Prevention of fatty liver in transition dairy cows by ...
78
Retrospective Theses and Dissertations Iowa State University Capstones, Theses and Dissertations 1-1-2004 Prevention of fatty liver in transition dairy cows by subcutaneous Prevention of fatty liver in transition dairy cows by subcutaneous glucagon injections glucagon injections Rafael Albertovich Nafikov Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/rtd Recommended Citation Recommended Citation Nafikov, Rafael Albertovich, "Prevention of fatty liver in transition dairy cows by subcutaneous glucagon injections" (2004). Retrospective Theses and Dissertations. 20207. https://lib.dr.iastate.edu/rtd/20207 This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected].
Transcript of Prevention of fatty liver in transition dairy cows by ...

Retrospective Theses and Dissertations Iowa State University Capstones, Theses and Dissertations
1-1-2004
Prevention of fatty liver in transition dairy cows by subcutaneous Prevention of fatty liver in transition dairy cows by subcutaneous
glucagon injections glucagon injections
Rafael Albertovich Nafikov Iowa State University
Follow this and additional works at: https://lib.dr.iastate.edu/rtd
Recommended Citation Recommended Citation Nafikov, Rafael Albertovich, "Prevention of fatty liver in transition dairy cows by subcutaneous glucagon injections" (2004). Retrospective Theses and Dissertations. 20207. https://lib.dr.iastate.edu/rtd/20207
This Thesis is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected].

Prevention of fatty liver in transition dairy cows by subcutaneous glucagon
injections
by
Rafael Albertovich Nafikov
A thesis submitted to the graduate faculty
in partial fulfillment of the requirements for the degree of
MASTER OF SCIENCE
Major: Animal Nutrition
Program of Study Committee: Donald C. Beitz, Major Professor
Ronald L. Horst Kenneth J. Koehler
James M. Reecy
Iowa State University Ames, Iowa
2004
Copyright© Rafael Albertovich Nafikov, 2004. All rights reserved.

ii
Graduate College Iowa State University
This is to certify that the master's thesis of
Rafael Albertovich Nafikov
has met the thesis requirements of Iowa State University
Signatures have been redacted for privacy

iii
TABLE OF CONTENTS
LIST OF FIGURES iv
GENERAL INTRODUCTION Thesis Organization 1 Literature Review 1
Introduction 1 Etiology of Fatty Liver Disease 2 Glucagon and Its Involvement in Regulation of Glucose Homeostasis 8 Gluconeogenesis 15 Preventatives and Treatments of Fatty Liver Disease 20
PREVENTION OF FATTY LIVER IN TRANSITION DAIRY COWS BY 14-DAY SUBCUTANEOUSE GLUCAGON INJECTIONS Abstract Introduction Materials and Methods
Experimental Design Sampling and Analysis Statistical Analysis
Results Discussion Conclusions Acknowledgments References
GENERAL CONCLUSIONS General Discussion Recommendations for Future Research
REFERENCES
ACKNOWLEDGMENTS
24 25 28 28 29 32 33 44 51 52 52
58 60
63
72

iv
LIST OF FIGURES
GENERAL INTRODUCTION
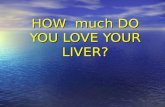
Figure 1. Mechanism of fatty liver development in transition dairy cows 4
Figure 2. The "two hits" hypothesis of nonalcoholic steatohepatitis 7
Figure 3. Pancreatic processing of preproglucagon 9
Figure 4. Intestinal cell processing of preproglucagon 10
Figure 5. Signal transduction pathway for glucagon 12
Figure 6. Regulatory signal transduction pathway of hepatic gluconeogenesis 14 and fatty acid oxidation
Figure 7. Glucose biosynthesis from different gluconeogenic precursors in 17 ruminant animals
PREVENTION OF FATTY LIVER IN TRANSITION DAIRY COWS BY 14-DAY SUBCUTANEOUSE GLUCAGON INJECTIONS
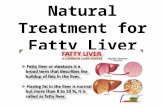
Figure 1. Liver lipid composition of cows treated with saline, 7.5, and 15 mg/d 34 of glucagon
Figure 2. Liver glycogen concentration of cows treated with saline, 7 .5, 35 and 15 mg/d of glucagon
Figure 3. Plasma metabolite concentrations of cows treated with saline, 7.5, 37 and 15 mg/d of glucagon
Figure 4. Plasma hormone concentrations of cows treated with saline, 7 .5, 39 and 15 mg/d of glucagon
Figure 5. Milk production of cows treated with saline, 7.5, and 15 mg/d 40 of glucagon
Figure 6. Milk composition of cows treated with saline, 7.5, and 15 mg/d 41 of glucagon

v
Figure 7. Feed intake of cows treated with saline, 7.5, and 15 mg/d of glucagon
Figure 8. Body condition scores of cows from saline, 7.5, and 15 mg/d of glucagon treatment groups
43
45

1
GENERAL INTRODUCTION
Thesis Organization
This thesis is presented as one paper prepared for the submission to the Journal of
Dairy Science from research performed to partly fulfill the requirements for a Master of
Science degree. The paper is complete in itself including an abstract, introduction, materials
and methods, results, discussion, conclusions, and references. A title of the paper is
"Prevention of fatty liver in transition dairy cows by 14-day subcutaneous glucagon
injections". The data from the paper indicate the potential use of a peptide hormone glucagon
for fatty liver prevention in transition dairy cows. The paper is preceded by a literature
review and followed by general conclusions containing a general discussion and
recommendations for future research sections. References conclude the thesis.
Literature Review
Introduction.
Fatty liver (hepatic lipidosis) is a metabolic disorder of dairy cows that occurs
generally during the first two weeks of lactation and is characterized by excessive lipid
accumulation in the liver. However, cows can develop fatty liver at any other time during

2
lactation because of many different reasons. The prevalence of fatty liver can be up to 54%
of a dairy herd (Jorritsma et al., 2000a), and the morbidity and mortality from this syndrome
may reach 90 and 25%, respectively (Raoofi et al., 2001). The consequences of fatty liver
development in dairy cows can be attributed to their reduced productivity, reproductive
performance, suppressed immunity, and increased susceptibility to different infectious and
metabolic diseases (Bremmer et al., 2000; Jorritsma et al., 2000a; Raoofi et al., 2001). In
particular, cows prone to fatty liver can develop ketosis, milk fever, udder edema, displaced
abomasum, retained fetal membranes, metritis, and mastitis (Drackley, 1999; Katoh, 2002;
Morrow, 1976; Van Winden et al., 2003). Metabolic disorders such as fatty liver, milk fever,
and ketosis tend to occur in complexes and probably could have some general cause.
Accumulation of high amounts of triacylglycerols (TAG) by liver of lactating dairy cows is
highly correlated with their decreased fertility and an increase in the interval from parturition
to first ovulation (Jorritsma et al., 2000b; Rukkwamsuk et al., 1999b). Fatty liver
development during the first two weeks postpartum is associated with decreased functional
capacities of polymorphonuclear neutrophilic granulocytes derived from blood and uterus,
which may be why cows with fatty liver have a higher incidence of infectious diseases such
as endometritis (Zerbe et al., 2000).
Etiology of Fatty Liver Disease.
Dairy cows after parturition are in a negative energy balance (NEB) state. This means
that their feed intake and body reserves cannot supply enough energy and nutrients for
maintenance and milk production. With the onset of lactation, cows have increased
requirements for glucose production, which is used as a fuel and for lactose biosynthesis.

3
High demands for glucose in dairy cows at the beginning of lactation exacerbate the energy
deficit. One of the reasons for cows not being able to meet their energy needs is a decline in
their feed intake a few days before calving. After parturition, feed intake of dairy cows rises
much slower than their energy needs.
To meet their energy and glucose production needs, cows mobilize TAG from
adipose tissue and use nonesterified fatty acids (NEFA) as a primary energy source. Thereby,
they can repartition glucose towards lactose biosynthesis. For some reasons, cows in a NEB
mobilize more TAG than they can utilize, which leads to an increased blood NEF A
concentration. A high blood NEF A concentration is considered to be one of the major risk
factors for the development of fatty liver disease (Herdt, 1988).
In liver, NEFA can undergo mitochondrial (Figure 1) or peroxisomal ~-oxidation to
acetyl-CoA, which is oxidized to carbon dioxide in the citric acid cycle with concomitant
ATP production or uncoupling of oxidative phosphorylation and production of reactive
oxygen species (ROS). Alternatively, NEFA can undergo incomplete oxidation with
production of ketone bodies. In addition, NEFA can be esterified into TAG and stored in the
liver. Triacylglycerols can be used for production of very low density lipoproteins (VLDL),
which are secreted into the blood stream (Gruffat et al., 1996). An imbalance between
complete and incomplete NEF A oxidation, production and secretion of VLDL, and TAG
formation and storage in liver can lead to the development of hepatic steatosis.
High blood NEFA concentration in dairy cows is highly correlated with fatty liver
development postpartum. The hepatic uptake of NEF A depends on its concentration in blood
and the rate of blood flow to the liver (Gruffat et al., 1996). Therefore, higher blood NEFA
concentration results in more fatty acid being taken up by liver. Ruminant animals are known

L., Jl.v
er
·-r ~
N· ·.'·E
· ;F··A
.. -. •
. '
• >
.
. .
. •.·
'
..
Bl{~~d·l
~
'V'
_ .... r
, N
E.·jl.Bf.
y ('.
' '
.. ~.
< ~ •
•• '. •
• ,.~,,..
'h
.....
. ~
I a
n·
!d··1
, r .
. j.
-~
--H I
.. ___
ypog
y·ce
rn1a
~
Adi
t ..
-·-r_~pose tis
sue
Fig
ure
1.
Mec
hani
sm o
f fa
tty
live
r de
velo
pmen
t in
tra
nsit
ion
dair
y co
ws.
N
EF
A,
none
ster
ifie
d fa
tty
acid
s; T
AG
, tr
iacy
lgly
cero
ls;
VL
DL
, ve
ry lo
w d
ensi
ty li
popr
otei
ns; N
EB
, neg
ativ
e en
ergy
bal
ance
.
.j:::
.

5
to have a relatively low capacity for production and secretion of VLDL from the liver
(Hocquette and Bauchart, 1999). So, the inability of liver to oxidize all NEPA that enters it
and impaired production and/or secretion of VLDL can lead to TAG accumulation and fatty
liver development.
Impairment in production and secretion of VLDL by the liver is considered as one of
the factors that contributs to the development of fatty Ii ver disease postpartum in dairy cows
(Bremmer et al., 2000; Katoh, 2002). The rate of liver TAG synthesis in ruminants and
nonrurninants is similar, but the rate of their secretion via VLDL is much slower in ruminants
than in nonruminants (Bremmer et al., 2000; Pullen et al., 1990). A possible explanation for
this could be the fact that ruminants, unlike nonruminants, use adipose tissue as a major site
for fatty acid synthesis, and as such, they do not need to have as good a mechanism for TAG
secretion from the liver (Katoh, 2002).
Cows with fatty liver disease have reduced VLDL secretion (Rayssiguier et al., 1988)
by the liver. Reduction in the secretion of VLDL from cows with fatty liver was attributed to
lower concentrations of apolipoprotein B-100 (apoB-100), which is a TAG-binding protein
that required for assembly of VLDL particles (Pullen et al., 1990; Yamamoto et al., 1995).
The apoB-100 rnRNA concentration in liver does not decrease substantially during earlier
stage of lactation, which indicates that apoB-100 concentration may be regulated
posttranslationally by proteolytic degradation of apoB-100 protein (Gruffat et al., 1997). The
reasons for increased proteolytic degradation of apoB-100 postpartum are not known.
Because of the high correlation between elevated blood NEPA concentration and
fatty liver development in transition dairy cows (Herdt et al., 1988), there have been several
attempts to relate the fatty acid composition of liver, blood NEPA, and adipose tissue to the

6
etiology of fatty liver development (Rukkwamsuk et al., 2000; Sato et al., 2004). Cows with
fatty liver disease had higher concentrations of palmitic, oleic, linoleic, but not stearic acid,
in liver. However, the composition of fatty acids in adipose tissue was the same in healthy
and fatty liver cows before and after parturition (Rukkwamsuk et al., 2000). Palmitic, stearic,
and oleic acids were the major fatty acids found in adipose tissue and blood. Different
feeding strategies (feed restriction or overfeeding) did not affect fatty acid composition in
adipose tissue and plasma.
Hepatic steatosis occurs in two forms: microvesicular and macrovesicular (Haque and
Sanyal, 2002). Microvesicular steatosis is characterized by cytoplasmic accumulation of
numerous small, fat-filled, globules that do not cause displacement of the nucleus. This
condition is associated with disorders of the urea cycle, which results in mitochondrial
abnormalities and hyperammonemia. Macrovesicular steatosis is characterized by
cytoplasmic accumulation of one or two large globules of fat, which causes displacement of
the nucleus to the periphery of the hepatocyte.
Even though there is a lack of the information about histopathological studies of fatty
liver cases in dairy cows, at least mild fatty liver in dairy cows could be characterized as a
microvesicular steatosis. This assumption is supported by data indicating that cows with fatty
liver could have mitochondrial dysfunction and suppressed ureagenesis (Hocquette and
Bauchart, 1999; Reid and Collins, 1980; Strang et al., 1998). However, severe fatty liver in
dairy cows could be an example of macrovesicular steatosis, which can develop into
steatohepatitis and/or fibrosis with the possible progression of fibrosis into cirrhosis.
It is obvious that fatty liver itself is not just an innocent lipid accumulation. Two main
pathways of liver injury are considered to be responsible for the pathogenesis of fatty liver-

7
oxidative stress-induced lipid peroxidation and cytokine-mediated injury (Day, 2002).
According to the "two-hit" hypothesis (Figure 2), high blood NEPA concentration can cause
steatosis (lipid accumulation by liver), which is "the first hit". Then, steatosis itself makes
liver vulnerable for "the second hit"-oxidative stress, endotoxin, and ATP depletion (Day,
2002).
The second 'hits'
Normal fa'./ content
The first 'hit'
t Peroxidation t Sensitivity to
TNF-a
Figure 2. The 'two hits' hypothesis of nonalcoholic steatohepatitis. ATP, adenosine triphosphate; MMPT, mitochondrial membrane permeability transition; UCP-2, uncoupling protein 2; TNF-a, tumor necrosis factor-a. Adopted from Day, 2002.

