
Quick Look - Healthcare Marketplace
28
LONG-TERM CARE CLINICAL MANUAL Barbara Acello, MS, RN Pressure Ulcers
Transcript of Quick Look - Healthcare Marketplace

Long-Term Care CLiniCaL manuaL
Barbara Acello, MS, RN
PressureUlcers
Long-Term Care CLiniCaL manuaL
Barbara Acello, MS, RN
PressureUlcers
Pressure Ulcers: Long-Term Care Clinical Manual is published by HCPro, Inc.
Copyright © 2010 Barbara Acello, MS, RN
Cover Image © kentoh, 2010 Used under license from Shutterstock.com
All rights reserved. Printed in the United States of America. 5 4 3 2 1
ISBN: 978-1-60146-719-5
No part of this publication may be reproduced, in any form or by any means, without prior written consent of
HCPro, Inc., or the Copyright Clearance Center (978/750-8400). Please notify us immediately if you have re-
ceived an unauthorized copy.
HCPro, Inc., provides information resources for the healthcare industry.
HCPro, Inc., is not affiliated in any way with The Joint Commission, which owns the JCAHO and Joint Commis-
sion trademarks.
Barbara Acello, MS, RN, Author Adam Carroll, Copyeditor
Adrienne Trivers, Editor Karin Holmes, Proofreader
Jamie Carmichael, Associate Group Publisher Matt Sharpe, Production Supervisor
Emily Sheahan, Group Publisher Susan Darbyshire, Art Director
Mike Mirabello, Senior Graphic Artist Jean St. Pierre, Director of Operations
Advice given is general. Readers should consult professional counsel for specific legal, ethical, or clinical ques-
tions. Arrangements can be made for quantity discounts. For more information, contact:
HCPro, Inc.
P.O. Box 1168
Marblehead, MA 01945
Telephone: 800/650-6787 or 781/639-1872
Fax: 781/639-2982
E-mail: [email protected]
Visit HCPro online at:
www.hcpro.com and www.hcmarketplace.com
07/201021787

Pressure Ulcers: Long-Term Care Clinical Manual
CD Contents ....................................................................................................................... ix
A Word from the Author .................................................................................................. xv
Disclaimer ....................................................................................................................... xviii
Chapter 1: Overview of Anatomy and Physiology of the Skin ....................................... 1
Facts About the Integumentary System .............................................................................................................1
The Integumentary System .................................................................................................................................2
Aging Changes ....................................................................................................................................................4
Pressure Ulcers ...................................................................................................................................................6
Wound Healing ....................................................................................................................................................6
Chapter 2: Pressure Ulcer Risk .......................................................................................... 9
Risk Factors .........................................................................................................................................................9
Effects of Pressure on the Skin ......................................................................................................................... 12
Written Risk Assessment Tools ........................................................................................................................ 14
Tissue Tolerance and Pressure Ulcers ............................................................................................................... 15
Additional Risk Factors for Pressure Ulcers ...................................................................................................... 18
Pressure Ulcers on the Feet ..............................................................................................................................20
Medical Conditions That Increase the Risk of Foot and Heel Ulceration........................................................... 21
Elements of a Prevention Program ....................................................................................................................23
Care Plan Approaches for Pressure Ulcer Prevention ....................................................................................... 24
Myths and Facts About Foot Care .................................................................................................................... 31
What to Do with This Information .....................................................................................................................32
Contents
iv
Pressure Ulcers: Long-Term Care Clinical Manual
Contents
Chapter 3: Pressure Ulcer Assessment and Documentation ........................................ 35
Pressure Ulcer Assessment ..............................................................................................................................35
Staging Pressure Ulcers ....................................................................................................................................43
The Kennedy Terminal Ulcer ............................................................................................................................. 47
Reverse Staging (Backstaging) ..........................................................................................................................49
Pressure Ulcers and the MDS ...........................................................................................................................49
The Pressure Ulcer Scale for Healing Tool ........................................................................................................ 51
Other Assessment Tools ...................................................................................................................................52
Chapter 4: Immobility and Positioning Bedfast Residents ........................................... 53
Immobility .........................................................................................................................................................53
Bedfast Residents .............................................................................................................................................54
30° Concerns ....................................................................................................................................................54
Resident Refusals: Positioning and Repositioning.............................................................................................56
Bridging .............................................................................................................................................................60
Survey Observations of the Bedfast Resident .................................................................................................. 61
Soaker Pads Not for Repositioning ....................................................................................................................63
Slider Sheets .....................................................................................................................................................64
Bed Mobility ......................................................................................................................................................66
Foot Care ...........................................................................................................................................................67
Chapter 5: Pressure Relief in Chairfast Residents ......................................................... 71
Pressure Ulcers in Chairfast Residents ............................................................................................................. 71
Repositioning the Seated Resident and Using the 90-90-90 Position ..............................................................72
Importance of Pressure Relief in the Chair ........................................................................................................ 76
Importance of Positioning the Wheels .............................................................................................................. 76
Pressure-Relieving Activities in the Wheelchair or Chair ..................................................................................77
Measuring Wheelchairs to Fit Residents...........................................................................................................79
Wheelchair Mobility ..........................................................................................................................................79
Chapter 6: Support Surfaces ........................................................................................... 83
Support Surfaces ..............................................................................................................................................83
Selecting a Support Surface ..............................................................................................................................84
v
Pressure Ulcers: Long-Term Care Clinical Manual
Contents
Types of Support Surfaces ................................................................................................................................85
Bariatric Support Surfaces ................................................................................................................................88
Entrapment Concerns Associated with Replacement Mattresses and Overlays ..............................................89
Risk of Entrapment with Low-Air-Loss Beds ....................................................................................................90
Support Surfaces for Chair and Wheelchair Seating .........................................................................................92
Wheelchair Cushions .........................................................................................................................................95
Final Word on the Subject .................................................................................................................................95
Chapter 7: Lower-Extremity Ulcers ................................................................................ 97
Lower-Extremity Ulcers ....................................................................................................................................97
