RAKHI RAJENDRAN
56
ASSESSMENT OF KNOWLEDGE OF PATIENTS WHO HAVE UNDERGONE MECHANICAL VALVE REPLACEMENT ABOUT HOMECARE MANAGEMENT PROJE_CT REPORT Submitted in partial fulfillment of requirements for Diploma in Cardiovascular and Thoracic Nursing. RAKHI RAJENDRAN CODE NO: 5879 SREE CHITA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY TRIVANDRUM 2009
Transcript of RAKHI RAJENDRAN
ASSESSMENT OF KNOWLEDGE OF PATIENTS WHO HAVE
UNDERGONE MECHANICAL VALVE REPLACEMENT ABOUT
HOMECARE MANAGEMENT
PROJE_CT REPORT
Submitted in partial fulfillment of requirements for Diploma in Cardiovascular and Thoracic Nursing.
RAKHI RAJENDRAN CODE NO: 5879
SREE CHITA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY TRIVANDRUM
2009
CERTIFICATE FROM SUPERVISORY GUIDE
This is to certify that Miss.Rakhi Rajendran has completed the project work on
the 'Assessment of knowledge of patients after mechanical valve replacement about
homecare management' under my direct supervision and guidance for !he partial
fulfillment of the Diploma in Cardiovascular and Thoracic Nursing in the university of
SCTIMST, Trivandrum.
It is also certified that no part of the report has been included in any other thesis
for procuring any other degree by the candidate.
Dr. P.P.Saramma
Senior Lecturer in Nursing
SCTIMST
Trivandrum
October 2009
CERTIFICATE FROM THE CANDIDATE
This is to certify that the assessment of knowledge of patients after mechanical
valve replacement about homecare management is a genuine work done by me, at
SCTIMST Trivandrum under the guidance of Dr.P.P.Sarainma. It is also certified that
this work has not been presented for award of degree, diploma or other recognition.
Trivandrum
October 2009
Miss.Rakhi Rajendran
Code No: 5879
SCTIMST
APPROVAL SHEET
This is to certify that Miss.Rakhi Rajendran bearing the code no: 5879 has been
admitted to the Diploma in Cardiovascular and Thoracic Nursing in January 2009 and has
undertaken the project entitled 'Assessm_ent of knowledge of patients after mechanical
valve replacement about the /zomecare management' which is approved for the Diploma
in Cardiovascular and Thoracic Nursing awarded by SCTIMST, Trivandrum, and it is
found satisfactory.
Examiners:
Guide:
Trivandrum October 2009
ACKNOWLEDGEMENT
First of all let me thank God almighty for the unending love, care and blessing
especially during the tenure of this study.
I take this opportunity to express my sincere gratitude to Dr. Saramma.P.P, Senior
Lecturer in Nursing, SCTIMST, Trivandrum for the guidelines she provided for
executing this study. Her advice regarding the concept, basic guidelines and analysis of
data was very much encouraging. Her contributions and suggestions have been a great
help for which I am extremely grateful.
With profound sentiments and gratitude I acknowledge the encouragement and
help received from the following persons for the successful completion of the study.
I am thankful to all the sisters in the Cardiac Surgical ICU and wards for their
constant support and encouragement.
I am extremely grateful to the participants of the study, who gave their valuable
time during data collection.
I thank all my friends and colleagues who directly or indirectly supported me in
completing this study.
CONTENTS
-Chapter No TITLE Page No
I INTRODUCTION 1
1.1 Introduction 1 .
1.2 Background of the study . 4
1.3 Need and significance of the study 6
1.4 Statement of the problem 7
1.5 Objectives of the study
7
1.6 Operatim:ml definitions 8
1.7 -. . Delimitations 9
1.8 Study setting
9
1.9 Study method 9
1.10 Sampling 9
1.11 Sample size 9
1.12 Tool 10
1.13 Organization 10
II REVIEW OF LITERATURE 11
2.1 Knowledge assessment of patients regarding valve
11 - replacement
2.2 Diet and warfarin therapy 12
2.3 Prevention of complications after mechanical valve 13
replacement
2.4 Discharge planning and follow up 16
III METHODOLOGY 20
3.1 Introduction 20
3.2 Research approach 20
3.3 Setting of the study 20
3.4 Study population 20
3.5 Sample and sampling technique 20 --
3.6 Exclusion criteria 21
3.7 Inclusion criteria 21
3.8 Development of the tool 21
3.9 Description of the tool 21
3.10 Pilot study 22
3.11 Data collection procedure 22
3.12 Plan of analysis 22
3.13 Summary 22
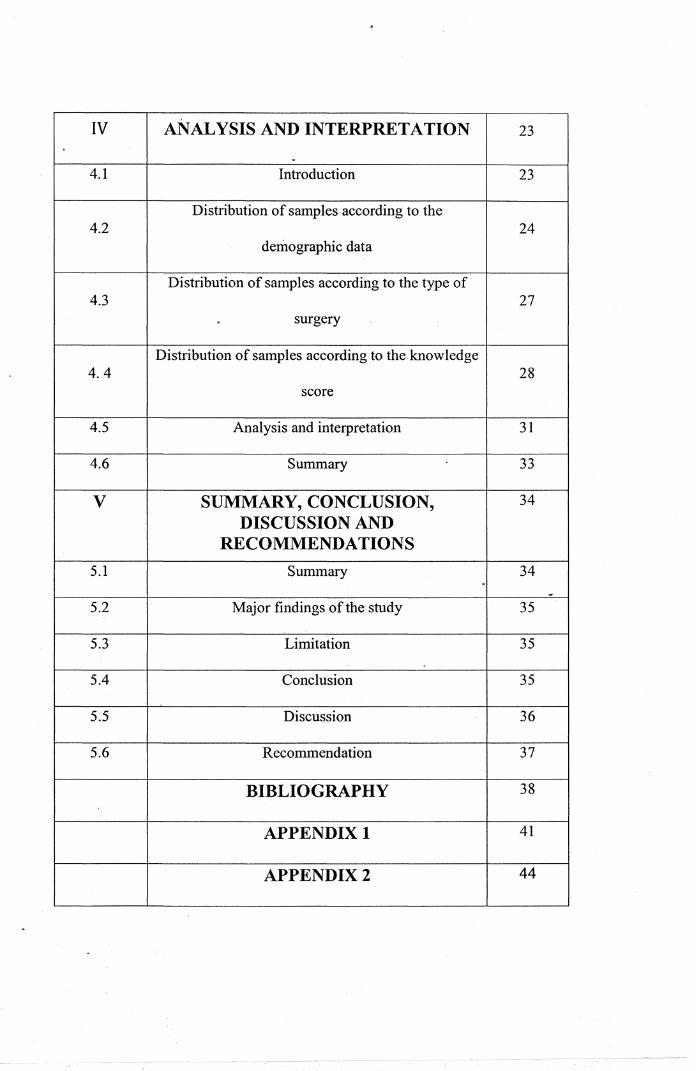
IV ANALYSIS AND INTERPRETATION 23
. 4.1 Introduction 23
Distribution of samples according to the 4.2 24
demographic data
Distribution of samples according to the type of 4.3 27
. surgery
Distribution of samples according to the knowledge 4.4 28
score
4.5 Analysis and interpretation 31
4.6 Summary 33
v SUMMARY, CONCLUSION, 34
DISCUSSION AND RECOMMENDATIONS
5.1 Summary 34 .
-5.2 Major findings of the study 35
5.3 Limitation 35
5.4 Conclusion 35
5.5 Discussion 36
5.6 Recommendation 37
BIBLIOGRAPHY 38
APPENDIX 1 41
APPENDIX2 44
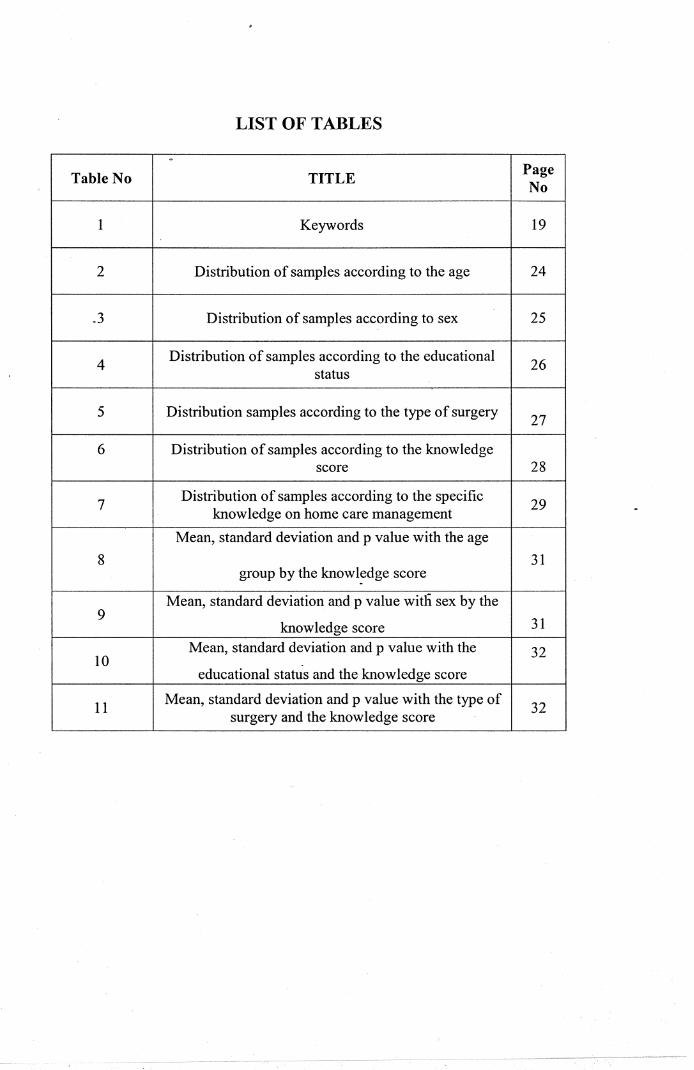
LIST OF TABLES
.
