Principles of Flap Design in Dental...
8
Volume 23, Number 6 June 2012 EDITOR ARUN K. GARG, DMD; EDITOR IN CHIEF EDITORIAL ADVISORS EDITOR EMERITUS: MORTON L. PEREL, DDS, MSCD RENZO CASSELINI, MDT, PROFESSOR OF RESTORATIVE DENTISTRY, LOMA LINDA UNIVERSITY, LOMA LINDA, CA LEON CHEN, DMD, MS, PRIVATE PRACTICE IN PERIODONTOLOGY, LAS VEGAS, NV SCOTT D. GANZ, DMD, PRIVATE PRACTICE OF PROSTHODONTICS, MAXILLOFACIAL PROS- THETICS AND IMPLANT DENTISTRY, FORT LEE, NJ ZHIMON JACOBSON, DMD, MSD, CLINICAL PROFESSOR, DEPARTMENT OF RESTORATIVE SCIENCES/BIOMATERIALS, BOSTON UNIVERSITY JIM KIM, DDS, MPH, MS, PRIVATE PRACTICE OF PERIODONTICS, DIAMOND BAR, CA ROBERT E. MARX, DDS, PROFESSOR OF SURGERY, CHIEF, ORAL & MAXILLOFACIAL SURGERY PETER MOY, DMD, PRIVATE PRACTICE, WEST COAST ORAL AND MAXILLOFACIAL SURGERY CENTER AND CENTER FOR OSSEOINTEGRATION, LOS ANGELES, CA MYRON NEVINS, DDS, ASSOCIATE PROFESSOR OF PERIODONTOLOGY, SCHOOL OF DENTAL MEDICINE, HARVARD UNIVERSITY, BOSTON, MA H. THOMAS TEMPLE, MD, PROFESSOR OF ORTHOPEDIC SURGERY AND DIRECTOR OF UNIVER- SITY OF MIAMI TISSUE BANK, UNIVERSITY OF MIAMI SCHOOL OF MEDICINE MIAMI, FL • The images conTained wiThin This issue are from dr. Jasim AL-JUBOORI’S PRACTICE. NOW AVAILABLE ON-LINE! Go to www.ahcmedia.com/online.html for access. Wounds and Suturing 44 Inside This Issue THE OFFICIAL PUBLICATION OF THE AMERICAN DENTAL IMPLANT ASSOCIATION Principles of Flap Design in Dental Implantology By Mohammed JA, BDS, MSc, SHAIFULIZAN ABR, DDS, MD, Hasan FD, BDS, MSc T HERE IS NO SINGLE FLAP DESIGN THAT SERVES AS THE OPTIMAL APPROACH FOR EVERY implant surgery, 1 and as the need for cosmetic procedures with minimally invasive techniques increases, so, too, does the variability in flap design. In other words, there is no single technique that is suited to every surgical situation, and the skilled surgeon must be thoughtful and creative in selecting every incision since the manner in which that incision is designed, executed, and sutured will have an enormous impact on implant success rates and overall aesthetic outcome. The site of implant placement, whether it is in the aesthetic zone or hidden pos- teriorly, also has an impact on the flap design. Another factor to consider is the width of the ridge in which the implant is placed. Some ridges are wide enough to place an implant with minimal tissue reflection, while other ridges are narrow and require wide flap reflection for better visualization and ridge width determi- nation. Further, narrow ridges sometimes need bone augmentation and guided bone regeneration membranes, which necessitate planning for wide flap design to cover the bone graft and the membrane. This article discusses the principles of flap design in dental implantology in an effort to summarize techniques to aid practitioners with optimal procedure selection. Principles Principle 1: New scalpel blades and sharp peri-osteal elevators are essential for making incisions and elevating flaps to protect the viability of the mucosa. The incision should be made clearly in order to avoid retracting, and elevation requires flawless use of a dedicated peri-osteal elevator. 2 Principle 2: Full visibility of the operative site is essential. It has been sug- gested that the incision be made longer than the amount required to expose the operative site. This offers greater visibil- ity of the bone. It should be pointed out that long incisions heal as rapidly as short ones. 2 (See Figures 1,2)
Transcript of Principles of Flap Design in Dental...

