Primary Cytomegalovirus Peritonitis Following Unrelated...
5
128 http://jsms.sch.ac.kr Primary Cytomegalovirus Peritonitis Following Unrelated Hematopoietic Stem Cell Transplantation Seong Kyu Park Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea Cytomegalovirus (CMV) has emerged as a significant opportunistic pathogen in the era of immunosuppression. Among patients with hematopoietic stem cell transplantation (HSCT), CMV has become an increasingly important cause of gastrointestinal disease. Almost cases of CMV peritonitis are due to CMV colitis with or without bowel perforation. However, primary CMV peritonitis com- bined without CMV colitis is very rare. We report the first case of primary CMV peritonitis not accompanied by CMV colitis or bowel perforation in a patient who underwent allogeneic HSCT from unrelated donor. Diagnosis of primary CMV peritonitis was made by computed tomography of abdomen, colonoscopy, peritoneal biopsy, and real time reverse transcription-polymerase chain reac- tion for CMV. Thereafter, he was treated successfully with intravenous ganciclovir. Keywords: Cytomegalovirus; Peritonitis; Stem cell transplantation INTRODUCTION Cytomegalovirus (CMV) seroprevalence in general population is high at 60% to 100% and has showed geographic variation [1]. CMV seroprevalence tended to be highest in South America, Afri- ca and Asia and lowest in Western Europe and United States. In Korea, the thorough surveillance of CMV infection and the devel- opment of an effective CMV therapeutic strategy may be especial- ly important, because CMV seroprevalence exceeds 90% [2]. Reac- tivation of latent CMV, or reinfection with a novel strain, com- monly occurs in immunocompromised patients [3]. CMV infec- tion and disease were associated with significant morbidity in the early period after allogeneic hematopoietic stem cell transplanta- tion (HSCT) and led to mortality. The clinical manifestations of CMV disease vary. The most common disease manifestation is gastrointestinal disease, which can escape blood-based surveil- lance by polymerase chain reaction (PCR) and the pp65 antigen- emia assay in approximately 25% of patients [4]. CMV pneumonia is clearly the most serious complication, but has become infre- quent with current prevention strategies [5]. CMV usually affects the colon and common manifestation of CMV colitis is diarrhea [6]. Within the colon, CMV colitis is generally characterized by mucosal ulceration, often associated with bleeding. CMV colitis can induce perforation and peritonitis. However, primary CMV peritonitis combined without CMV colitis is very rare. We present the first case of primary CMV peritonitis not accompanied by CMV colitis or bowel perforation in a patient who underwent al- logeneic HSCT. CASE REPORT A 59-year-old man who had done allogeneic HSCT 51 days ago complained diffuse abdominal pain for three days and had diffuse tenderness of abdomen. He had been diagnosed with acute my- eloid leukemia with myelodysplasia-related changes seven months earlier. Complete remission was achieved after administration of remission induction chemotherapy with idarubicin and cytara- bine. He underwent allogeneic HSCT from full matched unrelated donor who was CMV-seronegative after administering two cycles of consolidation. His CMV serological status was positive (anti- Soonchunhyang Medical Science 19(2):128-132, December 2013 pISSN: 2233-4289 I eISSN: 2233-4297 CASE REPORT Correspondence to: Seong Kyu Park Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicne, 170 Jomaru-ro, Wonmi-gu, Bucheon 420-767, Korea Tel: +82-32-621-5185, Fax: +82-32-621-5018, E-mail: [email protected] Received: Sep. 26, 2013 / Accepted after revision: Oct. 30, 2013 © 2013 Soonchunhyang Medical Research Institute This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/).
Transcript of Primary Cytomegalovirus Peritonitis Following Unrelated...
