Precordial Movements Right Ventricle Normal Children · phonocardiogram in the pulmonary area, (3)...
10
Precordial Movements over the Right Ventricle in Normal Children By ERNEST CRAIGE, M.D., AND ROLAND E. SCHMIDT, M.D. PHYSICAL diagnosis of the heart has im- proved considerably as a result of the availability of recording technics that enable the observer to check the physical signs with an instrumental record and thus to edu- cate himself. This technic has been particularly successful in the application of phonocardi- ography to auscultation, but the analysis of the cardiac impulse by palpation has lagged be- hind. The information to be gained by palpa- tion was recognized by James Hope' in his classic text of 1839, and the first attempt at recording precordial motion was made by Chauveau and Marey in 1861,2 using a pres- sure sensitive capsule. Later pioneers in this field include Frank,3 Mackenzie,4 Wiggers,5 and Dressler.6 Renewed interest has followed the development of electronic sensing technics and the opportunity to correlate the record with events observed at cardiac catheteriza- tion. A number of investigators7-19 have made important contributions; outstanding among these is the work of Hartman and his col- leagues in the Netherlands.20 21 It is hoped that a more scientific analysis and description of precordial motion will result, in place of the "thrust, heave and tap" to be found in most standard textbooks. The authors have studied precordial motion in normal children and, in particular, move- ments at the sternal border where alterations may be expected in congenital cardiac mal- formations affecting the right ventricle. Studies were made in the pediatric age group for three reasons: (1) no systematic study of pre- From the Departments of Medicine and Pediatrics, University of North Carolina School of Medicine, and the Cardiac Laboratory, St. George's Hospital, Lon- don, England. Supported by U. S. Public Health Service Grant 5 TI HE-5486-02, The Commonwealth Fund, and the Research Grants Committee of the University of North Carolina School of Medicine. cordial motion in normal children is available, (2) the mobile, thin chest wall of children is particularly suitable for graphic studies of low-frequency vibrations in the palpatory range, and (3) comparison of the results of these normal children with the findings in pathologic conditions is made easier by the usual absence of complicating degenerative disease of the heart or lungs. This paper concerns observations of precor- dial motion in 60 normal children who served as controls and provide a basis for comparison for certain pathologic conditions affecting the right ventricle to be described in a subsequent communication.22 Materials and Methods Sixty normal children, age 1 to 18, were studied. Their age distribution is given in table 1. There were equal numbers of boys and girls. All records were taken by one or other of the authors with the help of an assistant. Subjects were studied in the supine position with respira- Table 1 Distribution by Age and Sex of the 60 Normal Subjects Age Male 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 3 1 2 0 1 0 2 1 3 3 4 3 2 0 1 0 1 3 30 Female 0 0 0 2 5 2 4 1 2 2 3 3 1 0 1 1 3 0 30 Total C2u culation, Volume XXXII, August 1965 232 by guest on November 16, 2017 http://circ.ahajournals.org/ Downloaded from
Transcript of Precordial Movements Right Ventricle Normal Children · phonocardiogram in the pulmonary area, (3)...

Precordial Movements over the RightVentricle in Normal Children
By ERNEST CRAIGE, M.D., AND ROLAND E. SCHMIDT, M.D.
PHYSICAL diagnosis of the heart has im-proved considerably as a result of the
availability of recording technics that enablethe observer to check the physical signswith an instrumental record and thus to edu-cate himself. This technic has been particularlysuccessful in the application of phonocardi-ography to auscultation, but the analysis of thecardiac impulse by palpation has lagged be-hind. The information to be gained by palpa-tion was recognized by James Hope' in hisclassic text of 1839, and the first attempt atrecording precordial motion was made byChauveau and Marey in 1861,2 using a pres-sure sensitive capsule. Later pioneers in thisfield include Frank,3 Mackenzie,4 Wiggers,5and Dressler.6 Renewed interest has followedthe development of electronic sensing technicsand the opportunity to correlate the recordwith events observed at cardiac catheteriza-tion. A number of investigators7-19 have madeimportant contributions; outstanding amongthese is the work of Hartman and his col-leagues in the Netherlands.20 21 It is hopedthat a more scientific analysis and descriptionof precordial motion will result, in place ofthe "thrust, heave and tap" to be found inmost standard textbooks.The authors have studied precordial motion
in normal children and, in particular, move-ments at the sternal border where alterationsmay be expected in congenital cardiac mal-formations affecting the right ventricle. Studieswere made in the pediatric age group forthree reasons: (1) no systematic study of pre-
From the Departments of Medicine and Pediatrics,University of North Carolina School of Medicine, andthe Cardiac Laboratory, St. George's Hospital, Lon-don, England.