Table No TITLE Page No
1 Keywords 19
2 Distribution of samples according to the age 24
.3 Distribution of samples according to sex 25
4 Distribution of samples according to the educational 26
status
5 Distribution samples according to the type of surgery 27
6 Distribution of samples according to the knowledge score 28
7 Distribution of samples according to the specific 29
know ledge on home care management
Mean, standard deviation and p value with the age
8 31 group by the know ledge score
Mean, standard deviation and p value with sex by the 9 31 knowledge score
10 Mean, standard deviation and p value with the 32
educational status and the knowledge score
11 Mean, standard deviation and p value with the type of 32
surgery and the knowledge score
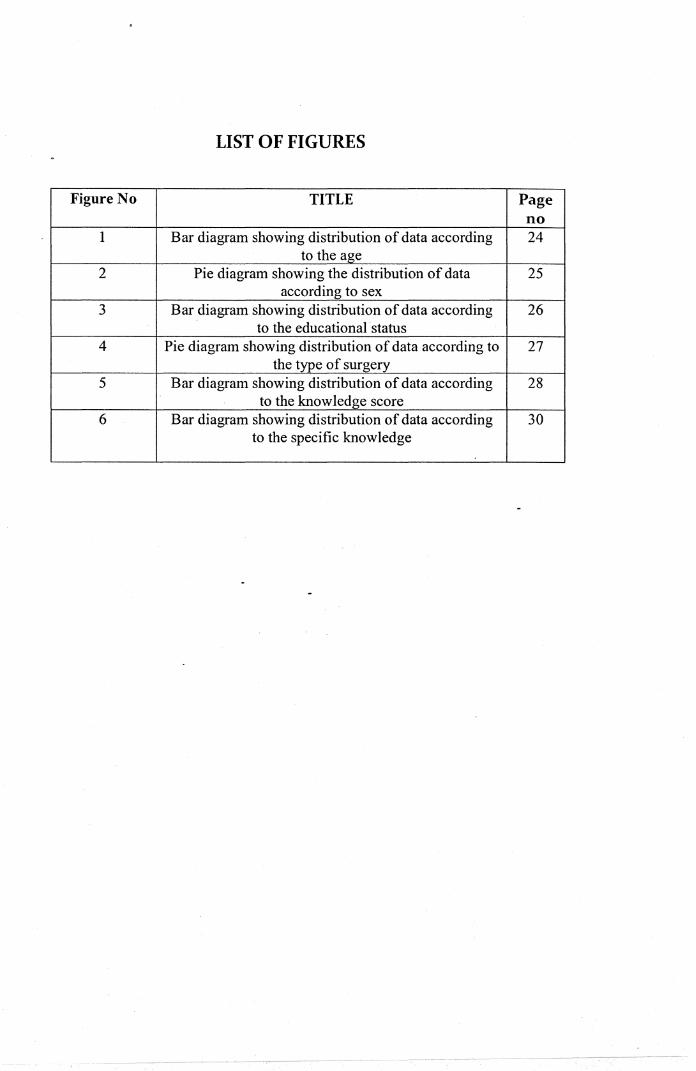
LIST OF FIGURES
Figure No TITLE Page no
1 Bar diagram showing distribution of data according 24 to the age
2 Pie diagram showing the distribution of data 25 according to sex
3 Bar diagram showing distribution of data according 26 to the educational status
4 Pie diagram showing distribution of data according to 27 the type of surgery
5 Bar diagram showing distribution of data according 28 to the knowledge score
6 Bar diagram showing distribution of data according 30 to the specific knowledge
1.1 Introduction
1
CHAPTER-1
INTRODUCTION
Valvular heart disease is a significant health problem in United States although it
is far less common than coronary artery disease. It is characterized by impaired function
of one or more of the four cardiac valves. Either or both of the two functional
abnormalities may be present: stenosis or regurgitation, Finkelmeier.B.A. (2000).
Primary valvular heart disease ranks well below coronary heart disease, stroke,
hypertension, obesity and diabetes as major threats to the public health. Nevertheless, it is
the source of significant morbidity and mortality. Rheumatic fever is the dominant cause
of valvular heart disease in developing countries. Its prevalence has been estimated to
range from as low as 1.01100000 school age children Costa Rica to as high as 150/100000
in China. RHD accounts for 12 to 65 % of hospital admissions related to cardiovascular
diseases and 2 to 10 % hospital discharges in some developing countries. Prevalence and
mortality rates vary among communities even within the same country as a function
crowding and the availability of medical resources and population wide programmes for
detection and treatment of Group A Streptococcal pharyngitis. In economically deprived .
areas, tropical and subtropical climates particularly on Indian subcontinent, Central
America and Middle East, Rheumatic valvular disease progresses more rapidly than in
more developed nations and frequently causes serious symptoms in patients less than 20
years of age. This accelerated natural history may be due to repeated infections with more
virulent strains of rheumatogenic Streptococci. Tricuspid stenosis, as relatively
1
2
uncommon valvular lesion in North America and Western Europe is more common in
tropical and subtropical climates especially in Southern Asia and in Latin America.
As the year of 2000, worldwide death rates for RHD approximated 5.5/ 100000
population with the highest rates reported from Southern Asia. Although there have been
reported cases of isolated outbreaks of Streptococcal infection in North America, valve
disease in developed countries is now dominated by degenerative or inflammatory
processes hat lead to valve thickening, calcification and dysfunction. The prevalence of
VHD increases with age. Important left sided valve disease may affect as many as 12 to
13% of adults over the age of 75. The incidence of Infective Endocarditis has increased
with the aging of the population, the more widespread prevalence of valve grafts and
intra cardiac devices, the emergence of more virulent multi drug resistant
microorganisms, and the growing epidemic of diabetes. I.E. has become a more frequent
cause of acute valvular regurgitation. Bicuspid aortic valve disease affects as many as 1 to
2 % of population, and an increasing number of childhood survivors of Congenital Heart
Diseases present later in life with valvular dysfunction: The past several years have
witnessed significant improvements in surgical outcomes with progressive refinement o.f
relatively less- invasive techniques; Bonow et al (2006) Circulation 114: 450.
The results of replacement of any valve are dependent primarily on ( 1 ). The
patients' myocardial function and general medical condition at the time of surgery;
(2). Technical abilities of the operative team and the quality of the postoperative care;
and (3). The durability, haemodynamic characteristics and thrombogenicity of the
prosthesis. Increased perioperative mortality is associated with advance age and co
morbidity ( eg: pulmonary or renal disease, the need for nonvalvular cardiovascular
2
--~ ·--------·--··--··-~-~---------··-··----·--------,------
3
surgery, diabetes mellitus) as well ad with greater levels of preoperative functional
disability and pulmonary hypertension. Late complications of valve replacement include
paravalvular leakage, thromboemboli, bleeding due to anticoagulants, structural
deterioration of the prosthesis and infective endocarditis.
The considerations involved in the choice between a bioprosthetic (tissue) and
artificial mechanical valve are similar in the mitral and aortic positions and in the
treatment of stenotic or regugitant or mixed lesions. All patients who have undergone
replacement of any valve with a mechanical prosthesis are at risk of thromboembolic
complications and must be maintained permanently on anticoagulants, a treatment that
imposes a hazard of hemorrhage. The primary advantage of bioprostheses over
mechanical prostheses is the virtual absence of trromboembolic complications 3 months
after implantation, and except for patients with chronic AF; with their use. The major
disadvantage of bioprostheses is their structural deterioration, the incidence of which is
inversely proportional to the patients' age. The deterioration results in the need·to replace_
the prosthesis in up to 30% of patients by 10 years and in 50% by 15 years. Rates of
structural valve deterioration are higher for aortic prosthesis. The plfenomenon may be
due to the greater closing pressure to which mitral prosthesis is exposed, WHO (2001).
Traditionally, a mechanical prosthesis was considered preferable for a patient
under the age of 65 who could take anticoagulation reliably. Bioprostheses were
recommended for older patients (>65years) who did not otherwise have an indication for
anticoagulation (e.g.: AF). A mechanical prosthesis is reasonable for aortic or mitral
valve replacement in patients < 65 years without a contraindication to anticoagulation.
Bioprosthesis is equally reasonable for aortic or mitral valve replacement in patients < 65
3
4
years who elect this strategy for lifestyle with full knowledge of the likely need for
reoperation overtime.
1.2 Background of the study
The valves of the heart control the flow of blood through the heart into the
pulmonary artery and aorta by opening and closing in response to the blood pressure
change as the heart contracts and relaxes through the cardiac cycle. The atrioventricular
valves separate the atria from the ventricles and include the tricuspid valve; which
separates the right atrium from the right ventricle and the mitral valve separates the left
atrium from the left ventricle. The tricuspid valve has three leaflets; the mitral valve has
two. Both valves have chordae tendinae that anchor the valve leaflets to the papillary
muscles and the ventricular wall. The semi lunar valves are located between the
ventricles and corresponding aretes. The pulmonic valve lies between the right ventricle
and the pulmonary artery; the aortic valve lies between the left ventricle _and the aorta.
When any of the heart valve s do not close or open properly, blood flow is
affected. When valves do not close completely, t4e blood flows backward through the
valve in a process called regurgitation. When the valves do not open completely, a
condition called stenosis, the flow ofblood through the valve is reduced.
Disorders of the mitral valve fall into the following categories; mitral valve
prolapse (i.e., the stretching of the valve leaflet into the atrium during systole); mitral
regurgitation and mitral stenosis. Disorders of the aortic valve are categorized as aortic
regurgitation and aortic stenosis. These valvular disorders may require surgical repair or
replacement of the valve to correct the problem, depending on the severity of the
4
5
symptoms. Tricuspid and pulmonary valve disorders also occur, usually with fewer
symptoms and complications. Regurgitation and stenosis may occur at the same time in
the same or different valves.
The indications for the aortic valve operations are dictated by severity of the
disease and symptoms produced. The most common symptoms include, dyspnoea on
exertion, chest pain, and lightheadedness or dizziness usually with sudden change of
position, such as standing quickly. Although patients with symptoms certainly require
correction; there are indication for valve replacement or repair for aortic stenosis in
patients who are asymptomatic i.e. in patients who have excessively high gradients or
valve areas below 0.75-squire em. When this situation exists, a very carefully performed
treadmill or exercise test can be performed to evaluate the patients' myocardial response
to a light form of exercise. For aortic valve regurgitation, obviously echo cardio graphic
findings and symptoms help determining the operation. If the patients' LV function starts
to fail or becomes dilated, it is appropriate to rec~mmend an operation. For stenosis,
similar events are tantamount to recommending valve replacement. Repair of aortic
stenosis has been tried with variqus forms of decalcification; ultra sonic debridement can
be recommended in these cases. There are incidents of fulminate scarring which caused
the leaflets to retract and these patients then turned with rather significant and sever aortic
regurgitation requiring reoperation and valve replacement.
Mitral regurgitation occurs especially from myxomatous disease or ruptured
chordae are ideal situations for valve repair. The presence of severe mitral regurgitation
alone has become the indication for valve repair because of the late effects on survival
and left ventricular function if the regurgitation is left to progress until symptoms or
5
6
severe cardiomegaly develops. Any acute infection requires the removal of all infected
tissue which limits repair when there is large area of valve replaced with vegetations.
