
Principle of Cancer Pain Management - Bangkok Hospital · PDF fileCancer Pain Management and...
58
Cancer Pain Management and Thai Clinical Practice Guideline Laksamee Chanvej, M.D., FRCAT, GradCertHlth (Palliative Care) 20 th June 2014 Wattanosoth Cancer Hospital, Bangkok
Transcript of Principle of Cancer Pain Management - Bangkok Hospital · PDF fileCancer Pain Management and...

Cancer Pain Management and Thai Clinical Practice Guideline
Laksamee Chanvej, M.D., FRCAT, GradCertHlth (Palliative Care)
20th June 2014
Wattanosoth Cancer Hospital, Bangkok

Topic to be Covered
• Cancer patient problem
• Causes of pain in cancer
• World Health Organization: analgesic ladder
• Pharmacological and non pharmacological pain concepts
• Specific cancer pain: • bone pain, neuropathic pain, tumor induced headache,
refractory pain
• End of life pain
• Clinical practice guideline for cancer pain (version TASP 2013)

Cancer Pain Patient
• 91.2 in 100,000 population in Thailand died from cancer
• Palliative care and supportive care need: a good evidence based report in 2010
Public health Statistic 2010, Thailand MOPH
Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 2010;363(8):733–42.

Cancer Pain Patient
• Advance oncologic treatment: cancer survivors
• An overall range 28–87%
• > 1/3 patients have moderately to severe pain • 33% in curative treatment patient
• 59% in patients on anticancer treatment
• 64% in metastatic, advanced or terminal phase
Van den Beuken-van Everdingen MHJ, et al. Ann Oncol 2007; 18: 1437–1449 Kanavos P. The rising burden of cancer in the developing world. Ann Oncol 2006;17:15–23..

Concept of Pain Assessment
• Initial and ongoing assessment
• Proper tools and self report
• Quality of pain and choice of pain therapy • Somatic, visceral, neuropathic
• Baseline, breakthrough pain (19-95%)
• Psychosocial distress assessment • Total pain concepts
Haugen DF, et al. Pain 2010; 149(3) Davies AN, et al. Eur J Pain 2009;13
Mehta A, Chan LS. J Hospice Palliative Care Nurs. 2008 Fallon M, Hanks G, Cherny N. Principles of control of cancer pain. BMJ. 2006

Causes of Pain in Cancer
• Cancer related pain • Due to invasion, metastasis, specific (NP, CIBP, malignant
bowel obstruction, tumor induced headache)
• Pain in cancer survivors: persistent post-surgical, radiation, chemotherapy, hormonal therapy, chronic graft vs host disease
Paice JA. PAIN 152 (2011) S84–S89

Causes of Pain in Cancer
• Pain other than cancer related pain • Acute procedural pain: diagnostic, biopsy, intervention
• Iatrogenic pain due to surgery, chemotherapy, radiation therapy, osteonecrosis of the jaws (ONJs), skin lesion, neuropathy, mucositis
• Co-morbidity: diabetic neuropathy, FM, PHN,

General Principles of Pain Management • Inform patient: onset pain, communication about
suffering, pain management
• Patient as an active role
• Clarify misconception of opioids
• Non pharmacological management

Recommendation of Analgesics
• By the clock: prevent onset of pain • Bioavailability, half life and duration of action
• Oral route: first choice, easy for self managed
• Prescribe for breakthrough pain episode: rescue dose (immediate release formed)
• Opioid analgesics are mainstay

• Ladder analgesics since 1986
WHO Strategy

Mild Pain Treatment
• Nonopioid analgesics: paracetamol, NSAIDs use in any stage
• no evidence to support superior safety or efficacy of one NSAID over any other
• Use only ONE NSAIDs/coxibs at a time
• Improve analgesia when add to WHO step III opioid
• Side effects: NSAIDs gastrointestinal bleeding, platelet dysfunction and renal failure
• COXIBs: risk of thrombotic cardiovascular adverse reactions
McNicol E, Strassels S, Gouds L et al. NSAIDs or paracetamol, alone or combined with opioids, for cancer pain. Cochrane Database of Systematic Reviews 2005, Issue 2
Nabal M, Librada S, Redondo S et al. The role of paracetamol and nonsteroidal anti-inflammatory drugs in addition to WHO Step III opioids in the control of pain in advanced cancer. A systematic review of the literature. Palliat Med 2012; 26(4): 305–312.

