Pyriform sinus tumours principles of management
28
PYRIFORM SINUS TUMOURS PRINCIPLES OF MANAGEMENT DR.ROOHIA
-
Upload
md-roohia -
Category
Health & Medicine
-
view
16 -
download
2
Transcript of Pyriform sinus tumours principles of management
PYRIFORM SINUS TUMOURS PRINCIPLES OF MANAGEMENT
DR.ROOHIA

The goals of treatment for this patient population are:
(1) cure with preservation of function (2) palliation with minimal morbidity
Factors Affecting Choice of Treatment
Age:pts above the age of 75yrs hv poor prognosis due to their general poor condition surviaval rate is about 10% comparable to others.
Associated Medical Conditions should be included when considering treatment options
Eligibility criteria for investigational nonsurgical chemoradiation protocols include
adequate performance status as well as reasonable hematologic, hepatic, renal
and cardiovascular function

Past Medical/Surgical History previous exposure to platinum
compounds makes significant responses less likely.
Repeat external irradiation or brachytherapy are poor options for patients who have received prior radiotherapy to the head and neck

TNM Staging, Quality of life
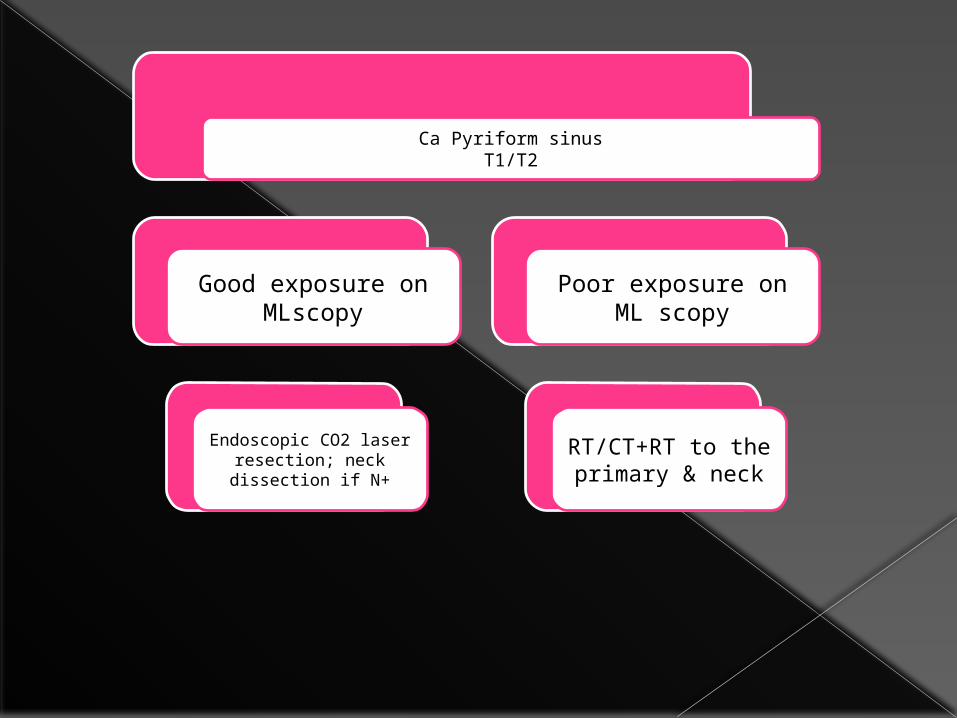
Ca Pyriform sinusT1/T2
Good exposure on MLscopy
Endoscopic CO2 laser resection; neck dissection if N+
Poor exposure on ML scopy
RT/CT+RT to the primary & neck

T3
Mobile cords; superficial infiltration
Good exosure on MLscopy