Ulcer Identification ............................................................................................................................................97
Arterial (Ischemic) Ulcers ..................................................................................................................................98
Venous (Stasis) Ulcers .....................................................................................................................................100
Graduated Compression Stockings .................................................................................................................104
The Unna Boot ................................................................................................................................................106
Diabetic (Neuropathic) Ulcers .......................................................................................................................... 107
Other Types of Ulcers ..................................................................................................................................... 112
Describing and Documenting the Wound ....................................................................................................... 115
Preventive Plan of Care ................................................................................................................................... 115
Chapter 8: Nursing Strategy: The Plan of Care for a Resident with a Pressure Ulcer ......................................................................................................119
Ongoing Plan of Care ...................................................................................................................................... 119
Planning Care .................................................................................................................................................. 119
Suggested Care Plan Approaches for Residents with Pressure Ulcers .......................................................... 121
Other Issues .................................................................................................................................................... 126
Diarrhea ........................................................................................................................................................... 126
Wound Pain ..................................................................................................................................................... 127
Chapter 9: Wound Dressings ......................................................................................... 129
Matching the Wound to the Dressing ............................................................................................................. 129
Selecting a Dressing ........................................................................................................................................ 132
Red, Yellow, or Black ....................................................................................................................................... 139
Art and Science of Changing Wound Dressings ............................................................................................. 139
vi
Pressure Ulcers: Long-Term Care Clinical Manual
Contents
Pain During Treatment and Dressing Change .................................................................................................. 139
Wound Care Technique ................................................................................................................................... 141
Initial Procedure Actions .................................................................................................................................. 141
Chapter 10: Other Treatment Options .......................................................................... 143
Recommended Treatment Options .................................................................................................................143
Procedure for Wound Care ..............................................................................................................................144
Observing and Cleansing the Wound ..............................................................................................................144
Hydrotherapy, Cleansing, and Irrigating the Wound ........................................................................................ 146
Negative Pressure Wound Therapy Systems .................................................................................................. 149
Cadexomer Iodine ........................................................................................................................................... 152
Debriding Agents............................................................................................................................................. 152
Silver................................................................................................................................................................ 153
Other Antimicrobials ........................................................................................................................................ 154
Honey in Wound Care ..................................................................................................................................... 155
Older Treatments ............................................................................................................................................ 158
Hypergranulation Tissue .................................................................................................................................. 159
Crusting for Skin Irritation ................................................................................................................................ 159
Poor or Abnormal Healing ...............................................................................................................................160
Delayed or Stalled Healing ..............................................................................................................................160
Chapter 11: Skin Tears .................................................................................................... 163
Skin Tears ........................................................................................................................................................163
Preventive Care ...............................................................................................................................................164
Skin Tear Assessment and Classification ........................................................................................................168
Skin Tear Treatment ......................................................................................................................................... 169
Chapter 12: Wound Infection ......................................................................................... 173
Systemic Factors That Increase the Risk of Wound Infection ......................................................................... 173
Pressure Ulcer Colonization ............................................................................................................................ 173
Wound Infection .............................................................................................................................................. 175
Wound Pain Related to Infection ..................................................................................................................... 177
Septic Conditions ............................................................................................................................................ 178

vii
Pressure Ulcers: Long-Term Care Clinical Manual
Contents
Osteomyelitis .................................................................................................................................................. 179
Wound Culture ................................................................................................................................................ 181
Necrotizing Fasciitis .........................................................................................................................................183
Risk of Tetanus in Pressure Ulcers, Skin Tears, and Chronic Wounds ............................................................ 186
Care Plan Approaches and Practices for Preventing Wound Infection ............................................................ 188
Chapter 13: Legal Issues ................................................................................................. 193
OBRA .............................................................................................................................................................. 193
Pressure Ulcers: Scope of the Problem ..........................................................................................................194
Regulatory Changes ........................................................................................................................................ 195
Declines in Condition Related to Pressure Ulcers ........................................................................................... 195
Resident Noncompliance and Refusals ........................................................................................................... 199
Legal Concerns ............................................................................................................................................... 201
Maintaining a Photographic Record .................................................................................................................203
Chapter 14: Regulatory Issues ....................................................................................... 207
State and Federal Regulations .........................................................................................................................207
Government Regulations .................................................................................................................................207
Type, Frequency, and Duration of Long-Term Care Facility Surveys ...............................................................208
Understanding the Inspection (Survey) Process .............................................................................................209