8
Glucagon and Its Involvement in Regulation of Glucose Homeostasis.
Glucagon is a 29-amino acid peptide hormone that is produced and secreted by the a-
cells of the islets of Langerhans in the pancreas (Drucker, 1990). In addition to the pancreas,
the glucagon gene expression also is observed in the small and large intestine, stomach, and
brain. However, instead of producing glucagon these other tissues produce different bioactive
peptides. The proglucagon cDNAs isolated from all these tissues are identical, which
indicates that the glucagon gene produces a single and unique mRNA transcript, despite
tissue specific glucagon gene localization.
Translation of glucagon mRNA results in a 180-amino acid peptide called
preproglucagon, which contains 20-amino acid signal peptide. After elimination of the signal
peptide, the ' 160-amino acid preglucagon peptide undergoes endoproteolytic processing in a-
cells of the pancreas (Figure 3) and intestinal L-cells (Figure 4), which leads to the
production of tissue specific bioactive peptides. Prohormone convertases 1 and 2 (PCl and
PC2) are responsible for tissue-specific posttranslational processing of the preglucagon
molecule (Tucker et al., 1996). The prohormone convertase 1 is localized in intestinal L
cells, and PC2 is localized in pancreatic a-cells. Posttranslational processing of preglucagon
molecule in pancreatic a-cells by PC2 leads to the production of glucagon, a 29-amino acid
peptide. However, preglucagon processing in intestinal L-cells leads to the production of
glicentin, oxyntomodulin, glucagon-like peptide 1 (GLP-1), and small amounts of glucagon
like peptide 2 (GLP-2) and intervening peptide 2 (IP-2).
Presence of the glucagon sequence in glicentin and oxyntomodulin makes these
peptides reactive with antisera against glucagon (Holst, 1997), which sometimes makes
determination of glucagon concentration by radioimmunoassays a bit challenging .

,-----------------------~
I P
RE
PR
OG
LU
CA
GO
N
\
2HN-ll
~-I GR
PP l-ll
•l-EJ
-IGLP-
1 H1PHGLP-II~COOH
.·.·.·.·.
·.·.·.·.·.
·.·.·.·.·
.·.·.·.·.
·.·.·.·.·
.·.·.·.·.·
.·.·.·.
----
----
---
,'
PR
OG
LU
CA
GO
N --
----
, \
2HN-l!~11111
+
IGRPP1-1
;:;:;:;:
;:;:;:;:
;:;:;:;:
;:;:;:;:
;:;:;:;:
;:;:;:;:
;:;:;:;:
;:;:;:;:
;:;:;:;:
;1__Q_~-1o
r-~ lDlll(l!f~ L
P-II C
OOH
~ s
ecre
ted
fro
m a
-cell
:,.,.,.,.,.,.,
.,.,.,.,.,.,.,.,
.;.,.,.,.,.,.,.,
.,.,.,.,.,_,_,_,
_,_,_,_,_,
IP
~ 1=
?=/:/)
====
=:::==
::::::::
:::I ~
11:~1
!~11:
!~1!
I GL
P-1
H IPHGL
P-II
~COO
H m
ajo
r p
rog
luca
go
n
\ fr
agm
ent
~
----
----
--F
igu
re 3
. Pan
crea
tic
proc
essi
ng o
f pre
prog
luca
gon.
GR
PP
, gl
icen
tin-
rela
ted
panc
reat
ic p
epti
de;
IP, i
nter
veni
ng p
epti
de; G
LP
-1
and
GL
P-11
, glu
cago
n-li
ke p
epti
de 1
and
2, r
espe
ctiv
ely.
\0

,~----------------------~
I P
RE
PR
OG
LU
CA
GO
N
'
2HN-~[
IJll!l I
GRPP
1«
•-eJ
-loLP-
r HrP
HGLP-rr~cooH
2 HN-llilll
l +
~ I GR
PP H~l•ll
\l-@-
loLP
-I HrPHoLP-rr~cooH
\ I
-~----
-~
I G
lie e
n ti
n
I I G
LP-I
I
~ I GR
PP I
j O
xy
nto
mo
du
lin
I
~
secr
eted
fro
m
du
od
enal
L c
ells
~loLP-nf-cooH
Fig
ure
4. I
ntes
tina
l ce
ll pr
oces
sing
of
prep
rogl
ucag
on.
GR
PP
, gl
icen
tin-
rela
ted
panc
reat
ic p
epti
de;
IP,
inte
rven
ing
pept
ide;
G
LP-
1 an
d G
LP-
11,
gluc
agon
-lik
e pe
ptid
e 1
and
2, r
espe
ctiv
ely.
........
. 0

11
Pancreatic glucagon and intestinal GLP-1 have attracted the most attention because of
their biological activities. Glucagon-like peptide 1 can stimulate insulin secretion even in
patients with severe type-2 diabetes mellitus and can inhibit glucagon secretion (Drucker et
al., 2000; Holst, 1997). In addition, GLP-1 may increase glucose uptake and insulin
sensitivity. The unique feature of GLP-1 is its very short half-life, which makes difficult to
study or to use that peptide for therapeutic purposes.
Glucagon is secreted from the pancreas in a pulsatile fashion, and such a delivery of
glucagon is more effective in stimulating hepatic glucose output in vivo (Jiang and Zhang,
2003). Glucagon signals via its receptor, which is localized to the liver, adipose, kidney,
heart, spleen, pancreatic islets, ovary, and thymus (Unson, 2002). At least two classes of G
protein coupled receptors, namely Gha and Gq, are involved in signal transduction pathways
associated with glucagon signalling (Jiang and Zhang, 2003). The activation of the Gha class
of glucagon receptors leads to the activation of adenylate cyclase (Figure 5), increase in
intracellular cAMP concentration, and activation of protein kinase A (PKA). Glucagon
signalling through this pathway is involved in the regulation of hepatic glucose output by
activating PKA, which results in a stimulation of glycogenolysis and gluconeogenesis and
inhibition of glycogenesis and glycolysis. The activation of Gq class of glucagon receptors
leads to the activation of phospholipase C, production of inositol 1,4,5-triphosphate, and
subsequent release of intracellular calcium. Diacylglycerol, the product of
phosphatidylinositol 4,5-bisphosphate hydtrolysis by phospholipase C, binds in concert with
calcium ions to protein kinase C and thereby activates PKA. Activated protein kinase C and
increased intracellular calcium concentration can have an effect on different metabolic
pathways regulated by glucagon.

DA
G G
l•11 C~GtJft
! .F~ ·w
'°'~"' -~
!
~~
•:
• \
-,,
2+
\ •
.. ca
'
W"
, ~
'A.
e C
a2+
~M
·p·
c ..
/: .. '.
"'
; ¥
Fig
ure
5. S
igna
l tr
ansd
ucti
on p
athw
ay f
or g
luca
gon.
Ga,
G~, a
nd G
y, G
-pro
tein
's a
, ~
' an
d y
subu
nits
, re
spec
tive
ly;
PL
C,
phos
phol
ipas
e C
; P
IP2,
ph
osph
atid
ylin
osit
ol 4
,5-b
isph
osph
ate;
DA
G,
diac
ylgl
ycer
ol;
IP3,
in
osit
ol
1,4,
5-tr
ipho
spha
te;
Ca2
+,
calc
ium
ion;
AT
P, a
deno
sine
trip
hosp
hate
; cA
MP
, cyc
lic
aden
osin
e m
onop
hosp
hate
; P
KA
, pro
tein
kin
ase
A.
-N

13
Regulation of hepatic gluconeogenesis is achieved by the combined action of
glucagon and insulin. Glucagon activates hepatic gluconeogenesis. It binds to a glucagon
receptor and stimulates production of the cyclic AMP ( cAMP), a cell second messenger
molecule. Cyclic AMP activates PKA, which phosphorylates cAMP response element
binding (CREB) protein (Figure 6). Phosphorylated CREB protein activates peroxisome
proliferative activated receptor-y co-activator 1 (PGC-1) gene expression (Herzig et al.,
2001). Recently, it was discovered that PGC-1, found before in skeletal muscle and brown
fat, is also involved in the regulation of hepatic gluconeogenesis (Yoon et al., 2001).
Peroxisome proliferative activated receptor-y co-activator 1 binds to hepatic nuclear factor-4a
(HNF-4a) and forkhead transcription factor (FOXOl). This binding of PGC-1 can co-activate
the expression of gluconeogenic enzymes such as phosphoenolpyruvate carboxykinase
(PEPCK) and glucose-6-phosphatase (Figure 6).
Interaction between transcription factor FOXOl and co-activator PGC-1 is required
for robust activation of gluconeogenesis (Puigserver et al., 2003). Insulin suppresses hepatic
gluconeogenesis by disrupting the interaction of FOXO 1 and PGC-1. This suppression is
achieved by insulin-stimulated phosphorylation of FOXOI through protein kinase B (PKB)
and Akt protein kinase (Akt) pathway (Figure 6). FOXOl phosphorylation does not only
disrupt the interaction of FOXO 1 and PGC-1, but also excludes FOXO 1 from the nucleus
(Puigserver et al., 2003).
Glucagon is not only involved in the regulation of hepatic gluconeogenesis, but it also
activates fatty acid oxidation by up-regulating gene expression of liver carnitine
palmitoyltransferase 1 (L-CPT 1) enzyme (Louet et al., 2002). Liver camitine
palmitoyltransferase 1 gene has to bind both phosphorylated CREB protein and HNF-4a

Gtu
ca
go
n
+ ..
)KA
L-C
PT
1 g
en
e
PE
PC
K g
en
e
Ins
uli
n
. . . .. P
'KB
. . .. Ak
t ~-··
........
"'11
l.1"
····~
. . . ·.:.it
Inh
ibit
ion
Fig
ure
6. R
egul
ator
y si
gnal
tra
nsdu
ctio
n pa
thw
ay o
f he
pati
c gl
ucon
eoge
nesi
s an
d fa
tty a
cid
oxid
atio
n. P
KA
, pr
otei
n ki
nase
A;
PG
C-1
, per
oxis
ome
prol
ifer
ativ
e ac
tiva
ted
rece
ptor
-y c
o-ac
tiva
tor
1; C
RE
B, c
AM
P r
espo
nse
elem
ent b
indi
ng p
rote
in;
HN
F-4
a,
hepa
tocy
te n
ucle
ar f
acto
r-4a
; L
-CP
T,
cam
itin
e pa
lmit
oylt
rans
fera
se;
PK
B,
prot
ein
kina
se B
; A
kt,
Akt
pro
tein
kin
ase;
FO
XO
l,
fork
head
tra
nscr
ipti
on f
acto
r; P
EP
CK
, pho
spho
enol
pyru
vate
car
boxy
kina
se.
-+:-

15
transcription factor to become active (Figure 6). Binding of PGC-1 co-activator to HNF-4a
transcription factor can strongly up-regulate L-CPT I gene expression. So, glucagon can
regulate L-CPT I gene expression through abundance of PGC-1 co-activator in the nucleus
(Louet et al., 2002). Adequate regulation of fatty acid oxidation is required for the prevention
of fatty liver development in dairy cows, because L-CPT I enzyme activity is lower in cows
with fatty liver (Mizutani et al., 1999).
Gluconeogenesis and fatty acid oxidation can also be regulated by nutritional means.
For example, HNF-4a transcription factor is involved in the regulation of both
gluconeogenesis and fatty acid oxidation (Hertz et al., 1998; Louet et al., 2002). Fatty acids
in the form of CoA thioesters can modulate the transcriptional activity of HNF-4a gene and
affinity of HNF-4a transcription factor for enhancers and/or promoter region on target genes
(Figure 6). Agonistic ligands of HNF-4a include fatty acyl-CoAs of C14:0 and C16:0 fatty
acids, whereas antagonistic ligands include w-3, w-6, and C18:0 fatty acyl-CoAs (Hertz et
al., 1998).
Gluconeogenesis.
Control of glucose metabolism postpartum is one of the major metabolic challenges
with which a dairy cow must cope. At the beginning of lactation, dairy cows have a great
demand for glucose, which is used primarily for lactose production in milk synthesis
(Overton et al., 1998).
The formation of glucose from nonhexose precursors is called gluconeogenesis.
Gluconeogenesis occurs primarily in liver and to a lesser extend in the kidney. The main
precursors for gluconeogenesis in dairy cows are propionate, some amino acids (mainly

16
alanine and glutamate), lactate, and glycerol (Greenfield et al., 2000a). The importance of
gluconeogenesis for dairy cows can be explained by the fact that only small amounts of
carbohydrates can escape microbial fermentation in the rumen and subsequently be available
for hydrolysis to glucose in the small intestine. The vast majority of the glucose used by a
dairy cow is endogenously produced via gluconeogenesis.
Propionate is converted first to succinyl-CoA in a series of reactions in which
propionyl-CoA carboxylase catalyzes the rate-limiting step (Figure 7). Glutamate is
converted to a-ketoglutarate. Then, both succinyl-CoA and a-ketoglutarate is converted to
oxaloacetate via TCA cycle. Oxaloacetate is exported from the mitochondrion into the
cytosol, where it is used for phosphoenolpyruvate production by PEPCK. Two molecules of
phosphoenolpyruvate are converted to one molecule of glucose via gluconeogenesis, and
glucose is released into a blood stream from the liver.
Alanine and lactate have to be converted to pyruvate before they can enter
gluconeogenesis (Figure 7). Pyruvate is then converted to oxaloacetate by pyruvate
carboxylase, which after conversion to phosphoenolpyruvate can undergo reverse glycolysis.
Glycerol undergoes changes to fructose 1,6-bisphosphate, which enters gluconeogenesis
(Figure 7). The rate-limiting step for the conversion of glycerol to glucose is a reaction
catalyzed by fructose 1,6-bisphosphatase.
In ruminants, PEPCK and glucose-6-phosphatase are the principal enzymes
responsible for the regulation of glucose production. The explanation for this phenomenon is
illustrated by the fact that the majority of the glucose in ruminants is produced from
propionate. Consequently, PEPCK is a good regulatory point. The appropriateness of using
glucose-6-phosphatase to regulate blood glucose concentration comes from the fact that this

Phosphoenol pyruvate
carboxykinase
Oxaloacetate ..
Pyruvate carboxylase
Pyruvate
/\
17
Glucose
Glucose-6-phosphatase
Fructose 1, 6-bisphosphatase
.ill ~ Glycerol
Phosphoenol
·. ·.
pyruvate
···· ... .
TCA cycle
Alanine L<lctate
ProJJionyl-C:ofi carboxylase
Propionate Glutamate
Figure 7. Glucose biosynthesis from different gluconeogenic precursors in ruminant animals. TCA cycle, tricarboxylic acid cycle.