Tricuspid valve rarely requires replacement except in s3everal extenuating
circumstances; e.g. carcinoid involvement, endocarditis, where replacement of tricuspid
valve is required. Significant dilatation from long standing tricuspid valve regurgitation
and even more frequently from device trapping and tethering of leaflets is and indication
for valve replacement.
1.3 Need and significance of the study
The incidence of valve replacement surgery and its complications are high in
United States and also in India. The lack of personal hygiene, adequate knowledge of
patient and care givers are the important factors in developing the complications such as
wound infections, thromboembolism, endocarditis etc. The study assesses the knowledge
of patients who have uiidergone v~lve replacement in SCTIMST, Trivandrurn about the
horne care management. In SCTIMST, 212 patients carne for valve replacement either
aortic or rnitra! or double valve replacement in the year of 2008.
Mechanical valve shares the advantage of long-term durability but have increased
risk of thromboembolism and the risk of bleeding secondary to the need of
anticoagulation to prevent thromboembolism. Temporary discontinuation of
anticoagulants increases the risk of valve thrombosis and embolism. It is necessary to
discuss the importance of maintaining good oral hygiene with daily care and regular trips
to the dentist. The patient must be instructed on anticoagulation therapy and the
importance of not taking over the counter medications without consulting the physician.
6
7
Importance must be give to the patient to discuss the allowances and limitations with
respect to the occupation, recreation and activities. If the patient is taking anticoagulants,
emphasize the need for adhering the schedule for prothrombin and international
normalized ratio laboratory tests and subsequent medication dosing. Effective prevention
of infectious and embolic complications requires thorough patient and family education.
Persons with mechanical valves and with valvular diseases complicated by atrial
fibrillation require detailed instruction on proper use of warfarin anticoagulation.
Intravenous heparin may be associated with a higher incidence of hemorrhage; a
randomized trial is needed to provide the best evidence regarding early postoperative
anticoagulation after mechanical valve implantation.
1.4 Statement of the problem
Assessment of knowledge of patients who have undergone Valve Replacement
abourhome care_ management.
1.5 Objectives
+ To assess the knowledge level of patients who have undergone valve replacement
about home care management.
+ To identify the relationship between knowledge levels of patients after valve
replacement and selected variables i.e. age, sex, educational status, and the
surgery done.
7
8
1.6 Operational definitions
KNOWLEDGE:
A state of awareness or understanding with conscious mind. In this study the
knowledge about home care management after valve replacement. In this study the
investigator assessing the knowledge by asking a validated questionnaire.
PATIENTS:
In this study, patients refer to the persons who have undergone valve replacement
in Sree Chitra Tirunal Institute For Medical Sciences And Technology.
VALVE REPLACEMENT:
The surgery performed to replace the diseased valve by an artificial valve or
bioprosthetic valve. The valve may be either mitral or aortic or double valve replacement.
HOME CARE MANAGEMENT:
Home care management is the health care or supportive care provided in the
patients home by family and friends, health care professionals or the patient himself.
8
9
1.7 Delimitations
The study is limited to
+ Patients who have undergone mechanical valve replacement, who are in cardiac
surgical wards and intensive care units.
+ Patients who are more than 18 years of age
+ Patients who understand and speak Malayalam
+ Patients who are willing to participate in the study
+ The data collection period is limited to one month
+ The study area is limited to only in SCTIMST, Trivandrum.
1.8 Study setting
Location: tlie cardiac surgical intensive care units and cardiac surgical wards in
SCTIMST, Trivandrum.
1.9 Study method
The study was conducted in patients who have undergone mechanical valve replacement
either aortic or mitral or double valve replacement. Consecutive sampling done in 30
patients at the third or fourth postoperative day.
1.10 Sampling
Consecutive sampling was used to collect the data.
1.11 Sample size
30 patients
9
10
1.12 Tool
In this study the investigator assess the knowledge level of patients after
mechanical valve replacement by asking a self-prepared questionnaire. The questionnaire
contains 1 0 numbers of questions about the medications, diet, physical activity, and rest
and blood investigations. Knowledge assessment was performed on the third or fourth
postoperative day of surgery in cardiac surgical intensive care unit and cardiac surgery
wards.
1.13 Organization
The report is organized with the introduction, background of the study, need and
significance of the study, objectives, operational definitions, delimitation, and
methodology.
10
11
CHAPTER-2
REVIEW OF LITERATURE
The review of literature relevant to this study is presented in following sections:
1.Knowledge assessment of patfents regarding valve replacement
2.Diet and warfarin therapy
3.Discharge planning and follow up and
4.Prevention of complication after mechanical valve replacement
2.1 Knowledge assessment of patients regarding valve replacement
Hu Amanda and Chow-Chi- Ming (2006) conducted a study to determine the
influence of both in hospital teaching practices and socio economic status and
demographic variables on patients' knowledge of warfarin therapy. The researchers
performed a telephone survey among 1 00 patients 3 to 6 months after mechanical heart
valve replacement. A twenty-item questionnaire was used to measure the knowledge of
patients about warfarin therapy, its side effects, and vitamin K food sources. They
concluded that 61% of participants had insufficient knowledge of warfarin therapy
compared to employed or self employed and they have improve their knowledge scores
after a post discharge counseling.
11
12
2.2 Diet and warfarin therapy
Bach et al (1996) conducted a study to find out whether Vitamin K is required to
convert specific glut amyl residues in a limited number of proteins to gamma
carboxyglutamyl residues with the response of various measures of vitamin K
insufficiency to the administration of 1 mg/d of the vitamin K antagonist warfarin. The
researchers studied in two groups of nine older (55-75 y) or younger (20-28 y) subjects.
They concluded that the concentration of serum under-gamma-carboxylated osteocalcin
was lower when subjects consumed 1 mg vitamin K than when they consumed their
normal diet.
Rohde et al (2007) conducted a study to evaluate the potential interaction of
dietary vitamin K and coagulation stability in elderly patients. Recent perspective
evidences suggested that the dietary intake more than 250 microg/day was shown to
decrease warfarin sensitivity in anticoagulated patients consuming regular diets. In a
randomized crossover study brief periods of changes on vitamin K intake had significant
effects on coagulation parameters. Dietary records that for each increase in 1 00 microg of
vitamin K intake would reduce the INR by 0.2 estimated it. A recent study demonstrated
that over the counter multivitamin supplements contain enough vitamin K1 to
significantly alter the coagulation parameters.
Sconce et al (2005) conducted a study to evaluate the effectiveness of dietary
intake of vitamin K in patients with unstable control of anticoagulation compared to
patients with stable control of anticoagulation. Study was conducted in twenty-six
patients with unstable and twenty-six with stable control of anticoagulation and they
completed dietary records of all foods and drinks consumed on a daily basis for two
12
13
consecutive weeks. The mean daily intake of vitamin K in unstable patients was
considerably lower than that for. stable patients during the study period. They concluded
that daily supplementation with oral vitamin K in unstable patients could lead to a more
stable anticoagulation response to warfarin
Hu et al (2006) conducted a study to determine the influence of knowledge
regarding the warfarin therapy in patients after mechanical valve replacement in hospital
teaching practices as well as socioeconomic status and demographic variables on patients'
knowledge of warfarin therapy. A telephone survey was conducted among 100 patients 3
to 6 months after mechanical heart valve replacement. A previously validated 20-item
questionnaire was used to measure the patient's knowledge of warfarin, its side effects,
and vitamin K food sources. They concluded that gender, ethnicity, and warfarin therapy
before surgery were not related to warfarin knowledge scores. Multivariate regression
analysis revealed that understanding the concept of International Normalized Ratio,
knowing the acronym, age, and receiving community counseling after discharge were the
strongest predictors of warfarin knowledge Gender, ethnicity, and warfarin therapy
before surgery were not related to warfarin knowledge scores.
2.3 Prevention of complication after mechanical valve replacement
Puri et al (2009) conducted a study to assess the complications related to the
anticoagulation treatment after mechanical valve replacement. Anticoagulation is started
soon after mechanical valve replacement, as the risk of thromboembolic complications is
especially high during the first six months after surgery. The authors conducted the study
in a total of 503 patients who underwent mechanical valve replacement surgery at the
13
14
authors institute between July 2001 and October 2006. The patients were allocated to
three comparable groups, depending on the anticoagulation regime administered. Group
A patients (n = 221) received only oral anticoagulation from the first postoperative day;
group B patients (n = 159) received oral anticoagulation plus low-molecular weight
heparin; and group C patients (n = 123) received unfractionated heparin within 12 h of
surgery in addition to oral anticoagulation. There were incidents of reinsertion of
additional intercostal drains for collections, cardiac tamponade, valve thrombosis, and re
explorations for excessive drainage. The authors concluded that early oral anticoagulation
alone provided optimum anticoagulation and is associated with minimum complications.
Early supplementation with heparin increased the risk of hemorrhagic complications but
without reducing the thromboembolic risk.
Heras et al (1995) studied the rate of thromboembolism in patients undergoing
bioprosthetic replacement of the aortic or mitral valve, or both, at serial intervals after
operation and the effects of anticoagulant or anti platelet treatment and risk facrors. The _
rate of thromboembolism was studied at three time intervals after operation: one to ten
days, eleven to ninety days and after ninety days. The study was ~onducted in 816
patients who underwent bioprosthetic replacement of the aortic or mitral valve, or both, at
the Mayo Clinic from January 1975 to December 1982.The authors evaluated the effect
of antithrombotic therapy with warfarin, aspirin and dipyridamole alone or in
combination. They concluded that thromboembolic risk was especially high for aortic and
mitral valve replacement for 90 days after operation, and increased with lack of
anticoagulation, mitral valve location, previous thromboembolism and increasing age.
14
15
Anticoagulation reduced thromboemboli and appeared to be indicated in all
1atients as early as possible fm: 3 months and thereafter in those with risk factors and
teeded prospective testing.
Konagai et al (2006) conducted a study to evaluate the coagulant activity after
nechanical heart valve replacement. PT-INR and TAT evaluated the coagulant activity.
~o evaluate whether coagulant activity was fully suppressed by the target range of 1.5 to
~.5; coagulant activity was evaluated by measuring thrombin antithrombin3rd complex
evels and valve related complications were enrolled in this study. The investigators
ound that under adequate warfarin control, there was no significant correlation between
>T~INR and TAT, however nine patients who exhibited a PT-INR of less than 2.0 had
righ levels of TAT. They finally concluded that monitoring of TAT was useful in
letecting potential coagulation factors and to determine the therapeutic range of warfarin
hat could normalize coagulant.
