Project to understand and potentially strengthen the influence in … · 2019. 11. 22. · Anthony...
19
1 Project to understand and potentially strengthen the influence in policy of applied psychologists in London Contract reference: RH/TR 2015 Date: 8 th July 2016 Report prepared by: Anne Richardson, Director Anne Richardson Consulting Ltd Oversight: Rod Holland, Chair of London Regional Psychology Advisory Committee, Zenobia Nadirshaw and Alison Beck (DCP chairs) Richard Pemberton, National DCP Date of report: 15 June 2016 A NNE R ICHARDSON C ONSULTING L TD EXPERIENCE , KNOWLEDGE AND EXPERTISE IN MANAGING RISK
Transcript of Project to understand and potentially strengthen the influence in … · 2019. 11. 22. · Anthony...

1
Project to understand and potentially strengthen the influence in policy of applied psychologists in London
Contract reference: RH/TR 2015
Date: 8th July 2016
Report prepared by: Anne Richardson, Director Anne Richardson Consulting Ltd
Oversight: Rod Holland, Chair of London Regional
Psychology Advisory Committee, Zenobia Nadirshaw and Alison Beck (DCP chairs) Richard Pemberton, National DCP
Date of report: 15 June 2016
ANNE RICHARDSON CONSULTING LTD EXPERIENCE, KNOWLEDGE AND EXPERT ISE IN MANAGING RISK

2
1. INTRODUCTION
To help to understand and potentially strengthen the influence in policy of applied psychologists in
London, the London Branch of the Division of Clinical Psychology (DCP) in consultation with the
London Regional Psychologists Advisory Committee (RPAC or LRPAC) commissioned a piece of work
during 2015 from Anne Richardson1,2. This involved a series of semi-structured interviews with
senior applied clinical and academic psychologists in London, all of whom had a strong reputation for
effectiveness in influencing policy and a record of success in service development, and two
workshops with trainees. The aim was to understand opinions and get ideas for strengthening the
resources and skills potentially available for others in London to develop their competence. This
report summarises the results of the interviews, and makes several recommendations for DCP
branch and LRPAC (now the London Strategic Network for Clinical Psychology) to consider.
2. BACKGROUND
Senior applied psychologists working as heads of department of psychology in London have been
meeting under the auspices of LRPAC since at least the late 1970s to discuss issues of common
interest for their work in health and social care. The DCP branch, along with other branches across
the country, had recently been re-structured. Planning meetings included Rod Holland (LRPAC chair),
Zenobia Nadirshaw (DCP chair) who was then replaced by Alison Beck, and Richard Pemberton chair
of the BPS UK DCP. Further information about the local and national context for the work is provided
in Section 5.
3. METHODOLOGY
A meeting in October 2015 formed the basis for taking forward work to interview a number of senior
Clinical Psychologists (`the experts’). All the names3 of those interviewed were either suggested at
the scoping meeting and/or approved by the RPAC and DCP chairs as having had a notable record of
success in influencing local or national policy. Most were, or had until relatively recently been based
in London.
A brief review of written material was undertaken, including information from the workforce review
undertaken by Alison Longwill for the BPS4 and material relating to the planning and commissioning
structures at local, regional and national level. Semi structured interviews with individuals and two
workshops with final year students (`the novices’) in London and Oxford were then undertaken to
cover the following broad categories of information:
Personal experience/examples of influencing policy (effective and ineffective).
1 Anne Richardson worked in government at the Department of Health as head of mental health policy, and in 2008 at the
Audit Commission as Head of Mental Health. Employed as a clinical psychologist in London prior to this, including as Head of Department in Newham, she also worked at UEL. In 1987 she helped to establish the new doctoral training programme at UCL, subsequently becoming joint course organiser. Since 2010 she has worked as one of a number of providers commissioned by NHS England of investigations into homicides by people with mental ill health. 2 BPS contract Reference: RH/TR 2015
3 Professor David Clark, Professor Peter Fonagy, Dr Alison Beck, Dr Rod Holland, Professor Zenobia Nadirshaw, Professor
Anthony Roth, Dr John Cape, Dr Ravi Rana, Dr Duncan Law, Dr Neil Ralph, Ms Wendy Wallace, Dr Michael Witney, Dr Lucy Marks, Professor Jamie Hacker-Hughes. 4 Available from the BPS.

3
Common themes, if any (e.g., training timing, culture, organisational structure)
Personal skills (e.g., attitudes, knowledge, behaviour, listening and communication).
The origins of competence (motivation, modelling, formal learning, incentives, rewards)
Developing competence in others (training, mentoring, leadership)
Obstacles and opportunities
Theoretical underpinnings (if any) and further reading
Issues for London
Models of good practice (if any)
Role of the BPS and DCP
Limitations of time alongside the fact that the work coincided with NHS annual planning deadlines
constrained the original plans to also interview a sample of commissioners and Chief Execs from the
NHS. The views of the psychologists are therefore presented alone.
4. CONTEXT
Home to many policy hubs and national centres of excellence and the centre of national
government, London has arguably presented applied psychologists with some very particular
challenges. For example, the capital contains the centre for government, the (now much reduced in
size) Department of Health and the London office of NHS England5 and it is also home to a number
of major national centres of excellence in health-related teaching, research and care. London also
faces particular population health-related challenges6, many of which are the focus for work by the
Mayor’s office. However, issues well beyond the boundaries of London were also discussed and four
of these provide important context for the work; each has contributed to the challenge that Clinical
Psychologists face to engage with and influence policy.
4.1 Health service reorganisation
In the past, a significant level of policy support for matters of interest to psychologists was provided
by experienced psychologists7 at the Department of Health working alongside medical, nursing and
other professional colleagues, civil servants and Ministers. Now, profession-specific representation
at the centre has gone and the Department is downsizing further as NHS England’s role grows. At
the same time, the Health and Social Care Act (2011) has secured devolution of responsibility to local
level for large proportion of health service commissioning, provision and assurance. Psychologists
can no longer rely on the relatively few professional colleagues with connections at the centre to
influence policy on their behalf. Instead, regardless of their knowledge and experience, many more
psychologists are being challenged by local decisions which affect their work and many feel that they
lack relevant knowledge, confidence and skill.
5 NHS England – the national commissioning wing of the NHS – is based in four regional offices: London, Midlands and East,
North and South (27 Area teams ceased to exist w.e.f. April 2015). NHS England liaises with Clinical Commissioning Groups, local authorities, health and wellbeing boards and GPs and provides professional leadership for finance, nursing, medical, specialised commissioning, patients and information, human resources, organisational development, assurance and delivery. The London office maintains oversight of over £15bn of services for over 8 million people. 6 London contains The London Health Commission, the London Assembly Health Committee which oversees the Mayor’s
Health Inequalities Strategy, the London Health Board, the London-wide Clinical Commissioning Council (all part of the Mayor’s Office), and many leading London-based national centres for NHS treatment and care (e.g., GOS, RNH, etc). 7 May Davidson, Ed Miller, Glenys Parry.

