Practical Class Manual Physiology
65
PRACTICAL CLASS MANUAL PRACTICAL CLASS MANUAL PRACTICAL CLASS MANUAL PRACTICAL CLASS MANUAL VETERINARY PHYSIOLOGY VETERINARY PHYSIOLOGY VETERINARY PHYSIOLOGY VETERINARY PHYSIOLOGY Cardiovascular and Respiratory Physiology Cardiovascular and Respiratory Physiology Cardiovascular and Respiratory Physiology Cardiovascular and Respiratory Physiology Name ___________________________ Name ___________________________ Name ___________________________ Name ___________________________ Admission No.___________________ Admission No.___________________ Admission No.___________________ Admission No.___________________ Compiled by Compiled by Compiled by Compiled by Dr. R. Kumar, Professor Dr. R. Kumar, Professor Dr. R. Kumar, Professor Dr. R. Kumar, Professor Dr. K. B. Sharma, Dr. K. B. Sharma, Dr. K. B. Sharma, Dr. K. B. Sharma, Professor Professor Professor Professor Department of Veterinary Department of Veterinary Department of Veterinary Department of Veterinary Physiology Physiology Physiology Physiology College of Veterinary & Animal Sciences College of Veterinary & Animal Sciences College of Veterinary & Animal Sciences College of Veterinary & Animal Sciences CSK HPKV, Palampur CSK HPKV, Palampur CSK HPKV, Palampur CSK HPKV, Palampur – 176 062 176 062 176 062 176 062 200 200 200 2009
Transcript of Practical Class Manual Physiology
-
PRACTICAL CLASS MANUALPRACTICAL CLASS MANUALPRACTICAL CLASS MANUALPRACTICAL CLASS MANUAL
VETERINARY PHYSIOLOGYVETERINARY PHYSIOLOGYVETERINARY PHYSIOLOGYVETERINARY PHYSIOLOGY Cardiovascular and Respiratory PhysiologyCardiovascular and Respiratory PhysiologyCardiovascular and Respiratory PhysiologyCardiovascular and Respiratory Physiology
Name ___________________________Name ___________________________Name ___________________________Name ___________________________
Admission No.___________________Admission No.___________________Admission No.___________________Admission No.___________________
Compiled byCompiled byCompiled byCompiled by
Dr. R. Kumar, ProfessorDr. R. Kumar, ProfessorDr. R. Kumar, ProfessorDr. R. Kumar, Professor
Dr. K. B. Sharma, Dr. K. B. Sharma, Dr. K. B. Sharma, Dr. K. B. Sharma, Professor Professor Professor Professor
Department of Veterinary Department of Veterinary Department of Veterinary Department of Veterinary PhysiologyPhysiologyPhysiologyPhysiology
College of Veterinary & Animal SciencesCollege of Veterinary & Animal SciencesCollege of Veterinary & Animal SciencesCollege of Veterinary & Animal Sciences
CSK HPKV, Palampur CSK HPKV, Palampur CSK HPKV, Palampur CSK HPKV, Palampur 176 062 176 062 176 062 176 062
2002002002009999
-
PRACTICAL CLASS MANUALPRACTICAL CLASS MANUALPRACTICAL CLASS MANUALPRACTICAL CLASS MANUAL
VETERINARY PHYSIOLOGYVETERINARY PHYSIOLOGYVETERINARY PHYSIOLOGYVETERINARY PHYSIOLOGY Cardiovascular and Respiratory PhysiologyCardiovascular and Respiratory PhysiologyCardiovascular and Respiratory PhysiologyCardiovascular and Respiratory Physiology
Name_________________________________Name_________________________________Name_________________________________Name_________________________________
Admission No.________________________Admission No.________________________Admission No.________________________Admission No.________________________
Compiled byCompiled byCompiled byCompiled by
Dr. R. Kumar, ProfessorDr. R. Kumar, ProfessorDr. R. Kumar, ProfessorDr. R. Kumar, Professor
Dr. K. B. Sharma, Professor Dr. K. B. Sharma, Professor Dr. K. B. Sharma, Professor Dr. K. B. Sharma, Professor
Department of Veterinary PhysiologyDepartment of Veterinary PhysiologyDepartment of Veterinary PhysiologyDepartment of Veterinary Physiology
College of Veterinary & Animal SciencesCollege of Veterinary & Animal SciencesCollege of Veterinary & Animal SciencesCollege of Veterinary & Animal Sciences
CSK HPKV, Palampur CSK HPKV, Palampur CSK HPKV, Palampur CSK HPKV, Palampur 176 062 176 062 176 062 176 062
2002002002009999
-
i
TABLE OF CONTENTS
Sr. No.
