Primary Teeth Trauma
4
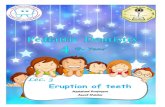
DENTAL UPDATE/MAY 1999 138 PAEDIA TRIC DENTISTRY PAEDIATRIC DENTISTRY C ases of orofacial trauma presenting to general dental practitioners are a relatively common event. It is therefore important that general dental practitioners are well versed in the management of trauma to permanent teeth and in treating trauma to the primary dentition. 1 Injuries to the primary dentition are common: it has been estimated that up to 30% of preschool children are affected 2 . Trauma often occurs in this population because young children tend to be unstable on their feet as they first start to walk—and then, in running around with their new-found mobility, suffer accidents which result in damaged teeth (Figure 1). The roots of the primary teeth are in close relationship to their developing permanent successors and an acute impact can easily be transmitted to the developing permanent dentition. 3 In addition, infection developing subsequent to injury to a primary tooth may damage the successional tooth. 4 Andreasen and Ravn 5 stated that the most important factor in determining whether damage to the successional tooth will result is the age of the child at time of injury. In their study of 213 traumatized primary teeth followed up clinically and radiographically , they found that over 60% of the permanent teeth were damaged if the trauma occurred in a child under 4 years of age. This corresponds to the timing of development and mineralization of the permanent incisor teeth. The prevalence of such disturbances, secondary to dental injuries in the primary dentition, ranges from 12 to 69%, according to different studies. 3,5,6 The most serious primary tooth injuries in terms of damage to the permanent successors are intrusive luxations, 69% of injuries resulting in damage to the permanent successor, followed by avulsions (52%), extrusions and subluxations (each 34%). 5 Th e treatment strategy following injury in the primary dentition is therefore dictated by concern for the safety of the permanent dentition. HOW COMMON IS TRAUMA TO PRIMARY TEETH? Reports of the incidence of trauma to the primary teeth vary from 1 1 to 30%. 2 The reason for this lar ge variation is the fact that injuries to the primary dentition, particularly the less serious injuries, are often not seen by dentists as the parents do not think the injury warrants examination. The most common age group in which primary tooth injury occurs is 1.5 to 2.5 years. 2 At this age the child has started to walk but is not particularly steady on his/her feet—and they are also at the same height as many pieces of household furniture. In the permanent dentition more boys suffer trauma than girls, 7 which is also the case in the primary dentition, although the difference is not as great. Also, owing to the resilient bone Diagnosis and Management of Trauma to Primary Dentition Jinous F . T ahmasseb i and Elizabet h A. O’Sullivan Jinous F. T ahmassebi, BDS, MDentSci, FRCD(C), Senior Dent al Offi cer/Research F ellow, Airedale NHS Trust and Department of Paediatric Dentistry, and Elizabeth A. O’Sullivan, BChD, MDentSci, MRCD(C), FDS (Paeds) RCS (Eng.), PhD, Senior Registrar, Department of Paediatric Dentistry, Leeds Dental Institute. Abstract: This article seeks to aid the busy dentist by providing a basic guide to treating fractured and traumati zed primary teeth and soft tissues. Simple guidelines for a step-by-step approach to the efficient care of traumati zed primary teeth are given. Dent Update 1999; 26: 138-142 Clinical Relevance: In view of the not uncommon occurrence of trauma to primary teeth and its possible adverse effects on the permanent successors, it is important for the general practitioner to be aware of its immediate and long-term management. Figure 1. Tra uma to the primary dentition of a toddler who fell against a coffee table.
-
Upload
riad-bacho -
Category
Documents
-
view
219 -
download
0
Transcript of Primary Teeth Trauma

8/2/2019 Primary Teeth Trauma
http://slidepdf.com/reader/full/primary-teeth-trauma 1/4
DENTAL UPDATE/MAY 1999138
PAEDIATRIC DENTISTRY PAEDIATRIC DENTISTRY
Cases of orofacial trauma presentingto general dental practitioners are
a relatively common event. It is thereforeimportant that general dental practitioners are well versed in themanagement of trauma to permanentteeth and in treating trauma to the primarydentition.1
Injuries to the primary dentition arecommon: it has been estimated that upto 30% of preschool children areaffected2. Trauma often occurs in this population because young children tend
to be unstable on their feet as they firststart to walk—and then, in runningaround with their new-found mobility,suffer accidents which result in damagedteeth (Figure 1).