18
enzyme can catalyze the conversion of glucose-6-phosphate, produced by glycogen
degradation, to glucose independent of gluconeogenesis.
Amino acids such as alanine and glutamate are considered to be important
gluconeogenic precursors in addition to propionate during the first two or three weeks of
lactation. However, it is very important not to overestimate the significance of amino acids as
gluconeogenic precursors at the beginning of lactation. The concentration of ammonia and
glutamine, and blood ammonia to urea ratio increases right after parturition (Zhu et al.,
2000). This indicates dysfunction of ureagenesis, which is accentuated by liver TAG
accumulation right after calving. Furthermore, amino acids have to be deaminated before
they can enter gluconeogenesis. The extra ammonia released as a result of amino acid
deamination leads to an increased blood ammonia concentration and possible overloading of
the urea cycle.
The feeding of extra rumen-undegradable protein (RUP) to ruminant animals before
and after parturition has been proposed to create a pool of extra amino acids that could be
used for glucose biosynthesis. However, feeding high amounts of crude protein (CP) and
RUP (CP=16 and 18%, RUP=33 and 40% on dry matter basis) to dairy cows during 28 days
before parturition resulted in decreased feed intake and milk production postpartum
(Greenfield et al., 2000b ). This result can be explained by the fact that excess of protein in a
diet could overwhelm the ability of liver to detoxify ammonia to urea at calving and right
after it. Consequently, the current NRC guidelines for protein content in diets of dry cows
(12% CP and 26% RUP on dry matter basis) seems adequate (Greenfield et al., 2000b).
Feeding extra RUP to dairy cows with fatty liver postpartum led to further TAG
accumulation by the liver and did not have an effect on gluconeogenesis (Murondoti et al.,

19
2002). In summary, even though alanine and glutamate are good substrates for glucose
biosynthesis, it is not reasonable to focus on them as a potential solution to the problem of
glucose production during the first weeks of lactation.
During lactation, hepatic gluconeogenesis is the major source of glucose production
in ruminants (Young, 1977). Therefore, there was an attempt to evaluate the effects of
overfeeding during a dry period together with fatty liver development on the function of key
gluconeogenic enzymes around parturition (Rukkwamsuk et al., 1999a). The activity of
PEPCK in the liver of cows overfed during a dry period was significantly lower than that in
the liver of control cows. The possible explanation underlying this finding is that overfed
cows were able to get most of their glucose from the ration, and, because of that, the rates of
their hepatic gluconeogenesis were low. The activity of PEPCK continued to be low after
parturition in the liver of overfed cows because of low adaptability of their livers to
gluconeogenesis during the dry period. Overfed cows had higher rates of lipolysis and,
consequently, higher glycerol concentration in blood. However, the increase in blood
glycerol concentration did not change the activity of liver fructose 1,6-bisphosphatase in
overfed cows. Possibly, blood glycerol concentration was not high enough to cause an
increase in the function of the enzyme. Surprisingly, the activity of glucose-6-phosphatase
was higher postpartum in the liver of overfed cows. Those cows possibly had higher rates of
glycogen degradation than did control cows because of limited availability of glucose from
gluconeogenesis in overfed cows.
The decreased rates of hepatic gluconeogenesis in fatty liver cows could be explained
not only by feeding high energy diet during dry period (Rukkwamsuk et al., 1999a), but also
by a fat infiltration of liver tissue itself (Cadomiga-Valino et al., 1997). Interestingly,

20
glucagon was able to increase the rates of hepatic gluconeogenesis regardless of whether
liver tissue had high TAG concentration or not (Cadomiga-Valino et al., 1997).
Preventatives and Treatments of Fatty Liver Disease.
Fatty liver, ketosis, and other peripaturient diseases associated with them decrease
productivity, reproductive performance, and well being of dairy cows. These all together
contribute to economic losses of dairy producers. Development of a preventive and/or
treatment for pathological fatty liver would place a tool in the hands of veterinarians and
dairy farmers that would improve the productivity, health, and well being of many cows thus
resulting in major savings for dairy producers.
Many research groups are trying to use different strategies to prevent or treat fatty
liver disease. There was an attempt to decrease blood NEFA and liver TAG concentrations
without decreasing blood glucose concentration and feed intake in healthy dairy cows during
the first week of lactation by a single intramuscular injection of several doses of slow-release
insulin (Hayirli et al., 2002). The results of this study showed that, even though there was
some decrease in blood NEF A and liver TAG concentrations and increase in dry matter
intake and milk production after insulin administration, high blood insulin concentration was
not able to suppress lipolysis from adipose tissue sufficiently because of existence of some
degree of insulin resistance in dairy cows right after calving.
Another attempt to decrease blood NEFA concentration and prevent liver TAG
accumulation in dairy cows postpartum was done by using a 3-day drenching with 500 ml of
propylene glycol, 454 g of fat, or the combination of both beginning at day 0 postpartum
(Pickett et al., 2003). Even though drenching with propylene glycol decreased blood NEFA

21
concentration in dairy cows during the first 21 days postpartum, it did not have any effects on
liver TAG concentration. The possible explanation to the inability of propylene glycol to
decrease liver TAG concentration lies in the magnitude of a difference in blood NEFA
concentration between control and the treatment group. The difference was not big enough to
cause any changes in liver TAG concentration.
Dairy cows have a low capacity for synthesis and secretion of VLDL from liver,
which is considered to be a contributing factor for the development of fatty liver disease
(Grummer, 1993). Increasing VLDL synthesis and secretion could prevent and/or treat fatty
liver. There was an attempt to feed extra rumen-protected choline (RPC) during
periparturient period to increase phosphatidylcholine synthesis and VLDL production and
secretion in dairy cows (Piepenbrink and Overton, 2003). There were no changes in plasma
BHBA, NEFA and liver TAG concentrations after feeding extra RPC. However, the hepatic
capacity for storage of palmitate in the form of TAG within liver slices tended to decrease as
the amount of RPC consumed by cows increased. The hepatic fatty acid oxidation to C02
was not affected by dietary choline.
The idea of using glucagon for fatty liver treatment and/or prevention originated from
investigators who studied secretion and clearance rates of glucagon in dairy cows under
different physiological conditions and changes in metabolite and hormone concentrations in
response to glucagon administration (De Boer et al., 1986). A single intravenous glucagon
injection increased blood insulin and glucose concentrations, thus creating a condition that
could lead to inhibition of lipolysis from adipose. Then, metabolic responses to 14-d
intravenous infusions of glucagon in lactating dairy cows were studied (She et al., 1999a).
The continuous glucagon infusion increased plasma glucose and insulin concentrations and

22
did not change the concentrations of plasma NEFA, BHBA, and urea. Liver glycogen
concentration was not significantly affected by glucagon but increased dramatically after the
cessation of glucagon administration. The continuous intravenous glucagon administration
decreased PEPCK mRNA concentration in normal cows but did not have any effects on
PEPCK mRNA in cows with fatty liver (She et al., 1999b). However, the concentration of
PEPCK was higher in fatty liver cows. There was a decrease in PEPCK mRNA in normal
midlactation cows after glucagon infusion. The data indicate that the expression of PEPCK
gene in normal cows is decreased after glucagon administration because of inhibitory effect
of insulin, which is secreted to balance elevated carbohydrate status after glucagon infusion.
The inability of glucagon to decrease PEPCK mRNA in fatty liver cows may be related to
some degree of insulin resistance existing in those cows.
Intravenous infusions of glucagon for 14 d alleviated fatty liver and ketosis in
lactating dairy cows (Hippen et al., 1999a). Feeding extra com during the dry period combine
with feed restriction and diet supplementation with ketogenic precursor postpartum were
used to induce fatty liver in those cows. In this study, glucagon did not increase plasma
insulin concentration but decreased plasma BHBA and NEFA and liver TAG concentrations,
and increased plasma glucose concentration. Liver glycogen concentration was not affected
by glucagon but increased after the end of glucagon administration.
To make a glucagon therapy easily applicable to field conditions in the dairy industry,
subcutaneous glucagon injections were used to test the treatment of fatty liver in transition
dairy cows (Bobe et al., 2003b). Glucagon was able to increase plasma glucose and insulin
concentrations and decrease plasma NEF A concentration. However, the treatment effect of
glucagon, as based on the changes in liver TAG concentration, was observed only in older

23
cows. Subcutaneous glucagon injections did not have any effects on the concentration of
different fractions of lipoproteins in plasma (Bobe et al., 2003a).

24
PREVENTION OF FATTY LIVER IN TRANSITION DAIRY
COWS BY 14-DAY SUBCUTANEOUS GLUCAGON
INJECTIONS
A paper to be submitted to the Journal of Dairy Science
Rafael A. Nafikov, Burim N. Ametaj, Kenneth J. Koehler, J. W. Young,
and Donald C. Beitz
Abstract
The main objective of this study was to test the extent to which subcutaneous
glucagon injections for 14 days beginning at d 2 postpartum would prevent fatty liver
development in transition dairy cows. Twenty-four multiparous Holstein cows were fed 6 kg
of cracked com in addition to dry cow ration during last 30 d of a dry period to induce fatty
liver development postpartum. Subcutaneous glucagon injections at either 7 .5 or 15 mg/d
dosages or saline as a control were given 3 times per day for 14 d beginning at d 2
postpartum. Glucagon administration at a dosage of 15 mg/d prevented liver triacylglycerol
accumulation and, consequently, fatty liver development in transition dairy cows postpartum.
Glucagon administration at 7.5 mg/d dosage showed a potential for fatty liver prevention.

25
Glucagon administration increased plasma glucose and insulin concentrations and decreased
plasma nonesterified fatty acid concentration. There were no significant effects of glucagon
administration on plasma B-hydroxybutyrate (BHBA) concentration. Cows treated with the
15 mg/d dosage of glucagon, however, tended to show an increase in plasma BHBA
concentration around d 9 postpartum. Glucagon had no effects on feed intake and milk
production of dairy cows. Moreover, milk composition was not altered by subcutaneous
glucagon injections. Milk urea concentration decreased, and plasma urea concentration
tended to decrease during glucagon administration, which indicates that treatment with
glucagon may improve protein utilization. Liver glycogen concentration was not affected by
glucagon administration. There were no significant differences in body condition scores
between cows from different treatment groups throughout the study. Our results show that
subcutaneous glucagon injections can be used for fatty liver prevention in transition dairy
cows.
Introduction
Transition dairy cows defined as 3 wk prior to and 3 wk after parturition, are at high
risk for the development of different metabolic diseases (Drackley, 1999). Fatty liver is one
of them. The prevalence of fatty liver in dairy herds could reach up to 50% (Jorritsma et al.,
2000a). The consequences of fatty liver development are decreased reproductive success and
suppressed immune function (Jorritsma et al., 2000b; Wentink et al., 1999). Increased liver
triacylglycerol (TAG) concentration increases the interval from parturition to first ovulation
and decreases functional capacities of polymorphonuclear neutrophilic granulocytes derived

26
from blood and uterus (Rukkwamsuk et al., 1999b; Zerbe et al., 2000). Fatty liver does not
develop alone and could be associated with other periparturient diseases such as ketosis,
retained fetal membranes, endometritis, displaced abomasum, mastitis, and milk fever
(Katoh, 2002; Van Winden et al., 2003). Ketosis is believed to be associated with fatty liver,
which is commonly the prerequisite for the development of ketosis (Katoh, 2002). Being able
to prevent and/or treat ketosis and other metabolic diseases is very important, because they
cause substantial economical losses to dairy farmers (Fourichon et al., 1999).
Around parturition dairy cows are in a state of negative energy balance (NEB),
because they cannot meet their nutrient requirements for maintenance, fetus growth and milk
production from feed consumption (Jorritsma et al., 2003). At the onset of lactation, the
mammary gland has increased demands for glucose, used primarily for lactose biosynthesis,
which exacerbates NEB, because glucose is in short supply. To meet energy requirements,
cows mobilize fatty acids from adipose tissue, which results in an elevated blood
nonesterified fatty acid (NEFA) concentration (Drackley, 1999; Grummer, 1993). Excess
blood NEFA is taken up by the liver and metabolized in different ways. Nonesterified fatty
acids can be oxidized completely to carbon dioxide or incompletely to ketone bodies,
esterified into TAG for storage in the liver, or secreted into blood as a part of very low
density lipoproteins (VLDL). When the rates of NEFA esterification into TAG for storage
exceed the rates of NEFA disposal, fatty liver can develop. The exact causes of fatty liver are
unknown. However, any factor that causes increased lipid mobilization could be responsible
for disease development. Periparturient ketosis is associated with fatty liver and developed
because of the condition of increased liver lipid infiltration and decreased liver glycogen
(Drackley et al., 1992).