Name of Experiment Page No.
Date Instructors Signature
1. Introduction to haematology 1
2. Introduction to anticoagulants 2
3. Collection of Blood Samples from various animals and birds
4
4. Coagulation of Blood, Bleeding Time and Clotting Time
6
5. Erythrocyte Sedimentation Rate 10
6. Determination of Packed Cell volume 13
7. Estimation of Haemoglobin 16
8. Erythrocyte Fragility test 20
9. Blood Grouping 22
10. Total Erythrocyte Count (TEC) 25 11. Total Leukocyte Count (TLC) 30 12. Preparation of Blood Smear and Differential
Leukocyte Count (DLC) 33
13. Platelet Counting 38
14. Blood Pressure- Mean Arterial Pressure (MAP) and Central Venous Pressure (CVP)
41
15. Recording of Electrocardiogram (E.C.G.) 45 16. Recording of Respiration rate, Heart rate
and Pulse rate 50
DEMONSTRATION EXERCISES:
17. Plasma Volume and Blood Volume 54
18. Cardiac Output 57
Annexure: Normal Cardiac, Respiratory And Hematological Values In Different Animals
61
-
1
INTRODUCTION TO HAEMATOLOGY Haematology is the study of blood and is concerned primarily with the study of formed
elements of blood. These include: Erythrocytes or red blood cells (RBC) Leucocytes or white blood cells( WBC) Thrombocytes or platelets (PLT)
Routine haematological examination includes the determination of haemoglobin concentration, haematocrit (HCT) or packed cell volume (PCV) of cells in circulation and differential count of leucocytes based on the study of stained blood smear. Besides this, bleeding time, clotting time, specific gravity of blood, erythrocyte fragility etc are also determined.
Components of blood and their functions Blood is the fluid tissue of the body that flows through the vascular channels (arteries,
capillaries and veins) and transports the vital nutrients and waste products of the body. Other important functions include defending the body against micro-organisms, homeostasis and maintenance of body temperature.
The blood has two major components- cellular and fluid. The cellular component consists of erythrocytes, leucocytes and thrombocytes. Thrombocytes are smallest (1 to 4 m in diameter) and the leucocytes are the largest of all the cells with a wide range of size (9 to 20 m).
Red blood cells constitute the highest number (6.3 106 /l) of formed elements in circulation followed by platelets (2.5 -5 lakh /l) and white blood cells (5 to12 103 /l). Note: 1 litre =106 l and 1l =1 cumm. Expression cumm is now obsolete.
Formed elements are suspended in the fluid component of blood called plasma and are thus able to perform their functions under normal conditions. However, if blood is removed from the blood vessel, it soon clots. The blood remains fluid as long as it remains inside the vascular system. On clotting, the clear fluid separates out called as serum, while the formed elements are trapped in the clot. Composition of serum is similar to plasma except that the protein fibrinogen, which is present in plasma is absent in serum as it is converted to fibrin and used in clot formation. Thus, if blood is being collected for haematological examination, it should not be allowed to clot.
-
2
EXERCISE NO. 1: INTRODUCTION TO ANTICOAGULANTS.
These are the chemicals which exert their effect by creating a clotting defect resembling that of certain clinical diseases, during which there is inhibition of formation of one or more clotting factors. The various anti-coagulants used are:
1. Ammonium and Potassium Oxalate: 6 parts of Ammonium Oxalate hydrated 1.38 gms, Potassium Oxalate hydrated 0.89 gms and Water 100 ml. 0.1 ml of this is enough for 1 ml of blood. To prevent deterioration, 1 ml of 40% formalin is added.
The blood collected can be very safely used for haematocrit, haemoglobin estimation, RBC and WBC counts, prothrombin time and bilirubin concentration etc except for ESR. If the blood film is to be drawn; it should be made without delay after the collection of blood with double oxalate.
Let the anti-coagulant (double oxalate) be mixed up with the blood in the collecting tube depending upon the volume of blood to be collected. For collecting 5 ml of blood, pipette 0.5 ml of double oxalate solution in the tube and keep in oven at 700 C. The oxalate will spread along the inner side of the tube uniformly.