Volume 23, Number 6 June 2012
EDITOR Arun K. GArG, DMD; EDitor in ChiEf
EDitoriAL ADViSorS EDitor EMErituS: Morton L. PErEL, DDS, MSCD
rEnzo CASSELini, MDt, ProfESSor of rEStorAtiVE DEntiStry, LoMA LinDA uniVErSity, LoMA LinDA, CA
LEon ChEn, DMD, MS, PriVAtE PrACtiCE in PErioDontoLoGy, LAS VEGAS, nV
SCott D. GAnz, DMD, PriVAtE PrACtiCE of ProSthoDontiCS, MAxiLLofACiAL ProS-thEtiCS AnD iMPLAnt DEntiStry, fort LEE, nJ
zhiMon JACobSon, DMD, MSD, CLiniCAL ProfESSor, DEPArtMEnt of rEStorAtiVE SCiEnCES/bioMAtEriALS, boSton uniVErSity
JiM KiM, DDS, MPh, MS, PriVAtE PrACtiCE of PErioDontiCS, DiAMonD bAr, CA
robErt E. MArx, DDS, ProfESSor of SurGEry, ChiEf, orAL & MAxiLLofACiAL SurGEry
PEtEr Moy, DMD, PriVAtE PrACtiCE, WESt CoASt orAL AnD MAxiLLofACiAL SurGEry CEntEr AnD CEntEr for oSSEointEGrAtion, LoS AnGELES, CA
Myron nEVinS, DDS, ASSoCiAtE ProfESSor of PErioDontoLoGy, SChooL of DEntAL MEDiCinE, hArVArD uniVErSity, boSton, MA
h. thoMAS tEMPLE, MD, ProfESSor of orthoPEDiC SurGEry AnD DirECtor of uniVEr-Sity of MiAMi tiSSuE bAnK, uniVErSity of MiAMi SChooL of MEDiCinE MiAMi, fL
• The images conTained wiThin This issue are from dr. Jasim AL-Juboori’S PrACtiCE.
NOW AVAILABLE ON-LINE!Go to www.ahcmedia.com/online.html for access.
Wounds and Suturing 44
Inside This Issue
thE offiCiAL PubLiCAtion of thE AMEriCAn DEntAL iMPLAnt ASSoCiAtion
Principles of Flap Design in Dental Implantology
By Mohammed JA, BDS, MSc, SHAIFULIZAN ABR, DDS, MD, Hasan FD, BDS, MSc
There is no single flap design that serves as the optimal approach for every implant surgery,1 and as the need for cosmetic procedures with minimally
invasive techniques increases, so, too, does the variability in flap design. In other words, there is no single technique that is suited to every surgical situation, and the skilled surgeon must be thoughtful and creative in selecting every incision since the manner in which that incision is designed, executed, and sutured will have an enormous impact on implant success rates and overall aesthetic outcome. The site of implant placement, whether it is in the aesthetic zone or hidden pos-teriorly, also has an impact on the flap design. Another factor to consider is the width of the ridge in which the implant is placed. Some ridges are wide enough to place an implant with minimal tissue reflection, while other ridges are narrow and require wide flap reflection for better visualization and ridge width determi-nation. Further, narrow ridges sometimes need bone augmentation and guided bone regeneration membranes, which necessitate planning for wide flap design to cover the bone graft and the membrane. This article discusses the principles of flap design in dental implantology in an effort to summarize techniques to aid practitioners with optimal procedure selection.
PrinciplesPrinciple 1: New scalpel blades and sharp peri-osteal elevators are essential
for making incisions and elevating flaps to protect the viability of the mucosa. The incision should be made clearly in order to avoid retracting, and elevation requires flawless use of a dedicated peri-osteal elevator.2
Principle 2: Full visibility of the operative site is essential. It has been sug-gested that the incision be made longer than the amount required to expose the operative site. This offers greater visibil-ity of the bone. It should be pointed out that long incisions heal as rapidly as short ones.2 (See Figures 1,2 )

Dental Implantology Update™ June 2012
42
Dental Implantology Update™ (ISSN 1062-0346) is published monthly by AHC Media, a division of Thompson Media Group LLC, 3525 Piedmont Road N.E., Building Six, Suite 400, Atlanta, GA 30305. Tele-phone: (404) 262-7436. Periodicals Postage Paid at At-lanta, GA 30304 and at additional mailing offices. The statement of ownership will appear in the November issue.
POSTMASTER: Send address changes to Dental Implantology Update™, P O Box 105109, Atlanta, GA 30348
AHC Media, in affiliation with the American Dental Implant Association, offers continuing dental education to subscribers. Each issue of Dental Implantology Up-date™ qualifies for 1.5 continuing education units.
Customer Service: (800) 688-2421. Fax: (800) 284-3291. Hours of operation: 8:30 a.m.-6 p.m. Monday-Thursday; 8:30 a.m.-4:30 p.m. Friday, EST.
E-mail: [email protected]. World Wide Web: www.ahcmedia.com.
Subscription rates: U.S., $599 per year. Add $17.95 for shipping & handling. Students, $320 per year. To re-ceive student/resident rate, order must be accompanied by name of affiliated institution, date of term, and the signature of program/residency coordinator on institu-tion letterhead. Orders will be billed at the regular rate until proof of student status is received. Outside U.S., add $30 per year, total prepaid in U.S. funds. Discounts are available for group subscriptions, multiple copies, site-licenses or electronic distribution. For pricing infor-mation, call Tria Kreutzer at 404-262-5482. Missing is-sues will be fulfilled by customer service free of charge when contacted within one month of the missing issue date. Back issues, when available, are $100 each. For 18 continuing education units, add $96 per year.
