Psychiatry
56
View with images and charts Quality of Inpatient Services in National Institute of Mental Health 1.1 Introduction To determine what psychiatric services are required for a community, it is necessary to know the frequency of mental disorder in the population and the needs for the treatment of the people with the disorders identified in this way. Policy decisions have to be made about the division of care between primary and specialist medical services, between medical and social services and people with different kind of mental disorders. In the National Health Service priority is given to people with serious mental illness. It is difficult to determine the exact frequency of mental disorders in a community, but approximate estimate are usually sufficient for service planning. (1) Assessment of the quality of psychiatric care is currently a challenge in the whole world. Definitions of quality in each country may be based on cultural values and national traditions. An international discussion should consider national peculiarities and priorities. Different papers and study in different countries, which presents a international approach to quality assessment of psychiatric care, is intended to contribute to such an international discussion. (1) Quality assurance project as proposed by the government of Bangladesh focuses on the following issues- Adequacy of the care provided – is the care provided appropriate for the patients and their health problem? Effectiveness of care provided – has the health care provided obtained his/her goal i.e has the health problem being solved? Safety of care provided – was the care provided safety and have preventable side effects been prevented or if not prevented have they been documented and taken care of? Efficiency of care provided – has care been provided with minimum of unnecessary use of resources?
-
Upload
regan-ahmed -
Category
Documents
-
view
213 -
download
1
description
Â
Transcript of Psychiatry

View with images and charts
Quality of Inpatient Services in National Institute of Mental Health
1.1 Introduction
To determine what psychiatric services are required for a community, it is necessary to know the frequency of mental disorder in the population and the needs for the treatment of the people with the disorders identified in this way. Policy decisions have to be made about the division of care between primary and specialist medical services, between medical and social services and people with different kind of mental disorders. In the National Health Service priority is given to people with serious mental illness. It is difficult to determine the exact frequency of mental disorders in a community, but approximate estimate are usually sufficient for service planning.(1)
Assessment of the quality of psychiatric care is currently a challenge in the whole world.Definitions of quality in each country may be based on cultural values and national traditions. An international discussion should consider national peculiarities and priorities. Different papers and study in different countries, which presents a international approach to quality assessment of psychiatric care, is intended to contribute to such an international discussion.(1)
Quality assurance project as proposed by the government of Bangladesh focuses on the following issues-
Adequacy of the care provided – is the care provided appropriate for the patients and their health problem?
Effectiveness of care provided – has the health care provided obtained his/her goal i.e has the health problem being solved?
Safety of care provided – was the care provided safety and have preventable side effects been prevented or if not prevented have they been documented and taken care of?
Efficiency of care provided – has care been provided with minimum of unnecessary use of resources?
Satisfaction among patients and health care workers with the care provided. Resources utilization – includes manpower and technology.
Approach to evaluation of a psychiatric service:There are two approaches to the evaluation of psychiatric services for a community;
Studies of whole services, and Studies of particular element of service, such as the inpatient’s care.
The two approaches are complementary. Either evaluation requires a clear statement of aims in which inputs, processes, and outcomes are distinguished. Inputs are the resources made available such as the number of beds or the number of community psychiatric nurses. Processes are the ways that resources are used ,for example the number of in-patient admissions and length of stay. Outcomes are the measures of the effects of the services such as symptom reduction, burden on cares and suicide rates.(ref.1,p-787).Wing and Haily (1972) suggested six questions that should be asked about the psychiatric services for a population:
How many patients are in contact with the service? What are their needs and those of the relatives? Are services meeting these needs at present? How many others, not in contact with the service, also have needs?
What new services, or modifications to existing services, are required to cater for unmet needs?
Having introduced the new or modified services, are the needs met?
The question can be asked as a check on an established service, or to examine the effect of a change such as the closure of a hospital. Question of cost can be added to the above list. (1)
An increasing concern with improving the quality of care in various components of health care system has led to the adoption of quality improvement approaches originally developed for industry. These include total quality management(TQM) (Deming 1986), an approach which employs process control measures to ensure attainment of defined quality standards and continuous quality improvement (CCQ) (Juran 1988), a strategy to engage all personnel in an organization in continuously improving quality of service. (4)
The quality assurance project for National Hospital inpatient quality measures was set by DGHS. There is also an international standard for Inpatient psychiatric services finalized. A three dimensional model was developed was developed in which 23 quality standards may be applied to 28 areas of practice. (2)
The group defined 23 quality standards in four categories: treatment goals, primary intentions, means and organization, and optimal use of resource. The group outlined 28 areas of practice of inpatient care to which the standards may be applied. These areas of practice are admission procedures; diagnostic procedures; drug therapy and other physical treatments; nonspecific and specific psychotherapy; occupational therapy and work therapy; support for living accommodations and self-care; support for work, occupation, and education; support for social contacts and leisure; interaction with relatives; meeting of basic material needs; discharge procedures; handling of compulsory treatment; general medical care and liaison service; therapeutic relationships; treatment and care planning; time management; the therapeutic milieu; operational ward policy; teamwork in treatment; the information and communication system; the documentation system; organization and administration on the ward; management of staff; the hospital’s management structure; cooperation between management and clinical staff; public relations; advocacy of patients’ interests; and accessibility. (14,15,16)
In theory, each quality standard may be applied to each area of practice, so that each aspect of quality may be assessed in any given area. This two-dimensional model was then extended by a third dimension. For any application of a standard in an area of practice, questions may be asked on the level of the individual patient, the treatment unit (usually a ward), and the whole institution or hospital. For the patient, a distinction is made between the treatment process and outcome. (2)
1.2 Background of the studyUntil the middle of the eighteenth century, there were hardly any special provisions for the mentally ill. In England the only hospital for these patients was the Bethlem hospital, founded in 1247.In most of the continental Europe, there was a similar lack of hospital provision; in the middle ages, hospitals in Spain were a notable exception(Chamberlain 1966).Nearly all mentally ill people lived in the community, often with help from Law provisions, or else they were in prison .In England the Vagrancy act of 1744 made the first legal distinction between paupers and lunatics, and made provision for the treatment of the latter. In response, private provisions for the mentally ill(madhouses-later to be called private asylums) were developed mainly for those who could pay for care, but also for some paupers supported by their parishes. At about the same time a few hospitals or wards were established through private benefaction and public subscription. The Bethel hospital in Norwich was founded in 1713.In London, the lunatic hospital was established in 1728,and in 1751, St.Luke’s hospital was
founded as an alternative to the overcrowded Bethel hospital. Then, as now, the value of psychiatric wards in general hospitals was debated. (1) Psychiatry in Bangladesh: Past and Present:Bangladesh did not have any psychiatric services in erstwhile East Pakistan until 1957.During that time only available psychiatric facilities was forty cells of Dhaka Central Jail. There was no mental hospital in the East Pakistan though there was three mental hospital in West Pakistan at Lahore, Hydrabad and Peshwar. Psychiatric services was vary unsatisfactory in undivided Banglal. Only observational unit was established in Barhampur in Murshidabad which was abolished following decision of establishing a modern mental hospital in Ranchi, Bihar jointly by the Govt. of Bengal and Bihar. Remnants of those patients of Ranchi are still be to found in Pabna who were transferred in 1962 following establishment of mental hospital in Pabna. There was no psychiatric subject in medical curriculum except a few lectures which were given by a teacher of Jurispudence. The situation was similar in both West Bengal and in erstwhile East Pakistan.
All the countries of this subcontinent shared same ancient law – Indian Lunacy Act, 1912 with modification here and there. Though there has been lot of improvement both in treatment facilities, law etc. in all countries which comprised Indian subcontinent but in Bangladesh treatment facilities and legal framework is still struggling with primitive treatment facilities, ancient law and highly prejudiced medical profession. Result is the suffering of the people and erosion of prestige of medical profession in general in Bangladesh due to mechanical approach to the art of medicine.
History of psychiatry in Bangladesh began in 1957 when temporary mental hospital was opened in a ranted building in Pabna which was well known as ‘sitlai house’. Site of the permanent hospital was selected at Pabna and was located in the premise of an abandoned ashram of Shree Thakur which subsequently turned into 200 beded permanent mental hospital. First outdoor clinic was established in Dhaka Medical college in1964.Psychiatric outpatient was opened in IPGMR in 1972.A course specialization in psychiatry was started initially as diploma of psychological medicine(DPM) and subsequently for FCPS in psychiatry in1978.During the same period WHO was sponsoring a mental health project in Bangladesh and was holding workshop in collaboration with Govt. of Bangladesh with participants from medical administrators, teacher, psychiatrists, social workers, nurses etc. In 1978 outdoor clinics were opened in Mymensing and Chittagong medical college Unfortunately this had to be developed in some places due to paucity of manpower. Funds for mental clinics allocated in several plan periods were diverted for some other purpose at of the clinics which was built in Dhaka medical college hospital is an example. Stories were same regarding the fund allocated for mental clinics in Chittagong, Rajshahi etc. in various plan period. In pursuance of a decision in a W.H.O. seminar organization of training in mental health was established which was subsequently rechristened Institute Of Mental Health and Research. Then a separate and permanent institute for psychiatry was established at Sher–E-Banglanagar, Dhaka named National Institute Of Mental Health in 2001.We are gradually though slowly developing but we have to go a long way. Every field of psychiatry needs change and modernization. It may be noted that a well equipped psychiatric unit in general hospital with adequate physical facilities, appropriate personnel like psychiatrist, psychologist, social worker, occupational therapist can only function effectively both for training and service delivery. Future of psychiatry in Bangladesh lie in the development of integrated service delivery at the level of primary health care, development of general hospital psychiatry specially in teaching hospital, improvement of training facilities,

development of skilled psychiatric manpower and modernization of Lunacy Act of 1912 and Pakistan Mental Health Act. (3)
The purpose of the study to evaluate the current services provided to the psychiatric patients of Bangladesh where many people even their family suffers for proper psychiatric treatment and diagnostic support. The service quality should be upto the mark so that it could meet the adequate requirement and increasing demand and people of our country can get standard psychiatric facilities.
1.3 Justification of the studyWHO has defined health as “a state of complete physical, mental and social well being and not merely an absence of disease or infirmity so that each citizen can lead a socially and economically productive life”, so mental health is one important component of health. Mental diseases are ancient one and any person can be suffer from such disease or disorder any time irrespective of age, sex, geographical and socio-demographic condition, environment, education etc. Though the actual scenario of psychiatric disorder and their magnitude is not identified in Bangladesh but trough a survey conducted by WHO we find that about !% of our total population are suffering from serious psychiatric disorder and 10% are with other mental illness. About 30% are at the risk of developing such diseases and 50% patients who are physically ill have psychotic symptoms. Unlike most physical diseases mental illness begins very early in life. Half of the cases begin by age 14; the prime of life, when three quarters have began by age 24.Thus mental disorders are really chronic of the young. For example anxiety disorders often begin in late childhood, mood disorders in late adolescence, and substance abuse in early 20’s.Unlike heart diseases or most cancers, young people with mental disorders suffer disability when they are in the prime of life, when they would normally be the most productive for the family, community and nation. Also major mental disorders cost the nation in lost earnings alone. Lost earning potential, costs associated with treating existing conditions, social security payments, homelessness and incarceration are just of the some of the indirect cost associated with mental illness that have been difficult to quantify.
Direct cost associated with treating mental disorders like medication, clinic visit and hospitalization are relatively easy to quantify, but they reveal only a small portion of the economic burden these illness place in the society. There are very selective hospitals and health personnel in Bangladesh who provide services for these patients. It is necessary to evaluate and explore the existing services are standard enough to meet the needs and requirement of the nation and society. The people of our country have every right to get accessibility to a standard quality of psychiatric services so that these people can lead a socially and economically productive life and can contribute in the prospects and economy of the country, even in the progress of the whole community. (22)
1.4 Limitation of the studyDue to the short time period and lack of fund and proper specialist guidance only a portion of inpatient services are studied in this study which are not sufficient to take a decision related to the quality of the total services provided by the institute. Even the complete inpatient services can not covered by the researcher like the physical facilities, cleanliness, food supply etc. Furthermore the outpatient services, the emergency services, specific therapy style and outcome, particular disease frequency and treatment outcome, patients’ satisfaction level, academic situation – all these chapter remain untouched which need proper assessment and evaluation. After complete evaluation, assessment and research among the whole services of the institute we can comment on the present quality status of the National Institute of Mental

