SEGMENTATION ON PHONOCARDIOGRAM Professor Kuh EE645 FINAL PROJECTS By Rebecca Longstreth.
32
SEGMENTATION ON PHONOCARDIOGRAM Professor Kuh EE645 FINAL PROJECTS By Rebecca Longstreth
-
Upload
troy-clarkston -
Category
Documents
-
view
218 -
download
0
Transcript of SEGMENTATION ON PHONOCARDIOGRAM Professor Kuh EE645 FINAL PROJECTS By Rebecca Longstreth.
SEGMENTATION ON PHONOCARDIOGRAM
Professor KuhEE645 FINAL PROJECTS
By Rebecca Longstreth

DEFINITIONS
• Phonocardiogram– Graph representing sounds made by the human heart
• Cardio cycle– Represented by S1, S2, S3 and S4
• S1– Orignates at the closure of the atrioventricular valves– recordable between 91hz and 179 hz
• S2– Originates at the aortic an pulmonic valves– Can reach 200 hz
• S3 and S4– Represent cardiac wall vibrations– Not all audible, low density
DEFINITIONS
• S1 and S2– Sound goes left to right
• S3 and S4– Right to left

Reason for Segmentation
• Tool to assist doctors in diagnosing heart malfunctions accurately
• Prevents mistakes in diagnoses
• Improved quality care for patients
• Doctors experience benefits everyone

Choices of Segmentation
• Fourier transform
• Laplace transform
• Wavelet decomposition

Fourier transform
• Reasons not used:– Phonocardiograms are not smooth wave
signals– Not linear time invariance– Non-stationary– Non-harmonic

Laplace transform
• Reasons not used:– Initial condition does not exist
Wavelet decomposition
• Preferred method of analyzing phonocardiograms
• Time limited and frequency limited
• Utilize digital filters and down sampling

Wavelet decomposition conditions
• Normalize the amplitude of all artifacts before transformation to avoid amplification errors
• Short segmentation window for high frequency
• Long segmentation window for low frequency
• Short lengths of data are considered due to file size considerations
Phonocardiogram anomalies
• Fetal acoustic signals inconsistent from one sound to the next
• Wave shape can change
• Frequency could shift
• Amplitude, duration and position in the cardiac cycle can change
• Background noise of the mother and the shielding affect of the womb
GOAL
• Isolate one cycle for analysis• Identify S1 and S2• Boundaries of S1 and S2• Systolic and diastolic periods
– Systolic: time interval from beginning of S1 to the beginning of S2
– Diastolic: time interval from beginning of S2 to the beginning of S1
• Associate frequency spectrum
Research
• According to Cardiologists interviewed– There is no way to recognize S1 and S2 using
only a phonocardiogram– Location of the probe can radically affect the
signal strengths of S1 and S2 on the same individual
Finding S1 and S2: Method 1
• Compare EKG and the phonocardiogram simultaneously to ensure accurate designation of S1 and S2
• S1 occurs shortly after the EKG peak– The first PCG signal following the EKG peak
is S1
• S2 occurs shortly after the 2nd EKG peak
Finding S1 and S2: Method 1
• Disadvantage– EKG requires expensive bulky and fragile
equipment to perform
• Need– Robust, portable, easy to use low cost
equipment
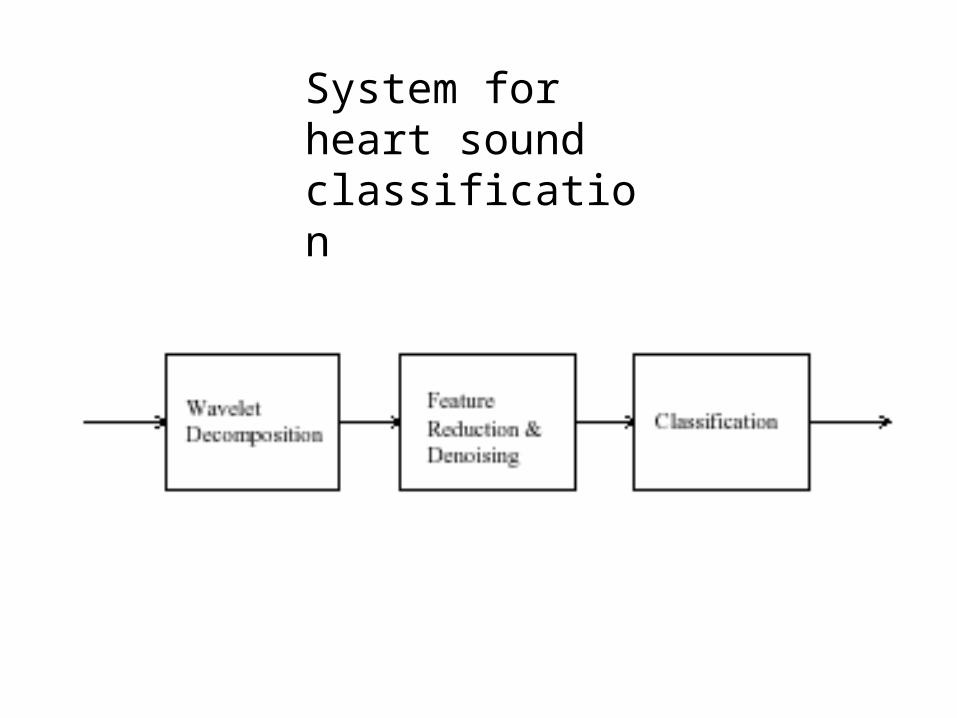
System for heart sound classification
Wavelet Decomposition
• Heart sounds (sampled at an 8kHz sample rate, 16 bits/sample) are first hand segmented into 4096 sample segments, each consisting of a single heartbeat cycle.
Feature Reduction & Denoising
• Figure 1. A Simple Heart Sound Classification System• .Each segment is transformed using a 7 level wavelet
decomposition, based on a Coifman 4th order wavelet kernel (relative symmetry and fast execution).
• The resulting transform vectors, 4096 values in length, are reduced to 256 element feature vectors by discarding the 4 levels with shortest scale.
• Neural network in the classifier reduces noise. The magnitudes of the remaining coefficients in each vector are calculated, then normalized by the vector’s energy.