Brueck et al (2006) conducted a study to evaluate the necessity of the antiplatelet
herapy by ASA with no postoperative antiplatelet therapy in terms of survival, major
>leedings and cerebral thromboembolism of patient~ undergoing biological aortic valve
·eplacement without thromboembolic risk factors. From January 2001 to December 2003,
~88 consecutive patients were selected with sinus rhythm and no other thromboembolic
'isk factors underwent single biological A VR with porcine or bovine pericardia! valves
without concurrent coronary artery bypass graft surgery. By surgeons' preference, 100
ng ASA was given to 132 patients, and 156 patients received no antiplatelet therapy. The
mthors concluded that patients without thromboembolic risk factors undergoing
>iological A VR admirristration of ASA confer no advantage compared to no antiplatelet
15
16
therapy. Functional status, thromboembolic events and survival were not adversely
affected by withholding any antiplatelet, therapy.
2.4 Discharge planning and follow up.
Naylor et al (1994) conducted a study to assess the effects of the discharge
planning and home follow up intervention on elders hospitalized with common medical
and surgical cardiac conditions. The authors collected data from 202 patients of 65 years
of age and above admitted for heart failure, myocardial infarction, CABG, angina, or
valve replacement. The authors performed a 24 week post discharge follow up
programme and concluded that high risk elders with significant problems might benefit
from a care programme and medical patients in the interventional group required fewer
multiple readmissions than in surgical group.
Theobald (2004) conducted a study to examine the post discharge issues, concerns
and needs of patients after CABG and -their family after discharge. A two-phase
naturalistic inquiry was performed in 35 patients and their carers for four to five weeks
after CABG. The findings sugge~ted that the periodic follow up and mechanisms of
mutual support and comparin~ experiences of cardiac patients and their carers need
further research for evaluation. Almost half of the patients experienced variety of changes
including pain, life style implications and financial implications.
Jaeger et al (1994) conducted a study to determine whether cardiac surgery
improves functional capacity in patients greater than 70 years of age. Self reported
functional capacity was assessed by Duke activity status index preoperatively and also
one year after CABG or valve replacement; in a total of 199 patients with a mean age of
16
,-~-----'-- ,_ -·-- _,--~-- __ , __ -----·--
17
76 years. Functional capacity improved significantly after surgery (mean Duke Activity
Status Index 27.9 at baseline vs. 36.8 at 12 months, p < 0.001), with improvements in
most patients (74%). Six preoperative factors were independent predictors of less
improvement in functional capacity between baseline and 1 year: smoking, female
gender, higher Charlson co morbidity index, syncope, previous cardiac operation and
older age. Older patients had meaningful improvements in functional capacity after
cardiac surgery and clinical factors appeared to modify the degree of improvement
attainable.
Davoodi et al (2009) conducted a study to evaluate the postoperative quality of
life in those who have undergone short and midterm results of triple valve surgery. The
authors reviewed 107 patients with multiple valve disease who underwent triple valve
surgery at Tehran University Heart Center from January 2002 through December 2007,
100 patients with complete, recorded the data were enrolled into the study. The authors
considered the demographic and ~linical characteristics and in hospital postoperative
complications. In quality of life assessment, suitable physical and social activities were
reported in 65.!)% and 60.6% of patients respectively. The researchers concluded that
despite patients' satisfaction with early outcomes of triple valve surgery and their
acceptable midterm survival rates, the improvement of quality of life is still far from
ideal.
Koertke et al (2009) conducted a study to evaluate INR self-management to
reduce severe thromboembolic and hemorrhagic complications following mechanical
heart valve replacement. Beginning anticoagulation therapy immediately in the
postoperative period further reduce anticoagulant-induced complications. The authors
17
18
collected the data from the first 600 surviving patients (from a total study sample of 1200
patients) who completed follow-up of at least 2 years. Patients were randomly divided
into a self-management group and a control group. INR self-management reduced severe
hemorrhagic and thromboembolic complications (P=0.018). Nearly 80% of INR values
recorded by patients themselves, regardless of educational level, were within the target
therapeutic range of INR 2.5-4.5, compared with 62% of INR values monitored by family
practitioners. Only 8.3% of patients trained in self-management immediately after
surgery were unable to continue with INR self-management. The results differed slightly
between patient groups with different levels of education. The authors concluded that all
patients for whom anticoagulation is indicated were candidates for INR self-management
regardless of education level.
18
19
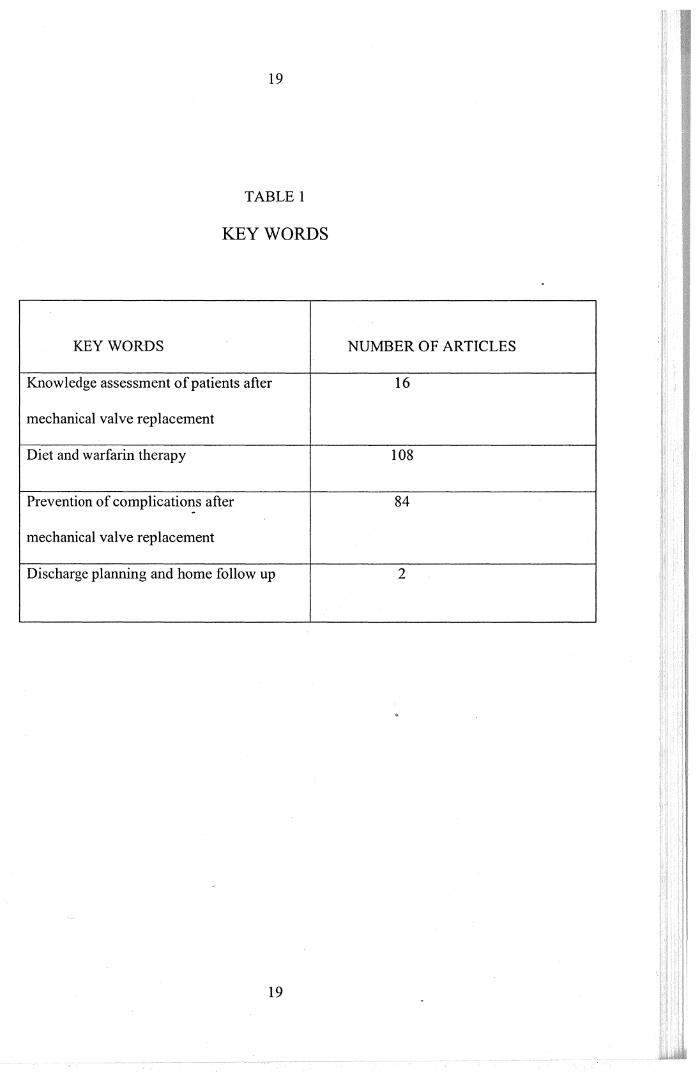
TABLE 1
KEYWORDS
KEYWORDS NUMBER OF ARTICLES
Knowledge assessment of patients after 16
mechanical valve replacement
Diet and warfarin therapy 108
Prevention of complications after 84 -mechanical valve replacement
Discharge planning and home follow up 2
19
3.1 Introduction
20
CHAPTER-3
METHODOLOGY
This chapter contains research approach, study design, the sample and sampling
technique, development and description of the tool, pilot study, data collection and plan
of analysis.
3.2 Research approach
Survey approach was used in this study.
3.3 Setting of the study
The study was conducted in cardiac surgical intensive care units and cardiac
surgical wards of Sree Chitra Tirunal Institute For Medical Science and Technology,
Thiruvananthapuram.
3.4 Study population
Population of the study are the patients m cardiac surgery ICU and wards of
SCTIMST, those who have undergone mechanical valve replacement either aortic valve
or mitral valve or double valve replacement.
3.5 Sample and sampling technique
Consecutive sampling is done for this study; 30 samples collected. The pilot study
was done in 7 patients. The total period of study is one month from September to October
2009.
20
21
3.6 Exclusion criteria
+ Patients who understand language other than Malayalam are excluded.
• The study is limited to SCTIMST Trivandrum.
3. 7 Inclusion criteria
Patients who have undergone aortic valve replacement or mitral valve
replacement, or double valve replacement with a mechanical prosthesis and those who
are willing to study are included in the study.
3.8 Development of the tool
Self-prepared questionnaire developed to assess the knowledge of patients who
have undergone valve replacement in SCTIMST Thiruvananthapuram. Several journals
and textbooks helped to develop the tool and experts in SCTIMST Trivandrum approved
it. The self-prepared questionnaire contain 10 questions regarding several aspects of
home care management after valve replacement about the medication, diet, rest and
physical activity, and blood investigations.
3.9 Description of the tool
The tool used in this study contains the following parts:
• Demographic data
• Questions about the different aspects of the home care of patients after
mechanical valve replacement.
21
22
3.10 Pilot study
Pilot study was conducted on the month of September 2009 after obtaining
permission from the authorities of hospital management. The study was conducted in 7
patients both male and female between the age group of 29 to 69 years of age with a self
prepared questionnaire. After pilot study assessment has been done on the third or fourth
post operative day of mechanical valve replacement after making necessary corrections in
the questionnaire.
3.11 Data collection procedure
Formal permission obtained from the authorities for the collection of data. The
period of data collection was from September to October 2009. The data was collected
from the cardiac surgical intensive care units and cardiac surgical wards of SCTIMST
Trivandrum. The investigator first introduced her and explained the need and purpose of
the study, the knowledge level assessed aftergetting consent from the patients.
3.12 Plan for analysis
The investigator developed the plan of analysis after the pilot study. The data
obtained from the samples was analyzed by using descriptive statistics.
3.13 Summary
This chapter contains research approach, settings, population, sample and
sampling technique, development and description of the tool, data collection and plan of
analysis.
22
23
CHAPTER4
ANALYSIS AND INTERPRETATION OF DATA
4.1 Introduction
Analysis is categorizing, ordering, manipulating and summarizing the data to an
intelligible and interpretable form so that the research problem can be studied and tested
including the relationship between different variables.
This chapter deals with the analysis and interpretation of the data collected from
30 patients who have undergone mechanical valve replacement in SCTIMST
Trivandrum.
The findings of the study were arranged and analyzed under the following sections.