The roots of the primary teeth are inclose relationship to their developing
permanent successors and an acuteimpact can easily be transmitted to thedeveloping permanent dentition.3 Inaddition, infection developingsubsequent to injury to a primary toothmay damage the successional tooth.4
Andreasen and Ravn5 stated that themost important factor in determiningwhether damage to the successionaltooth will result is the age of the childat time of injury. In their study of 213traumatized primary teeth followed upclinically and radiographically, they found
that over 60% of the permanent teethwere damaged if the trauma occurred in achild under 4 years of age. Thiscorresponds to the timing of development and mineralization of the permanent incisor teeth. The prevalenceof such disturbances, secondary todental injuries in the primary dentition,ranges from 12 to 69%, according todifferent studies.3,5,6
The most serious primary toothinjuries in terms of damage to the permanent successors are intrusiveluxations, 69% of injuries resulting indamage to the permanent successor,followed by avulsions (52%), extrusions
and subluxations (each 34%).5
Thetreatment strategy following injury in the primary dentition is therefore dictated byconcern for the safety of the permanentdentition.
HOW COMMON IS TRAUMATO PRIMARY TEETH?
Reports of the incidence of trauma tothe primary teeth vary from 11 to 30%.2
The reason for this large variation is thefact that injuries to the primarydentition, particularly the less seriousinjuries, are often not seen by dentistsas the parents do not think the injurywarrants examination.
The most common age group in which primary tooth injury occurs is 1.5 to 2.5years.2 At this age the child has startedto walk but is not particularly steady onhis/her feet—and they are also at thesame height as many pieces of household furniture.
In the permanent dentition more boyssuffer trauma than girls,7 which is alsothe case in the primary dentition,
although the difference is not as great.Also, owing to the resilient bone
Diagnosis and Management of Traumato Primary Dentition
Jinous F. Tahmassebi and Elizabeth A. O’Sullivan
Jinous F. Tahmassebi, BDS, MDentSci, FRCD(C),
Senior Dental Officer/Research Fellow,Airedale NHS Trust and Department of Paediatric Dentistry, and Elizabeth A.O’Sullivan, BChD, MDentSci, MRCD(C), FDS (Paeds) RCS
(Eng.), PhD, Senior Registrar, Department of Paediatric Dentistry, Leeds Dental Institute.
Abstract: This article seeks to aid the busy dentist by providing a basic guide to treating fractured and traumatized primary teeth and soft tissues. Simple guidelines
for a step-by-step approach to the efficient care of traumati zed primary teeth are
given.
Dent Update 1999; 26: 138-142
Clinical Relevance: In view of the not uncommon occurrence of trauma to primary
teeth and its possible adverse effects on the permanent successors, it is important
for the general practitioner to be aware of its immediate and long-term
management.
Figure 1. Trauma to the primary dentition of a toddler who fell against a coffee table.

8/2/2019 Primary Teeth Trauma
http://slidepdf.com/reader/full/primary-teeth-trauma 2/4
1391999 MAY/DENTAL UPDATE
PAEDIATRIC DENTISTRY
surrounding the primary teeth, injuriesusually result in avulsions, luxations, etc.,rather than fractures of the crown.2
AETIOLOGY
Primary tooth trauma is uncommon duringthe first year of life, but may result from achild being dropped, or falling from its pram.8 Injuries usually occur in falls,collisions or bumps as the child startswalking.2 Non-accidental injury (physicalabuse) should also be considered incircumstances where the injuries do notcorrespond to the history given.9
ASSESSMENTIt is often difficult to examine youngchildren, although asking theaccompanying parent to lie the childacross their knees and hold onto their hands will help to ensure a thoroughexamination. Vitality tests are unreliablein young children so should not beattempted as they will rarely give anyuseful information.
Radiographic examination may behelpful in determining whether a toothhas been avulsed or fully intruded if the
parents are not able to confirm thewhereabouts of a missing tooth. Theeasiest method is to take an anterior oblique occlusal view. Sometimes asmall, child-size bitewing film can be of use in a small mouth (Figure 2). Lateralfilms can be used in a child who finds itdifficult to accept radiographic films inthe mouth, and may be useful indetermining the relationship of thetraumatized primary tooth to thedeveloping permanent dentition. Oftena child is upset at the initial visit and itmay be appropriate to postponeradiographic examination to the reviewvisit.