Opinions expressed are not necessarily those of this publication. Mention of products or services does not constitute endorsement. Clinical, legal, tax, and other comments are offered for general guidance only; profes-sional counsel should be sought for specific situations.
Copyright © 2012 by AHC Media. Dental Implan-tology Update™ is a trademark of AHC Media. The trademark Dental Implantology Update™ is used herein
under license. All rights reserved. Reproduction, distribu-tion, or translation of this newsletter in any form or incor-poration into any information retrieval system is strictly prohibited without express written permission. For reprint permission, please contact AHC Media Address: P.O. Box 105109, Atlanta, GA 30348. Telephone: (800) 688-2421.Managing Editor: Leslie Hamlin, (404)
262-5416, ([email protected]).Executive Editor: Shelly Morrow Mark, (352)
351-2587, ([email protected]). Senior Vice President/Group Publisher: Donald R. John-ston, (404) 262-5439, ([email protected]).
Figure 1: The incision is made longer than the amount required in order to adequate-ly expose the operative site
Principle 3: The periosteum serves as the major vascular supply to the bone; therefore, at most, only a mini-mal amount, if any, of the periosteum should be removed.3
Principle 4: If papillae are involved, they should not be bisected but elevated in total.2
Principle 5: If the implant proce-dure is to involve the alveolar ridge, the incision should be made at the crest within the linea alba.2 (See Figure 3 )
Principle 6: If tension-relieving in-cisions are required to avoid stretching or tearing the tissues, these incisions should be made obliquely to ensure broad-based flaps.2
Principle 7: Flexibility in position-ing the surgical guide4 must be provided.
Principle 8: Allow for proper iden-tification of important anatomical landmarks: The location and path of the blood vessels and nerves should be evaluated, protected, and preserved during the duration of the surgical pro-cedure. Beyond general knowledge of these structures, acknowledging their precise locations is crucial in specific areas (for example, the mental foram-ina and incisal canal4). This is an essen-tional part of preoperative planning.
Principle 9: Identification of the contours of the adjacent teeth, as well as the concavities or protrusions on the
surface of the bone,5 is essential and will facilitate implant placement.
Principle 10: It is also essential to ensure that all wounds have clean edges, which will facilitate closure and optimize healing by primary intention.3
(See Figure 4)Principle 11: Permitting the raising
of a full mucoperiosteal flap ensures that it has a good vascular supply. In-sufficient blood supply compromises the survival of the unreflected tissue, which can lead to necrosis as well as the potential for a deleterious aesthetic result. The choice of flap design should allow for maintenance of optimal and sufficient blood supply to all parts of the mobilized tissues as well as the soft tissues in the surrounding area.3
Principle 12: Flap blood perfusion must be maintained up to the point at which the ratio of length to the width of the parallel pedicle flap equals 2:1. The length/width ratio requirement usually favors a slight trapezoidal shape of the flap.3
Principle 13: The tissue flap must be kept moist at all times to help avoid shrinkage and dehydration of the tissue. With prolonged duration of the surgical procedure, the involved tissues are at risk of drying out, especially when a high de-gree of hemostasis has been achieved.3
Principle 14: The goal is always to minimize scarring and avoid vestibular flattening.6
Figure 2: Long incisions heal as rapidly as short ones

June 2012 Dental Implantology Update™
43Principle 15: It is imperative to
provide for closure away from the sub-merged fixture installation or augmen-tation site.6
Principle 16: As with any operative technique, the minimization of postsur-gical bacterial contamination improves outcome and decreases morbidity.4
Principle 17: Minimal tension dur-ing reapproximation and after suturing is important to avoid impairment of the circulation at the wound margins. Shrinkage of the reflected tissue with wound dehiscence will ultimately lead to increased scar formation.4
Principle 18: Tissue trauma, such as stretching, tearing, or distortion, should be avoided through appropriate and careful reflection and manipulation of tissue flap. Excessive trauma from re-traction may cause increased swelling and delay healing.6 (See Figure 5 )
Principle 19: The integrity of the periosteum should be maintained throughout. The periosteum will serve as a barrier against the connective tissue cells so that these cells cannot invade the bone cavity during the healing pro-cess and prevent a complete bone fill.3
Principle 20: Providers should avoid oblique relieving incisions over prominent root surfaces because reces-sion may result if there is an underlying bony dehiscence.
Principle 21: In cases of reduced quantity of keratinized tissue, it is beneficial to position the crestal inci-sion toward the palatal aspect, the area where more keratinized tissue as it ex-tends onto the palatal mucosa.