1. Distnoution sample according to the demographic data
2. Distribution of sample according to the type of surgery
3. Distribution of sample according to the knowledge score
23
---·----··----·-····--~-----········
.•
24
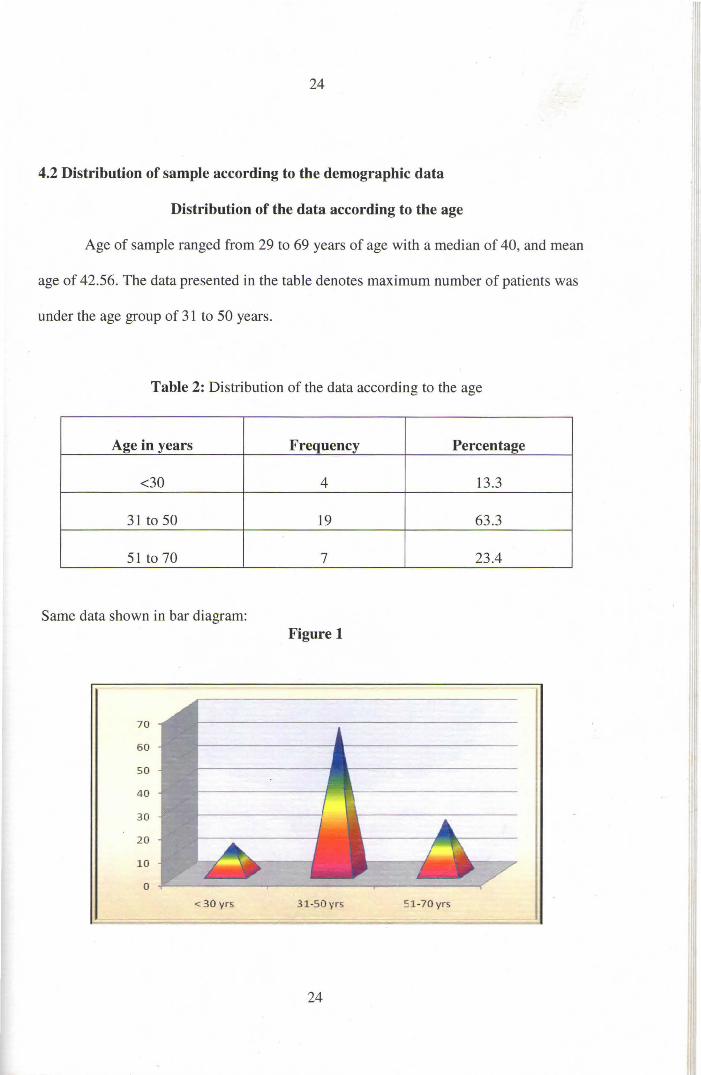
4.2 Distribution of sample according to the demographic data
Distribution of the data according to the age
Age of sample ranged from 29 to 69 years of age with a median of 40, and mean
age of 42.56. The data presented in the table denotes maximum number of patients was
under the age group of 31 to 50 years.
Table 2: Distribution of the data according to the age
Age in years Frequency Percentage
<30 4 13.3
31 to 50 19 63 .3
51 to 70 7 23.4
Same data shown in bar diagram: Figure 1
70
60
50
40
30
20
10
0
< 30 yrs 31-SO v rs 5 1 -70 y rs l 24
--1 -; _= ~ '}il- '---"I_' _:_ill --~-~ -
25
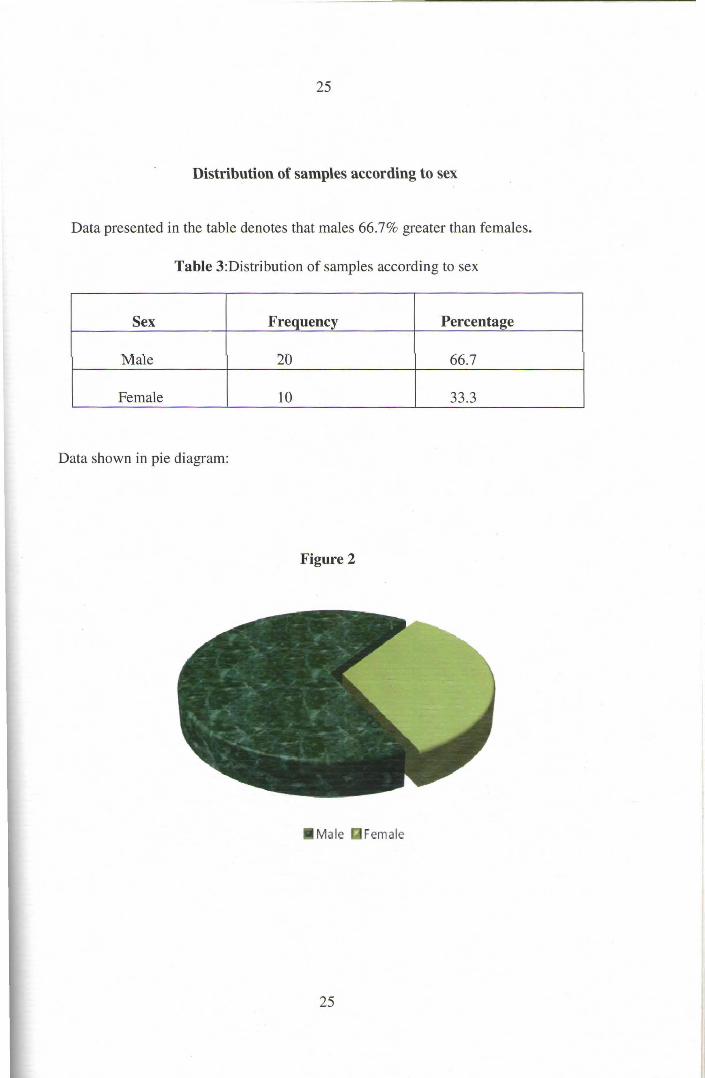
Distribution of samples according to sex
Data presented in the table denotes that males 66.7% greater than females.
Table 3:Distribution of samples according to sex
Sex Frequency Percentage
Male 20 66.7
Female 10 33.3
Data shown in pie diagram:
Figure 2
Male Female
25
--~ . '"'" ~:. ' .~ ,_ _;;.~- = ===--=- ~
26
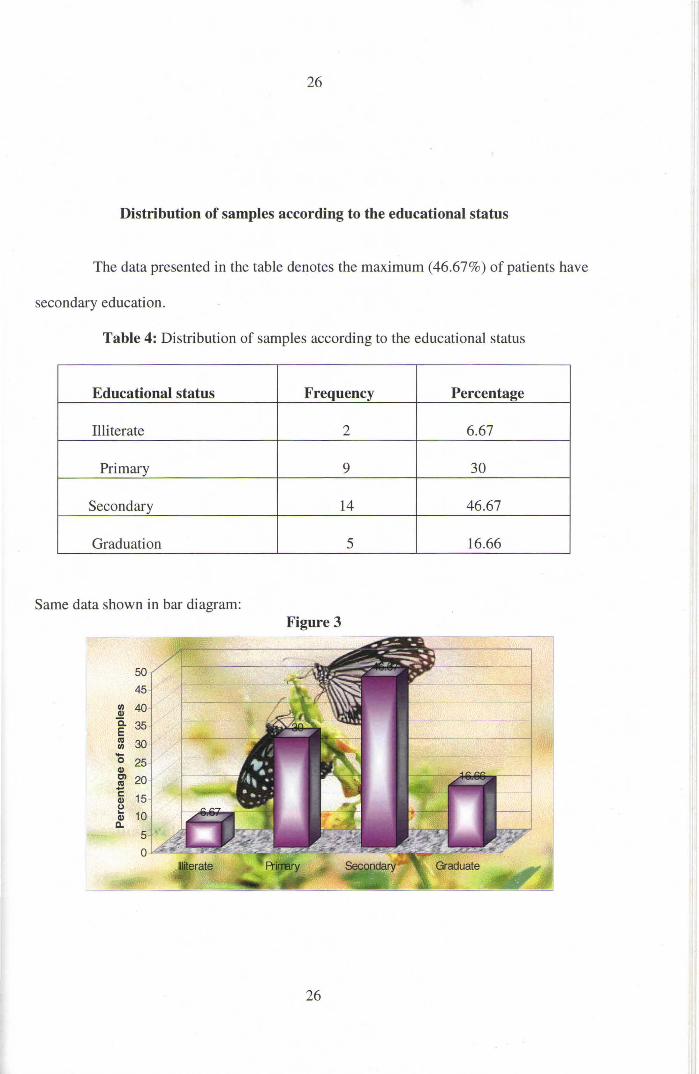
Distribution of samples according to the educational status
The data presented in the table denotes the maximum (46.67%) of patients have
secondary education.
Table 4: Distribution of samples according to the educational status
Educational status Frequency Percentage
Illiterate 2 6.67
Primary 9 30
Secondary 14 46.67
Graduation 5 16.66
Same data shown in bar diagram: Figure 3
50 45
Ill 40 Q)
Q. 35 E Ill 30 Ill -0 25 Q) Cl 20 Ill -c::: 15 Q) (J .. 10 Q)
a.
26
-
-. ~~ - - _, ~- -·-·
27
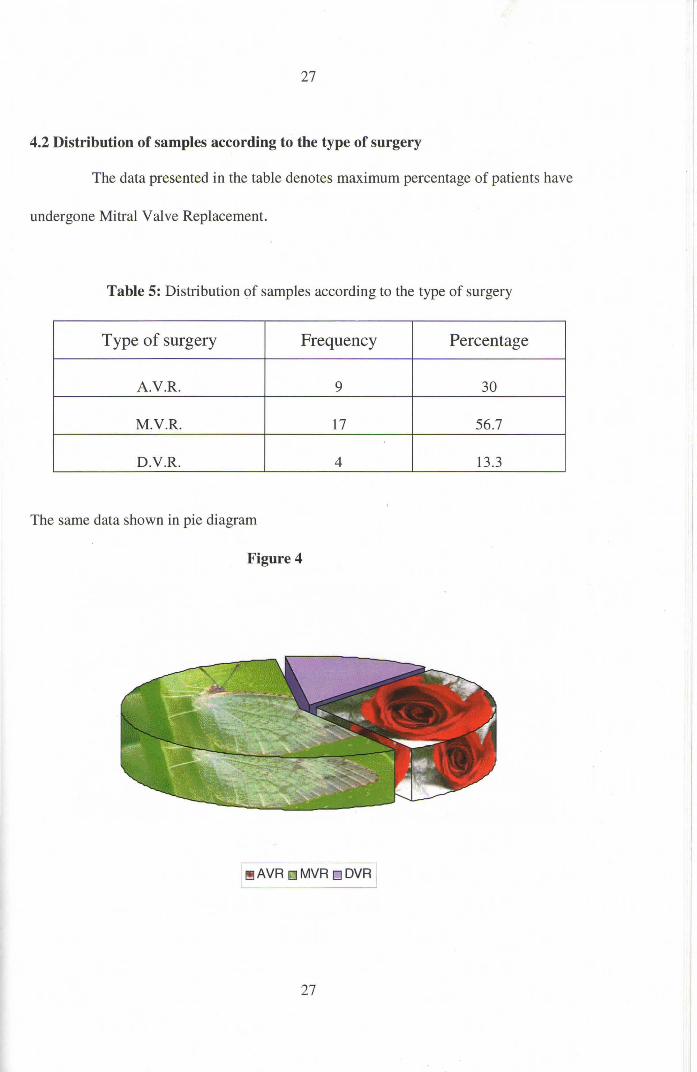
4.2 Distribution of samples according to the type of surgery
The data presented in the table denotes maximum percentage of patients have
undergone Mitral Valve Replacement.