Quality Indicator Survey .................................................................................................................................. 210
Survey Team Preparation ................................................................................................................................ 211
OSCAR ............................................................................................................................................................ 213
Quality Measures ............................................................................................................................................ 214
Chapter 15: Documentation ............................................................................................217
What to Document .......................................................................................................................................... 217
What Not to Document ................................................................................................................................... 218
Fraud and Abuse ............................................................................................................................................. 221
Guidelines for Nursing Documentation ...........................................................................................................222

Pressure Ulcers: Long-Term Care Clinical Manual
Chapter 1
Anatomy Diagram: The Integumentary System
Anatomy Diagram: Macule
Anatomy Diagram: Papule
Anatomy Diagram: Nodule
Anatomy Diagram: Wheal
Anatomy Diagram: Plaque
Anatomy Diagram: Types of Vesicles
Anatomy Diagram: Pustule
Anatomy Diagram: Crust
Anatomy Diagram: Ulcer
Anatomy Diagram: Scar
Anatomy Diagram: Atrophy
Chapter 2
AHCPR Nutrition Guidelines
Care Area Assessment Process
MDS 3.0 Chapter 3 Skin Assessment Guidelines
MDS 3.0 Section M
MDS 2.0 Section M
Estimated Fluid Needs
Geriatric Lab Values
Importance of Nutrition in Pressure Ulcer Management
Maslow’s Hierarchy of Needs
CD Contents
Panic Values
Prerenal Azotemia and Dehydration
Pressure Ulcer RAP MDS 2.0
Development of a Plan of Care for a Resident at High Risk of Developing a Pressure Ulcer
Pressure Ulcer Risk Factors
Pressure Ulcer Road Map
Reportable Lab Values
Significance of Lab Values
Weight Monitoring
Chapter 3
Hemoglobin A1c Conversions
Pressure Ulcer Assessment and Documentation
Braden Scale
Lawsuit Report
Management Overview
Other Areas to Consider When Assessing Residents
Pressure Ulcer Look-Alikes
Pressure Ulcer Definitions
Pressure Ulcer Overview
MDS Coding Tip Sheet
Tissue Test
Wound Drainage Definitions
Wound Pain
x
Pressure Ulcers: Long-Term Care Clinical Manual
CD Contents
Chapter 4
Body Positions
Bridging
Complications of Immobility
Cost Analysis for Positioning
Effects of Unrelieved Pain
Guidelines for Applying a Trapeze to the Bed
Guidelines for Moving Residents with Slings
Moving Residents with Low-Friction Slings and Slides
Nursing Assistant Guidelines for Bed Positioning
Positioning Residents
Tips for Easier Movement of Bedfast Residents
Procedure for Applying a Footboard
Procedure for the Semi-Prone Position
Procedure for the Semi-Supine Position
Procedure for the Boston Roll
Chapter 5
Chair and Wheelchair Support Surfaces
Guidelines for Chair Positioning
Guidelines for Leaning to the Sides for Pressure Relief
Guidelines for Wheelchair Push-Ups
Tip-the-Waiter Technique
Positioning for Wheelchair Measurement
Optional Wheelchair Accessories
Standard Wheelchair Sizes
Wheelchair Fit
Wheelchair Parts
Chapter 6
Advantages and Disadvantages of Support Surfaces
AHCPR Support Surfaces Decision Tree
Chair and Wheelchair Support Surfaces
Characteristics of Common Support Surfaces
Draft Guidance for Industry and FDA Staff Hospital Bed System Dimensional Guidance to Reduce Entrapment
FDA Entrapment Pictures
FDA Memo April 2010
FDA Side Rails Guidance
Low-Air-Loss Bed Policies and Procedures
Managing Tissue Loads
Potential Alternatives to Side Rail Use
Side Rail Configurations
Statement of Deficiencies
Support Surface Categories
Chapter 7
Hemoglobin A1c Conversions
Care Plan Approaches for Feet and Legs
Features to Consider When Selecting Diabetic Socks
Evaluating Edema
Measuring Compression Hosiery
Lawsuit Expert Report
Graduated Compression Stockings and Implications for Nursing Research
Graduated Compression Stockings: Compression Strengths
Graduated Compression Stockings
Graduated Compression Stockings Guidelines for Care and Monitoring
Resident Teaching Diabetic Foot Care
Leg Ulcer Comparison
Chapter 8
Pressure Ulcer Assessment and Documentation
Best Practices Bookmark
xi
Pressure Ulcers: Long-Term Care Clinical Manual
CD Contents
Care Planning Form
Nursing Strategy: The Preventive Plan of Care
Pressure Ulcer: Development of a Plan of Care for Residents at High Risk
Decision Trees
Pressure Ulcers: Essential Systems for Quality Care
Expert Report
Interventions Table: Pressure Ulcers
Formulating a Nursing Diagnosis
Pressure Ulcer Sample Protocol
Nutritional Wound Healing Guidelines
Ongoing Plan of Care
Pain Problem
Wound Pain
Pressure Ulcer Prediction, Prevention, and Treatment Pathway
Pressure Ulcers: Essential Systems
Development of a Plan of Care for a Resident with a Pressure Ulcer
Commitment to Pressure Ulcer Management in Your Facility
Pressure Ulcers: Development of a Plan of Care
Care Plan Approaches for Pressure Ulcer Prevention
Chapter 9
Dressing Type for Wound Characteristics
Procedural Actions
Procedure for Applying a Hydrocolloid Dressing
Procedure for Applying a Transparent Film Dressing
Pressure Ulcer Treatment Product Categories
Red, Yellow, and Black
Types of Dressings
Chapter 10
Average Water Temperatures for Hydrotherapy Treatments and Procedures
Procedure for Changing a Clean Dressing
Cleanser Toxicities
Disinfecting the Permanent Whirlpool Tub
Growth Factors
Guidelines for Cleansing and Observing a Wound
Guidelines for Culturing the Whirlpool
Disinfecting the Hubbard Tank, Low Boy, or Extremity Whirlpools
Guidelines for Removing a Soiled Dressing
Hydrotherapy Equipment Log
Irrigation Pressures
Procedural Actions
Procedure for a Therapeutic Whirlpool Treatment
Procedure for Changing a Clean Dressing and Applying a Treatment Product
Procedure for Changing a Sterile Dressing
Procedure for Removing a Dressing
Seven Rights of a Dressing Change
Guidelines for Sterile Procedures
The Story About Culturing the Whirlpool
Infection Control Precautions for Dressing Changes Clean Procedures and Using the Treatment Cart
VAC Therapy
Procedure for Changing Wet-to-Dry Dressings
Guidelines for Whirlpool Therapy
Whirlpool Log
Whirlpool Safety Precautions
Wound Drainage Definitions
Wrapping a Bandage

xii
Pressure Ulcers: Long-Term Care Clinical Manual
CD Contents
Chapter 11
Quick Assessment
Skin Tears
Suggested Skin Tear Protocols
Chapter 12
Adult Immunization Schedules
Alcohol Hand Cleaner Contraindications
F441 Infection Control
Fecal Drainage Collector
Hand Hygiene
Infection Criteria
MRSA Change Strategies
MRSA FAQ
MRSA Useful Resources
MRSA CDC Brochure
Overview: Managing Colonization and Infection
PPE Sequence
CDC Poster: Applying and Removing PPE
Procedure for Needle Aspiration
Procedure for Swab Wound Culture
Procedure for Tissue Biopsy
Standard Precautions
Chapter 13
Gauging Pressure Ulcers Toolkit
Chapter 14
Additional Survey Information
CMS Criteria: Pressure Ulcers
F314 Investigative Criteria
F314 Summary Handout
Facility Assessment Checklist
F-Tags Associated with Pressure Ulcers
Pressure Ulcer Framework
Pressure Ulcer Regulation (314) and AMDA Guidelines
Pressure Ulcer MDS Codes
QI/QM Resources
Quality Measures: Pressure Ulcer Risk (3 Chapters from QM book)
Scope and Severity
Survey Comparison
Systems Investigative Audit
Top 10 Deficiencies
Chapter 15
Daily Documentation
Expert Report
F514
Refusals, Noncompliance, and Behavior Problems
Forms
Admission Physician Order Sheet
AMDA 24-Hour Report
Assessment
Nursing Assessment Skin Observations on Bath/Shower Day
Comparison Chart: Pressure Ulcer Prevention
Comparison Chart: Pressure Ulcer Treatment
Pressure Ulcer Checklist
CNA Communication Log
CNA–Nurse Communication
CNA Resident Observations
Skin Monitoring: Comprehensive CNA Shower Review
Comprehensive Admission Skin Assessment
xiii
Pressure Ulcers: Long-Term Care Clinical Manual
CD Contents
Skin Monitoring: Daily Skin Check
Data Tracking Tool
Systems Check for Physician Calls
Order Sheet for Enteral Feeding
Pressure Ulcer Assessment
Impaired Skin Integrity Audit
Insulin and Blood Glucose Monitoring Orders
Licensed Nurse Weekly Skin Check
Dehydration Risk Assessment
Form: Nursing Assistant Care Plan
Pain Flow Sheet
Pain Assessment
Pain Screen
Pressure Sore Log
Pressure Ulcer Record
Pressure Ulcer Communication with Physician
QA&A Pressure Ulcer Evaluation
Quality Assessment/Improvement Tool
Pressure Ulcer Assessment Report
SBAR: Skin Care Instructions
Skin Breakdown Checklist
Skin Tear Risk Assessment
Skin Observation Protocol: Pressure Ulcer Assessment and Documentation
Skin Tolerance and Turning Schedule
Weight Record
Wound Care Competency
Wound Evaluation and Follow-Up
Pain Scales
Forms: Pain Scales
PowerPoint Slides
Pressure Ulcer Jeopardy
Pressure Ulcer PowerPoints
Skin Care Fair
Skin Care Fair Instructions
Skin Care Fair Take-Home Sheet
Skin Care Fair Train-the-Trainer
Stop the Pressure: The CNA’s Role
Stop the Pressure: Tracking Quality Improvement
Useful Resources
CFMC Glossary
In-Service Resources
Other Resources
Pressure Ulcer Framework
Pressure Ulcer Football Contest
Pressure Ulcer Flows
Quality Improvement Organizations
Resources/URLs
Pressure Ulcer Terminology
Links to U.S. Quality Improvement Organizations
Wheelchair Rodeo


Pressure Ulcers: Long-Term Care Clinical Manual
Introduction
According to an old maxim, long-term care facilities are more highly regulated than nuclear power. One
area of recent regulation is pressure ulcers. Pressure ulcers (F314) is always on the annual top 10 list of
most commonly cited survey citations. However, this subject isn’t really about rules. Pressure ulcers are
painful. Treatments can be very painful. Residents have a right to be free from pain. In addition to being
a source of pain, pressure ulcers often lead to many additional complications due to the disruption of
skin integrity. These include infection of the soft tissues surrounding the wound (cellulitis), infection of
the bone (osteomyelitis), infection of a joint (septic arthritis), abscesses, chronic infection, development
of undermining, tunneling, and sinus tracts. Worse yet, pressure ulcers can cause systemic spread of
bacteria (bacteremia/septicemia) and septic shock, which can lead to death. Complications can occur
despite apparent improvement in the ulcer.
