Progression of whole-heart Atherosclerosis by coronary CT ...
9
Research paper Progression of whole-heart Atherosclerosis by coronary CT and major adverse cardiovascular events Alexander R. van Rosendael a, b , Fay Y. Lin a , Inge J. van den Hoogen a, b , Xiaoyue Ma c , Umberto Gianni a , Omar Al Hussein Alawamlh a , Subhi J. Al’Aref a , Jessica M. Pe~ na a , Daniele Andreini d , Matthew J. Budoff e , Filippo Cademartiri f , Kavitha Chinnaiyan g , Jung Hyun Choi h , Edoardo Conte d , Hugo Marques i , Pedro de Araújo Gonçalves i , Ilan Gottlieb j , Martin Hadamitzky k , Jonathon Leipsic l , Erica Maffei m , Gianluca Pontone d , Gilbert L. Raff g , Sanghoon Shin n , Yong-Jin Kim o , Byoung Kwon Lee p , Eun Ju Chun q , Ji Min Sung r, s , Sang-Eun Lee r, s , Donghee Han r, t , Daniel S. Berman t , Renu Virmani u , Habib Samady v , Peter Stone w , Jagat Narula x , Jeroen J. Bax b , Leslee J. Shaw a, * , James K. Min a , Hyuk-Jae Chang r a Department of Radiology, NewYork-Presbyterian Hospital and Weill Cornell Medicine, New York, USA b Department of Cardiology, Leiden University Medical Center, Leiden, the Netherlands c Department of Healthcare Policy and Research, NewYork-Presbyterian Hospital and Weill Cornell Medicine, New York, USA d Centro Cardiologico Monzino, IRCCS Milan, Italy e Department of Medicine, Los Angeles Biomedical Research Institute, Torrance, CA, USA f Cardiovascular Imaging Center, SDN IRCCS, Naples, Italy g Department of Cardiology, William Beaumont Hospital, Royal Oak, MI, USA h Pusan University Hospital, Busan, South Korea i UNICA, Unit of Cardiovascular Imaging, Hospital da Luz, Lisboa, Portugal j Department of Radiology, Casa de Saude S~ ao Jose, Rio de Janeiro, Brazil k Department of Radiology and Nuclear Medicine, German Heart Center Munich, Munich, Germany l Department of Medicine and Radiology, University of British Columbia, Vancouver, BC, Canada m Department of Radiology, Area Vasta 1/ASUR Marche, Urbino, Italy n Division of Cardiology, Department of Internal Medicine, Ewha Womans University Seoul Hospital, Seoul, South Korea o Department of Internal Medicine, Seoul National University College of Medicine, Cardiovascular Center, Seoul National University Hospital, Seoul, South Korea p Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, South Korea q Seoul National University Bundang Hospital, Sungnam, South Korea r Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Yonsei University Health System, Seoul, South Korea s Yonsei-Cedars-Sinai Integrative Cardiovascular Imaging Research Center, Yonsei University College of Medicine, Yonsei University Health System, South Korea t Department of Imaging and Medicine, Cedars Sinai Medical Center, Los Angeles, CA, USA u Department of Pathology, CVPath Institute, Gaithersburg, MD, USA v Division of Cardiology, Emory University School of Medicine, Atlanta, GA, USA w Cardiovascular Division, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA x Icahn School of Medicine at Mount Sinai, Mount Sinai Heart, Zena and Michael A. Wiener Cardiovascular Institute, and Marie-Jos ee and Henry R. Kravis Center for Cardiovascular Health, New York, NY, USA ARTICLE INFO Keywords: Coronary artery disease Risk stratification Plaque progression Coronary CTA ABSTRACT Background: The current study aimed to examine the independent prognostic value of whole-heart atherosclerosis progression by serial coronary computed tomography angiography (CCTA) for major adverse cardiovascular events (MACE). Methods: The multi-center PARADIGM study includes patients undergoing serial CCTA for symptomatic reasons, 2 years apart. Whole-heart atherosclerosis was characterized on a segmental level, with co-registration of Abbreviations: CCTA, coronary computed tomography angiography; IVUS, intravascular ultrasound; MACE, major cardiovascular events; PAV, percent atheroma volume; TAV norm , Total atheroma volume normalized for vessel length. * Corresponding author. Dalio Institute of Cardiovascular Imaging, New York-Presbyterian Hospital and Weill Cornell Medical College 413 E. 69th Street, Suite 108 New York, NY, 10021, USA E-mail address: [email protected] (L.J. Shaw). Contents lists available at ScienceDirect Journal of Cardiovascular Computed Tomography journal homepage: www.JournalofCardiovascularCT.com https://doi.org/10.1016/j.jcct.2020.12.007 Received 15 October 2020; Received in revised form 25 November 2020; Accepted 22 December 2020 Available online 1 January 2021 1934-5925/© 2020 Society of Cardiovascular Computed Tomography. Published by Elsevier Inc. All rights reserved. Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
Transcript of Progression of whole-heart Atherosclerosis by coronary CT ...

Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
Contents lists available at ScienceDirect
Journal of Cardiovascular Computed Tomography
journal homepage: www.JournalofCardiovascularCT.com
Research paper
Progression of whole-heart Atherosclerosis by coronary CT and majoradverse cardiovascular events
Alexander R. van Rosendael a,b, Fay Y. Lin a, Inge J. van den Hoogen a,b, Xiaoyue Ma c,Umberto Gianni a, Omar Al Hussein Alawamlh a, Subhi J. Al’Aref a, Jessica M. Pe~na a,Daniele Andreini d, Matthew J. Budoff e, Filippo Cademartiri f, Kavitha Chinnaiyan g,Jung Hyun Choi h, Edoardo Conte d, Hugo Marques i, Pedro de Araújo Gonçalves i, Ilan Gottlieb j,Martin Hadamitzky k, Jonathon Leipsic l, Erica Maffei m, Gianluca Pontone d, Gilbert L. Raff g,Sanghoon Shin n, Yong-Jin Kim o, Byoung Kwon Lee p, Eun Ju Chun q, Ji Min Sung r,s,Sang-Eun Lee r,s, Donghee Han r,t, Daniel S. Berman t, Renu Virmani u, Habib Samady v,Peter Stone w, Jagat Narula x, Jeroen J. Bax b, Leslee J. Shaw a,*, James K. Min a, Hyuk-Jae Chang r
a Department of Radiology, NewYork-Presbyterian Hospital and Weill Cornell Medicine, New York, USAb Department of Cardiology, Leiden University Medical Center, Leiden, the Netherlandsc Department of Healthcare Policy and Research, NewYork-Presbyterian Hospital and Weill Cornell Medicine, New York, USAd Centro Cardiologico Monzino, IRCCS Milan, Italye Department of Medicine, Los Angeles Biomedical Research Institute, Torrance, CA, USAf Cardiovascular Imaging Center, SDN IRCCS, Naples, Italyg Department of Cardiology, William Beaumont Hospital, Royal Oak, MI, USAh Pusan University Hospital, Busan, South Koreai UNICA, Unit of Cardiovascular Imaging, Hospital da Luz, Lisboa, Portugalj Department of Radiology, Casa de Saude S~ao Jose, Rio de Janeiro, Brazilk Department of Radiology and Nuclear Medicine, German Heart Center Munich, Munich, Germanyl Department of Medicine and Radiology, University of British Columbia, Vancouver, BC, Canadam Department of Radiology, Area Vasta 1/ASUR Marche, Urbino, Italyn Division of Cardiology, Department of Internal Medicine, Ewha Womans University Seoul Hospital, Seoul, South Koreao Department of Internal Medicine, Seoul National University College of Medicine, Cardiovascular Center, Seoul National University Hospital, Seoul, South Koreap Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, South Koreaq Seoul National University Bundang Hospital, Sungnam, South Korear Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Yonsei University Health System, Seoul, South Koreas Yonsei-Cedars-Sinai Integrative Cardiovascular Imaging Research Center, Yonsei University College of Medicine, Yonsei University Health System, South Koreat Department of Imaging and Medicine, Cedars Sinai Medical Center, Los Angeles, CA, USAu Department of Pathology, CVPath Institute, Gaithersburg, MD, USAv Division of Cardiology, Emory University School of Medicine, Atlanta, GA, USAw Cardiovascular Division, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USAx Icahn School of Medicine at Mount Sinai, Mount Sinai Heart, Zena and Michael A. Wiener Cardiovascular Institute, and Marie-Jos�ee and Henry R. Kravis Center forCardiovascular Health, New York, NY, USA
A R T I C L E I N F O
Keywords:Coronary artery diseaseRisk stratificationPlaque progressionCoronary CTA
Abbreviations: CCTA, coronary computed tomogvolume; TAVnorm, Total atheroma volume normaliz* Corresponding author. Dalio Institute of Cardiov
New York, NY, 10021, USAE-mail address: [email protected] (L.J. S
https://doi.org/10.1016/j.jcct.2020.12.007Received 15 October 2020; Received in revised forAvailable online 1 January 20211934-5925/© 2020 Society of Cardiovascular Com
A B S T R A C T
Background: The current study aimed to examine the independent prognostic value of whole-heart atherosclerosisprogression by serial coronary computed tomography angiography (CCTA) for major adverse cardiovascularevents (MACE).Methods: The multi-center PARADIGM study includes patients undergoing serial CCTA for symptomatic reasons,�2 years apart. Whole-heart atherosclerosis was characterized on a segmental level, with co-registration of
raphy angiography; IVUS, intravascular ultrasound; MACE, major cardiovascular events; PAV, percent atheromaed for vessel length.ascular Imaging, New York-Presbyterian Hospital and Weill Cornell Medical College 413 E. 69th Street, Suite 108
haw).
m 25 November 2020; Accepted 22 December 2020
puted Tomography. Published by Elsevier Inc. All rights reserved.

A.R. van Rosendael et al. Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
baseline and follow-up CCTA, and summed to per-patient level. The independent prognostic significance ofatherosclerosis progression for MACE (non-fatal myocardial infarction [MI], death, unplanned coronary revas-cularization) was examined. Patients experiencing interval MACE were not omitted.Results: The study population comprised 1166 patients (age 60.5 � 9.5 years, 54.7% male) who experienced 139MACE events during 8.2 (IQR 6.2, 9.5) years of follow up (15 death, 5 non-fatal MI, 119 unplanned re-vascularizations). Whole-heart percent atheroma volume (PAV) increased from 2.32% at baseline to 4.04% atfollow-up. Adjusted for baseline PAV, the annualized increase in PAV was independently associated with MACE:OR 1.23 (95% CI 1.08, 1.39) per 1 standard deviation increase, which was consistent in multiple subpopulations.When categorized by composition, only non-calcified plaque progression associated independently with MACE,while calcified plaque did not. Restricting to patients without events before follow-up CCTA, those with futureMACE showed an annualized increase in PAV of 0.93% (IQR 0.34, 1.96) vs 0.32% (IQR 0.02, 0.90), P < 0.001.Conclusions: Whole-heart atherosclerosis progression examined by serial CCTA is independently associated withMACE, with a prognostic threshold of 1.0% increase in PAV per year.
1. Introduction
Coronary computed tomography angiography (CCTA) allows for ac-curate and detailed characterization of atherosclerotic plaque from theentire coronary tree.1 Multiple studies have demonstrated a strongconcordance between the coronary atherosclerotic burden on CCTA andfuture major cardiovascular event.1–3 Similar data in carotid ultrasoundand coronary angiography support stong prognostic impact of athero-sclerotic extent.4,5 This relationship between disease burden and risk forfuture events implies prognostic importance of changes in atheroscleroticburden, which can be detected by serial imaging. This hypothesis wasconfirmed among >3000 patients undergoing serial intravascular ultra-sound (IVUS), demonstrating assocations between the magnitude ofatheroma increase and major events dominated by unplanned revascu-larization.5 A threshold of 1.0% increase in percent atheroma volume(PAV) per year was observed in patients experiencing events.
Software packages have recently allowed quantification of the extentof coronary plaque in CCTA.6–10 CT differs from IVUS by characterizationof plaque from all coronary segments, albeit at lower resolution, and theinclusion of lower risk patients. Prior serial CCTA studies have useddifferent plaque quantification methodologies (non-calcified plaqueonly, single artery or only main branches), exclusion of interval events, orwere too small in size to evaluate independent prognostic value of plaquechanges over time.9,11–14 The PARADIGM (Progression of AtheRoscle-rotic PlAque DetermIned by Computed TomoGraphic Angiography Im-aging) is the largest serial CCTA registry to date using rigorousquantification metholology and has long-term follow-up for eventsavailable. The current study aimed to evaluate the prognostic signifi-cance of atherosclerosis progression in CCTA and aimed to define aclinically relevant threshold of whole-heart atheroma progression.
2. Methods
2.1. Patients
The PARADIGM study is a multicenter (13 sites, 7 countries), obser-vational registry with prospective collection of follow-up data for MACEof patients undergoing serial CCTA at least 2 years apart.10 A rationaleand design has been previously published.15 The study was approved bythe institutional review board of all participating centers. Patients un-derwent baseline CCTA (CCTA-1) and follow-up CCTA (CCTA-2) forevaluation of suspected anginal symptoms. For the current analysis, pa-tients with prior revascularization before CCTA-1 (N ¼ 282), plannedrevascularization (<90 days) after baseline CCTA (N ¼ 83), or missingfollow-up information for MACE (N ¼ 229) were excluded, leaving 1166patients in the current study.