Table 5: Distribution of samples according to the type of surgery
Type of surgery Frequency Percentage
A.V.R. 9 30
M.V.R. 17 56.7
D .V.R. 4 13.3
The same data shown in pie diagram
Figure 4
~ AVA oMVR oDVR
27
28
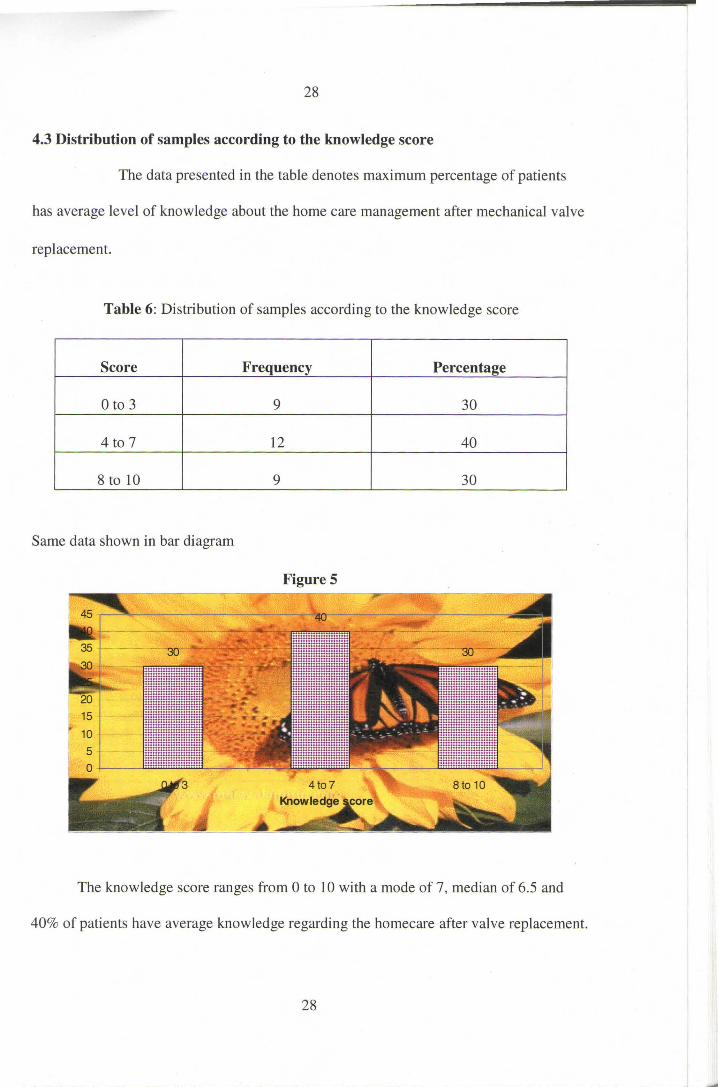
4.3 Distribution of samples according to the knowledge score
The data presented in the table denotes maximum percentage of patients
has average level of knowledge about the home care management after mechanical valve
replacement.
Table 6: Distribution of samples according to the knowledge score
Score Frequency Percentage
0 to 3 9 30
4 to 7 12 40
8 to 10 9 30
Same data shown in bar diagram
Figure 5
The knowledge score ranges from 0 to 10 with a mode of 7, median of 6.5 and
40% of patients have average knowledge regarding the homecare after valve replacement.
28
--=------------ -. - ____ ·-- - -==-
- - -~ Ltil ' -
29
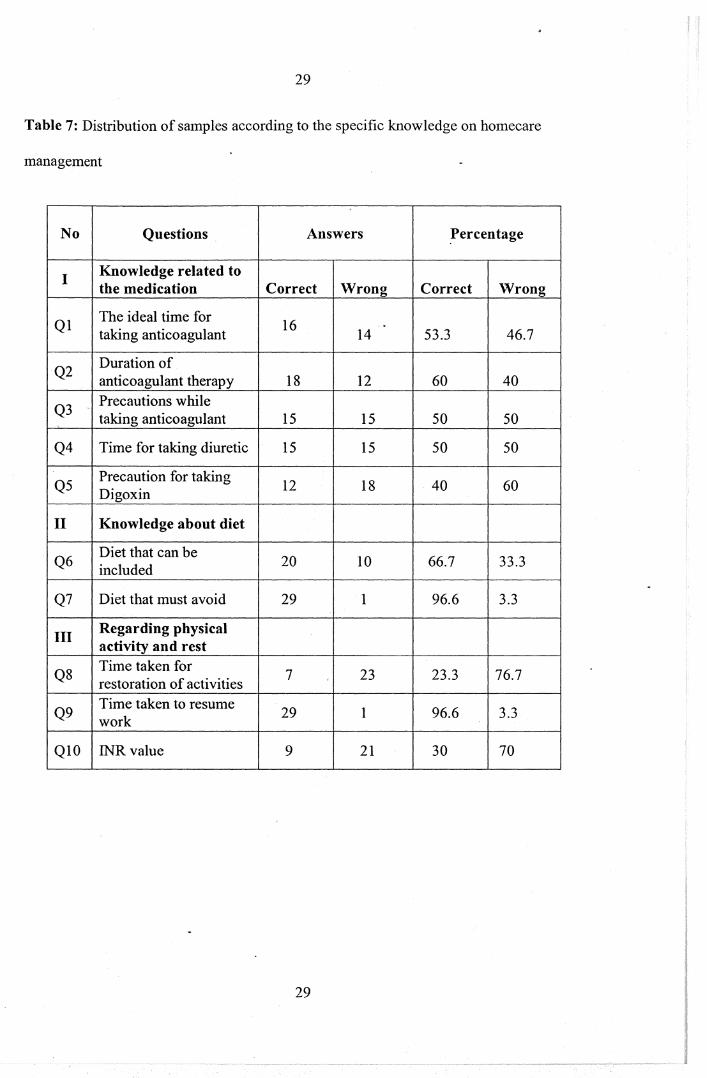
Table 7: Distribution of samples according to the specific knowledge on homecare
management
No Questions Answers Percentage
I Knowledge related to the medication Correct Wrong Correct Wrong
Ql The ideal time for 16 . taking anticoagulant 14 53.3 46.7
Q2 Duration of anticoagulant therapy 18 12 60 40
Q3 Precautions while taking anticoagulant 15 15 50 50
Q4 Time for taking diuretic 15 15 50 50
Q5 Precaution for taking 12 18 40 60 Digoxin
II Knowledge about diet
Q6 Diet that can be
20 10 66.7 33.3 included
Q7 Diet that must avoid 29 1 96.6 3.3
III Regarding physical activity and rest
Q8 Time taken for 7 23 23.3 76.7 restoration of activities
Q9 Time taken to resume
29 1 96.6 3.3 work
QIO INR value 9 21 30 70
29
30
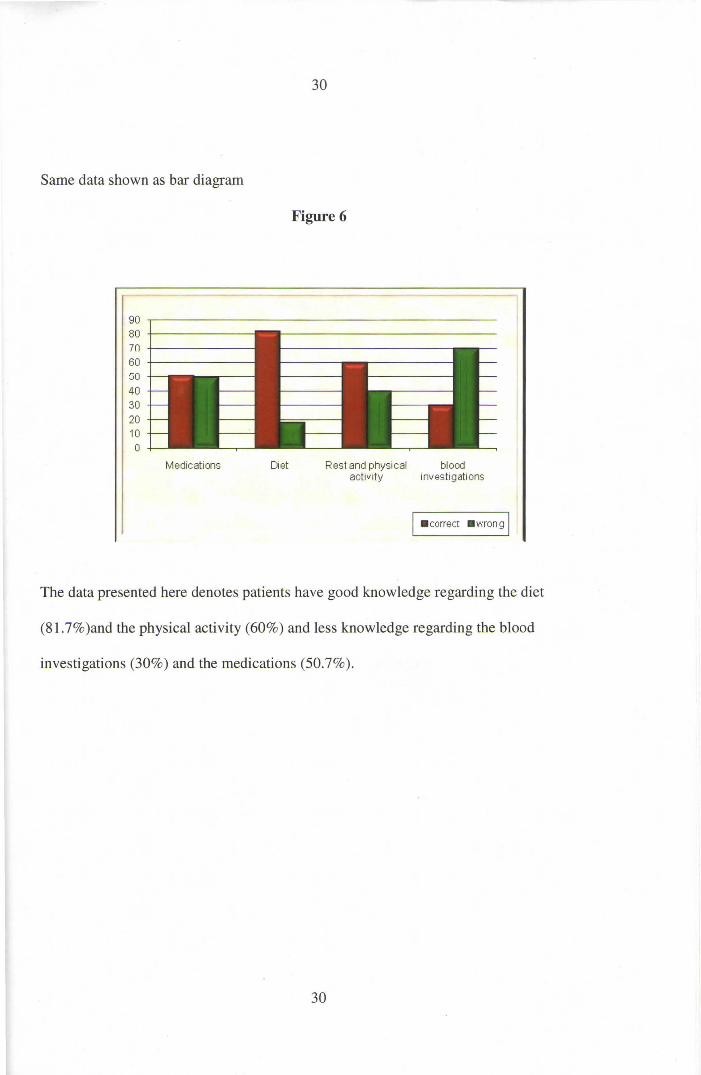
Same data shown as bar diagram
Figure 6
90 .-----------------------------------------80 +------------70 +-----------60 +------------GO 40 30 20 10 0
Medications Diet Rest and physical blood activity investi gations
I • correct • wrong I
The data presented here denotes patients have good knowledge regarding the diet
(81.7%)and the physical activity (60%) and less knowledge regarding the blood
investigations (30%) and the medications (50.7% ).