2. Sodium Citrate: 3.8% aqueous solution is used. To 9 parts of blood, 1 part of sodium citrate is added and mixed. One ml of blood requires 2-4 mg of sodium citrate.
3. Heparin: It is a natural anti-coagulant which aids in maintaining blood in a fluid state. The main source in the body is mast cells (liver, lungs etc). Heparin inhibits the reaction between thrombin and fibrinogen and also interferes with the formation of thromboplastin, which is potentiated by Heparin co-factor normally present in the blood. Heparin retards agglutination and lyses of platelets. Heparin is used in the ratio of 0.1 to 0.2 mg per ml of blood. Heparinised blood should not be used for blood films as it gives faint blue colouration to the back-ground on staining.
4. E.D.T.A. or Versene or Sequestrene: The di-sodium salt of ethylene diamine-tetra-acetic acid (EDTA) is a powerful anti-coagulant. It forms highly stable chelates with divalent metals. It is used in the concentration of 1 to 2 mg per ml of blood. This can be used in the blood transfusion also. It also prevents blood platelets clumping in vitro, so can be employed for platelets count.
5. Dicoumarol (Bishydroxycoumarin): It is obtained from spoiled sweet clover. This is inactive in vitro. The coumarin anti-coagulants affect the transport of vitamin K to its site of action. Vitamin K is required for normal synthesis of prothrombin and other clotting factors. It interferes with factor VII and factor X in the liver. It also reduces the Christmas factor (IX). It reduces the adhesiveness of platelets. It also increases
-
3
antithrombin concentration in plasma (the interaction between thrombin and antithrombin has a destructive nature). It is used to check the intravascular coagulation effect which is reversed by administration of vitamin K.
6. Hirudin: It is present in the buccal glands of leech. It is a powerful anti-coagulant. It inhibits the conversion of prothrombin to thrombin.
7. Venoms: The venoms of certain snakes contain a powerful anti-coagulant effect, which interferes with the action of thromboplastin or they deplete the blood fibrinogen.
8. Contact and Smoothness of Surface: The clotting of the blood can be prevented when it comes in contact with the tissue fluid or with the substance which is wet or has a smooth surface. When the vessel in which the blood is collected is coated with thin layer of paraffin wax, blood remains in fluid state for half an hour.
-
4
EXERCISE NO. 2: COLLECTION OF BLOOD SAMPLES FROM DIFFERENT FARM ANIMALS.
Blood: It is a connective tissue in a fluid state. Blood consists of cellular elements and the fluid called the plasma in which are suspended the red cells (Erythrocytes), white cells (leukocytes) and platelets (Thrombocytes). The mammalian blood contains about 52% plasma and 48% corpuscles by volume. By weight they are 55% and 45% respectively. The plasma contains a large number of proteins and enzymes. For the studies on the blood, it is collected from various sites/ routes in different farm animals. Procedure: The blood can be collected from different blood vessels of the body (artery, arteriole, capillaries, small veins, large veins and even from heart), but the veins being superficial in their location and quite easily approachable, the blood is normally collected from the veins. The venous blood also gives a clear picture of the arterial blood and also serves well for both haematological examinations and biochemical estimations. The capillary and the arterial blood can also be used but is difficult to collect. In case of large animals such as cattle, horses, sheep, goat, camel and buffalo, the blood is mostly collected from jugular veins (present in the jugular furrow at the neck). In case of smaller animals e.g. dog and cat, the blood is collected from cephalic vein or femoral vein. The blood can easily be colllected with a syringe and needle or with a hypodermic needle alone. The needle used should be sharp. Before collecting the blood, see that the syringe and needle are clean and sterile. Hairs from the area over the jugular furrow are clipped and the part is cleansed and disinfected with 70% alcohol or methylated spirit. The vein is distended by putting a little pressure at the base of neck at jugular furrow with the thumb or fingers and needle of appropriate gauge is inserted in the jugular vein. The gauge/length of the needle and site of blood collection for different animals should be as follows:
Species Gauge* Length of needle in inches Site of blood collection Horse 18 - 20 2 - 3 Jugular Vein Camel 18 - 20 2 - 3 Jugular Vein Cattle 16 - 18 2 - 3 Jugular Vein Dog 20 - 22 2 - 3 Cephalic/Femoral Vein Sheep & Goat 18 - 20 2 - 3 Jugular Vein Pig 16 - 20 2-3 & 6 when the blood is to
be collected from the ear Jugular Vein or Ear Vein
Cat 20 - 24 1 Cephalic/Femoral Vein Poultry 20 - 24 3/4 - 1 Heart or wing vein Rabbit 18 - 22 1 - 3 Heart
*One gauge =One part of an inch, for example 15 gauge is 1/15th of an inch.