323
2.2. CCTA imaging and analysis protocol
CCTAs were acquired using �64 detector row CT scanners, withimage acquisition protocols in accordance with the Society of Cardio-vascular Computed Tomography guidelines including routine adminis-tration of betablocker and nitroglycerin before acquisition.16 DICOM filesfrom both CCTA’s were transferred to a Central Core Laboratory forblinded image analysis. Level III experienced CTA readers from theCentral Core Laboratory performed qualitative and semi-quantitativeCCTA analysis using dedicated software (QAngioCT Research Editionv2.1.9.1; Medis Medical Imaging Systems, Leiden, the Netherlands) withroutine measurement of inter- and intra-observer variability, which wasexcellent (inter- and intraobserver intra-class correlation coefficient forplaque volume >0.90).10,17 Per segment and per lesion analysis wereperformed for coronary plaque, lumen, vessel in all coronary arterysegments �2 mm in diameter (determined by software) from the coro-nary tree. Atherosclerosis was defined as any tissue �1 mm2 within oradjacent to the lumen that can be distinguished from the surroundingpericardial tissue, epicardial fat or the coronary lumen.1 Segmental datawere summed to per-patient level according to a modified 16-segmentcoronary tree model (Fig. 1).18 Plaque volume was set to zero innon-diseased cross sections. Fiduciary landmarks were used forco-registration of segments an lesions as previously described.10
Non-evaluable segments in either CCTA-1 or CCTA-2 were excludedpairwise for plaque progression analyses to obtain the same number ofevaluated coronary segments at the two CCTA scans. Segments that hadbeen stented between CCTA-1 and CCTA-2 were excluded in both scans.
2.3. Quantitative measurement of plaque burden and plaque change
Coronary plaque burden was defined by percent atheroma volume(PAV, plaque volume normalized for vessel volume) and total atheromavolume normalized for vessel length (TAVnorm).7–9,12–14,19 PAV waschosen as primary exposure and data for TAVnorm are reported in Ap-pendix. A prior CCTA study showed the lowest variance for the measurePAV.20 Annualized changes in plaque over time were calculated as theabsolute difference between CCTA-2 and CCTA-1, and divided by the CTinterval in years. The following definitions were used:
2.4. Baseline plaque burden
Plaque volume (PV) ¼ Vessel volume – Lumen volume.Percent atheroma volume (PAV) ¼ (PV/Vessel volume) * 100%Total atheroma volume normalized (TAVnorm)¼ (PV/Vessel length) *
mean population vessel length.

A.R. van Rosendael et al. Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
2.5. Absolute change
ΔPAV, % ¼ PAVCCTA-2 – PAVCCTA-1
2.6. Annualized changes
ΔPAV/year, % ¼ (PAVCCTA-2 – PAVCCTA-1)/ CT interval (years)
2.7. Study endpoints
Annualized plaque progression rates were assessed for their prog-nostic significance to discriminate individuals who experience MACE,defined as the occurrence of non-fatal myocardial infarction, death orunplanned, symptom driven revascularization (>90 days) after CCTA-1.Second, the patient cohort was restricted to patients free from MACEbefore CCTA-2 to evaluate progression rates associated with futureMACE. For analyses requiring a binary threshold of plaque progression,the average value of PAV progression per year in patients withMACEwaschosen (approximately 1.0% delta PAV/year). Also, annualized versusabsolute progression rates were compared for prognostic performance,and the influence of time duration between serial CCTA on magnitudes ofabsolute and annualized plaque progression associated with MACE wereevaluated. Follow-up was systematically performed by each local centerby a dedicated physician or research nurse, as previously described.15
Fig. 1. Example of whole-heart atherosclerosis progression. Coronary atherosclerosismid, distal and posterolateral branch), LAD (left main, proximal, mid, distal, and fi
sectional evaluation of the LAD is displayed (white dashed arrow) showing an increassummed from all coronary segments at baseline was 20.7% and 25.7% at follow upbaseline and follow-up CT was 2.7 years). The patient underwent urgent revasculariLAD, left anterior coronary artery; RCA, right coronary artery; LCX, left circumflex;
324
Myocardial infarction was defined according to contemporarydefinitions.21,22
2.8. Statistical analysis
Continuous variables were expressed as means � standard deviation(SD) and categorical variables as counts (percentage). Plaque data areprovided as median with interquartile range (IQR) because of their leftskewed distribution. Continuous data were compared with the inde-pendent T-test, Mann-Whitney U test, or Kruskal-Wallis test for unpaireddata, and Wilcoxon Signed Rank test for paired data, as appropriate.Categorical variables were compared with Chi-square test or McNemartest, as appropriate. The atheroscerlerotic cardiovascular disease(ASCVD) risk score was calculated for each patient.23 A Multivariablelogistic model to assess the association between plaque progression andMACE after adjusting for important baseline variables was constructed.Age, sex, diabetes, hypertension, current smoking, chest pain symptoms(non-anginal, atypical, or typical angina), statin use, baseline total- andlow-density lipoprotein cholesterol and baseline PAV were consideredfor inclusion into the multivariable model. The Kaplan-Meier methodwas utilized to display MACE-free survival according to baseline andprogression of PAV, and comparisons were made with the log-rank test.Large and small baseline plaque burden was defined by the median inPAV and plaque progression was dichotomized according to the medianin patients with MACE. Discrimination for MACE was assessed with theC-statistic and compared with the DeLong methods.24 Annualized andabsolute plaque progression were reported according to MACE occur-rence, and compared for differences between CT interval duration
was quantified from both baseline and follow-up CT scans in the RCA (proximal,rst diagonal), and LCX (proximal, distal, and ramus). In the mid panel, crosse in cross-sectional PAV (plaque area/vessel area * 100%) from 60 to 80%. PAV, which resulted in an annual increase in PAV of 1.7% (the duration betweenzation 1 year later of the LAD.PAV, percent atheroma volume.

Table 2CCTA data at baseline and follow-up.