30
--- ·- ~-----,;c------~c~:. - ---
--
31
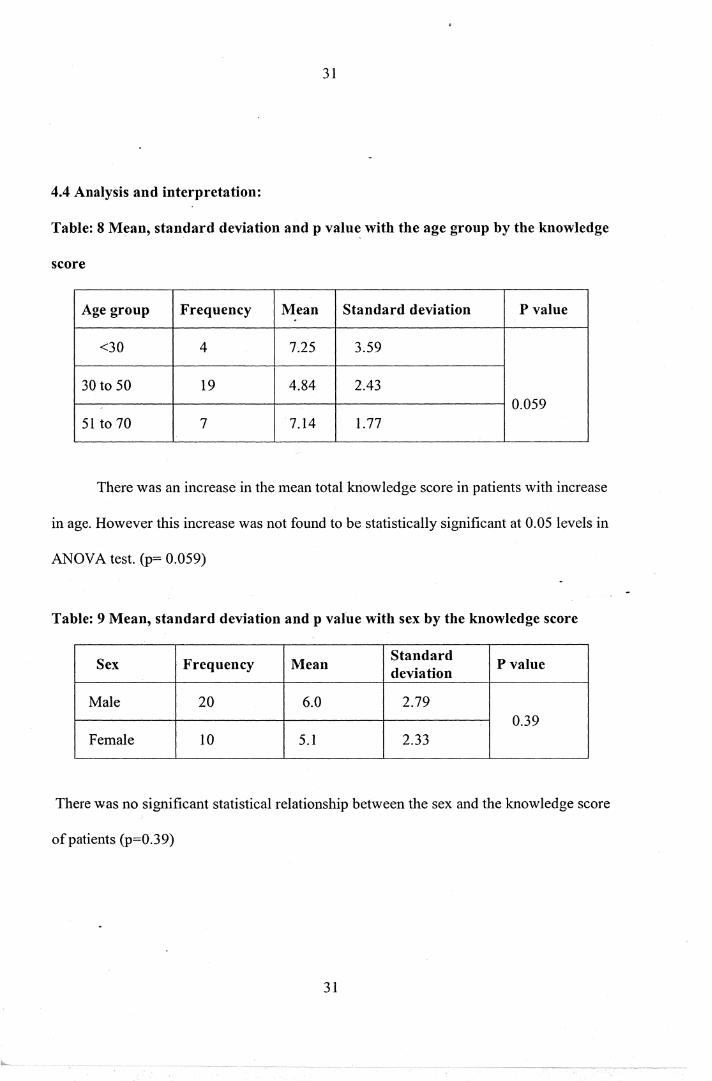
4.4 Analysis and interpretation:
Table: 8 Mean, standard deviation and p value with the age group by the knowledge
score
Age group Frequency Mean Standard deviation P value .
<30 4 7.25 3.59
30 to 50 19 4.84 2.43 0.059
51 to 70 7 7.14 1.77
There was an increase in the mean total knowledge score in patients with increase
in age. However this increase was not found to be statistically significant at 0.05 levels in
ANOV A test. (p= 0.059)
Table: 9 Mean, standard deviation and p value with sex by the knowledge score
Sex Frequency Mean Standard
P value deviation
Male 20 6.0 2.79 0.39
Female 10 5.1 2.33
There was no significant statistical relationship between the sex and the knowledge score
of patients (p=0.39)
31
32
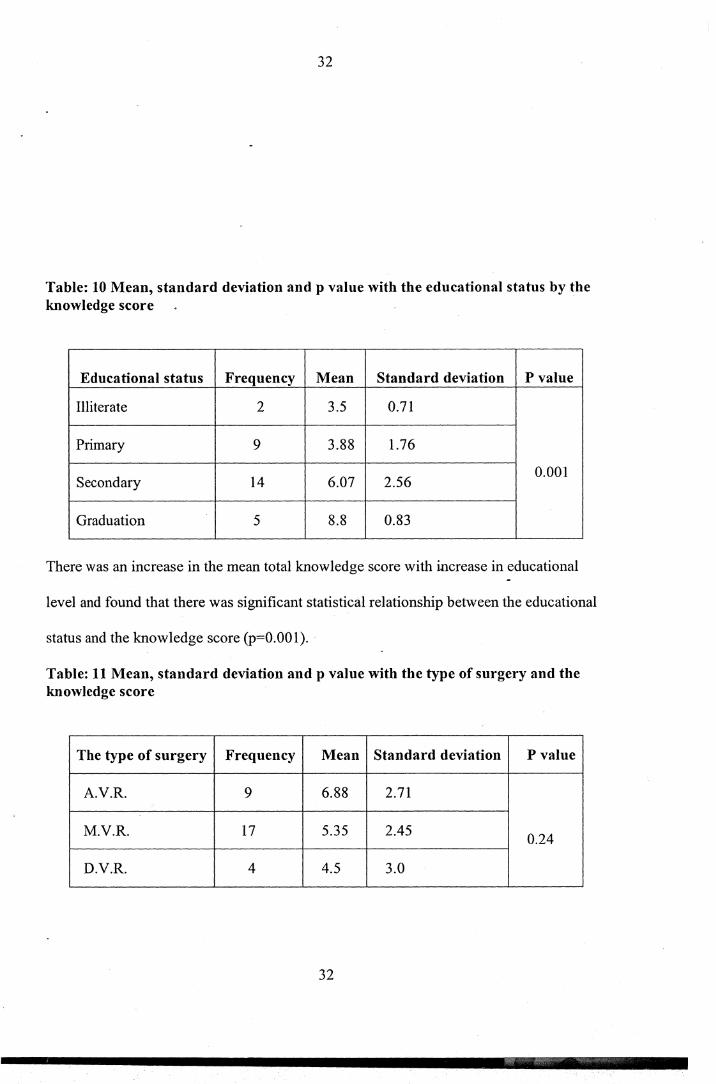
Table: 10 Mean, standard deviation and p value with the educational status by the knowledge score
Educational status Frequency Mean Standard deviation P value
Illiterate 2 3.5 0.71
Primary 9 3.88 1.76
Secondary 14 6.07 2.56 0.001
Graduation 5 8.8 0.83
There was an increase in the mean total knowledge score with increase in educational
level and found that there was significant statistical relationship between the educational
status and the knowledge score (p=O.OOl).
Table: 11 Mean, standard deviation and p value with the type of surgery and the knowledge score
The type of surgery Frequency Mean Standard deviation P value
A.V.R. 9 6.88 2.71
M.V.R. 17 5.35 2.45 0.24
D.V.R. 4 4.5 3.0
32
33
There is no significant statistical relationship between the type of surgery and the
knowledge scere (p= 0.24).
4.5 Summary
This ·chapter contains distribution of samples according to the demographic data
and the knowledge score, analysis and interpretation of the data collected.
33
34
CHAPTERS
SUMMARY, CONCLUSION, DISCUSSION AND
RECOMMENDATIONS
5.1 Summary
The study is to assess the knowledge level of patients who have undergone
valve replacement about home care management.
The objectives of the study was:
1. To assess the knowledge level of patients who have undergone valve
replacement about home care management.
2. To identify the relationship between knowledge levels of patients after valve
replacement and selected variables i.e. age, sex, educational status, and the
surgery done.
The study has been done in- SCTIMST Trivandrum with the permission from
authorities. A self-prepared questionnaire approved by the experts of SCTIMST used for
assessing the knowledge of patients who have undergone valve replacement either aortic
or mitral or double valve replacement. Pilot study conducted on the september2009 in
seven patients and sample collections has been started after making necessary corrections
in the questionnaire. The samples were collected from the cardiac surgical ICU and
postoperative wards of SCTIMST Trivandrum. The period of study was from·September
to October 2009. Thirty samples collected and their knowledge regarding the home care
assessed. Data analysis done and 40% patients have average knowledge regarding home
care after mechanical valve replacement.
34
35
5.2 Major findings of the study
The sample size was limited to 30 patients even though the maximum percentage
of patients has average level of knowledge regarding the homecare management after
valve replacement. Most of the patients have good knowledge regarding the diet and the
rest and physical activity and less knowledge regarding the blood investigations and
medications to be taken after valve replacement. The study revealed that there is
significant statistical relationship between the educational status and knowledge and also
some significant relationship was found with the age of the samples.
5.3 Limitation
The study to assess the knowledge level of patients who have undergone
mechanical valve replacement is limited to SCTIMST Trivandrum. The period of study
was only one month. The sample size is also limited to thirty. The samples were collected
from tlfe cardiac ~urgical ICU and cardiac surgical wards and those who are coming in
the review department are avoided.
The study conducted only in those who were willing to the study and those who are
speaking Malayalam.
5.4 Conclusion
The study concluded that most of the patients have good knowledge regarding the
diet and physical activity and rest: especially about the diet that must avoid and the time
to resume their work.
5.5 Discussion
35
36
The study was aimed to estimate the knowledge regarding the medications, diet, need
of rest and physical activity and the follow up after mechanical valve replacement. In
addition the study revealed positive association between the knowledge of homecare
management and the educational level. The study discussed the importance ofknowledge
of homecare management regarding the medications, diet, rest and physical activity and
the investigations to be done. The data entered in Microsoft excel and descriptive
statistics done in Epi info Version 3.2.The study revealed that 70% of patients had
insufficient know ledge regarding the homecare management.
Throughout the world, 95% of all valve replacements are performed for mitral or
aortic valves. There are approximately 225,000-heart valve procedures world wide each
year. According to American College of Cardiology/ American Heart Association
guidelines for the management -of patients with prosthetic heart valves the following
International Normalized Ratios are recommended for bileaflet valves. For the first 3
_months after valve replacement: INR= 2.5 to 3.5.Three or more months after valve
replacement:INR= 2 to 3 (Aortic Valve Replacement), INR= 2.5 to 3.5 (AVR with risk
factors), INR= 2.5 to 3.5 (Mitral Valve Replacement).
The risk factors of anticoagulation therapy include atrial fibrillation, left
ventricular dysfunction, previous thromboembolism and hypercoagulable condition. Food
and alcohol also affect the anticoagulation level.
Bacteria may enter the blood stream during dental and some medical procedures and
causing bacterial endocarditis in the tissue surrounding the artificial heart valve.
Antibiotic prophylaxis should be taken before these procedures to avoid endocarditis.
36
37
he knowledge of the patients is average regarding the homecare after mechanical valve
!placement. The complications of the valve replacement surgery can be avoided by
iving adequate knowledge regarding the homecare management after the surgery.
5.6 Recommendation
• The study has been performed in other hospitals.
• The study can be performed with a large sample size.
• The samples can be selected from the patients who are coming to the review
department can also include for this study.
37
38
BIBLIOGRAPHY
1. Bonow.R.O. et al, (2006) Guidelines for the Management ofpatients with
valvular heart disease: Executive Summary.Circulation: 114-450.
