
Process used by the banks for tissue processing and ...
18
2 Recruitment Control cases: both Edinburgh and Oxford retrieve brain tissue from Coronial (Oxford) and Procurators Fiscal (Edinburgh) instructed PMs. The relevant authority gives permission to approach relatives following the death of an individual. If relatives give permission the brain is taken for research purposes, and clinical data is sought retrospectively from GP records. Neurological disorders: all 4 banks are built around existing clinical cohorts, in line with researchers needs. For example all MND and Dementia with Lewy bodies cases are part of well-defined clinical cohorts known to local clinicians with detailed clinical information. Likewise dementia cases come through the BDR network, this network having an associated clinical database. All 4 banks still receive donation requests from outwith clinical cohorts, such as “my mum had dementia, can I donate her brain”. 2 of the banks only accept these donations in exceptional circumstances (Edinburgh and Newcastle). Oxford and KCL are going to review their policy, although all 4 banks were mindful of the importance of public relations. However, there was general agreement that, in absence of good clinicopathological correlation, the tissue was likely to be of limited value to a research group. Key development point: all 4 banks to increasingly restrict retrieval to cases with good clinical information (preferably linked to well-defined clinical cohorts) Sampling protocols Sampling protocols are disease specific but there is a clear ethos between the banks supporting a standardized core set of tissue regions available from all cases, the core samples reflecting BDR recommended core samples. All banks sample both fresh brain tissue and formalin-fixed brain tissue. A core set of samples has been agreed between all 4 banks, and is in operation (figure 1). 1- Core small samples, particularly suited to DNA extraction, in small tubes a. Frontal (BA46) b. Temporal (BA21) c. Parietal (BA5/7) d. Occipital (BA19) e. cerebellum 2- Core frozen samples a. Frontal (BA46) b. Cingulate (BA32/24) c. Anterior hippocampus d. Striatum e. Superior temporal (BA41/42) f. Posterior hippocampus
Transcript of Process used by the banks for tissue processing and ...

2
Recruitment Control cases: both Edinburgh and Oxford retrieve brain tissue from Coronial (Oxford) and Procurators Fiscal (Edinburgh) instructed PMs. The relevant authority gives permission to approach relatives following the death of an individual. If relatives give permission the brain is taken for research purposes, and clinical data is sought retrospectively from GP records. Neurological disorders: all 4 banks are built around existing clinical cohorts, in line with researchers needs. For example all MND and Dementia with Lewy bodies cases are part of well-defined clinical cohorts known to local clinicians with detailed clinical information. Likewise dementia cases come through the BDR network, this network having an associated clinical database. All 4 banks still receive donation requests from outwith clinical cohorts, such as “my mum had dementia, can I donate her brain”. 2 of the banks only accept these donations in exceptional circumstances (Edinburgh and Newcastle). Oxford and KCL are going to review their policy, although all 4 banks were mindful of the importance of public relations. However, there was general agreement that, in absence of good clinicopathological correlation, the tissue was likely to be of limited value to a research group. Key development point: all 4 banks to increasingly restrict retrieval to cases with good clinical information (preferably linked to well-defined clinical cohorts) Sampling protocols Sampling protocols are disease specific but there is a clear ethos between the banks supporting a standardized core set of tissue regions available from all cases, the core samples reflecting BDR recommended core samples. All banks sample both fresh brain tissue and formalin-fixed brain tissue. A core set of samples has been agreed between all 4 banks, and is in operation (figure 1).
1- Core small samples, particularly suited to DNA extraction, in small tubes a. Frontal (BA46) b. Temporal (BA21) c. Parietal (BA5/7) d. Occipital (BA19) e. cerebellum
2- Core frozen samples a. Frontal (BA46) b. Cingulate (BA32/24) c. Anterior hippocampus d. Striatum e. Superior temporal (BA41/42) f. Posterior hippocampus