Principle 22: When graft materials or membranes are used, it is sensible to place relieving incisions at least at one tooth, proximal to the area of augmen-tation.
Principle 23: If doubt exists as to the need to expose anatomical struc-tures, such as the incisive nerve, or if augmentation techniques may be in-dicated, then the wider flap design in-cluding papillae is mandatory .
Principle 24: For larger implant sites that are 8 mm and larger, choose a
Figure 3: The incision should be made at the crest within the linea alba
Figure 5: Appropriate and careful reflection and manipulation of the tissue flap is imperative
Figure 4: Clean edges are essential to fa-cilitate primary closure and optimize heal-ing by primary intention
Figure 6: Use proper suture material, with an atraumatic needle There should be minimal tension during reapproximation

Dental Implantology Update™ June 2012
44mesiodistal crestal incision of 5-6 mm to allow for nonreflection of papillary tissue. For sites that are less than or equal to 7 mm mesiodistally, there is a need to reflect the papillae.
Principle 25: Atraumatic wound handling avoids tension and pressure to the flap that may lead to impaired blood flow and interrupted lymph drainage.1
Principle 26: Controlling intraoper-ative bleeding (adequate hemostasis) is necessary to avoid the possibility of he-matoma formation, another causative factor in delayed wound healing.1
Principle 27: Practitioners should strive to eliminate the formation of any dead space in which fluids might col-lect after wound closure1.
Principle 28: The use of proper suture materials with an atraumatic needle must be practiced.1 Further, practitioners must have exceptional surgical knotting and suture selection techniques. (See Figure 6 )
Principle 29: Avoid any local or ex-ternal pressure on the wound during the healing period.1 Educate patients about the importance of postoperative care.
Principle 30: In cases of non-sub-merged implants, the flap edge should be repositioned upward to prevent overgrowth of the gingiva above the healing cap or cover screw postopera-tively; the provider can achieve this by making the connective tissue (perios-teum) face the healing cap rather than the epithelium.7,8 n
REFERNCES 1. Askary ASE. Reconstructive Aes-
thetic Implant Surgery: Blackwell Munksgaard 2003:66-90.
2. Cranin AN. Implant surgery: The management of soft tissues. J Oral Implantol. 2002;28:230-237.
3. Velvert P, Peters IC, Peters AO. Soft tissue management: Flap design, incision, tissue elevation, and tis-sue retraction. Endodontic Topics. 2005;11:78-97.
4. SclarAG.Guidlinesforflaplesssurgery. American Association of
be the “father of modern dentistry,” a French physician who practiced den-tistry similar to what we know today from the late 17th to mid 18th centuries, the man also touted as the individual who first created dental prostheses, can be credited with early methods of den-tal surgical technique. This review ar-ticle covers types of wounds and wound healing, the healing process itself, and basic surgical knotting techniques.
Surgical Wounds and Wound Healing
Suturing and surgical knotting is an important component of the surgeon’s skill set. Dental implant practitioners require specific, high-quality technique in this area, given the importance of the aesthetic outcome in the evolution of more advanced implant procedures. In addition to the aesthetic outcome, proper wound healing is essential to re-duce the risk of postoperative infection, or worse, treatment failure.
Types of Wounds and Wound Healing
There are four types of surgical wounds based on risk of infection dur-ing and after surgery: clean, clean-con-taminated, contaminated, and dirty and infected.2,3 Any surgical process in the mouth almost ensures at least a clean-contaminated or contaminated wound secondary to the capacity of infection of oral flora. Some oral wounds are con-sidered dirty and infected at the outset and require a high degree of attention, such as an oral abscess, for example. Wound healing in oral mucoperiosteal tissues after surgical wound healing is unique relative to other types of surgi-cal wounds. Flap design plays a large role in this process. Further, dental im-plant surgery also conveys the prospect of approximating a vascular soft-tissue surface with an avascular root surface. As mentioned in the previous article featured in this issue of Dental Im-plantology Update, flap design should be trapezoidal in shape, with a wider portion at the base of the flap to pro-vide adequate blood supply to healing
Oral and Maxillofacial Surgeons. 2007;65:20-32.
5. Kleinheinz J, Buchter A, Kruse-Losler B, et al. Incision design in implant dentistry based on vascu-larization of the mucosa. Clin Oral Implants Res. 2005;16:518-523.
6. Hunt WB, Sandifer JB, Assad DA, GherME.Effectofflapdesignonhealing and osseointegration of den-tal implants. International Journal of Periodontics & Restorative Den-tistry 1996;16:583-593.
7. Al-Juboori MJ, bin Abdulrahaman S,SubramaniamR,TawfiqOF.Lessmorbiditywithflaplessimplant.Dent Implantol Update. 2012;23:25-30.