27
Hepatic gluconeogenesis is impaired in cows fed high concentrate diets during the dry
period because of low phosphoenol-pyruvate carboxykinase (PEPCK) activity 1 wk before
and 2 wk after parturition (Rukkwamsuk et al., 1999a). As a result, inadequate glucose
production further increases the ongoing high rates of lipolysis and promotes fatty liver
development. The fatty liver condition itself, however, can inhibit ureagenesis, leading to
increased blood ammonia concentration (Zhu et al., 2000), which can decrease the rates of
hepatic gluconeogenesis from propionate (Overton et al., 1999). Thus, it was demonstrated in
vitro that hepatic TAG accumulation can decrease the rates of gluconeogenesis (Cadomiga
Valino et al., 1997).
Glucagon is a 29-amino acid peptide hormone produced and secreted by the a-cells in
the islets of Langerhans in the pancreas. The secretion of glucagon occurs in a pulsatile
fashion, which generates a maximal effect on hepatic glucose output. Glucagon is involved in
the regulation of glucose homeostasis by stimulating gluconeogenesis and glycogenolysis
and by inhibiting glycogenesis and glycolysis. Half-life of a glucagon molecule in blood of
dairy cows is about 5 min. (De Boer et al., 1986). Based on in vitro studies glucagon has
been considered for a long time to have a lipolytic effect in humans (Richter et al., 1989).
However, recent data indicate that glucagon does not have a direct effect on the rates of
lipolysis in human adipose tissue (Bertin et al., 2001). In rats, the glucagon to insulin molar
ratio is responsible for the control of ketogenesis, but it has no effect on the rates of lipolysis
(Ubukata et al., 1996). Thus, a high glucagon to insulin ratio increases the concentration of
ketone bodies in blood and a low glucagon to insulin ratio has an opposite effect.
Previously, we demonstrated that 14-d intravenous infusion of glucagon could be
used to treat fatty liver and, associated with it, ketosis in early lactation cows (Hippen et al.,

28
1999a). In this study, feeding extra com grain to dry cows together with energy restriction
and diet supplementation with 1,3-butanediol postpartum were used to induce fatty liver and
ketosis in dairy cows. Intravenous infusions of glucagon, however, are not practical for use in
the dairy industry, and the conditions associated with naturally occurring fatty liver and
ketosis could be different from those artificially created in the Hippen et al. study. The
objectives of this study were to determine whether subcutaneous glucagon injections for 14 d
beginning at d 2 postpartum would prevent development of fatty liver in transition dairy
cows and to evaluate the effects of glucagon treatment on feed intake, milk production, and
blood composition of dairy cows.
Materials and Methods
Experimental Design
In this study, 24 multiparous Holstein cows were randomly assigned to saline
(control), 7.5 mg/d, or 15 mg/d glucagon treatment groups with 8 cows per group. One cow
from the 7.5 mg/d of glucagon treatment group was dropped from the study, because she
developed a fatty liver disease prepartum before we started the treatment administration for
preventive purposes. During wk 4 of gestation, all cows were supplemented with 6 kg of
cracked com in addition to their regular dry cow diet (Bobe et al., 2003b), which was fed
according to NRC requirements (National Research Council, 2001), to stimulate the
development of fatty liver disease postpartum (Hippen et al., 1999a). Cows were housed in a
straw-bedded free-stall with free access to water and hay. After parturition, cows were

29
housed in a tie-stall barn and fed ad libitum a lactation diet (Bobe et al., 2003b) that was
formulated to meet NRC requirements (National Research Council, 2001).
Beginning at d 2 postpartum, cows were injected subcutaneously with saline (0.15 M
NaCl), 7.5 mg/d, or 15 mg/d of glucagon for 14 d. Injections were given in the area between
the fifth and seventh intercostal space three times per day in 8-h intervals. The volume of a
single injection was 60 ml. Lyophilized glucagon (donated by Eli Lilly and Co.,
Indianapolis, IN) was dissolved in 0.15 M NaCl (pH 10.25) at 41.67 mg/Land 83.33 mg/L to
create the dosage of 7.5 and 15 mg/d of glucagon, respectively. Glucagon solution were
prepared every other day, stored at 4 °c and used within 48 h when needed. To prevent
adherence of glucagon, all glassware and utensils were rinsed with 1 % bovine serum albumin
in 0.15 M NaCl before use. All animals were treated in accordance with guidelines
established by the Iowa State University Committee on Animal Care.
Sampling and Analysis
Liver. Liver samples were obtained by puncture biopsies at d -4, 2, 6, 9, 16, 20, 27,
34, and 42 postpartum and stored at -80 c0 for later analysis for concentration of total lipids,
TAG, phospholipids, total cholesterol, and glycogen. Total lipid concentration of liver was
determined gravimetrically by using the Folch method (Folch et al., 1957) with the following
modifications. Liver tissue with wet weight between 300-400 mg was homogenized in 8 ml
of chloroform-methanol (2:1 vol/vol) in a screw-top 25 x 150 extraction tube and sonicated
for 30 s (model 350 sonifier, Bronson Sonic Power Corp., Danbury, CT). The samples were
shaken for 1 h (model 75 wrist-action shaker, Burrel Scientific, Pittsburg, PA), and 2 ml of
0.15 M NaCl was added. After vortexing for a few seconds, the mixture was centrifuged at

30
500 x g for 20 min. (model K centrifuge, International Equipment Co., Needham Heights,
MA), and the methanol-water layer was aspirated.
The chloroform-containing fraction was filtered through a Buchner funnel and a 42.5
mm glass microfiber filter (Whatman International Ltd., Maidstone, England) and washed
three times with 2, 4, and 4 ml of chloroform, respectively. Liver total lipid extract was dried
under constant air flow at 50 c0 for 2.5 h (SC/48R sampler concentrator, Brinkmann
Instruments, Inc., Westbury, NY). Liver total lipid extraction was performed twice using the
same set of liver samples. One of the liver total lipid extracts was used for liver phospholipid
and total cholesterol analysis, and the other extract was used for total lipid and TAG
determination. For phospholipid and total cholesterol determination, dried liver lipid extracts
were reconstituted with 5 ml of 1 % Triton X-405 (Amresco Inc., Solon, OH) in 0.15 M NaCl
at 37 c0, and liver phospholipid (Phospholipids B kits number 991-38492, Wako, Richmond,
VA) and total cholesterol (Cholesterol kit number C7510, Pointe Scientific, Lincoln Park,
Ml) concentrations were determined on a microplate spectrophotometer (SPECTRA max
Plus, Sunnyvale, CA). For liver TAG determination, dried liver lipids were reconstituted
with chloroform, and a small aliquot of the liver lipid in chloroform solution was used for
analysis. After chloroform evaporation, lipids were subjected to base hydrolysis in a solution
containing 20% of 2 N KOH and 80% of 96% ethanol for 1hat80 c0.
The pH of the mixture was neutralized by 12.1 N hydrochloric acid, and the
concentration of a glycerol in the mixture was determined enzymatically (TAG kit number
T7532, Pointe Scientific, Lincoln Park, Ml) and expressed as a TAG concentration. Liver
glycogen determination was done as described earlier (Bobe et al., 2003b ).

31
Plasma. Blood samples were collected in the morning from the coccygeal vein at d 1
through 17, 20, 27, 34, and 41 postpartum. During the treatment period, blood samples were
taken at 1 h after the morning injection of glucagon or saline. We used 10-ml Vacutainer
tubes (Beckton Dickinson and Co., Rutherford, NJ) containing Na3-EDTA for blood
sampling. After centrifugation, blood plasma samples were stored at -20 c0 until further
analysis for the concentration of glucose (glucose kit number 315 Sigma), NEPA (NEFA-C
kit number 994-75409; Wako, Richmond, VA), BHBA (BHBA; Pointe Scientific, Lincoln
Park, MI), PUN (BUN kit number B 7552, Pointe Scientific; Lincoln Park, Ml), and
glucagon (glucagon kit number GL-32K; LINCO Research, Inc. St Charles, MO). Aprotinin
(Boehringer -Mannheim, Indianapolis, IN), a protease inhibitor, was added at 500 KIU to the
1 ml plasma to be analyzed for glucagon.
Plasma insulin concentration was determined by RIA using antisera for bovine insulin
(Bovine Insulin Antisera catalog number 1010, LINCO Research, Inc.; St. Charles, MO). The
rest of the reagents for RIA were from the rat insulin kit (rat insulin RIA kit number RI-13K).
Bovine insulin (bovine insulin catalog number I 0516; Sigma) standards were prepared in the
prescribed assay buffer.
Other measurements. Feed intake was measured twice daily at d 1 through 17
postpartum. Cows were milked at 6.30 and 18.30 h, and production was recorded daily at d 1
through 41 postpartum. Milk samples were collected from two adjacent milking at d 2, 6, 9,
16, 20, 27, 34, and 41 postpartum and analyzed for fat, protein, lactose, and urea N by mid
infrared spectrophotometry (Milk-0-Scan 203, Foss Food Technology, Eden Prairie, MN).
Body condition scores (BCS) were evaluated by three individuals at d -22, -9, 5, 19, and 32

32
postpartum. Cows were tested for urinary ketones (i.e., acetone plus acetoacetate, Ketostix®;
Miles Inc. Diagnostics Division, Elkhart, IN).
Statistical Analysis
Data were analyzed as repeated measures using the MIXED procedure of SAS,
Version 8.2 (2001). Effects of 7.5 and 15 mg/d of glucagon administration on response
variables were evaluated by comparing each glucagon-treated group with the saline (control)
group. Separate comparisons were made for data obtained during the treatment period and
the post treatment period.
The statistical models contained response variables as the dependent variables. The
fixed effects were treatment (saline, 7.5, and 15 mg/d of glucagon), time, and treatment by
time interaction. A different set of random effects was used for the set of measurements taken
on each cow. The Toeplitz covariance structure was selected based the Schwarz's Bayesian
Information Criterion (BIC, smaller is better), the design of the study, and the biology of the
experiment. The Toeplitz covariance structure assumes equal variances on the main-diagonal,
equal correlations for any pair of measurements equally distant in time, but different
correlation for pairs of observations with separation in time. The logarithmic transformation
of some data was used to meet the requirements for normality. The overall effects of the
different treatment administration were evaluated by comparing changes in response
variables from the glucagon-treated groups with corresponding changes in response variables
from saline (control) group by using a t-test in the LSMEAN statement. The
KENW ARDROGER option was used to obtain the correct degrees of freedom. Means and

33
SEM shown in the figures were calculated from the original, non-transformed data.
Significance was declared at P:S0.05.
Results
Liver lipid composition and glycogen. Glucagon administration tended to prevent
lipid accumulation by liver of lactating dairy cows (Figure lA), although the effects of 7.5
and 15 mg/d of glucagon treatments were not significant (P:S0.096 and P:S0.057,
respectively). A postpartal increase in liver TAG concentration was prevented by glucagon
administration at 15 mg/d dosage (P:S0.028), (Figure lB). Liver TAG concentration in cows
from 7 .5 mg/d of glucagon treatment group, however, was not as effectively suppressed
(P:S0.20). Concentrations of liver phospholipids and total cholesterol (Figure 1 C and 1 D,
respectively) in the glucagon-treated groups were not significantly different from those
concentrations in the control group (liver phospholipids: P:S0.12 and P:S0.31 for 7.5 and 15
mg/d of glucagon treatment groups, respectively; liver total cholesterol: P:S0.41 and P:S0.32
for 7.5 and 15 mg/d of glucagon treatment groups, respectively). Nevertheless, the
concentrations of liver phospholipids and total cholesterol tended to be higher in the control
group than in the glucagon-treated groups. There were significant time effects on liver TAG,
phospholipids, and total cholesterol concentrations (P:S0.024, P:S0.038, and P:S0.024,
respectively) for the posttreatment period (d 17 through 41 postpartum).
Liver glycogen concentration declined after parturition through d 6 postpartum in all
treatment groups (Figure 2). Then, it started to rise with different paces for the different
treatment groups, reaching prepartal values around d 34 postpartum. There were no

9
~8 Ill
:E 7 c.
!6 0 ... ; 5 > :J 4
l 1.2
... Q) ~ 1.1 ~ 0
~ 1.0 ·c.. ~ 0.9 c. t/I _g 0.8 c. a..
1 Treatment 1 A 1 l\l --o-Soll•• 1 1 _._7.5 mg glucagon y I -+-15 mggl""'°" ,-
I
~· jj( I
~~ -4 0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
: Treat\ment : C 1 I --o- Saline
I / I -+-7.5 mggl"'"°" I I ......._ 15 mg glucagon I
I I ~~ ........... I I e
~ 0.1-----------........ :J -4 0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
34
7
~ 6 ... ~ 5 ~ 0
~ 4 (!) <C I- 3 a.. Q)
> :J 2
l ... 0.45
; ~ 0.40
e o.35 ! ~ 0.30 0 ..c: (.,) 0.25
J!! .s 0.20 a..
~ :J
1 Treatment 1 B
: l\--o-Soll•o I 1 _._ 7.5 mg glucagon
~ I -+-15 mggl""O°" ,'a""
~ -~ +~ I I
-4 0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
I Treatment 1 D
1 1 ~7.5 mg glucagon
I I I I
/
1 a\ : --o-Saline
I ........_s......._15 mg glucagon
,- ~[J
l:t~Y~~ It: : ~ ~
-4 0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
Figure 1. Liver lipid composition of cows treated with saline, 7.5, and 15 mg/d of glucagon. A. Liver total lipids. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are PS0.096 and PS0.057, respectively; and during post treatment period are PS0.21 and PS0.23, respectively. SEM= 0.36 to 0.78. B. Liver TAG. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are PS0.20 and PS0.028, respectively; and during post treatment period are PS0.52 and PS0.24, respectively. Time effect for post treatment period is PS0.024. SEM= 0.38 to 0.84. C. Liver phospholipids. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are PS0.12 and PS0.31, respectively; and during post treatment period are PS0.73 and PS0.87, respectively. Time effect for post treatment period is PS0.038. SEM= 0.07 to 0.11. D. Liver total cholesterol. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are PS0.41 and PS0.13, respectively; and during post treatment period are PS0.91 and PS0.32, respectively. Time effect for post treatment period is PS0.024. SEM= 0.02 to 0.05.

l 3.0
..... ; 2.5
';!. c: 2.0 Cl> C> 8 1.5 ~ -C> ..... 1.0 g? ·-
I Treatment I
35
..J 0.5 ~-_.....,__ ................ ....-i_ ..... ,...... ..........................
-4 0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
Figure 2. Liver glycogen concentration of cows treated with saline, 7.5, and 15 mg/d of glucagon. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P::;0.11 and P::;0.36, respectively; and during post treatment period are P::;0.094 and P::;0.045, respectively. Time effect for treatment period is P<0.0001. Treatment by time interaction for post treatment period is P::;0.0025. SEM= 0.17 to 0.20.