It goes without saying that pressure ulcers increase the legal exposure of facilities and nurses. Pressure
ulcers are the leading cause of lawsuits against long-term care facilities, accounting for approximately
17,000 lawsuits each year. There are usually many additional peripheral and contributing factors, such as
development of contractures, malnutrition, dehydration, infection, and sepsis. Surprisingly, many facility
residents develop malnutrition and dehydration despite the presence of feeding tubes, and this is a
common factor in skin breakdown. The plaintiff often names the director and assistant director of
nursing, MDS nurse, and various shift supervisors and charge nurses in addition to the facility, its own-
ers, and board members. A nonmedical jury is responsible for sorting it all out, and saying that juries are
often “grossed out” by the details, photos, and autopsy findings is an understatement. Laypeople view
medical conditions very differently from those of us who are exposed to them day after day, year after
year. Pressure ulcer lawsuits often invoke strong emotions and feelings of sympathy, and it shows when
million dollar verdicts are awarded to residents or their survivors.
A Word from the Author

xvi
Pressure Ulcers: Long-Term Care Clinical Manual
A Word from the Author
You probably learned the maxim “pressure ulcers are easier to prevent than to treat” when you were in
nursing school. We have many sacred cows in nursing, but this old adage is absolutely true. This book
contains useful clinical pearls, helpful factoids, and functional tools with which to do your job. You
already know how to be a nurse, so it is not a rehash of familiar policies and procedures. It was not
written to be highly technical, theoretical, or to present the results of complex research. Rather, the
primary goal is to provide information and tools that will be both practical and functional to nurses in
developing, enhancing, improving, or revamping a pressure ulcer prevention and management program.
The book focuses on resources you need and beneficial information for administering a successful
program. It is not meant to be an exhaustive or comprehensive source of information, such as a textbook.
It includes current clinical information that will complement more exhaustive sources of long-term care
nursing reference material. Some of the information is likely to be new, and some not. Take what makes
sense and adapt whatever works to your facility and your residents. Pressure ulcer care is so highly
individualized that providing rigid rules is impossible.
When I was a director of nursing at a large skilled nursing facility, I conducted various wound product
studies, looking for the panacea to quickly heal all pressure ulcers. I finally concluded that no panacea
existed, and I learned to match the treatment product to the wound characteristics. This was effective,
and a good learning experience. However, the most important lesson I learned was that I had fewer
wounds if I paid a great deal of attention to the numbers. My staff did not want me on their units check-
ing behind them, monitoring and adjusting care plans, or generally ranting and raving about the evils
associated with in-house pressure ulcers, and thus did all they could to prevent them. If a minor area
developed, their goal was to identify and heal it quickly, before I found out about it, although no one
would admit it. If I got busy or distracted for a few weeks, the numbers seemed to find a way of increasing.
Because of this, I encourage you to make your dislike of pressure ulcers very clear. It doesn’t matter
whether you are a nurse manager or staff nurse. This is an area where all nurses have a modicum of
control. Develop a weekly tracking and reporting system. If a new ulcer develops or an existing ulcer is
not healing, make it your business to investigate the situation. I think you will be surprised and pleased,
just as I was when I learned that simply paying close attention to pressure ulcers had a dramatic effect on
resident care in the facility!
Working in long-term care is the toughest job you will ever love. Your mission and responsibility are
monumental, and the essence of quality care resides in the manner in which staff considers and relates to
residents as individuals. Quality of life is the result of a culture of caring. When the facility has a culture
of caring, quality of care flourishes. Nurses with a vision create this culture. Everyone benefits. Long-term
care nursing is a calling. Don’t view it as a chore. We hope this book provides you with useful tools with
xvii
Pressure Ulcers: Long-Term Care Clinical Manual
A Word from the Author
which to further the process. Your work is sacred, and by providing quality care, you are making a
difference. Believe in that, and believe in yourself!
Acknowledgments
Pressure Ulcers: Long-Term Care Clinical Manual was written with a great deal of personal and professional
collaboration. I am sincerely grateful for the assistance and cooperation of my colleagues:
Gwen Valois, MS, RN, BC, Director of Education, CiNet Healthcare Learning
Jayne Ball, Barbara Braden, and Nancy Bergstrom, Prevention Plus & TexTeach, LLC
National Pressure Ulcer Advisory Panel (NPUAP)
Frances Lovett, RN, WCC, LNCC
Bernard Pradines, MD, Centre Hospitalier, Albi, France
Karen Lou Kennedy-Evans, RN, CS, FNP
Cynthia Salzman, MHA, Northwest Regional Spinal Cord Injury System
Laura Grey More, MSW, LCSW
Ryan Sparks, MS, MBA, Vice President, General Manager, Care2Learn Enterprise
New Zealand Medical Association
Steve Warren, Vice President, Skil-Care Corporation
I am grateful for the unfailing support and assistance of my son, Jon Acello, for the professional quality
scans and photos. Adrienne Trivers, HCPro, Inc. Managing Editor, has shaped the book you hold in your
hands. She is committed to quality, and I sincerely appreciate the many hours she has devoted to making
this the best book possible. Many unnamed individuals at HCPro handle the manuscript as it makes its
way through the production process. Each makes a contribution that ultimately enhances the value of the
book, and I sincerely appreciate their efforts.
Good luck with your mission to provide quality pressure ulcer prevention and management. Geriatric care
is my first love, and I sincerely admire those who work in the difficult financial and regulatory environ-
ment we call long-term care. I believe in you, support you, admire your commitment, and sincerely hope
this information is useful to you. Please feel free to contact me through HCPro or by e-mail if you have
questions or comments.