Endoscopic CO2 laser resection
1.If resection margins
unsatisfactory –postop RT
2.If N+ Neck
dissection+post op RT
If resection margins satisfactory ,N0
-withhold RT, treat with 2 cycles of adj
CT &follow up regularly
Poor exposur on Mlscopy
Lateralised lesion
1.CT followed by a. RT in good resonders b.NTPL+RT in poor
res2.NTPL+RT
Cord fixity; deep infiltration
Non-lateralised
1.sequential/concurrent chemo radiation
2.Total LP+RT
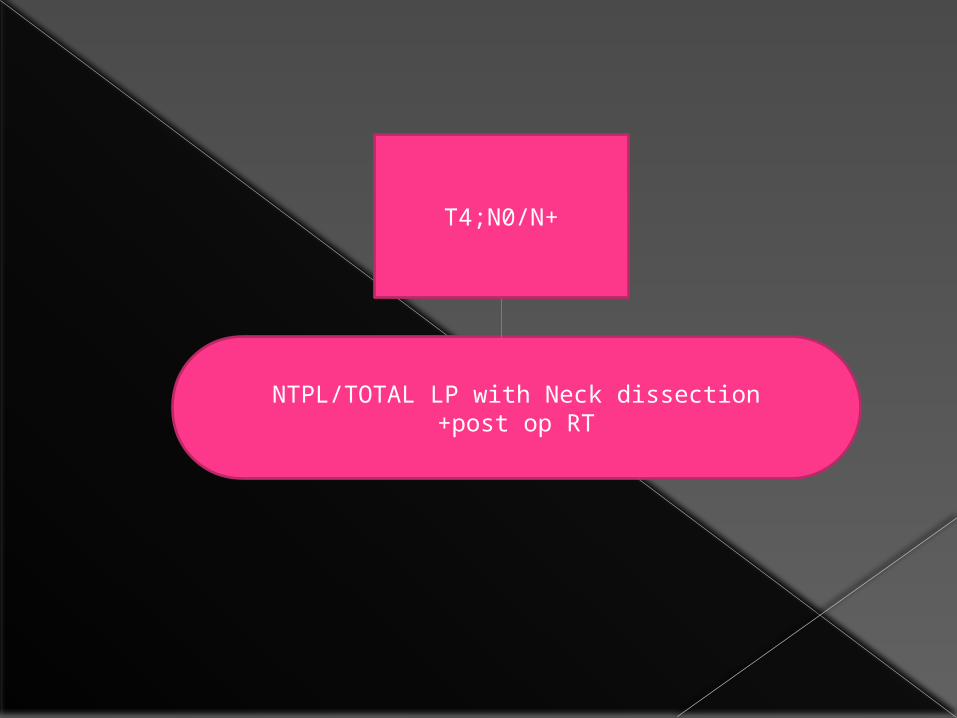
NTPL/TOTAL LP with Neck dissection+post op RT
T4;N0/N+
Radiotherapy
Radiotherapy as a single treatment modality for early (T1-T2) pyriform sinus carcinoma(curative RT)
The rates of local control decrease in bulky T2 lesions, in those larger than 2.5 cm,
and in those extending to the apex of the pyriform
sinus. Better results in terms of local control are observed in patients with favorable T2 lesions characterized
by exophytic tumor, good airway, normal cord mobility, and uninvolved apex.
Conventionally fractionated radiotherapy employing total doses of 60-70 Gy in 30-35 fractions,(2Gy/fraction) over 6-7 weeks
Accelerated fraction RT: same dose given over shorter period
HyPer fraction RT: traditional dose broken into smaller fractions over same time
Prevents repopulation of tumour Decrese duration of treatment and hos stay
In too advanced disease,distant metastasis,poor condition for sugery palliative RT .
Dose depends on extent &tolerance of tissues.