8. Heydenrijk K, Raghoebar GM, Batenburg RH, Stegenga BA. Com-parison of labial and crestal inci-sions for the 1-stage placement of IMZ implants: A pilot study. J Oral Maxillofac Surg. 2000;58:1119-23; discussion 1123-1124.
Wounds and Suturing in Dental Implant Surgery
By Arun Garg, DMD
In 2006, french and italian scientists reported in Nature that Stone Age
humans used dental drills made of flint some 9,000 years ago.1 The Neolithic dentists drilled teeth to cure toothaches. Modern analysis suggests that the drill-ing was “surprisingly effective” in re-moving rotting tooth material.1 What’s more, and somewhat surprising in light of the advancements made in modern medicine and dentistry, including but not limited to surgical sterility, antibiot-ic therapy, and novel imagining modali-ties like X-ray and computed tomogra-phy (CT) scanning, early dental patients survived the drilling and went on to use their teeth after the procedures; this was assessed by looking at the surfaces of the teeth that had been drilled. Perhaps Pierre Fauchard, the man considered to
June 2012 Dental Implantology Update™
45
tissues, as well as flexibility to help ensure non-tension primary wound closure.4 Passive positioning of soft tissue reduces tears on flap edges dur-ing the suturing process, which limits retraction; this can be best achieved with properly placed vertical releas-ing incisions and appropriate flap re-flection.5
Types of wound healing are de-scribed by rates and pattern of heal-ing, and are generally divided into three categories: healing by first in-tention, healing by second intention,
and healing by third intention, also known as delayed primary closure.
Healing by first intention is a four-stage process involving normal wound-healing processes with mini-mal edema, the absence of local infec-tion, no serious discharge or separation of wound edges, and minimal scar-ring. The four stages of wound healing are described below. This should abso-lutely be the goal in many dental im-plant surgical procedures (specifically, first-stage dental implants, root cov-erage, bone grafting, and membranes
used for tissue regeneration), where appropriate. Healing by second inten-tion involves a more complicated or prolonged healing in which infection, trauma, lost tissue, or poor approxi-mation of wound edges has occurred. An example of a procedure wherein healing by secondary intention occurs is gingevectomy. Healing by third in-tention involves bringing two surfaces of granulation tissue together because of contaminated, traumatic wounds with high risk of infection3,6 (extrac-tion sockets without flap or advanced soft-tissue graft). Generally, there is significant scarring in this type of wound healing.
Wound healing follows a step-by-step process that includes hemostasis, inflammation, and repair — known formally as hemostasis, inflamma-tion, proliferation or granulation, and remodeling or maturation. When skin is punctured, the body’s immune system reacts. Polymorphonucleo-cytes (PMNs), platelets, and plasma proteins enter the wound, causing lo-cal vasoconstriction. Platelets at the wound help to form a stable clot to seal punctured vessels, and local acti-vating factors lead to aggregation and clumping. Adenosine diphosphate from surrounding tissues causes ad-hesion with local collagen, and plate-let production of thrombin leads to the production of fibrin from fibrino-gen. Platelet-derived growth factor and transforming growth factor beta (TGF-beta) attract PMNs, which lead to the inflammation stage.
Inflammation, classically appear-ing as swelling and warmth, is a fac-tor associated with this second stage of healing. Macrophages replace PMNs after approximately 48 hours to continue the inflammation process, removing wound debris and releasing more growth factors.
Approximately 72 hours after tis-sue puncture, the proliferation stage begins, wherein fibroblasts are drawn to the site by inflammatory cell growth factors, which synthesize collagen.