-
5
When little blood is required, it can be obtained from the ear vein. Select small vein on the back of the earlobe, clip the hair, clean the site with methylated spirit and allow it to dry. Keep the head steady. The vein is punctured by a sharp prick with the help of a hypodermic needle. If the blood flow is in stasis and comes after squeezing only, then make a fresh puncture and collect the blood. Pigs: The blood is collected from tail, ear vein and heart using hypodermic needle of 14-20 gauge and 1-6" length depending upon the site of the collection of blood. The neck of the pig is very thick, so it is difficult to approach the jugular vein. While collecting the blood from the heart, insert the needle between 2nd and 3rd ribs; push it downward and forward until it pierces the heart. There will be a gush of blood. But once the heart is injured, there will be continuous bleeding and that may lead to the death of the animal. So the collection of blood from the ear and tail is safe. Poultry: In poultry blood is collected from wing vein and heart. Remove the feathers over the vein. Apply 70% methanol. Press the vein with the help of thumb and wing vein will become prominent. Insert hypodermic needle of 20 - 24 gauge and 3/4" - 1" length in opposite direction to the flow of the blood. A needle of 3" length and 20 - 24 gauge should be used for collection of blood from heart. Push the needle downward and between the clavicles or over the window on the left side of tissues formed by ventral canal and ribs. If the heart is injured more, excessive bleeding will cause the death of the bird.
Precautions: 1. The needle should always be inserted in opposite direction of the flow of blood. 2. The blood can be collected directly or transferred into a vial or tube containing
anticoagulants. Pressure should be released before the withdrawal of hypodermic needle from the vein to avoid formation of haematoma.
3. Four to five ml of the blood is sufficient for all haematological examinations. 4. Syringe used must be cleaned and dried and the blood must not be allowed to
coagulate in the syringe. The syringe should be cleaned immediately after the collection of the blood.
-
6
EXERCISE NO. 3: COAGULATION OF BLOOD
It is the conversion of fibrinogen to fibrin which forms meshwork of proteins, in the interstices of which the formed elements of blood are entangled and the serum, a yellow coloured fluid oozes out. During coagulation, first of all, there is formation of thromboplastin which is formed from two sources that is Extrinsic (from tissue) and Intrinsic (from plasma), which converts prothrombin to thrombin in the presence of ionized calcium and globulin fractions of normal plasma that is Factor V, Factor VII and Factor X. The thrombin so formed acts on the two arginyl - Glycine bonds of fibrinogen to liberate peptide material and expose the donor groups required for subsequent polymerization of molecules by disulphide bonds to form fibrin. The whole process of coagulation of blood can be divided into three phases i.e. First Phase: Antihaemophilic Globulin + Platelets+Plasma thromboplastin Component (PTC) Intermediate product Intermediate product + Factor V+ Factor VII + Ca Thromboplastin + Ca Second Phase: Prothrombin Thrombin Third Phase: Fibrinogen Fibrin (Clot) + Factor XIII (Firmness of clot or syneresis) Coagulation Time or Clotting Time: Many methods have been used by the haematologists for the determination of coagulation time and the results obtained do not match with one another due to differences in the techniques used and the conditions to which blood samples are subjected. 1. Drop Method: Place several drops of blood on a clean glass slide and go on
passing a needle through one drop at a time at one minute interval. When the fibrin threads stick to the needle and are dragged along it, the coagulation has taken place and the time is noted from a stop watch from the time of collection of blood to the time of coagulum formation. In dry warm weather, the slide should be kept on beaker of warm water to avoid evaporation. Precaution: The blood should be collected from a sharp deep puncture and the first few drops should be discarded.
2. Modified drop method: Two glass discs 5mm in diameter are cemented to glass slide. Blood is placed in these and the slide is kept inverted on beaker of warm water (40 0C). The coagulation is noted by seeing the shape of the drop while keeping the slide vertical.