Mild to Moderate Pain Treatment
• Codeine, tramadol or low dose strong opioid
• Tramadol for neuropathic pain
• ( beneficially of tramadol combined with paracetamol but beware of over-dosage)
• Beware of serotonin syndrome (using TCA,SSRI,SNRI), ceiling effect
• Dose 200-400 mg/d
• Side effects: nausea, vomiting, vertigo, anorexia and asthenia

Moderate to Severe Pain Treatment • Strong opioids are the mainstay
• Morphine, fentanyl, methadone, oxycodone, buprenorphine
• Oral morphine if urgent IV (oral:IV 3:1)
• Transdermal (TD) fentanyl, buprenorphine • When pain is stable
• Unable to swallow, poor tolerance of morphine, poor compliance
• Renal dialysis patient

Ideal Opioid Regimen for Background Pain and BTP
BTP
BTP
0
10
Pain score
24 Time
To minimized pain pathway sensitization

Moderate to Severe Pain Treatment • Methadone for expert use
• Interindividual differences in plasma half life and duration
• Opioid switching to improve pain relief and drug tolerability

Opioid that should be Avoided
• Pethidine • N-demethylated to norpethidine which is toxic metabolites
(12-16 hr) • may cause seizures, mood alterations, and confusion • Naloxone does not reverse this effect

Opioid Side Effects
• Constipation
• Nausea/vomiting
• Urinary retention
• Pruritus
• Central nervous system (CNS) toxicity • drowsiness, cognitive impairment, confusion,
hallucinations, myoclonic jerks ,opioid-induced hyperalgesia/allodynia

Strategic Management of Opioid Side Effects • Reduce dose of opioid
• Add coanalgesic
• Continued use antiemetics, routine use of laxatives, transquilizers
• Alternative approach • Nerve block, radiation therapy
• Switching to another opioid/route

Conversion Morphine and Fentanyl
Ripamonti CI. Annals of Oncology 23 (Supplement 10): x294–x301, 2012

Conversion Morphine and Methadone
Ripamonti CI. Annals of Oncology 23 (Supplement 10): x294–x301, 2012

Non-pharmacological Treatment
• Complementary therapies • Massage and aromatherapy
• Music therapy
• Acupuncture
• Transcutaneous electrical nerve stimulation (TENS)
• Others: reflexology, reiki, hypnotherapy
• Specific conditions: CIBP, refractory pain

Interventional Pain Management
• Specific conditions • Cementoplasty in metastatic bone cancer
• Anesthetic intervention • E.g. neuraxial block, neurolysis

Specific Pain in Cancer Patient
• Cancer induced bone pain (CIBP)
• Neuropathic pain in cancer
• Tumor induced headache
• Refractory pain
• Pain at the end of life

Cancer Induced Bone Pain
• Metastatic bone pain is most common
• Morbidity due to: fracture, hypercalcemia, metastatic spinal cord compression (MSCC)
• Background pain, breakthrough pain
• Analgesic drugs: rescue medication
Coleman RE 2006 Oct 15;12(20 Pt 2):6243s-6249s

Metastatic Spinal Cord Compression (MSCC) • Pain in 95% of patients: local, radicular, preceding
days, weeks
• Early diagnosis and prompt therapy
• Imaging (MRI) then dexamethasone 16 mg/d and taper over 2 weeks
• Radiotherapy is the first line in majority of patients (35% disappeared pain, 58% pain relief)
• Surgery in selected group
Annals of Oncology 23 (Supplement 7): vii139–vii154, 2012

Painful Bone Metastasis Management • Radiotherapy: pain relief 60-80% of patients,
recurrent required RT related to single =20% multiple fractions =8%
• Radioisotopes for bone pain in breast and lung cancer: able to control for 1-6 months
• Targeted therapy: Bisphophonates, denosumab
Roqu M, Cochrane Review). In: The Cochrane Syst Rev, 2011; CD003347

Neuropathic Pain
• Incidence study in cancer pain patients (Spain) 33% had NP, 69% tumor related, 43% treatment related (79% chemotherapy)
• Opioid + adjuvant drugs: tricyclic antidepressants, gabapentin
• Steroid in nerve compression
Garcia de Paredes ML, et al. Ann Oncol 2011; 22: 924–930.