Supported by U. S. Public Health Service Grant5 TI HE-5486-02, The Commonwealth Fund, andthe Research Grants Committee of the University ofNorth Carolina School of Medicine.
cordial motion in normal children is available,(2) the mobile, thin chest wall of childrenis particularly suitable for graphic studies oflow-frequency vibrations in the palpatoryrange, and (3) comparison of the results ofthese normal children with the findings inpathologic conditions is made easier by theusual absence of complicating degenerativedisease of the heart or lungs.
This paper concerns observations of precor-dial motion in 60 normal children who servedas controls and provide a basis for comparisonfor certain pathologic conditions affecting theright ventricle to be described in a subsequentcommunication.22
Materials and MethodsSixty normal children, age 1 to 18, were studied.
Their age distribution is given in table 1. Therewere equal numbers of boys and girls.
All records were taken by one or other of theauthors with the help of an assistant. Subjectswere studied in the supine position with respira-
Table 1Distribution by Age and Sex of the 60 NormalSubjectsAge Male
123456789101112131415161718
312010213343201013
30
Female
00025241223310113030
Total
C2u culation, Volume XXXII, August 1965232
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

PRECORDIAL MOVEMENTS IN NORMAL CHILDREN
tion uncontrolled in the younger children. Inthem, we analyzed those cardiac cycles immediate-ly following expiration when a reasonably steadybaseline was achieved. In the older children,records were made during held expiration, al-though care was taken to avoid a Valsalva maneu-ver. The transducer was of capacitance type*23 andwas held on the chest by a web or rubber strap.Its probe (17 by 6 mm.) projected 4 mm. beyonda light aluminum housing, and the tip of theprobe fitted easily between the narrow interspacesof the ribs at the left sternal border. The trans-ducer has a flat response between 0.3 and 150c.p.s. according to Brecht and Boucke.23 Its timeconstant is 1.2 sec. when connected via a BeckmanAC control box, set at longest available timeconstant. Under these conditions a flat responsewas found down to 4 c.p.s. with a loss of voltageof 50 per cent between 4 and 0.5 c.p.s. Its sensi-tivity is 3 mV per 0.001 mm. excursion of theprobe.23 An outward movement of the chestyielded an upward movement on the recordingpaper. In order to check the ability of the ACsystem, with its limited time constant, to reproduceaccurately the very low frequency vibrationswhich comprise the palpable precordial move-ments, it was compared with a direct-current sys-tem,t (time constant infinite) in 13 subjects andfound to be similar though not identical (fig. 1).
Reference tracings, made simultaneously, in-cluded a single lead of the electrocardiogram wherethe QRS complex was well defined (usually leadII), a phonocardiogram, and, when feasible, anindirect carotid pulse and a respiratory tracing.The paper speed was 100 mm./sec. All curveswere monitored on an oscilloscope before theactual permanent tracing was made.
Records of precordial motion were made in thesecond, third, and fourth left intercostal spacesat the left sternal border, as well as at the apex.Tracings at the apex were taken with the subjectin the left lateral decubitus in order to bringthe heart nearer the surface of the chest. Apicaltracings were recorded with a piezo-electric trans-ducer,* since its probe, on the end of a hollowrubber tube, can be more easily moved about byhand on the dependent part of the chest while
-Infraton D-3 of Brecht and Boucke, distributed inU.S.A. by Beckman Instruments Inc., Palo Alto, Cali-fornia.
tThis modification was constructed by Dr. WilliamE. Thornton. It permitted the measurement of capaci-tative change in the Infraton transducer by means ofa bridge and carrier amplifier.:Of the several types of piezo-electric transducers
that were tried, the Pulse Microphone of Fritz Hellige& Company, Freiburg, proved to be the most satis-factory.Circulation, Volume XXXII, August 1965
A.McK.° 12 Normal
DC
DC
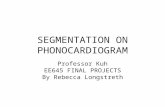
Figure 1Displacement records of a normal 12-year-old girl atthe second, third, fourth left intercostal spaces, andapex, for comparison of the Infraton transducer withAC (time constant 1.2 sec.) and DC (time constant,infinity) systems. The five curves, from above down-ward are (1) carotid pulsation, (2) phonocardiogram,(3) precordial motion, AC system, (4) precordial mo-tion, same location, DC system, and (5) electrocardio-gram. The DC record was in each case takenimmediately after the AC record and superimposed,with use of a common position of the Q wave tofacilitate comparison.
searching for the optimum location. The currentcommunication, however,- concerns the recordstaken over the right ventricle, and therefore theapexcardiogram will not be further discussed.