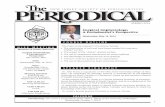
Figure 1: The Square Knot
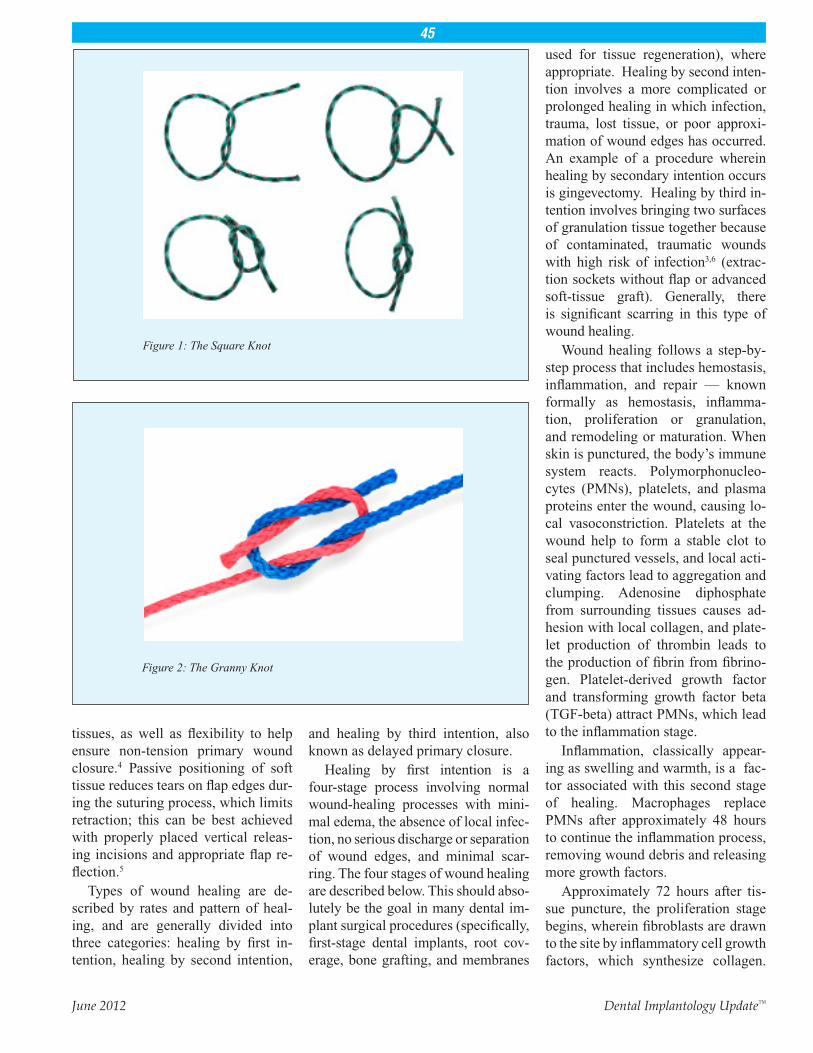
Figure 2: The Granny Knot

Dental Implantology Update™ June 2012
46
Clinical signs of granulation include granular red tissue at the base of the wound, dermal and subdermal tissue replacement, and wound contraction. In this stage, fibroblasts release collagen, which forms a framework for increased dermal growth. New collagen is sup-ported by angiogenesis as new capillar-ies appear. Further, keratinocytes start epithelialization of the wound, causing further contraction and the formation of a layered wound covering.
The final stage of wound healing, known as remodeling, involves the continued work of collagen as it re-structures itself over weeks to repair the skin. Wound tensile strength in-creases as dermal cells are remodeled by fibroblasts over the course of many months to years.
Periodontal healing patterns can involve the downgrowth of epithelial cells into the wound, resulting in a long junctional epithelium. Proliferation of connective tissue can cause connec-tive tissue adhesion and root resorp-tion. Bone cell predominance can also cause root resorption, ankylosis, or both. Ingress of the periodontal liga-ment and perivascular cells from bone
can regenerate periodontium with new cementum.7
Factors Affecting Wound Healing
Wound healing, described above, is a physiologic process and, as such, is af-fected by a variety of physiologic vari-ables and determinants. Age, weight, nutritional status, fluid status, the pres-ence or absence of other chronic under-lying diseases, the status of a patient’s immune status, and history of chemo-therapy and radiation exposure all affect a body’s ability to heal. Certainly, loss of tissue elasticity, slower metabolisms, and poor circulation seen in elderly in-dividuals provide unique challenges to the implant surgeon, as do vitamin and protein deficiencies or tobacco expo-sure history, diabetes, and hypertension (which are also more prevalent in older populations). In this setting, and in light of the fact that aging populations are more likely to seek implant procedures, dental implant surgeons must know about tissue mechanics, factors that in-fluence wound healing, and strategies to employ when wound healing is thwart-ed or prolonged.
The most essential aspect to insure proper wound healing is practicing a sterile and aseptic surgical technique. Attention to the length and direction of the incision, as well as dissection tech-niques, tissue handling, hemostasis, tissue irrigation, debridement, closure material selection, elimination of dead space, closure tension, and postsurgi-cal wound stressors are also impera-tive, and some of these were described in this issue’s previous article on flap design.