Tumor Induced Headache
• Brain metastasis or brain tumor itself
• Increase intracranial pressure
• Surgery, radiotherapy, chemotherapy
• Steroids taper in 2 weeks
• Others: anticonvulsants, analgesics

Malignant Bowel Obstruction
• Mechanical or functional
• Radiologic assessment: indicative of surgery
• Antiemetic: cyclizine, low dose haloperidol dexamethasone, octreotide
• Analgesics : antispasmodic (hyoscine N butyl bromide)
• Opioids, anticholinergic
• Palliative intervention: rectal stent
Dolan EA. Am J Hosp Palliat Care 2011; 28(8)

Refractory Pain
• Difficult to manage by oral/TD
• Intervention pain management
• Switching from oral to epidural or continuous subcutaneous
• Intrathecal delivery in patient wih expectancy > 3 months • 20-40% epidural, 10% intrathecal of systemic dose
• Neurolytic block: celiac plexus lasts 3-6 months

Pain at the End of Life
• Hours or months before death
• 70% alternate route of opioid
• Some are refractory
• Total suffering assessment with multidisciplinary approach
• Other symptoms: dyspnea, agitation, delirium and anxiety
• Sedation: benzodiazepines, neuroleptics
Chapman L, Ellershaw J. Medicine 2011; 39: 674-677. Sykes N. End of life issues. Eur J Can 2008; 44: 1157-1162 Pantilat SZ. Med Clin N Am 2008: 92 : 349–370

Development Pathway of Clinical Practice Guideline ( Thai-CPG) • Content synthesis
• Review of related data from electronic databases • RCT, International recommendation
• Peer reviewing by expert panels • Pain specialist
• Related Royal Colleges of Physician
• Public hearing
• Finalizing content in the end of 2013
http://www.pain-tasp.com/main/images/stories/download/cpg/cover_cpg_cancer_pain.pdf

โครงเนอหา บทน า
ตารางท 1 สรปนาหนกคาแนะนาการรกษาความปวดจากมะเรง แผนภมท 1 แนวทางการประเมนความปวด และอาการรวมตางๆ ในผ ปวยมะเรง แผนภมท 2 แนวทางการบาบดความปวดจากมะเรง ตารางท 2 ระดบการตอบสนองของความปวดแบบตางๆ ทพบได ในผ ปวยมะเรงตอยาแก
ปวดกลมตางๆ Check list: Comprehensive pain assessment
การประเมนประสบการณความปวด
การประเมนทางด านจตใจ อารมณ และสงคม
การประเมนสภาวะสขภาพ
การตรวจรางกายและการตรวจทางระบบประสาท
การให การวนจฉยความปวด
การตรวจเพมเตมเพอชวยการบาบดความปวด

โครงเนอหา ภาคผนวก 1 อาการเฉพาะอนๆ
1.1 Dyspnea 1.2 Lymphedema 1.3 Constipation 1.4 Deconditioning and fatigue
ภาคผนวก 2 ภาวะทางจตเวช 2.1 Distress 2.2 Anxiety 2.3 Depression 2.4 Delirium

โครงเนอหา
ภาคผนวก 3 การสอสารและการใหความร 3.1 บทบาทของผ ปวยและญาต 3.2 ความเข าใจคลาดเคลอนเกยวกบการใช ยากลม opioids
ภาคผนวก 4 การรกษาเฉพาะของความปวดจากมะเรงทเกดจากสาเหตตางๆ
4.1 Neuropathic cancer pain (NCP) 4.2 Cancer-induced bone pain (CIBP) 4.3 Tumor-induced headache (TIH) 4.4 Visceral pain and malignant bowel obstruction (MBO)

โครงเนอหา ภาคผนวก 5 Opioids
5.1 เภสชวทยาคลนกของยาในกลม opioids 5.2 Equianalgesic dose ของยาในกลม opioids และการคานวณ 5.3 หลกการใช ยา opioids 5.4 การจดการอาการไมพงประสงคจากการใช opioids
ภาคผนวก 6 Non-opioids
ภาคผนวก 7 Adjuvants
ภาคผนวก 8 Pain at the end of life