36
significant effects of glucagon administration on liver glycogen concentration during the
treatment period (PS0.11 and PS0.36 for 7.5 and 15 mg/d of glucagon treatment groups,
respectively). However, glucagon administration at 15 mg/d dosage caused an increase in
liver glycogen concentration during the posttreatment period (PS0.045). Liver glycogen
concentration also tended to be higher in the 7.5 mg/d of glucagon treatment group during the
posttreatment period as compared with that of the control (PS0.094). There were a significant
time effect on liver glycogen concentration for treatment period (P<0.0001) and a significant
time by treatment interaction for posttreatment period (PS0.0025).
Plasma metabolites. Plasma glucose concentration increased during the treatment
period in 7.5 and 15 mg/d of glucagon treatment groups (P<0.0001 and P<0.0001,
respectively) in a dosage-dependent manner (PS0.017, Figure 3A). There were no significant
differences in plasma glucose concentrations after the end of treatment period. Plasma NEF A
concentration was very high in cows from all treatment groups around d 2 postpartum
(Figure 3B). After glucagon administration, plasma NEFA concentration declined rapidly as
compared with that of the control group. As a result, plasma NEF A concentration was lower
in glucagon-treated groups (PS0.046 and PS0.007 for 7.5 and 15 mg/d of glucagon treatment
groups, respectively) during the treatment period. There were significant time effects on
plasma NEFA concentration for treatment (PS0.0089) and posttreatment (PS0.0013) periods.
Plasma BHBA concentration tended to be lower in the 7 .5 mg/d of glucagon treatment group
(P:s;0.35, Figure 3C) during treatment period. Glucagon administration at 15 mg/d dosage did
not have a significant effect on plasma BHBA concentration (P:s;0.77). Moreover, the pattern
of changes in BHBA concentration during the treatment period was the same for both

90
'C -en 80 E CIJ Ill
8 70 ::I
en
!¥ 60 Ill ~ a..
:0
12.0
Ci 10.5 E <(,~
9.0 al :::c al ns 7.5 E Ill ~ a.. 6.0
I Treatment 1
:. ll~lft 1\ ~. • l /'.· ,v.. ...
A
~Saline
~7.5 mg glucagon ......._15 mg glucagon
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
1 Treatment 1 C I a~. I I I
1 I ~Saline I a I ~7.5 mg glucagon
:~1M\ ~ : \J~~"/~ I I
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
37
700
:E 600 ::1.
<i 500 LL. w z 400 ns E Ill 300
.!:!! a..
200
20
32 en E 18 ns e ::s 16 ns E Ill ns a: 14
B I Treatment I cl I
Pl\ ~Saline CcC\i
1 \ 1 ~7.5 mg glucagon
11 1 ......._15 mg glucagon
I 1,.\ \a& : ~·11.'f•\ a ~~ , \~i9r-aA -~ ~ / : ~ /~ I I
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
I Treatment I
-o-Saline _.,_7,5 mg glucagon --.t.-15 mg glucagon
0 4 8 12 16 20 24 28 32 36 40
Time oostoartum. d
Figure 3. Plasma metabolite concentrations of cows treated with saline, 7.5, and 15 mg/d of glucagon. A. Plasma glucose. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P<0.0001 and P<0.0001, respectively; and during post treatment period are P:S0.96 and P:S0.33, respectively. Dosage effect for treatment period is P:S0.017. SEM=l.31to1.74. B. Plasma NEFA. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.046 and P:S0.007, respectively; and during post treatment period are P:S0.99 and P:S0.48, respectively. Time effect for treatment period is P:S0.0089; and for post treatment period is P:S0.0013. SEM=26.52 to 64.80. C. Plasma BHBA. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.35 and P:S0.77, respectively; and during post treatment period are P:S0.69 and P:S0.43, respectively. SEM=0.49 to 1.37. D. Plasma urea. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.24 and P:S0.17, respectively; and during post treatment period are P:S0.65 and P:S0.76, respectively. Time effect for treatment period is P:S0.0008; and for post treatment period is P:S0.034. SEM=0.76 to 0.89.

38
15 mg/d of glucagon and saline treatment groups. Plasma urea concentration tended to be
lower in glucagon-treated groups (P:S0.24 and P:S0.17 for 7.5 and 15 mg/d of glucagon
treatment groups, respectively, Figure 3D) during the treatment period. There were
significant time effects on plasma BHBA concentration during the treatment (P:S0.0008) and
posttreatment (P:S0.034) periods.
Plasma insulin concentration rose steadily after the beginning of glucagon
administration (Figure 4A). Cows from the glucagon treatment groups had higher plasma
insulin concentration as compared with that of the control group (P:S0.012 and P:S0.0011 for
7.5 and 15 mg/d of glucagon treatment groups, respectively) during the treatment period.
There were no significant differences in plasma insulin concentration between the glucagon
treatment groups and the control group during the posttreatment period.
Milk production and composition. Glucagon administration did not have a
significant effect on milk production during the treatment (P:S0.78 and P:S0.51 for 7.5 and 15
mg/d of glucagon treatment groups, respectively) and posttreatment (P:S0.46 and P:S0.50 for
7.5 and 15 mg/d of glucagon treatment groups, respectively) periods (Figure 5). There were
significant time effects on milk production during the treatment (P<0.0001) and
posttreatment (P:S0.049) periods.
Although milk lactose concentration tended to be slightly higher in 7 .5 mg/d of
glucagon treatment group it was not a statistically significant difference either during the
treatment (P:S0.19) or posttreatment (P:S0.11) periods as compared with that of the control
group (Figure 6A). Glucagon administration at 15 mg/d dosage did not have a significant
effect on milk lactose concentration (P:S0.96 and P:S0.71) for the treatment and posttreatment

1.5
E c, 1.2 c ~
c ·-:; 0.9 en c
E 5 -C> c r! 4 0 C> CG (.)
~3 C> ns E en 2 ns -D.
•
39
A
~Saline
----7.5 mg glucagon __..._ 15 mg glucagon
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
Treatment I e e I
:~ .. jA f"f~
B
~Saline
1 ----7.5 mg glucagon __..._ 15 mg glucagon
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
Figure 4. Plasma hormone concentrations of cows treated with saline, 7.5, and 15 mg/d of glucagon. A. Plasma insulin. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.012 and P:S0.0011, respectively; and during post treatment period are P:S0.33 and P:S0.62, respectively. SEM=0.05 to 0.08. B. Plasma glucagon. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.47 and P:S0.86, respectively; and during post treatment period are P:S0.80 and P:S0.82, respectively. SEM=0.12 to 0.40.

42
en 36 ~
"' s:: 30 0 ·-... (.)
::J 24 "t:J 0 "'" Q.
~ 18 -::?:
12
40
I Treatment I 0 °b I I ~ l \
D D d D I • orfoDD o lid o NA. • 1 rY1~ .. -.. ... I 'f..aD -.~ ~ 1;• 'A,t..&AA~ I
~Saline
• 7.5 mg glucagon .. 15 mg glucagon
•
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
Figure 5. Milk production of cows treated with saline, 7.5, and 15 mg/d of glucagon. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:'.S0.78 and P:S0.51, respectively; and during post treatment period are P:'.S0.46 and P:'.S0.50, respectively. Time effect for treatment period is P<0.0001; and for post treatment period is P:'.S0.049. SEM=l.32 to 2.79.

5· 1 1 Treatment I
4.8
~ ai 4.5 I Ill .s (.)
j 4.2
3.9
: ~Saline 1 -+-7.5 mg glucagon 1 -6- 15 mg glucagon
A
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
c
6 I Treatment I
• 5
c
,Sl 4 I
e
'~saline :-+-7.5 mg glucagon
1 -6-15 mg glucagon
Q.
.ll::
~ 3
2 ........................................................................... _... 0 4 8 12 16 20 24 28 32 36 40
Time postparum, d
41
4.8
~ 4.4
..J
.f!
B
~Saline
-+-7.5 mg glucagon -6- 15 mg glucagon
.ll:: 4.0 I
:!!:
3.6
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
Treatment 1 I
D 18 I
Nlr ·i' "C -~ 15
C'O ~ :::s 12
.ll::
I
~Saline L ' --+-7.5 mggl""'"" I -6-15 mg glucagon I
•
0 4 8 12 16 20 24 28 32 36 40
Time postpartum, d
Figure 6. Milk composition of cows treated with saline, 7.5, and 15 mg/d of glucagon. A. Milk lactose. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.19 and P:S0.96, respectively; and during post treatment period are P:S0.11 and P:S0.71, respectively. Time effect for treatment period is P<0.0001. SEM=0.078 to 0.083. B. Milk fat. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.71 and P:S0.66, respectively; and during post treatment period are P:S0.63 and P:S0.83, respectively. Time effect for treatment period is P:S0.0031. SEM=0.11 to 0.22. C. Milk protein. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.13 and P:S0.20, respectively; and during post treatment period are P:S0.64 and P:S0.52, respectively. Time effect for treatment period is P<0.0001; and for post treatment period is P:S0.028. SEM=0.052 to 0.098. D. Milk urea. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:S0.0208 and P:S0.0018, respectively; and during post treatment period are P:S0.50 and P:S0.49, respectively. SEM= 0.55 to 1.34.

42
periods, respectively). There was a time effect on milk lactose concentration during the
treatment period (P<0.0001). Milk fat concentration was not affected by glucagon treatments
during both the treatment (P:S:0.71 and P:::;0.66 for 7.5 and 15 mg/d of glucagon treatment
groups, respectively) and posttreatment (P:S:0.63 and P:S:0.83 for 7.5 and 15 mg/d of glucagon
treatment groups, respectively) periods (Figure 6B). There was a significant time effect on
milk fat concentration during the treatment period (P:S:0.0031 ). Milk protein concentration
declined rapidly since the beginning of lactation until it reached a base line in the range
between 2.50 and 2.75% (Figure 6C). There were no significant differences in milk protein
concentration between glucagon-treated groups and the control group during the treatment
(P:S:0.13 and P:S:0.20 for 7.5 and 15 mg/d of glucagon treatment groups, respectively) and
posttreatment (P:S:0.64 and P:S:0.83 for 7.5 and 15 mg/d of glucagon treatment groups,
respectively) periods. There were significant time effects on milk protein concentration
during the treatment (P<0.0001) and posttreatment (P:S:0.028) periods. Milk urea
concentration was significantly higher in the control group as compared with that of the
glucagon-treated groups (P:S:0.0208 and P:S:0.0018 for 7.5 and 15 mg/d of glucagon treatment
groups) during the treatment period (Figure 6D). There were no significant differences in
milk urea concentration between the glucagon-treated groups and the control group during
the posttreatment period.
Feed intake and BCS. Feed intake of dairy cows was not affected by glucagon
administration during the treatment period (P:S:0.99 and P:S:0.95 for 7.5 and 15 mg/d of
glucagon treatment groups, respectively, Figure 7). However, cows given 7.5 mg/d glucagon
tended to have higher feed intake around d 9 postpartum. There were no differences in BCS

80
~70 .. Q) ~
~ 60 c: ·-"'C Q) Q) 50
LL
43
Treatment
a
0 2 4 6 8 10 12 14 16 18
Time postpartum, d
Figure 7. Feed intake of cows treated with saline, 7.5, and 15 mg/d of glucagon. Effects of 7.5 and 15 mg/d of glucagon administration during treatment period are P:::;0.99 and P:::;0.95, respectively. SEM=4.28 to 6.12.