2, ACC foundation and American heart Association. (2002). ACC/ AHA 2002
guideline update for exercise testing: A report of the ACC/ AHA Taskforce on
practice guidelines. Available at: htt_p://www.acc.org/clinicallguidelines/exercise.
3. Bayer, A.S., Bolger, A.F., Taubert, K.A., Wilson, W., Stecklberg, J., Karchmer,
A.W., et al. (1998). Diagnosis and management of infective endocarditis.
Circulation, 96(1), 358- 366.
4. Murphy. (Ed.). (2007). Mayo clinic Cardiology Review (3rd edn). Philadelphia:
Lippincot Williams And Wilkins.
5. Mcttale, D.J., and Carlson, K.K. (2001). AACN Procedure manual for critical
care (4th edn).
6. Finkelmeier, B.A. (2000). Cardiothoracic Nursing (2nd edn. pp.l69- 188).
Philadelphia: Lippincot Williams Wilkins.
38
39
7. Feldman. Grossman. (2006) Profiles in VHD. In Baim.D.
Grossman's Cardiac Catheterization, angiography and
Intervention, 7th edn. Lippincot Williams AND Wilkins.
8. Bonow, R.O., Valvular Heart Diseases, In P Libby et al (eds) Brunwald's Heart
Disease, 8th edn. Philadelphia, Saunders, 2008.
9. Hargrave, K., Kothari, M.J., 2006 Neurological Sequelae of
InfectiousEndocarditis.http://www.Emedicine.com/neuro/topic264htm.
10. Hudak, C.M.Gallo, B.M., &Mortan, P.G. (1998). CriticalCare Nursing: A Holistic
Approach (7th edn). Philadelphia; Lippincot-Raven.
11. Wikipedia. Cardiovascular Diseases. Retrived on October 4, 2009, from
http:/ I en. wikipedia.org/wiki/C ardiovascular disease.
12. lung B, Gohlke-Ba··rwolfC, Tomos P, Tribouilloy C, Hall R, Butchart EG,
Vahanian A. Recommendations on the management of the asymptomatic patient
with valvular heart disease. European Heart Joumal2002; 23:1253-1266
13. Gohlke-Ba··rwolfC, Acar J, Oakley C, Butchart EG, Burkhardt D, Bodnar E,
Hall R, Delahaye JP, Horstkotte D, Krayenbuhl HP, Krzeminska-Pakula M,
39
40
Kremer R, Samama M. Guidelines for the prevention of thromboembolic events in
valvular heart disease. European Heart Journal i 995; 16:1320-1330.
14. Massel D, Little SH. Risks and benefits of adding antiplatelet therapy to warfarin
among patients with prosthetic heart valves: a meta-analysis. Journal of American
College of Cardiology 2001; 37:569-578.
15. Cappelleri JC, Fiore LD, Brophy MT, Deykin D, Lau J. Efficacy and safety of
combined anticoagulant and antiplatelet therapy versus anticoagulant
monotherapy after mechanical heart valve replacement: a metaanalysis.
American Heart Journal1995; 130:547-552.
40
41
APPENDIX 1
Demographic data
1. Name of the patient
2. Age
3. Sex
4. Marital status
5. Educational status
6. Socioeconomic data (category)
7. Surgery done
8. Source of information
41
42
. A QUESTIONNAIRE REGARDING THE HOME CARE MANAGEMENT OF
PATIENTS AFTER MECHANICAL VALVE REPLACEMENT
(Choose the correct answer for the questions from the following options)
KNOWLEDGE REGARDING THE DRUG THERAPY
1. What is the ideal time for taking anticoaguiant?
(A) With food
(B) One hour before food or one hour after taking food
(C) In empty stomach
2. For how long will you continue anticoagulant?
(A) For 6 months
(B) For 5 years
(C) Life long
3. What will you do if you forget to take one dose of anticoagulant?
(A) Take the drug same dose, at the time when you remember
(B) Take the double dose the next day
(C) No harm if you withhold the drug for one day
4. When will you take the drug LASIX?
(A) One hour after food
(B) Every morning before food
(C) Every night
5. What is the precaution to be taken before taking the drug DIGOXIN?
(A) Check blood pressure
(B) Check blood sugar
. (C) Check pulse rate
42
KNOWLEDGE REGARDING DIET
6. Item to be included in diet!?
(A) Fish and fish products
(B) Cabbage and potato
(C) Green leafy vegetables
7. Item to be excluded from diet?
(A) Milk
(B) Fruits
(C) Ghee
43
KNOWLEDGE REGARDING PHYSICAL ACTIVITY AND REST
8. How many months will you take rest after operation?
(A) Up to 3 months
(B) For 4 to 6 months
(C) More than 6 months
9. After how long can you resume your work?
(A) At 3 months
(B) After 3 to 6 months
(C) Only after 6 months
KNOWLEDGE REGARDING BLOOD TESTS
10. At what range should you keep the INR level?
(A) 1
(B) 2.5 to 3.5
(C) 3 to 4
43
44
APPENDIX2
cru am <m nJ t<m o
nO 18<W OJQaffioJ 12:1Qg1ruco)<f16)affi UOmJl<IDlcfu 1CQ) cfuW16TID'IDOJa> & 6)5
((f(c)o1ru
o.ij)mJ. crul sl
~OJ6ffi6)12lffh1e..J&o o.mm1oo n.J1om1ro1CQJ0@12lon&o, o.ij)@oB crunncfuro6TT>~IZIQ
m1CQJn.Ocfua>6TT>~I2lQ o.mm1oo eJI51<£16)&on UO&LUOldU@<W 6TlJQW1<£16)&cfuCQ)1@~on&o
6TIDQcro mmcw1eJQ<f16)& on&. o.ij)~Q ru1ruro6ID3~& 0 <m1cfu~& 0 ffin()(T\) ~12)QCQ)1
cruldhl::J1<£16)&@12lon&o ((f(c)OJ n.Jomamn1m& IZIQL<ID@IZI ~n.J~CQ)Q(f)1<£16)&cfuCQ)&~l
o.mcm& o 6TIDQrrO mmCQJ1eJ0<£16)& on&. CIDQ)CQJ<m1m0am cruJmmCQJ06) eJ 6TID 0cro ~rn
n.Jomam»1@oB . g Q(f) IZIQcfu 0@12:1 (Jl) cruiZill <m1<£16) 6 on&·
<TUOQ.Jo
<m"l CQ)<ID1
-ru1ruroo m«fficfu&on ru~c6<ID1CQJ&@S 63iJ
44
45
APPENDIX3
1. a>tB<mo cfu§nJ1s1c66)o<m1ro1c66)om~~ (f)~~1cfu n(i)a'MouB db\P1Wc66)~cmcmo6Tl)
<GTOr51cfuOI2l.:) o '?
(a) «nQ>nDOroaarrmo@SO'Mo
(b) (J)~~ldb dbw1m>c66)~cmcm1m 63ro~ m6ffi1c66)lro m~cmnJ~o dbw1~ 63ro~
f2l6ffi1c66) l ro db\Pl<D.l ~ cm<m ~ (U@ffi<D.l J o IS cfu9:16mo 63\P10JOc66) ~db
(c) @ruo~o ruwglarn (f)J~1db db\P1Wc66)~db
2. rotB<mo cfu§nJ1S1c66)o<m1ro1c66)0mJ~ (f)J~ldb n(j)L<m moun db\P1Wc66)6ffio? (a) 6 mocruaarrmc66) (b) 6 rurod!:1o QJ6)(0
(c) ~irul<mcfuoe.Jo m~w~rucm
3. 63roJ aMomJ' (f)~~1db dbw1wc66)ocm mocm~ anJom>oarn n(j)m»~ 6)!LI<:gno? (a) «rro a em Blrucruo 63 oroc£16) J amJOu3 «rroa em aMomJ db wlw c66)6ffio.
(b) nJ1ag Blrucruo ~ro31 _aMOmJ (f)J~ldb cfu\P1Wc66)6ffio
(c) 63<0J ammo m~s6lffi1a53 dbJ\P'Mf2l1~.
4. eJocrulcfu~ (f)J~1db n(J)a'MouB cfu\P1c66)~cmcmo6Tl) «rrors1dbOf2lc)o?
(a) r5cfu9:16ffio c:fu\91~ 63<0J f2l6ffi1c66)lo1mJ aUl>d!:1o
(b) n(j)~o Blrucruru~o rooru16)e.J Cffi0nDoroarrm1m mJcmo1
(c) n(j)~O B1rucruru~o <OOL<m1m>1a53
5.
lnJWOfficfuO<O.:) o '?
(a) rotB<m crul2l2lrol3o nJro1awow1c66) J db
(b) rotB<marrm16)eJ Wl ac66)ocru16)crB <GTO~ru nJrola wowlc£16) J db
(c) moM1m1s1iJ nJro1awow1c66)~db.
45
46
( 6) ®0 6> !9 nJOCQ)), CTnOJCO>lffiB Cffi'0o.D0ffi((ffi)) lam ~ W 6><MS), ~((ffi))Gmcd) nij3 cd)?
(a) mmru c\ rulcsruWBw
(b) dh0~6TlJ~, ~ffi),~dh1!96ID3
(c) gQ8.1cflt))Oldhun
7. ®06>!9 <MOCQ) 6 CTnOJCO>lffiB C5 dh9::16m((ffi))lffiB ml<Ti) 63!910JO~cflt))6mcd) nfficd)?
(a) nJoam
(b) nJWOJffi<&WBW
(c) G>mcg1
8. (f()mJ l ®l dh leo> dh w16'nffi)) nfj) L cm m OmJ ~ ((ffi)) cB6) OJ lL (f()Q)o Cffi'0 OJ (f().,) m o 6TT)?
(a) 3 momJo OJG>ffi
(b) 4-6 mom.>o OJG>ffi
(c) 6 Q)Offi)((ffi))lffiB dh l s 6 cmam
. 9. (f()mJL®Ldh1m>' cflt)) 6 ~ (f()cYJ1o nfi)L®moun dh w16mTIDoffiB nJWCO>® 6 ~nJ06>8.1 ~~ 08.11
®),SffiOo?
(a) 3 mOmJ((ffi))lffidho
(b) 3 Q)6®ffiB 6 Q)OmJ((ffi))lffidho
(c) 6 mom.>((ffi))lm ~(f()cYJ1o
10. ffid1<ID((ffi))lffiB INR G>oB arro~ru nfi)L® ruG>cneo>oGTT) mJldh9::11~cflt))6m©?
(a) 1
(b) 2.5 m6a»am 3.5 ruG>m
(c) 3 Q)6®ffiB 4 OJ6)ffi
46