
RAMAN SINGH, M.D. MEDICAL / MENTAL HEALTH DIRECTOR LOUISIANA DEPARTMENT OF PUBLIC SAFETY &...
17
RAMAN SINGH, M.D. MEDICAL / MENTAL HEALTH DIRECTOR LOUISIANA DEPARTMENT OF PUBLIC SAFETY & CORRECTIONS Medicaid Maximization & Criminal Justice Involved Individuals
-
Upload
leonardo-brummel -
Category
Documents
-
view
212 -
download
0
Transcript of RAMAN SINGH, M.D. MEDICAL / MENTAL HEALTH DIRECTOR LOUISIANA DEPARTMENT OF PUBLIC SAFETY &...

RAMAN SINGH, M.D. MEDICAL / MENTAL HEALTH DIRECTOR LOUISIANA DEPARTMENT OF PUBLIC SAFETY & CORRECTIONS
Medicaid Maximization &Criminal Justice
Involved Individuals
Medicaid was created on July 30, 1965, through Title XIX of the Social Security Act.
Each state administers its own Medicaid program while the federal Centers for Medicare and Medicaid Services (CMS) monitors the state-run programs and establishes requirements for service delivery, quality, funding, and eligibility standards.

Who is eligible for Medicaid?FPG(Federal Poverty
Guidelines)and any of the following:
Aged – 65 or olderBlind Pregnant Woman needing treatment for breast cancer
Disabled – meet Social Security Administration’s (SSA) disability criteria

Medicaid and Offender Population FFP not available for un allowable
services Upon incarceration Medicaid is
suspended. Termination or suspension
Term Definition
Inmate An individual confined involuntary or serving time for a criminal offense in state or federal prisons, jails, detention facilities or other penal facilities.

Exceptions to the rule
Health care for offenders is the responsibility of the institution housing the offenders .
Any federal dollar ( FFP)can not be claimed for offender care except in the following circumstances: Infants living with the inmate in the public institution Paroled individuals Inmates who become inpatients of a hospital, nursing
facility or intermediate care facility ( subject to meeting other requirements of the State’s Medicaid program)
50% of the administrative cost for the discharge planning for otherwise eligible offenders

Louisiana Offender Population
Offender Type/Location Number
DOC Offenders in State Facilities 18,723
DOC Offender in Local Facilities 21,327
Parish Offenders in Local Facilities 2,737
Pre-Trial Offenders in Parish Prison 21,199
Juveniles (OJJ) 436
Probation & Parole 69,845
Total 134,267

Snapshot of Prisoner Population Highest incarceration rate in world Louisiana has a very high rate of PLWHA, we sit
in the cancer belt, and have one of the worst obesity problems leading to a higher number of heart disease and strokes.
So offenders show similar trends. Staggering numbers of individuals are
incarcerated who have; serious mental health conditions, multiple risk factors for heart conditions, cancers and infectious diseases who lacked access to health care before their incarceration.
The number of elderly offenders is growing at an alarming rate, further burdening already strained state budgets. Offenders 50 or older comprises 25% of Louisiana DOC population.

Current Chronic Illnesses Diagnosed in Louisiana DOC run Prisons (average age: 43 years)
Disease for Year 2012 Number Diagnosed / Percentage of Population in DOC facilities
Hypertension 5,409 30%
Diabetes 1,300 7%
Cancer 211 1.2%
Heart Disease 305 2%
Pulmonary Disease 1,196 7%
HIV + 525 3%
Serious Mental Illness 3,332 18%
Substance Abuse 13,480 73%