44
between cows from all treatment groups (Figure 8). Precalving BCS were not as high as in
an earlier study from our research group (Hippen et al., I999a), which slightly decreased the
severity of fatty liver development in the present study.
Discussion
Subcutaneous glucagon injections administered for I 4 d beginning at d 2 postpartum
tended to prevent liver total lipid accumulation (Figure IA). However, the differences in liver
total lipids between the glucagon-treated groups and the control group were not statistically
significant because of the small numbers of cows in the treatment groups and the high
variability among cows within treatment groups. The peak of lipid accumulation by liver was
around d 9 postpartum, which agrees with data of others (Greenfield et al., 2000b).
Glucagon administration at I5 mg/d dosage prevented liver TAG accumulation as
compared with that of the control group (Figure IB). However, the decrease in liver TAG
accumulation provided by the 7 .5 mg/d dosage of glucagon was smaller and statistically
insignificant.
Liver phospholipid (Figure IC) and total cholesterol (Figure ID) concentrations
tended to be higher in control cows as compared to glucagon-treated cows. Our data disagree
with earlier published work (Bobe et al., 2003a). An increase in liver phospholipid and total
cholesterol concentrations in control cows was caused by liver TAG accumulation. The
percentages of liver TAG, phospholipid, and total cholesterol nearly added up to the
percentages of liver total lipids determined gravimetrically, showing indirectly that analysis
of liver lipid composition included all major lipids.

45
Figure 8. Body condition scores of cows from saline, 7.5, and 15 mg/d of glucagon treatment groups. Difference in body condition score between saline and 7.5 mg/d of glucagon treatment groups, saline and 15 mg/d of glucagon treatment groups, and 7.5 mg/d and 15 mg/d of glucagon treatment groups throughout the study are P<0.9971, P<0.9703, and P<0.9525, respectively. SEM=0.12 to 0.23.

46
Liver glycogen concentration declined from d 0 until d 6 postpartum in cows from all
treatment groups and then started to rise, reaching precalving values around d 32 postpartum
(Figure 2). There were no significant treatment differences in liver glycogen concentrations
during the treatment period. This suggests that plasma glucose concentration did not increase
in glucagon-treated groups at the expense of glycogen degradation. Moreover, glucagon had
an inhibitory effect on glycogen synthesis, because, despite a higher plasma glucose
concentration in cows from the glucagon-treated groups (Figure 3A), liver glycogen
concentration was not significantly different between treatments during the treatment period.
The inhibitory effect of glucagon on glycogen synthesis observed in our study agrees with
data from the literature (Jiang and Zhang, 2003). After glucagon administration, liver
glycogen concentration started to rise very steeply, reaching very high levels at d 20 and 27
postpartum, which were significantly different from the values in the control group. A huge
increase in liver glycogen concentration after the end of glucagon administration can be
explained by the fact that there were no significant differences in plasma glucose
concentration after the end of treatment period and most extra glucose produced via
gluconeogenesis in glucagon-treated groups after the end of treatment period was used for
glycogen synthesis. Evidently, enzymes of gluconeogenesis were still up-regulated in cows
from glucagon-treated groups after the end of glucagon administration, which caused extra
glucose production.
Plasma glucose concentration was increased during glucagon administration in a
dosage-dependent manner (Figure 3A). The fact that glucagon administered to dairy cows
causes an increase in blood glucose concentration agrees with the data of others (De Boer et
al., 1986; Hippen et al., 1999a). The increase in plasma glucose concentration probably

47
occurred because of the activation of gluconeogenesis and/or repartitioning of glucose from
the use in glycolysis. Glucagon administration did not increase plasma glucose concentration
at the expense of glycogen degradation; there were no significant differences in liver
glycogen concentration during glucagon administration (Figure 2).
Plasma NEFA concentration declined substantially during the time of glucagon
administration (Figure 3B), which is in agreement with our earlier published work (Hippen et
al., 1999a). Our data support the findings of recent studies that suggest that glucagon has no
direct effect on the rates of lipolysis in human subcutaneous adipose tissue in vivo (Bertin et
al., 2001; Jensen et al., 1991), although some earlier studies indicated glucagon lipolytic
effects in vivo and in vitro (Carlson et al., 1993; Perea et al., 1995). Moreover, changes in the
insulin to glucagon ratio have no effect on the rates of lipolysis as shown in rats (Ubukata et
al., 1996). Most likely, an increase in plasma insulin concentration after glucagon
administration suppresses lipolysis (Elks and Manganiello, 1985) and/or enhances
reesterification of NEFA in adipose tissue into TAG (Campbell et al., 1992). High blood
glucose concentration (Figure 3A) can be responsible for enhanced antilipolytic action of
insulin (Amer et al., 1983).
There were no significant differences in the concentrations of plasma BHBA (Figure
3C) and urinary acetone and acetoacetate (Figure 9) between either of the glucagon treated
groups and the control group. The concentration of ketone bodies in plasma and urine
however, tended to be higher in both the 15 mg/d of glucagon and control (saline) treatment
groups. Plasma BHBA concentration in the control group was elevated around d 9
postpartum probably because of high liver TAG (Figure lB) and low liver glycogen (Figure
2) concentrations in those cows around that time (Drackley et al., 1992). Cows from the 15

48
mg/d glucagon treatment group also had elevated plasma BHBA concentrations, which might
be explained by possible activation of liver carnitine palmitoyltransferase 1 (LCPT-1) by
glucagon (Louet et al., 2002). Cows from the 7 .5 mg/d of glucagon treatment group did not
have increased ketone body production, because glucagon dosage probably was not high
enough to induce ketogenesis.
Plasma urea tended to decrease in the glucagon-treated groups (Figure 3D), but the
difference between the control and either of the glucagon-treated groups were not significant,
which agrees with other studies (Hippen et al., 1999a, b ). The data provide indirect evidence
that glucagon does not increase utilization of amino acids as gluconeogenic precursors.
Around d 9 postpartum, plasma urea concentration was the lowest in the glucagon-treated
groups and the highest in the control group.
Glucagon injections caused a large increase in plasma insulin concentration, which
was sustained until the end of the treatment period (Figure 4A). The data agree with earlier
published work from our research group (She et al., 1999b). There was a steep rise in plasma
insulin concentration above 900 pg/ml after d 8 postpartum in the 15 mg/d glucagon
treatment group, which led to a substantial decrease in plasma NEF A. On the bases of
Figures 3B and 4A, the reduction in plasma NEF A concentration below 400 µM can be
achieved if plasma insulin concentration is above 900 pg/ml. Insulin inhibitory effect on
lipolysis had been shown earlier.
Plasma glucagon concentrations were around 4000 pg/ml and were not significantly
different between the control group and either of the treatment groups throughout the study
(Figure 4B). The fact that we did not observe any increase in plasma glucagon concentration
after glucagon administration might be explained by a short half-life (5 min) of glucagon in

49
bovine blood (De Boer et al., 1986). Since we collected blood samples at 1 hr after glucagon
administration, this indicates that most of the injected glucagon was degraded by that time.
However, in comparison with the De Boer study, we used subcutaneous glucagon injections
instead of intravenous application, which can produce lower glucagon peaks in blood after
the injection and prolong slightly elevated glucagon concentrations in blood similar to what
was observed in a human study (Muhlhauser et al., 1985).
Milk production (Figure 5) was not affected by glucagon administration and was not
significantly different between either of the glucagon-treated groups and the control group
throughout the study. There was a rapid jump in milk production after parturition, which
reached 27 kg/d by d 4 postpartum in all treatment groups. Then, milk production increased
gradually in all treatment groups until the end of the study.
Lactose concentration (Figure 4A) was not significantly different between either of
the glucagon-treated groups and the control group throughout the study. However, lactose
concentration in milk from 7.5 mg/d of glucagon treatment was observed to be slightly
higher than in milk from the other treatment groups. Aside from variability among the cows,
it is difficult to explain the cause of increase in lactose concentration in 7.5 mg/d of glucagon
treatment group, but our data suggests that there is no direct relationship between blood
glucose concentration and lactose biosynthesis.
There were no significant differences in milk fat concentration between either of the
glucagon-treated groups and the control group throughout the study (Figure 6B). Milk fat
concentration was slightly higher in the control group around d 6 postpartum, and those
control cows also exhibited higher plasma NEFA concentrations. In general, in cows with the

50
same milk production, milk fat concentration might be correlated positively with plasma
NEF A concentration.
Milk protein concentrations (Figure 6C) in all treatment groups declined during the
first two weeks postpartum until it reached a plateau. There were no significant differences in
milk protein concentrations between either of the glucagon-treatment groups and the control
group, which disagrees with an earlier study from our group (Hippen et al., 1999a). Our data
suggest that glucagon administration has no effect on milk protein concentration, which
suggests the fact that glucagon does not facilitate the utilization of amino acids as
gluconeogenic precursors during periparturient period.
Milk urea concentration was significantly higher in the control group compared to
glucagon-treated groups during the treatment period (Figure 6D), which indicates that
treatment with glucagon may improve protein utilization.
Feed intake of dairy cows (Figure 7) rose slowly throughout the treatment period, but
feed intake was not significantly different between either of the glucagon-treated groups and
the control group. Cows from the 7.5 mg/d of glucagon treatment group tended to have
slightly higher feed intake around d 9 postpartum, which can be explained by lower ketone
body concentration in blood and in urine around that time. Subcutaneous glucagon injections
did not decrease feed intake as observed during intravenous glucagon administration (Hippen
et al., 1999a). Surprisingly, increases in plasma glucose concentration caused by glucagon
administration were not accompanied by increases in feed intake, which raises questions
about (1) whether cows do not have enough gluconeogenic precursors around parturition
(Gerloff, 2000) and (2) whether suppression of gluconeogenesic activity limits the use of
glucose precursors available in feed (Rukkwamsuk et al., 1999a). We think that it is possible

51
that glucagon increases plasma glucose concentration not only by activating hepatic
gluconeogenesis, but also by repartitioning glucose from use for energy production to milk
production. Otherwise, it is difficult to explain why such a large increase in plasma glucose
concentration after glucagon administration was not accompanied by increase in feed intake.
Conclusions
The results of our study show that subcutaneous injections of 15 mg/d of glucagon for
14 d beginning at d 2 postpartum help to prevent fatty liver development in transition dairy
cows. Glucagon administration at 7 .5 mg/d dosage shows a potential for fatty liver
prevention, but possibly at a lower level. Subcutaneous glucagon injections increased plasma
glucose and insulin concentrations, which decreased the rates of lipolysis from adipose tissue
and possibly increased the rates of blood NEFA reesterification, causing a reduction in
plasma NEFA concentration. As a result, liver TAG accumulation was prevented in the 15
mg/d of glucagon treatment group. Glucagon administration at 7.5 mg/d dosage showed a
potential for the prevention of liver TAG accumulation, but possibly at a reduced level.
Increase in plasma glucose concentration in response to glucagon injections was mainly
because of an activation of gluconeogenesis and possibly an increase in glucose
repartitioning from utilization as an energy source. Glucagon did not cause liver glycogen
depletion. There were no negative effects of glucagon administration on feed intake and milk
production and composition of dairy cows. Glucagon injections decreased milk urea
concentration and tended to decrease plasma urea concentration, which suggests a role of
glucagon in improvement of protein utilization. There were no significant effects of glucagon

52
administration on the rates of ketogenesis. Considered together, these changes indicate that
glucagon could be very useful tool for the control of fatty liver disease in transition dairy
cows.
Acknowledgments
The authors thank Swiss Valley Farms (Davenport, IA) for analysis of milk samples
and Eli Lilly (Indianapolis, IN) for provision of glucagon. The research was partly supported
by grant number 99-35005-8576 from the US Department of Agriculture and was part of the
regional research project NC-185. Appreciation is also extended to the management and staff
of the Iowa State University Dairy Farm for provision of cows and to many undergraduate,
graduate and veterinary medical students for assistance with collection and analysis of liver
and blood samples.
References
Amer, P., J. Bolinder, and J. Ostman. 1983. Glucose stimulation of the antilipolytic effect of
insulin in humans. Science 220: 1057-1059.
Bertin, E., P. Amer, J. Bolinder, and E. Hagstrom-Toft. 2001. Action of glucagon and
glucagon-like peptide-1-(7-36) amide on lipolysis in human subcutaneous adipose
tissue and skeletal muscle in vivo. J Clin Endocrinol Metab 86: 1229-1234.
Bobe, G., B. N. Ametaj, J. W. Young, andD. C. Beitz. 2003a. Effects of exogenous glucagon
on lipids in lipoproteins and liver of lactating dairy cows. J Dairy Sci 86: 2895-2903.

53
Bobe, G., B. N. Ametaj, J. W. Young, and D. C. Beitz. 2003b. Potential treatment of fatty
liver with 14-day subcutaneous injections of glucagon. J Dairy Sci 86: 3138-3147.
Cadomiga-Valino, C., R.R. Grummer, L. E. Armentano, S.S. Donkin, and S. J. Bertics.
1997. Effects of fatty acids and hormones on fatty acid metabolism and
gluconeogenesis in bovine hepatocytes. J Dairy Sci 80: 646-656.
Campbell, P. J., M. G. Carlson, J. 0. Hill, and N. Nurjhan. 1992. Regulation of free fatty acid
metabolism by insulin in humans: Role of lipolysis and reesterification. Am J Physiol
263: E1063-1069.
Carlson, M. G., W. L. Snead, and P. J. Campbell. 1993. Regulation of free fatty acid
metabolism by glucagon. J Clin Endocrinol Metab 77: 11-15.
De Boer, G., A. Trenkle, and J. W. Young. 1986. Secretion and clearance rates of glucagon
in dairy cows. J Dairy Sci 69: 721-733.
Drackley, J. K. 1999. Adsa foundation scholar award. Biology of dairy cows during the
transition period: The final frontier? J Dairy Sci 82: 2259-2273.
Drackley, J. K., M. J. Richard, D. C. Beitz, and J. W. Young. 1992. Metabolic changes in
dairy cows with ketonemia in response to feed restriction and dietary 1,3-butanediol.
J Dairy Sci 75: 1622-1634.
Elks, M. L., and V. C. Manganiello. 1985. Antilipolytic action of insulin: Role of camp
phosphodiesterase activation. Endocrinology 116: 2119-2121.
Folch, J., M. Lees, and G. H. Sloane Stanley. 1957. A simple method for the isolation and
purification of total lipides from animal tissues. J Biol Chem 226: 497-509.

