Preconception Care and Contraception for HIV-infected Women
31
Preconception Care and Contraception for HIV- infected Women Deborah Cohan, MD, MPH Associate Professor University of California San Francisco
description
Preconception Care and Contraception for HIV-infected Women. Deborah Cohan, MD, MPH Associate Professor University of California San Francisco. I have no financial disclosures. Learning Objectives. Describe the elements of a preconception evaluation for HIV+ women who desire conception - PowerPoint PPT Presentation
Transcript of Preconception Care and Contraception for HIV-infected Women

Preconception Care and Contraception for HIV-infected Women
Deborah Cohan, MD, MPHAssociate Professor
University of California San Francisco

I have no financial disclosures.

Learning Objectives
Describe the elements of a preconception evaluation for HIV+ women who desire conception
Discuss counseling points to review during a preconception visit with an HIV+ woman
Describe a safe method of conception for HIV+ woman/HIV- man serodiscordant couple.
List the pros/cons of various contraceptive methods for HIV+ women

What are reproductive rights?
The basic right of all couples and individuals to decide freely and responsibly the number, spacing and timing of their children and to have the information and means to do so, and the right to attain the highest standard of sexual and reproductive health.
World Health Organization

amfAR, n=4831 US adultsemail survey (2008)

HIV+ women internalize stigma around conception
Women Living Positive Survey n=700 HIV+ women on ARVs for 3+ yrs 59-61% believed could have children if appropriate care 59% believed society strongly urges not to have
children Caucasian (67%) vs. Hispanic (53%), (p < 0.05) South (66%) vs. Northeast (52%) or Midwest (55%), (p <
0.05) ID (62%) vs. FP/GP (62%) vs. NP or PA care (48%) (p <
0.05)
Squires et al. AIDS PATIENT CARE and STDs 2011

Fertility desires among HIV+US reproductive-aged women 35%Cross-sectional, n=118
Rochester 20% yes, 15% unsure12% of previously sterilized (4% tubal regret in US)
Cross-sectional, n=182
British Columbia
25.8%
Cross-sectional, n=181
Baltimore 59%
Probability sample, n=1421 (34,833 women, 53,177 men)
US, HCSUS 29% women28% men
¹Chen Fam Plann Persp 2001, ²Stanwood Contraception 2007, ³Ogilvie AIDS 2007, 4Oladapo J Natl Med Assoc 2005, Finocchario-Kessler AIDS Behav 2010

Chen et al. Family Planning Perspectives, 2001
“Being infected with HIV dampens but does not come close to eliminating individuals’ desires and intentions to have children.”

Unintended pregnancy
US general population 49% pregnancies unintendedUS, WIHS
232 adults 77% pregnancies while using contraception (vs. 60% HIV-)
US 1090 adolescents 83.3% unplanned49-52% HIV status known
Italy 334 on ARV 57.6% unplanned
Finer/Henshaw Perspec Sex Repro Health 2006; Massad AIDS 2004; Koenig AJOG 2007; Floridia Antivir Ther 2006

Establish reproductive desires
WHO? Every reproductive-aged women Even if amenorrhea, no current male sexual
partner WHEN?
Early and Often▪ Puts the issue “on the map”▪ New life circumstances/partners, new medications
(drug-drug interactions), new developments in HIV

I want to get pregnant!

Preconception Care HIV history
Nadir/current CD4, viral load, ARV hx, resistance Disclosure, adherence Serostatus of children
Medication review (HIV, non-HIV, OTC) Medical hx
Asthma, DM, HTN, obesity, HBV, HCV Reproductive hx
STIs, dysplasia/Tx, prior pregnancy outcomes, sexual, contraceptive, menstrual, infertility hx
Social hx/Habits EtOH, drug, nicotine, nutrition/exercise Violence/abuse, social support
Family genetic history