Health. We seek proper attention of government and particular authority for the evaluation and standardization of such hospitals and their services.
1.5 Research questionWhat is the quality of services provided to the indoor patients in National Institute Of Mental Health?
1.6 Research objectivesGeneral objectiveTo assess the quality of services provided to the indoor patients in National Institute Of Mental Health.
Specific objectives 1. To assess the quality of treatment facilities for the indoor patients in National Institute Of Mental Health.2. To identify the quality of diagnostic facilities available in National Institute Of Mental Health.3. To estimate the manpower in indoor department of National Institute Of Mental Health.
1.7 Key variables
1.7.1 Dependent variableQuality of inpatient services of National Institute Of Mental Health.
1.7.2 Independent variableAge of respondentsSex of respondentsReligion of respondentsDesignation of respondentsExperience of respondentsAdmission procedureDiagnostic facilitiesOther laboratory facilitiesDischarge procedureTreatment facilitiesFollow up careManpower facilitiesJob satisfactionVisitor’s restrictionLength of staySupport services for rehabilitation of patientsAdvocacy for patientsRecreation facilitiesSupervision by managementDocumentation and record systemInformation and communication system
1.8 Operational definition:QualityThe term refers to an attribute of goodness or degree of excellence of any work.
In patient departmentThat section of the hospital with all physical facilities ,regularly scheduled hours and personnel in sufficient numbers assigned to provide health care to the patients who are admitted and registered.Standard The precise count or quantity or model that specifies an adequate ,acceptable or optimal level of quality.Quality of serviceIt is the effective health care to improve the health status and satisfaction of a population within the resources which society and individual have chosen to spend or that care or it means the degree of excellence of medical attention offered to patient by a hospital.UtilizationEvaluation of the necessity, appropriateness and efficiency of the use of medical services, procedure or facilities.
EvaluationEvaluation means whether or not the organization is meeting planned activities. Evaluation requires that goals, objectives and activities be translated into standard that provide the basis for comparing planned activities or the programs with actual performance.Service facilitiesIt includes equipment, manpower and other facilities required for waiting, consultation, physical examination, diagnostic procedure and clinical care of patients. These facilities have got direct bearing on the overall management of patients and have impact on the quality of service as well.AssessmentThe identification and analysis of variety of factors that might explain function.Service providerHealth care workers including doctors, nurses, other support stuffs like cleaners, word boys, ayas, security stuffs etc. as engaged in providing health care services for the patients of NIMH.ProblemIt is a question or difficulty which requires a solution. It is the gap between the desired and actual state of affaires.A systemIt may be defined as an aggregation of functional interrelated units designed to achieve predetermined objectives. EfficiencyIt refers to the measure of how economically resources are utilized to achieve predetermined objectives. It involves reaching end by only the necessary means or by the least wasteful use of resources.EffectivenessIt is the relationship between an objective and the actual output.Psychiatric HospitalHospitals specializing in treatment of serious mental disorder. They vary widely in size and grading.Mental health lawArea of the law that is applied specifically to persons with a diagnosis or possible diagnosis of mental illness and to the people involved in managing or treating others in this situation. This includes area in both common law and statute law.Community law

It is based on case law rather than statues, issues includes such concepts as insanity defenses, sane and insane automatism amongst other. The laws generally allow for compulsory treatment in a psychiatric hospital or in the community.
1.9 Conceptual framework
Quality of inpatient service
Rehabilitation facilities Work therapy Support for living,
accommodation and self-care
Support for work, occupation and education
Support for social contacts
Manpower facilities Doctors Nurses Ward-boys Cleaners Security guards Management of the
staff Job satisfaction Public relation
Diagnostic facilities Admission procedure Diagnostic procedure Other diagnostic
procedures Discharge procedure
Other facilities Information and
communication system Documentation system Advocacy of patient’s
interests Reacreation Visitor restriction
Treatment facilities Drug therapy Cognitive therapy Electroconvulsive
therapy Nonspecific
psychotherapy Specific
psychotherapy Other physical
treatment Occupational therapy Handling of
compulsory treatment Treatment and care
planning Time management

Literature review
2. LITERATURE REVIEWIn Shorter Oxford Textbook of psychiatry the total management of psychiatric services in every type of psychiatric hospital and institute are described elaborately and stepwise. It describes the standard psychiatric services and treatment facilities. (1)
In Germany at the year of 1998 a study on assessing the quality of psychiatric hospital care was done to develop a tool for assessing the quality of psychiatric hospital care by a nonprofit organization which was commissioned by the German Ministry of Health. In this study a three-dimensional model was developed in which 23 quality standards may be applied to 28 areas of practice. For each application, question asked at four levels to stimulate ongoing quality management: the individual treatment process, the individual outcome, the treatment unit and the hospital as a whole. The authors provide sample questions to illustrate the approach. The quality assessment embodied in the model is comprehensive and addresses ethical issues, but it is also complicated and difficult to handle. Unlike model developed in the United States, it is not intended to be objective or standardized and it does not yield a score. To some extent, the model’s approach to assessment may reflect German cultural values and traditions. Although the manual has 373 pages, it does not give a specific definition of quality of hospital care or outline any implications for action. It provides guidelines for various potential users on how to assess the quality of a given hospital care procedure and how to ask questions about specific aspects of it. (2)
A study on “Analysis of healthcare quality indicator using data mining and decision support system” was done in South Korea by the Graduate school of Health Science and Management in and Department of Quality Improvement of Severance Hospital under Yonsei University Medical Centre. This study presents an analysis of health care quality indicators using data mining for developing quality improving strategies. Specifically important factors influencing the inpatient mortality were identified using a decision tree method for data mining based on 8405 patients who were discharged from the study hospital during the period of December 2000 to January 2001. Important factors for the inpatient mortality were length of stay, disease classes, discharge departments and age groups. The optimum range of target group in inpatient healthcare quality indicators were identified from the gains chart. In addition, a decision support system (DSS) was developed to analyze and monitor trends of quality indicators using Visual Basic 6.0. Guidelines and tutorial for quality improvement activities were also included in the system. Among the 8405 patients, 4451 (53.0%) were male and 3954 (47.0%) were female. Patients who were discharged from Internal Medicine departments were almost three times (6109). Patients in age group of 41-60 had the highest proportion (31.3%). Among all disease classes, neoplasm had the highest proportion (28.8%). Disease classes with the proportion of less than 5% were grouped under miscellaneous. The decision tree for inpatient mortality had 17 statistically significant nodes at 5% level. About 170 (2.0%) were inpatient mortality cases. The most significant factor explaining the infant mortality was length of stay (LOS). Discharge departments were the next significant factors, followed by the age groups. (4)
A study named “The evaluation and medical service quality of inpatient department of public and nonprofit hospital” in Choungguing, China affirmed by the Health Bureau of Nanjing. This study construct the evaluation index system of medical service quality for inpatient department and employs the analytical hierarchy process to determine weights of forces based on the judgment of the specialists. Ten public and nonprofit hospitals in Nanjing have
been studied; the result of evaluation of their medical service quality for inpatient department is gained, by using TOPSIS method and cluster analysis method. (5)
The Niagra Health System (NHS), Canada formed a quality improvement monitoring and reporting structure which is a series of linked committees and support departments. They developed a NHS quality reporting framework which serves to co-ordinate quality monitoring and reporting of information to continuously improve and enhance and to meet the Accreditation Canada standards. Now the quality framework is the foundation for the quality improvement throughout the NHS. They have utility management, laboratory accreditation, emergency preparedness, risk assessment tools, leadership walkarounds, automated unit dose drug system, medication unit dose, proper inpatient and outpatient services which are assured on the basis of their quality framework. (6,7)
A study was done by Department of Medicine and Prevented medicine, Uniformed Services University of the Health Sciences, Bethesda, USA named “Validity of the Department of Defense Standard Inpatient Data Record for quality Management and health services research”. Here the subjects were the patients whose inpatient charts were abstracted through the Civilian External Peer Review Program’s studies of acute myocardial infarction (N = 1,432) and 1993 review of the birth product line (N = 9,705). The ultimate result and analysis indicate that the Department of Defense’s SIDR (Standard Inpatient Data Record) is a reliable source of administrative data that compares favorably with traditional civilian quality management and health services research data sources, such as those from the Health Care Financing Administration and large insurers. (8) National Centre for Workforce Analysis, American Nurses Association, American Academy of Nurse Practitioners jointly conduct a study to see the relationship between the nursing services with the quality of patient care and patients outcomes in acute care and nurse staffing strategies that improved patient outcomes. The result was that the higher registered nurse staffing was associated with less hospital related mortality, failure of rescue, hospital acquired pneumonia and other adverse events but the association is not necessarily causal. The effect of increased registered nurse staffing on patient’s safety was strong and consistent. Greater registered nurse hours spent on direct patient care were associated with decreased risk of hospital related death and shorter length of stay. No studies directly examined the factors the factors that influence nurse staffing policy. Few studies addressed the role of agency staff. No studies evaluated the role of internationally educated nurse staffing policies. (9)
Agency for Healthcare Research and Quality (AHRQ) of Utah Department of Health conduct a study on “Using Hospital Inpatient Discharge Data for Quality Improvement and Statewide Surveillance: AHRQ Inpatient Indicators.” Here the comparison of the risk adjusted rate for Utah inpatient discharge and the national rate from the AHRQ National Healthcare Quality Report. The results reflect the association of quality improvement of inpatient service with the increased discharge and short stay in hospital. (10)
Quality assurance project as proposed by the government of Bangladesh has an accreditation checklist for the Upajila Health complex for primary health care but no such criteria for tertiary level hospital and psychiatric care. Any further evaluation or study not yet performed to improve the quality of inpatient services of a psychiatric hospital or other tertiary level hospital. (11)
Another quality measures developed by the North Carolina Healthcare Quality Alliance (NCHQA) in 2010 which was established to improve health care for North Carolinians