4
4.2 BPS and DCP reorganisation
In the wake of the establishment of the Health and Care Professions Council (HCPC), there has been
discussion about the structure and function of the British Psychological Society (BPS) and the DCP.
The HCPC is one of nine councils (perhaps to be further reduced in number8 in the future) carrying
responsibility for setting standards for qualifications, dealing with concerns about professional
behaviour such as fitness to practice or misconduct and maintenance of the register of individuals
approved to practice. For Clinical Psychologists, these were all areas formerly managed by the BPS.
Questions have therefore been asked about how the BPS might now be organised, and what its main
functions should be. There is clearly division of opinion about how Clinical Psychologists should be
represented and whether support for and development of policy in this area is working effectively. A
resolution at a Special General Meeting of the DCP9 expressed grave concern about the way the BPS
has provided professional leadership, direction and strategy in the past and discussion continues
about the best organisational arrangements going forward.
4.3 Austerity in the NHS
Austerity and other measures within the NHS have had a major effect10 upon the way in which
decisions about local health policy are now taken. Furthermore, the economics of care, rising care
costs, and rising demand for care has led to significant service cuts in many areas. An analysis of over
a thousand responses from Clinical Psychologists to a survey undertaken by Alison Longwill (2015)
for the BPS, showed widespread concern about the impact of austerity on recruitment and retention
to posts at the upper end (Band 9) of the pay scale. There have been reports of down-banding for
some senior posts and some evidence of an increase in fixed and short term employment contracts
and locum work. One or two very senior Clinical Psychologists11 have been made redundant. It is
possible that the absence of senior, more experienced Clinical Psychologists in management roles
has left more junior staff uncertain about how to influence policy or participate in management
decisions.
4.4 Agenda for Change
Agenda for Change12 provides the background to changes in the way that Clinical Psychologists are
graded and its impact has been quite significant. It is a fundamental tenet of Agenda for Change that
remuneration and grading for jobs is based not upon the qualifications of the individual employee
but rather upon the nature of the job. Not only are comparisons between professions much easier to
make, but there is more competition. For example, when Agenda for Change was initially
implemented, salaried trainee Clinical Psychologists (unlike nurse trainees in receipt of bursaries)
8 Regulation of Health Care Professionals. Regulation of Social Care Professionals in England (April 2014) Cmd 8839
presented to Parliament by the Law Commission (345), Scottish Law Commission (237) and N.I. Law Commission (18). ISBN 9781474101837. http://lawcommission.justice.gov.uk/areas/Healthcare_professions.htm 9 Motion proposed by Prof Mike Wang and Dr Bernard Kat at a SGM of the DCP May 2016, supported by the majority of
those present, that the BPS was failing to meet the professional needs of Clinical Psychologists. More information is available from [email protected] 10
Kings Fund Briefing (2015) Gilbert, H. `Mental Health Under Pressure’ http://www.kingsfund.org.uk/ 11
Doncaster. 12
Agenda for Change (2004) is a framework for remuneration based upon assessment of job responsibilities rather than individual qualifications which brought together into a single structure all salaried non-medical or dental NHS staff and all (except the most senior) managers.

5
who transferred to the new arrangements received significant increases in their pay13. This meant
that more experienced nurses competing at the same pay grade often appeared to offer much
better value for money. In addition, although perhaps not as a direct consequence of Agenda for
Change, more Clinical Psychologists are now working in multi-disciplinary teams alongside other
professionals and many more are taking on generic roles as managers of therapy services. It is
difficult to see this as anything other than a positive development for the NHS as a whole and the
individuals concerned say it has opened new career opportunities for them. However, they were
doubtful about the reaction of the profession as whole. Together with widespread variation in
access to therapy services, staff shortages and problems of low morale, it seems clear that the need
to get more rather than less involved in policy issues is challenging.
5. THEMES EMERGING FROM INTERVIEWS
5.1 Theory
5.1.1 The theory, such as it is, concerned with developing influence over NHS policy or other decision
making has a long if not always very respectable history14. Like Dale Carnegie who achieved huge
popular success with his book `How to win friends and influence people’ there has been a reluctance
to consider advocates of models of organisational change as part of mainstream Clinical Psychology,
even though their writing is popular. To some extent, this is not surprising. It has been developed in
large part alongside support for management and organisational change in the NHS15; it is
characterised by language and terminology which owes more to campaigning and political
imperatives than to recognisable theory (e.g., “the helicopter view for doing things better”; “Project
management in policy” “linear delivery cycles” “Achieving dynamic stability”, etc). Whilst there are a
number of very reputable consultancies providing support for organisational change whose work is
very soundly embedded in evidence (e.g., Philip Stokoe16 or The Tavistock17 courses on leadership,
Board and team functioning) it is not unusual for much of the work to mix personal, social and
communication skills with advice on personality, personal learning styles, team structure and
management methods and it arguably lacks theoretical coherence.
5.1.2 It is therefore possible that success in influencing policy, or of leadership and management
with which policy success is commonly linked, fails to hold the same attraction for Clinical
Psychologists as clinical work, research or teaching because it also lacks academic value. If so, Clinical
Psychologists could be counted alongside doctors (although perhaps not nurses) about whom the
same general conclusion could be drawn. For example, a doctor working in management is not as
well respected by his/her profession as a surgeon or a researcher. For Clinical Psychologists, this may
have implications for the way that they think, train and write about the profession. It may also have
13
Turpin, G and Llewellyn, S (2009) Chapter 29 `Development, Organisation and Dilemnas’. In Clinical Psychology in Practice Beinart, H., Kennedy P., and Llewellyn S (eds). The British Psychological Society and Blackwell Publishing Ltd. ISBN 978-1-4051-6767-3. 14
Dale Carnegie (1937) `How to Win Friends and Influence People’ Simon and Shuster. ISBN 1-4391-6734-6 15
NHS Leadership Academy www.leadershipacademy.nhs.uk Leadership and organisational development at the King’s Fund: www.kingsfund.org.uk NHS Institute for Innovation and Improvement www.institute.nhs.uk (now closed) Commissioning Support Units (CSUs) www.england.nhs.uk/commissioning and other independent providers of teaching and training such as the Work Foundation at www.workfoundation.com and NHS Employers at www.nhsemployers.org 16
http://www.philipstokoeconsultancy.co.uk/ 17
http://www.tavistockconsulting.co.uk/