3
g. Thalamus h. Posterior parietal lobule (BA39) i. Primary visual cortex (BA17) j. Cerebellar cortex k. Midbrain l. Pons m. Medulla n. Spinal cord (cervical, thoracic, lumbar)
Discuss with UK Brain Bank Network colleagues to resolve issue of which side to sample
3- Core diagnostic samples (FFPE) taken from cerebral/cerebellar hemispheres
a. Frontal (BA46) b. Cingulate (BA32/24) c. Superior temporal (BA41/42) d. Amygdala e. Anterior hippocampus f. Posterior hippocampus g. Striatum h. Thalamus i. Posterior parietal lobule (BA39) j. Primary visual cortex (BA17) k. Cerebellar cortex l. Midbrain m. Pons n. Medulla o. Spinal cord (cervical, thoracic, lumbar)
4- Immunohistochemical on core blocks for staging; tau (AT8), β-amyloid (4G8), α-synuclein (novocastra), TDP43 (TARDBP Protein Tech Group)
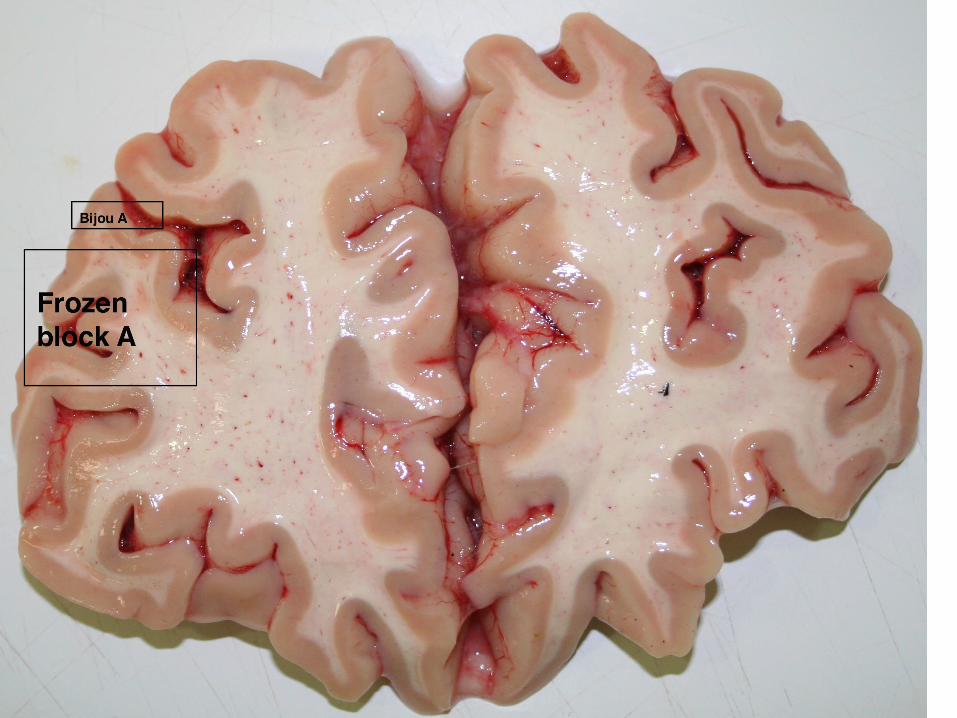
Newcastle, Oxford and KCL: the whole brain is bisected with one cerebral hemisphere being sampled fresh (always left in Newcastle, alternating in Oxford and KCL). The fresh hemisphere is cut in coronal sections and all coronal slices including core frozen samples are then frozen using either nitrogen vapour or brass plates, and then placed in -80C freezer. All banks are considering moving to nitrogen vapour for freezing for preservation of cytoarchitecture, anticipating future single cell technologies. The opposite hemisphere is fixed in 10% neutral buffered formalin for between 4-6 weeks. Coronal sections are cut and the core diagnostic blocks are taken. There is no evidence to suggest that a variation between 4-6 weeks results in any meaningful differences to tissue quality for research purposes. Edinburgh: the whole brain is cut fresh due to the consent available for the clinical cohorts being studied (organs are returned to the body for burial and no whole brains are retained). The core frozen blocks are sampled from the left hemisphere, and frozen using nitrogen vapour before being placed in -80C freezer. The core diagnostic blocks are sampled from the right hemisphere.