54
Fourichon, C., H. Seegers, N. Bareille, and F. Beaudeau. 1999. Effects of disease on milk
production in the dairy cow: A review. Prev Vet Med 41: 1-35.
Gerloff, B. J. 2000. Dry cow management for the prevention of ketosis and fatty liver in
dairy cows. Vet Clin North Am Food Anim Pract 16: 283-292.
Greenfield, R. B., M. J. Cecava, T. R. Johnson, and S.S. Donkin. 2000. Impact of dietary
protein amount and rumen undegradability on intake, peripartum liver triglyceride,
plasma metabolites, and milk production in transition dairy cattle. J Dairy Sci 83:
703-710.
Grummer, R.R. 1993. Etiology of lipid-related metabolic disorders in periparturient dairy
cows. J Dairy Sci 76: 3882-3896.
Hippen, A. R. et al. 1999a. Alleviation of fatty liver in dairy cows with 14-day intravenous
infusions of glucagon. J Dairy Sci 82: 1139-1152.
Hippen, A. R. et a~. 1999b. Metabolic responses of dairy cows and heifers to various
intravenous dosages of glucagon. J Dairy Sci 82: 1128-1138.
Jensen, M. D., V. J. Reiling, and J.M. Miles. 1991. Effects of glucagon on free fatty acid
metabolism in humans. J Clin Endocrinol Metab 72: 308-315.
Jiang, G., and B. B. Zhang. 2003. Glucagon and regulation of glucose metabolism. Am J
Physiol Endocrinol Metab 284: E671-678.
Jorritsma, R. et al. 2000a. Prevalence and indicators of post partum fatty infiltration of the
liver in nine commercial dairy herds in the netherlands. Livestock Production Science
68: 53-60.

55
Jorritsma, R., H. Jorritsma, Y. H. Schukken, and G. H. Wentink. 2000b. Relationships
between fatty liver and fertility and some periparturient diseases in commercial dutch
dairy herds. Theriogenology 54: 1065-1074.
Jorritsma, R., T. Wensing, T. A. Kruip, P. L. Vos, and J.P. Noordhuizen. 2003. Metabolic
changes in early lactation and impaired reproductive performance in dairy cows. Vet
Res 34: 11-26.
Katoh, N. 2002. Relevance of apolipoproteins in the development of fatty liver and fatty
liver-related peripartum diseases in dairy cows. J Vet Med Sci 64: 293-307.
Louet, J. F., G. Hayhurst, F. J. Gonzalez, J. Girard, and J. F. Decaux. 2002. The coactivator
pgc-1 is involved in the regulation of the liver carnitine palmitoyltransferase i gene
expression by camp in combination with hnf4 alpha and camp-response element
binding protein (creb). J Biol Chem 277: 37991-38000.
Muhlhauser, I., J. Koch, and M. Berger. 1985. Pharmacokinetics and bioavailability of
injected glucagon: Differences between intramuscular, subcutaneous, and intravenous
administration. Diabetes Care 8: 39-42.
Overton, T. R. et al. 1999. Substrate utilization for hepatic gluconeogenesis is altered by
increased glucose demand in ruminants. J Anim Sci 77: 1940-1951.
Perea, A., F. Clemente, J. Martinell, M. L. Villanueva-Penacarrillo, and I. Valverde. 1995.
Physiological effect of glucagon in human isolated adipocytes. Horm Metab Res 27:
372-375.

56
Richter, W. 0., H. Robl, and P. Schwandt. 1989. Human glucagon and vasoactive intestinal
polypeptide (vip) stimulate free fatty acid release from human adipose tissue in vitro.
Peptides 10: 333-335.
Rukkwamsuk, T., T. Wensing, and M. J. Geelen. 1999a. Effect of fatty liver on hepatic
gluconeogenesis in periparturient dairy cows. J Dairy Sci 82: 500-505.
Rukkwamsuk, T., T. Wensing, and T. A. Kruip. 1999b. Relationship between triacylglycerol
concentration in the liver and first ovulation in postpartum dairy cows.
Theriogenology 51: 1133-1142.
She, P., G. L. Lindberg, A. R. Hippen, D. C. Beitz, and J. W. Young. 1999. Regulation of
messenger ribonucleic acid expression for gluconeogenic enzymes during glucagon
infusions into lactating cows. J Dairy Sci 82: 1153-1163.
Ubukata, E., 0. Mokuda, Y. Sakamoto, and N. Shimizu. 1996. Effect of various
glucagon/insulin molar ratios on blood ketone body levels in rats by use of osmotic
minipumps. Diabetes Res Clin Pract 34: 1-6.
Van Winden, S. C., R. Jorritsma, K. E. Muller, and J.P. Noordhuizen. 2003. Feed intake,
milk yield, and metabolic parameters prior to left displaced abomasum in dairy cows.
J Dairy Sci 86: 1465-1471.
Wentink, G. H., T. S. van den Ingh, V. P. Rutten, K. E. Muller, and T. Wensing. 1999.
Reduced lymphoid response to skin allotransplants in cows with hepatic lipidosis. Vet
Q 21: 68-69.

57
Zerbe, H. et al. 2000. Altered functional and immunophenotypical properties of neutrophilic
granulocytes in postpartum cows associated with fatty liver. Theriogenology 54: 771-
786.
Zhu, L. H., L. E. Armentano, D. R. Bremmer, R. R. Grummer, and S. J. Bertics. 2000.
Plasma concentration of urea, ammonia, glutamine around calving, and the relation of
hepatic triglyceride, to plasma ammonia removal and blood acid-base balance. J
Dairy Sci 83: 734-740.

58
GENERAL CONCLUSIONS
General Discussion
The objective of the current study was to test whether multiple subcutaneous
glucagon injections of 7.5 and/or 15 mg/d dosages for 14 d beginning at d 2 postpartum
could prevent the development of fatty liver disease in transition dairy cows. The idea of
using glucagon for fatty liver prevention came from earlier work done in our research group
(Hippen et al., 1999a), which demonstrated the use of 14-d intravenous infusion of glucagon
to treat fatty liver and ketosis induced by feed restriction and diet supplementation with 1,3-
butanediol in lactating dairy cows. The results of the current study show that 14-d
subcutaneous injections of 15 mg/d of glucagon beginning at d 2 postpartum prevent fatty
liver development in transition dairy cows. Glucagon injections at 7 .5 mg/d dosage show a
potential for fatty liver prevention.
Subcutaneous glucagon injections increased plasma glucose and insulin and
decreased plasma NEPA concentrations in transition dairy cows predisposed to fatty liver
development postpartum because of overfeeding during the dry period. These beneficial
effects of subcutaneous glucagon administration are thought to be responsible for decrease in
liver total lipid and TAG concentrations and consequently fatty liver prevention in transition
dairy cows. There were no significant effects of glucagon administration on plasma BHBA
concentration. However, cows given the 15 mg/d of glucagon dosage tended to show

59
increase in plasma BHBA concentration around d 9 postpartum, which was similar to an
increase in BHBA concentration in the control group around the same time.
A mechanism by which glucagon is able to prevent fatty liver development is
unknown. It is possible that glucagon indirectly inhibits the rate of lipolysis and stimulated
uptake and reesterification of NEFA by adipose tissue because of increases in plasma insulin
and glucose concentrations. Glucagon also can have an effect on depletion of liver TAG pool
and/or increase of fatty acid utilization in liver by activating camitine palmitoyltransferase-1,
which leads to increased ~-oxidation and/or ketogenesis. It seems like glucagon has no effect
on the rates of VLDL synthesis and secretion from liver. This statement is supported
indirectly by our data showing that glucagon has no effect on plasma TAG concentration.
The effect of glucagon in this study was not confounded with the differences in body
condition score between cows from different treatment groups, because there were no
significant differences in body condition score between the cows from different treatment
groups throughout the study.
A use of glucagon as a preventive for fatty liver development did not cause any
negative effects on feed intake, milk production, and milk composition of dairy cows, which
makes glucagon a very useful tool for the disease prevention. Glucagon administration
decreased milk urea concentration, which suggests that it has a beneficial effect on improving
protein utilization in transition dairy cows.

60
Recommendations for Future Research
The current study demonstrated that subcutaneous glucagon injections could be used
for fatty liver prevention in transition dairy cows. However, there are still some questions
that have to be answered in order to optimize the use of glucagon for fatty liver prevention or
to come up with better ways to prevent and/or treat the disease. One of the questions is what
is the best model for fatty liver disease in transition dairy cows? Earlier studies conducted in
our research group used feed restriction and diet supplementation with 1,3-butanediol to
induce fatty liver and ketosis in lactating dairy cows. Such an approach produced a relatively
high incidence of fatty liver and ketosis in lactating dairy cows, but the etiology of naturally
occurring fatty liver disease could be completely different from what was induced by those
conditions. In the current study, we used diet supplementation with cracked corn to increase
energy density of a dry cow ration during the last 30 d of a dry period to make cows more
susceptible for fatty liver development postpartum because of over conditioning. It is
believed that cows with higher body condition scores have a higher incidence of fatty liver
disease. However, this approach was not very successful, because most of the cows in our
study did not develop severe fatty livers. A possible explanation for a failure to develop a
severe fatty liver disease in our study is that feed intake of dairy cows can start declining
during the last month of a dry period, and, in this case, extra corn feeding might not be able
to increase cows' body condition scores. Better models of fatty liver disease should be
created in the future. One of the approaches that can be used is overfeeding of cows during
the entire dry period or during the end of the lactation period plus during the dry period. Fatty

61
liver development is not only associated with high body condition scores of dairy cows but
also could be developed by feeding large amounts of grain during a dry period. So, other
alternatives than over conditioning should be considered for the disease development.
More research has to be done to study the physiology of transition and lactating dairy
cows. It would be very helpful to know what type of metabolic changes occur under normal
and pathological conditions, because in the literature you can find contradictory statements
about what is happening. For example, many authors claim that after calving transition dairy
cows experience hypoglycemic conditions while the others suggest the opposite. None of
them say what normal glucose concentration in blood of dairy cows should be around that
time. That is why greater knowledge about the physiology of transition and lactating dairy
cows would be very useful for data interpretation. Moreover, disagreements among results
from different publications sometimes happen only because of differences in approaches
used to analyze samples. Developing standardized assays would facilitate better data
comparison across different studies.
According to a current theory of fatty liver development in transition dairy cows, high
blood NEFA concentration is highly correlated with postpartum disease incidence. Future
studies of regulation of lipolysis in dairy cows can provide very useful information about the
etiology and other possible ways of fatty liver treatment and prevention.
Recent studies established a relationship between fatty liver and reproduction and
between fatty liver and immune function of dairy cows. More studies have to be done to
understand those relationships and to check whether glucagon administration has any effects
on them. Some authors are trying to relate infertility problems seen in dairy cows to low
blood insulin concentration around breeding time. More study of possible improvements of

62
reproductive performance of transition dairy cows related to the ability of glucagon
administration to increase blood insulin concentration should be done.
In addition, subcutaneous glucagon injections for 14 days are not practical for on
farm use. Other alternatives such as a slow-release formulation of glucagon should be
developed in the future and tested on transition dairy cows.

63
REFERENCES
Amer, P., J. Bolinder, and J. Ostman. 1983. Glucose stimulation of the antilipolytic effect of
insulin in humans. Science 220: 1057-1059.
Bertin, E., P. Amer, J. Bolinder, and E. Hagstrom-Toft. 2001. Action of glucagon and
glucagon-like peptide-1-(7-36) amide on lipolysis in human subcutaneous adipose
tissue and skeletal muscle in vivo. J Clin Endocrinol Metab 86: 1229-1234.
Bobe, G., B. N. Ametaj, J. W. Young, and D. C. Beitz. 2003a. Effects of exogenous glucagon
on lipids in lipoproteins and liver of lactating dairy cows. J Dairy Sci 86: 2895-2903.
Bobe, G., B. N. Ametaj, J. W. Young, andD. C. Beitz. 2003b. Potential treatment of fatty
liver with 14-day subcutaneous injections of glucagon. J Dairy Sci 86: 3138-3147.
Bremmer, D. R. et al. 2000. Etiology of fatty liver in dairy cattle: Effects of nutritional and
hormonal status on hepatic microsomal triglyceride transfer protein. J Dairy Sci 83:
2239-2251.
Cadomiga-Valino, C., R.R. Grummer, L. E. Armentano, S.S. Donkin, and S. J. Bertics.
1997. Effects of fatty acids and hormones on fatty acid metabolism and
gluconeogenesis in bovine hepatocytes. J Dairy Sci 80: 646-656.
Campbell, P. J., M. G. Carlson, J. 0. Hill, and N. Nurjhan. 1992. Regulation of free fatty acid
metabolism by insulin in humans: Role of lipolysis and reesterification. Am J Physiol
263: E1063-1069.