ResultsThe records of precordial motion at the
left sternal border in the third and fourthinterspaces were remarkably constant and re-
producible in this group of normal children.At the second interspace, however, perhapsowing to the greater and more variable dis-tance of the transducer from the heart, theresults were not consistent enough to analyze.Of the tracings from the third and fourth in-terspaces, no differences were found between
233
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

CRAIGE, SCHMIDT
Carotid
a pi ~~2 2
pFigure 2
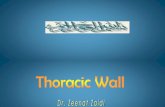
Displacement record of a normal 12-year-old boy.From above downward (1) carotid pulsation, (2)phonocardiogram in the pulmonary area, (3) displace-ment record of precordial motion in the fourth leftintercostal space, and (4) electrocardiogram, lead I.
a represents atrial systole. OM, outward movementassociated with right ventricular systole with the area
of outward movement shaded; duration of the OM is
0.15 sec. 0, outward movement. I, inward movement.To, tricuspid opening. a2 and p2, elements of thesecond sound.
the infants and older children or between thetracings of boys and girls.The normal record consists of three phases
related to atrial and ventricular activity (fig.2): (1) An atrial wave beginning approxi-mately 0.06 sec. after the onset of the P wave
was noted in 35 of the 60 subjects. It was
low and rounded in configuration and was
believed to be due to ventricular filling re-
sulting from atrial systole.24 Its inconspicuous-ness in normal subjects is in contrast to itsexaggerated appearance in certain pathologicconditions22 characterized by interference withfilling of the ventricle. (2) The onset of ven-tricular systole was marked by a sudden out-ward movement (OM) beginning 0.02 to 0.04sec. (mean 0.03 sec.) after onset of the Qwave. This period of 0.03 sec. represents the
electromechanical interval or time between on-set of electrical activity and first evidence ofmechanical contraction of the ventricle. Theonset of ventricular systole, manifest by thesudden outward movement, in turn, precededthe first sound by 0.02 to 0.03 sec. The meanQ-1 time in this series was 0.52 sec. The out-ward movement at the beginning of ventricularsystole in normal subjects was brief in dura-tion, often notched by the time of the majorelements of the first sound, and it declinedrapidly at approximately the time. of onset ofright ventricular ejection. A nadir was reachedusually by mid-systole, followed by a variableconfiguration in late systole, and further sharpnotches at the time of the second sound.(3) Diastole. The interval from the pulmonarycomponent of the second sound to a dip rep-resenting tricuspid opening had a range of0.03 to 0.08 sec. (mean 0.053 sec.). Immediate-ly following, there was an outward movementassociated with filling of the right ventricle.It did not have the briskness of the rapidfilling wave seen in the left ventricular apex-cardiogram and it merged imperceptibly withfurther variable undulations during diastasis.To characterize the curve representing ven-
tricular systole in a more objective fashion forsubsequent comparison with abnormal sub-jects three criteria were adopted (fig. 2).
1. Duration of outward movement (GO ).An arbitrary baseline was drawn horizontallyfrom the end of the electromechanical intervalacross the base of the OM. Its length repre-sented the duration of the GM. Usually no diffi-culty was encountered in finding the suddenchange in direction of the curve which markedthe onset of ventricular systole, but occasional-ly in normal, and not infrequently in abnormalsubjects, the waning portion of the "a" wavemerged with the OM. Even in these instances,however, locating the onset of the OM was notdifficult. The duration of the OM was brief,having a mean duration of 0.107 sec. in thethird, and an identical mean duration in thefourth interspace. The range was 0.00 to 0.25sec. with only two exceptions among the 60subjects. In them, the prolongation was notedin only one of the two interspaces under anal-
Circulation, Volume XXXII, August 1965
234
I
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

PRECORDIAL MOVEMENTS IN NORMAL CHILDREN
ysis and reached a maximum of 0.34 sec.2. Ratio of outward to inward movement.
Although duration of certain phases of thecardiac cycle can be accurately measured bystudies of precordial motion, amplitude ofpulsation cannot. The uncertain contributionof thickness of the chest wall and lung makefor variations in amplitude which may bemisleading. Therefore, it has been found con-venient to measure the height or depth ofoutward and inward movements in relativeterms.'12 13A ratio of outward movement to inward
movement (O/I) was calculated for the thirdand fourth interspace locations (fig. 2).Height of OM was measured from the baselineat the end of the electromechanical intervalto the peak achieved in early systole. Inwardmovement was measured as the extent of in-ward retraction from the peak of OM to thelowest point reached prior to the aortic com-ponent of the second sound. This point waschosen rather than the pulmonary componentbecause the latter could not be clearly seenin some of the abnormal subjects.Outward movement was less than inward
movement, giving a ratio less than 1.0 in allexcept two instances. The mean ratio was 0.47in the third and 0.39 in the fourth interspace.The two exceptions showed a ratio of 0/Iabove 1.0 in only one of the two interspacesanalyzed.