TREATMENT APPROACHES
Treatment should be organized in order first to relieve the child of pain or
discomfort and then restore thedentition, keeping the prognosis of the permanent successor foremost in themind. As primary tooth trauma usuallyoccurs in the very young child, co-operation is the main problem. It may be necessary after initial examination toadvise the parents regarding analgesia,soft diet and oral hygiene, and thenarrange to review the child the followingweek when he or she is less upset. Thisis particularly relevant if it is the child’sfirst dental experience. As long as thereis no danger of the tooth coming loose
or being inhaled, this may be anappropriate decision.
Laceration of Soft Tissue
This is common in trauma to the primarydentition that causes displacement of thetooth or teeth. Often the injured area isobscured by blood, and in order to carryout a full assessment the area needs to becleaned up either by irrigating or wipingthe area with water or normal saline. Oncethe area is clear of blood, the practitioner
can establish whether there has beensignificant soft-tissue injury. If the area isseverely lacerated, the soft tissues will needto be sutured (Figure 3): in a co-operativechild this may be done under localanaesthesia, but some patients will requirereferral for general anaesthesia. If the softtissue injury is severe or the site of traumais dirty, antibiotic coverage for 5 days may be necessary. If the injury occurred outside,it is wise to ask the mother to check withher general medical practitioner on thechild’s anti-tetanus status.
A recall for a review after 7 to 10 days
is prudent to check healing.
Tooth Fractures
The main aim is to prevent injury to the permanent successor and then to savethe primary tooth (if compatible withthe first aim). The dental practitioner should aim to restore tooth andaesthetics, if possible, with the leastamount of active treatment compatiblewith the child’s co-operation.
Should the Injured Tooth be Saved?
There are several factors to consider before restoring a fractured primary tooth:
q if there have been other injuries tothe tooth, such as luxation injuries, theremay be a high risk of damage to the permanent tooth;q patient co-operation may be suchthat restorative treatment is not anoption—this is often the case in veryyoung children;q the parent might not be prepared toattend review visits to assess for vitalityof the damaged tooth or other pathology;q if the fractured primary tooth is near to exfoliation and symptomless it maynot be necessary to carry outcomplicated restorative treatment, andinstead review it until exfoliation.
Treatment Approaches
The co-operation of the child is again amajor factor here. If the child isdistressed or very young, little in theway of treatment may be possible. Themain aim at the initial presentation isto relieve pain. Enamel fractures: If the fractureinvolves just a small chip this may beleft or the edge smoothed off and topicalfluoride applied. A larger chip willrequire restoration with composite resin.All enamel fractures should bereviewed, as often luxation injury hasalso occurred (see below). Enamel and dentine fractures: The firstaim is to protect the pulp with calciumhydroxide or glass ionomer liningmaterial. Following this the damagedcrown can be restored with composite
Figure 2. Anterior occlusal radiograph using a bitewing film.
Figure 3. The soft tissues injured in
this child were sutured under local anaesthesia.

8/2/2019 Primary Teeth Trauma
http://slidepdf.com/reader/full/primary-teeth-trauma 3/4
DENTAL UPDATE/MAY 1999140
PAEDIATRIC DENTISTRY
resin restoration, or using the strip crowntechnique as shown by Pollard et al.10
Again, these teeth should be reviewed at
regular intervals.Whole crown fractures (Figure 4): Thetreatment of whole crown fracturesdepends on the extent of fracture and theco-operation of the patient. The followingtreatment options may be appropriate:
q coronal pulpotomy and stripcrown;
q pulpectomy and strip crown;q extraction.
There has been conflicting evidence tosuggest that these procedures may leadto hypoplastic defects of the developing permanent successor teeth.11
Root fractures: Root fractures areuncommon in small children. A periapicalradiograph is required, as described earlier,to determine the position of the fracture.If the coronal fragment is stable it may befeasible to monitor the tooth and leave italone if no symptoms occur. If the rootfracture communicates with the gingivalmargin, then the prognosis is poor andthe tooth should be extracted. In this caseit is often best to extract the coronal
portion but leave the apical portion toresorb, unless it can be located easily withforceps. Under no circumstances shouldan attempt be made to remove any smallroot fragments—the risk of damage to theunderlying permanent tooth crown is highwith instrumentation. The coronalfragment may be removed with forceps.