through promotion of evidence – based practice in primary care and measurement of health care quality using nationally recognized standards for care for specific health conditions. There is considerable scientific research into the design of measures to capture health care quality and numerous national organizations have developed and endorsed measures for preventive and acute care. Providers across North Carolina currently report data for quality measures as part of their participation in Community Care of North Carolina (CCNC) and/or as part of their agreements with state insurers. The implementation of the NCHQA will expand current reporting statewide and represents a significant initiative that can serve as a model to other states seeking to improve the health of their citizens through improved health care quality. Measures of quality have been chosen by the NCHQA partners to assess quality of care in the following five areas which represent a significant portion of health problems and health care expenditures among North Carolinas. Measures used in the NCHQA are based on nationally recognized evidence based standards such as those developed by the National Committee for Quality assurance and endorsed by the National Quality Forum (NQF) and which have been widely accept in the North Carolina Provider community. Assessment in progress regarding quality of care will be regularly conducted and will include critical review of the measures being used and the need to adjust them. But the extension of NCHQA to measures for other conditions and across the continuum of care is a long term goal. (12)
A study in Clearinghou was done titled “Hospital based inpatient psychiatric services: the percentage of patients discharged from a hospital based inpatient psychiatric setting with a continuing care plan created.” This measure is used to assess the percentage of patients discharge from a hospital based inpatient psychiatric setting with a continuing care plan created. Patients may not be able to fully report to their next level of care health care provider their course of hospitalization or discharge treatment recommendations. The aftercare instructions given the patient may not be available to the next level of care provider at the patient’s initial intake or follow up appointment. In order to provide optimum care, next level of care providers need to know details of precipitating events immediately preceding hospital admission, the patient’s treatment course during hospitalization, discharge medications and next level of care recommendations. (13,14,21,23) Evidence supporting the measures of criterion of quality were a clinical practice guideline for other peer-reviewed synthesis of the clinical evidence and one or more research studies published in a National Library of Medicine (NLM) indexed, peer-reviewed journal. Use of the measures is to improve performance. Currently it is used for routine use for internal quality improvement of hospitals, single health care delivery organizations. Here the target population were all patients age one year and older, either male or female and stratification by vulnerable population are children. (18,19,,21) A survey was conducted by an independent research organization named the Picker Institute Europe, on behalf of the local hospitals and it is about the National Health Service Hospital and recent experiences of the patients in the inpatient and emergency department. The survey totally based on the patient’s satisfaction level about the quality care of the inpatient and emergency services of the National hospitals. (20)
On April 19, 2010, the Centers for Medicare & Medicaid Services (CMS) issued a proposed rule that would revise policies and payment rates for general acute care hospitals that are paid for inpatient services under the Inpatient Prospective Payment System (IPPS), effective for discharges in fiscal (FY) 2011 – that is, on or after October 1, 2010. In addition to promoting accurate payment for inpatient services to Medicare beneficiaries, the proposed rule strengthens the relationship between payment and quality of service by expanding the quality
measures that hospitals must report in order to receive the full market basket update in fiscal year 2012. Under the Medicare law, hospitals that choose not to participate in the voluntary reporting program or do not participate successfully will receive an inflation update equal to the hospital market basket less two percentage points The proposed rule projects a market basket update of 2.4 percent, and, therefore, hospitals that do not successfully report the quality measures would receive updates currently projected to be 0.4 percent. (22,23)
A group of health professionals in the United States and United Kingdom commissioned with a similar task of developing an assessment tool would try to work out a rating scale that could be tested for its psychometric properties and could be used in an operationalized way. Such a scale would yield scores, like BASIS-32 does. Mental health professionals in quite a few hospitals have started to use the manual in line with the more or less established quality management procedures in each hospital. Although some positive experiences have been reported, a systemic evaluation has not yet been entirely done. (27)
The proposed rule does not substantively change the list of hospital-acquired conditions (HACs) in FY 2011, but describes the results of CMS’s evaluation of the impact of the existing policy on hospital practices and patient care. This Fact Sheet discusses only the quality provisions of the IPPS FY 2011 proposed rule; separate fact sheets also issued today provide more detail on the payment and policy changes. The proposed rule does not substantively change the list of hospital-acquired conditions (HACs) in FY 2011, but describes the results of CMS’s evaluation of the impact of the existing policy on hospital practices and patient care. (28) The Agency for Healthcare Research and Quality (AHRQ) in United States has a broad portfolio of mental health research. This report focuses specifically on AHRQ-funded research that has led to the development of programs, methods, and tools for evaluating and improving the quality of mental health services and improving the education of mental health professionals. AHRQ’s wide range of mental health research has producedprograms, methods, and tools that can improve the quality of mental health services. The PIC program allows people suffering from depression to collaborate in their care with their providers and has been shown to improve outcomes. Providers who treat schizophrenia patients have toolkits that use evidence-based treatment recommendations to assess the care and treatment they provide. AHRQ research supported the development of a simple tool to screen adolescents at risk for suicide. Research is also directed toward finding ways to evaluate and promote quality improvement programs for mental health services in school-based programs and MBHO’s. In addition, AHRQ’s research helps identify solutions that can improve education and training for mental health care professionals. (30)
The New Hampshire Department of Health and Human Services used the Schizophrenia PORT recommendations for key policy initiatives. The New Hampshire Division of Public Health used the PORT findings to highlight racial disparities in the provision of care, directly influencing New Hampshire’s Healthy People 2010 plan, which is aimed ateliminating health care disparities. Partnering with the Dartmouth College Psychiatric Research Center, the Division of Mental Health restructured care protocol for patients with schizophrenia based on the PORT findings. The restructuring effort included the development of evidence-based toolkits for retraining community mental health staff. (32)
AHRQ-supported studies helped to develop a systematic approach to evaluating expanded school mental health (ESMH) programs in middle and high school and discovered that the costs of ESMH programs were low compared to the costs of programs in the community or

private sectors.24 A cost-of-care evaluation conducted for one school mental health program found that clinician services cost less than $50 per hour–much less than private services, which were estimated to cost $100 to $120 per hour. A typical program provides assessment; individual, group, and family counseling; crisis intervention; prevention and case management activities; teacher consultation; and collaboration with school staff and the community. (30)
The RSQ was the result of a clinical practice guideline (CPG) program conducted at Children’s Hospital Boston.40 The program provided training to emergency room nurses on psychiatric issues such as how to perform patient searches, de-escalating techniques, and risk factors for suicide.40 At the beginning of the training, emergency room nurses at Children’s Hospital stated that they were uncomfortable dealing with children who had psychiatric problems or asking parents or children about thoughts of suicide.40 In addition, 94.4 percent of nurses stated that suicidal patients were the most difficult patients to treat40. Two years into the CPG program, nurses reported a significant increase in their confidence and less stress when dealing with psychiatric patients.They also stated that they preferred using the screening tool to the previous method of simply judging when to ask about suicidal behavior.39,40 Parents also expressed relief that emergency room clinicians were asking about suicide. (31, 33, 37)
According to researchers funded by AHRQ, an ESMH evaluation plan should systematically measure the outcomes of the program’s goals, such as identifying emotional, behavioral, and academic problems early and improving school attendance. An AHRQ-funded study that used the Consumer Assessment of Behavioral Health Services (CABHS) prompted quality improvement efforts in several managed behavioral health care organizations. (34)
CABHS is based on CAHPS®a and was developed to collect ratings from consumers about services received from MBHOs.The survey assessed patient satisfaction in five commercial and five public assistance plans.5 Based on the results of these surveys, three MBHOs implemented quality improvement efforts. Based on the CABHS data collected in this AHRQ-funded study, along with data from a previous study using the Mental Health Statistics Improvement Program (MHSIP), researchers developed the Experience of Care and Health Outcomes (ECHO™). (35) The ECHO™ 3.0 has two surveys–one for MBHOs and one for health plans. Both surveys ask the same questions, but the health plan survey includes questions about administrative services, such as filling out paperwork and finding information in written materials.42AHRQ cosponsored the National Conference on Behavioral Health Workforce Education in Annapolis, Maryland, September 10-11, 2001. The proceedings from this conference resulted in a special double-issue volume of Administration and Policy in Mental Health in May 2002. The proceedings present problems and solutions toeducating behavioral health professionals. (36)
Methodology 3. Methodology 3.1 Study design Descriptive type of cross sectional study.3.2 Study placeNational Institute Of Mental Health, Sher-E- Bangle Nagar, Dhaka.3.3 Study duration January to June 2011.

3.4 Study populationAll the Indoor Department health care providers – doctors, nurses, supporting stuffs of all ages including male and female at indoor department of National Institute Of Mental Health.3.5 Sample sizeThe sample size could be measure as follows- Z2pq n = ------------ d2
The sample size according to this equation is 384. But due to short period sample size will be fixed by convenient sampling technique into 60.3.6 Research instrument Questionnaire to health care providers Observational Check list
3.7 Data collection techniqueA questionnaire and a check list were designed to obtain required information. Questionnaires were used to obtained data from the respondent by face to face interview. The facilities related to psychiatric management at the inpatient ward were observed and recorded with the help of the check list.
3.8 Data collection procedureThe researcher herself attended the NIMH inpatient department for collecting data. One Questionnaire was used for each health care provider for data collection. The check list was filled by the researcher after observing the facilities directly.3.10 Sample techniqueNo statistical sampling was done among the health care provides of inpatient department of NIMH as the researcher wanted to cover all the professionals working in inpatient department of NIMH. So, convenient sampling technique was applied for this study.3.11 Data processing and analysisBoth the check list and questionnaire were pre tested and finalized. During data analysis study objectives were kept in consideration. Frequency table were made for each variable and cross tabulation were also made for some related variables. Chi square test was done for comparison. Data will be processed and analyzed by using SPSS (Statistical package for social science) software.Results
4. RESULTSEvaluation by the check listHospital records:Number of patients admitted per month: 200 – 250/monthNumber of patients discharge per month: 200 – 230/monthBed occupancy rate: 95% - 97%Male : Female bed occupancy rate – 140:60Average hospital stay of a patient – 30 days
Diagnostic facilities:Admission procedure
Completed within 30 minutes of arrival of patient. Filling of forms, examination and treatment sheet – properly done. Separate recording and reporting forms and register – maintained. Confidentiality and preservation of records – maintained.
Diagnosis: Proper physical and mental examination – present and applied. Common laboratory investigation facilities like blood, urine and imaging, ECG etc –
present and used. Necessary psychiatric investigation facilities like EEG, CT scan, MRI etc – present
and used.Discharge procedure
Patient discharged with proper diagnosis So, available diagnostic facilities present in NIMH is satisfactory and the use of these facilities are near to standard.Treatment facilities:
Normal physical treatment facilities – present and used. Specific psychiatric treatment facilities like psychiatric drug therapy, cognitive
therapy, electroconvulsive therapy, psychotherapy, counseling, occupational therapy and rehabilitative therapy etc – present and used where needed.
Treatment care planning and teamwork for treatment, accessibility care – present but not sufficient.
Available essential drugs but supply is not adequate. Support for living, accommodation, self care, education and rehabilitation – present
but support for work and occupation are not adequate and support for social contacts is absent.
There is no provision for recreation or leisure time and advocacy for patients. Other common facilities like hygiene, emergency light, ideal waste disposal, infection
and injury prevention - on practice but 24 hours emergency ambulance service is not available on regular basis.
We can see that, more emphasis on medicine supply is needed. There is also no 24 hour emergency service which should be ensuring for better management of patients. Other treatment facilities are near to standard.
Manpower facilities:
No .of medical officers attending per shift – 10/12 at morning shift, but 1 at evening and night shift.
No. of Nurses attending per shift – 12/15 at morning shift but 5 at evening and night shift.
No. of security guards working per shift - 8 at morning shift but 5 at evening and night shift.
No. of cleaners working per shift – 4/5 at morning shift but 3 at evening and night shift.
No. of ward boy attending per shift – 8 at morning shift but 5 at evening and night shift.
So, overall the manpower is not enough for 200 patients who are admitted in this hospital.