128 http://jsms.sch.ac.kr
Primary Cytomegalovirus Peritonitis Following Unrelated Hematopoietic Stem Cell TransplantationSeong Kyu Park
Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea
Cytomegalovirus (CMV) has emerged as a significant opportunistic pathogen in the era of immunosuppression. Among patients with hematopoietic stem cell transplantation (HSCT), CMV has become an increasingly important cause of gastrointestinal disease. Almost cases of CMV peritonitis are due to CMV colitis with or without bowel perforation. However, primary CMV peritonitis com-bined without CMV colitis is very rare. We report the first case of primary CMV peritonitis not accompanied by CMV colitis or bowel perforation in a patient who underwent allogeneic HSCT from unrelated donor. Diagnosis of primary CMV peritonitis was made by computed tomography of abdomen, colonoscopy, peritoneal biopsy, and real time reverse transcription-polymerase chain reac-tion for CMV. Thereafter, he was treated successfully with intravenous ganciclovir.
Keywords: Cytomegalovirus; Peritonitis; Stem cell transplantation
INTRODUCTION
Cytomegalovirus (CMV) seroprevalence in general population is high at 60% to 100% and has showed geographic variation [1]. CMV seroprevalence tended to be highest in South America, Afri-ca and Asia and lowest in Western Europe and United States. In Korea, the thorough surveillance of CMV infection and the devel-opment of an effective CMV therapeutic strategy may be especial-ly important, because CMV seroprevalence exceeds 90% [2]. Reac-tivation of latent CMV, or reinfection with a novel strain, com-monly occurs in immunocompromised patients [3]. CMV infec-tion and disease were associated with significant morbidity in the early period after allogeneic hematopoietic stem cell transplanta-tion (HSCT) and led to mortality. The clinical manifestations of CMV disease vary. The most common disease manifestation is gastrointestinal disease, which can escape blood-based surveil-lance by polymerase chain reaction (PCR) and the pp65 antigen-emia assay in approximately 25% of patients [4]. CMV pneumonia is clearly the most serious complication, but has become infre-quent with current prevention strategies [5]. CMV usually affects
the colon and common manifestation of CMV colitis is diarrhea [6]. Within the colon, CMV colitis is generally characterized by mucosal ulceration, often associated with bleeding. CMV colitis can induce perforation and peritonitis. However, primary CMV peritonitis combined without CMV colitis is very rare. We present the first case of primary CMV peritonitis not accompanied by CMV colitis or bowel perforation in a patient who underwent al-logeneic HSCT.
CASE REPORT
A 59-year-old man who had done allogeneic HSCT 51 days ago complained diffuse abdominal pain for three days and had diffuse tenderness of abdomen. He had been diagnosed with acute my-eloid leukemia with myelodysplasia-related changes seven months earlier. Complete remission was achieved after administration of remission induction chemotherapy with idarubicin and cytara-bine. He underwent allogeneic HSCT from full matched unrelated donor who was CMV-seronegative after administering two cycles of consolidation. His CMV serological status was positive (anti-
Soonchunhyang Medical Science 19(2):128-132, December 2013 pISSN: 2233-4289 I eISSN: 2233-4297
CASE REPORT
Correspondence to: Seong Kyu ParkDepartment of Internal Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicne, 170 Jomaru-ro, Wonmi-gu, Bucheon 420-767, KoreaTel: +82-32-621-5185, Fax: +82-32-621-5018, E-mail: [email protected]: Sep. 26, 2013 / Accepted after revision: Oct. 30, 2013
© 2013 Soonchunhyang Medical Research InstituteThis is an Open Access article distributed under the terms of the
Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/).
Primary CMV Peritonitis Following Unrelated HSCT • Park SK
Soonchunhyang Medical Science 19(2):128-132 http://jsms.sch.ac.kr 129
CMV immunoglobin-G, positive; anti-CMV immunoglobin-M, negative) before transplantation. Tacrolimus and sirolimus were initially used for the prophylaxis of acute graft versus host disease. However, sirolimus was discontinued after the event of viral hem-orrhagic cystitis. He complained dysuria and hematuria day +21 after transplantation. Urine microscopic examination, urine cul-tures, cytological examination of urine specimens, and molecular studies for viruses including polyomavirus were performed. Re-verse transcription-PCR (RT-PCR) of urine samples yielded re-sults positive for BK virus and negative for JC virus and adenovi-rus. We administered three times of weekly infusions of 5 mg/kg cidofovir to the patient. Symptoms and signs of cystitis were im-proved three weeks later without nephrotoxicity and RT-PCR sta-tus for BK virus was converted to negative.