If RT alone- can be delivered with external beam or brachytherapy or both
Combined RT with surgery or CT Preop RT: poorly oxygenated cells are
much less susceptible to irradiation than oxygenated cells
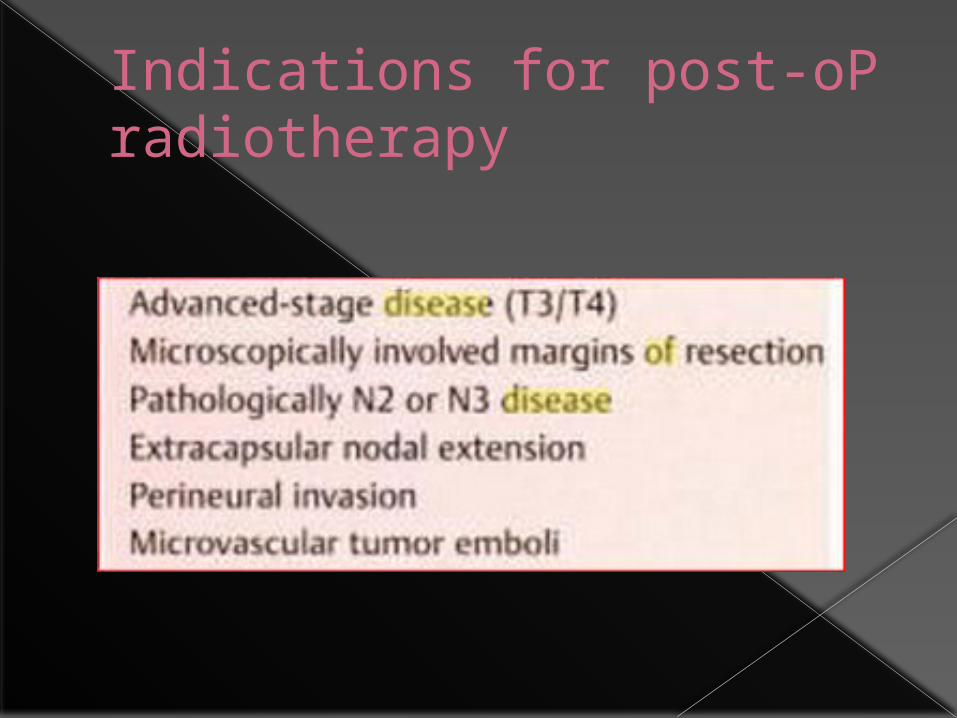
Indications for post-oP radiotherapy
POST OP RT: Identification of tumour extent more accurate Technical performance easier in tissue planes
have not been altered by fibrosi,fusions,increased vascularity due to RT.
Results are poor if delayed beyond 6 wks Minimum tumour dose 50-60Gy daily fractions
2Gy to whole operative bed with boost 63Gy to sites of increased risk.
DFS- 2yrs -74% Over all survival 5yrs -31%(RTOG)
RT to nodes : >3cm nodes oor response to RT 53-83% response rste seen in nodal involvement N0,N1- cotrol with RT N2,N3- needs CT/RT if clinically radiologically
incomplete resonse then surgery. If neck dissetion lanned after 4-6wks of RT then
dose can be reduced frm 70 to 50Gy. Involvement of low level nodes –needs reduction
in dose to avoid damage to brachial plexus
Advances in RT: Ct based high precision RT IMRT IGRT Advantage increased QOL Eg: decreased dose to arotid gland –
saliva flow preserved-xerostomia reduced
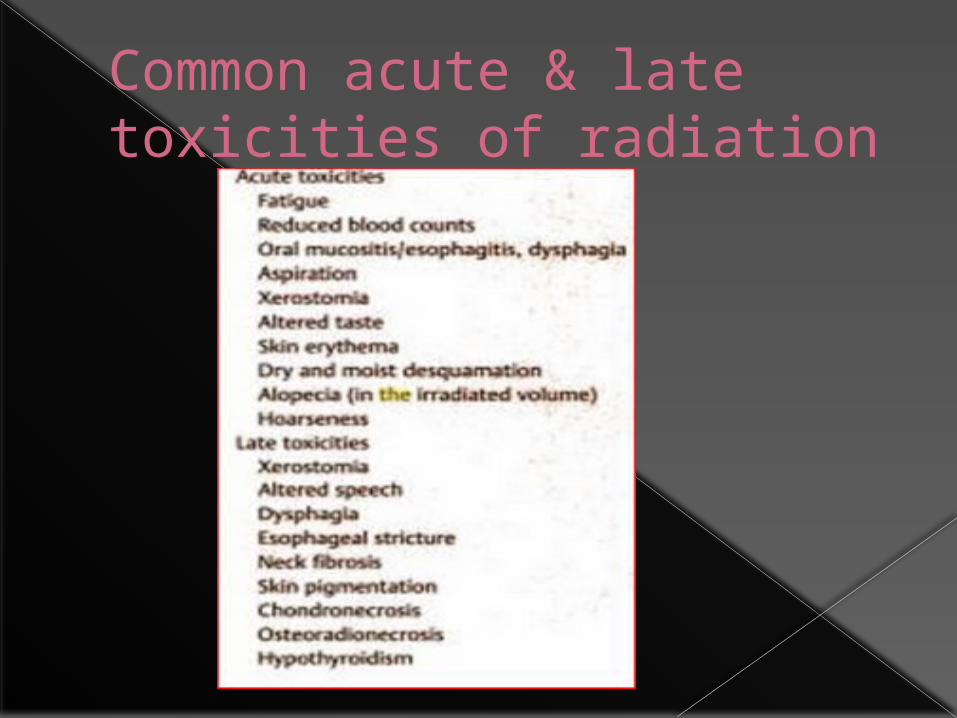
Common acute & late toxicities of radiation
CHEMOTHERAPY
Goals of organ preservation: Maintainance of oral alimentation Protection of laryngeal airway Intelligible laryngeal speech
Chemotherapy
Role of chemotherapy is mainly as combination or for palliation
Neoadjuvant chemotherapy followed by RT(The Veteran’s Affairs study)
CT given before surgery/RT.more efficient drug delivery can occur.
A)CT responders well respond to RT B)CT response downstage disease may allow RT
effective C)CT may reduce incidence of distance metastasis
