Radioembolization of Hepatic Malignancies Using 90 Yttrium ......Alberta Hepatocellular Carcinoma...
45
Radioembolization of Hepatic Malignancies Using Yttrium-90 Microsphere Brachytherapy April 12, 2014 Lawrence Lou, MD, FRCPC
Transcript of Radioembolization of Hepatic Malignancies Using 90 Yttrium ......Alberta Hepatocellular Carcinoma...

Radioembolization of Hepatic
Malignancies Using Yttrium-90
Microsphere Brachytherapy
April 12, 2014
Lawrence Lou, MD, FRCPC

Objectives
• To understand transarterial radioembolization(TARE)
• To understand its indications in hepatic malignancies
• To learn the steps in performing TARE, focusing on the nuclear medicine aspects

TARE
• A procedure in which intra-arterially injected radioactive microspheres are used for internal radiation purposes
• To selectively deliver a high radiation dose to targeted tumors within the liver, while limiting radiation to normal liver to tolerable levels

Radiation from “inside out”
External Beam TARE

Liver blood supply
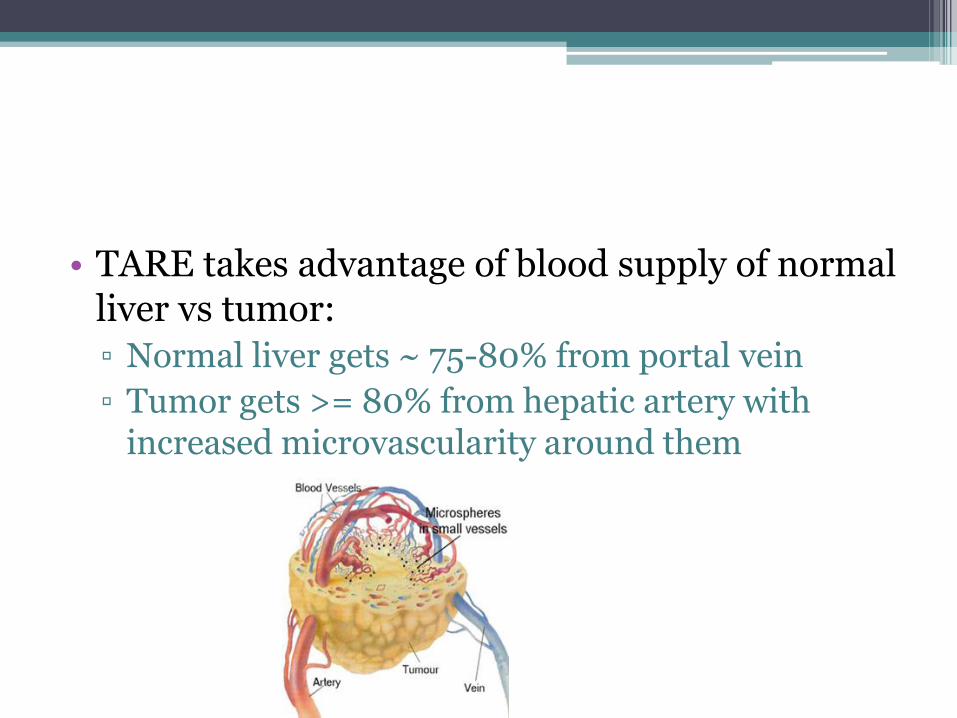
• TARE takes advantage of blood supply of normal liver vs tumor:
▫ Normal liver gets ~ 75-80% from portal vein
▫ Tumor gets >= 80% from hepatic artery with increased microvascularity around them

TARE vs. TACE
• TACE = transarterial chemoembolization
▫ occlusion of medium and large size arteries (with the use of particles 3–10 times larger than those used in radioembolization) -> tumor ischemia, with drug delivery potentially enhancing tumor cell killing
• TARE = transarterial radioembolization
▫ deliver tumoricidal doses of radiation, not by ischemia due to vessel occlusion

• TARE appears to provide better disease control with less toxicity than TACE with equivalent survival
• safe in more advanced disease including portal vein invasion and larger tumors
• Meta-analysis (425 pt with HCC) - median survival from 9.4 to 24 months. Response rates were complete response 0–9%, partial response 16–72%, and stable disease 29–65%.