Displacement Injuries toPrimary Teeth
With all luxation injuries to teeth, if theinjury has taken place outside or if thetraumatized site is particularly dirty,antibiotic therapy and review of anti-
tetanus status should be considered.
Avulsions
Never attempt to reimplant primary teethdue to the danger of damaging theunderlying permanent teeth.
Luxation Injuries
If the luxation injury is slight, and the toothis not at risk of coming out of the socketspontaneously, then it can be left andadvice regarding soft diet and careful oralhygiene instruction given.
If the tooth has been luxated palatally itmight be possible to gently reposition itmanually—but only if the displacement isless than 2 mm. If the tooth has been
displaced by more than 2 mm, no attemptshould be made to reposition as this mayrisk damage to the underlying permanenttooth. Extraction may be more appropriatein this case. Where teeth have beenrepositioned they need to be monitoredfor loss of vitality and mobility. If upper primary incisors have been displaced palatally, if they are firm and if there isanterior open bite, there is no need to tryto reposition the teeth.
If the tooth does not show animprovement in mobility over 2 weeks, the practitioner should consider extraction.
Intrusion Injuries
The approach to treatment for these teethis largely to establish where they are inthe alveolus and then to leave them alone.
q If less than three-quarters of thecrown is intruded then the tooth can beallowed to re-erupt spontaneously. Normally this occurs within 2 to 4 monthsafter injury.q If more than three-quarters of the
crown has intruded, the tooth may stillerupt and should be monitored carefully
(Figure 5). In circumstances like this thedamage to the alveolus may causesymptoms such as pain, and the tooth mayrequire extraction.
An anterior lateral radiograph should be taken to determine the position of the primary tooth in relation to the permanentsuccessor. If the intruded tooth is veryclose to or touching the permanent tooth,the primary should be extracted.
It should be noted that intruded andlater re-erupted primary incisors candevelop pulp necrosis, a complicationfound in approximately one-third of re-erupted primary teeth.3 It is therefore veryimportant that these injuries are reviewedat regular intervals until the toothexfoliates.
Extrusion Injuries (Figure 6)
Extrusion injuries which occur in the primary dentition usually interfere with theocclusion; therefore extraction is oftenindicated. If, however, there is an anterior open bite the tooth may be left in placeand monitored. The following treatment
approaches should be considered:
q if the extrusion is less than 1 or 2 mmthen leave and monitor;q if extruded by more than 2 mm the toothwill almost certainly have lost its vitalityand therefore should be extracted.
MONITORING
Injuries to primary teeth should bemonitored after one week, one month,three months, six months, one year andthen yearly, until exfoliation. It is notnecessary to take radiographs at everyreview; at injury, six months after injury and
Figure 4. Whole crown fracture of the upper right central incisor with soft tissue injuries.
Figure 5. Severe intrusion of the upper
right lateral and avulsion of the upper right central incisor. The patient’s mother is retracting the lips.
Figure 6. Extrusion injuries to the upper central incisors.

8/2/2019 Primary Teeth Trauma
http://slidepdf.com/reader/full/primary-teeth-trauma 4/4
DENTAL UPDATE/MAY 1999142
PAEDIATRIC DENTISTRY
then at yearly intervals is appropriate.Additional radiographs may be necessaryif symptoms occur.
If periapical pathology occurs the toothwill usually need to be extracted, althoughin some instances a pulpectomy may beappropriate, especially if the parent or childis keen not to lose the tooth.
Discoloration of primary teeth is notalways an indicator of loss of vitality:reversible colour changes of the crown
are common in traumatized primary teeth.Clinical studies have shown that mostdiscoloured primary teeth do not developradiographic or clinical signs of infectionand are exfoliated at the expected time.12,13
Grey discoloration is related to morefrequent pathological change.14
INJURY TO PERMANENTSUCCESSORS
Traumatic injuries to the developing teethcan influence their future growth and
maturation, usually leaving a child with a permanent deformity. Injuries to thedeveloping teeth can be classified asfollows:2
q white or brown discoloration of the permanent tooth with or withouthypoplastic defects;q dilaceration of the crown of the tooth— causing eruption disturbance or failure;q dilaceration of the root of the tooth— causing eruption disturbance or failure(Figure 7);q odontome-like formation;q root duplication;q partial or total failure of root
Figure 8. Trauma to a primary incisor
has caused failure of development of its permanent successor.
development;q total failure of tooth development(Figure 8).