64
Carlson, M. G., W. L. Snead, and P. J. Campbell. 1993. Regulation of free fatty acid
metabolism by glucagon. J Clin Endocrinol Metab 77: 11-15.
Day, C. P. 2002. Pathogenesis of steatohepatitis. Best Pract Res Clin Gastroenterol 16: 663-
678.
De Boer, G., A. Trenkle, and J. W. Young. 1986. Secretion and clearance rates of glucagon
in dairy cows. J Dairy Sci 69: 721-733.
Drackley, J. K. 1999. Adsa foundation scholar award. Biology of dairy cows during the
transition period: The final frontier? J Dairy Sci 82: 2259-2273.
Drackley, J. K., M. J. Richard, D. C. Beitz, and J. W. Young. 1992. Metabolic changes in
dairy cows with ketonemia in response to feed restriction and dietary 1,3-butanediol.
J Dairy Sci 75: 1622-1634.
Drucker, D. J. 1990. Glucagon and the glucagon-like peptides. Pancreas 5: 484-488.
Drucker, D. J. et al. 2000. New developments in the biology of the glucagon-like peptides
glp-1 and glp-2. Ann NY Acad Sci 921: 226-232.
Elks, M. L., and V. C. Manganiello. 1985. Antilipolytic action of insulin: Role of camp
phosphodiesterase activation. Endocrinology 116: 2119-2121.
Folch, J., M. Lees, and G. H. Sloane Stanley. 1957. A simple method for the isolation and
purification of total lipides from animal tissues. J Biol Chem 226: 497-509.
Fourichon, C., H. Seegers, N. Bareille, and F. Beaudeau. 1999. Effects of disease on milk
production in the dairy cow: A review. Prev Vet Med 41: 1-35.

65
Gerloff, B. J. 2000. Dry cow management for the prevention of ketosis and fatty liver in
dairy cows. Vet Clin North Am Food Anim Pract 16: 283-292.
Greenfield, R. B., M. J. Cecava, and S.S. Donkin. 2000a. Changes in mrna expression for
gluconeogenic enzymes in liver of dairy cattle during the transition to lactation. J
Dairy Sci 83: 1228-1236.
Greenfield, R. B., M. J. Cecava, T. R. Johnson, and S.S. Donkin. 2000b. Impact of dietary
protein amount and rumen undegradability on intake, peripartum liver triglyceride,
plasma metabolites, and milk production in transition dairy cattle. J Dairy Sci 83:
703-710.
Gruffat, D., D. Durand, Y. Chilliard, P. Williams, and D. Bauchart. 1997. Hepatic gene
expression of apolipoprotein blOO during early lactation in underfed, high producing
dairy cows. J Dairy Sci 80: 657-666.
Gruffat, D., D. Durand, B. Graulet, and D. Bauchart. 1996. Regulation of vldl synthesis and
secretion in the liver. Reprod Nutr Dev 36: 375-389.
Grummer, R.R. 1993. Etiology of lipid-related metabolic disorders in periparturient dairy
cows. J Dairy Sci 76: 3882-3896.
Haque, M., and A. J. Sanyal. 2002. The metabolic abnormalities associated with non
alcoholic fatty liver disease. Best Pract Res Clin Gastroenterol 16: 709-731.
Hayirli, A., S. J. Bertics, and R.R. Grummer. 2002. Effects of slow-release insulin on
production, liver triglyceride, and metabolic profiles of holsteins in early lactation. J
Dairy Sci 85: 2180-2191.

66
Herdt, T. H. 1988. Fatty liver in dairy cows. Vet Clin North Am Food Anim Pract 4: 269-
287.
Herdt, T. H., T. Wensing, H.P. Haagsman, L. M. van Golde, and H.J. Breukink. 1988.
Hepatic triacylglycerol synthesis during a period of fatty liver development in sheep.
J Anim Sci 66: 1997-2013.
Hertz, R., J. Magenheim, I. Berman, and J. Bar-Tana. 1998. Fatty acyl-coa thioesters are
ligands of hepatic nuclear factor-4alpha. Nature 392: 512-516.
Herzig, S. et al. 2001. Creb regulates hepatic gluconeogenesis through the coactivator pgc-1.
Nature 413: 179-183.
Hippen, A. R. et al. 1999a. Alleviation of fatty liver in dairy cows with 14-day intravenous
infusions of glucagon. J Dairy Sci 82: 1139-1152.
Hippen, A. R. et al. 1999b. Metabolic responses of dairy cows and heifers to various
intravenous dosages of glucagon. J Dairy Sci 82: 1128-1138.
Hocquette, J. F., and D. Bauchart. 1999. Intestinal absorption, blood transport and hepatic
and muscle metabolism of fatty acids in preruminant and ruminant animals. Reprod
NutrDev 39: 27-48.
Holst, J. J. 1997. Enteroglucagon. Annu Rev Physiol 59: 257-271.
Jensen, M. D., V. J. Reiling, and J.M. Miles. 1991. Effects of glucagon on free fatty acid
metabolism in humans. J Clin Endocrinol Metab 72: 308-315.

67
Jiang, G., and B. B. Zhang. 2003. Glucagon and regulation of glucose metabolism. Am J
Physiol Endocrinol Metab 284: E671-678.
Jorritsma, R. et al. 2000a. Prevalence and indicators of post partum fatty infiltration of the
liver in nine commercial dairy herds in the netherlands. Livestock Production Science
68: 53-60.
Jorritsma, R., H. Jorritsma, Y. H. Schukken, and G. H. Wentink. 2000b. Relationships
between fatty liver and fertility and some periparturient diseases in commercial dutch
dairy herds. Theriogenology 54: 1065-1074.
Jorritsma, R., T. Wensing, T. A. Kruip, P. L. Vos, and J.P. Noordhuizen. 2003. Metabolic
changes in early lactation and impaired reproductive performance in dairy cows. Vet
Res 34: 11-26.
Katoh, N. 2002. Relevance of apolipoproteins in the development of fatty liver and fatty
liver-related peripartum diseases in dairy cows. J Vet Med Sci 64: 293-307.
Louet, J. F., G. Hayhurst, F. J. Gonzalez, J. Girard, and J. F. Decaux. 2002. The coactivator
pgc-1 is involved in the regulation of the liver carnitine palmitoyltransferase i gene
expression by camp in combination with hnf4 alpha and camp-response element
binding protein (creb). J Biol Chem 277: 37991-38000.
Mizutani, H. et al. 1999. Preliminary studies on hepatic camitine palmitoyltransferase in
dairy cattle with or without fatty liver. Vet Res Commun 23: 475-480.
Morrow, D. A. 1976. Fat cow syndrome. J Dairy Sci 59: 1625-1629.

68
Muhlhauser, I., J. Koch, and M. Berger. 1985. Phannacokinetics and bioavailability of
injected glucagon: Differences between intramuscular, subcutaneous, and intravenous
administration. Diabetes Care 8: 39-42.
Murondoti, A., M. T. Tivapasi, M. J. Geelen, T. Wensing, and A. C. Beynen. 2002. The
effect of postpartum rumen undegradable protein supplementation on hepatic
gluconeogenic enzyme activities in dairy cows with fatty liver. Int J Vitam Nutr Res
72: 336-340.
Overton, T. R., J. K. Drackley, C. J. Ottemann-Abbamonte, A. D. Beaulieu, and J. H. Clark.
1998. Metabolic adaptation to experimentally increased glucose demand in
ruminants. J Anim Sci 76: 2938-2946.
Overton, T. R. et al. 1999. Substrate utilization for hepatic gluconeogenesis is altered by
increased glucose demand in ruminants. J Anim Sci 77: 1940-1951.
Perea, A., F. Clemente, J. Martinell, M. L. Villanueva-Penacarrillo, and I. Valverde. 1995.
Physiological effect of glucagon in human isolated adipocytes. Horm Metab Res 27:
372-375.
Pickett, M. M., M. S. Piepenbrink, and T. R. Overton. 2003. Effects of propylene glycol or
fat drench on plasma metabolites, liver composition, and production of dairy cows
during the periparturient period. J Dairy Sci 86: 2113-2121.
Piepenbrink, M. S., and T. R. Overton. 2003. Liver metabolism and production of cows fed
increasing amounts of rumen-protected choline during the periparturient period. J
Dairy Sci 86: 1722-1733.

69
Puigserver, P. et al. 2003. Insulin-regulated hepatic gluconeogenesis through foxol-pgc
lalpha interaction. Nature 423: 550-555.
Pullen, D. L., J. S. Liesman, and R. S. Emery. 1990. A species comparison of liver slice
synthesis and secretion of triacylglycerol from nonesterified fatty acids in media. J
Anim Sci 68: 1395-1399.
Raoofi, A., T. T. Bazargani, and A.H. Tabatabayi. 2001. An abattoir survey on the frequency
of fatty liver syndrome in dairy cows from the suburbs of tehran. Trop Anim Health
Prod 33: 15-19.
Rayssiguier, Y., A. Mazur, E. Gueux, I. M. Reid, and C. J. Roberts. 1988. Plasma
lipoproteins and fatty liver in dairy cows. Res Vet Sci 45: 389-393.
Reid, I. M., and R. A. Collins. 1980. The pathology of post-parturient fatty liver in high
yielding dairy cows. Invest Cell Pathol 3: 237-249.
Richter, W. 0., H. Robl, and P. Schwandt. 1989. Human glucagon and vasoactive intestinal
polypeptide (vip) stimulate free fatty acid release from human adipose tissue in vitro.
Peptides 10: 333-335.
Rukkwamsuk, T., M. J. Geelen, T. A. Kruip, and T. Wensing. 2000. Interrelation of fatty
acid composition in adipose tissue, serum, and liver of dairy cows during the
development of fatty liver postpartum. J Dairy Sci 83: 52-59.
Rukkwamsuk, T., T. Wensing, and M. J. Geelen. 1999a. Effect of fatty liver on hepatic
gluconeogenesis in periparturient dairy cows. J Dairy Sci 82: 500-505.

70
Rukkwamsuk, T., T. Wensing, and T. A. Kruip. 1999b. Relationship between triacylglycerol
concentration in the liver and first ovulation in postpartum dairy cows.
Theriogenology 51: 1133-1142.
Sato, H., T. Mohamed, A. Goto, S. Oikawa, and T. Kurosawa. 2004. Fatty acid profiles in
relation to triglyceride level in the liver of dairy cows. J Vet Med Sci 66: 85-87.
She, P. et al. 1999a. Metabolic responses of lactating dairy cows to 14-day intravenous
infusions of glucagon. J Dairy Sci 82: 1118-1127.
She, P., G. L. Lindberg, A. R. Hippen, D. C. Beitz, and J. W. Young. 1999b. Regulation of
messenger ribonucleic acid expression for gluconeogenic enzymes during glucagon
infusions into lactating cows. J Dairy Sci 82: 1153-1163.
Strang, B. D., S. J. Bertics, R.R. Grummer, and L. E. Armentano. 1998. Effect of long-chain
fatty acids on triglyceride accumulation, gluconeogenesis, and ureagenesis in bovine
hepatocytes. J Dairy Sci 81: 728-739.
Tucker, J. D., S. Dhanvantari, and P. L. Brubaker. 1996. Proglucagon processing in islet and
intestinal cell lines. Regul Pept 62: 29-35.
Ubukata, E., 0. Mokuda, Y. Sakamoto, and N. Shimizu. 1996. Effect of various
glucagon/insulin molar ratios on blood ketone body levels in rats by use of osmotic
minipumps. Diabetes Res Clin Pract 34: 1-6.
Unson, C. G. 2002. Molecular determinants of glucagon receptor signaling. Biopolymers 66:
218-235.

71
Van Winden, S. C., R. Jorritsma, K. E. Muller, and J.P. Noordhuizen. 2003. Feed intake,
milk yield, and metabolic parameters prior to left displaced abomasum in dairy cows.
J Dairy Sci 86: 1465-1471.
Wentink, G. H., T. S. van den Ingh, V. P. Rutten, K. E. Muller, and T. Wensing. 1999.
Reduced lymphoid response to skin allotransplants in cows with hepatic lipidosis. Vet
Q 21: 68-69.
Yamamoto, 0., S. Oikawa, and N. Katoh. 1995. Enzyme-linked immunosorbent assay for
serum apolipoprotein b-100, a major triglyceride-transport protein in dairy cows. Am
J Vet Res 56: 1413-1417.
Yoon, J. C. et al. 2001. Control of hepatic gluconeogenesis through the transcriptional
coactivator pgc-1. Nature 413: 131-138.
Young, J. W. 1977. Gluconeogenesis in cattle: Significance and methodology. J Dairy Sci
60: 1-15.
Zerbe, H. et al. 2000. Altered functional and immunophenotypical properties of neutrophilic
granulocytes in postpartum cows associated with fatty liver. Theriogenology 54: 771-
786.
Zhu, L. H., L. E. Armentano, D. R. Bremmer, R. R. Grummer, and S. J. Bertics. 2000.
Plasma concentration of urea, ammonia, glutamine around calving, and the relation of
hepatic triglyceride, to plasma ammonia removal and blood acid-base balance. J
Dairy Sci 83: 734-740.

72
ACKNOWLEDGMENTS
Completion of the M. S. degree accomplishes one of my goals on the way to getting a
Ph.D. degree and becoming a university professor. Many people have helped me to achieve
this goal, and I apologize to those whose names are not mentioned here, but I offer them my
gratitude and best wishes.
I express sincere appreciations to my parents and my sister without whose support
and love I would not have achieved anything in this life. I thank Dr. Donald Beitz for his
support and friendship as my major professor. Recognitions and thanks are given to Dr.
Ronald Horst, Dr. Kenneth Koehler, and Dr. James Reecy for serving as my Program of
Study Committee members.
Special thanks are given to Dr. Dennis Marple for his support during my application
process to graduate school in the Animal Science Department at Iowa State University. I also
thank Dr. Mykhailo Zubets, the President of Ukrainian Academy of Agrarian Sciences, for
serving as my major professor, when I was in graduate school at the National Agricultural
University of Ukraine, and for supporting me in graduate school and during an application
process to Iowa State University.