Classification
Each feature vector is classified using a three layer neural network (256 input nodes, 50 hidden nodes, and 5 output nodes).
Results And Discussion
• RESULTS AND DISCUSSION• The system was evaluated using heart sounds
corresponding to – normal– mitral valve prolapse(MVP)– coarctation of the aorta (CA), – ventricular septal defect (VSD), – and pul-monary stenosis (PS).
• The classifier was trained using 10 shifted versions (over a range of 100 samples) of a single heartbeat cycle from each type.
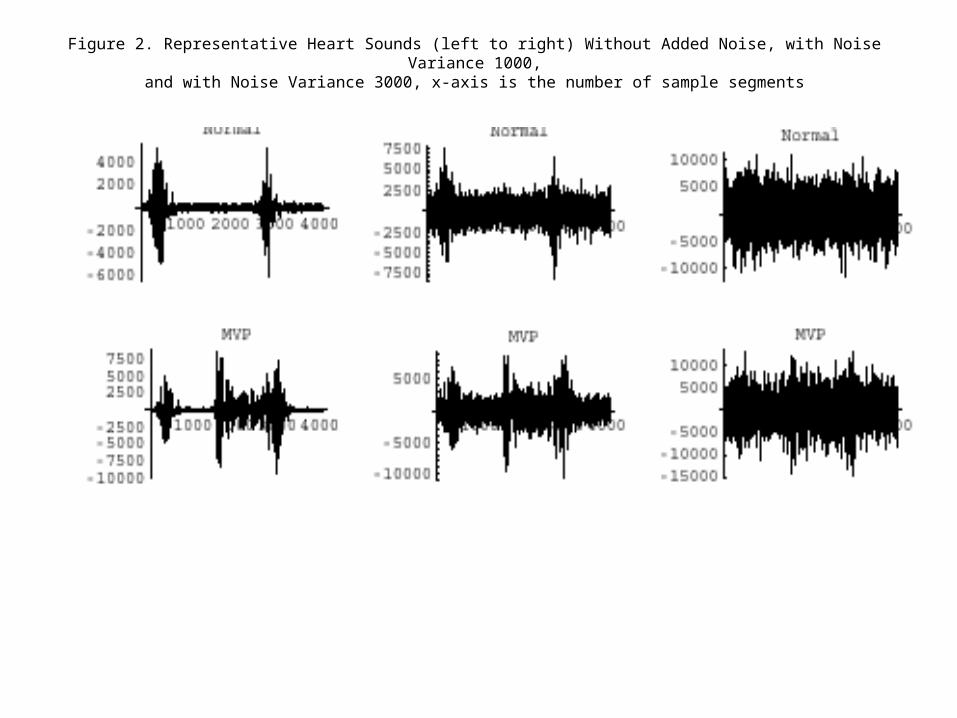
Figure 2. Representative Heart Sounds (left to right) Without Added Noise, with Noise Variance 1000,and with Noise Variance 3000, x-axis is the number of sample segments