4
These blocks are placed in 10% buffered formalin for at least 1 week and then processed. Again, there is no scientific evidence to suggest the shorter fixation period has any detrimental effect on standardized scientific protocols. The shorter period in fixative purely reflects the smaller volume of the tissue being fixed. All the banks have more extensive sampling protocols for both frozen and FFPE tissues, the protocols often reflecting the needs of local research groups or specific requests received from national or international research groups. However, it was felt that the core samples would satisfy a majority of tissue research requests, and this will continue to be audited and reported by all banks. Tissue processing protocols For all banks brain tissue is fixed in 10% neutral buffered formalin. Oxford, King’s College and Newcastle fix whole hemispheres for approximately 4-6 weeks prior to sampling and processing, whereas Edinburgh fixes tissues in formalin for only 3-4 days as the tissue samples are considerably smaller and require much shorter fixation (2x2cm cubed tissue samples as opposed to a whole hemisphere). Samples are then processed on a 3-day cycle. This is a standard cycle passing through alcohol (dehydration) and chemicals for removal of lipid. The protocols used for tissue freezing all currently use brass/ copper plates and liquid nitrogen for snap freezing. Nitrogen vapour is being trialed to compare cytoarchitecture preservation between techniques (Oxford and Edinburgh). Diagnostic protocols: All banks use standard diagnostic protocols when assessing brains. Diagnosis is based on assessment of the 13 core FFPE blocks, using standard grading criteria outlined below. Each block is stained with haematoxylin and eosin (H&E) and luxol fast blue/ cresyl violet (LFB/CV). Immunohistochemistry is assessed using same antibody clones in each banks: tau (AT8); β-amyloid (4G8); α-synuclein (Novocastra); TDP43 (TARDBP Protein Tech Group). For Alzheimer’s disease- NIA-AA criteria (Montine TJ et al., 2012, Acta Neuropathol 123:1-11), Neurofibrillary tangle Braak stages (Braak H et al., 2006, Acta Neuropathol 112:389-404; Alafuzoff I et al., 2008, Brain Pathol 18:484-496) For Lewy body disease- McKeith criteria for Lewy body disease (McKeith IG et al., 2005, Neurology 65:1863-1872) including modification by Leverenz (Leverenz JB et al., 2008, Brain Pathol18:220-224) For FTD cases- Frontotemporal lobar degeneration (FTLD) is assessed according to: McKenzie IRA et al 2010, Acta Neuropathol 119:1-4; in case of FTLD with TDP-43 pathology according to: McKenzie IRA et al 2011, Acta Neuropathol 122:111-113

5
For white matter pathology- White matter pallor and small vessel disease in white and deep gray matter is scored as described in: Smallwood A et al., 2012, Neuropathol Appl Neurobiol 38:337-343 Tissue quality parameters: Tissue pH and RNA quality as assessed by RIN values are used as tissue quality parameters across all the MRC Brain banks. pH is assessed using a standardized hand-held pH meter (the same meter is used by each bank) at the time of post mortem. pH values are taken from the frontal regions. RIN values are determined in-house in Edinburgh, Newcastle and Oxford, and using an internal collaboration in London. An Agilent Bioanalyser system is used to determine this value. All banks use previously frozen (at -80C) brain tissue to assess RIN value, and prospectively only cerebellar tissue will be used. Summary The MRC-funded brain banks have demonstrated significant moves towards harmonization of tissue sampling, processing and characterization such that researchers can be re-assured of consistency across the banks with regards to neuroanatomical definitions of regions, tissue quality, and neuropathological diagnosis (table 1). In particular all banks have a core sampling strategy in line with BDR recommendations, but have also developed additional samples based on researcher feedback. New approaches to tissue freezing are being trialed to investigate which is the best technique for cytoarchitectural preservation. Early results suggest liquid nitrogen vapour results in superior cytoarchitectural preservation compared with slow-freezing between pre-cooled brass plates.

Edinburgh King’s College
London
Newcastle Oxford Reasons for
differences, if any
Tissue dissection:
fresh
Whole brain cut fresh
One hemi cut fresh
One hemi cut fresh
One hemi cut fresh
Edinburgh has no consent for
retaining whole brain and all
sampling must be done at time
of the post mortem
examination
Core 5 regions for
bijou Core 14
regions frozen
Core 5 regions for
bijou Core 14
regions frozen
Core 5 regions for
bijou Core 14
regions frozen
Core 5 regions for
bijou Core 14
regions frozen
Spinal cord all levels + dorsal
root ganglia
Spinal cord all levels + dorsal
root ganglia
Spinal cord all levels + dorsal
root ganglia
Spinal cord all levels + dorsal
root ganglia
Freezing
method
Liquid nitrogen
and nitrogen vapour for
cytoarchitecture
Freezing
method? Brass / copper
plates and liquid
nitrogen
Freezing method?
Brass / copper plates and liquid
nitrogen
Liquid nitrogen
and nitrogen vapour for
cytoarchitecture