Suture MaterialsA primary goal of dental surgery is
to establish nontension closure of pri-mary wounds for soft-tissue flaps so that wounds heal properly. Nontension primary closure is essential to implant success (for the implant and for any site requiring a bone graft), but several flap designs can facilitate surgical wound healing with minimal complications. In order to obtain optimal positioning and securing of surgical flaps to provide ideal conditions for wound healing, practitioners must understand three ar-eas of suturing: types of sutures, sutur-ing techniques, and surgical knotting techniques.8,9
A large study of the effect of suture materials on wound healing revealed no significant difference between su-ture materials and suture techniques.10 There are two basic categories of su-tures — nonresorbable and resorb-able, and each has advantages and disadvantages. Nonresorbable suture materials are naturally elastic, which helps secure knotting. Conversely, re-sorbable sutures tend to reduce postop-erative inflammation. Suture size refers to the diameter of the suture material, measured from 1-0 to 10-0, and grow-ing increasingly smaller in diameter and lower in tensile strength. As size decreases, cost of suturing materials tends to increase.2 Dental surgeons tend to use the 3-0 and 4-0 diameter suture materials most commonly; the 5-0 and 6-0 are reserved for delicate muco-gingival surgery. The principle rule of
Figure 3: The Surgeon’s Knot

June 2012 Dental Implantology Update™
47thumb in suture selection is to choose the smallest diameter suture that will hold the wound tissue together during healing. Smaller diameter fibers allow the provider to complete more sutures without decreasing blood supply to the tissue.
Nonresorbable sutures are made of silk or polyester (monofilament and polytetrafluoroethylene). While knot tying is facilitated with the use of non-resorbable materials, there does tend to be a localizing process that draws fluids and bacteria to the wound site. Braided strands of polyester fibers can be coated with a lubricant to facilitate passage through tissue, although this certainly diminishes the capacity of the knot to stay tied.
Resorbable sutures have become more popular because they tend to reduce postoperative inflammation, and patients prefer them because they do not require a return visit for su-ture removal. Natural resorbable su-tures include plain gut (lost 24 hours after insertion into the oral cavity) and chromic gut (treated with chro-mium salt to resist oral enzymes for 7-10 days). These materials are con-traindicated in patients with severe gastroesophageal reflux disease and bulimia with purging, as breakdown will occur much faster. Synthetic re-sorbables do exist and are made from a naturally occurring polymer of the body: polyglycolic acid; these tend to resorb naturally within 21-28 days. Poliglecaprone 25 sutures have a 90-day resorption rate, with high tensile strength, but many patients consider them to be stiff and abrasive.11
Suturing TechniquesMaximizing healing requires the
proper choice of surgical technique, and different clinical scenarios war-rant different technique application. Sutures are typically placed distal to the last tooth, in interproximal spaces, and should be inserted first through the most mobile tissue flap with a circular needle. Suture needles must be grasped by needle drivers (never
a practitioner’s direct grasp), and ten-sion should be limited to secure the flap without reducing blood flow to the tissue being closed. Blanching must be avoided. The clinician should grasp the needle in the center, avoiding the needle and suture juncture; needle entry should be made at right angles to the tissues. Periosteum-to-perios-teum and tissue-to-tissue techniques should be employed when multiple levels are being sutured.11 Swelling, as described above, occurs within the first 48 hours postoperatively, and, as such, sutures should not be placed closer than 2-3 mm from the edge of the flap to prevent tearing. The most common suturing techniques are in-terrupted, sling, mattress, continuous inter-locking, and anchor sutures.
Continuous sutures: These su-tures are used for securing flaps more than several centimeters long and for repositioning surgical flaps apically or coronally; they can be used for joining two or more inter-dental papillae of the same flap. The advantages of this suture are that it minimizes multiple knots, employs teeth-to-anchor flaps, and enables independent placement and tension of buccal, lingual, and palatal flaps. Disadvantages include loose flaps or untied sutures. In Fig-ure 8, modification of this technique, specifically for highly restricted ar-eas and for coapting tissue and re-sembling the simple loop interrupted suture technique with second needle penetration through the outer surface of the lingual flap. The knot is tied at the buccal aspect of the flap after the needle passes back under the contact point.
Mattress suture: These sutures are used for increased security and control of the flap to enable a more precise placement of the flap. This technique is often used with perios-teal stabilization. It is used to resist muscle pull, to adapt flaps to bone, as a regenerative barrier, implant or tooth, and to avert surgical flap edges. It also facilitates papillary stabiliza-tion and placement.
Periosteal suturing: These su-tures are used to penetrate the peri-odontal/peri-implant tissues and periosteum to the bone, and then ro-tate the needle back to the original direction through the periosteum and keratinized tissues
Simple loop modification to the interrupted sutures: These sutures are used to approximate and coapt surgical flaps. There is no placement of suture material between the tissue flaps.
Single interrupted sling sutures: These sutures are used for a flap el-evated on one side of the arch or for positioning facial and lingual flaps at different levels. It involves only two papillae to adapt the flap around the tooth or implant, started on the mesial side of the site, with the needle encir-cling the tooth before being passed under the distal point.
Sling suture about single tooth: This suture is used principally for a flap raised on one side of the tooth, and involves only one or two adjacent papillae — most often in flaps posi-tioned coronally and laterally, requir-ing one of the interrupted sutures, anchored about the adjacent tooth or slung around the tooth, for holding both papillae. The buccal or lingual is reflected, and the clinician passes a 3/8 circle reverse cutting needle under the distal contact point of the most distal interdental papilla, then the in-ner side of the elevated surgical flap 3 mm from the papilla tip. The clinician then passes the needle under the next contact point in a mesial direction be-fore piercing the inner surface of the elevated surgical flap 3 mm from the tip of the interdental papilla.