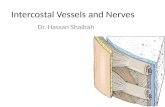
3. The area under the OM, a function ofits height and duration, was found to besmall. Again, for reasons mentioned above,the area of the OM is expressed as a ratio orArea Index (fig. 3). This ratio gives one anindex of the height and duration of the OMrelative to the depth and duration of retractionduring systole. It was found to be less than1.0 in all except three instances. In theseexceptions, the index was greater than 1.0 inonly one of the two interspaces studied.The shape of the downward curve which
followed the peak of the OM was found tobe concave in all except one subject.
In summary, these three criteria are all ex-pressions of the brevity and low amplitudeof the OM which is confined to early systoleCirculation, Volume XXXII, August 1965
PCG2 LIC'
1.1Ii''P -np P-
7
Precordi0alMovement4 LICS
2
Area index = O.0 IECG4 m1_
Figure 3Displacement record of a normal child at the fourthleft intercostal space to illustrate calculation of thearea index. The area of OM (cross-hatched) is small incomparison to the area representing retraction duringsystole (stippled). The ratio of the OM to the area ofretraction is 0.11-the area index. a2, aortic componentof second sound. p2, pulmonary component of secondsound. To, tricuspid opening.
in records taken over the right ventricle innormal children.
DiscussionThe subject of precordial pulsations is con-
fused by the variations in technics of record-ing that lead to a variety of curves, all purport-ing to represent vibrations related to cardiacactivity. It is important, therefore, to statewhat is being recorded. The vibrations ema-nating from the heart are modified and dimin-ished in intensity as they pass through over-lying structures to the surface of the chest.Here they present a spectrum of frequencies,some of which are in the audible range andare appreciated with the stethoscope. Someare lower and may, if strong enough, be per-ceived by palpation. Since the amplitude ofthese vibrations diminishes greatly with in-creasing frequency,25 there is relatively enor-mous energy in the very low frequency portion
235
, 111 *
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

CRAIGE, SCHMIDT
of the spectrum. The ear selectively discrimi-nates, thus permitting one to appreciate faint,high-frequency sounds and murmurs thatwould otherwise be blotted out by the morepowerful low-frequency vibrations. Transduc-ers used in studies of vibratory phenomenavary in their ability to respond to vibrations oflow or high frequency, and further discrimina-tion can be obtained by means of filters. Anadequate sensitivity in the lowest frequencyrange is necessary to obtain an undistorteddisplacement tracing.26 Our transducer, whenconnected with its Beckman AC control box,had a moderate fall in response below 4c.p.s. This did not result, however, in seriousalteration in configuration of the tracings asshown in comparative studies with a DC sys-tem (fig. 1). No filtering is required, since theenergy of the extremely low frequency vibra-tions effectively dominates the resulting trac-ing. A system of filters emphasizing the slightlyhigher range of 5 to 25 c.p.s., such as thatemployed by Rosa, yields useful curves but ofa completely different configuration and fordifferent purposes.9To achieve an adequate representation of
ultra-low frequency vibrations, the transducer-recording system must have a time constant(TC) of adequate length.28 With too short aTC, either at the level of the transducer, con-trol box, recorder, or connections, tracings ofa sustained pressure are distorted by rapiddecay. Thus the plateau, which should repre-sent graphically a sustained thrust at theprecordium, would appear as a peak withrapid decline and exaggerated negative phase.For ideal recordings of systolic pressure wavesof duration 0.3 sec., a TC of 10 times thisduration might be sought.28 Some of the mostwidely used commercially available trans-ducers, however, have a TC of only 0.3 sec.,thus producing serious distortions in the dura-tion and configuration of important featuresof the apexcardiograms in published papers.Our records were made with a TC of 1.2sec. which is probably shorter than ideal. Thatthis TC was satisfactory for our purposes,however, was demonstrated by comparisonof companion tracings made with DC circuitry
having a TC of infinity (fig. 1). Althoughtheoretically superior, the DC method wasnot adopted for routine use, since it is tech-nically slightly more difficult to use in theyounger subjects whose breathing cannot becontrolled. Furthermore, we preferred to usea system that is commercially available.