3. Capillary Method: The method is most commonly used and found satisfactory. In this method, the blood is drawn into the fine capillary tubes. The site is cleaned, dried
-
7
and punctured with a sharp needle. First drop is wiped off. The second drop is drawn into the capillary tube filled by capillary action. Avoid touching of the tube to the skin of the animal. After one minute place the capillary tube in such a way that index finger is kept above and thumb below the capillary tube and break a bit of the capillary with slight pressure from thumb. If there is no thread formation between the two broken ends when taken apart gently, then break the other one after every 30 seconds intervals till the gap is bridged. Note the time from the time of receiving the blood till the bridge formation. This is the coagulation time of that individual.
4. Lee and White Method: Take three clean test tubes rinsed with 0.85% normal saline. Remove blood from vein with a clean syringe and needle rinsed with saline. Remove needle and transfer gently about 1 ml of blood to each tube. Place the tube in water bath at 370C. After about two minutes, gently tilt one of the tubes and observe for clotting. If the clot has not formed, tilt the second tube followed by third tube. Repeat the process after every one minute interval till the third tube shows clotting. The time is noted since the puncturing of vein and the development of firm clot in third tube. Precautions: The tube used should be small in internal diameter i.e. 8 mm. The vein should be punctured cleanly with the first attempt. The suction of the blood should be gentle to avoid drawing of air bubbles into syringe. The tube should be kept close to the body temperature.
Haemostasis: It is the arrest of bleeding. When a blood vessel is damaged, the platelet masses aggregate at the site of the injury occluding the flow of blood and prevent bleeding. The immediate arrest of bleeding is aided by:
1. Constriction of blood vessel walls (by 5-HT liberated from disintegration of platelets).
2. Formation of blood platelet plug (The platelets first of all agglutinate and then fuse to form a solid mass). The agglutination of platelets requires the presence of ADP, traces of thrombin and a protein factor. The action of ADP is calcium dependent.
A few minutes after the onset of bleeding, the clotting of blood occurs. After about half an hour when the capillaries reopen due to accumulation of the tissue metabolites, the area is sealed and the haemostasis is maintained. Later the clot retracts and is replaced by the fibrous tissue. The fibrin network of the clot may act as scaffold for the new collagen and new capillaries. The haemostasis will be normal when there is: 1. Vasoconstriction. 2. Formation of plug by platelets and 3. The coagulation takes place in normal way. Otherwise haemostasis is deranged e.g. during thrombocytopenia
-
8
when the circulating platelets concentration is below 50,000/cu mm and the blood continues to ooze in small drops (purpura haemorrhagica). The bleeding time is prolonged due to failure of constriction of minute blood vessels, low concentration of platelets and due to the defective coagulation. Bleeding Time: It is the time taken for the formation of clot at the point of puncture, detected by watching when bleeding stops as ascertained by frequent soaking of the blood by means of a filter paper. It can be measured by:
Dukes' Method: To determine the bleeding time by Dukes' method, the hair are clipped from the back of ear lobe. Moisten a piece of cotton with 70% alcohol and sterilize the middle or tip of the ear of animals and middle of the finger in human being. Let this dry. Make an incision 4 to 5 mm deep with a sharp scalpel near the tip of the lobe of ear or in the pulp of finger. Place a half folded filter paper after half minute interval over the site from where the blood is oozing out of the puncture. The filter paper should be placed gently over the site. The blood spot on the filter paper become smaller and smaller with passage of time. This shows that the flow of the blood is gradually ceasing. When the blood ceases to flow, record the time. Bleeding time is the time elapsed between the puncture and cessation of bleeding. The normal clotting and bleeding time in the farm animals and man is as follows:
Animal Coagulation Time
Bleeding Time
Horse < 11 min. 1 to 5 minutes in most domestic animals.
Cattle or Ox 6 min. Sheep 1 to 2 min Goat 2 min.
Buffalo 4 to 6 min. Pig 3 min. Dog 2 min. Cat 1 min. Fowl 4 min.
Rabbit 4 min. Man 3 to 10 min.