Co operation between management and clinical stuffs- present. Communication and information system – poorly established. Public relation present but not satisfactory. Visitor restriction is also not a satisfactory level due to lack of manpower. Supervision by the hospital administration is done only once in a week which should
be increased.The most important drawback in NIMH is it’s limited manpower. Though the institute is 200 bedded but the manpower present here can serve 100 patients properly. So, every staff has to do double work which obviously hamper the quality of services.
Figure 1 Distribution of respondents by age
The Bar diagram shows the frequency of the age group of the respondents. Among the 70 respondents 15 are in the age group of 20- 30, 48 are in the age group of 31- 40 and the rest 7 are in the age group of 41- 50
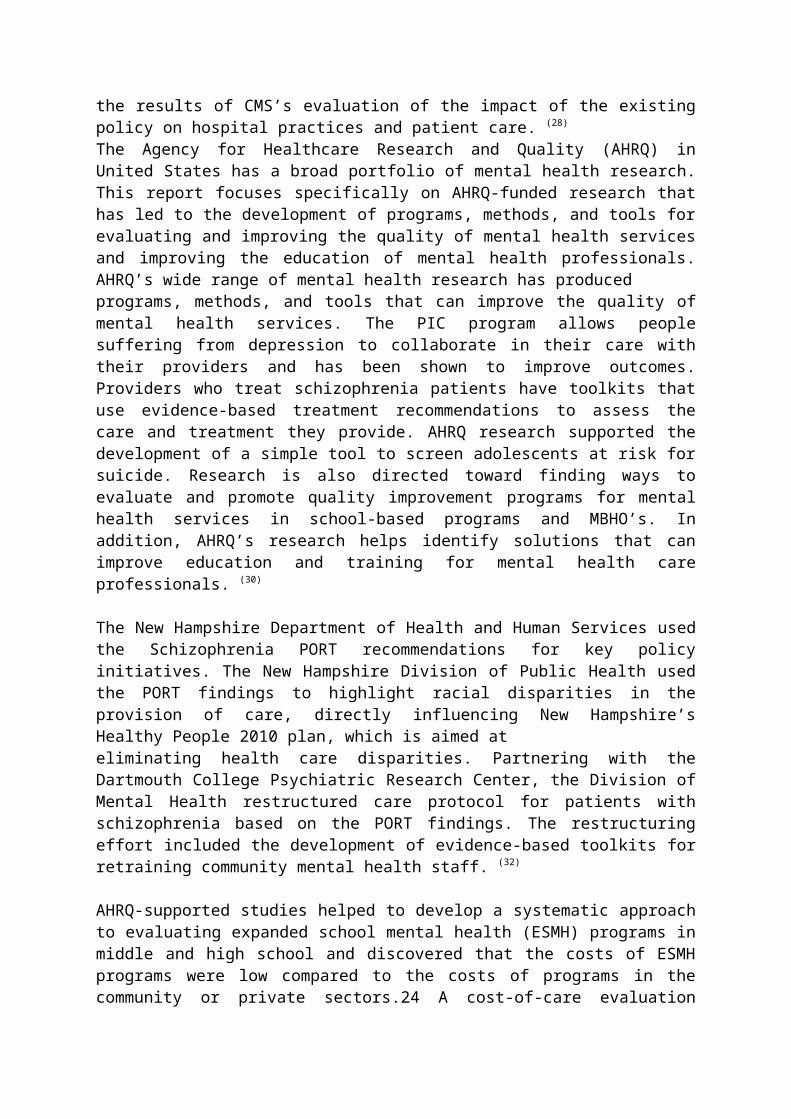
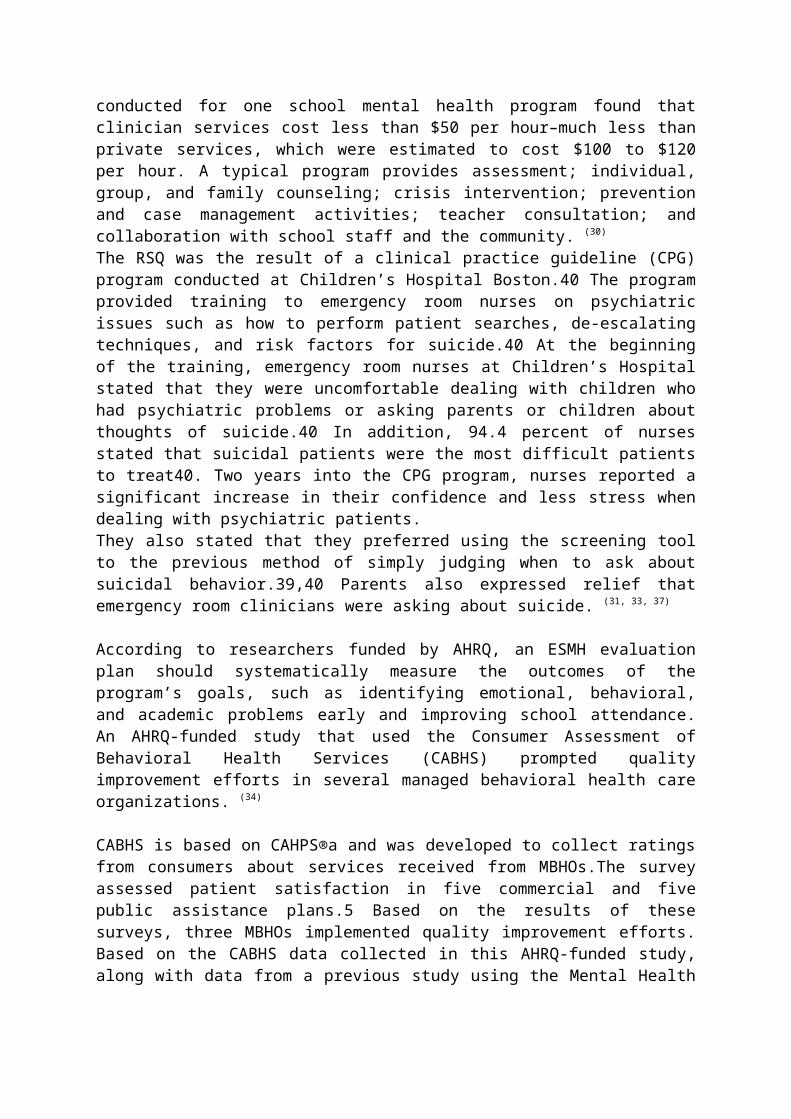
Figure 3 Distribution of respondents by experience

The above bar chart shows the total experience of the respondents. Here 17 respondents have 0-5 years work experience, 27 respondents have 5-10 years work experience and 26 respondents have more than 10 years work experience.
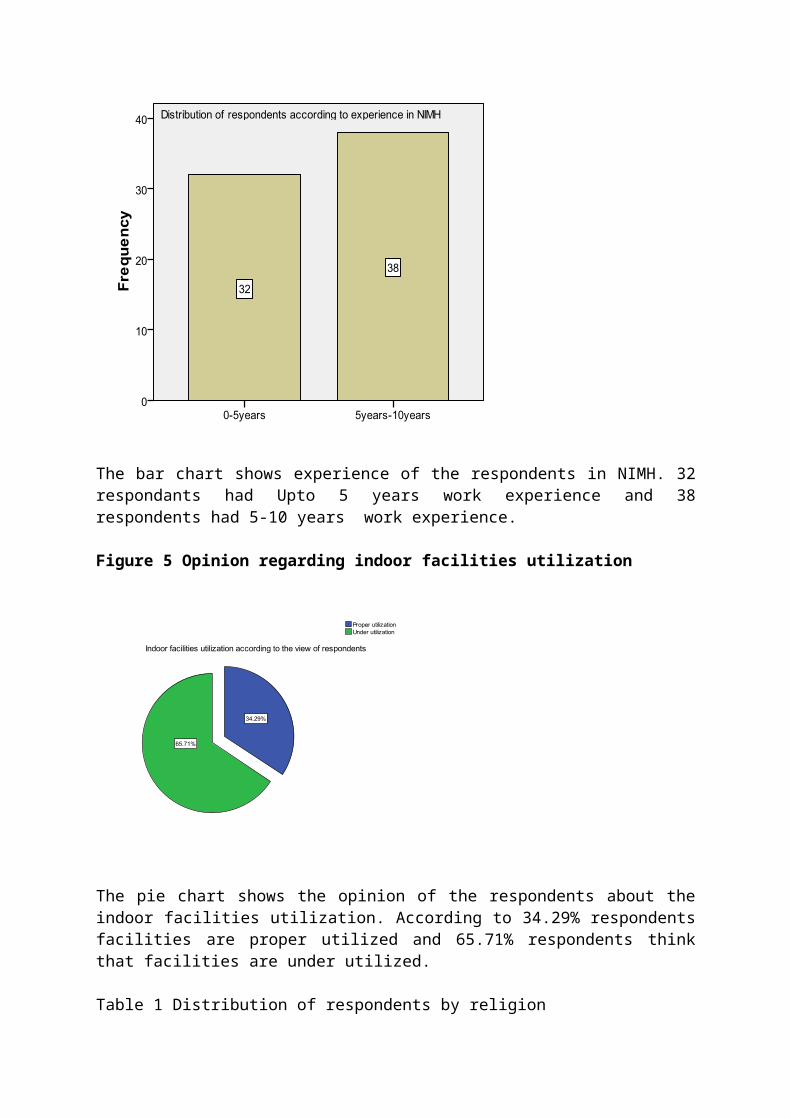
Figure 4 Distribution of respondents by experience in NIMH
The bar chart shows experience of the respondents in NIMH. 32 respondants had Upto 5 years work experience and 38 respondents had 5-10 years work experience.
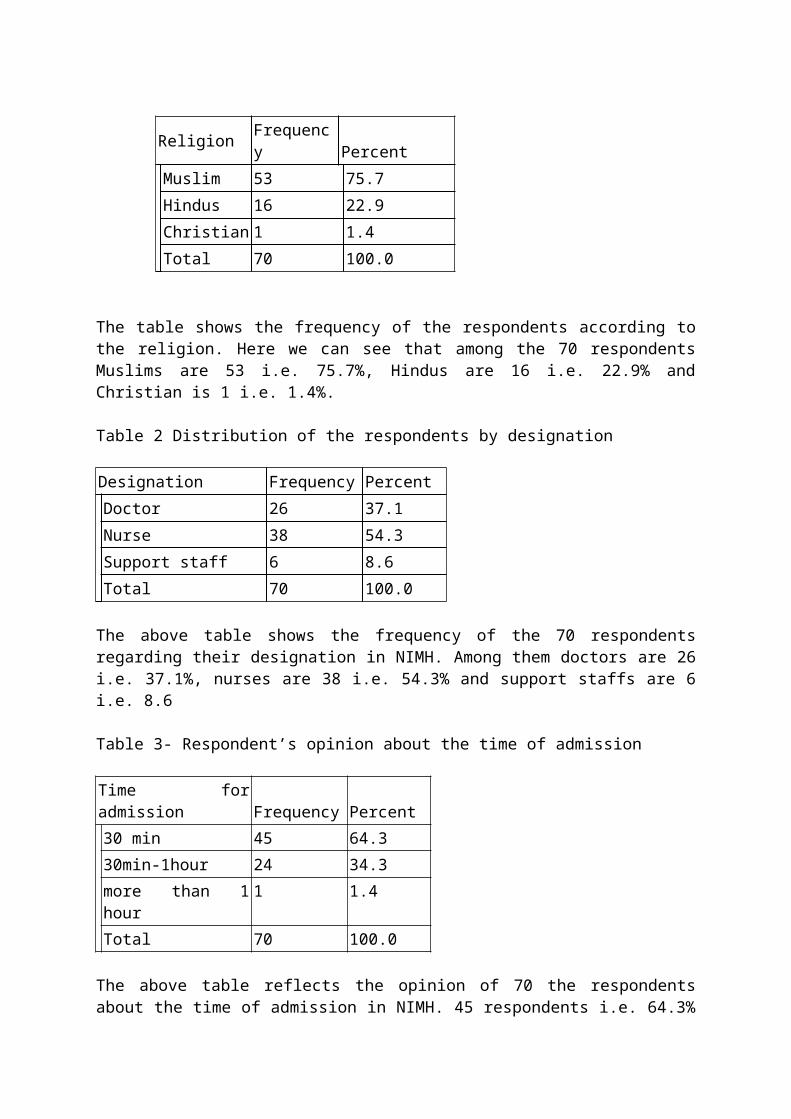
Figure 5 Opinion regarding indoor facilities utilization
The pie chart shows the opinion of the respondents about the indoor facilities utilization. According to 34.29% respondents facilities are proper utilized and 65.71% respondents think that facilities are under utilized.
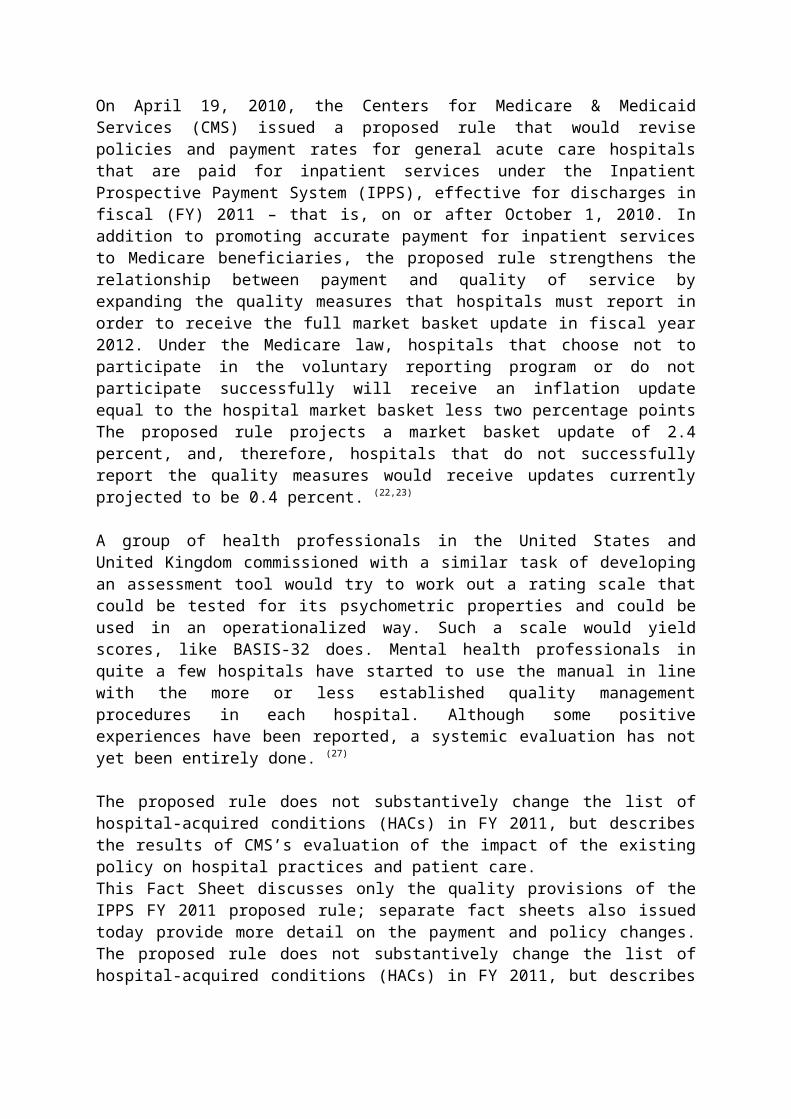
Table 1 Distribution of respondents by religion
Religion Frequency PercentMuslim 53 75.7Hindus 16 22.9Christian 1 1.4Total 70 100.0
The table shows the frequency of the respondents according to the religion. Here we can see that among the 70 respondents Muslims are 53 i.e. 75.7%, Hindus are 16 i.e. 22.9% and Christian is 1 i.e. 1.4%.
Table 2 Distribution of the respondents by designation
Designation Frequency PercentDoctor 26 37.1Nurse 38 54.3Support staff 6 8.6Total 70 100.0
The above table shows the frequency of the 70 respondents regarding their designation in NIMH. Among them doctors are 26 i.e. 37.1%, nurses are 38 i.e. 54.3% and support staffs are 6 i.e. 8.6
Table 3- Respondent’s opinion about the time of admission
Time for admission Frequency Percent30 min 45 64.330min-1hour 24 34.3more than 1 hour 1 1.4Total 70 100.0
The above table reflects the opinion of 70 the respondents about the time of admission in NIMH. 45 respondents i.e. 64.3% think that admission time is within 30 minute, 24 respondents i.e. 34.3% say that the time is between 30 min. to 1 hour and the remain 1 respondent i.e. 1.4% thinks the admission time require is more than 1 hour.Table 4- Respondent’s opinion about easiness of admission
Answer Frequency PercentYes 35 50.0No 35 50.0Total 70 100.0
The table shows the opinion of the 70 respondents about the easiness of the admission procedure in NIMH. 35 respondents i.e. 50% think that the admission procedure is easy enough but the remain 50% i.e. 35 respondents think that it is not easy enough for the public.Table 5 - Response about the planned admission list
Planned admission list Frequency PercentPresent 15 21.4
Absent 55 78.6Total 70 100.0
The above table showing the response of the 70 respondents about the presence of planned admission list. Among them 15 respondents (21.4%) think that planned admission list present in NIMH but 55 respondents (78.6%) know that there is no planned admission list in NIMH.Table 6- Respondent’s opinion about the admission process
Organization of admission process Frequency PercentFairly organized 60 85.7Very organized 10 14.3Total 70 100.0
The above table describes the opinion of the 70 respondents about the admission process. 60 respondents (85.7%) marked the admission process as fairly organized and 10 respondents (14.3%) marked it as very organized.
Table 7 Respondent’s opinion about changing admission date by the hospital
Change admission date by hospital Frequency PercentYES 30 42.9No 40 57.1Total 70 100.0
The table shows the opinion of the 70 respondents about the change of admission date by the hospital administration. Here 30 respondents (42.9%) think it is changed by the hospital but 40 respondents (57.1%) think that it is not changed by the hospital.
Table 8 Respondent’s opinion about satisfactory follow up care
Satisfactory follow up care Frequency PercentYes 69 98.6No 1 1.4Total 70 100.0
The above table shows the opinion of the 70 respondents about the follow up care. 69 respondents (98.6%) told that the follow up care is satisfactory in NIMH and 1 respondent (1.4%) told it is not satisfactory. Table 9 Respondent’s opinion about possible better care
Possible better care Frequency PercentYes 69 98.6No 1 1.4Total 70 100.0
The above table describes the opinion of the 70 respondents about the possibility of better care or services in NIMH. Here 69 respondents (98.6%) think that the services can be better than present but only 1 respondent (1.4%) thinks it is not possible
Figure 6 Opinion about appropriate diagnostic facilities
The pie chart shows response of the 70 respondents about the diagnostic facilities in NIMH whether it is appropriate or not. 60% respondents think the diagnostic facilities are appropriate for the diagnosis of the patient but 40% think that it is not appropriate.