สรปนาหนกคาแนะนาการรกษาความปวดจากมะเรง ค าแนะน าทวไป น าหนก
ประเมนความปวดแบบครอบคลมทงทางรางกาย จตใจ และสงคม ++
ประเมนสาเหต ชนด และความรนแรงของความปวด ++
การตรวจเพมเตมอนๆ (additional investigation) เพอการบ าบดอาการปวด
+
ใหการรกษาทจ าเพาะกบอาการเฉพาะอนๆทเกดรวมเชน neuropathic pain, CIBP +
การใช adjuvant analgesics ทเหมาะสม +
พจารณาการรกษาทไมใชยาในกรณทเหมาะสม เชน รงสรกษา เวชศาสตรฟนฟ หตถการทางวสญญวทยา ฯลฯ
+
ใหค าแนะน าและสอสารกบผปวยและญาตเกยวกบโรคและการดแลรกษาเปนระยะๆ ++
การวางแผนดแลรกษาลวงหนา (advance care plan) +
ตดตามการเปลยนแปลงของโรคมะเรงและภาวะทางจตเวช เชน ทกข วตกกงวล ซมเศรา การ
ปรบตว +
การรกษาความปวดดวยการใชการแพทยแบบผสมผสานและการแพทยทางเลอก +/-

สรปนาหนกคาแนะนาการรกษาความปวดจากมะเรง ค าแนะน าการรกษาความปวดดวยยา น าหนก
การใชหลกการ multimodal analgesia ในการรกษาความปวดจากมะเรง ++
การปรบยาแกปวดตามระดบความปวดตาม WHO analgesic ladder ++
การสงใช opioids แบบ around-the-clock ในการรกษา ผปวย cancer pain ซงม
continuous pain
++
การม rescue analgesic ส าหรบ breakthrough pain และประเมนความปวดซ า
ทก 48-72 ชวโมง ++
การใชมาตรการเพอปองกนอาการทองผกลวงหนาในผปวย cancer pain ทไดรบ
opioids ในระยะยาว ++
ตดตามการท างานของตบและไตของผปวยเปนระยะๆ +
การใช pethidine ในผปวย chronic cancer pain - -
การใหยาหรอสารอนๆ เพอหวง placebo effect - -

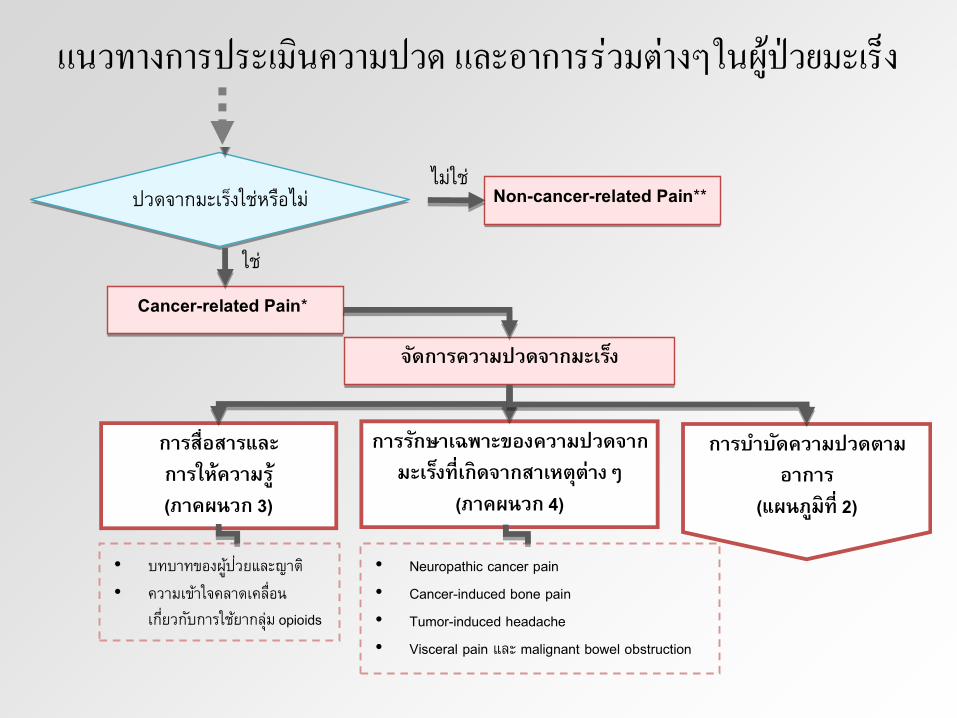
แนวทางการประเมนความปวด และอาการรวมตางๆในผปวยมะเรง
( 1)
( 2)
( 2)
( 3)
( 4)
• Neuropathic cancer pain • Cancer-induced bone pain • Tumor-induced headache • Visceral pain malignant bowel obstruction
Non-cancer-related Pain**
Cancer-related Pain*
• •
opioids
( Check list: comprehensive pain assessment)
•
•
•
Cancer Pain Diagnosis
• Dyspnea • Lymphedema • Constipation • Deconditioning and
fatigue
• Distress • Anxiety • Depression • Delirium