-
9
Exercise No. 3: Determination of Clotting Time and Bleeding Time:
Species Clotting Time Bleeding Time
Cattle
Buffalo
Sheep
Goat
Dog
Fowl
Human
Date: (Instructor)
-
10
EXERCISE NO. 4: ESTIMATION OF ERYTHROCYTE SEDIMENTATION RATE (ESR)
Erythrocyte Sedimentation Rate (ESR): When citrated or oxalated blood is allowed to stand undisturbed, the corpuscles aggregate into clumps and start falling down at a certain rate. The fall of corpuscles during a certain fixed time in the blood is determined. Normally, this rate is uniform by virtue of the plasma viscosity due to serum globulin, fibrinogen, lipids, amino acids etc and out of which globulin is probably the most important factor. The increase in fibrinogen and globulin concentration leads to an increase in sedimentation rate whereas increase in albumin decreases the sedimentation rate. The various methods employed for the study are: 1. Linzenmeier method 2. Westergren method 3. Wintrobe method 1. Linzenmeier method: The time required for the upper level of corpuscles to fall to
a fixed distance is measured. 2. Westergren method: The fall of the corpuscles which have taken place during the
specified time is noted. This is widely used method and most accurate. Method: Fill the Westergren tube up to `0' mark and fix it in the stand. While fixing the tip of the tube, it must be pressed hard against the rubber at the bottom before releasing the finger; otherwise the blood will flow out. Note the fall of the corpuscles after a fixed time. 3. Wintrobe method: i) Collect the venous blood in a tube containing an anti-coagulant. ii) Take a clear dry Wintrobe tube and fill the tube up to the 10 cm mark either with
the help of a syringe and needle with polyethylene catheter sufficient to reach to the bottom of Wintrobe tube or with a Pasteur pipette.
iii) Adjust the blood present above the mark with the help of a filter paper or cotton. Place the tube in the stand and keep it undisturbed.
iv) Note the fall of the corpuscles at intervals of 10, 20, 30, 60 minutes to 24 hours. The erythrocyte sedimentation rate is always represented as mm/time interval.
Precautions: i) The blood collected should be used for determination of sedimentation rate within
two hours of its time of collection. Further delay may be associated with increased suspension stability of the blood.
ii) Since the sedimentation rate increases with the increase in temperature, so the test be carried out at a temperature not less than 220C and not more than 370C. If
-
11
the blood used has previously been kept in a refrigerator, it should be allowed to come to the above temperature before being used.
iii) The haematocrit tubes should be kept vertical as a 30 change in the angle from the vertical will considerably increase sedimentation rate.
Factors affecting ESR: i) Presence of anticoagulants: - An increase in sodium salicylates will lower the
ESR. It also depends on the plasma fibrinogen concentration. ii) External temperature: - ESR is increased during increase in temperature i.e. when
the temperature is more than 37.50C and decreased when environmental temperature is less than 220 C.
iii) Presence of fibrinogen and globulin in high concentration increases the ESR. iv) Presence of albumin in high concentration retards the ESR. v) Concentration of RBC: - In anaemia, the ESR is increased (organic diseases) but
under certain conditions there is no effect on ESR e.g during anaemia (functional disorders) as retardation force is equal to sedimentation rate.
vi) Addition of lecithin delays the ESR. vii) Addition of cholesterol increases the ESR. viii) Presence of pneumococcus type III produces an increase in ESR. It is also
increased during pulmonary TB, old age, traumatic pericarditis. ix) Position of the tube: - In horizontal condition the retardation force is equal to the
downward force, but when the tube is inclined the retardation force is less than downward force, so there is an increase in ESR.
x) The size of the displacing particle i.e. by aggregating the RBC (Rouleaux formation) causes increased ESR during normal conditions, diseases and during pregnancy.
xi) In conditions of inflammation or tissue destruction, the globulin content as also fibrinogen content go up and consequently there is increase in the sedimentation rate. A steady rise is an indication of worsening of the condition.
xii) During chronic infections, globulin and fibrinogen contents are increased i.e. Pulmonary tuberculosis, Pneumonia, septic infections and pregnancy etc
Erythrocyte Sedimentation Rate in different domestic species of animals: Horse : 15-38 mm. /40 Min. Cattle : 0-2 mm. /60 Min. Dog : 1-6 mm. /30 Min. Pig : 0-6 mm. /30 Min. Cat : 1-6 mm. /30 Min.
-
12
Exercise No. 4. : - Determination of Erythrocyte Sedimentation Rate (ESR) in cattle and Buffalo blood.