Yttrium-90 (90Y) • Production: 89Y (neutron) → 90Y
• Decay: 90Y (b-, 64.2 hr/2.67 days) 90Zr; a pure β emitter
• β energy: 0.937 MeV (mean) & 2.28 MeV (max)
90Y deposits >90% energy in 5 mm of tissue & in 11 days; 2.5 mm (mean) & 11 mm (max)
90Y can deliver radiation absorbed doses of 50Gy/kg of tissue with 1 GBq activity
Sarfaraz et al., Med Phys 31, 2449-53, 2004


Indications
• for radiation treatment or as a neoadjuvant to surgery or transplantation in patients with unresectable HCC who can have placement of appropriately positioned hepatic arterial catheters

Contraindications
• whose Tc-99m MAA hepatic arterial perfusion scintigraphy shows any deposition to the gastrointestinal tract which cannot be corrected by angiographic techniques
• who show shunting of blood to the lungs which could result in delivery of > 16.5 mCi of Y-90 to the lungs. Radiation pneumonitis has been seen in patients receiving doses to the lungs > 30 Gy in a single treatment
• in whom hepatic artery catheterization is contraindicated; such as patients with vascular abnormalities or bleeding diathesis
• who have severe liver dysfunction or pulmonary insufficiency

Barcelona Clinic Liver Cancer staging system


Alberta Hepatocellular Carcinoma algorithmBurak KW, Kneteman NM. Can J Gastroenterol 2010; 24(11):643-650

Indications
• Patient with confirmed HCC
• Not suitable for surgery, RFA/PEI or TACE
• Failed TACE with progressive disease by mRECIST/ EASL
• Liver transplant candidate qualifying for down-staging
• *TARE may be alternative to TACE, especially in patients with portal vein thrombosis*

Steps in TARE
• Procedure Day 1 (mapping +/- embolization)
• 1st angiogram
▫ To map arterial vascular anatomy and possibly embolize arteries that may lead to inadvertent delivery of radiation to other areas (GI tract)
▫ to calculate the lung shunt fraction, and
▫ the safe and effective dose of radiation
Y90 outside
the liver =
BAD!

• Procedure Day 2
▫ Deliver the Y-90 particles

How is the NM part done?
• Following hepatic arterial catheterization
• 75-150 MBq (2-4 mCi) of Tc-99m MAA administered
• determine the extent of A-V shunting to the lungs (pulmonary shunt fraction) and
• Look for extrahepatic activity to confirm the absence of gastric/duodenal flow
Planar and SPECT/CT






• use geometric means calculation,
• correct for background activity,
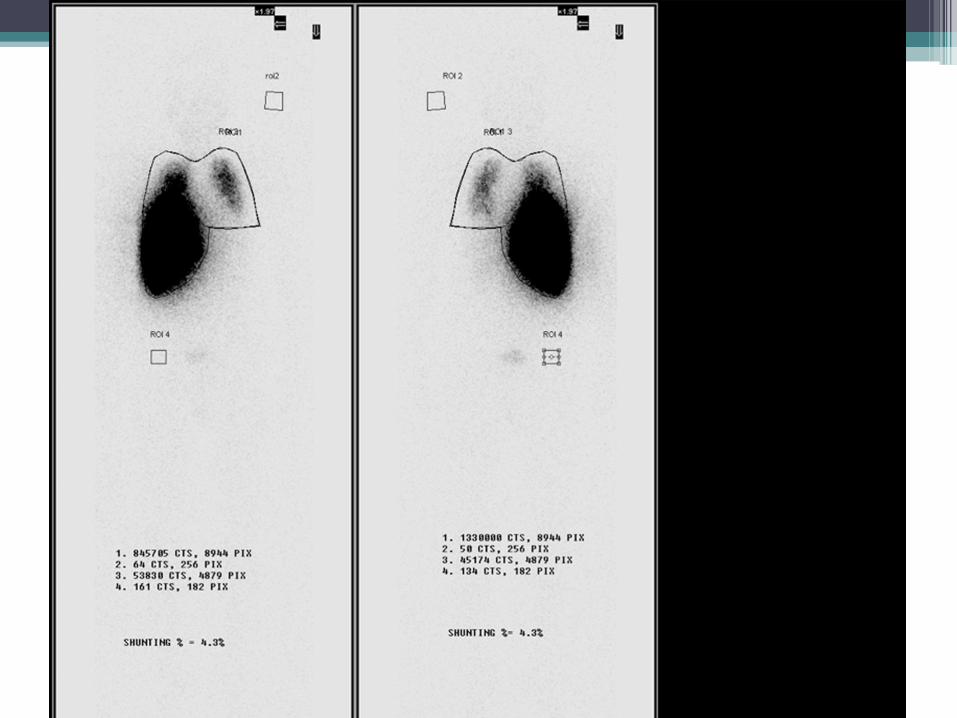
• % lung shunt =
▫ Total lung counts / (Total lung counts + Total liver counts) x 100
TheraSphere - Calculation of “total counts” is not explicitly described
SIR-Spheres - Calculate ROI counts for liver and lung regions from geometric-mean images

Example Calculation: % lung shunt
Lung
Liver

Why do we care?
• Radiation pneumonitis can been seen in patients receiving doses to the lungs > 30 Gy in a single treatment
• Limit lung absorbed dose < 30 Gy/Rx (50 Gycumulative)

