assay for the detection of antibody to Trichomonasvaginalis in sera and vaginal secretions. Br. J. Vener. Dis.58:330-333.
30. Su, K. E. 1982. Antibody to Tric/homonas vaginalis in humancervicovaginal secretions. Infect. Immun. 37:852-857.
31. Su-Lin, K. E., and B. M. Honigberg. 1983. Antigenic analysis ofTric/homnonas vaginalis strains by quantitative fluorescent anti-body methods. Zentralbl. Bakteriol. Parasitenkd. Infektionskr.Hyg. Abt. 1 Orig. Reihe A 69:161-181.
32. Szmarch, H., E. MaLyszko, A. Wronski, and E. Niczyporuk.1983. Diagnostic and epidemiologic significance of multinuclearand round forms of Trichoinonas vaginalis. Z. Hautkr. 58:1179-1182.
33. Torian, B. E., R. J. Connelly, R. S. Stephens, and H. H. Stibbs.1984. Specific and common antigens of Tricho,nonas vaginalisdetected by monoclonal antibodies. Infect. Immun. 43:270-275.
34. Ungar, B. L. P., R. H. Yoelken, T. E. Nash, and T. C. Quinn.1984. Enzyme-linked immunosorbent assay for the detection ofGia-dia l/anblia in fecal specimens. J. Infect. Dis. 149:90-97.
VOL. 24, 1986
on March 25, 2020 by guest
http://jcm.asm
.org/D
ownloaded from