Immunological Diseases
27
Navid Jubaer Lecturer The University of Asia Pacific IMMUNOLOGICAL DISORDERS 1
-
Upload
navid-jubaer -
Category
Healthcare
-
view
421 -
download
1
Transcript of Immunological Diseases

Navid JubaerLecturer
The University of Asia Pacific
IMMUNOLOGICAL DISORDERS
1

2
An immune disorder is a dysfunction of the immune system. These disorders can be characterized in several different ways:
• By the component(s) of the immune system affected
• By whether the immune system is overactive or underactive
• By whether the condition is congenital or acquired
IMMUNOLOGICAL DISORDER

3
Definition:
A state of altered reactivity in which the body reacts with an exaggerated immune response to what is perceived as a foreign substance.
Immune response that results in tissue injury or other physiological changes are called hypersensitivity (allergic) reactions”.
HYPERSENSITIVITY (ALLERGY)

4
Hypersensitivity reactions are classified into four types:
• Type I: Anaphylactic hypersensitivity
• Type II: Cytotoxic hypersensitivity
• Type III: Immune complex hypersensitivity
• Type IV: Cell mediated hypersensitivity
TYPES OF HYPERSENSITIVITY REACTIONS

5
• It is an immediate reaction beginning within minutes of exposure to an antigen.
• It is mediated by antibodies.
• It requires previous exposure to specific antigen.
• It usually affects on skin, lungs and gastrointestinal tract.
• Examples:– Asthma– Allergic rhinitis– Systemic anaphylaxis.– Atopic dermatitis
TYPE I: ANAPHYLACTIC HYPERSENSITIVITY:

6
Anaphylactic (type I) Hypersensitivity

7
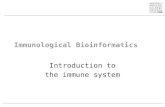
• It occurs when the system mistakenly identifies a normal constituent of the body as foreign.
• This reaction may be a result of cross-reacting antibody, possibly leading to cell and tissue damage
• It involves activation of complement by IgG or IgM antibody binding to an antigenic cell.
Examples:
• Myasthenia gravis
• Thrombocytopenia
TYPE II: CYTOTOXIC HYPERSENSITIVITY

Pathogenesis of type II hypersensitivity8
Cytotoxic (type Il) Hypersensitivity

9
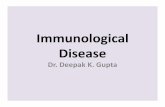
• It involves in the formation of immune complexes when antigen binds to antibodies.
• These type III complexes deposit in tissues or vascular endothelium and leads to injury with the help of vasoactive amines and the increase number of circulating complexes.
• The joints and kidneys are particularly susceptible.
Examples:
• Systemic lupus erythematous
• Rheumatoid arthritis
• Serum sickness
TYPE III: IMMUNE COMPLEX HYPERSENSITIVITY

10
IMMUNE COMPLEX (TYPE III) HYPERSENSITIVITY
Pathogenesis of type III hypersensitivity

11
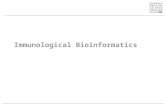
• Also known as cellular hypersensitivity
• It occurs 24-72 hrs after exposure to an allergen
• The reaction is mediated by sensitized T cells and macrophages.
• The reaction results In tissue damage by releasing lymphokines, macrophages and lysozymes.
Examples:
• Contact dermatitis
• Tuberculin test.
TYPE IV: CELL MEDIATED HYPERSENSITIVITY

12
CELL MEDIATED (TYPE IV) HYPERSENSITIVITY
Pathogenesis of type IV hypersensitivity

13
It is also called as Hay FeverDefinition: It is an inflammation of the nasal mucosa by an allergen.
ALLERGIC RHINITIS

PATHOGENESIS: ALLERGIC RHINITIS
14
Inhalation of an antigen (sensitization)
Re-exposure
Nasal mucosa reacts (histamine is mediator)
Slowing of ciliary action, edema formation and leukocyte infiltration
Tissue edema and increase capillary permeability (vasodilatation).

15
Clinical manifestations:• Nasal congestion• Clear to greenish rhinorrhea• Intermittent sneezing and nasal itching• Headache • Epistaxis• Fatigue, loss of sleep and poor coordination.
Medical management:• Oral anti histamines (blocks the action of histamine)• Nasal decongestant• Mast cell stabilizers.• Analgesics and antipyretics.

ATOPIC DERMATITIS (ECZEMA)
16
Definition:Inflammation of the skin
Incidences/Causes:• Familial tendency
• It is highest in infants and children
• 1% population is suffering from this disease
• Aggravated in low humidity and in winter.