Edinburgh King’s College
London
Newcastle Oxford Reasons for
differences, if
any
Tissue fixation 3-4 days in 10%
neutral buffered formalin in
cassettes
4-6 weeks in
10% neutral buffered formalin
(whole hemisphere –
spinal cord)
4-6 weeks in 10%
neutral buffered formalin (whole
hemisphere – spinal cord)
4-6 weeks in
10% neutral buffered formalin
(whole hemisphere –
spinal cord)
Edinburgh has
no consent for retaining whole
brain, and the small tissue
samples require far less fixation
time
Tissue processing
3 day process in automated
processor (ethanol, xylene,
paraffin wax)
3 day process in automated
processor (ethanol, xylene,
paraffin wax)
3 day process in automated
processor (ethanol, xylene,
paraffin wax)
3 day process in automated
processor (ethanol, xylene,
paraffin wax)
Tissue
dissection:
FFPE
15 core blocks 15 core blocks 15 core blocks 15 core blocks
Staining Core diagnostic
set on all core FFPE blocks
Core diagnostic
set on all core FFPE blocks
Core diagnostic
set on all core FFPE blocks
Core diagnostic
set on all core FFPE blocks
Diagnostic protocols
Standard protocols:
AD: NIA-AA criteria, tangle
Standard protocols:
AD: NIA-AA criteria, tangle
Standard protocols:
AD: NIA-AA criteria, tangle
Standard protocols:
AD: NIA-AA criteria, tangle

Braak stages. Lewy body
disease: McKeith
criteria. FTD cases:
McKenzie White matter
pathology: as described in
Smallwood
Braak stages. Lewy body
disease: McKeith
criteria. FTD cases:
McKenzie White matter
pathology: as described in
Smallwood
Braak stages. Lewy body
disease: McKeith
criteria. FTD cases:
McKenzie White matter
pathology: as described in
Smallwood
Braak stages. Lewy body
disease: McKeith
criteria. FTD cases:
McKenzie White matter
pathology: as de scribed in
Smallwood
Edinburgh King’s College
London
Newcastle Oxford Reasons for
differences, if any
Tissue quality
control
Tissue pH –
frontal
Tissue pH –
frontal
Tissue pH –
frontal
Tissue pH –
frontal
RIN value -
cerebellum
RIN value -
cerebellum
RIN value -
cerebellum
RIN value -
cerebellum







Annex I
1
Milestone 3 July 2014
Information should be available on the MRC website about how data is linked to GP / clinical records (and adjudicated where necessary), anonymised and stored securely, and the process for securing this information. How the summary diagnosis report is put together from these records, e.g. by a review group, should also be described.
The information provided in this report is based on feedback from Edinburgh, Newcastle, King’s College, London and Oxford.
Sources of Clinical data
All 4 brain banks have different clinical cohorts, but strive to collect core data to allow easy comparisons between cohorts for researchers. Following a brain donation all MRC banks record clinical information obtained from the donors medical records.
Consent for access to these medical records is now routinely sought by all banks with the consent for retention and use of the brain and spinal cord tissue. Currently banks record relevant information from a range of sources, including hospital (incorporating specific clinical trial/cohort records) and GP records depending on availability and diagnostic group. There is ongoing discussion between the banks regarding the possibility of identifying a template for recording a more extensive set of core clinical variables (such as blood pressure, blood glucose tests etc) which could be recorded across all the brain banks but given the very different conditions to be studied this is far from straightforward.
Approaches to core data
Currently, standard information recorded across the banks includes:
• age of onset • symptoms at presentation • course of disease • additional medical history • relevant medications • final illness/cause of death • age at death
Much of this information is recorded as free text/vignettes as it is difficult to standardise the form in which it is recorded due to the wide range of possible variables. In addition banks record other clinical information relevant to the disease group in which they specialise (such as specific symptoms associated with speech, visual hallucinations etc). Banks use the clinical information together with the neuropathology report to reach the final diagnosis, which will categorise the tissue for future research use, and later to select suitable cases for tissue requests. It is also available in an anonymised form to researchers where requested. Access to data by researchers is controlled by the identified Data Manager (Brain Bank Manager) at each bank who will have responsibility for information governance as part of the ethics and Caldicott approvals.