On day +51 after transplantation, the patient complained mild to moderate fever, and diffuse abdominal pain for three days, which were different from those of BK virus associated cystitis. He didn’t have diarrhea, or hematochezia. On physical examination, the ab-domen was distended due to mild ileus and there were diffuse ab-dominal tenderness, wall rigidity, and guarding. Anemia, jaun-dice, skin lesions, and enlarged lymph nodes in neck and groin
were not detected.In laboratory findings, blood cell count was subnormal (white
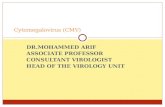
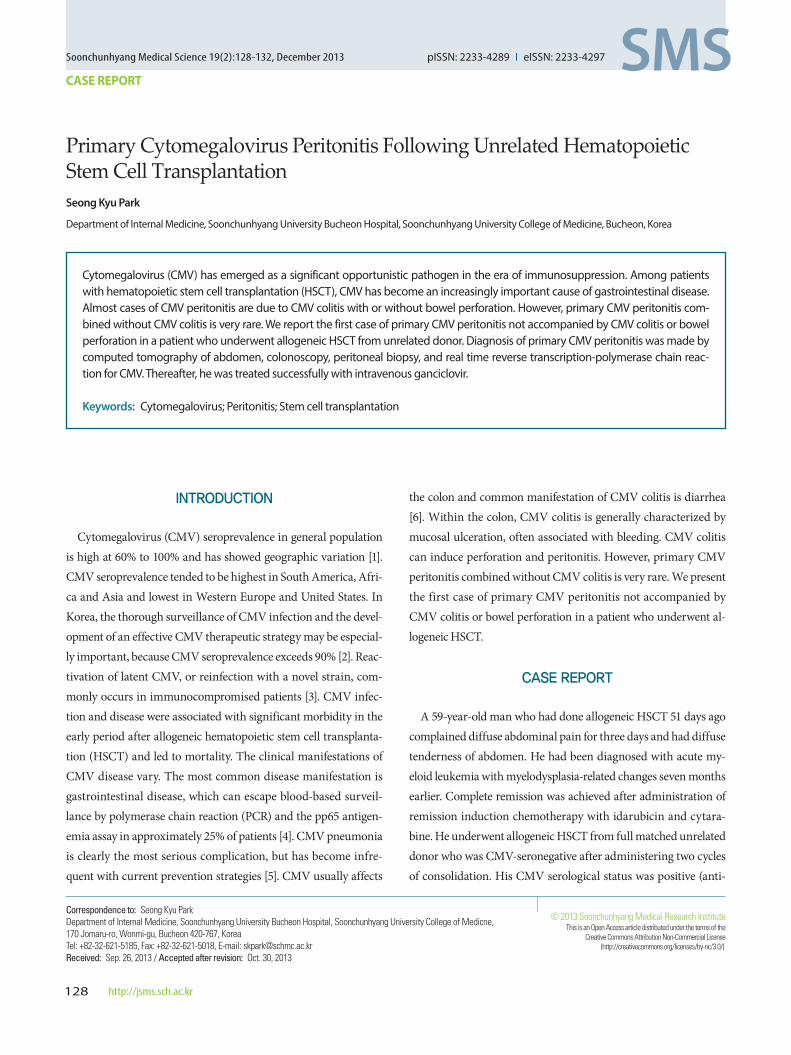
blood cell count, 2,810/µL; absolute neutrophil count, 2,200/µL; hemoglobin, 8.6 gm/dL; hematocrit, 24.8%; and platelet 75,000/µL). Liver and kidney function test were normal. Lactate dehydro-genase was slightly increased (492 IU/L; normal, 219 to 480 IU/L) and C-reactive protein was also increased (14.66 mg/dL; normal, 0 to 0.5 mg/dL). Routine cultures of blood and urine sample were all negative for bacteria and fungi. The follow-up study for BK virus by RT-PCR was negative. CMV titer determined by real-time RT-PCR was rapidly increased (376,045 copies/mL) comparing with that of a week before the event (650 copies/mL) (Fig. 1). And CMV antigenemia using pp65 antigen assay was also detected (8 positive cells on 2×105 leukocytes). However, it took some time to confirm the result of pp65 antigen assay due to requested test and labor-in-tensive procedure.