when local disease well controlled Laryngeal preservation 62% Overall survival35%
Concurrent chemo-RT(RTOG)(T3/T4) RT &CT used simultaneously in uresectable
disease. 3arm study 1)neoadjuvant CT(cisplatin+5FU) followed by
RT. 2)RT with concurrent CT(cisplatin100mg/m2 on
1,22,43 days) 3)RT alone Excluded T4 those cartilage eroded,inavde
tongue
ResultsatA)2 yr intact larynx in 88% RT+concurrent CT 75% neoadjuvant CT followed RT 70% RT aloneB)Locoregional control 78%,61%,56% C)Distant metastasis suressed inCT based regeme….
Over all survival rate is sameD)High-grade toxic effects greater with CT Based
regemeE)Mucosal toxicity concurrent RT+cisplatin higher
Adjuvant CT: CT after surgery or RT goal of this secondary treatment is palliation &rarely has longterm benefits.
Induction CT+ concurrent chemoRT: Addition of taxane tomcisplatin ,5FU
under study to imrove survival outcomes.
Commonly used CT agents in pyriform sinus tumours
Cis platinum: Inorganic metal comound binds to DNA causes
inter or intra strands cross linking Dose:80-120mg/m2 every 3-4wkly with mannitol
diuresis. 5FU: Competes with enzyme thymidylate
synthetase,inhibiting tymidine formation decrese in DNA synthesis.
Dose:10-15mg/kg/wk 400-500mg/m2 daily for 5days IV as loading dose
followed by 400-500mg/m2 wkly IV.OR
Side effects of chemotherapy
TAXANES:paclitaxel-135-250mg/m2 3-24hrs every 3wks
docetaxel-60-100mg/m2 bolus every 3wks
These act on G2 phase cause arrest of cell cycle
Toxocity:neutropenia,infection

Novel CT agents which acts on EGFR: Monoclonal antibodies-
cetuximab4oomg/m2 initially followed by 250mg/m2 per wk
Small molecular tyrosine kinase inhibitors -erlotinib -gefitinib 80-90% of H&N cancers over expresses
EGFR…

SURGICAL MANAGEMENT
THANK YOU