Further confusion is added by methods thatdo not measure displacement, but rather rateof displacement (velocity) or rate of changeof velocity (acceleration). We have preferredto concentrate on a method measuring insofaras possible displacement rather than the twotypes of differentiated curves. Displacementrecords in the very low frequency rangeprobably represent most closely the move-ments appreciated by palpation.Another source of difference in published
reports on precordial motion is the methodof applying the transducer to the chest wall.The method of holding the probe rigid froman overhanging bar or stand'0' 14 has the ad-vantage that absolute movements of the chestwall are recorded with reference to a fixedpoint in space. Where the transducer is heldby a web or rubber strap, as in our method,a record is obtained of the difference betweenthe movement of the probe and the far smallermovement of its housing which is firmlypressed against the ribs. Theoretically, wherethe whole chest moves in a heaving manner,this method would fail to represent themovement adequately and falls short of beinga true displacement record. In comparativestudies, however, we have not found that thisis a serious problem. As a practical matter,in children, where one cannot control respira-tion, the suspension of the transducer on arigid bar is unsatisfactory, since the grossmovements of respiration completely dominatethe resulting record.
In brief then, as regards technic, for com-parable tracings to be obtained in differentlaboratories, investigators should use transduc-ers that are adequate in their frequency re-sponse to pick up the vibrations under study,and the system of filtering (or absence offiltering) must be known, as well as the timeconstant. It must be made clear whether a
Circulation, Volume XXXII, August 1965
236
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

PRECORDIAL MOVEMENTS IN NORMAL CHILDREN
study is being made of displacement, or veloc-ity, or acceleration. Finally, and of somewhatless importance, is the manner in which thetransducer is applied to the chest.The interpretation of the graphic records
is very complicated. The records no doubtreflect the heart beat, but the relative con-tributions of volume and pressure changes,thrusts, recoil, and torsion are difficult toassess. The overlying lung and chest wallmodify and diminish the curves and there arefurther alterations depending on technicalaspects of the transducer-recording system.Analysis of simultaneous reference curves,however, including the indirect carotid pulse,phonocardiogram, electrocardiogram and, inabnormal subjects frequently, the intracardiacpressure pulses, enable tentative conclusionsto be drawn about the genesis of the variousfeatures of the tracings.The "a" wave that follows the onset of the
P wave of the electrocardiogram by about 0.06sec. probably represents filling of the ventriclewith atrial systole.20 25 It is absent in atrialfibrillation and follows the P waves in com-plete heart block. It is exaggerated in certainconditions characterized by altered compli-ance of the ventricle, or powerful contractionsof the right atrium. A large "a" wave is oftenaccompanied by an atrial sound, since it ismerely the palpable component of a spectrumof low-frequency vibrations some of which arein the audible range.The ventricular complex begins approxi-
mately 0.03 sec. after the onset of the QRS.No doubt there is some contraction of individ-ual muscle fibers before the gross movementthat marks the end of the electromechanicalinterval. This outward movement preceded theupward stroke of right ventricular systole insimultaneous intracardiac pressure pulses ina number of abnormal subjects who werestudied at catheterization. In them, the pres-sure pulse began its rapid upward movementat an average time of 0.06 sec. following theonset of Q. Even allowing for a cathetertransmission time of 10 msec., it is apparentthat the OM precedes the onset of the rightintraventricular pressure pulse by approxi-Circulation, Volume XXXII, August 1965
mately 20 msec.The quickly rising outward movement
reached a peak coinciding approximately withthe onset of ejection from the right ventricleand was followed by a rapid decline.The curves of precordial motion over the
right ventricle in normal subjects are, nodoubt, profoundly influenced by pulsations ofthe underlying, more powerful left ventricle.The low-frequency contribution of the ventri-cles (principally the left) to the whole surfaceof the precordium has been called the "basicpattern" by Lohr.27 It is positive during sys-tole at the apex with the subject in the leftlateral decubitus and inverted, in completemirror image, medial to this point. At the leftsternal border, however, a smaller early sys-tolic thrust of right ventricular origin is seen.Evidence that curves at the sternal border arenot merely inverted images of the apextracing, but are influenced by right ventricularemptying and filling as well, is afforded bythe trough at the time of tricuspid openingand the outward moving filling wave imme-diately following.29The diminished intensity of the "basic pat-
tern" at the left sternal border and the relativeweakness of the right ventricular contributionresult usually in the necessity of turning upthe amplitude of the recording apparatus.Thus the sharp notches, which are infrasoniccounterparts of the heart sounds, become com-paratively prominent in records taken overthe right ventricle.27
Interesting data from animal studies byAnzola30 (fig. 4) throw additional light on thepossible genesis of the precordial curves overthe right ventricle. In his experiments, dimen-sional gauges were fastened to dogs' heartsand recordings were made with the chestclosed. Normally, a prominent upward deflec-tion was noted following the R wave of theelectrocardiogram. This movement, represent-ing expansion of the ventricle at onset of sys-tole, corresponded to a change in shape of theright ventricular cavity without a change in itsvolume. This early systolic spike, (I.S.E. infig. 4) was abruptly terminated at onset ofejection, at which point there was a sharp
237
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

CRAIGE, SCHMIDT
Gauge in position no.4ISE
Gauge in position no. I
2.2
R V pressure
40mm. |;Hg.~
ECG Lead II
Figure 4Curves taken from work of Anzola showing expansionof the right ventricle of a dog in early systole, withsudden fall at time of ejection. Position number 4 ismade with a dimensional gauge fastened verticallyover the surface of the right ventricle and positionnumber I with gauge fastened horizontally. Rapidfilling (1) and slow filling (2) waves are seen in diastole.S, systole; D, diastole; A, atrial contraction; ISE,initial systolic expansion. From Anzola, J.: Am. J.Physiol. 184: 569, 1956. Reproduced by permissionof the director of the laboratory and the publisher.