There are other suture techniques available to clinicians, including modifications of standard techniques described above.
Knot tying is used in a multitude of disciplines outside of healthcare, and the principles are the same even if the scales of purpose are vastly dif-ferent. Surgical knotting techniques

Dental Implantology Update™ June 2012
48
To reproduce any part of this newsletter for promotional purposes, please contact:Stephen VancePhone: (800) 688-2421, ext. 5511Fax: (800) 284-3291Email: [email protected]
To obtain information and pricing on group discounts, multiple copies, site-licenses, or electronic distribution please contact:Tria KreutzerPhone: (800) 688-2421, ext. 5482 Fax: (800) 284-3291Email: [email protected]: AHC Media 3525 Piedmont Road, Bldg. 6, Ste. 400, Atlanta, GA 30305 USA
To reproduce any part of AHC newsletters for educational purposes, please contact:The Copyright Clearance Center for permissionEmail: [email protected]: www.copyright.comPhone: (978) 750-8400Fax: (978) 646-8600Address: Copyright Clearance Center 222 Rosewood Drive, Danvers, MA 01923 USA
are also a relevant skill for the implant surgeon to master. There are more than 1,400 available knots, but only a few of these are used in implant dentistry. Knots should have the following: firm-ness, simplicity, smallness, avoidance of instrument damage to the suture or surrounding tissues, adequate but not too much tension, approximation of tis-sues, traction, flatness, and avoidance of extra throws (wherein bacteria can settle). The most important knots for the dental implant practitioner include the square knot (Figure 1), the slipknot, and the surgeon’s knot (Figure 3).
The square knot involves two over-hand knots completed in opposite di-rections. First, the clinician makes a loop over the jaws of the needle holder, grabs the end of the suture, and pulls the knot to the flap. Then, the clinician makes a second overhand knot, plac-ing a loop under the jaws of the needle holder again. The suture is caught, and the two ends of the suture are pulled together.
The slipknot is similar to the square knot, except two single overhand knots are made in the same direction. Further tightening of the knot is possible before it is locked by an overhand knot made in the opposite direction.
The surgeon’s knot is the most com-monly used in implant surgery, and it is generally used with braided sutur-ing material and a standard mattress technique. It consists of a modified square knot made up of two overhand knots completed in opposite direc-tions. The first is a double overhand knot; the second is a single. Doubling the first overhand knot can prevent knot loosening. n
References1. Coppa A, Bondioli L, Cucina A,
et al. Palaeontology: Early Neo-lithic tradition of dentistry. Nature. 2006;440:755-756.
2. O’Neal RB, Alleyn CD. Suture materialsandtechniques.Current Opinoins in Periodontology. 1997;4:89-95.
3. Dunn DL, editor. Ethicon Wound Closure Manual. Sommerville, NJ. 2005. Johnson&Johnson. Accessed online on 5/1/2012 at http://www.surgery.uthscsa.edu/pediatric/train-ing/woundclosuremanual.pdf.
4. Heller JW, Heller RL, Cook G, D’Orazio R, Rutkowski J. Soft tissue managementtechniquesforimplantdentistry: A clinical guide. Journal of Oral Implantology. 2000;26(2):91-103.
5. Moore RL, Hill M. Suturing tech-niquesforperiodontalplasticsurgery. Periodontology 2000. 1996;11:103-111.
6. Mercandetti M, Cohen AJ. Wound healing and repair. EMedicine.Updated August 3, 2011. Available online at http://emedicine.medscape.com/article/1298129-overview.
7. Rose LF, Mealey BL. Periodontics: Medicine, suergery and implants. St. Louis. Mosby, 2004.
8. Hurzeler MB, Weng D. Functional and esthetic outcome enhancement of periodontal surgery by applica-
tion of plastic surgery principles. International Journal of Periodon-tics and Restorative Dentistry. 1999;19(1):36-43.
9. Silverstein LH, Kurtzman GM. A review of dental suturing for optimal soft-tissue management. Compendium of Continuing Educa-tion in Dentistry. 2005;26(3):163-166, 169-170.
10. Gabrielli F, Potenza C, Puddu P, et al. Suture materials and other fac-tors associated with tissue reactiv-ity, infection, and wound dehiscence among plastic surgery outpatients. Plastic and Reconstructive Surgery. 2001;107(1):38-45.
11. Silverstein LH. Principles of Dental suturing: The complete guide to sur-gical closure. Majwah, New Jersey. 1999. Montage Media Corporation.