Advantages of Medicaid : Advantages of Medicaid : Access and costAccess and cost

Pre-Incarceration
Lafayette – Mental Health Courts
Act 389Diversion Program

During
Incarceration
In patient stay coveredFiscal year 2012/2013 1,070 off-site admits, 3,042 on-site admissions
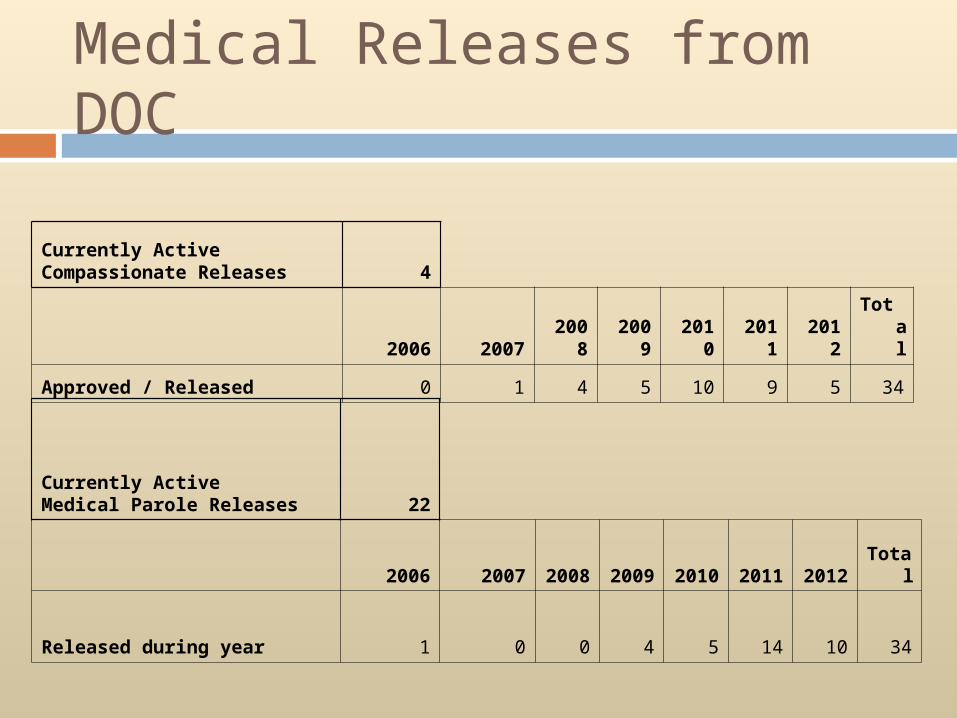
Currently Active Compassionate Releases 4
2006 2007 2008 2009 2010 2011 2012Tota
l
Approved / Released 0 1 4 5 10 9 5 34
Currently Active Medical Parole Releases 22
2006 2007 2008 2009 2010 2011 2012 Total
Released during year 1 0 0 4 5 14 10 34
Medical Releases from DOC

Release Planning / Release Planning / Reentry Reentry
DOC releases approximately 15,000 DOC releases approximately 15,000 offenders per year.offenders per year.
DOC is engaged with with community DOC is engaged with with community mental health providers and Medicaid mental health providers and Medicaid providers for a seamless transition for providers for a seamless transition for offenders upon release.offenders upon release.
Common drug formulary for prisons, Common drug formulary for prisons, jails, mental health and Medicaid.jails, mental health and Medicaid.
Pre-release conferencing to assure Pre-release conferencing to assure services are readily available to the services are readily available to the most seriously mentally ill.most seriously mentally ill.

Multi-Agency Multi-Agency CollaborationsCollaborations
OBH and DOC collaboration for expedited OBH and DOC collaboration for expedited mental health services for releasing mental health services for releasing offender with severe mental illnessoffender with severe mental illness
DHH and DOC worked together to expand DHH and DOC worked together to expand and improve the Medicaid application and improve the Medicaid application process for releasing offendersprocess for releasing offenders
DHH and DOC data exchange placing DHH and DOC data exchange placing Medicaid services on hold for incarcerated Medicaid services on hold for incarcerated offenders offenders
SSA and DOC collaborate to improve the SSA and DOC collaborate to improve the application process for releasing offendersapplication process for releasing offenders
DCI Discharge Program for releasing DCI Discharge Program for releasing offendersoffenders

Article: Medicaid for Prisoners http://www.pewstates.org/projects/stateline/headlines/states-missi
ng-out-on-millions-in-medicaid-for-prisoners-85899485969 So far, only Arkansas, California, Colorado, Delaware, Louisiana,
Michigan, Mississippi, Nebraska, North Carolina, Oklahoma, Pennsylvania, Washington and some scattered local governments are tapping Medicaid to pay for inpatient medical and nursing home care. A few more states are looking into it, including Georgia, Massachusetts, Minnesota, New Mexico, New York and Virginia.
Only a dozen states have taken advantage of a long-standing option to stick the federal government with at least half the cost of hospitalizations and nursing home stays of state prison inmates.
The other states have left tens of millions of federal dollars on the table, either because they didn’t know about a federal rule dating to 1997 or they were unable to write the laws and administrative processes to take advantage of it.

Impact of ACA
CMS is not changing the exceptions when FFP is allowed for actively incarcerated offenders.
Discharge planning and continuity of care
Mental health parity

And Going Forward……


