downward deflection. The shape of thesecurves of right ventricular dimensions resem-bles very closely those obtained over the surfaceof the chest in our normal subjects. Anzolaattributed the initial spike to early contrac-tion of papillary muscles, drawing the tricus-pid valves down into the chamber, associatedwith a simultaneous assumption of a sphericalshape by the left ventricular cavity withbulging of the interventricular septum intothe right ventricular cavity and outward dis-placement of the wall of the right ventricle.The subsequent sharp decline occurred withejection of blood and loss of volume from theright ventricle. In early diastole a troughwas noted at the time of opening of the atrio-ventricular valves followed by a rapid fillingwave (1, fig. 4) and a slow filling wave (2,fig. 4).
The effect of increasing age on the configu-ration of precordial records has been investi-gated by Coleman et al.,3' using the technic ofkinetocardiography of Eddleman. Althoughthe method differs from ours in some respects,the curves obtained over the right ventricleare quite similar. The "right parasternal up-stroke" at the onset of right ventricular con-traction is attributed to closure and bulgingof the tricuspid leaflets. Its pattern is similarto the OM noted in our records and to the"initial systolic expansion" described by Anzo-la. It is of interest that Coleman et al.31 noteda progressive decline in motions attributed toright ventricular activity with increasing age-a fact that probably explains the lack ofattention paid to curves from the right ven-tricle in many of the studies of apexcardi-ography dealing primarily with adult sub-jects.32The measurements of duration and relative
height and the configuration of the OM justdescribed were selected to give some objec-tive criteria for the normal precordial pulsationover the right ventricle in children. The mea-surements of duration and relative height ofthe OM are similar to those introduced byEddleman.12' 13 Insofar as possible, one wouldlike to employ existing criteria, so that com-parisons can be made between studies indifferent laboratories. The brief duration ofthe OM and its relatively low amplitude withrespect to the depth of the systolic retractionin our normal subjects are similar to the re-sults of Eddleman.12 Our studies, however,are not altogether comparable owing to dif-ferences in technic, apparatus, and age ofsubjects. The criteria for defining the systolicmovement disclosed a striking uniformityamong the curves of normal children and auseful basis for comparison with abnormalsituations characterized by increased pressurein the right ventricle owing to outflow ob-struction.22The pattern of the curves of precordial
motion in early diastole reflects the effectsof tricuspid opening and filling of the rightventricle. As in the case of the systolic move-ments, it is impossible to separate altogether
Circulation, Volume XXXII, August 1965
238
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

PRECORDIAL MOVEMENTS IN NORMAL CHILDREN
the effects of left ventricular activity. Never-theless, the fact that there is a trough at thetime of tricuspid opening followed by an out-ward movement is consistent with the supposi-tion that we are observing the effects of rightventricular filling rather than merely the in-verse mirror image of left ventricular activityas seen at the apex. The trough of tricuspidopening is located 0.03 to 0.08 sec. (mean0.053 sec.) after P2. This point correspondswith the apex of the V wave in the jugularvenous pulse, which has been found in a seriesof normal subjects to be 0.056 sec. after P2by Kesteloot and Joosens.33 The measure-ment of the interval between P2 and thetrough representing tricuspid opening maybe of some value, since it has been found byHartman20 to be prolonged in pulmonary hy-pertension owing to a lengthening of isomet-ric relaxation.The definition of the range of normal ultra-
low frequency records of displacement overthe right ventricle may be of value for severalreasons: (1) timing of events of the cardiaccycle, particularly where pulsatory tracingsare taken in conjunction with other referencetracings; (2) assessment of the range of normalon palpation with improvement to be expectedin technic of this aspect of the physical exami-nation in much the same fashion as ausculta-tion is improved by phonocardiography; (3)comparison with abnormal curves obtained inconditions of right ventricular overload. Here,the inexpensive and nontraumatic aspects ofthe method are advantageous.The limitations of the method should also
be listed and include the following: (1) theresults are largely nonspecific and empirical;(2) great care and experience are required inorder to obtain accurate and reproduciblecurves; (3) unless the equipment is capableof sensing and recording displacement curvesin the ultra-low frequency range, misleadingartifacts may be encountered; (4) much workhas to be done to standardize and makecomparable the results from different labora-tories. Mackenzie summarized the situationin 1925 by saying "The whole subject ofcardiography is in need of thorough and pains-Circulation, Volume XXXII, August 1965
taking review." This is still true.