Figure 2. Representative Heart Sounds (left to right) Without Added Noise, with Noise Variance 1000,
and with Noise Variance 3000,x-axis is the number of sample segments

Figure 3. Feature Vectors Corresponding to the Heart Sounds in Figure 2, x-axis is the number of feature vectors

Figure 3. Feature Vectors Corresponding to the Heart Sounds in Figure 2, x-axis is the number of feature vectors
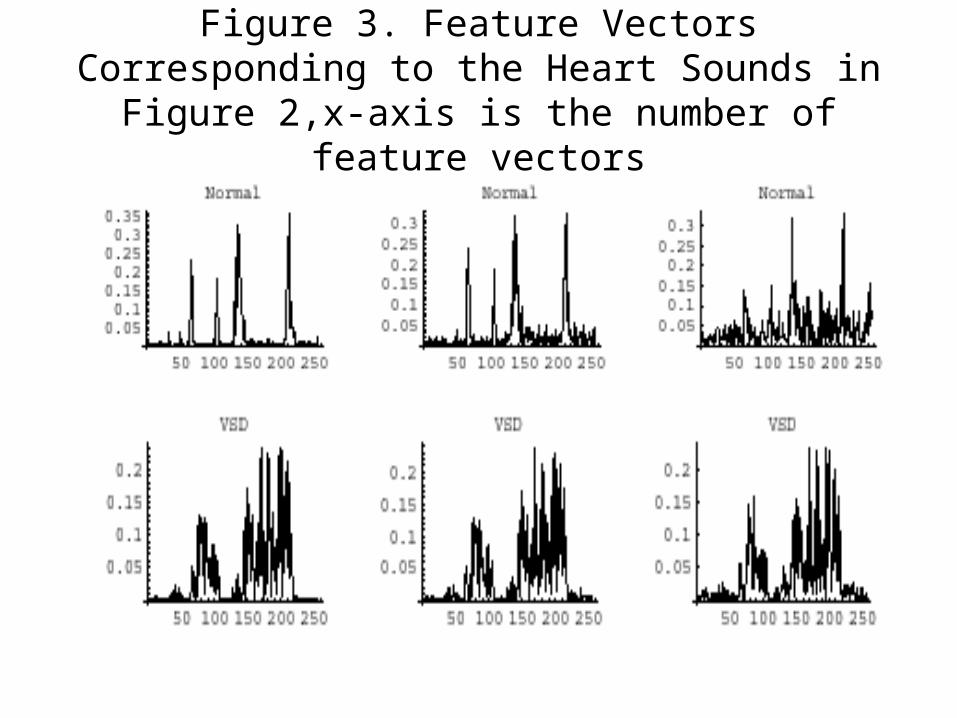
Figure 3. Feature Vectors Corresponding to the Heart Sounds in Figure 2,x-axis is the number of
feature vectors

Figure 3. Feature Vectors Corresponding to the Heart Sounds in Figure 2,x-axis is the number of
feature vectors
Feature vectors with additive noise
• The feature vectors produced for these examples in Figure 3. key features remain relatively stable even with addiditive noise.

Figure 4. Classification Accuracy (in Percent) as a Function of the Variance of the Added Noise
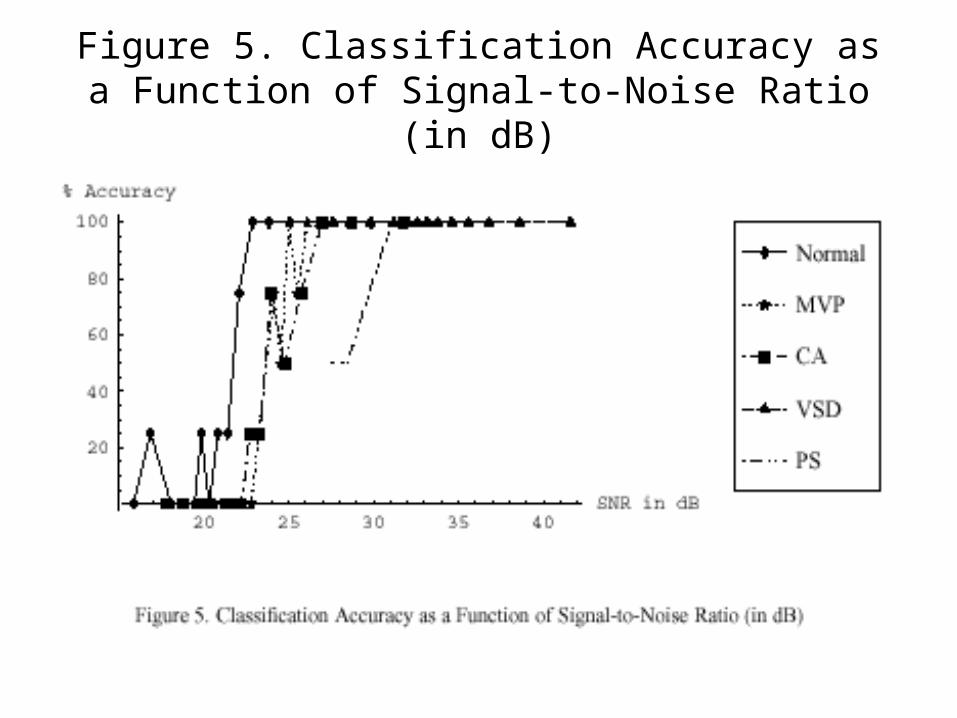
Figure 5. Classification Accuracy as a Function of Signal-to-Noise Ratio (in dB)