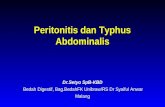
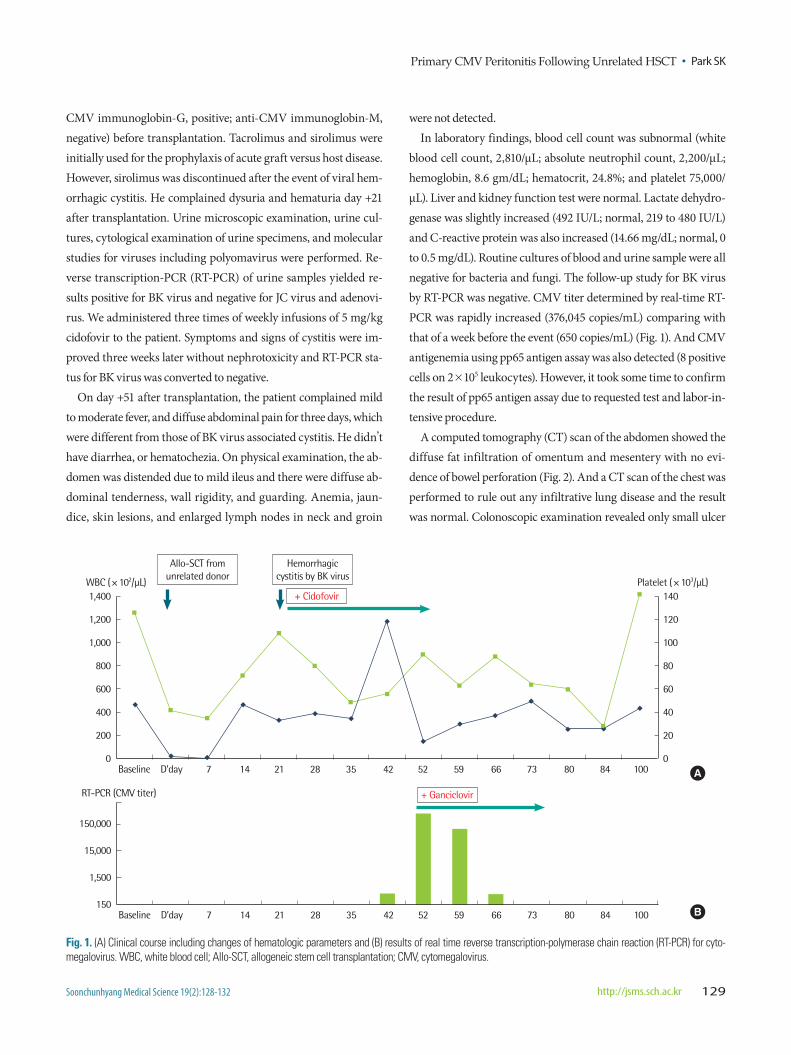
A computed tomography (CT) scan of the abdomen showed the diffuse fat infiltration of omentum and mesentery with no evi-dence of bowel perforation (Fig. 2). And a CT scan of the chest was performed to rule out any infiltrative lung disease and the result was normal. Colonoscopic examination revealed only small ulcer
Fig. 1. (A) Clinical course including changes of hematologic parameters and (B) results of real time reverse transcription-polymerase chain reaction (RT-PCR) for cyto-megalovirus. WBC, white blood cell; Allo-SCT, allogeneic stem cell transplantation; CMV, cytomegalovirus.