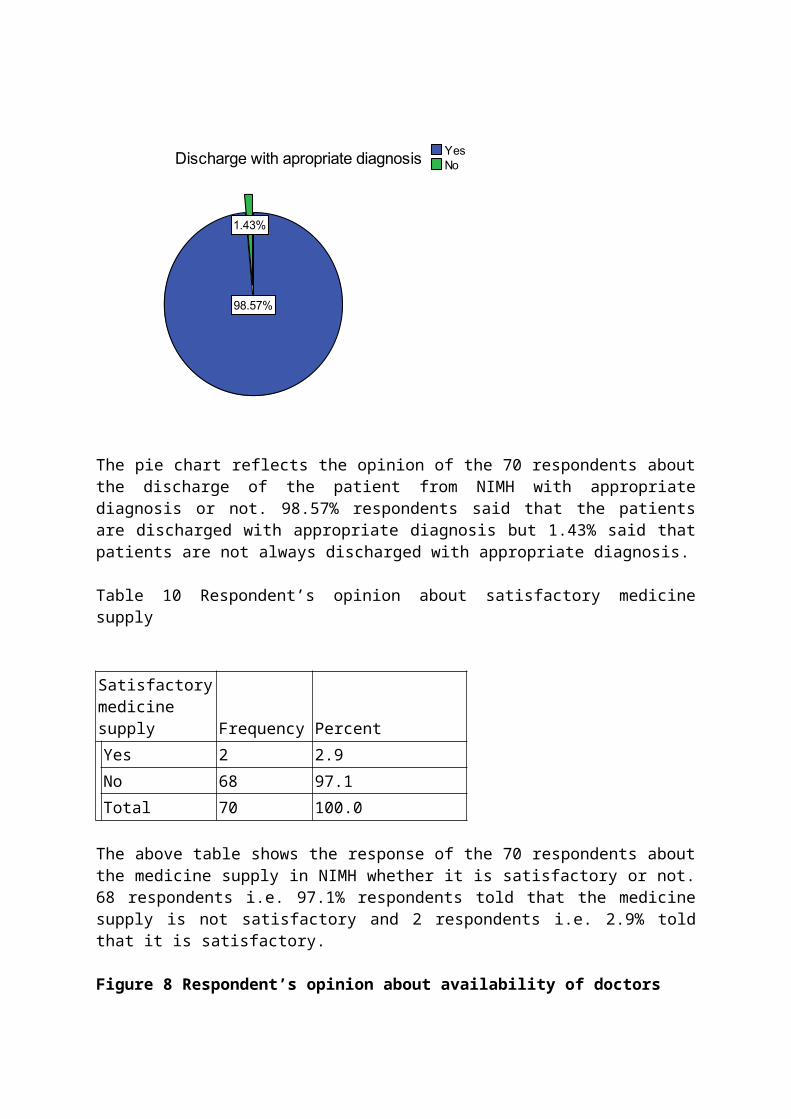
Figure 7 Opinion regarding discharge patient with diagnosis
The pie chart reflects the opinion of the 70 respondents about the discharge of the patient from NIMH with appropriate diagnosis or not. 98.57% respondents said that the patients are discharged with appropriate diagnosis but 1.43% said that patients are not always discharged with appropriate diagnosis.
Table 10 Respondent’s opinion about satisfactory medicine supply
Satisfactory medicine supply Frequency PercentYes 2 2.9No 68 97.1Total 70 100.0
The above table shows the response of the 70 respondents about the medicine supply in NIMH whether it is satisfactory or not. 68 respondents i.e. 97.1% respondents told that the medicine supply is not satisfactory and 2 respondents i.e. 2.9% told that it is satisfactory.
Figure 8 Respondent’s opinion about availability of doctors