6
implications for the way that the professional body, the BPS, represents the breadth and depth of
work undertaken by its practitioner members.
5.1.3 Some exceptional examples of how theory can be helpful are provided by Susan Michie18 and
colleagues who write cogently about impediments to the implementation in practice of policy
guidelines. Pendleton and Furnham’s book was also recommended19 by several experts, as was the
work of Graham Thornicroft20 and Michele Tansella who describe translational roadblocks that delay
the transfer of knowledge `from lab to life’ or from `bench to bedside’. They identify obstacles such
as the degree of flexibility in how policy information is drafted; its brevity; the reputation of those
promoting it; the time requirements; the determination of the `change agent’ to repeatedly urge its
use, and the rewards and recognition that may accrue. These are all issues with which those wanting
to effect policy and practice change must be concerned.
5.1.4. It is beyond the scope of a short report to do justice to a review of the theories that might
provide helpful underpinnings to policy development for psychologists. Suffice to say, most experts
acknowledged a significant impact of their preferred clinical or psychological therapies model
including, in particular, psychoanalytic and systems theories. Most commonly, they referred to the
importance of so-called non-specific clinical skills such as listening, empathising, and formulating.
Several spoke of the importance of `nudging’ rather than `shoving’ colleagues towards beliefs or
behaviours that would assist them in the realisation of their (not the expert’s) goals. More
information about this is provided in Section 5.4.
5.2 Practice
5.2.1. Relatively few qualified senior level Clinical Psychologists attending London DCP and LRPAC
meetings thought that the views of the profession were being heard in their workplaces. Some are
clearly struggling actively in an effort to participate in decisions being taken by management teams
which appear, at least on the surface, to be dominated by a more powerful (and certainly more
numerous) medical and nursing hierarchy.
5.2.2. Part of this seems to relate to the environment. Like other NHS employees, Clinical
Psychologists have had to deal with an ever-changing organisational landscape21. For example, in
2006, local Health Authorities were replaced by 150 Primary Care Trusts (PCTs) and 152 local (social
services) authorities, and eight regional offices became 10 Strategic Health Authorities (SHAs). In
2011 the Health and Social Care Act led to further reforms that David Nicholson famously said were
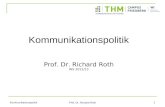
‘so big you can see them from space’ (see Figure 1 below). PCTs were replaced by Clinical
Commissioning Groups (CCGs); ten SHAs became five, and the Department of Health separated from
the NHS Commissioning Board (now NHS England). Local Health and Wellbeing Boards (HWBs) now
18
Michie, S., Webb TL and Sniehotta FF. (2010). The importance of making explicit links between theoretical constructs and behaviour change techniques. Addiction 105 1897-1898 19
Pendleton, D. and Furham A. (2012) Leadership: All you need to know’ ISBN 970-0-230-35442-5 www.palgrave.acmillan.com 20
Tansella, M. and Thornicroft, G (2009) `Implementation science: understanding the translation of evidence into practice.’ The British Journal of Psychiatry. 195. 283-285 and Thornicroft, G. Lempp, H and Tansella, M (2011) `The place of implementation science in the translational medicine continuum’ Psychological Medicine. 41 2015-2021. 21
Richardson, A. (2015) ‘The historical political and NHS Context’. Chapter 6 in `Clinical Psychology in Britain: Historical Perspectives.’ HoPC Monograph No. 2 Hall, J. Pilgrim, D. Turpin, G. (eds) www.bps.org/hopc

7
draw up local `Joint Strategic Needs Assessments’ (JSNAs) to inform the development of `Health and
Wellbeing Plans’ (HWPs) and new Clinical Commissioning Groups (CCGs) carry responsibility to
secure an appropriate level of service.
Figure 1. Structure of the NHS following the Health and Social Care Act, 2011
The Health and Social Care Act, 2011
Public health
Local Authorities
Public health providers
NHS
NHS EnglandMonitor
NHS Trust Development AuthorityCare Quality Commission
Clinical Commissioning GroupsHealth and wellbeing BoardsLocal Healthwatch (old LINks)
NHS providers
Adult social care
Local Authorities
Social care providers
National Institute for Health and Care ExcellenceHealth and Social Care Information Centre
Ministers and the Department of Health
5.2.3. Those involved (including myself) in the development of the National Service Framework for
Mental Health (1999) found these changes challenging as scope was widened not only to develop a
market in health care, but also to allow greater local flexibility in how national policy22 could be
interpreted (see report by Chris Ham and colleagues for the King’s Fund (op cit). The pressures were
significant for commissioners, yet even before the 2011 reforms, the environment was challenging
for them. For example, a report by the Audit Commission (2006)23 had shown that commissioning
decisions owed less to population need than to long-term historical pattern of spend. Although there
are now signs of benefit arising from an approach that is more `joined up’ between health and social
care, the early signs suggest that there is a long way to go before the current need for cost savings
cease to be commissioners’ leading motivation. This presents difficulties for all those working in the
NHS but as the Clinical Psychologists are fewer on the ground and not all of them very experienced
in this area, it is arguably more difficult.
22
The Kings Fund (2015) `The NHS under the coalition government’ Ham, C et al. 23
The Audit Commission (2006) `Managing Finances in Mental Health: a review to support improvement in best practice’. ISBN 1 86240 521 2 Richardson, A.