Check list: Comprehensive pain assessment • การประเมนประสบการณความปวด
• ต าแหนง ลกษณะ ความรนแรง ปจจยทมผล ผลกระทบ อาการรวมอน การตอบสนองตอยาทใชอยหรอเคยใชมากอน
• การประเมนทางดานจตใจ อารมณ และสงคม
• การประเมนสภาวะสขภาพ
• การตรวจรางกายและการตรวจทางระบบประสาท
• การสงตรวจทางหองปฏบตการและภาพถายรงส

Check list: Comprehensive pain assessment (ตอ)
• การให การวนจฉยความปวด (pain diagnosis) • ตามสาเหต (etiology)
• มะเรง • การรกษามะเรง • สาเหตอนๆ ทไมเกยวข องกบมะเรง
• ตามพยาธสรรวทยา (pathophysiology) • Nociceptive pain เชน ความปวดจากก อนมะเรงทกดเบยดเนอเยอสวนกายเชน กล ามเนอ
กระดกหรอเนอเยอออนอนๆ หรอ visceral organ เชน ตบกระเพาะอาหาร • Neuropathic pain เชนความปวดจากมะเรงทกระจายไปท somatosensory
system เชน เส นประสาทสวนปลาย และไขสนหลง

ปวดจากมะเรงใชหรอไม?
• *Cancer-related pain หมายถงความปวดทเกดจากมะเรง การลกลามของมะเรง หรอเปนผลจากการรกษามะเรง ไมวาจะเปนจากการผาตด ฉายรงส หรอ เคมบาบด
• **Non cancer-related pain หมายถงอาการปวดทเกดในผ ปวยมะเรง แตสาเหตของอาการปวดไมได เกดจากมะเรงหรอผลพวงของมะเรง เชน อาการปวดจากงสวด อาการปวดหวไมเกรน เปนต น
Check list: Comprehensive pain assessment (ตอ)
• การตรวจเพมเตมอนๆ (additional investigation) เพอการบ าบดอาการปวด • สงสยหรอไมแนใจในสาเหตหรอทมาของอาการปวด ซงจะมผลตอการตดสนใจในการ
รกษา สวนใหญจะเปนการตรวจทางรงส • ตรวจสอบประสทธภาพการทางานของรางกายตรวจหาโรคทเปนรวม เพอชวยในการ
ตดสนใจเลอกยา ปรบยา หรอวธการรกษาให ปลอดภยกบผ ปวยมากทสด