Baseline Follow-up P-value
CAD severity (core-lab)
<0.001
0% 276 (23.7) 184 (15.8)1–29% 355 (30.4) 330 (28.3)30–49% 417 (35.8) 448 (38.4)50–69% 111 (9.5) 180 (15.4)�70% 7 (0.6) 24 (2.1)
Baseline laboratoryTotal cholesterol, mg/dl 186.6 � 37.7 171.61 � 37.08 <0.001LDL, mg/dl 114.3 � 33.9 98.67 � 31.53 <0.001Triglycerides, mg/dl 145.3 � 86.3 128.77 � 74.60 <0.001CRP, mg/L 0.86 (0.02, 1.15) 0.42 (0.05, 1.09) 0.989
CAD burdenPlaque volume, mm3 45.67 (4.36,
142.58)88.30 (19.52,217.16)
<0.001
PAV, % 2.32 (0.17, 7.00) 4.04 (0.99, 10.43) <0.001
Data provided as counts (%), mean � SD, or median (25th and 75th interquartilerange).CCTA, coronary computed tomography angiography; CAD, coronary artery dis-ease; CRP, C-reactive protein; LDL, low density lipoprotein; PAV, percentatheroma volume.
A.R. van Rosendael et al. Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
categories (tertiles). A 2-sided P-value <0.05 was considered statisticallysignificant. Statistical analyses were performed using SAS (version 9.4;SAS Institute Inc., Cary, NC) and R 3.3.0 (R Development Core Team,2016).
3. Results
3.1. Patient cohort
In total, 1166 patients who underwent serial CCTA were included(age 60.5 � 9.5 years, 54.7% male). At CCTA-1, 91.3% of the patientspresented with chest pain, and the majority was of East-Asian ethnicity,Table 1. ASCVD risk was low (7.5%) in 41.3%, intermediate (7.5–20%) in37.3% and high (>20%) in 21.4% of the population. Patients underwentCCTA-2 in 96% for symptomatic reasons (persisting, worsening, or new-onset of symptoms). Whole heart atherosclerosis included 397� 120mmof evaluated coronary artery length. At baseline, the prevalence of no,non-obstructive and obstructive CAD (�50% stenosis) was 22.6%,64.0%, and 13.4% (Table 2). Plaque volume and PAV increased signifi-cantly at follow-up: from 46 mm3 (IQR 4.36, 143) to 88 mm3 (IQR 20,217), P< 0.001, and from 2.3% (IQR 0.17, 7.0) to 4.0% (IQR 0.99, 10.4),P < 0.001. During 8.2 (IQR 6.1, 9.5) years of follow-up, 139 (11.9%)MACE events occurred (15 death, 5 non-fatal myocardial infarction, 119unplanned revascularization).
3.2. Baseline and plaque progression rates according to MACE
Baseline and annualized progression rates of PAV were significantly
Table 1Baseline characteristics.
Characteristic Value
(N ¼ 1166)
DemographicsAge, years 60.5 � 9.5Male 638 (54.7)Body mass index, kg/m2 25.2 � 3.3
EthnicityCaucasian 144 (12.3)East-Asian 960 (82.3)Other 62 (5.3)
Cardiac symptomsNo chest pain 100 (8.7)Non-anginal 121 (10.4)Atypical 888 (76.7)Typical 49 (4.2)
Cardiovascular risk factorsDiabetes 262 (22.6)Hypertension 674 (58.2)Dyslipidemia 392 (33.9)Familial history for CAD 327 (28.0)Currently smoking 234 (20.2)
ASCVD scoreLow (<7.5%) 482 (41.3)Intermediate (7.5–20%) 435 (37.3)High (>20%) 249 (21.4)
MedicationsAspirin 456 (39.9)ACE-I/ARB 350 (30.8)Beta blocker 300 (26.3)Calcium channel blocker 286 (25.2)Statin 456 (41.5)
Data provided as mean � SD or counts (%).ACE-I, angiotensin converter enzyme inhibitor; ARB, angio-tensin receptor blocker; CAD, coronary artery disease.
325
associated with MACE, Table 3. Baseline PAV in patients experiencingMACE was 7.09% (IQR 2.31, 13.31) vs 1.93% (IQR 0.00, 6.01) in thosewithout. The annualized progression rate in MACE among subgroups ofpatients experiencing early or late MACE (time to MACE above or belowthe median), men, women, age above or below 65 years, presence andabsence of diabetes or hypertension, ranged from 0.71% to 1.19% andwas significantly higher than in patients not experiencing MACE, whichranged from 0.23% to 0.54% within the subgroups. Adjusting for base-line PAV, the annual increase in PAV demonstrated independent prog-nostic value for MACE: OR 1.23 [95% CI 1.08, 1.39] per 1 SD increase inPAV/year. A consisistent 20% increase in risk for MACE per 1 SD increasein PAV/year was observed across the several suggroups, Table 3. Multi-variable analysis revealed that variables independently associated withMACE were baseline PAV, change in PAV, and the presence of typicalangina at baseline, Table 4. When plaque progression was categorizedaccording to the composition, only progression of non-calcified plaque,but not calcified, was independently associated with MACE. An increasein maximal stenosis, or the segment involvement score was not inde-pendently associated with MACE, Table 4. APPENDIX Table 1 reportsbaseline and progression values of TAVnorm, .
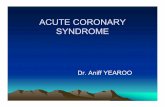
For Kaplan-Meier analyses, a cut-off of 1.0% increase in PAV per yearwas chosen given its aforementioned association with events. The 10-year MACE-free survival was 90.5% versus 72.8% for patients with lessversus more than 1.0% increase in PAV/year, log-rank P < 0.001, Fig. 2.Fig. 3 shows further separation of curves when patients were also strat-ified by the median baseline plaque burden.
3.3. Comparison of absolute versus annualized plaque progressionpredictive for future MACE
While excluding 42 patients with MACE events prior to CCTA-2,annualized PAV progression in patients with future MACE was 0.93%(IQR 0.34, 1.96) versus 0.32% (IQR 0.02, 0.90) for patients withoutfuture MACE, P < 0.001. When comparing the prognostic value of ab-solute with annualized PAV progression rates for MACE, discriminatoryperformances by C-statistic were similar: 0.673 (95% CI 0.612, 0.734) vs0.681 (95% CI 0.619, 0.742), P ¼ 0.295. However, with increasingduration between CCTA-1 and CCTA-2, absolute progression rates inMACE increased significantly (P¼ 0.001 for comparison between tertilesof CT-interval), while annualized progression rates not different withlonger CT-interval durations (P ¼ 0.468 for comparison between tertiles

Table 3Baseline and annualized plaque progression according to MACE occurrence.
