Prof james bently endometrial ca generalist
32
Endometrial Cancer care by the gynecologist James Bentley Professor Department of Obstetrics and Gynecology Dalhousie University Halifax NS
-
Upload
basalama-ali -
Category
Education
-
view
171 -
download
0
Transcript of Prof james bently endometrial ca generalist

Endometrial Cancer care by the gynecologist
James BentleyProfessor
Department of Obstetrics and Gynecology Dalhousie University
Halifax NS

Disclosure of Potential for Conflict of Interest
Facilitator’s Name: Dr James Bentley
Grants/research support: Merck, GSK, Guided Therapeutics, Amgen
Speaker’s bureau/honoraria: Merck, GSK
Consulting fees: GSK

Mitigation of Potential for Conflict of Interest
• Although I have been involved with HPV vaccine companies and a new screening modality, I will not be discussing this in my presentation today.

Epidemiology
• Commonest malignancy of the female genital tract– About 5600 cases per year and 1000 deaths per year in Canada– 4th commonest malignancy in Canadian women after breast, lung, colorectal– 9th as cause of death in women– < 25% occur before menopause, peak at 58-60– 5 % in women less than 40– 2.6 % rise in incidence per year
Canadian Cancer Statistics 2014

Endometrial Cancer; Risk factors
Increased RiskObesity 21-50 lbs 3X
Obesity > 50lbs 10X
Nulliparous 2X
Menopausal > 52 yrs 2.4X
Diabetes 2.5X
PCOS
E2 secreting tumor
Unopposed E2 4-7X
Tamoxifen 4X
HNPCC 40-60X
Decreased RiskOvulation
Hormonal Contraception (E2) 0.46X
progestin
Menopause <49
Normal weight
multiparity
smoking

Pathology
• Endometroid ( good prognosis)– Classical risk factors– presents early– good survival
• Others:Uterine serous, clear cell, undifferentiated ( poor prognosis)– classic associations not present– present with advanced disease – poor survival

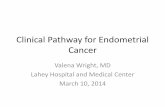
What is endometrial cancer?Endometriod
Grade 1
Grade 2
Grade 3
Uterine papillary serous
Clear Cell

FIGO Staging 2009Stage I Tumor confined to the corpus uteri
IA No or less than 50% myometrial invasion
IB Invasion equal to or greater than 50% of the myometrium
Stage II Tumor invades cervical stroma, but does not extend beyond uterus*
Stage III Local and/or regional spread of the tumor
IIIA Tumor invades the serosa of the corpus and/or adnexae
IIIB Vaginal and/or parametrial involvement
IIIC Metastases to pelvic and/or para-aortic lymph nodes
IIIC1 Positive pelvic nodes
IIIC2 Positive para-aortic nodes +/- positive pelvic nodes
Stage IV Tumor invades bladder and/or bowel mucosa and or distant mets
IVA Tumor invades bladder and/or bowel mucosa
IVB Distant mets, including intra abdominal and/or inguinal lymph nodes
* Endocervical glandular involvement only is considered as Stage I


Post menopausal bleeding: evaluation• Recommendations?• Pap test (if not done recently)• Endometrial Biopsy
• What if can’t do office Bx?• US +/- hysteroscopy D&C

Challenges: preoperative biopsy
• How accurate is the biopsy?– Can underestimate the stage in up to 20%– Challenges of AEH, up to 40% will have
endometrial cancer on final biopsy– Should be able to identify Grade 3 and pap
serous/ clear cell carcinomas

Management post diagnosis
• Consider pathology review• Grade 1:
– Pre-op assesment• CXR
– Hysterectomy BSO• Grade 2, 3, Uterine Papillary Serous Carcinoma, Clear
Cell• Unfit for Surgery• Obvious metastatic/ unresectable disease
– REFER TO Gynecologic Oncologist for management

Not a generalist case!