Summary and Conclusions1. Sixty normal children were studied by
means of ultra-low frequency displacementrecords from the chest wall over the rightventricle, in conjunction with other referencetracings.
2. The record of normal children in thislocation is characterized by (a) an incon-stant and small movement associated withatrial systole; (b) a brief outward move-ment beginning 0.03 sec. after Q and ofonly moderate height with respect to thesubsequent inward movement which beginsat approximately the onset of right ventricularejection; (c) quick vibrations at the time ofthe elements of the second sound followedby a trough marking tricuspid opening andan outward movement representing filling ofthe right ventricle.
3. Criteria for measuring the outward move-ment are described: (a) duration of outwardmovement is less than 0.25 sec.; (b) ratio ofoutward to inward movement is less than 1.0;(c) the area under the outward movement issmall relative to the area of the curve repre-senting systolic retraction; (d) the fallingslope of the outward movement is concave.
4. The possible genesis of the main featuresof the displacement record are discussed.
5. Ultra-low frequency displacement recordsover the right ventricle in normal childrenare useful in timing events of the cardiaccycle, in improvement of palpation by meansof graphic records, and as a basis for compari-son with abnormal records in conditions ofright ventricular overload.
6. The limitations of the method are given.
AcknowledgmentWe are indebted to Dr. A. Leatham and Mr. G.
Davies and the staff of the Cardiac Laboratory ofSt. George's Hospital for help and advice as well asfor providing the physiologic and angiocardiographicstudies on many of the patients. Dr. H. A. Lohr andMr. E. vail Vollenhoven of Utrecht provided manyvaluable suggestions, and we are grateful to theInstitute of Medical Physics of Utrecht for testing thefrequency characteristics of our transducer. Additionalhelp was provided by Dr. H. Harned and Dr. W. E.
239
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

CRAIGE, SCHMIDT
Thornton of North Carolina Memorial Hospital andDr. Jack Fleming of Pensacola, Florida.
References1. HOPE, J.: A Treatise on the Diseases of the
Heart and Great Vessels. Ed. 3. London, Wil-liam Kidd, 1839.
2. CHAUVEAU, A., AND MAREY, E. J.: Determinationgraphique des rapports de la pulsation cardi-aque avec les mouvements de l'oreillette etdu ventricule, obtenue au moyen d'un ap-pareil enregistrant. Gaz. med. Paris 31: 675,1861.
3. FRANK, O., AND HESS, 0.: Ober das Cardiogramund den ersten Herzton. Verhandl. d. Kong.f. inn. Med. 25: 285, 1908.
4. MACKENZIE, J.: Diseases of the Heart. Ed. 4.London, Oxford University Press, 1925.
5. WIGGERS, C. J.: An adaptation of Frank's seg,ment capsules for clinical use. J. A. M. A. 64:1305, 1915.
6. DRESSLER, W. P.: Pulsations of the wall of thechest. Arch. Int. Med. 60: 225, 1937.
7. LUISADA, A. A., AND MAGRI, G.: The low fre-quency tracings of the precordium and epi-gastrium in normal subjects and cardiac pa-tients. Am. Heart J. 44: 545, 1952.
8. JOHNSTON, F. D., AND OVERY, D. C.: Vibrationsof low frequency over the precordium. Circula-tion 3: 579, 1951.
9. ROSA, L. M.: The "displacement" vibracardio-gram of the precordium in the low frequencyrange. Am. J. Cardiol. 4: 191, 1959.
10. EDDLEMAN, E. E., WILLIS, K., REEVES, T. J.,AND HARRISON, T. R.: The kinetocardiogram.I. Method of recording precordial movements.Circulation 8: 269, 1953.