Delta PAV/year, % Baseline PAV, %
MACE þ MACE – P-value Adjusted* OR (95% CI) of ΔPAV/year forMACE, per SD
P-interaction**
MACE þ MACE – P-value
Overall 0.86 (0.30,1.91)
0.32 (0.02,0.91)
<0.001 1.23 (1.08, 1.39) 7.09 (2.31,13.31)
1.93 (0.00,6.01)
<0.001
Time to MACEEarly MACE(<median)
0.75 (0.24,1.93)
– 8.24 (2.55,13.71)
–
Late MACE(>median)
0.90 (0.37,1.86)
– 5.31 (2.03,13.21)
–
Sex 0.229Men 0.80 (0.32,
1.88)0.38 (0.04,0.95)
<0.001 1.20 (1.03, 1.40) 7.24 (3.55,13.16)
2.49 (0.38,6.73)
<0.001
Women 1.04 (0.13,1.96)
0.27 (0.00,0.82)
<0.001 1.28 (1.03, 1.60) 6.59 (1.47,14.43)
1.41 (0.00,5.07)
<0.001
Age 0.167<65 0.71 (0.21,
1.70)0.26 (0.00,0.80)
<0.001 1.29 (1.06, 1.57) 5.10 (1.46,10.32)
1.52 (0.00,4.79)
<0.001
�65 1.19 (0.55,1.99)
0.48 (0.04,1.22)
<0.001 1.17 (0.99, 1.38) 9.87 (5.08,16.52)
3.14 (0.42,9.02)
<0.001
Diabetes 0.340Yes 1.19 (0.37,
2.12)0.53 (0.14,1.33)
0.009 1.15 (0.93, 1.43) 8.34 (3.79,12.82)
2.95 (1.03,7.11)
<0.001
No 0.75 (0.23,1.78)
0.27 (0.00,0.81)
<0.001 1.25 (1.07, 1.46) 6.31 (1.48,13.55)
1.63 (0.00,5.62)
<0.001
Hypertension 0.945Yes 0.93 (0.36,
2.04)0.41 (0.05,1.01)
<0.001 1.22 (1.05, 1.42) 7.99 (3.82,15.83)
2.44 (0.41,6.92)
<0.001
No 0.70 (0.05,1.51)
0.23 (0.00,0.73)
0.012 1.22 (0.96, 1.54) 4.28 (0.63,11.67)
1.42 (0.00,4.83)
0.002
Data provided as median (25th and 75th interquartile range).MACE, major adverse cardiovascular events; PAV, percent atheroma volume.*Adjusted for baseline PAV.** P-value for interaction of delta PAV/year between the several subgroups, including the main effects in the model.
Table 4Multivariable model of variables associated with MACE.
Variable Odds-ratio (95% CI) forMACE
P-value
Model 1Baseline PAV, per SD 1.34 (1.20, 1.50) <0.001Delta PAV/year, per SD 1.22 (1.08, 1.39) 0.002Presence of typical angina 2.46 (1.20, 5.05) 0.014
Model 2Baseline PAV, per SD 1.49 (1.34, 1.65) <0.001Delta noncalcified PAV/year, per SD 1.21 (1.05, 1.40) 0.010Presence of typical angina 2.46 (1.20,5.06) 0.014
Model 3Baseline PAV, per SD 1.39 (1.20, 1.62) <0.001Delta calcified PAV/year, per SD 1.09 (0.89, 1.22) 0.417Presence of typical angina 2.52 (1.24, 5.14) 0.001
Model 4Baseline PAV, per SD 1.46 (1.32, 1.62) <0.001Delta maximal stenosis severity 1.26 (0.92,1.72) 0.159Presence of typical angina 2.42 (1.19, 4.93) 0.015
Model 5Baseline PAV, per SD 1.47 (1.33, 1.63) <0.001Delta segment involvement score(SIS)
1.12 (0.96, 1.31) 0.137
Presence of typical angina 2.47 (1.21,5.02) 0.013
Other candidate variables for the stepwise model were: age, sex, diabetes, hy-pertension, current smoking, statin use, baseline total- and low-density lipopro-tein cholesterol.
of CT-interval), Fig. 4. Annualized PAV progression was approximately1.0% in the CT-interval tertiles in patients with MACE. Data regardingabsolute and annualized progression rates of TAVnorm predictive forfuture MACE are shown in APPENDIX Table 2, showing similar findingsof annualized progression rates of TAVnorm of approximately 18 mm3
unaffected by interval CT duration.
4. Discussion
The current study investigated the prognostic significance of whole-heart plaque progression on CCTA for MACE. We observed an associa-tion between plaque progression and major events independent frombaseline plaque burden; and further defined an relevant threshold to be1.0% annual increase in PAV.
4.1. Whole-heart quantification of coronary plaque
CCTA allows non-invasive evaluation of coronary plaque from theentire coronary tree and multiple prior studies demonstrated a strongrelationship between disease burden and risk for major events.1,25 Plaqueburden has traditionally been examined by integrated CCTA scores (e.g.segment stenosis score or segment involvement score) or coronary arterycalcium score.1,26,27 With the advent of semi-automated plaque software,quantification of whole-heart atherosclerosis has become possible. Usingrigorous quantification methodology including routine intra- andinter-observer checks, excellent reproducibility measures have been ob-tained with good concordance compared with IVUS imaging.10,15,17,28,29
These foundations have enabled reliable assessment of plaque burdenwith CCTA permitting assessment of changes in plaque over time by se-rial CCTA.30 Among 1255 patients from the same PARADIGM registry as
Definitions: MACE, major adverse cardiovascular event; PAV, percent atheromavolume; SD, standard deviation.326
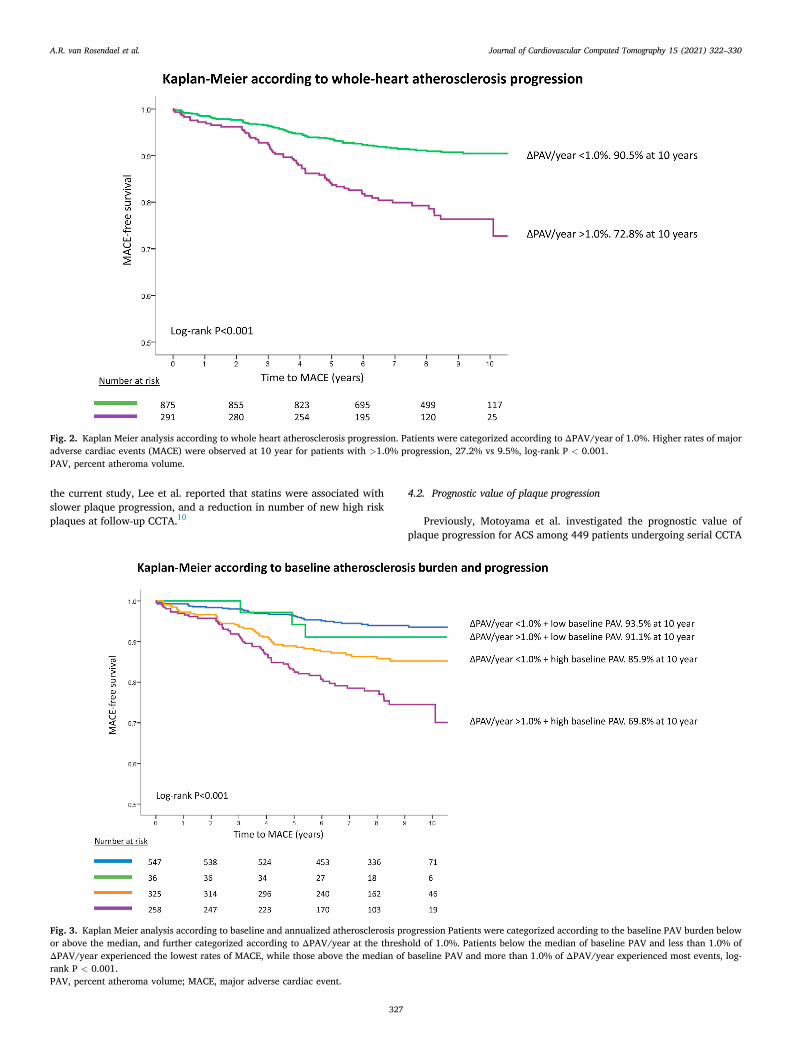
Fig. 2. Kaplan Meier analysis according to whole heart atherosclerosis progression. Patients were categorized according to ΔPAV/year of 1.0%. Higher rates of majoradverse cardiac events (MACE) were observed at 10 year for patients with >1.0% progression, 27.2% vs 9.5%, log-rank P < 0.001.PAV, percent atheroma volume.