8
5.3 Training
5.3.1. The experts were asked about the origins of their competence in the policy area and a number
of common themes emerged. Almost all the experts were doubtful that their competence could be
attributed to their training. None had completed formal post-registration courses in policy,
leadership or management. However, some were very complimentary about skills in the policy
domain that were exhibited by supervisors and/or Course leaders and they identified an early wish
to emulate this.
5.3.2. Few (possibly no more than four or five out of about sixty) of the almost-trained psychologists
(the novices) who participated in the workshops expressed confidence in their abilities in relation to
influencing policy in the re-organised environment. Very few knew how to read a budget sheet;
hardly any were familiar with the annual planning cycle, or the organisational structures with which
the latest NHS reforms are associated. None knew the name of the Chief Executives in the Trusts
where they worked and none knew names of any non-Executive Directors.
5.3.3. At one level, this is not surprising. CP trainees are, after all, the most junior members of the
profession. However, most come into training with exceptional levels of very diverse pre-training
work and relevant experience. Many have worked in the NHS and many have experience of
managing people. For some therefore, their lack of confidence in being able to contribute to the
policy environment once they qualify appears to relate to the degree to which their experience is
legitimised, developed and valued during their Clinical Psychology training: they aren’t sure that
their knowledge and experience `counts’. One or two experts agreed; they thought training could
potentially be limiting trainees’ scope. Others suggested that trainees’ ambivalence or lack of
confidence reflected a conflict of identity in the profession as a whole about whether Clinical
Psychologists should be scientists, therapists or change agents working to intervene with individuals,
families, organisations and communities24. Whatever the case, most experts were keen to encourage
trainees to get more involved in policy matters and most trainees themselves expressed a wish to
learn more.
“There’s no magic bullet or special knowledge that they [the trainees] haven’t
got – it’s all about being prepared to have a go. I don’t see that in our trainees.
They’re too cautious and too ready to stand aside.”
5.3.4. Some training courses do provide teaching (e.g., RHBNC, University of Hertfordshire, UCL and
UEL) where varying levels of input on policy issues is provided and is positively received. However,
training is mainly course-based rather than based in placements. Although one expert25 took her
final year Trainees to a Service Delivery Board, an experience which he found exciting and
illuminating, few trainees questioned about their clinical placements reported a very positive
experience. Their supervisors apparently say that policy is more reasonably something that trainees
24
Turpin, G. Hall, J. (2015) Chapter 25 in `Clinical Psychology in Britain: Historical Perspectives.’ HoPC Monograph No. 2
Hall, J. Pilgrim, D. Turpin, G. (eds) www.bps.org/hopc 25
Dr Rana did this following an example set by her Chief of Operations who routinely does the same thing for medical trainees.

9
should focus on later as part of their continuing professional development, and many were aware
that the BPS does provide support here26. However, supervisors were apparently likely to say that
their own time for supervision was more appropriately taken up with therapy skills training, about
which they were careful, protective and thorough. This may be short sighted in a reorganised and
decentralised NHS where there is no guarantee of a more senior CP in post from whom support,
guidance or policy skills can be obtained. There may therefore be merit in including more coverage
of leadership, policy development and organisational change in pre-registration clinical psychology
training (theory and practice) to better equip trainees who will compete for jobs with nurses who
appear to have more confidence and competence.
5.3.5. As indicated above, the experts tended to see the acquisition of their skills in more personal
than professional terms. They learned from their experiences of success and failure; by working
alongside non-Clinical Psychologists and, notably, by making close connections with their clients and
managerial colleagues at work. Most denied any connection between their own views and those
expressed publically by the BPS or DCP. Indeed, on more than one occasion, an expert reported
feeling somewhat `rogue’ in relation to the professional body. Unfortunately, most were also unable
to identify examples when the BPS provided them with effective support, leadership or modelling.
Indeed, several gave examples of occasions when they had been very disappointed in decisions
taken or statements made by the BPS. Several said that they would like the Society to be much more
inclusive and outwardly supportive of patients’ interests and population health, rather than simply
support what appeared to be members’ self interests.
5. 4 Knowledge, attitudes and behaviours associated with effectiveness in policy
5.4.1. The experts tended to concur that motivation was an essential pre-requisite for engagement
in policy and it was generally acknowledged that work in this area is not to everyone’s taste, even
though Clinical Psychologists should be good at it. Some referred to the way that departments of
Clinical Psychology used to be organised with a much greater division of tasks than is generally now
possible. In the past, a more senior person might carry responsibility for policy through membership
of, for example, a District Health Board or a top management team.
“Now, it isn’t possible for Clinical Psychologists to avoid the issue by saying `I’m
just here for the patients I see, not for anything else.’”
5.4.2. National planning guidance27 is essential background reading. This sets out ` the steps to help
local organisations deliver a sustainable, transformed health service and improve the quality of care,
wellbeing and NHS finances’. It is published by NHS England in partnership with the bodies that
developed the Five Year Forward View (October 2014) and sets out how, this year, localities must
develop `Sustainability and Transformation Plans’ or STPs. Additional funding (a Sustainability and
Transformation Fund or STF) to support implementation is also available.
26
Leadership modules now form part of several pre-registration training programmes (e.g., at RHBNC). In 2010 the BPS/DCP established a Clinical Psychology Leadership Development Framework http://www.bps.org.uk/ and in 2002 the Leadership and Management Faculty was established to support psychologists exchange information and opinion. 27
NHS Providers: shared planning guidance for 2016/17 to 2020/21 www.gov.uk/guidance/delivering-the-forward-view-nhs-planning-guidance-for-201617-to-202021