Barbara Acello, MS, RN

Pressure Ulcers: Long-Term Care Clinical Manual
In addition to the care provided by physicians, some facilities are also fortunate to have the services of
advanced practice nurses (including nurse practitioners and clinical nurse specialists) and physician
assistants. These well-educated and highly qualified individuals provide excellent care to residents in
long-term care facilities. Collectively, we refer to these individuals as “healthcare providers” or “health-
care practitioners.” Occasionally, the term “physician” is used for brevity only. This is not intended to
minimize the important work of advanced practice nurses and physician assistants. When the reader is
advised to notify the physician, facilities may also notify the advanced practice nurse or physician assis-
tant, if available, and as required by state law and facility policies.
Every effort has been made to ensure that this material is timely and accurate at the time of publication,
but pressure ulcer care involves evidence-based practices that change frequently. The author, editors, and
publisher have done everything possible to ensure that this book is current and in compliance with the
standards of care. The author, editors, and publisher are not responsible for errors or omissions or for
consequences from application of the book, and make no warranty, expressed or implied, in regard to
the contents of the book. Neither the author nor the publisher nor any other individual or party involved
in the preparation of this information will be liable for any special, consequential, or exemplary damages
resulting in whole or in part from any individual’s use of or reliance on this material. The practices de-
scribed in this book should be applied in accordance with facility policies and procedures, state and
federal laws, the nurse practice act for your state, professional standards of practice, and the individual
circumstances that apply to each resident encounter and situation.
Disclaimer
Pressure Ulcers: Long-Term Care Clinical Manual
Facts About the Integumentary System
The skin is the largest organ of the body. The total skin weight of an average-size adult is about 6–8.8
lb. The skin covers an area of about 78.4 inches. It renews itself every 28 days. Each square inch of skin
consists of approximately 19 million cells, 60 hairs, 90 oil glands, 19 ft. of blood vessels, 650 sweat
glands, and 19,000 sensory cells. About one-third of the blood circulating in the body is used to nourish
the skin.
About 500 million skin cells fall off each day. This is about 1.5 lb. per year. By age 70, the average person
has lost about 105 lb. of skin. We shed and regrow about 1,000 new skins in a lifetime. Everyone has about
the same number of melanocytes, or cells that produce skin color. The skin color is determined by how
much or how little melanin each melanocyte cell produces. The skin has about 100,000 bacteria per
square centimeter. Ten percent of human dry weight is attributed to bacteria. The normal flora on the
skin provide a measure of protection from harmful pathogens.
The skin stretches in obesity, edema, and during pregnancy. The ability to stretch is called extensibility.
The ability to contract after stretching is called elasticity. Severe stretching may cause small tears. These
are initially red in color. Over time, they lose the redness and remain visible as silvery-white streaks called
striae (stretch marks).
Nails are extensions of the skin. It takes a nail approximately six months to grow from base to tip. The
fingernails grow faster than toenails and provide a permanent record of some illnesses and exposure to
certain chemicals. Hair is also part of the integumentary system. It too maintains a record of chemicals,
toxins, and other problems. There are more than 5 million hair follicles on the body. The average human
has about the same amount of hair as other hairy primates, but human body hair is short and fine. Scalp
hair grows faster than other body hair. The average scalp has about 100,000 hairs. Each lives about two to
Overview of Anatomy and Physiology of the Skin
Chapter 1
Chapter 12
Pressure Ulcers: Long-Term Care Clinical Manual
four years. The hair on the head grows at a rate of approximately 1 cm (0.3937 inches) per month. The
average person loses approximately 50–100 hairs from the head each day.
There are 650 sweat glands in 1 square inch of skin. Sweat from the underarm and genital areas is
odorless. Unpleasant body odors result from the action of bacteria on the sweat. The human body smell
is distinctive, as individual as a fingerprint, and unique to family groups.
The Integumentary System
The integumentary system consists of skin, hair, nails, sweat glands, nerves, and oil glands. It is elastic,
regenerates, and provides protection, thermoregulation, sensation, and elimination. These functions are
essential for life. Changes in the appearance of the skin are related to aging, abnormalities, or diseases.
The skin constantly interacts with the environment. It has many functions that are critical to the well-
being of the body:
• Protection—forms a continuous membranous covering for the body
• Storage—stores fat and vitamins
• Elimination—loses water, salt, and heat through perspiration
• Sensory perception—contains nerve endings that keep us aware of environmental changes
The skin tells us much about the general health of the body:
• If fever is present, the skin is hot and dry
• Cool and clammy skin accompanies certain cardiovascular problems
• Redness or flushing of the skin occurs when someone is embarrassed or after strenuous activity
• Many medical conditions produce pale skin
• The skin is cyanotic when oxygen content of the blood is low
Skin layersThe skin (Figure 1.1) consists of three distinct layers: epidermis, dermis, and subcutaneous tissue. The
epidermis, or top layer, is fastened to the dermis, or second layer. The dermis consists of thick connective
tissue. Persons with thin skin have a thin epidermis; those with thick skin have a fairly thick epidermis.
Overview of Anatomy and Physiology of the Skin 3
Pressure Ulcers: Long-Term Care Clinical Manual
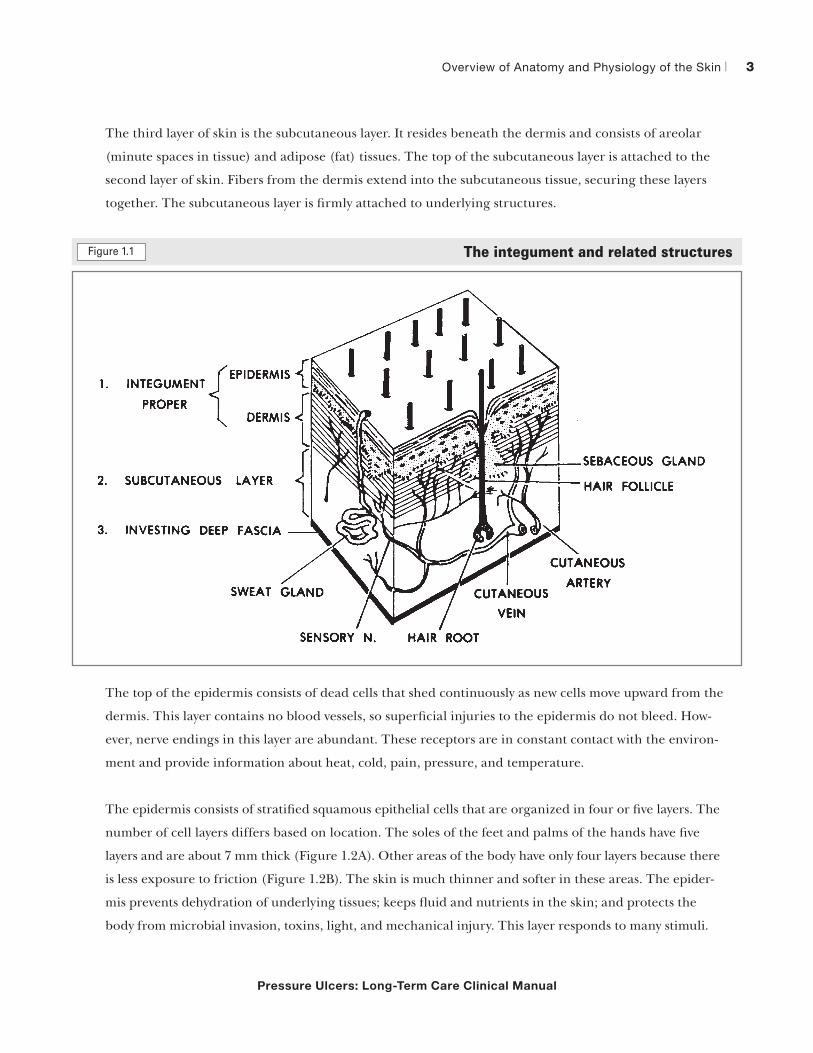
The third layer of skin is the subcutaneous layer. It resides beneath the dermis and consists of areolar
(minute spaces in tissue) and adipose (fat) tissues. The top of the subcutaneous layer is attached to the
second layer of skin. Fibers from the dermis extend into the subcutaneous tissue, securing these layers
together. The subcutaneous layer is firmly attached to underlying structures.
