Presumed Ocular and Central Nervous System Tuberculosis in a Patient With the Acquired...
3
Fig. 2 (Brown and Del Monte). Computed tomography of the orbits. Bilateral optic nerve head calcification is evident (arrows). The optic nerves are of normal size. known. Parents or older siblings who display more advanced optic nerve head drusen may ensure the diagnosis. Although optic nerve head drusen in patients as young as 3 years old have been described, 4,5 and several reports of choroidal neovascular membranes caused by optic nerve head drusen in children exist, 6 the condition is not widely recognized in this popula- tion. In cases where typical features of true papillede- ma are absent (bilateral involvement, venous engorge- ment, nerve fiber layer hemorrhages, and exudate), ophthalmologists should use a thorough clinical ex- amination of the patient and family members, and ultrasound or photography, to discover optic nerve head drusen. Doing so will spare the child an expensive neuroradiologic examination, which may require sedation, or even general anesthesia, and prevent needless parental worry about a brain tumor. Subretinal surgery for removal of choroidal neovas- cular membranes related to optic nerve head drusen is unknown. The predominantly fibrous and involuted appearance of the choroidal neovascular membrane in our patient, combined with the foveal pigmentary changes, led our retina service to advise against surgical intervention. REFERENCES 1. Erkkila H. The central vascular pattern of the eyeground in children with drusen of the optic disk. Graefes Arch Klin Exp Ophthalmol 1976;199:1-10. 2. Wilhelm JL, Gutman FA. Macular choroidal neovascular membrane with bilateral optic nerve drusen: case report. Ann Ophthalmol 1983;15:48-51. 3. Schon JK, Nasemann JE, Boergen KP. Vergleichende untercu- chung tiefliegender Drusen der Papille mit Scanning Laser Ophthalmoskop und Funduskamera. Klin Monatsbl Augenheilkd 1992;200:175-7. 4. Anderson CJ, Zauel DW, Schlaegel TF, Meyer SM. Bilateral juxtapapiUary subretinal neovascularization and pseudopa- pilledema in a three year old child. J Pediatr Ophthalmol Strabismus 1978;15:296-9. 5. Saudax E, Martin-Beuzart S, Lesure P, George JL. Membrane neovasculaire sous-maculaire et drusen de la papille. J Fr Ophtalmol 1990;219-22. 6. Hoover DL, Robb RM, Petersen RA. Optic disc drusen in children. J Pediatr Ophthalmol Strabismus 1988;25:191-5. Presumed Ocular and Central Nervous System Tuberculosis in a Patient With the Acquired Immunodeficiency Syndrome Cristina Muccioli, M.D., and Rubens Belfort, Jr., M.D. PURPOSE: To elucidate a case of tuberculous choroiditis in a patient with the acquired immuno- deficiency syndrome (AIDS). METHODS: We treated a 35-year-old woman who had AIDS with neurologic involvement caused by Mycobacterium tuberculosis. She developed a yellow-white chorioretinal infiltrate with indistinct borders and mild vitreitis in the right eye, probably caused by this pathogen. RESULTS: The patient's visual acuity improved in the right eye with healing of the ocular lesion and her neurologic condition improved after specific therapy with isoniazid, rifampin, and ethambutol. CONCLUSION: Tuberculosis must be considered in the differential diagnosis of posterior uveitis and choroiditis in AIDS patients. T HE GLOBAL PANDEMIC OF THE ACQUIRED IMMUNO- deficiency syndrome (AIDS) has led to dramatic resurgence of tuberculosis. A growing body of evi- Accepted for publication Sept. 1, 1995. Department of Ophthalmology, Federal University of Sβo Paulo, Paulista School of Medicine, Sβo Paulo Hospital. Inquiries to Rubens Belfort, Jr., M.D., Rua Botucatu, 822, Sβo Paulo, SP, 04023-062, Brazil; fax: (55) 11-5734002. VOL.121, N o . 2 BRIEF REPORTS 217
Transcript of Presumed Ocular and Central Nervous System Tuberculosis in a Patient With the Acquired...