The proximity of the root of the primaryincisor to the crown of its permanentsuccessor means that, when a primary toothis injured, there is significant potential for damage to the permanent successor. Inmany cases damage to the permanent toothtakes place at the time of injury and the abilityto limit damage by some form of interventionis minor.
However, it is important to ascertain, usingradiographs, if there has been collision between a displaced primary tooth and its permanent successor. If this has occurred,
the displaced incisor should be removed— the longer the tooth is left in this positionthe greater the danger of damage to the permanent tooth.
Review of traumatized primary teeth isimportant, because if periapical pathologyoccurs around these teeth in the proximityof developing permanent crowns, the risk of hypoplastic change to the crownincreases.
Often the damage that occurs is not predictable, and it is important to warn parents of potential damage to the permanenttooth so that they are prepared and more
diligent about keeping their child’s dentitionunder review.
CONCLUSION
Trauma to the primary dentition is a commonexperience, and the initial treatment andfollow up is very important—particularly in
respect to the effect on the permanentsuccessors.
Discoloration of incisors does notautomatically indicate a non-vital pulp andthe colour change often reverses. It isimportant to monitor healing regularly, withroutine clinical and radiographicexaminations.
This guide to the management of damaged primary teeth will allow the dental practitioner to manage the young child effectively, andto advise parents as to the long-term effectsof primary tooth trauma.
References
1. Hamilton FA, Hill FJ, Holloway PJ. An
investigation of dento-trauma and its treatmentin an adolescent population. Part 1 and 2. Br Dent J 1997; 182: 91-95, 129-133.2. Andreasen JO, Andreasen FM. Textbook and Colour Atlas of Traumatic Injuries to Teeth ,3rd ed. Copenhagen: Munksgaard, 1994.3. Ravn JJ. Sequelae of acute mechanicaltraumata in the deciduous dentition. J Dent Child 1968; 35: 281-289.4. Andreasen JO, Sundstrom B, Ravn JJ. Theeffect of traumatic injuries to primary teeth ontheir permanent successors. I. A clinical andhistologic study of 117 injured permanent teeth.Scand J Dent Res 1971; 79: 219-283.5. Andreasen JO, Ravn JJ. The effect oftraumatic injuries to primary teeth on theirpermanent successors. II. A clinical and
radiographic follow-up study of 213 teeth. Scand J Dent Res 1971; 79: 284-294.6. Schreiber CK. The effect of trauma on theanterior deciduous teeth. Br Dent J 1959; 106:340-343.7. Office of Population Censuses and Surveys.Social Survey Division. Children’s Dental Health in the United Kingdom . London: HMSO, 1993.8. Roberts G, Longhurst P. Oral and Dental Trauma in Children and Adolescents. Oxford:Oxford University Press, 1996.9. Welbury RR, Murphy JM. The dentalpractitioner’s role in protecting children fromabuse. 2. The orofacial signs of abuse. Br Dent J 1998; 184: 61-65.10. Pollard MA, Curzon JA, Fenlon WL. Therestoration of decayed primary incisors usingstrip crowns. Dent Update 1991; 18: 150-152.11. Pruhs RJ, Olen GA, Sharma PS. Relationshipbetween formocresol pulpotomy in primary teethand enamel defects in their permanentsuccessors. J Am Dent Assoc 1977; 94: 698-700.12. Schroder U, Wannberg E, Granath LE, MollerH. Traumatized primary incisors—follow upprogram based on frequency of periapicalosteitis related to tooth color. Swed Dent J 1977;70: 95-98.13. Jacobsen I, Sangnes G. Traumatized primaryanterior teeth. Prognosis related to calcificreactions in the pulp cavity. Acta Odontol Scand 1978; 36: 199-204.14. Croll TP, Pascon EA, Langeland K.
Traumatically injured primary incisors: a clinicaland histological study. ASDC J Dent Child 1987;54: 401-422.
Figure 7. Root dilaceration following
trauma to a primary incisor.