การตรวจเพมเตมอนๆ เพอชวยการบาบดความปวด การตรวจเพอชวยหาสาเหตของอาการปวด
Plain film: CXR ดการแพรกระจายของมะเรงไปทปอดชองเยอห มปอด หรอชองเยอห มหวใจ
Plain abdomen อาการปวดในชองท องทอาจเกดจากลาไส อดตน ภาวะลาไส หรอกระเพาะอาหารทะล
Bone scan อาการปวดทสงสยวาอาจเกดจากการแพรกระจายของมะเรงไปยงกระดก
CT ดการแพรกระจายของมะเรงไปยงอวยวะตางๆ ทสมพนธกบอาการปวดนนๆ ดลาไส อดตน ภาวะลาไส หรอกระเพาะอาหารทะลการกระจายไปทสมอง
MRI ดการแพรกระจายของมะเรงไปยงเส นประสาทหรอไขสนหลง รวมถงการกดทบเส นประสาท
การตรวจสอบประสทธภาพการท างานของรางกาย เพอชวยในการตดสนใจเลอกยาหรอปรบขนาดยา
CBC ตรวจดภาวะ anemia ทอาจเกดจากยาบางกลม เชน NSAIDs ททาให เกดเลอดออกในทางเดนอาหาร
BUN และ electrolyte การได ยาระงบปวดหลายตว อาจทาให เกดอาการงวงซม ในขณะเดยวกน ภาวะ electrolyte imbalance และการเพมขนของคา BUN กมผลทาให ผ ปวยงวงซมด วยเชนกน
LFT การทาลายยาแก ปวดสวนใหญจะเกดขนทตบโดยอาศยเอนไซมของตบ หากหน าทของตบผดปกต อาจจะทาลายยาได ช าลงสงผลให ยาออกฤทธได นานขน
Creatinine
clearance
แสดงถงประสทธภาพของไต การลดลงของคา creatinine clearance หมายถงการทางานของไตแยลง การขบยาแก ปวดบางชนดออกจากรากายอาจลดลงด วย ทาให ต องลดขนาดยาลง หรอเพมระยะหางของการให ยา
แนวทางการประเมนความปวด และอาการรวมตางๆในผปวยมะเรง
( 1)
( 2)
( 2)
( 3)
( 4)
• Neuropathic cancer pain • Cancer-induced bone pain • Tumor-induced headache • Visceral pain malignant bowel obstruction
Non-cancer-related Pain**
Cancer-related Pain*
• •
opioids
( Check list: comprehensive pain assessment)
•
•
•
Cancer Pain Diagnosis
• Dyspnea • Lymphedema • Constipation • Deconditioning and
fatigue
• Distress • Anxiety • Depression • Delirium

ตวอยางแบบประเมนความปวดอยางครอบคลมในผปวยมะเรง

ตวอยางแบบตดตามความปวดในผปวยมะเรง

การสอสารและการให ความร
• บทบาทของผ ปวยและญาต
• ความเข าใจคลาดเคลอนเกยวกบการใช ยากลม opioids • ยากลมนถกมองทางลบวาเปนยาเสพตด
• สาเหตททาให บคลากรทางการแพทยคดวาผ ปวยตดยา • ผ ปวยร องขอยาในปรมาณทบคลากรทางการแพทยเหนวามากเกนไป หรอขอบอยเกนไป • ไมสามารถลดขนาดการใช ยาลงได หยดใช แล วกระวนกระวายเหมอนลงแดง ต องใช ไปเรอยๆ และ
เพมขนาดยาขน
• ยามผลตอสขภาพจตผ ปวย ดเหมอนเคลมๆ มความสข
• ผ ปวยเคยมประวตตดสารเสพตดมากอน
• ความเชอทวา opioids จะกดการหายใจ ทาให ผ ปวยตายเรวขนได • ความเชอทวาผ ปวยมะเรงตดยากไมเปนไร เพราะเวลาในชวตกเหลอน อยอยแล ว

แนวทางการบาบดความปวด จากมะเรง
(Pain Score NRS 4-6/10)
(Pain Score NRS 1-3/10)
(Pain score NRS 7-10/10)
/
regimen
*
• Consult pain/palliative care team/specialist
• Pain at the end of life( 8)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 1
Opioids for Mild to
Moderate Pain ( 5)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 2
Opioids for Moderate to
Severe Pain( 5)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 3
*
*
*

(Pain Score NRS 4-6/10)
(Pain Score NRS 1-3/10)
(Pain score NRS 7-10/10)
/
regimen
*
• Consult pain/palliative care team/specialist
• Pain at the end of life( 8)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 1
Opioids for Mild to
Moderate Pain ( 5)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 2
Opioids for Moderate to
Severe Pain( 5)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 3
*
*
*
NRS = Numerical rating scale คะแนน 0-10

(Pain Score NRS 4-6/10)
(Pain Score NRS 1-3/10)
(Pain score NRS 7-10/10)
/
regimen
*
• Consult pain/palliative care team/specialist
• Pain at the end of life( 8)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 1
Opioids for Mild to
Moderate Pain ( 5)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 2
Opioids for Moderate to
Severe Pain( 5)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 3
*
*
*

(Pain Score NRS 4-6/10)
(Pain Score NRS 1-3/10)
(Pain score NRS 7-10/10)
/
regimen
*
• Consult pain/palliative care team/specialist
• Pain at the end of life( 8)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 1
Opioids for Mild to
Moderate Pain ( 5)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 2
Opioids for Moderate to
Severe Pain( 5)
Non-opioids ( 6)
Adjuvants ( 7)
STEP 3
*
*
*