Fig. 2 (Brown and Del Monte). Computed tomography of the orbits. Bilateral optic nerve head calcification is evident (arrows). The optic nerves are of normal size.
known. Parents or older siblings who display more advanced optic nerve head drusen may ensure the diagnosis.
Although optic nerve head drusen in patients as young as 3 years old have been described,4,5 and several reports of choroidal neovascular membranes caused by optic nerve head drusen in children exist,6
the condition is not widely recognized in this population. In cases where typical features of true papillede-ma are absent (bilateral involvement, venous engorgement, nerve fiber layer hemorrhages, and exudate), ophthalmologists should use a thorough clinical examination of the patient and family members, and ultrasound or photography, to discover optic nerve head drusen. Doing so will spare the child an expensive neuroradiologic examination, which may require sedation, or even general anesthesia, and prevent needless parental worry about a brain tumor.
Subretinal surgery for removal of choroidal neovascular membranes related to optic nerve head drusen is unknown. The predominantly fibrous and involuted appearance of the choroidal neovascular membrane in our patient, combined with the foveal pigmentary changes, led our retina service to advise against surgical intervention.
REFERENCES
1. Erkkila H. The central vascular pattern of the eyeground in children with drusen of the optic disk. Graefes Arch Klin Exp Ophthalmol 1976;199:1-10.
2. Wilhelm JL, Gutman FA. Macular choroidal neovascular membrane with bilateral optic nerve drusen: case report. Ann Ophthalmol 1983;15:48-51.
3. Schon JK, Nasemann JE, Boergen KP. Vergleichende untercu-chung tiefliegender Drusen der Papille mit Scanning Laser Ophthalmoskop und Funduskamera. Klin Monatsbl Augenheilkd 1992;200:175-7.
4. Anderson CJ, Zauel DW, Schlaegel TF, Meyer SM. Bilateral juxtapapiUary subretinal neovascularization and pseudopa-pilledema in a three year old child. J Pediatr Ophthalmol Strabismus 1978;15:296-9.
5. Saudax E, Martin-Beuzart S, Lesure P, George JL. Membrane neovasculaire sous-maculaire et drusen de la papille. J Fr Ophtalmol 1990;219-22.
6. Hoover DL, Robb RM, Petersen RA. Optic disc drusen in children. J Pediatr Ophthalmol Strabismus 1988;25:191-5.
Presumed Ocular and Central Nervous System Tuberculosis in a Patient With the Acquired Immunodeficiency Syndrome Cristina Muccioli, M.D., and Rubens Belfort, Jr., M.D.
PURPOSE: To elucidate a case of tuberculous choroiditis in a patient with the acquired immunodeficiency syndrome (AIDS). METHODS: We treated a 35-year-old woman who had AIDS with neurologic involvement caused by Mycobacterium tuberculosis. She developed a yellow-white chorioretinal infiltrate with indistinct borders and mild vitreitis in the right eye, probably caused by this pathogen. RESULTS: The patient's visual acuity improved in the right eye with healing of the ocular lesion and her neurologic condition improved after specific therapy with isoniazid, rifampin, and ethambutol. CONCLUSION: Tuberculosis must be considered in the differential diagnosis of posterior uveitis and choroiditis in AIDS patients.
THE GLOBAL PANDEMIC OF THE ACQUIRED IMMUNO-deficiency syndrome (AIDS) has led to dramatic
resurgence of tuberculosis. A growing body of evi-
Accepted for publication Sept. 1, 1995. Department of Ophthalmology, Federal University of Sβo Paulo,
Paulista School of Medicine, Sβo Paulo Hospital. Inquiries to Rubens Belfort, Jr., M.D., Rua Botucatu, 822, Sβo Paulo,
SP, 04023-062, Brazil; fax: (55) 11-5734002.