PATHOPHYSIOLOGY: ATOPIC DERMATITIS
17
Allergen /Sensitizing antigen
Affect the skin (changes in lipid content, sebaceous gland activity and sweating)
Reduced water-binding capacity of the skin
Higher trans epidermal water loss and decreased water content
Dry skin
Itching, rubbing leads to infection

18
Clinical manifestations: Atopic dermatitis
• Red oozing crusting rash (in childhood)• Dry thick brownish – grey and scaly skin (later
stage)• Pruritus• Lesion are mostly found on hand, foot, back of
the knees, neck, face, eyelids and elbow bands.
Medical Management: Atopic dermatitis • Moisturizers• Antibiotics• Antihistamines

19
AnaphylaxisDefinition:It is an immediate life threatening systemic reaction that can occur on exposure to particular substances
It is an immediate (type I hypersensitivity) immunologic reaction, results from IgE antibody
This reaction affects many tissues and organs. Death may occur due to respiratory tract spasm and constriction or collapse.
Causes
• Food ( peanuts, fish, milk, eggs, wheat and chocolate).
• Medications (penicillin, NSAID’s)
• Insects stings (bees, ants)

20
Pathophysiology: Anaphylaxis
Interaction of foreign antigen with IgE antibodies
Release of histamine
Activation of platelets, eosinophils and neutrophils
smooth muscle spasm, bronchospasm, mucosal edema and inflammation.

Mild Moderate Severe
Occurs within first 2hrs of exposure
Same Same
Peripheral tingling Flushing Bronchospasm
Sensation of warmth
Itching Laryngeal edema
Fullness in mouth and throat
Bronchospasm Severe Dyspnea, cyanosis
Nasal congestion Edema of larynx Hypotension
Periorbital swelling
Dyspnea Cardiac arrest and coma may follow.
Pruiritus Cough
Sneezing wheezing
21
Clinical manifestations: Anaphylaxis

22
Medical management: Anaphylaxis
1. If cardiac arrest then cardiopulmonary resuscitation initiated.
2. Antihistamine to prevent recurrence reaction3. Start intravenous fluids to maintain hemodynamics.4. Give aminophylline for bronchospasm

23
• Transplant rejection occurs when transplanted tissue is rejected by the recipient's immune system, which destroys the transplanted tissue.
• Transplantation can be:
autologous (own)
homologous (alogenic) - human tissue
heterologous - animal tissue (pig skin, ovine pericardium)
TRANSPLANTATION REJECTION

24
• hyperacute (Ab mediated) - widespread arteriolitis, arteritis, ischemic necrosis (minutes-hours)
• acute (cell mediated) - vasculitis, tubulitis, edema (days-months)
• chronic - vascular changes - sclerosis, intimal fibrosis (months-years)
REJECTION REACTIONS

25
• GVHD happens when particular types of white blood cell (T cells) in the donated bone marrow or stem cells attack host body cells. This happens because the donated cells (the graft) see the body cells (the host) as foreign and attack them.
• It is difficult to say who will develop GVHD after a transplant. We don’t know exactly, but somewhere between 1 and 4 out of every 5 people (20 to 80%) having a donor transplant will develop some degree of GVHD. Some people have a very mild form which doesn’t last long. For others, GVHD can be severe. It may even be life threatening in a few cases. Some people may have GVHD over many months, or even years.
GRAFT VERSUS HOST DISEASE

26
• GVHD happens because the transplant affects your immune system. The donor's bone marrow or stem cells will contain some T cells. T cells are a type of white blood cell that help us fight infections. T cells attack and destroy cells they see as foreign, and potentially harmful, such as bacteria and viruses. Normally T cells don’t attack our own body cells, because they recognize proteins on the cells called HLA (human leukocyte antigens). We inherit our HLA from our parents. Apart from identical twins HLA is unique to each person.
• Before a bone marrow or stem cell transplant, you and your donor have blood tests to check how closely your HLA matches. This test is called tissue typing. If you and your donor have very similar HLA this lowers the chance of GVHD. The more differences there are between your HLA and your donor's, the more likely you are to get GVHD.
• After a transplant your bone marrow starts making new blood cells from the donor stem cells. These new blood cells have the donor's HLA pattern. They recognize the HLA pattern on your body cells as different (foreign) and may begin to attack some of them. The GVHD may affect different areas of your body. Most commonly it affects the
• Skin
• Digestive system (including the bowel and stomach)
• Liver
HOW GVHD DEVELOPS

27
THANK YOU