A.R. van Rosendael et al. Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
the current study, Lee et al. reported that statins were associated withslower plaque progression, and a reduction in number of new high riskplaques at follow-up CCTA.10
Fig. 3. Kaplan Meier analysis according to baseline and annualized atherosclerosis pror above the median, and further categorized according to ΔPAV/year at the threshΔPAV/year experienced the lowest rates of MACE, while those above the median ofrank P < 0.001.PAV, percent atheroma volume; MACE, major adverse cardiac event.
327
4.2. Prognostic value of plaque progression
Previously, Motoyama et al. investigated the prognostic value ofplaque progression for ACS among 449 patients undergoing serial CCTA
ogression Patients were categorized according to the baseline PAV burden belowold of 1.0%. Patients below the median of baseline PAV and less than 1.0% ofbaseline PAV and more than 1.0% of ΔPAV/year experienced most events, log-

Fig. 4. Absolute and annualized progression rates according to CT-interval tertiles In patients with MACE, ΔPAV is significantly larger with increasing CT-intervaltertile, but ΔPAV/year is not different. In patient not experiencing MACE, both ΔPAV and ΔPAV/year are not significantly different according to the CT-intervaltertiles. Boxes represent 25th and 75th interquartile ranges with the median as line in the middle; whiskers extent to 1.5 times the height of the box; the pointsrepresent outliers. P-values are calculated with the Kruskal-Wallis test.MACE, major adverse cardiac event; PAV, percent atheroma volume.
A.R. van Rosendael et al. Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
during 4 years of follow-up, where progression of plaque was defined asan increase in stenosis severity or increase in remodeling ratio.31 While56 (12.5%) patients experienced plaque progression, they experienced 8of the 9 ACS events in total. In serial IVUS imaging, atherosclerosisprogression has usually been quantified from single coronary arteries(>30 mm in length) and progression reported as annualized change inPAV.32 Nicholls et al. pooled data from 6 clinical trials including 3130patients undergoing serial IVUS and demonstrated an annualized in-crease in PAV of 1.0% in patients experiencing MACE (predominated byrevascularization events).
Data of whole-heart atherosclerosis progression and major events inCCTA are unavailable. Previous serial CCTA studies were too smallwithout long-term follow-up to evaluate this aim.9,11–14 The currentstudy included a patient cohort at low-risk undergoing serial CCTA withwhole-heart quantification of approximately 400 mm of coronary artery(Fig. 1) with 1 to 1 matching of coronary segments of baseline andfollow-up. As expected, baseline plaque burden was significantly higherin those experiencing MACE. In addition, those experiencing MACEdemonstrated an approximately 3-fold higher mangnitude of plaqueprogression and a 1.2-fold higher risk for MACE per standard deviationincrease, independent from baseline plaque burden. These results wereconsistent across multiple clinical subpopulations. In a separate analysisrestricting to patients not experiencing MACE before follow-up imaging,patients with future events showed an annual increase in PAV of 0.93%
328
compared to 0.32% for those without. This threshold of approximately1.0% for future MACE remained unchanged when patients were dividedaccording to different time durations between serial CCTA, indication itsrobustness. Although the number myocardial infarctions was small(inherent with the low-risk population), these findings link the baselineextent of disease and magnitude of progression to a clinical sequele ofworsening cardiovascular outcomes.
In the current study, atheroma progression was dependent on base-line plaque burden. Less than 10% of those starting with less than themedian of baseline PAV had an annualized increase in PAV of >1.0% atfollow-up, and 10 year MACE rates were <10% for those with more andless than 1.0% increase in PAV, but low baseline PAV. These resultsstrongly support the long-term warranty period of a normal or mildlyabnormal baseline CCTA. Examination of the MACE-free survival curvesdemonstrate marked prognostic importance of atheroma progression inthose starting with a baseline plaque burden above the median, indi-cating variety in disease progression in those with established plaque.Both baseline and progression of plaque were independent associates ofMACE in the multivariable analysis together with typical angina. Further,the non-calcified component of plaque progression showed the strongestassociation withMACE. This observation supports prior evidence that thebaseline magnitude of soft/low-attenuation plaque is most vulnerable toplaque destabilization.33 Further, this supports that calcification of pla-que – which may happen with statin use – may be prognostically

A.R. van Rosendael et al. Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
beneficial.34
4.3. Limitations
The current study is of observational design with its inherent limi-tations including selection bias and unmeasured confounding. Theincluded cohort included low-risk patients, with replication of the cur-rent findings needed in patients at higher risk. Most patients were fromEast-asian ethnicity which may limit the generelizibility of the results.Plaque progression was quantified from the entire coronary tree, but it isunclear whether the specific lesion responsible for the future eventdemonstrated a similar pattern of plaque progression. However, giventhe inability of imaging to identify lesions at high likelihood for futurehard events,35,36 per-patient results are currently most applicable. Cor-onary segments with total occlusion were excluded because they couldnot be reliably quantified for plaque volumes. The current study exam-ined the role between atherosclerotic burden and outcomes, but futurestudies should identify patients and plaque phenotypes most likely toprogress in atheroma burden. Finally, most events were re-vascularizations, which are considered a ‘softer’ endpoint.