VOL.121, No . 2 BRIEF REPORTS 217

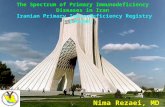
Fig. 1 (Muccioli and Beifort). Focal active chorioretinitis with mild vitreitis in the right eye.
dence now strongly suggests that tuberculosis may be the most common human immunodeficiency virus (HlV)-related illness in the world. The impact of the HIV epidemic on global tuberculosis patterns has been profound. In the United States, HIV appears to be responsible for a resurgence of tuberculosis that has resulted in more than 25,000 cases since 1985. In developing countries, tuberculosis is the most common opportunistic pathogen in persons with HIV infection.1
Tuberculosis in AIDS patients is characterized by atypical features such as cutaneous anergy to purified protein derivative skin testing, diffuse pulmonary infiltrates, and extrapulmonary disease. Before the AIDS diagnosis, signs and symptoms of tuberculosis were usually typical.2
Extrapulmonary tuberculosis is markedly more common in AIDS patients than in HIV-seronegative persons. Most cases of tuberculosis in HIV-infected patients occur before the profound immune decline associated with AIDS. The most common site of extrapulmonary tuberculosis in HIV-infected persons is the lymphatic system followed by the gastrointestinal and urogenital tracts and bone marrow. Many other extrapulmonary sites have been described, including the blood and central nervous system. Ocular involvement is rare.2
There are a few previous clinical reports of tuberculous choroiditis associated with AIDS in the literature.3,4 Morinelli and associates5 described a series of
18 patients with multifocal choroiditis diagnosed at autopsy and found only one patient with multifocal choroiditis caused by Mycobacterium tuberculosis.
A 3 5-year-old woman who was a drug abuser was hospitalized in February 1994 because of fever, lym-phadenopathy, pneumonia, weight loss, mental status changes, and lethargy. Tests of the patient's serum were positive for HIV-1. The patient fulfilled the Centers for Disease Control criteria for the diagnosis of AIDS.
Chest x-rays disclosed a reticulonodular infiltrate in the left upper lung field. Cerebrospinal fluid findings were as follows: 2,322 cells/mm3: 96% poly-morphonuclear cells and 4% lymphocytes; protein 86 mg/dl; glucose 36 mg/dl. Computed tomography suggested tuberculous meningitis, and the sputum smear was positive for M. tuberculosis.
Visual acuity was R.E.: 20/200 and L.E.: 20/20. Ophthalmologic examination showed a mild vitreitis in both eyes and a yellow-white choroidal infiltrate with indistinct borders in the superotemporal quadrant and temporal to the macula in the right eye (Fig. 1). The retina of the left eye appeared to be unin-volved. There was no papilledema in either eye. A diagnosis of presumed tuberculous chorioretinitis in the right eye was made.
The patient was treated with a triple drug therapy of isoniazid, rifampin, and ethambutol. After three months of therapy, her systemic and ocular conditions were markedly improved. The cerebrospinal
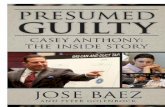
Fig. 2 (Muccioli and Belfort). Same lesion after treatment. Healed lesion. A choroidal scar is present.
218 AMERICAN JOURNAL OF OPHTHALMOLOGY FEBRUARY 1996

fluid findings were normal and she returned to normal neurologic conditions. The ophthalmologic examination disclosed a best-corrected visual acuity of 20/20 in both eyes and examination of the fundus showed a healed lesion in the right eye, without vitreitis (Fig. 2).
REFERENCES
1. Centers for Disease Control. Update: Tuberculosis elimination—United States. MMWR 1990;39:153-6.
2. Chaisson RE, Schechter GF, Theuer CP, Rutherford GW, Echenberg DF, Hopewell PC. Tuberculosis in patients with the acquired immunodeficiency syndrome: clinical features, response to therapy, and survival. Am Rev Respir Dis 1987;136:570-4.
3. Croxatto JO, Mestre C, Puente S, Gonzalez G. Nonreactive tuberculosis in a patient with acquired immune deficiency syndrome. Am J Ophthalmol 1986;102:659-60.