The pie chart shows the opinion of the respondents about the availability of the doctors at inpatient department of NIMH. 95.71% said that doctors are always available at inpatient department and 4.29% said that doctors are not always available.
Table 11 Respondent’s opinion about the overall Charge On one doctor
Overall charge on one doctor Frequency PercentYes 2 2.9No 68 97.1Total 70 100.0
The above table shows the opinion about the overall treatment charge on one doctor or not. Among 70 respondents 68 persons i.e. 97.1% said that the treatment charge of the patients are not on one doctor but 2 persons i.e. 2.9% think that one specific doctor is on charge of the patients.
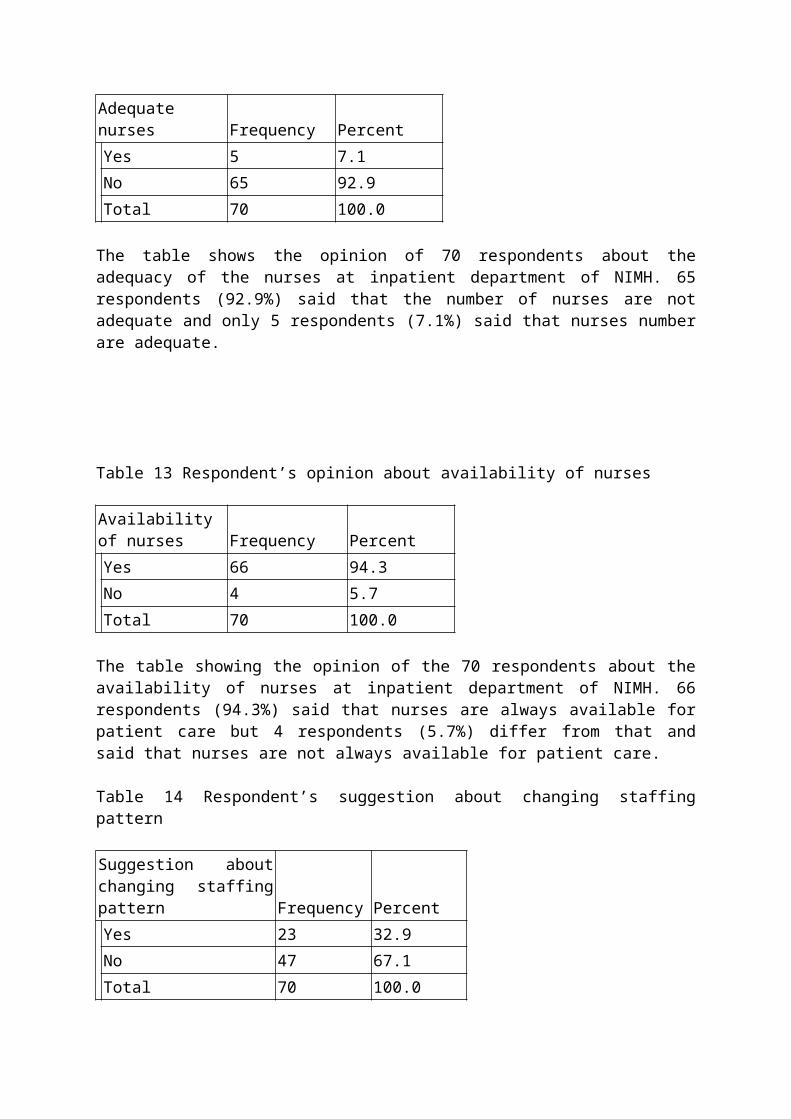
Table 12 Respondent’s opinion about adequacy of nurses
Adequate nurses Frequency PercentYes 5 7.1No 65 92.9Total 70 100.0
The table shows the opinion of 70 respondents about the adequacy of the nurses at inpatient department of NIMH. 65 respondents (92.9%) said that the number of nurses are not adequate and only 5 respondents (7.1%) said that nurses number are adequate.

Table 13 Respondent’s opinion about availability of nurses
Availability of nurses Frequency PercentYes 66 94.3No 4 5.7Total 70 100.0
The table showing the opinion of the 70 respondents about the availability of nurses at inpatient department of NIMH. 66 respondents (94.3%) said that nurses are always available for patient care but 4 respondents (5.7%) differ from that and said that nurses are not always available for patient care.
Table 14 Respondent’s suggestion about changing staffing pattern
Suggestion about changing staffing pattern Frequency PercentYes 23 32.9No 47 67.1Total 70 100.0
The above table shows the suggestion of the respondents regarding the change of present staffing pattern. Among 70 respondents 23 respondents (32.9%) wants to change the present staffing pattern of NIMH but 47 respondents (67.1%) don’t want to change the present staffing pattern.
Figure 9 Respondent’s opinion about presence of adequate support staff
Adequate support staff

The pie chart showing the opinion of the 70 respondents about the adequacy of support staff at inpatient department of NIMH. 98.57% said that the number of support staffs are not adequate and only 1.43% said the number are adequate.
Figure 10 Respondent’s opinion about staffing pattern
The pie chart represent the opinion of the 70 respondents about the category of staffing pattern. 71.43% marked the staffing pattern at inpatient department of NIMH as average, 27.14% marked it as good and only 1.43% marked it as not good.
Figure 11 Respondent’s opinion about job satisfaction of staffs
The pie chart shows the job satisfaction of the respondents who are working at inpatient department of NIMH. 60% respondents are satisfied with their present job and 10% are not satisfied with their present job.
Table 15 Respondent’s opinion about Condition of visitor restriction
Visitor restriction Frequency PercentYes 54 77.1No 16 22.9Total 70 100.0
The above table shows the opinion of the 70 respondents about the visitor restriction at inpatient department of NIMH. 54 respondents (77.1%) said that visitors are restricted except visiting period and 16 respondents (22.9%) said that visitors are not always restricted.
Table 16 Respondent’s opinion about Availability of the records
Availability of records Frequency PercentYes 61 87.1
No 9 12.9Total 70 100.0
The above table showing the opinion of the 70 respondents about the availability of the records in NIMH. 61 respondents (87.1%) said that records are available when asked for and 9 respondents (12.9%) said that records are not always available when asked for.
Table 17 Respondent’s opinion about Presence of adequate psychiatric exam
Adequate psychiatric exam Frequency PercentPresent 62 88.6Absent 8 11.4Total 70 100.0
The table represents the opinion of the respondents about the presence and practice of adequate psychiatric examination in NIMH. Among 70 respondents 62 (88.6%) said that adequate psychiatric examination facilities present and practiced in NIMH but 8 respondents (11.4%) said that examination facilities are not perfectly adequate or not perfectly always practiced.
Table 18 Respondent’s opinion about Available treatment care plan
Treatment care plan Frequency PercentYes 60 85.7No 10 14.3Total 70 100.0
The above table shows the opinion of the respondents about the availability of treatment care plan for every patient in NIMH. 60 respondents (85.7%) said that there is treatment care plan for every patient and it is followed throughout their treatment but 10 respondents ( 14.3%) said that treatment care plan is not always available for every patient.
Table 19 Presence of recreation facilities
Recreation facilities Frequency PercentAbsent 70 100.0
The table represents the opinion of the 70 respondents about the presence of recreation facilities for the patient at inpatient department of NIMH. All the respondents i.e. 100% said that there is no recreation facilities for the patient in NIMH.Table 20 Respondent’s opinion about Supervision of inpatient service
Supervision Frequency PercentYes 70 100.0
The table showing the opinion of the 70 respondents about the of supervision of the inpatient services by the administration is regular or not. All the respondents i.e. 100% assured that the administrator regularly supervised the services of the inpatient department of the NIMH. Table 21 Respondent’s opinion about Sufficiency of doctors
Sufficient no. of doctors Frequency PercentNo 70 100.0
The above table is showing the opinion of the respondents whether the number of doctors are sufficient or not for the patient at inpatient department of NIMH. All the respondents are anonymously said that the present number of doctors are not sufficient for the patients and the number should be increased.
Figure 12 Respondent’s opinion about presence of support service
The pie chart is showing the opinion of the respondents about the availability of all the support services for the patient in NIMH. 68.57% said that all the support services are present here but 31.43% said that all the support services needed for the patients are not available here.
Table 22 Respondent’s opinion about the helpful support staff
Helpful support staffFrequency Percent
Yes 38 54.3No 32 45.7Total 70 100.0

The table shows the opinion of the 70 respondents about the nature of support staffs, whether they are helpful enough or not. 38 respondents (54.3%) said that the support staffs are not helpful enough to the patient and their behavior should be changed and improved. 32 respondents (45.7%) think that the support staffs are helpful enough to the patients.
Figure 13 Respondent’s opinion about quality of inpatient service
Bar diagram represents the opinion about quality of the inpatient services in NIMH. 47 respondents said that the quality is satisfactory, 15 respondents said that the quality is good and 8 respondents said the quality of services is not satisfactory. Chi-Square Test 1 shows significance of appropriate diagnostic facilities
Apropriate_diagnostic_facilitiesObserved N Expected N Residual
Yes 42 70.0 -28.0No 28 .0 28.0Total 70
Test StatisticsApropriate_diagnostic_facilities
Chi-Square 111966.403a
df 1Asymp. Sig. .000a. 1 cells (50.0%) have expected frequencies less than 5. The minimum expected cell frequency is .0.
According to the test results, null hypothesis is rejected. So appropriate diagnostic facilities are pre-requisite for proper diagnosis and standard patient care service and in NIMH the facilities are present and used.
Chi-Square Test 2 Significance of job satisfaction of staffs
Job_satisfactionObserved N Expected N Residual
Yes 60 70.0 -10.0No 10 .0 10.0Total 70
Test StatisticsJob_satisfaction
Chi-Square 99982.858a
df 1Asymp. Sig. .000a. 1 cells (50.0%) have expected frequencies less than 5. The minimum expected cell frequency is .0.
According to the test results, null hypothesis is rejected and alternative hypothesis selected. Job satisfaction of the staffs is an important factor for proper and standard patient care service. In NIMH the job satisfaction of the staffs working in the inpatient department is satisfactory.
Chi-Square 3 Test shows the significance of number of nurses and their availability
Adequate_nursesObserved N Expected N Residual
Yes 5 70.0 -65.0No 65 .0 65.0Total 70
Availibility_of_nursesObserved N Expected N Residual
Yes 66 70.0 -4.0No 4 .0 4.0Total 70

Test StatisticsAdequate_nurses
Availibility_of_nurses
Chi-Square 4.225E6 15992.458a
df 1 1Asymp. Sig. .000 .000a. 1 cells (50.0%) have expected frequencies less than 5. The minimum expected cell frequency is .0.
According to the test results, null hypothesis is rejected which indicates that adequate number of nurses and their availability are needed or proper inpatient care.
Chi-Square Test 4 Significance of follow up care, medicine supply with inpatient service and treatment.
Satisfactory_fu_careObserved N Expected N Residual
Yes 52 70.0 -18.0No 18 .0 18.0Total 70
Satisfactory_medicine_supplyObserved N Expected N Residual
Yes 2 70.0 -68.0No 68 .0 68.0Total 70
Test StatisticsSatisfactory_fu_care
Satisfactory_medicine_supply
Chi-Square 323973.258a 4.624E6df 1 1Asymp. Sig. .000 .000a. 1 cells (50.0%) have expected frequencies less than 5. The minimum expected cell frequency is .0.
According to the test results, null hypothesis is rejected which proves that satisfactory follow up care, satisfactory medicine supply are needed for proper treatment of the patient and better inpatient service.
Chi square test 5 Significance of adequate support staff with inpatient service.
Adequate_supportstuffsObserved N Expected N Residual
Yes 1 70.0 -69.0No 69 .0 69.0Total 70
Test statisticsAdequate_supportstuffs
Chi-Square 4.761E6df 1Asymp. Sig. .000
a. 1 cells (50.0%) have expected frequencies less than 5. The minimum expected cell frequency is .0.
According to the test results, null hypothesis is rejected and shows significance of adequate number of support staffs with the better inpatient service.
Discussion
DISCUSSION
Like other countries of the world there are many psychiatric patients in Bangladesh and the number is increasing with days. But there is very little opportunity and facilities for their treatment in Bangladesh and the present facilities are also not adequate for the large number of patients and increasing demands. The National Institute of Mental Health is the only complete institute for the treatment and rehabilitation of psychiatric patients which has all the treatment, diagnostic facilities for patients and training and educational facilities for the medical personnel. But after establishment there was no evaluation or assessment study of the services provided by the NIMH. So, we have decided to go through the inpatient services of this institute. For this reason W.H.O. quality assurance program was taken as a standard and then pre tested questionnaire and check list were made and used. Total 70 health care personnel were interviewed and inpatient services were checked during the study period. Only inpatient diagnostic and treatment facilities with manpower for the 200 admitted patients were assessed because of time and resource limitation.
Regarding age group of the respondents in NIMH, in between 20-30 years are 15, 31- 40 years age group are 48 and 7are of 41-50 years age group and regarding percentage of the sex of the respondents we can see that males are 38.57% and females are 61.43%. Usually age and sex do not matter in this study but age reflects the experience and maturity and sex reflects the gender equity.