1,400
1,200
1,000
800
600
400
200
0
WBC (×102/μL)
Allo-SCT from unrelated donor
Hemorrhagic cystitis by BK virus
+ Cidofovir 140
120
100
80
60
40
20
0
Platelet (×103/μL)
Baseline D’day 7 14 21 28 35 42 52 59 66 73 80 84 100
+ Ganciclovir
150,000
15,000
1,500
150
RT-PCR (CMV titer)
Baseline D’day 7 14 21 28 35 42 52 59 66 73 80 84 100
A
B
Park SK • Primary CMV Peritonitis Following Unrelated HSCT
Soonchunhyang Medical Science 19(2):128-132130 http://jsms.sch.ac.kr
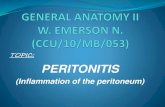
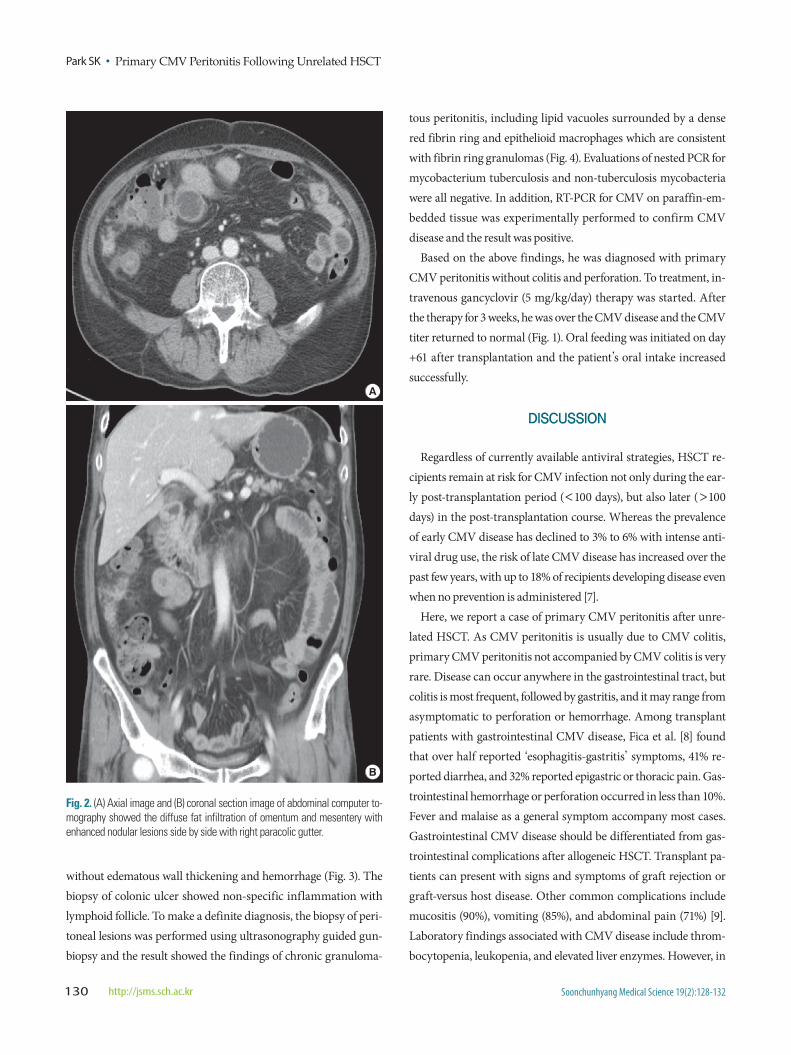
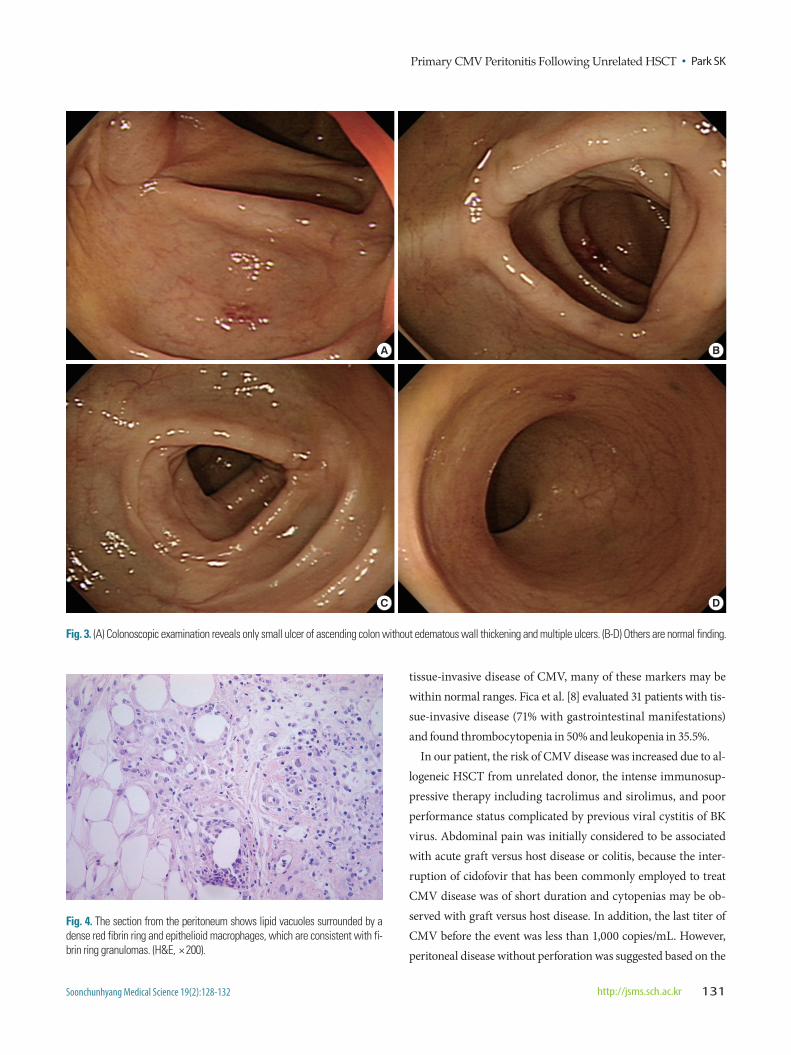
without edematous wall thickening and hemorrhage (Fig. 3). The biopsy of colonic ulcer showed non-specific inflammation with lymphoid follicle. To make a definite diagnosis, the biopsy of peri-toneal lesions was performed using ultrasonography guided gun-biopsy and the result showed the findings of chronic granuloma-
tous peritonitis, including lipid vacuoles surrounded by a dense red fibrin ring and epithelioid macrophages which are consistent with fibrin ring granulomas (Fig. 4). Evaluations of nested PCR for mycobacterium tuberculosis and non-tuberculosis mycobacteria were all negative. In addition, RT-PCR for CMV on paraffin-em-bedded tissue was experimentally performed to confirm CMV disease and the result was positive.
Based on the above findings, he was diagnosed with primary CMV peritonitis without colitis and perforation. To treatment, in-travenous gancyclovir (5 mg/kg/day) therapy was started. After the therapy for 3 weeks, he was over the CMV disease and the CMV titer returned to normal (Fig. 1). Oral feeding was initiated on day +61 after transplantation and the patient’s oral intake increased successfully.
DISCUSSION
Regardless of currently available antiviral strategies, HSCT re-cipients remain at risk for CMV infection not only during the ear-ly post-transplantation period (<100 days), but also later (>100 days) in the post-transplantation course. Whereas the prevalence of early CMV disease has declined to 3% to 6% with intense anti-viral drug use, the risk of late CMV disease has increased over the past few years, with up to 18% of recipients developing disease even when no prevention is administered [7].