10
5.4.3. Experts agreed that it was essential to know the environment in which decisions are taken.
They emphasised the importance of `mapping the territory’, and of `knowing the people’. This
means understanding where, as well as how, and by whom decisions are taken in the wider system
of health and social care; for example, whether commissioning for particular services is local,
regional or national; which are the decision making teams and what are their needs - for example, to
make efficiency savings or meet local imperatives for safer services.
5.4.4. There is a large volume of web-based guidance on commissioning and the planning cycle and
most Clinical Psychologists will be able to find this as it relates to their localities. However, it is also
worth checking local Board papers which are public documents. Mapping the territory also means
understanding more about features of the local population epidemiology (age and socioeconomic
profile, housing and education issues, health issues) likely to have a bearing upon health needs
assessments and hence upon Joint Strategic Needs Assessments which are used to inform service
plans.
5.4.5. It also means understanding the financial context and the pressures on local services to make
efficiency savings and the associated timeframes. In this way health needs, financial pressures and
evidence can be `triangulated’ to develop proposals for effective interventions. There are several
illustrations of the way that work by Clinical Psychologists has made a powerful impact in some
relatively novel areas including work to reduce the use of expensive `Out of Area Treatments’ in
mental health28; work to reduce inpatient admissions; meet A & E Waiting Times targets, or improve
patient experience. Other examples mentioned by the experts relate to evidence for psychological
interventions to promote better workplaces29 based in work (the `Whitehall Studies’) led by
Professor Michael Marmot30,31 and work by West et al (2002)32 showing a correlation between HR
practices in acute hospitals and patient mortality.
5.4.6. Knowing the people involves identifying decision makers, meeting them, and perhaps reducing
social distance perhaps by lunching together or meeting to discuss common interests. Several
experts commented on the perceptible difference between Clinical Psychologists and medical or
nursing staff in this regard with the former much more likely to hold back from work based social
engagement. However, engagement involving face to face contact, sharing ideas in advance of a
proposal, helps to promote allegiances and it reduce the hesitation which can be associated with
unfamiliarity. One expert summed up effective networking as the process of ensuring that ideas and
views are “socialised”.
5.4.7. Among the behaviours most often mentioned by experts, there is an attitude or a stance
which many experts went to lengths to explain. It is perhaps best summarised by the advice given by
28
More information about this is available from Dr John Cape. 29
Sainsbury Centre for Mental Health (2007), Mental Health at Work. 30
www.ucl.ac.uk/gheg/marmotreview 31
Siegrist, J et al (2009) `Employment arrangements, work conditions and health inequalities: report on new evidence on health inequality reduction produced by Task Group 2 for the Strategic Review of Health Inequalities post 2010.’ www.ucl.ac.uk/gheg/marmotreview/ 32
Wells M et al (2002). `The link between the management of employees and patient mortality in acute hospitals.’ The International Journal of Personnel and Human Resource Management 13 (8) 1299-1310.

11
Duncan Law to `Be useful first and a psychologist second’. This is about Clinical Psychologists
aligning themselves in public with the values underpinning the NHS system of care within which they
work, and about the importance of prioritising patients’ interests over self-interest. Wendy Wallace,
formerly a CP and now an NHS Chief Executive in London spoke very coherently on this point; she
said:
“It should never, ever, ever, be about the profession; it should always be about
care quality.”
5.4.8. For Dr Rana, this was partly about Clinical Psychologists learning to take risks, to commit to
assisting the organisation to deliver its goals rather than stand on the fence or stay isolated from the
mainstream. “There’s a perfectionist streak in us”, she said. “We’re not risk takers” and “We don’t
like to compromise.” Another expert said “We are paralysed by a need for consensus”’ and “You
don’t see the psychiatrists worrying about that.” Of course, this is not meant to imply that no Clinical
Psychologist should ever oppose policy; rather it is a recommendation about the strategies that are
most likely to be effective at the point when policy is developing.
Figure 2. Quotes from the experts about the early stages of influencing policy
`Know the ground and the environment you’re working in.’
`Be useful first and a psychologist second.’
`Collaborate. Work in partnership. Find common ground.’
`Talk, listen, meet, share.’
It does help if you can lunch, drink and network.’
`Make relationships personal.’
`It’s vital if you want an idea to be taken forward, you have to socialise it first’
`No-one should be surprised at a meeting to hear an idea for the first time,’
`It is absolutely essential to be prepared to take responsibility although some of
those roles are incredibly demanding.’
Patience and resilience `Choose your battles carefully. There are some you’ll
never win.’
5.4.9. Figure 2 contains some of the quotes from the experts about the important things to think
about in the early stages of influencing policy, including: `choose your moment’ and `keep it simple’
The experts agree that a short narrative will almost always be better than a long academic paper,
but..