5. Conclusion
Whole-heart atherosclerosis progression examined by serial CCTA is
329
independently associated with MACE, with a prognostic threshold of1.0% increase in PAV per year.
Funding
This work was supported by the Leading Foreign Research InstituteRecruitment Program through the National Research Foundation (NRF)of Korea funded by the Ministry of Science and ICT (MSIT) (Grant No.2012027176). The study was also funded in part by a generous gift fromthe Dalio Institute of Cardiovascular Imaging (New York, NY) and theMichael Wolk Foundation (New York, NY).
Declaration of competing interest
Dr. James K. Min receives funding from the Dalio Foundation, Na-tional Institutes of Health, and GE Healthcare. Dr. Min serves on thescientific advisory board of Arineta and GE Healthcare, and has an equityinterest in Cleerly. Dr. Habib Samady serves on the medical advisoryboard of Philips and has equity holding in Covanos. The remaining au-thors have no relevant disclosures.
Appendix A
Table 1Baseline and annualized TAVnorm progression according to MACE occurrence
Delta TAVnorm/year, mm3 Baseline TAVnorm, mm3
MACE þ
MACE – P-value Adjusted* OR (95% CI) of ΔTAVnorm/year for MACE, per SDP-interaction
MACE þ
MACE – P-valueOverall
16.84 (5.82,45.02)6.21 (0.27,19.11)
<0.001
1.34 (1.11, 1.60) 127.05 (41.49,245.87)37.41 (0.00,122.08)
<0.001
Time to MACE
Early MACE(<median)16.49 (5.48,42.79)
145.80 (50.33,242.65)
Late MACE(>median)
18.04 (6.75,46.58)
99.73 (37.37,266.60)
Sex
0.764 Men 18.02 (7.81,45.56)
7.49 (1.16,21.51)<0.001
1.48 (1.17, 1.87) 139.71 (62.29,239.41)49.09 (7.54,138.56)
<0.001
Women
16.43 (2.43,45.01)4.87 (0.00,17.47)
<0.001
1.12 (0.82, 1.54) 104.21 (20.01,266.55)26.27 (0.00,101.19)
<0.001
Age
0.039 <65 12.63 (3.81,39.22)
5.31 (0.00,15.52)<0.001
1.56 (1.18, 2.06) 88.75 (22.97,188.34)29.74 (0.00,97.18)
<0.001
�65
20.56 (8.29,53.16)10.19 (0.87,27.14)
<0.001
1.17 (0.92, 1.49) 193.85 (95.67,336.23)63.42 (12.89,198.42)
<0.001
Diabetes
0.512 Yes 18.34 (7.91,52.12)
11.71 (2.52,27.46)0.022
1.22 (0.88, 1.69) 145.32 (63.79,261.37)57.88 (17.75,144.08)
<0.001
No
17.42 (5.34,40.28)6.40 (0.00,16.78)
<0.001
1.37 (1.10, 1.71) 119.84 (31.50,248.19)31.11 (0.00,115.89)
<0.001
Hypertension
0.808 Yes 19.01 (8.31,51.39)
7.84 (1.17,22.24)<0.001
1.30 (1.07, 1.59) 159.07 (64 95,286.11)49.17 (7.94,144.58)
<0.001
No
10.08 (0.98,30.73)4.72 (0.00,15.27)
0.038
1.38 (0.88, 2.17) 86.70 (9.01,188.53)26.18 (0.00,91.34)
0.004
Data provided as median (25th and 75th interquartile range).MACE, major adverse cardiovascular events; TAVnorm, total atheroma volume normalized for vessel length.*adjusted for baseline TAVnorm.

A.R. van Rosendael et al. Journal of Cardiovascular Computed Tomography 15 (2021) 322–330
Appendix B
Table 2Influence of CT time interval on absolute and annualized change in TAVnorm according to MACE
MACE þ P- MACE – P-
330
value
valueCT-interval
Tertile 1 Tertile 2 Tertile 3 Tertile 1 Tertile 2 Tertile 3Absolute change
ΔTAVnorm, mm3 43.25 (7.81,89.21)
62.06 (7.54,192.45)106.79 (48.50,316.28)
0.002
17.19 (1.24,52.63)19.83 (1.21,61.82)
26.16 (0,82.04)
0.078
Annualized change
ΔTAVnorm/year,mm317.55 (3.45,37.69)
18.04 (1.98, 61.30)
20.27 (8.33, 54.84) 0.434 7.52 (0.59, 22.93) 6.14 (0.36, 18.88) 5.38 (0, 16.7) 0.071Data provided as median (25th and 75th interquartile range).MACE, major adverse cardiovascular events; TAVnorm, total atheroma volume normalized for vessel length.
References
1. Min JK, Shaw LJ, Devereux RB, et al. Prognostic value of multidetector coronarycomputed tomographic angiography for prediction of all-cause mortality. J Am CollCardiol. 2007;50:1161–1170.
2. Hoffmann U, Ferencik M, Udelson JE, et al. Prognostic value of noninvasivecardiovascular testing in patients with stable chest pain: insights from the PROMISEtrial (prospective multicenter imaging study for evaluation of chest pain). Circulation.2017;135:2320–2332.
3. van Rosendael AR, Shaw LJ, Xie JX, et al. Superior risk stratification with coronarycomputed tomography angiography using a comprehensive atherosclerotic riskscore. JACC Cardiovasc Imag. 2019 Oct;12(10):1987–1997.
4. O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson Jr SK. Carotid-artery intima and media thickness as a risk factor for myocardial infarction andstroke in older adults. Cardiovascular Health Study Collaborative Research Group.N Engl J Med. 1999;340:14–22.
5. Nicholls SJ, Hsu A, Wolski K, et al. Intravascular ultrasound-derived measures ofcoronary atherosclerotic plaque burden and clinical outcome. J Am Coll Cardiol.2010;55:2399–2407.
6. Lee SE, Sung JM, Rizvi A, et al. Quantification of coronary atherosclerosis in theassessment of coronary artery disease. Circ Cardiovasc Imaging. 2018;11, e007562.
7. Hauser TH, Salastekar N, Schaefer EJ, et al. Effect of targeting inflammation withsalsalate: the TINSAL-CVD randomized clinical trial on progression of coronaryplaque in overweight and obese patients using statins. JAMA cardiology. 2016;1:413–423.
8. Budoff MJ, Ellenberg SS, Lewis CE, et al. Testosterone treatment and coronary arteryplaque volume in older men with low testosterone. Jama. 2017;317:708–716.