Here, we report a case of primary CMV peritonitis after unre-lated HSCT. As CMV peritonitis is usually due to CMV colitis, primary CMV peritonitis not accompanied by CMV colitis is very rare. Disease can occur anywhere in the gastrointestinal tract, but colitis is most frequent, followed by gastritis, and it may range from asymptomatic to perforation or hemorrhage. Among transplant patients with gastrointestinal CMV disease, Fica et al. [8] found that over half reported ‘esophagitis-gastritis’ symptoms, 41% re-ported diarrhea, and 32% reported epigastric or thoracic pain. Gas-trointestinal hemorrhage or perforation occurred in less than 10%. Fever and malaise as a general symptom accompany most cases. Gastrointestinal CMV disease should be differentiated from gas-trointestinal complications after allogeneic HSCT. Transplant pa-tients can present with signs and symptoms of graft rejection or graft-versus host disease. Other common complications include mucositis (90%), vomiting (85%), and abdominal pain (71%) [9]. Laboratory findings associated with CMV disease include throm-bocytopenia, leukopenia, and elevated liver enzymes. However, in
Fig. 2. (A) Axial image and (B) coronal section image of abdominal computer to-mography showed the diffuse fat infiltration of omentum and mesentery with enhanced nodular lesions side by side with right paracolic gutter.
A
B
Primary CMV Peritonitis Following Unrelated HSCT • Park SK
Soonchunhyang Medical Science 19(2):128-132 http://jsms.sch.ac.kr 131
Fig. 3. (A) Colonoscopic examination reveals only small ulcer of ascending colon without edematous wall thickening and multiple ulcers. (B-D) Others are normal finding.
A
C
B
D
Fig. 4. The section from the peritoneum shows lipid vacuoles surrounded by a dense red fibrin ring and epithelioid macrophages, which are consistent with fi-brin ring granulomas. (H&E, × 200).
tissue-invasive disease of CMV, many of these markers may be within normal ranges. Fica et al. [8] evaluated 31 patients with tis-sue-invasive disease (71% with gastrointestinal manifestations) and found thrombocytopenia in 50% and leukopenia in 35.5%.
In our patient, the risk of CMV disease was increased due to al-logeneic HSCT from unrelated donor, the intense immunosup-pressive therapy including tacrolimus and sirolimus, and poor performance status complicated by previous viral cystitis of BK virus. Abdominal pain was initially considered to be associated with acute graft versus host disease or colitis, because the inter-ruption of cidofovir that has been commonly employed to treat CMV disease was of short duration and cytopenias may be ob-served with graft versus host disease. In addition, the last titer of CMV before the event was less than 1,000 copies/mL. However, peritoneal disease without perforation was suggested based on the

Park SK • Primary CMV Peritonitis Following Unrelated HSCT
Soonchunhyang Medical Science 19(2):128-132132 http://jsms.sch.ac.kr
result of computed tomography and colonoscopic findings. And then we performed peritoneal biopsy. We couldn’t find intra-nu-clear inclusion or cytoplasmic inclusions in the peritoneal biopsy because of the limitation of blunt biopsy. CMV has been shown to be a causal agent of chronic granulomatous disease [10] and fibrin ring granuloma of the peritoneal tissue may be seen in a variety of infections including CMV. By follow-up study of CMV and no in-fection evidence on any other sites except peritoneum, CMV dis-ease of peritoneum was strongly suggested. Therefore, we tried to test RT-PCR on paraffin-embedded tissue to confirm CMV dis-ease of peritoneum although it was not routine test. Recently Mills et al. [11] reported the usefulness of PCR method for CMV detec-tion in tissue. The major benefit of this CMV PCR is its use of par-affin-embedded tissue. Prior PCR based investigations of viral load in the biopsies have relied on fresh tissue, which can be diffi-cult to acquire in routine practice. The use of paraffin-embedded tissue allows histologic review before performing PCR, facilitating the selection of the most appropriate block for testing and allow-ing initial testing by immunohistochemical stain. In addition, oth-er potential advantage of the PCR method is its ability to quantify viral burden.