11. EDDLEMAN, E. E.: Ultra low frequency precordialmovements. Kinetocardiograms. Am. J. Cardiol.4: 649, 1959.
12. EDDLEMAN, E. E., AND THOMAS, H. D.: Therecognition and differentiation of right ven-tricular pressure and flow loads. Am. J. Cardiol.4: 652, 1959.
13. EDDLEMAN, E. E., HUGHES, M. L., AND THOMAS,H. D.: Estimation of pulmonary artery pres-sure and pulmonary vascular resistance fromultra-low frequency precordial movements(kinetocardiograms). Am. J. Cardiol. 4: 662,1959.
14. DELIYANNIS, A. A., GILLAM, P. M. S., MOUNSEY,J. P. D., AND STEINER, R. E.: The cardiac im-pulse and the motion of the heart. Brit. HeartJ. 26: 396, 1964.
15. AGRESS, C. M., AND FIELDS, L. G.: New methodfor analyzing heart vibrations. I. Low fre-quency vibrations. Am. J. Cardiol. 4: 184,1959.
16. NIXON, P. G. F., AND WOOLER, G. H.: Phases ofdiastole in various syndromes of mitral valvu-
lar disease. Brit. Heart J. 25: 393, 1963.17. HOLLDACK, K., AND WOLF, D.: Einfiihrung in
die Mechanokardiographie. Stuttgart, GeorgThieme Verlag, 1960, XII.
18. BENCHIMOL, A., DIMOND, E. G., WAXMAN, D.,AND SHEN, Y.: Diastolic movements of theprecordium in mitral stenosis and regurgita-tion. Am. Heart J. 60: 417, 1960.
19. LoHR, H. A., VOLLENHOVEN, E. VAN, ROTTER-DAM, W. VAN: Fundamentals in vibrocardiog-raphy. Precordial accelerography and accelera-tion ballistocardiography. Am. Heart J. 66:108, 1963.
20. HARTMAN, H.: The External Jugular VenousTracing and the Apex Cardiogram. Proceed-ings of the third European Symposium forBallistocardiography. Brussels, 1962.
21. SNELLEN, H. A.: Diagnostiek door handoplegging.Nederle. tydschr. geneesk. 103: 2039, 1959.
22. SCHMmT, R., AND CRAIGE, E.: Precordial move-ments over the right ventricle in childrenwith pulmonary stenosis. Circulation 32:, 241,1965.
23. BRECHT, K., AND BOUCKE, H.: Neues elektro-statisches Tiefton-Mikrophon und seine An-wendung in der Sphygmographie. Pfluger'sArchiv. ges. Physiol. 256: 43, 1952.
24. HARRISON, T. R., LOWDER, J. A., HEFNER, L. L.,AND HARRISON, D. C.: Movements and forcesof the human heart. Circulation 18: 82, 1958.
25. RAPPAPORT, M. B., AND SPRAGUE, H. B.: Thegraphic registration of the normal heartsounds. Am. Heart J. 23: 591, 1942.
26. FOULGER, J. H., SMITH, P. E., AND FLEMING,A. J.: Changes in the cardiac vibrational in-tensity in response to physiologic stress. Am.Heart J. 34: 507, 1947.
27. LOHR, H. A.: Precordial motion: The nature ofprecordial displacement and the condition ofits recording. In press.
28. ROBERTS, D. V., AND SHERWOOD JONES, E.: Anew system for recording the apex beat. Lan-cet 1: 1193, 1963.
29. LoHR, H. A.: Personal communication.30. ANZOLA, J.: Right ventricular contraction. Am.
J. Physiol. 184: 567, 1956.31. COLEMAN, H. N., FINNEY, J. O., SHEFFIELD,
L. T., PRUITT, C., AND HARRISON, T. R.: Pre-cordial movements in relation to age. Am.Heart J. 67: 53, 1964.
32. COULSHED, N., AND EPSTEIN, E. J.: The apex-cardiogram: Its normal features explained bythose found in heart disease. Brit. Heart J.25: 697, 1963.
33. KESTELOOT, H., AND JOOSENS, J. V.: Le poulsveineux jugulaire. Confrontation hemodynam-ique. Proceedings of the third European Sym-posium for Ballistocardiography. Brussels,1962.
Circulation, Volume XXXII, August 1965
240
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from

ERNEST CRAIGE and ROLAND E. SCHMIDTPrecordial Movements over the Right Ventricle in Normal Children
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1965 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.32.2.232
1965;32:232-240Circulation.
http://circ.ahajournals.org/content/32/2/232.citationlocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on Novem
ber 16, 2017http://circ.ahajournals.org/
Dow
nloaded from