12
“Never underestimate the ignorance of your audience. Always show respect;
they are often very able”.
5.4.10. A distinction between the personal interests of Clinical Psychologists and the interests of
those on the receiving end of their advice was also drawn by Professor Fonagy. He contrasted what
he called public and private competence. For him, clinical skill lies at the heart of policy
competence, and some of the key features include listening, `mentalising’ or empathising with the
other’s perspective; and helping to solve their (not your) problems. He also commented on the skill
of `nudging’ slightly in the desired direction at the point when solutions start to be sought, rather
than pushing or shoving. Importantly, competence involves being careful to avoid the defensiveness,
alienation and criticism which may promote social distance. It also involves effective personal
emotional management as policy competence is seldom associated with behaviour that is angry,
indignant or self-justificatory.
5.4.11. The importance of timing was also reinforced by Professor Clark whose work with Lord
Richard Layard33 to develop the Improving Access to Psychological Therapies (IAPT) programme34.
“In Britain there are two key moments when you can inject new ideas into
public policy – one is before a general election and other is before the
Government’s periodic spending reviews”.
For Professor Clark, there was an important message about the moment when partners and those
with influence were keen to pull in the same direction. He also talked about the importance of
knowing when to back down; to bide your time, and save your plans for another day. Of course, few
psychologists are likely to achieve change of the magnitude of IAPT or have the influence that
Professors Clark or Fonagy have, but the message about timing of decision-making and of dates for
local commissioning and planning cycles are no less important.
5.4.12. Many experts talked about the importance of personal resilience and of the need to take
`the long view’. However, it is clear that unexpected opportunities to realise a vision cannot be
grasped if the vision and reasons for it are not readily brought to hand. This requires preparation,
reflection and planning. This reinforces a message for other Clinical Psychologists about risk taking
and about what some called `just sticking your neck out’ if you believe that an approach is the right
one to take. It reinforces the importance of patience, readiness and resilience.
5.4.13. Figure 3 summarises some of the points made by experts that chime with Professor Fonagy’s
helpful distinction between `public’ and `private’ although, inevitably, people vary in the words they
use. For Professor Hacker-Hughes the essential skills are summed up as needing to achieve
`Presence, Voice, Visability and Impact’. For him, too, there is clear focus on preparing the ground,
understanding the organisational framework, meeting and getting to know the people, and being
33
Professor David Clark was responsible for a number of major developments of health policy, most notably with Lord Richard Layard for the Improving Access to Psychological Therapies (IAPT) programme developed in the NHS in 2012. 34
Layard, R. and Clarke, DM (2014) `Thrive: the power of Psychological Therapies’ Penguin Books ISBN 978 1 846 14605 3.

13
clear about their (as against your own) priorities, not least because of widespread suspicion amongst
some managers in the NHS about the professional protectionism which has characterised some of
the more public negotiations between professional bodies and government.
5.4.14. For many others, including Dr Ralph, once an initial assessment of the environment for
change has been undertaken, therapy skills (potentially from a number of different perspectives) are
the ones they tend to draw upon. For them, the task is about listening, formulating, asking
questions, and understanding what they called the `sub-text’ of, for example, Board and team
meetings.
Figure 3. Public and private competencies associated with influencing policy
PUBLIC
• Empathy
• Understanding
• Partnership
• Alignment
• Communication
• Helpfulness not opposition
• Inquisitive stance
• Know context and time frames
PRIVATE
• Resilience• Tenacity• Reflection• Personal emotional
management• How to triangulate your
view, their view and the evidence.
• When to `nudge’ rather than push.
“Competencies fall into two types: public and private...”
5.4.15. All the experts referred to the importance of measuring outcomes. Professor Clark was clear
that without clear evidence of good outcomes for CBT, IAPT would have failed to gain initial support
from government. Furthermore, he said, it was only the evidence of the impact of the programme
that led to its continued and ring-fenced funding by the Coalition government at a time of austerity.
Several experts spoke about the importance of outcomes measurement. Several also expressed
surprise and regret that there appears still to be resistance amongst some psychologists not only to
the package of outcome measures associated with IAPT but also to the use of routine measures of
outcome in their own work. Several mentioned psychodynamically oriented Clinical Psychologists in
particular here (something that Professor Fonagy has worked to address).
5.4.16. All the experts also agreed on the absolutely essential need to work in partnership with
representatives from other professions, particularly psychiatrists and senior nurses who are so often
in senior management roles. One expert, for example, attended the recent annual conference for
Allied Health Professionals (AHPs)35 and was surprised to see no other Clinical Psychologists present.
Many felt it important for the BPS to work more closely with other professional bodies (e.g., Royal
35
NHS England Chief Allied Health Professions Officer Conference. London 23rd
June 2016. Focused on the solutions
AHPs can deliver to the challenges faced in New Care Models and outlined in the Five Year Forward View.

14
College of Psychiatrists, Royal College of Nursing, the Royal College of General Practitioners,
voluntary and charitable groups, and service users and carers). It was also thought important for the
BPS to make stronger partnerships with groups representing AHPs who work across a variety of
specialisms in health, including acute medicine.
5.4.17. Collaboration and partnership is a particularly powerful way to strengthen engagement with
and influence over policy and experts gave a number of different examples36. Clinical Psychologists
are also now managed alongside and/or by staff from other professional groups; they also manage
other professionals. This, along with the fact that other professionals are also actively engaged in the
delivery of psychological therapies, means that closer relationships between Clinical Psychologists
and others are very important to cultivate.
5.4.18. A number of policy papers now reinforce the importance of partnerships with service users
as a way to deliver better outcomes in health care. Many would argue that arguments for changes in
policy can no longer be successful without this. The NHS Outcomes Framework37, for example,
enshrines user-focused Patient Reported Outcome Measures (PROMS) and Patient Reported
Experience Measures (PREMS) as one basis for reporting on the effectiveness of NHS care. Other
examples of patient involvement includes the move towards recovery-oriented models of care which
emphasise user-defined outcomes and shared decision-making about treatment, or the formal
engagement of patients as stakeholders on Health and Wellbeing Boards where they now have
power to refer CCGs to NHS England if their commissioning plans fail to be aligned with the local
health strategy.
5.4.19. Last but not least, expert Clinical Psychologists, mention luck as an important feature of
policy competence. Although at least two of the experts interviewed were represented on Strategic
Clinical Networks, both attributed their involvement to a mixture of good timing and serendipity, as
did Professor Clark in relation to other national work with which he has been engaged. However,
prior to their involvement, all these individuals all had a notable record of success in working in close
partnership with precisely the key groups and service users with whom NHS England or the
Department of Health wanted to engage and in at least one case, the working partnerships that DH
wanted to support had already been established. It is therefore tempting to say that these
individuals, to some degree, made their own luck rather than waiting for it to arrive.
6. Special issues for London
6.1 Most experts were not of the view that London presented an exceptional challenge, although
they were all clear that the presence of large centres of excellence in research, teaching and clinical
practice meant competition was steep for places on London-based policy forums.
36
`MindEd’ is a free educational resource on children and young people’s mental health for adults developed in a partnership with NHS England, the medical and nursing royal colleges, the BPS, BACP and Young Minds funded by DH and the DoE with which Duncan Law was involved in helping to establish. 37
Department of Health (2010). The NHS Outcomes Framework 2011-2012, London: Department of Health and Office for
National Statistics (July 2011), Measuring National Well-being: Measuring What Matters, Office for National Statistics. Available online at: <http://www.ons.gov.uk/ons/guide-method/user-guidance/well-being/index.html>