HIV-related counseling
Pregnancy impact on HIV ARV efficacy
Sexual transmission (92% with ARV) Perinatal (0.4% if VL <500 at delivery) Adherence and disclosure
ARV safety Avoid preconception/1st trimester EFV Caution with d4T/ddI Avoid NVP initiation if CD4 > 250 ARVs and PTD
▪ Preconception/1st trimester: OR 1.71 (1.09-2.67) Pros/cons of ARV initiation preconception vs. 2nd trimester
Donnell Lancet 2010; Tubiana CID 2005; Hitti JAIDS 2004; Shapiro NEJM 2010; Kourtis AIDS 2007

OI-related counseling
<200: TMP-SMX risk NTD, CV and urinary defects Folic acid (mostly 6mg)
▪ CV anomalies OR 1.24 (0.94-1.62) ▪ Multiple anomalies OR 6.4 (none) to 1.9 (+ folic acid)▪ BUT… risk TMP-SMX prophylaxis/Tx failure
Defer pregnancy until d/c TMP-SMX? <50: Azithromycin vs. clarithromycin
DHHS Guidelines 2010 (aidsinfo.nih.gov); Hernandez-Diaz 2000; Czeizel 2001; Hernandex-Diaz 2001; Safrin 1994; Razavi 2002

Other preconception counseling
Co-infections HBV (2 active NRTIs) HCV
▪ 10-20% transmission▪ RBV = category X
Avoiding incident CMV, Toxo Prenatal/postnatal care
Genetic testing Delivery route (TOL if VL < 1000) Infant feeding, AZT prophylaxis, HIV testing
Optimizing health Vaccination, diet/exercise, smoking/drug use Psychosocial referrals Contraception Tovo CID 1997, Gibb Lancet 2000, Alter 2006; Polis CID 2007; Ng-Giang 2010

How to manage serodiscordant couples?

Many HIV+ heterosexual adults in serodiscordant relationships
POS NEG
UNK
HCSUS, (1996 data) Currently married or with heterosexual partner
Chen et al. Family Planning Perspectives, 2001
HIV + WOMEN HIV+ MEN
54% 52%

Safe conception:HIV+ woman and HIV- man
1. Predict ovulation (kit, BBT, cervical mucus) 2. Ejaculate into cup or spermicide-free condom 3. Home insemination with 5-10 cc syringe
+ +or

I don’t want to get pregnant!

A case….
32 yo G4P1T3 coming for her routine HIV appointment.
On TDF/FTC/DRV/r
Irregular menses but no other complaints
She is sexually active with HIV-negative male partner of 4 months.
Uses condoms “always”

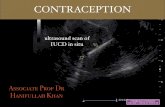
Contraception Failure (1st Year)
Hatcher: Contraceptive Technology 16th Edition 1994.
14%
20%
19%
3%
6%
9%
0.5%
0.5%
0.2%
0.1%
0.8%
0.02%
0% 5% 10% 15% 20%
Vasectomy
Implants
Injectable Progestin
Tubal Ligation
Copper IUD
Pill
Condom
Diaphragm
Withdrawal/Rhythm
TypicalLowest Expected

What method of contraception would you recommend?
1. Combined oral contraceptive pill 2. Vaginal ring 3. Depo-provera (DMPA)4. Intrauterine device (IUD)5. IUD or DMPA

ARVs and Oral Contraceptive Pills
NO CHANGE TDF (FEM-PrEP?) RAL
HORMONE LEVELS EFV (400mg): EE AUC ETR ATV IDV
HORMONE LEVELS EFV (600mg): NG AUC NVP APV DRV/r LPV/r NFV RTV TPV/r
El-Ibiary Eur J Contracept Reprod Health Care. 2008, Sevinsky Antivir Ther 2011, Anderson Br J Clin Pharmacol. 2011

Depo-medroxyprogesterone acetate (DMPA) and ARVs
No Δ DMPA levels among women on: NFV NVP EFV Other PIs?
No Δ CD4 or viral load with DMPA
Cohn Clin Pharm Ther 2007; Nanda Fertil Steril 2008; Watts Contraception 2008