ความหมายของ “ควบคมความปวดได ”
• หมายถง ความปวดมระดบความรนแรงอยในระดบทผ ปวยยอมรบได และ ผ ปวยสามารถทนอาการไมพงประสงคของยาแก ปวดได
• ถ าผ ปวยใช opioids ให ดเพมเตมในภาคผนวก 5.3 การจดการอาการไมพงประสงคจากการใช opioids

ระดบการตอบสนองของความปวดแบบตางๆทพบไดในผปวยมะเรง ตอยาแกปวดกลมตางๆ
Nociceptive
Pain*
NCP** CIBP** TIH** Vis/MBO**
Opioids ดมาก ปานกลาง ดมาก ด ดมาก
สาหรบอาการปวดตลอดเวลา
ปานกลาง สาหรบอาการปวดบด
เปนพกๆ NSAIDs/Coxibs ดมาก ไมด ดมาก ด ไมแนะนา
*Nociceptive pain เชน ความปวดจากก อนมะเรงทกดเบยดเนอเยอสวนกาย เชน กล ามเนอ กระดก หรอเนอเยอออนอนๆ หรอ visceral organ เชน ตบ กระเพาะอาหาร **มการรกษาเฉพาะให ดใน ภาคผนวก 4 การรกษาเฉพาะของความปวดจากมะเรงทเกดจากสาเหตตางๆ คายอ:NCP = Neuropathic cancer pain, CIBP = Cancer-induced bone pain, TIH = Tumor-induced headache, Vis/MBO = Visceral pain และ malignant bowel obstruction

ระดบการตอบสนองของความปวดแบบตางๆทพบไดในผปวยมะเรง ตอยาแกปวดกลมตางๆ
Nociceptive
Pain*
NCP** CIBP** TIH** Vis/MBO**
Antidepressants
TCAs และ SNRIs
น อย ดมาก ปานกลาง ไมแนะนา ไมแนะนา
Gabapentinoids น อย ดมาก ด ไมแนะนา ด สาหรบ visceral
hyperalgesia
Carbamazepine ไมด ด สาหรบ
paroxysmal
sharp shooting
pain
น อย น อย
ยกเว นใช เปน
ยากนชก
ไมด
*Nociceptive pain เชน ความปวดจากก อนมะเรงทกดเบยดเนอเยอสวนกาย เชน กล ามเนอ กระดก หรอเนอเยอออนอนๆ หรอ visceral organ เชน ตบ กระเพาะอาหาร **มการรกษาเฉพาะให ดใน ภาคผนวก 4 การรกษาเฉพาะของความปวดจากมะเรงทเกดจากสาเหตตางๆ คายอ:NCP = Neuropathic cancer pain, CIBP = Cancer-induced bone pain, TIH = Tumor-induced headache, Vis/MBO = Visceral pain และ malignant bowel obstruction

ระดบการตอบสนองของความปวดแบบตางๆ ทพบไดในผปวยมะเรงตอยาแกปวดกลมตางๆ
Nociceptive
Pain*
NCP** CIBP** TIH** Vis/MBO**
Bisphosphonates ไมด ไมด ด
เมอให ยาในระยะยาว
ไมด ไมด
Corticosteroids ไมแนะนา ดมาก
สาหรบ
nerve/spinal
cord
compression
ปานกลาง ดมาก ด
สาหรบ liver capsule
distension
*Nociceptive pain เชน ความปวดจากก อนมะเรงทกดเบยดเนอเยอสวนกาย เชน กล ามเนอ กระดก หรอเนอเยอออนอนๆ หรอ visceral organ เชน ตบ กระเพาะอาหาร **มการรกษาเฉพาะให ดใน ภาคผนวก 4 การรกษาเฉพาะของความปวดจากมะเรงทเกดจากสาเหตตางๆ คายอ:NCP = Neuropathic cancer pain, CIBP = Cancer-induced bone pain, TIH = Tumor-induced headache, Vis/MBO = Visceral pain และ malignant bowel obstruction

Topic wrapped
• Cancer patient problem
• Causes of pain in cancer
• World Health Organization: analgesic ladder
• Pharmacological and non pharmacological pain concepts
• Specific cancer pain: • bone pain, neuropathic pain, tumor induced headache,
refractory pain
• End of life pain
• Clinical practice guideline for cancer pain TASP 2013


