The integument and related structuresFigure 1.1
MD0006 3-2
LESSON 3
THE HUMAN INTEGUMENTARY AND FASCIAL SYSTEMS
Section I. GENERAL
3-1. DEFINITIONS
An organ system is a group of organs together performing an overall function.Portions of two organ systems, the integumentary and fascial systems, are representedin figure 3-1.
Figure 3-1. The integument and related structures.
a. Integumentary System. The integumentary system includes the integumentproper and the integumentary derivatives. We know the integument proper as the skin.It is the outermost covering of the whole body. The integumentary derivatives includethe hairs, nails, and various glands of the skin.
b. Fascial System. A fascia is a sheet or collection of fibrous connective tissue(FCT). The superficial fascia is the connective tissue which lies immediately beneaththe skin and is often known as the subcutaneous layer. Deep fasciae (plural) formenvelopes for muscles and other organs and fill spaces. One deep fascial membrane isthe third envelope of the whole body, beneath the skin and the subcutaneous layer. It isknown as the investing deep fascia.
The top of the epidermis consists of dead cells that shed continuously as new cells move upward from the
dermis. This layer contains no blood vessels, so superficial injuries to the epidermis do not bleed. How-
ever, nerve endings in this layer are abundant. These receptors are in constant contact with the environ-
ment and provide information about heat, cold, pain, pressure, and temperature.
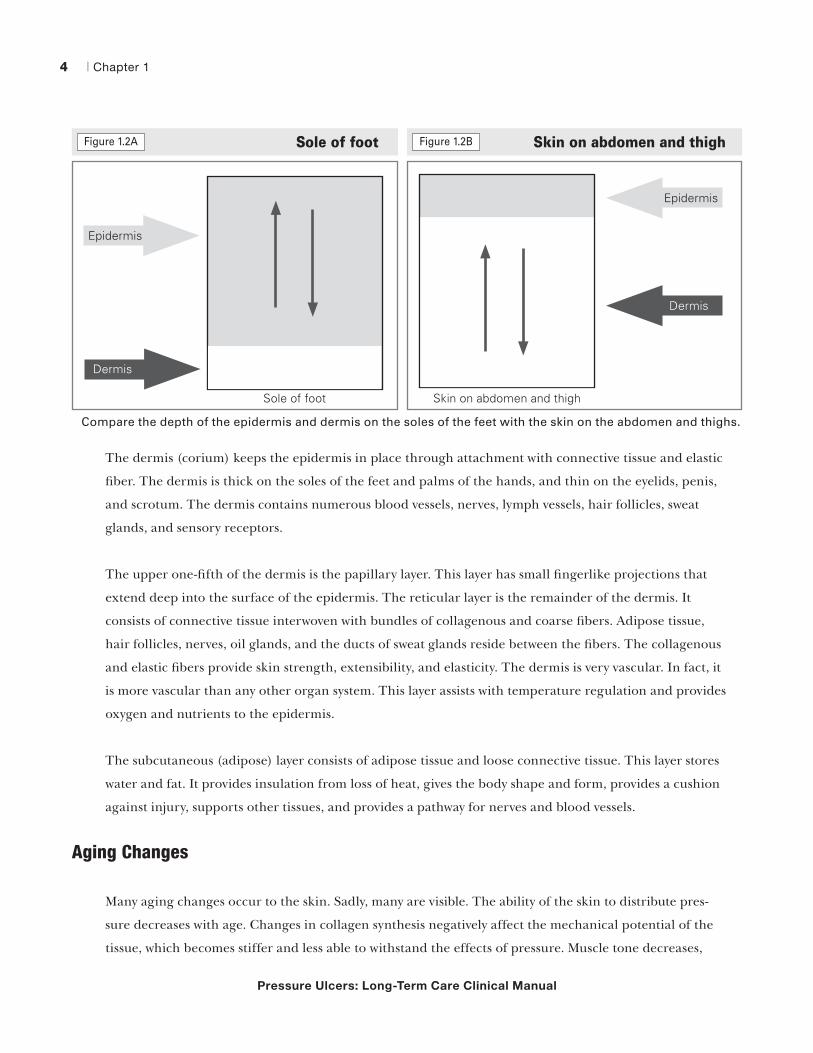
The epidermis consists of stratified squamous epithelial cells that are organized in four or five layers. The
number of cell layers differs based on location. The soles of the feet and palms of the hands have five
layers and are about 7 mm thick (Figure 1.2A). Other areas of the body have only four layers because there
is less exposure to friction (Figure 1.2B). The skin is much thinner and softer in these areas. The epider-
mis prevents dehydration of underlying tissues; keeps fluid and nutrients in the skin; and protects the
body from microbial invasion, toxins, light, and mechanical injury. This layer responds to many stimuli.
Chapter 14
Pressure Ulcers: Long-Term Care Clinical Manual
Sole of footFigure 1.2A
Sole of foot
Epidermis
Dermis
The dermis (corium) keeps the epidermis in place through attachment with connective tissue and elastic
fiber. The dermis is thick on the soles of the feet and palms of the hands, and thin on the eyelids, penis,
and scrotum. The dermis contains numerous blood vessels, nerves, lymph vessels, hair follicles, sweat
glands, and sensory receptors.
The upper one-fifth of the dermis is the papillary layer. This layer has small fingerlike projections that
extend deep into the surface of the epidermis. The reticular layer is the remainder of the dermis. It
consists of connective tissue interwoven with bundles of collagenous and coarse fibers. Adipose tissue,
hair follicles, nerves, oil glands, and the ducts of sweat glands reside between the fibers. The collagenous
and elastic fibers provide skin strength, extensibility, and elasticity. The dermis is very vascular. In fact, it
is more vascular than any other organ system. This layer assists with temperature regulation and provides
oxygen and nutrients to the epidermis.