9. Shin S, Park HB, Chang HJ, et al. Impact of intensive LDL cholesterol lowering oncoronary artery atherosclerosis progression: a serial CT angiography study. JACCCardiovascular imaging. 2017;10:437–446.
10. Lee SE, Chang HJ, Sung JM, et al. Effects of statins on coronary atheroscleroticplaques: the PARADIGM study. JACC Cardiovascular imaging. 2018;11:1475–1484.
11. Gu H, Gao Y, Hou Z, et al. Prognostic value of coronary atherosclerosis progressionevaluated by coronary CT angiography in patients with stable angina. Eur Radiol.2018;28:1066–1076.
12. Papadopoulou SL, Neefjes LA, Garcia-Garcia HM, et al. Natural history of coronaryatherosclerosis by multislice computed tomography. JACC Cardiovascular imaging.2012;5:S28–S37.
13. Ceponiene I, Nakanishi R, Osawa K, et al. Coronary artery calcium progression isassociated with coronary plaque volume progression: results from a quantitativesemiautomated coronary artery plaque analysis. JACC Cardiovascular imaging. 2018;11:1785–1794.
14. Nakanishi R, Ceponiene I, Osawa K, et al. Plaque progression assessed by a novelsemi-automated quantitative plaque software on coronary computed tomographyangiography between diabetes and non-diabetes patients: a propensity-scorematching study. Atherosclerosis. 2016;255:73–79.
15. Lee SE, Chang HJ, Rizvi A, et al. Rationale and design of the Progression ofAtheRosclerotic PlAque DetermIned by Computed TomoGraphic AngiographyIMaging (PARADIGM) registry: a comprehensive exploration of plaque progressionand its impact on clinical outcomes from a multicenter serial coronary computedtomographic angiography study. Am Heart J. 2016;182:72–79.
16. Abbara S, Blanke P, Maroules CD, et al. SCCT guidelines for the performance andacquisition of coronary computed tomographic angiography: a report of the societyof cardiovascular computed tomography guidelines committee: endorsed by thenorth American society for cardiovascular imaging (nasci). J Cardiovasc ComputTomogr. 2016;10:435–449.
17. Park HB, Lee BK, Shin S, et al. Clinical feasibility of 3D automated coronaryatherosclerotic plaque quantification algorithm on coronary computed tomography
angiography: comparison with intravascular ultrasound. Eur Radiol. 2015;25:3073–3083.
18. Leipsic J, Abbara S, Achenbach S, et al. SCCT guidelines for the interpretation andreporting of coronary CT angiography: a report of the Society of CardiovascularComputed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2014;8:342–358.
19. Zeb I, Li D, Nasir K, et al. Effect of statin treatment on coronary plaque progression - aserial coronary CT angiography study. Atherosclerosis. 2013;231:198–204.
20. van Rosendael AR, Lin FY, Ma X, et al. Percent atheroma volume: optimal variable toreport whole-heart atherosclerotic plaque burden with coronary CTA, thePARADIGM study. J Cardiovasc Comput Tomogr. 2020;14:400–406.
21. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardialinfarction. Eur Heart J. 2012;33:2551–2567.
22. Mendis S, Thygesen K, Kuulasmaa K, et al. World Health Organization definition ofmyocardial infarction: 2008-09 revision. Int J Epidemiol. 2011;40:139–146.
23. Goff Jr DC, Lloyd-Jones DM, Bennett G, et al. ACC/AHA guideline on the assessmentof cardiovascular risk: a report of the American college of cardiology/American heartassociation task force on practice guidelines. Circulation 2014. 2013;129:S49–S73.
24. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or morecorrelated receiver operating characteristic curves: a nonparametric approach.Biometrics. 1988;44:837–845.
25. Schulman-Marcus J, Hartaigh BO, Gransar H, et al. Sex-specific associations betweencoronary artery plaque extent and risk of major adverse cardiovascular events: theCONFIRM long-term registry. JACC Cardiovascular imaging. 2016;9:364–372.
26. Budoff MJ, Young R, Burke G, et al. Ten-year association of coronary artery calciumwith atherosclerotic cardiovascular disease (ASCVD) events: the multi-ethnic studyof atherosclerosis (MESA). Eur Heart J. 2018;39:2401–2408.
27. van Rosendael AR, Maliakal G, Kolli KK, et al. Maximization of the usage of coronaryCTA derived plaque information using a machine learning based algorithm toimprove risk stratification; insights from the CONFIRM registry. J Cardiovasc ComputTomogr. 2018;12:204–209.
28. Boogers MJ, Broersen A, van Velzen JE, et al. Automated quantification of coronaryplaque with computed tomography: comparison with intravascular ultrasound usinga dedicated registration algorithm for fusion-based quantification. Eur Heart J. 2012;33:1007–1016.
29. Kim U, Leipsic JA, Sellers SL, et al. Natural history of diabetic coronaryatherosclerosis by quantitative measurement of serial coronary computedtomographic angiography: results of the PARADIGM study. JACC Cardiovascularimaging. 2018;11:1461–1471.
30. Lee SE, Park HB, Xuan D, et al. Consistency of quantitative analysis of coronarycomputed tomography angiography. J Cardiovasc Comput Tomogr. 2019;13:48–54.
31. Motoyama S, Ito H, Sarai M, et al. Plaque characterization by coronary computedtomography angiography and the likelihood of acute coronary events in mid-termfollow-up. J Am Coll Cardiol. 2015;66:337–346.
32. Nissen SE, Nicholls SJ, Sipahi I, et al. Effect of very high-intensity statin therapy onregression of coronary atherosclerosis: the ASTEROID trial. Jama. 2006;295:1556–1565.
33. Williams MC, Kwiecinski J, Doris M, et al. Low-attenuation noncalcified plaque oncoronary computed tomography angiography predicts myocardial infarction: resultsfrom the multicenter SCOT-heart trial (scottish computed tomography of theHEART). Circulation. 2020;141:1452–1462.
34. van Rosendael AR, Narula J, Lin FY, et al. Association of high-density calcified 1Kplaque with risk of acute coronary syndrome. JAMA Cardiol. 2020 Mar 1;5(3):282–290.
35. Stone GW, Maehara A, Lansky AJ, et al. A prospective natural-history study ofcoronary atherosclerosis. N Engl J Med. 2011;364:226–235.
36. Ferencik M, Mayrhofer T, Bittner DO, et al. Use of high-risk coronary atheroscleroticplaque detection for risk stratification of patients with stable chest pain: a secondaryanalysis of the promise randomized clinical trial. JAMA cardiology. 2018;3:144–152.