4. Biodi BA, Johnson MW, McLeish WM, Gass JDM. Presumed choroidal tuberculosis in a human immunodeficiency virus infected host. Am J Ophthalmol 1989;108:605-6.
5. Morinelli EN, Dugel PU, Riffenburg R, Rao NA. Infectious multifocal choroiditis in patients with acquired immune deficiency syndrome. Ophthalmology 1993;100:1014-21.
Squamous Cell Carcinoma of the Eyelid and the Acquired Immunodeficiency Syndrome Hunter Maclean, F.R.C.S.(Ed.) F.R.C.Ophth., Baljean DhiUon, B. Med. Sci., F.R.C.S.(Glasg.), F.R.C.Ophth., and James Ironside, MRC.Path.
PURPOSE: We studied a case of squamous cell carcinoma of the eyelid in a 42-year-old homosexual man with the acquired immunodeficiency syndrome (AIDS) to explore the link between squamous cell carcinoma and human Papillomavirus infection. METHOD: A rapidly growing, 3-mm lesion was removed from the right lower eyelid by excisional biopsy. RESULTS: Examination of the lesion confirmed squamous cell carcinoma. Polymerase chain reaction for human Papillomavirus 16 was positive. CONCLUSION: This case suggests a role for human Papillomavirus infection in the cause of squamous cell carcinoma in AIDS patients.
I MMUNOSUPPRESSED PATIENTS HAVE AN INCREASED
risk of developing malignancies.1 Our patient with antibodies to human immunodeficiency virus (HIV) developed squamous cell carcinoma of the eyelid skin.
In November 1991, a 42-year-old homosexual man with the acquired immunodeficiency syndrome (AIDS) was referred to our institution because of a lesion on his right lower eyelid. The AIDS-defining illness was Pneumocystis carinii pneumonia, contracted in February 1991. Other AIDS-related illnesses that he contracted included oral candidiasis, Kaposi's sarcoma, and atypical mycobacterial infection. The patient lived in Edinburgh, Scotland, and had not been exposed to excessive quantities of ultraviolet radiation.
The lesion was located in the middle third of the right lower eyelid and, at examination, measured 1 mm in diameter. It had been present for two weeks and was causing some irritation. Visual acuity was 20/20 in each eye with no abnormality on ophthal-moscopic examination. At the time of the patient's initial visit to the eye hospital his CD4+ count was 40 cells/mm3. Swabs for herpes simplex virus were negative, and the lesion was only observed. One month later the lesion had grown rapidly in size, now measuring 3 mm in diameter (Fig. 1, top). The lesion was then removed by excisional biopsy.
Pathologic examination of the biopsy material showed a well differentiated keratinizing squamous cell carcinoma that infiltrated the subepithelial tissues down to skeletal muscle (Fig. 1, bottom).
Polymerase chain reaction analysis for human Pa-pillomavirus serotypes 6, 11, 16, and 18 was performed on the biopsy material by an established technique.2 A positive band from the sample was present at a position corresponding to the human Papillomavirus 16 lane, no positive reactions were identified for the other human Papillomavirus primers, and no reaction was obtained in the negative control lanes (Fig. 2).
Accepted for publication Aug. 9, 1995. Princess Alexandra Eye Pavilion (H.M., B.D.); and Department of
Pathology, Western General Hospital (J.I.). Supported by grants from the Melville Trust for the care and cure of cancer, Western General Hospital, Edinburgh, Scotland, and the W. H. Ross Foundation, Lin-lithgow, Scotland (Dr. Ironside); and by the Medical Research Council, London, England.
Inquiries to Baljean Dhillon, B.Med.Sci., F.R.C.S., (Glasg.), F.R.C.Ophth., Princess Alexandra Eye Pavilion, Chalmers St., Edinburgh EH3 9HA, Scotland, United Kingdom; fax: (44) 31-536-3897.
VOL.121, No . 2 BRIEF REPORTS 2 1 9