The subcutaneous (adipose) layer consists of adipose tissue and loose connective tissue. This layer stores
water and fat. It provides insulation from loss of heat, gives the body shape and form, provides a cushion
against injury, supports other tissues, and provides a pathway for nerves and blood vessels.
Aging Changes
Many aging changes occur to the skin. Sadly, many are visible. The ability of the skin to distribute pres-
sure decreases with age. Changes in collagen synthesis negatively affect the mechanical potential of the
tissue, which becomes stiffer and less able to withstand the effects of pressure. Muscle tone decreases,
Skin on abdomen and thighFigure 1.2B
Skin on abdomen and thigh
Epidermis
Dermis
Compare the depth of the epidermis and dermis on the soles of the feet with the skin on the abdomen and thighs.
Overview of Anatomy and Physiology of the Skin 5
Pressure Ulcers: Long-Term Care Clinical Manual
subcutaneous tissue is reduced, and inadequate nutrition (which is common in older persons) affects
healing ability. Dehydration and inadequate fluid intake further reduce skin elasticity and increase the
risk of injury. Aging changes include:
• Subcutaneous fat and elastin diminishes
• The skin thins, loses elasticity, and develops wrinkles
• The skin becomes dry and fragile
• Blood vessels near the skin surface become more prominent
• Blood vessels that nourish the skin become more fragile with reduced capillary blood flow; senile
purpura are common and healing is delayed
• Blood supply to lower extremities is reduced, increasing the risk of skin breakdown, gangrene,
amputation, and related complications
• Sensitivity to pressure and temperature is reduced
• Age spots become evident
• Risk of injury increases; the skin bruises, cuts, tears, and breaks more readily
• A person may complain of feeling cold
• Risk of pressure, friction, and shearing injuries increases
• Glandular activity decreases
• Oil glands secrete less, causing the skin to dry and possibly become pruritic (scratching may
cause injury)
• Perspiration decreases
• Thermoregulatory ability is impaired
• Veins dilate
• Risk of injury increases due to impaired sensation
• Melanin production is decreased; color is lost and hair turns gray
• Hormone production changes; females develop facial, chin, and upper lip hair
• Scalp, pubic, and axillary hair thins
Chapter 16
Pressure Ulcers: Long-Term Care Clinical Manual
• Finger and toenail growth slows
• Nails become brittle, develop longitudinal ridges, and split or tear
Pressure Ulcers
An ulcer is a skin lesion in which the epidermis and upper dermis have been destroyed. Ulcers have many
causes, including skin trauma, chemicals, parasites, tumors, and infections. Those caused by pressure
often result in rapid, extensive tissue destruction. An ulcer always results in a scar.
A pressure ulcer is any lesion caused by unrelieved pressure that results in damage to underlying tissue.
Humans have more pain receptors than any other type of sensory nerve receptor. Even a small red area
or break in the skin can be very painful.
Pressure ulcers usually occur over bony prominences and are staged to classify the degree of tissue
damage that is observed or identified during the nursing assessment. Ulcers that are covered with eschar
or large amounts of slough are considered unstageable. Pressure ulcers do not necessarily progress from
Stage I to Stage IV or heal from Stage IV to Stage I.1
Although friction and shear are not primary causes of pressure ulcers, they are some of the most impor-
tant contributing factors to pressure ulcer development.2 Pressure ulcers are largely, but not 100%
preventable,3 and they are much easier to prevent than treat. They take a long time to heal, and even
after healing, the tissue is scarred and is never as strong as it was previously.
Wound Healing
Partial-thickness wounds involve the epidermis and upper dermis and heal by regeneration. Function is
not lost, and scar tissue does not form for most superficial injuries. Full-thickness wounds result from
destruction of the epidermis, dermis, and subcutaneous tissue. Muscle and other structures may also be
damaged. Full-thickness wounds heal by scar tissue formation, which involves granulation, contraction
(wound shrinkage), and epithelialization. A full-thickness pressure ulcer (Stage III or IV) can never
revert to a partial-thickness wound (Stage I or II). Healing occurs in three stages:
• The inflammatory phase occurs immediately after injury and lasts a brief time in partial-thickness
wounds. The wound experiences an inflammatory response with heat, redness, pain, swelling, and
impaired function. Inflammation usually lasts about three days. Vasoconstriction occurs within seconds
Overview of Anatomy and Physiology of the Skin 7
Pressure Ulcers: Long-Term Care Clinical Manual
after injury and lasts a few minutes. It is followed by vasodilation, which is caused by local stimulation
of the nerve endings. The wound produces a serous exudate that forms a scab if allowed to dry.
• The proliferative phase overlaps the inflammatory phase slightly and continues until the wound
heals. This phase involves regrowth of the epidermis. (Epithelialization is part of this stage but
actually begins within hours of injury, during the inflammatory phase.) Small partial-thickness
wounds that have been left open to air will heal in about six to seven days. Moist wounds will heal in
about four days. Wounds involving loss of the epidermis and dermis repair both layers simultane-
ously. By the ninth day, collagen fibers emerge in the wound bed of a Stage II ulcer. Collagen synthe-
sis continues until about 10 or 15 days after the injury and continues to produce new connective
tissue. Collagen synthesis requires vitamin C, amino acid, and adequate nutritional intake. Some
experts theorize that cells surrounding hair follicles contribute con siderably to dermal repair,
accelerating healing in hairy areas of the body. In wounds with substantial tissue loss, granulation
tissue contracts to close the area. This contracture does not occur in wounds with little tissue loss.