2
Data anonymisation and storage
All data is stored electronically and password protected. Information on registered donors, detailing clinical and pathological diagnosis, post mortem details of fixed and frozen tissue and demographic data such as age, sex and source of donation is stored. Personal information is not available to researchers, but anonymised, general details (age and sex of patient, autopsy details etc) are made available with other appropriate biodata on request. There is also some information on any assessments carried out in cohort studies. Some of the banks record genetic information for a sub-set of cases. Access to additional clinical data is reserved to specific individuals (NBTR Directors and Manager) and this is held on separate encrypted database which is held on separate University server. Patient medical records are held in purpose built locked stores within a secure room which has limited access to study personnel who all have local NHS Trust approval.
All Brain Banks subscribe to the MRC policy on data sharing and preservation, and to the local University policies/legal requirements on Freedom of Information. All Brain Banks enforce the Data Protection Act (1998) (http://www.opsi.gov.uk/Acts/Acts1998).
Local Caldicott Guardians are appointed to oversee data governance and can be consulted if there is a query regarding confidentiality. All Brain Banks subscribe to the MRC policy on data sharing and preservation, and to the local University policies/legal requirements on Freedom of Information. All Brain Banks enforce the Data Protection Act (1998) (http://www.opsi.gov.uk/Acts/Acts1998).
In accordance with HTA best practice guidelines details of all tissue requests and the tissue supplied is also recorded on our database. Information is secured and backed up by local IT departments.
Future directions
The banks are working together to develop a standard ‘core dataset’ capturing data commonly requested by researchers. Much of this is general medical data unrelated to the specific neurological condition (weight, blood pressure, blood glucose etc), and we are actively looking at linking with large scale medical datasets across the UK. In addition we are looking at linking imaging, genetic and other disease-specific data with the existing neuropathological databases. However, this approach may be limited by the resources available, and we are actively looking at the most cost effective ways to link multiple datasources.

3
Milestone 4 November 2014
As outlined in the Board Assessment Template 10/07/2013, the 4 MRC funded brain banks are requested to provide Milestone updates. This response is in relation to the November 2014 Milestone updates.
The Board have requested the following:
1. An update on harmonisation since November 2013 should be provided. This should specifically consider any gaps identified at the first review point.
2. The MRC banks submitted an agreed disposal strategy to the July 2013 NMHB
meeting. The banks are asked to report on what has been delivered against this strategy, and whether the strategy has been adjusted to take account of Network-wide policies on disposal and donation. The disposal strategy should inform and refine what is collected as well as what is disposed of.
Harmonisation As outlined in the submission dated November 2013 the 4 banks have tried to harmonise sampling protocols, tissue processing protocols, and a standardized approach to diagnostic procedures where possible. Differences that were identified at the initial assessment of procedures included paraffin block sampling (FFPE) and the development of a summary report for each case reported in a brain bank. All 4 banks are committed to the increased focus of activity in relation to well-defined clinical cohorts, rather than cases with limited pre-mortem characterization. Control cases, which are a principle focus of both Edinburgh and Oxford, are by their nature, exceptions. These are typically cases of sudden unexpected death, and clinical information is retrieved retrospectively through accessing GP records, and any other relevant medical notes. However, where activity is based around known neurological disease (Newcastle- LBD, vascular dementia, dementia; Oxford- MND, dementia, autism; Edinburgh- intracerebral haemorrhage, MND, CJD, dementia, normal cognitive ageing; KCL- fAD, MND, FTD, dementia) recruitment is from well-studied clinical cohorts. We continue to audit this activity across all 4 banks and can provide end of year data showing activity. We have adopted the core sampling protocols for frozen tissues and small samples for DNA assessment. We suggest cerebellum be used for standard DNA assessments, and frontal tissue be used for RIN values, correlating with pH studies (from frontal tissues). A core sample of paraffin blocks has been agreed and incorporated in to the blocksheet of each of the banks. There has been discussion between the banks in relation to freezing protocols. Oxford and Edinburgh use N2 vapour while Newcastle uses copper plates. Both provide excellent results in relation to cytoarchitecture quality and DNA/RNA. We do not propose to impose one approach over the other as both provide similar quality tissues for researchers. This will continue to form an on going audit.
A summary template report has been developed which outlines the key clinical and pathological features. This is a single page A4 summary, and all pathological diagnoses
4
are supported by existing consensus diagnostic criteria. These diagnostic criteria will be represented on the MRC brain bank network database.
We are still strongly supportive of a move towards a more integrated IT system, hopefully aligned with the UK dementia platform. This remains an issue of funding and IT integration which is beyond the current remit of the brain banks, but we remain fully committed to integration in any IT developments.
Disposal Strategy
We developed a tissue disposal strategy in line with HTA requirements and donor wishes, which has previously been submitted to the Board (Policy on Tissue Disposal for Brain Banks; June 2013).
All 4 banks have adopted and have implemented this strategy. Cases with priority for retention are highlighted, and there is discussion between banks before tissue disposal should another bank have a specific collection which includes the tissue being considered for disposal (for example Newcastle are contacted by other banks before any LBD cases are disposed of). The physical disposal of tissues complies with MRC, HTA and local NHS policies, and data disposal complies with MRC and local policies on research data.
All 4 banks have ongoing audit and review of tissues requested by researchers, and use this to inform sampling protocols. All 4 banks are developing a SOP in relation to their local audit and tissue disposal protocols, the SOP being informed by audit of researchers’ needs. These will be provided in the end of year reports from each bank.

