There have been reported only two cases of primary CMV peri-tonitis in immunocompromised patients in the world. Wilcox et al. [12] reported a 29-year-old Hispanic bisexual man with AIDS (acquired immune deficiency syndrome) for the first time. He was admitted to hospital for severe abdominal pain, and surgical treat-ment was done. And then CMV peritonitis could be confirmed by the biopsy of lesions. There was absence of intestinal or colonic perforation. Second case was a renal transplantation patient with CMV peritonitis after administering anti-CD52 antibody alemtu-zumab combined with methylprednisone, followed by a sequential immunosuppressive therapy with tacrolimus [13]. She was admit-ted because of abdominal pain and persistent leucopenia. In the second case report, CMV peritonitis was diagnosed by perform-ing quantitative RT-PCR of the culture-negative peritoneal fluid and routine CMV monitoring using CMVpp65 antigen initially failed to identify CMV peritonitis. Therefore, authors suggested complications of CMV disease might be under-diagnosed in im-munocompromised patients due to the sensitivity of CMV moni-
toring method. Cases of CMV peritonitis including our case were successfully treated with intravenous ganciclovir treatment.
In conclusion, we here report primary CMV peritonitis without colitis or bowel perforation after allogeneic HSCT from unrelated donor. Meticulous monitoring for CMV by high quantitative RT-PCR is mandatory in patients of allogeneic HSCT.
REFERENCES
1. Cannon MJ, Schmid DS, Hyde TB. Review of cytomegalovirus seroprev-alence and demographic characteristics associated with infection. Rev Med Virol 2010;20:202-13.
2. Yoo KH, Lee SH, Sung KW, Koo HH, Chung NG, Cho B, et al. Current status of pediatric umbilical cord blood transplantation in Korea: a mul-ticenter retrospective analysis of 236 cases. Am J Hematol 2011;86:12-7.
3. Monkemuller KE, Wilcox CM. Diagnosis and treatment of colonic dis-ease in AIDS. Gastrointest Endosc Clin N Am 1998;8:889-911.
4. Boeckh M, Boivin G. Quantitation of cytomegalovirus: methodologic as-pects and clinical applications. Clin Microbiol Rev 1998;11:533-54.
5. Marty FM, Ljungman P, Papanicolaou GA, Winston DJ, Chemaly RF, Stras-feld L, et al. Maribavir prophylaxis for prevention of cytomegalovirus dis-ease in recipients of allogeneic stem-cell transplants: a phase 3, double-blind, placebo-controlled, randomized trial. Lancet Infect Dis 2011;11: 284-92.
6. Feasey NA, Healey P, Gordon MA. Review article: the aetiology, investi-gation and management of diarrhoea in the HIV-positive patient. Aliment Pharmacol Ther 2011;34:587-603.
7. Einsele H, Hebart H, Kauffmann-Schneider C, Sinzger C, Jahn G, Bader P, et al. Risk factors for treatment failures in patients receiving PCR-based preemptive therapy for CMV infection. Bone Marrow Transplant 2000; 25:757-63.
8. Fica A, Cervera C, Perez N, Marcos MA, Ramirez J, Linares L, et al. Im-munohistochemically proven cytomegalovirus end-organ disease in solid organ transplant patients: clinical features and usefulness of conventional diagnostic tests. Transpl Infect Dis 2007;9:203-10.
9. Barker CC, Anderson RA, Sauve RS, Butzner JD. GI complications in pe-diatric patients post-BMT. Bone Marrow Transplant 2005;36:51-8.
10. Zumla A, James DG. Granulomatous infections: etiology and classifica-tion. Clin Infect Dis 1996;23:146-58.
11. Mills AM, Guo FP, Copland AP, Pai RK, Pinsky BA. A comparison of CMV detection in gastrointestinal mucosal biopsies using immunohisto-chemistry and PCR performed on formalin-fixed, paraffin-embedded tissue. Am J Surg Pathol 2013;37:995-1000.
12. Wilcox CM, Forsmark CE, Darragh TM, Yen TS, Cello JP. Cytomegalo-virus peritonitis in a patient with the acquired immunodeficiency syn-drome. Dig Dis Sci 1992;37:1288-91.
13. Meier M, Hiss M, Hafer C, Buth W, Radermacher J, Haller H, et al. Cyto-megalovirus peritonitis after renal transplantation under induction ther-apy with alemtuzumab in a young woman previously treated with perito-neal dialysis. Nephrol Dial Transplant 2005;20:1771.