• the sounds differ widely (e.g., by a factor of approximately 16:1 comparing a typical normal heartbeat• with one exhibiting VSD). Accounting for this variation, classification accuracy as a function of signal-to-• noise ratio (SNR) is shown in Figure 5. For an SNR above 31dB (which is easily obtainable under• most practical circumstances) classification accuracy is 100%.

• REFERENCES• Barschdorff, D., U. Femmer, and E. Trowitzsch (1995, Sept. 10-13). Automatic phonocardiogram
signal analysis in infants based on wavelet transforms and artificial neural networks. In Computers in Cardiology 1995, pp. 753–756. IEEE, Vienna, Austria.
• http://www.ida.liu.se/~rtslab/publications/2001/reed01a-eurosim.pdf• Barschdorff, D., U. Femmer, and E. Trowitzsch (1995, Sept. 10-13). Automatic
phonocardiogram signal analysis in infants based on wavelet transforms and artificial neural networks. In Computersin Cardiology 1995, pp. 753–756. IEEE, Vienna, Austria.
• Donnerstein, R. L. and V. S. Thomsen (1994, September). Hemodynamic and anatomic factors affecting the frequency content of Still’s innocent murmur. The American Journal of Cardiology 74, 508–510.
• Durand, L.-G. and P. Pibarot (1995). Digital signal processing of the phonocardiogram: review of the most recent advancements. Critical Reviews in Biomedical Engineering 23(3/4), 163–219.
• El-Asir, B., L. Khadra, A.H. Al-Abbasi, and M.M.J. Mohammed (1996, Oct. 13-16). Multireso-lution analysis of heart sounds. In Proc. of the Third IEEE Int’l Conf. on Elec., Circ., and Sys., Volume 2, pp. 1084–1087. Rodos, Greece.
• Rajan, S., R. Doraiswami, R. Stevenson, and R. Watrous (1998, Oct. 6-9). Wavelet based bank
• of correlators approach for phonocardiogram signal classification. In Proc. of the IEEE-SP Int’l Symp. on Time-Frequency and Time-Scale Analysis, pp. 77–80. Pittsburgh, PA.

• REFERENCES
• Shino, H., H. Yoshida, K. Yana, K. Harada, J. Sudoh, and E. Harasawa (1996, Oct. 31 - Nov. 3). Detection and classification of systolic murmur for phonocardiogram screening. In Proc. of the
• 18th Int’l Conf. of the IEEE Eng. in Med. and Biol. Soc., Volume 1, pp. 123–124. Amsterdam, The Netherlands.
• http://www.cinc.org/Program/p7b-1.htm• THE ANALYSIS OF HEART SOUNDS FOR SYMPTOM
DETECTION AND MACHINE-AIDED DIAGNOSIS, Todd R. Reed, Nancy E. Reed and Peter Fritzson, The Netherlands
• H. Liang, S. Lukkarinen, and I Hartimo, Heart Sound Segmentation Algorithm Based on Heart Sound Envelogram, Helsinki, Finland
• H. Liang, S. Lukkarinen, and I Hartimo, A Boundary Modification Mehtod for Sound Segmentation Algorithm, Helsinki, Finland
• Abdelhani Djebbari, and Fethi Bereski Reguig, Short-time Fourier Transform Analysis of the Phonocardiogram Signal, Algiers