15
6.2 Most concurred that it would be important for all local Clinical Psychologists in London to read
the report of the National Transformation Board for London38 created by London CCGs in
partnership with NHS England to implement the NHS Five Year Forward View (October 2014) . This
set out plans to:
Do more to tackle the root causes of ill-health
Give patients more control of their own care including the option of combining health and
social care
Change to meet the needs of a population that lives longer
Develop and deliver new models of care
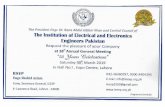
6.3 Priorities for London’s mental health in particular can be found in the report from NHS England39
summarised in Figure 4. This sets out a number of issues distinguishing London from other parts of
the country. For example, in London “...child poverty is a third higher than elsewhere in England and
the obesity rate is the highest of any other region”. In London, mental illness and homelessness are
“more prominent than elsewhere....” The report points out that people with mental ill health die
10-15 years before others, and only 14% get the help they need in a crisis. It also discusses
challenges in training and support for GPs; and early intervention for children. The Children’s
Strategic Clinical Network40 has also highlighted major gaps here. London apparently has the highest
demand for child and adult mental health services of the whole country, yet it also has poor rates of
access to crucial services, such as IAPT, and the lowest rates of recovery and improvement in
England. These areas provide potential opportunities for psychologists to strengthen their influence.
Figure 4. Priorities for the development of London’s Mental Health Services (NHS England, 2015)
The NHS in London has come together to agree five joint priorities for mental health for 2015/16 and beyond to address these demands and issues for the benefit of our patients:
1. Address the gap in life expectancy ‘the stolen years’ between those with SEMI and the rest of the adult population
2. Reduce the variation and improve quality, access and co-ordination for people in crisis and meet the crisis care concordat
3. Strengthen mental health in primary care to meet the challenges
4. Improve access to meet new standards for mental health services as outlined in the FYFV, focusing on; early identification and access to psychosis services; perinatal mental health and IAPT
5. Improve the use and sharing of data and information
38
NHS England (2015) `Transforming London’s Health and Care Together’ www.england.nhs.uk/london/wp-content 39
Achieving Better Access to Mental Health Services by 2020 (2014) NHS England www.gov.uk/government/uploads/system/uploads/attachment_data/file/361648/mental-health-access.pdf 40
Strategic Clinical or Care Networks were established by NHS England in 2012 in key areas of challenge for health and
wellbeing. They work on cross-cutting themes aligned to the NHS Outcomes Framework. The two likely to be the most relevant to CPs are 1. Mental health, dementia and neurological conditions. 2. Maternity, Children and Young People.

16
6.4. Improving policy competence
6.4.1 Table 1 summarises the comments that those contributing this work made concerning the
strengths, weaknesses, opportunities and threats (SWOT) that currently affect the policy
competence of Clinical Psychologists which could potentially form the basis for a framework to
strengthen policy competence amongst London Clinical Psychologists.
Table 1. A `SWOT’ analysis of factors affecting policy competence
STRENGTHS
WEAKNESSES
OPPORTUNITIES
THREATS
Intellectual capital Ignorance of the system, budgets and funding flows; decision making processes, people and time-frames
Outcome measurement and impact assessment
Rising care costs
Understanding of systems and processes
A lack of public alignment with NHS values.
Work in safety, system governance and risk management
Increasing transparency of activity and outcomes
Social and communication skills
Professional Protectionism and special pleading
Diminishing resources and how to achieve value during austerity
Small numbers and competition from others
Persistence and resilience
Isolation: a failure to work in partnership or make allegiances
Integration and partnership (physical and mental health41, acute medicine, MI and PD).
Poor morale and confidence
People management skills
Unwillingness - to share, bend, compromise, take risks
Workforce issues: low productivity, staff morale and sickness absence42
Failure to prioritise or afford status to policy work
A broad-based theoretical understanding
Reluctance to research in practice and measure outcomes
Primary care and early intervention
High cost of CPD and training
A very good training
A lack of leadership
Public demand Impact of austerity
Clinical and research skills
A lack of assertiveness
Technological (digital) development43 e.g., CCBT?
Low public profile
41
Stopping Over-Medication of People with a Learning Disability (STOMPLD) pledge New guidance published as part of the
pledge supports prescribing healthcare professionals to review inappropriate prescriptions for people with a learning disability and/or autism. 42
NHS England (2016) `NHS Staff health and wellbeing: CQUIN guidance’ Gateway ref. 05221 offering financial incentives to improve the health and wellbeing of NHS staff in England, as part of the Healthy Workplaces scheme. www.nhs 43
national reimbursement route for new medtech innovations to accelerate uptake of new medtech devices and apps for patients with diabetes, heart conditions, asthma, sleep disorders, and other chronic health conditions announced June 16.