Why stage?
• Extent of disease• Determine adjuvant disease• Prognostication• Compare results• ? Therapeutic benefit

Grade 1: myometrial evaluation
• MRI can evaluate depth of invasion and hence identify women who may benefit from lymphadenectomy
• Grade 1 with deep myoinvasion, lymph node involvement ~10%
• Can be assessed at time of OR either by gross inspection or frozen section

Surgical approach
• Just because FIGO describes Hyst BSO and nodes does not mean that all cases need “full staging”
• Role of laparoscopy• Nodes for who• Overall nodal risk for Grade 1 disease is ~ 3%
for pelvic and 2 % for paraortic nodes• No evidence that lymphadenectomy in proves
outcome

Kwon et al.2009
• Ontario data• 316 women with lymphadenectomy 1996-2000• Mean age 62.2• 12% +ve nodes• 23% adjuvant Rx• Risk of death increased with:
– Invasion >50%– Cervical stromal invasion– Age >60 yrs– Grade 3

Kwon et al

Role of Adjuvant Rx

GOG 99TAH BSO most had nodesall stage 1B 1C 2A 2Brandomized to WPXRT vs observation reassessed LIR and HIRrisk factors: increasing age, grade 2-3, LVI, outer third MIreduced local recurrence 9% to 0.5%; distant 6.4% to 5.3%overall slight survival advantage to RT (86% to 92%) but not stat. significantLIR survival similar in both arms, but in HIR somewhat lower overall death rate

Portec 1TAH BSO (no nodes done) grade 1 stage 1C, grade 2 1B 1C, grade 3 stage 1Brandomized to WPXRT or observationlocoregional recurrence-4% vs 14%(73% vagina--70 % salvaged)distant mets 8% vs 7%overall survival no diffgrade 1+2 >50%, grade 3= 10% risk of locoregionalrecurrencegrade 3-- 14% risk of distant mets, and 16% risk of deathlocoregional relapse 3 fold higher if age was over 60CRITICISM low risk disease over-represented (30% 1B gr2)

What is High risk disease?
• Grade 3• Stage 1B (2009)• Stage 2

ASTEC/EN5
intermediate and high risk ECrandomized to EBRT vs observationabout half of the observation pts got brachyno survival advantage of EBRTlocoregional recurrence 7% vs 3.6%
lower than PORTEC likely b/c of brachy

PORTEC-2 march 2010
• 427 pts stage 1 or IIA endometriod ca• Routine Lymphadenectomy not done• Eligible if:
– >60 yrs old– Stage 1C grade 1 or 2, 1B grade 3, stage 2A any age
• Randomised to brachy vs. WPT• 3 rec’s vs 4• No benefit of WPT

Who needs radiation?
• No improved survival• Better pelvic control• Less vaginal recurrences• BUT….• Vaginal recurrences usually salvaged
• ? In combination with chemo Rx
• Stage 2 (beware grade 3!)

Role of chemotherapy
• GOG 122• Stage III and IV with minimal extrauterine
disease• WART vs AP• AP had improved survival• Recurrences in pelvis and abdomen

Which Chemo Regieme
• No great evidence yet for carbo taxol• BUT..• Hogberg
– European trial in abstract form:– 382 patients with stage I, II, IIIA or IIIC and adverse
features • Deep MI, clear cell, serous, anaplastic, nondiploid
– Chemo one of :AP, TAP, TP vs. XRT– Improved PFI at 5 yrs with chemo rx (7%)– No difference between chemo arms

Practical approach: SurgeryGrade 1, clinical stage 1 Hysterectomy BSO and 1 set
of washingsGrade 2, 3 clinical stage 1 Hysterectomy BSO PLND,
consider PA nodesStage 2 clinically Consider Radical
HysterectomyClinically advanced disease Individualise, but TAHBSO
and debulkClear cell, serous Hysterectomy BSO, PLND,
PAND and staging

Practical approach: Adjuvant Rx
Stage 1 No high risk features NFTStage 1 High risk features* Study, Brachy; chemo and
brachy for 1C gr 3Stage 2 WPRStage 3 c Study, combined therapyClear cell, serous Study, chemo XrtStage 4B chemotherapy
Adverse features: grade 3, deep MI, cervical stromal involvement, age > 60

Follow- Up
• No distinct benefit of follow-up in low risk disease• BUT provides psychological benefit• Commonest sites of recurrence vagina, pelvis and chest• No role for Pap smear, CT scans• Hx and Exam
– q 3 months for first year– q 4 months second year– q 6 months third year +/- CXR– Annually to 5 years

Conclusion
• Endometrial Cancer is common and will be increasing in your practice
• Carefully evaluate the patient• Work closely with the gynecologic oncologists
in your center re referral practices etc

SOGC/GOC Guidelines April 2013
Epidemiology and Investigation for Suspected Endometrial CancerThe Role of Adjuvant Therapy in Endometrial CancerThe Role of Surgery in Endometrial Cancer
http://sogc.org/clinical-practice-guidelines/