Though religion have no connection with the quality assurance of the health service or inpatient service but due to social context of Bangladesh the religion was taken as a variable. Here we can see that among the 70 respondents Muslims are 53 i.e. 75.7%, Hindus are 16 i.e. 22.9% and Christian is 1 i.e. 1.4%.
Experience is very important for the quality management of the patient. In the study result we can see that 17 respondents have work experience of 0-5 years, 27 respondents have 5-10 years experience and 26 respondents have more than 10 years work experience. Study result also shows the experience of the respondents in NIMH where upto 5 years experience present in case of 32 respondents and 5-10 years experience present in case of 38 respondents. According to quality assurance the health personnel should have experience of minimum 1 year. So, the staff of the inpatient department of NIMH has sufficient experience for the diagnosis, treatment and care of the psychiatric patients.
One of the most important variable in which the quality of the inpatient service is dependent is the admission procedure. According to the standard we used in this study the admission process should be easy enough for the general population and the admission should be complete within 30 minutes of arrival of the patient. The admission process should be organized in a fairly organized manner. With the checklist the admission process was observed and also the opinion of the respondents was taken. Basically in most of the cases the admission is completed within 30 minutes of the arrival of the patient and the admission process is easy enough for the public and the overall fairly organized. The opinion of the respondents are as follows - the 35 respondents i.e. 50% think that the admission procedure is easy enough but the remain 50% i.e. 35 respondents think that it is not easy enough for the public. 60 respondents (85.7%) marked the admission process as fairly organized and 10 respondents (14.3%) marked it as very organized. The opinion of the respondents about the time of admission in NIMH shows that 45 respondents i.e. 64.3% think the admission time is completed within 30 minute, 24 respondents i.e. 34.3% say that the time is between 30 min. to 1 hour and the remain 1 respondent i.e. 1.4% thinks the admission time require is more than 1 hour.
There should be ideally present a planned admission list for the patient who are needed to get admitted in the hospital and the admission date can be changed by the patient or the hospital according to their comfort level or need basis. With the check list it is found that there is no planned admission list in NIMH which is present in Pubna mental hospital. But in NIMH a temporary admission list used for the emergency patients and they got admitted according to the list with available vacancy of the bed as first come first admission. Among the respondents 15 respondents (21.4%) think that planned admission list present in NIMH but 55 respondents (78.6%) know that there is no planned admission list in NIMH. Regarding the opinion about the changing date of admission, 30 respondents (42.9%) think that it is changed by the hospital but 40 respondents (57.1%) think that it is not changed by the hospital. These opinion reflects and signify the truth of the absence of the ideal planned admission list and its changing.
Another important factor for the better quality of the inpatient service is the discharge procedure. Ideally a patient who got admission in the inpatient department should be discharge after appropriate diagnosis and nearly after completing the treatment. Here the discharge procedure follows the rule but in case of patients interest or willingness for discharge may hamper the rule because of lack of time for appropriate diagnosis. In the opinion reflects that the 98.57% of the respondents said that the patients are discharged with
appropriate diagnosis but 1.43% said that patients are not always discharged with appropriate diagnosis.
Appropriate diagnostic facilities for the patient admitted in NIMH are satisfactory and the use of these facilities are near to standard which was checked with the checklist. The standard describes that there should present all the diagnostic facilities for the psychiatric patients like complete psychiatric examination with EEG, CT scan, MRI and the common diagnostic facilities like blood, urine, X-ray, imaging, ECG, organ related investigations etc. All these facilities available in NIMH and used as necessary. According to the opinion of 70 respondents 62 (88.6%) said that adequate psychiatric examination facilities present and practiced in NIMH but 8 respondents (11.4%) said that examination facilities are not perfectly adequate or not perfectly always practiced. 60% respondents think the diagnostic facilities are appropriate for the diagnosis of the patient but 40% think that it is not appropriate.
There should be ideally present a initial, proper treatment care plan for every patient. In the result we can see that treatment care plan is made according to the type of disease diagnosis and respective treatment. Due to lack of manpower the treatment care plan for every individual patient may not possible here in NIMH. 60 respondents (85.7%) said that there is treatment care plan for every patient and it is followed throughout their treatment but 10 respondents ( 14.3%) said that treatment care plan is not always available for every patient.
The treatment care facilities are almost ideal and according to the standard psychiatric treatment in NIMH. Normal physical treatment facilities are present here and used where needed. Specific psychiatric treatment facilities like psychiatric drug therapy, cognitive therapy, electroconvulsive therapy, psychotherapy, counseling, occupational therapy and rehabilitative therapy etc are present and used adequately according to patient diagnosis and treatment demand. Treatment care planning and teamwork for treatment, accessibility care are also present but not sufficient enough for the actual quality standard. Other treatment facilities are near to standard.
Support services are the component of adequate psychiatric management for such type of patients. Support for living, accommodation, self care, education and rehabilitation are present in NIMH but support for work and occupation are not adequate and support for social contacts is absent. The opinion of the respondents about the availability of all the support services for the patient in NIMH are as follows - 68.57% said that all the support services are present here but 31.43% said that all the support services needed for the patients are not available here.
Recreation facilities is an important factor for the perfect curative treatment of mantal patients and it should be present in a psychiatric hospital because it helps in mental stability and social awareness and bonding of the patients. But there is no provision for recreation or leisure time and advocacy for patients in NIMH. All the respondents i.e. 100% certified that there is no recreation facilities and advocacy for the patient in NIMH.
Other common facilities like maintenance of hygiene, use of emergency light, ideal waste disposal, infection and injury prevention are on regular practice.
Visitor restriction is important not only for the surgical or medicine patient but also for the psychiatric patients. In NIMH indoor department only one attendants is allowed to stay with

the patient and other visitors are restricted except visiting hour for the security of both the patient and visitor. 54 respondents (77.1%) said that visitors are restricted except visiting period and 16 respondents (22.9%) said that visitors are not always restricted because of limited security guards.
After the discharge a very important factor regarding the cure of the patient is the follow up care. If the follow up care is regular and adequate the treatment response will be long lasting and effective. 69 respondents (98.6%) told that the follow up care is satisfactory in NIMH and 1 respondent (1.4%) told it is not satisfactory.
Another important factor for the better treatment of the patient is the adequate medicine supply i.e. the supply of the essential life saving drugs with appropriate psychiatric drugs should be available for the admitted patients. In NIMH the medicine supply is impressive but regarding the huge number of patients and long stay time in the hospital make the supply inadequate. Even some rare disease also causes absence of some specific drugs which are needed for the treatment of the disease. 68 persons i.e. 97.1% respondents told that the medicine supply is not satisfactory and 2 respondents i.e. 2.9% told that it is satisfactory. So, obviously the medicine supply is not adequate according to the demand and more emphasis on medicine supply is needed.
There is absence of 24 hour emergency service which should be present for better management of the patients.
Among the respondents there are 26 i.e. 37.1% doctors, nurses are 38 i.e. 54.3% and support staffs are 6 i.e. 8.6%. On the basis of the quality assurance program set by WHO we know that there should be at least 3 nurses in ratio of 1 doctor but in NIMH the ratio is lower than the standard. 65 respondents (92.9%) said that the number of nurses are not adequate and only 5 respondents (7.1%) said that nurses number are adequate. 66 respondents (94.3%) said that nurses are always available for patient care but 4 respondents (5.7%) differ from that and said that nurses are not always available for patient care. 95.71% said that doctors are always available at inpatient department and 4.29% said that doctors are not always available. 98.57% said that the number of support staffs are not adequate and only 1.43% said the number are adequate. 38 respondents (54.3%) said that the support staffs are not helpful enough to the patient and their behavior should be changed and improved. 32 respondents (45.7%) think that the support staffs are helpful enough to the patients. All the respondents are anonymously said that the present number of doctors are not sufficient for the patients and the number should be increased. Among 70 respondents 68 persons i.e. 97.1% said that the treatment charge of the patients are not on one doctor but 2 persons i.e. 2.9% think that one specific doctor is on charge of the patients.
No .of medical officers attending per shift are 10/12 at morning shift, but 1 at evening and night shift. No. of Nurses attending per shift are 12/15 at morning shift but 5 at evening and night shift. No. of security guards working per shift are 8 at morning shift but 5 at evening and night shift. No. of cleaners working per shift are 4/5 at morning shift but 3 at evening and night shift. No. of ward boy attending per shift are 8 at morning shift but 5 at evening and night shift. Co operation between management and clinical stuffs is present.
Overall the manpower is not enough for 200 patients who are admitted in this hospital. The manpower should be increased according to the standard quality assurance plan for perfect quality care of the inpatient department of the NIMH.