17
6.4.2 First, several experts agreed that there would be value in building on work that has already
started at national level within the BPS44 for the development of competence in leadership, policy
development and organisational change. Several commented that, during his term as President,
Professor Hacker-Hughes had set out a clear vision for the BPS Divisions, Faculties and Sections as
part of an internal re-structuring which, if this work is continued, should help further. One or two
experts also pointed to the importance of the professional body taking a less centralised or
`command and control’ approach by providing support for individuals who have become influential
outwith the auspices of the BPS45.
6.4.3. Detailed questions about resources did not form part of the interviews with experts and there
was widespread recognition that provision of CPD in the policy area would potentially be expensive -
BPS membership fees are currently considerably lower than those charged by the BMA and it would
appear that there is no surplus of funds. However, experts felt that the BPS and national DCP could
potentially help to promote interest and enthusiasm to participate and learn more amongst Clinical
Psychologists and their trainers, and re-balance interest amongst trainees to work in areas other
than psychological therapy by ensuring that the profile for policy work was raised in the The
Psychologist and Clinical Psychology Forum.
6.4.4. Strong and positive comments were made about the breadth and depth of Clinical Psychology
trainees and the qualities that they bring. A focus within CTiCP might legitimise their use and help
more junior members of the profession who, it seems, are currently at risk of undermining
themselves in the face of competition. Some thought that trainers might work together through the
national Committee on Training in Clinical Psychology (CTiCP) to identify and share models of good
practice in teaching and supervised practice. This would help those on pre-registration training
courses with relatively low levels of input to potentially raise their game. This is also an approach
that could be supported by the London courses alone.
6.4.5. Some thought it might be helpful for Clinical Psychologists with particular expertise in
localities to develop short policy briefings as an aide to planning and involvement by Clinical
Psychologists who feel that they lack expertise. These, it was agreed, should be practical, short,
written in plain English and managed by the DCP branch which could potentially broker
development, distribution and extension in the form of workshops or conferences.
6.4.6. Third, there may be scope to develop support on an individual or small group basis for
qualified Clinical Psychologists in London who do not currently feel that their voices are being heard.
As already indicated, there are private providers of consultancy (e.g., The Tavistock) where support
and training are available and there is one model of good practice in the delivery of formalised
Continuing Professional Development for Clinical Psychologists operating in London46 based at UCL,
albeit with uncertain future funding. However, the diversity of the policy challenge in London,
coupled with the individual needs and personal experiences of those involved, suggest that a more
bespoke approach might also be helpful.
44
DCP Leadership and Management Faculty http://www.bps.org.uk/networks-and-communities 45
Dr Law highlighted Julia Faulconbridge outgoing chair of the DCP CYPF faculty as exemplifying very good practice
here. 46
Dr Kat Alcock UCL, Executive Lead, DCP mentoring scheme organised between the 6 London courses to increase ethnic diversity of CPs [email protected]

18
6.4.7. Several experts said that they would be prepared to offer supervised placements and/or
mentoring for qualified staff wanting to strengthen their competence. This might consist of
orientation and learning about local systems and structures, direct observation of and/or
participation in planning meetings, modelling, reflection and discussion of relevant theory and
practice. London contains some of the country’s leading experts in a variety of fields who may be
prepared to help. Two experts suggested that the London DCP Branch might helpfully develop a
Resource Directory to support potential learners. Some experts were very puzzled by the lack of
apparent uptake of new(ish) digital technologies like Skype which would make distance learning
easier.
6.4.8. Several experts referred to the scope for individual Clinical Psychologists to take on work
outside their traditional sphere of competence in a temporary role within their Trusts. Many
referred to their own experience of effectively `volunteering’ to help a Board or a manager to solve a
problem. Examples included help for commissioners to understand statistical data on outcomes and
performance; help for HR teams to tackle sickness absence in the NHS workforce; reflective practice
to improve team functioning; and work to strengthen clinical governance and patient safety. In each
case, work undertaken by the Clinical Psychologist was essentially `extra-curricular’; it was not
formally part of the job description. However, the results were generally well regarded by all
concerned and provided a key opportunity for learning and influence.
7. Conclusions and recommendations
7.1 To help to understand and potentially strengthen the influence in policy of applied psychologists
in London, a series of semi-structured interviews with senior applied clinical and academic
psychologists in London and two workshops with trainees were undertaken. All the names of the
`experts’ were identified as a result of their having either a strong national or local profile (or both)
and a record of success in influencing policy and promoting organisational change. This report
summarises the results of those interviews, and it makes recommendations for the DCP branch and
LRPAC to consider.
7.2 There was a high level of consistency amongst those interviewed in terms of the themes and
opinions that they shared about the development of policy competence. Most notably, the experts
failed to attribute their personal success either to their training or to connections with the
professional body.
7.3. They were united in thinking that the current organisational context coupled with changes in the
way that Clinical Psychologists work are challenging practitioners in new ways. Rising demand for
Clinical Psychologists, low levels of supply, some shrinkage in the availability of more senior qualified
staff to provide policy support, and competition from other professions together lead to some
Clinical Psychologists feeling isolated and in need of support.
7.4 Potential solutions are not complicated or difficult to find and follow logically from a review of
the underlying potential causes – in other words, there is no `magic bullet’. Recommendations at
three levels are made for the DCP and London Regional Psychology Advisory Committee to consider.

19
National
7.5 Build on work that has already started at national level within the Leadership and Management
Faculty of the BPS to support the development of policy competence. Initially, this might be helped
by further discussion between the London Branch of the DCP and the Head of the Faculty.
7.6. The Group of Trainers in Clinical Psychology might helpfully gather models of good practice and
disseminate this information to the courses as a way to promote best practice in the development of
policy competence in pre-registration training.
7.7. The DCP could potentially help to create interest and enthusiasm amongst Clinical Psychologists
and their trainers to participate and learn more, and re-balance interest amongst trainees to work in
policy or areas other than psychological therapy by profiling articles about policy success in Clinical
Psychology Forum and the Psychologist. The aim here is to try to elevate the status of such work
within the profession.
Local
7.8. The London DCP Branch might consider developing a Directory or list of those prepared to offer
support and supervision to Clinical Psychologists in London whose problems warrant a more
`bespoke’ approach designed to address their individual needs and circumstances.
7.9. The London DCP branch could support this work in areas of common interest with the LRPAC by
hosting workshops and meetings; by commissioning short briefing papers or speakers (e.g., about
the work of the Mayor’s office, activities of the London based Strategic Networks, London office of
NHS England, etc).
Individual
7.10. Clinical Psychologists wanting to strengthen their influence in policy might usefully approach
colleagues with expertise for support, mentoring and/or supervision.
7.11. Clinical Psychologists might consider developing an individual SWOT analysis and personal
development plans to strengthen their policy knowledge and competence. Ideally, these would be
developed with line managers so that delivery of local priorities could also be supported.
AKNOWLEDGEMENTS
I am very grateful to all those who were interviewed for their time and help to identify the themes
and their competencies with which they judged their effectiveness to have been associated and to
the members of the Steering Group and the DCP branch for their contribution. The mistakes in
summarising some very interesting conversations are mine.