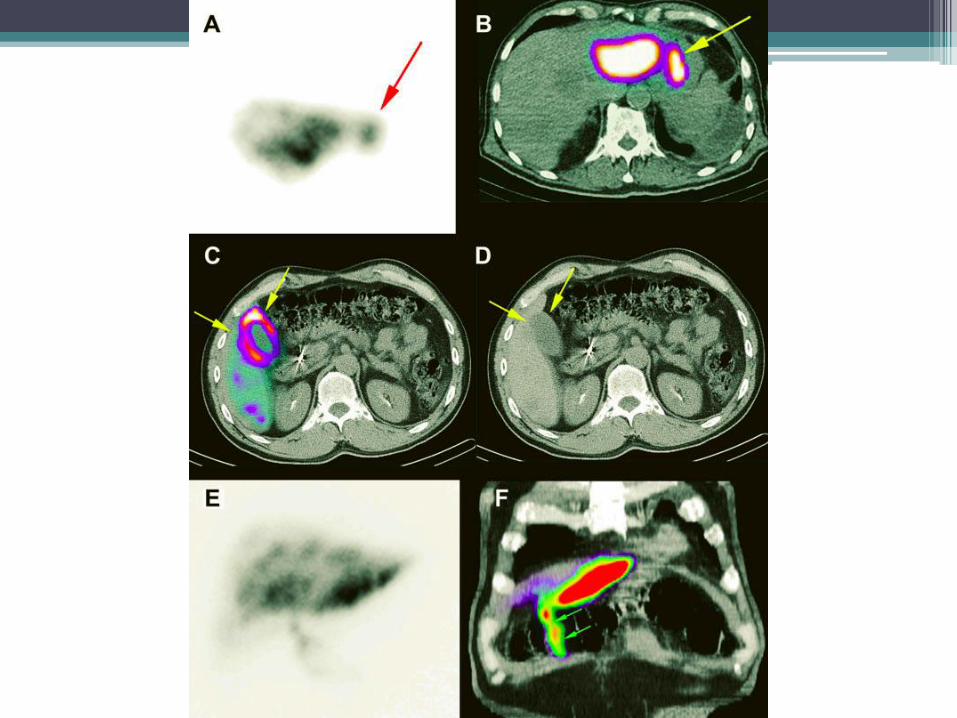
SPECT/CT
• Evaluation of extrahepatic tracer deposition
▫ Planar - Difficult to differentiate radiotracer accumulation in the liver from that in an adjacent organ
▫ SPECT/CT – increase the sensitivity in the diagnosis of abdominal extrahepatic shunting, leading to a change in approach and therapy

SPECT/CT
• Evaluation of intrahepatic tracer distribution
▫ The aim of RE is to treat the total hepatic tumour load while avoiding delivery of particles to healthy liver tissue.

SPECT/CT
• Pretherapeutic dose estimation and dosimetry
▫ more accurate dose estimation for well delineatedtumours such as HCC but is of limited value in multiple/disseminated lesions.


Dezarn et al: AAPM recommendations Y-90 microsphere brachytherapy. Med. Phys. 38(8), August 2011

Therapy Planning Calculations
CLINICAL VALIDATION – Ph III IA FUDR +/- SIR-Spheres Gray BN et al Annals of Oncology 2002.
Package inserts
Device Method Equation
SIR-Spheres
3GBq
Non-Unit Activity
BSA*GBq = [BSA - 0.2] +
(Tumor Vol) / (Tumor+Liver Vol)
Empiric
Liver Involvement by Tumor<25% ►2.0 GBq25-50% ►2.5 GBq>50% ►3.0 GBq
Partition Liver RT Tolerance 40Gy
TheraSphere
3, 5, 7, 10, 15, 20 GBq
Individualized Activity
Recommended dose 80-150 Gy
Activity (GBq) = [D (Gy) x M (kg)] / 50
Lung Shunt Reduction
For SIR-Spheres
<10% ► 0
10-15%► 20
15-20%► 40
>20% ► 100



Bremsstrahlung (BS) SPECT/CT after
radioembolization• BS means “braking radiation”, produced by the
deceleration of emitted beta particles when they lose energy in the tissue


• Performed within 24 hrs of radioembolization
• to confirm satisfactory microsphere delivery to the target arterial territory
▫ absence of Y-90 accumulation in a considerable lesion correlates well with an unfavourable response.
• to confirm the safe distribution of 90Y microspheres and for the prediction of GI side effects, , for an appropriate and timely management strategy if extrahepatic tracer deposition occurs.

ComplicationsRadiation cholecystitis
Radiation induced biliary complications
Gastroduodenal ulceration
Radiation induced liver disease
Radiation pneumonitis



QUESTIONS?