Hormonal contraception and HIV progression
Any impact probably mitigated by HAART
Cohort Kenya, n=248
DMPA vs none @ HIV acquisition
viral set-point (0.33log), lower CD4
Cohort Kenya, n=283
DMPA vs OCP vs none postpartum
No difference in viral load, CD4 to 24 mos postpartum
Cohort Multicenter, n=4109
Impant/inject vs. OCP vs none
No difference in progression (ART-eligible/death)
RCT Zambia, n=595
IUD vs. DMPA vs. OCPs, ARV-naïve
Progression (CD4<200/death) DMPA (AHR 1.6; 1.2-2.3), OCP (AHR 1.7; 1.1-2.5) vs. IUD
Cohort Uganda, Zimbabwe, n=303
DMPA vs OCP vs none after seroconversion
No difference in progression to AIDS (CD4<200 or WHO 3/4)
Baeten AIDS 2005, Richardson AIDS 2007, Stringer AIDS 2009, Morrison JAIDS 2011

Morrison BJOG 2001; Sinei Lancet 1998; Richardson AIDS 1999; Heikinheimo Human Repro 2006
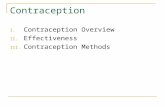
IUDs are safe for HIV+ women
No evidence of infectious complications 156 HIV+, 493 HIV- (Kenya; Copper IUD) Overall complications @ 24 mos: HR 1.0 (0.6-1.6) PID: 2% for HIV+ vs. 0.4% for HIV- (p=0.09)

Morrison BJOG 2001; Sinei Lancet 1998; Richardson AIDS 1999; Heikinheimo Human Repro 2006
IUDs are safe for HIV+ women
No evidence of infectious complications 156 HIV+, 493 HIV- (Kenya; Copper IUD) Overall complications @ 24 mos: HR 1.0 (0.6-1.6) PID: 2% for HIV+ vs. 0.4% for HIV- (p=0.09)
No evidence of genital tract shedding of HIV Copper IUD n=98 (Kenya): 4 mos s/p insertion: OR 0.6
(0.3-1.1) LNG-IUS (Mirena) n=12: no difference pre vs. post-
insertion ▪ 10/12 on HAART▪ On-going studies

Morrison BJOG 2001; Sinei Lancet 1998; Richardson AIDS 1999; Heikinheimo Human Repro 2006
IUDs are safe for HIV+ women
No evidence of infectious complications 156 HIV+, 493 HIV- (Kenya; Copper IUD) Overall complications @ 24 mos: HR 1.0 (0.6-1.6) PID: 2% for HIV+ vs. 0.4% for HIV- (p=0.09)
No evidence of genital tract shedding of HIV Copper IUD n=98 (Kenya): 4 mos s/p insertion: OR 0.6
(0.3-1.1) LNG-IUS (Mirena) n=12: no difference pre vs. post-
insertion ▪ 10/12 on HAART▪ On-going studies
WHO Medical Eligibility Criteria category 2 Benefits generally outweigh theoretical or proven risk AIDS, but NOT “clinically well on ARV” category 3 for insertion▪ Not recommended unless other methods not available/not
acceptable

Caring for an HIV+ woman of reproductive age?
Comprehensive sexual hx and determine fertility desires
Preconception visit = harm reduction Validating fertility desires Optimize woman’s health Prevent perinatal and sexual HIV transmission
Contraception visit Consider drug-drug interactions with hormones Promote long-acting reversible methods
▪ IUD = underutilized option

National Perinatal HIV Hotline (24/7) (888) 448-8765
UCSF RID Pager (24/7) (415) 443-8726
ReproIDHIV listserv Sponsored by NCCC, IDSOG, UCSF RID
Fellowship Want to join? contact Shannon Weber at:

Thank you!
“Do we have to fill our patients’ lives with years or those years with life?”
Augusto Enrico Semprini