Communication and information system is poorly established. Public relation present but not satisfactory.
Among 70 respondents 23 respondents (32.9%) wants to change the present staffing pattern of NIMH but 47 respondents (67.1%) don’t want to change the present staffing pattern which indicates that the present staffing pattern is good enough for the quality assurance.Job satisfaction of the staffs is very important for the quality care of treatment for the patients. If the staffs are not satisfied with their job they can not deliver perfect and standard health care to the patients. 60% respondents are satisfied with their present job and 10% are not satisfied with their present job. So, the results reflects that most of the staffs are satisfied with their job and the quality care is adequate from this perspective. The condition regarding the proper utilization of the facilities available for the management purpose of the patients are somehow under utilized. If proper concentration can be given, with these limited facilities and resources a more improved quality care can be given to the patients. According to 34.29% of the respondents facilities are proper utilized in NIMH and 65.71% respondents think that facilities are under utilized. Supervision is a very important variable for the quality care improvement of health service and it’s evaluation. If the services are regularly supervised the drawbacks can be find out and the problems might be sort out. In NIMH the administrator weekly supervised the service which is certified by the opinion of the respondents. All the respondents i.e. 100% assured that the administrator regularly supervised the services of the inpatient department of the NIMH. But the frequency of the supervision should be more i.e. at least twice a week will be more effective for the better quality of the services than present condition.
The records should be always available when these are asked for. In NIMH the records are available but little time consuming which should be more prompt. Due to absence of perfect digitalization more time is needed for the preservation of the records and search of them. 61 respondents (87.1%) said that records are available when asked for and 9 respondents (12.9%) said that records are not always available when asked for. Filling of forms, examination and treatment sheet are properly done here. Separate recording and reporting forms and register are maintained. Confidentiality and preservation of records are maintained properly. From the record we can learn about the vital statistics such as the number of patients admitted per month in NIMH are 200 – 250, the number of patients discharge per month are 200 – 230, bed occupancy rate is 95% - 97%, Male : Female bed occupancy rate is 140:60, average hospital stay of a patient are30 days and more.
69 respondents (98.6%) think that the services can be better than present but only 1 respondent (1.4%) thinks it is not possible that indicates that there is every scope for the improvement of the quality of the present services which are provided to the indoor patients. The opinion about quality of the inpatient services in NIMH shows the true picture of the situation. Here 47 respondents said that the quality is satisfactory, 15 respondents said that the quality is good and 8 respondents said the quality of services is not satisfactory.
Conclusion andRecommendation
6.1 Conclusion
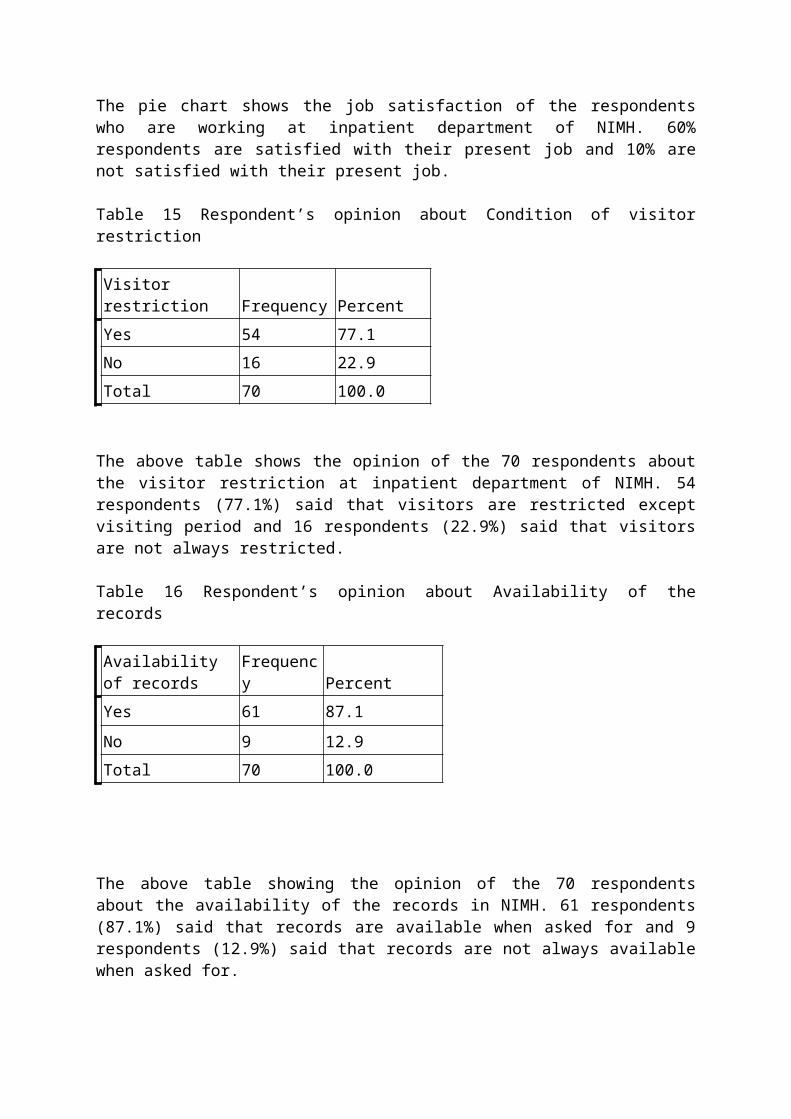
Overall in the study the small portion of the total inpatient service of NIMH was assessed and the evaluation reflects that the quality of care can be improved more. There are some fields where concentration should be given immediately and some fields where a little change can make them excellent. But as a whole the National Institute of Mental health is serving as a quality care psychiatric institute but due to lack of manpower and adequate resources it’s function can not reach the international standard. On the other hand, new dimensions of the psychiatry and psychiatric diseases need more evaluation, assessment, study and research as well as proper and adequate training of all the stuffs regarding patients care, behaviors, professionalism, self assessment and motivation. Also effort should be taken to improve the community care and awareness regarding this issue and special consideration should be taken to work with the family and volunteers.
There should be regular supervision and reassessment by the appropriate authority for meeting the needs, proper diagnosis, treatment care, rehabilitation both medical and psychological, satisfactory follow up care, occupational therapy and training of the patients. Lack of these arrangements may hamper the total treatment and rehabilitation care of the psychiatric patients whether major or minor. Along with these proper and adequate manpower, suitable and necessary resource allocation like medicine, leisure facilities, advocacy for patients’ interest should be added for better quality.Further Review needed by the government to improve the total psychiatric care.
Psychiatric Services seeks expert reviewers in the following areas:♦ Cost and effectiveness of depot medications♦ Length of hospital stay♦ Mental retardation and mental illness♦ Outcome and clinical measurement scales
6.2 RecommendationThough there are some ethical problems in the provision of standard psychiatric services regarding resource allocation, care in the community, confidentiality, Autonomy, conflicts of interest, coordination of services but if the government wants and proper community awareness and participation present then a perfect psychiatric service can be establish in our country.
There are some basic requirements of the services to provide long term care – Suitable and well-supported carers. Appropriate accommodation Suitable occupation arrangement. Arrangements to ensure the patient’s collaboration with treatment. Regular reassessment, including assessment of the physical health. Effective collaboration amongst carers. Continuity of care and rapid response to crisis.
Though the authority have the interest and willingness to improve the quality of the services of the institute but due to some drawbacks they did not get complete success yet. We can wish and hope that these problems can be solved by adequate assessment and further reassessment of the institute regularly so that this institute can become a proud for us and the community can be benefited by it’s standard quality services.
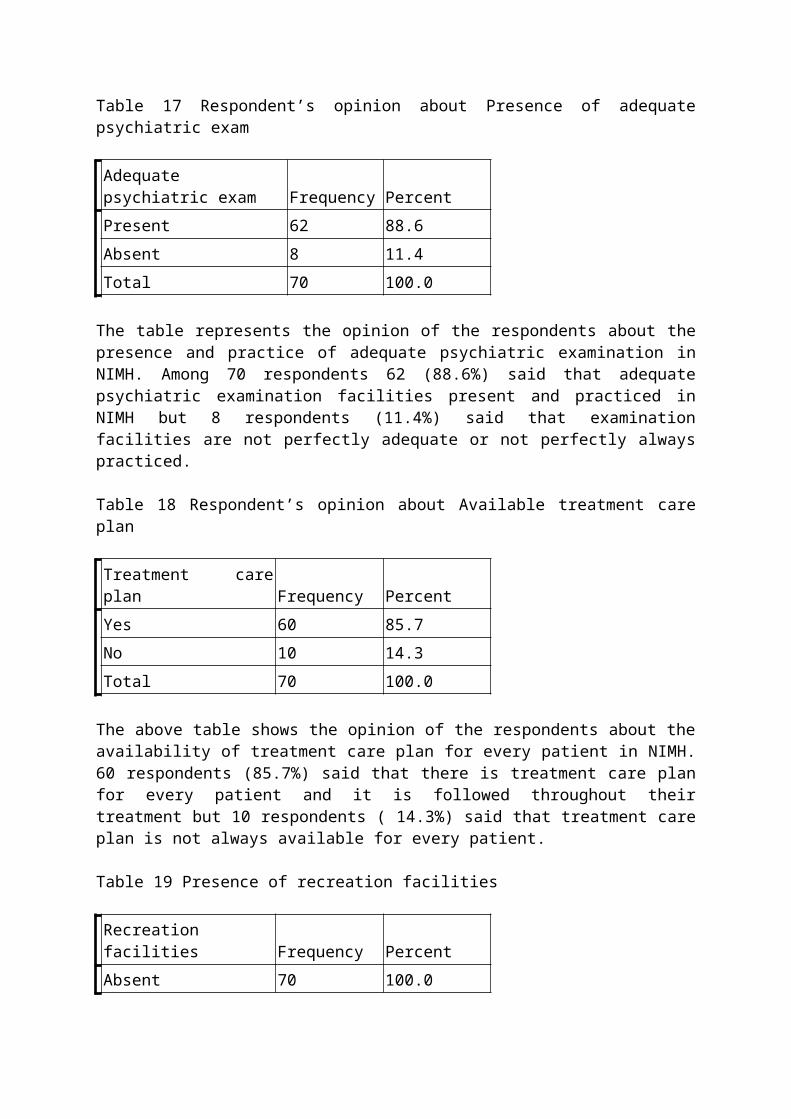
According to hospital health care providers some recommendations come forward for the quality assurance of NIMH which are as follows-
Increase the medicine and resource supply are needed. Proper training of the stuffs of all level should give an emphasis. Adequate communication system should be developed like PABX or Intercom in
every ward and doctors and nurses duty stations. Above all manpower should be increased for the better management of the patients. 24 hours emergency ambulance service should be ensure. The work load of the health personnel should be minimized. Proper training for the behavior improvement of the support staffs should be given. Supervision of the inpatient service by the administration should be increased. Resource allocation should be more regarding patient management as well as staffs
perspective.
Further most the assessment of every institute and hospital should be done completely so that the quality can be improved and a ideal quality assurance plan should be set which can help the quality improvement. Such a way the large number of patients in Bangladesh can get an access to a better quality treatment and health care facilities.
REFERANCES
1. Gelder M, Mayer R, Cowen P. Shorter Oxford Textbook of Psychiatry. 12 th edition: 767 – 792.2. Kunze H, Priebe S. Assessing the Quality of Psychiatric Hospital Care: A German Approach; Psychiatric Services 1998; 49:794–796.3.Islam H. Bangladesh Journal of Psychiatry. vol 20(1): 12-14.4. Graduate school of Health Science and Management in and Department of Quality Improvement of Severance Hospital under Yonsei University Medical Centre, South korea - Analysis of healthcare quality indicator using data mining and decision support system.5. The evaluation and medical service quality of inpatient department of public and nonprofit hospital in Choungguing, China affirmed by the Health Bureau of Nanjing.6. Niagra Health System (NHS), Canada.7. Niagra Health System Framework(NHSF), Canada.8. Validity of the Department of Defense Standard Inpatient Data Record for quality Management and health services research, Department of Medicine and Prevented medicine, Uniformed Services University of the Health Sciences, Bethesda, USA9. National Centre for Workforce Analysis, American Nurses Association, American Academy of Nurse Practitioners joint collaboration of nursing quality measures.10. Hospital Inpatient Discharge Data for Quality Improvement and Statewide Surveillance: AHRQ Inpatient Indicators by the Agency for Healthcare Research and Quality (AHRQ) of Utah Department of Health.11. Accreditation check list prepared by the DGHS, Government of People Republic of Bangladesh.12. North Carolina Healthcare Quality Alliance (NCHQA) 2009-2010.13. Hospital based inpatient psychiatric services: the percentage of patients discharged from a hospital based inpatient psychiatric setting with a continuing care plan created, National Quality Measures Clearinghou.14. Kunze H. Staffing directive for psychiatric hospitals as an instrument for quality assurance. Quality Assurance in Psychiatry.1997; 5 -255.15. Blumenthal D: Quality of care: New England Journal of Medicine.1996; 335: 891–894.

16. Lundberg GD, Wennberg JE. Quality of care: a call for papers for the annual coordinated theme issues of the AMA journals. JAMA. 1996; 102: 276-1514.17. Eisen SV. Behavior and symptom identification scale (BASIS-32), in Outcomes, assessment, and Clinical Practice. 1996; 34-245.18. AACP continuity of care guidelines: best practices for managing transitions between levels of care. American Academy of community psychiatrists (AACP);200119. American Psychiatric Association (APA). Practice guideline for psychiatric evaluation of adults.20. National Health Service Hospital and recent experiences of the patients in the inpatient and emergency department, Picker Institute Europe.21. National Institute of Mental Disorders (NIMD), National Institute of Mental Health, Bethesda 2008, Medical disorders in America.
22. World Health Organization, The World Health Report 2004.23. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE – Prevalence, severity and comorbidity survey Replication. Arch Gen Psychiatry 2005.24.Specification manual for joint commission National Quality Core Measures (Version 2010) : The Joint Commission; 2010 Jan.25. General Hospital Psychiatry, 9th edition.26. Lishman A. Lishman’s organic psychiatry.19th edition.27. United States and United Kingdom commission, Health care manual.28. The Centers for Medicare & Medicaid Services (CMS), April 19, 2010.30. Programs and Tools to Improve the Quality of Mental Health Services, Research in action, Department of health and human services, USA, issue 16.31. Nabors LA, Leff SS, Mettrick JE. Assessing the costs of school-based mental health services. J Sch Health 2001; 71(5)199-200.32. National Institute of Mental Health. The numbers count. Mental disorders in America. NIH Pub No. 01-4584. Web site: http://www.nimh.nih.gov/publicat/numbers.cfm. Accessed Apr 7, 2003.33. Eisen SV, Shaul JA, Clarridge B, et al. Development of a consumer survey for behavioral health services. Psychiatr Serv 1999; 50(6):793-8.34. Hoge MA. The training gap: an acute crisis in behavioral health education. Admission Policy Mental Health 2002; 29(4/5):305-17.35. RAND Health. Partners In Care. Hope for those who struggle with hope. Research Highlights. Web site: http://www.rand.org/publications/RB/RB4528. Accessed Oct 23, 2002.36. Stuart GW, Burland J, Ganju V, et al. 37. Public Health Service [U.S.]. The Surgeon General’s call to action to prevent suicide, 1999. Web site: http://www.surgeongeneral.gov/library/calltoaction/ default.htm. Accessed Apr 15, 2003.