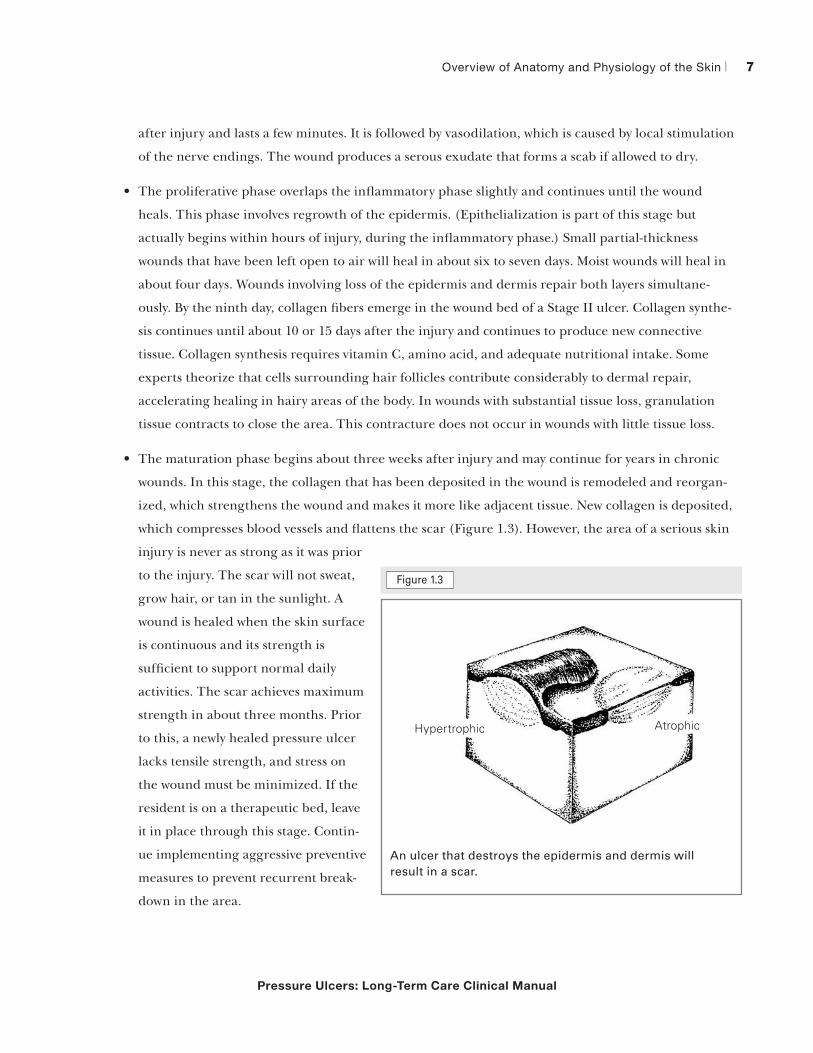
• The maturation phase begins about three weeks after injury and may continue for years in chronic
wounds. In this stage, the collagen that has been deposited in the wound is remodeled and reorgan-
ized, which strengthens the wound and makes it more like adjacent tissue. New collagen is deposited,
which compresses blood vessels and flattens the scar (Figure 1.3). However, the area of a serious skin
injury is never as strong as it was prior
to the injury. The scar will not sweat,
grow hair, or tan in the sunlight. A
wound is healed when the skin surface
is continuous and its strength is
sufficient to support normal daily
activities. The scar achieves maximum
strength in about three months. Prior
to this, a newly healed pressure ulcer
lacks tensile strength, and stress on
the wound must be minimized. If the
resident is on a therapeutic bed, leave
it in place through this stage. Contin-
ue implementing aggressive preventive
measures to prevent recurrent break-
down in the area.
Figure 1.3
Figure 3-12. Scar.
(7) Keloid. A keloid appears in an area of injury or just arises spontaneously; it is a smooth overgrowth of fibroblastic tissue (tissues composed of spindle-shaped cells). A typical keloid is first noticeable as a small, fairly firm nodule and slowly becomes a marked, several-lobe mass of a dark brown color. The keloid has spontaneous burning, itching, and tingling. Keloids are more frequent in blacks.
(8) Atrophy. Skin atrophy (figure 3-13) is a thinning and wrinkling of the epidermis often seen in the aged. Another type of skin atrophy is the stretch marks seen in the skin of women who have been pregnant or in the skin of people who have had a large weight loss. Glistening white bands in the skin are typical of these stretch marks, the bands having been caused by overstretching and weakening of the elastic tissue of the skin.
Figure 3-13. Atrophy.
e. Special Skin Lesions.
(1) Comedo (blackhead). A comedo or blackhead develops when sebaceous glands become enlarged because of accumulated serum. Blackheads more commonly happen during adolescence and are usually found over the face, chest, and
MD0575 3-10
AtrophicHypertrophic
An ulcer that destroys the epidermis and dermis will result in a scar.

Chapter 18
Pressure Ulcers: Long-Term Care Clinical Manual
Healing by primary intentionWounds that are cleanly incised with approximated edges can be sutured. This is healing by primary
intention. Very little granulation tissue is present, and a wound of this type usually heals rapidly with
minimal scar tissue. The stages of healing are the same as with any other wound.
Healing by secondary intentionWounds heal by secondary intention when they are not sutured and left to close naturally. These wounds
take longer to heal than those closed by primary intention. In healing by secondary intention, granula-
tion tissue helps fill the wound. Contraction and epithelialization occur, which usually results in consid-
erable scar tissue. The tissue will always be more susceptible to recurrent breakdown.
References
1. The National Pressure Ulcer Advisory Panel (NPUAP). (2007). “Pressure Ulcer Stages Revised by NPUAP.” Retrieved March 2, 2010,
from www.npuap.org/pr2.htm
2. Cuddigan, J.; Ayello, E.A.; Sussman, C.; & Baranoski, S. (Eds.). (2001). “Pressure Ulcers in America: Prevalence, Incidence, and
Implications for the Future.” National Pressure Ulcer Advisory Panel Monograph (p. 181). Reston, VA: NPUAP.
3. NPUAP. “Not All Pressure Ulcers Are Avoidable.” Press release, March 3, 2010. Online April 29, 2010, www.npuap.org/A_UA%20
Press%20Release.pdf
Name
Title
Organization
Street Address
City State ZIP
Telephone Fax
E-mail Address
Order your copy today!
Title Price Order Code Quantity Total
$
Shipping* $ (see information below)
Sales Tax** $ (see information below)
Grand Total $
*Shipping InformationPlease include applicable shipping. For books under $100, add $10. For books over $100, add $18. For shipping to AK, HI, or PR, add $21.95.
**Tax InformationPlease include applicable sales tax. States that tax products and shipping and handling: CA, CO, CT, FL, GA, IL, IN, KY, LA, MA, MD, ME, MI, MN, MO, NC, NJ, NM, NY, OH, OK, PA, RI, SC, TN, TX, VA, VT, WA, WI, WV.
State that taxes products only: AZ.
BIllInG OPTIOnS:
Bill me Check enclosed (payable to HCPro, Inc.) Bill my facility with PO # ________________
Bill my (3 one): VISA MasterCard AmEx Discover
Signature Account No. Exp. Date
(Required for authorization) (Your credit card bill will reflect a charge from HCPro, Inc.)
© 2008 HCPro, Inc. HCPro, Inc. is not affiliated in any way with The Joint Commission, which owns the JCAHO and Joint Commission trademarks. Code: EBKSMPL
Order online at www.hcmarketplace.com Or if you prefer: MAIl ThE COMPlETEd OrdEr fOrM TO: HCPro, Inc. P.O. Box 1168, Marblehead, MA 01945
CAll Our CuSTOMEr SErvICE dEPArTMEnT AT: 800/650-6787
fAx ThE COMPlETEd OrdEr fOrM TO: 800/639-8511
E-MAIl: [email protected]
P.O. Box 1168 | Marblehead, MA 01945 | 800/650-6787 | www.hcmarketplace.com
Please fill in the title, price, order code and quantity, and add applicable shipping
and tax. for price and order code, please visit www.hcmarketplace.com. If you
received a special offer or discount source code, please enter it below.
Your order is fully covered by a 30-day, money-back guarantee.
Enter your special Source Code here:


