Observations: - For Cattle Time (Min.) Fall of Corpuscles (mm) E. S. R (mm/min.) 0 5 10 15
30 60 120
For Buffalo: Time (Min.) Fall of Corpuscles (mm) E. S. R (mm/min.) 0 5 10 15
30 60 120
Date: (Instructor)
-
13
EXERCISE NO. 5: DETERMINATION OF PACKED CELL VOLUME (PCV) OR HAEMATOCRIT VALUE
The term haematocrit means to separate the blood. By centrifugation, the blood is separated into three distinct compartments namely; (a) the erythrocyte mass at the bottom called the packed cell volume or PCV, (b) a white to grey layer of leukocytes and occurring immediately above the red cell mass and called Buffy coat and (c) the blood plasma on the top. There are two methods of determining PCV i.e. Wintrobe tube method and Micro-capillary method.
a) Wintrobe Method: Procedure: i) Take a Wintrobe tube having a uniform 3mm bore and calibrated by a 10 cm scale
with millimetre divisions. The scale on the left side is read from top to bottom for ESR while scale on the right in the reverse order for PCV.
ii) Take anticoagulant added blood in a syringe to which a needle is already fixed with a polyethylene tubing of a 2mm diameter or suck the blood into a Pasteur pipette with a rubber bulb attached.
iii) The tip of the polyethylene tubing or Pasteur pipette having a long narrow end is inserted to the bottom of the haematocrit tube (Wintrobe tube) and the blood is forced out by pressure on the syringe/rubber bulb. The pipette is slowly withdrawn simultaneously.
iv) Fill the Wintrobe tube up to the mark 0, i.e. 1 ml of blood. v) Place the tubes in the centrifuge machine and centrifuge at the speed of 3000 rpm
for 30 minutes. vi) After thirty minutes, read the packed cell volume from the bottom to top. The
packed cell volume is read in percentage.
b) Micro-capillary Method: Procedure:
Take micro capillary tube and fill 2/3rd of it with blood (anticoagulant mixed blood for non-heparinized capillary and fresh blood without anticoagulant for heparinized capillary). Apply sealing wax/clay on one side and centrifuge at 8000 rpm for 8 minutes. Place the capillary tube on the reading plate device and PCV in percentage.
-
14
Precautions: 1. Use anticoagulant added blood for estimating the PCV with Wintrobe tube method
and while using non-heparinized capillary in Micro-capillary method. 2. The Wintrobe tube should be filled up to the top i.e. up to 0.00 and avoid formation
of air bubble(s) in the tube. 3. In case the level of the blood has gone above 0.00 mark, adjust it immediately with
cotton or cloth.
Normal PCV values in % for various domestic species are: Cattle - 35 (24-48) Cat - 37 (24-45) Horse - 42 (32-55) Sheep - 38 (24-50) Dog - 45 (37-55) Goat - 35 (24-48)
-
15
Exercise No. 5: Determination of Packed Cell Volume (PCV) or Haematocrit value.
Cattle Buffalo PCV in % as determined by
(i) Wintrobe Method ----- -----
(ii) Micro-capillary Method ----- -----
Date: (Instructor)
-
16
EXERCISE NO. 6: ESTIMINATION OF HAEMOGLOBIN
The haemoglobin can be measured by: 1. Colorimetric procedures. 2. Gasometric methods: i) Oxygen Capacity ii) Carbon Monoxide Capacity 3. Physical measurement: i) Sp. Gr. of blood ii) Haematocrit readings iii) Refractive Index. 4. Chemical Methods: i) Iron concentration. 1. Colorimetric Procedures: Either by visual means or by photometric methods, haemoglobin is measured by: 1) Direct method: Tallquist Method 2) Indirect methods: Oxyhemoglobin method or first convert the haemoglobin to a) Acid hematin b) Alkali-hematin c) Cynamethemoglobin d) Cyanohaematin e) Pyridine-hemochromogen 1. Tallquist Method: Tallquist in 1900 designed a series of lithographed colours
supposedly representing haemoglobin values in grades of 10 to 100%. The non-diluted blood, collected on a piece of absorbent paper, is compared with these. The margin of error is between 20 and 50% making it unsuitable for use.
2. Oxyhaemoglobin Method: In this method, blood is diluted with water and matched by eye with a standard picrocarmine solution or a wedge of glass or variable glass standards.
a. Acid Haematin Method or Sahli's Method (1895) (Clinical Method). 1. Principle: When haemoglobin reacts with N/10 HCl, it forms Acid Haematin which
is brown in colour. 2. Apparatus: Sahli's haemoglobinometer, N/10 HCl, pipette with adapter. 3. Chemical reaction: Haemoglobin + HCl ------------> Globin + Acid haematin
(Brown colour) The maximum colour is attained in 40 minutes and after this the colour begins to fade.
4. Procedure: Take N/10 HCl up to 2 mark into an empty graduated tube. Suck in the blood up to the 20 l mark of the measuring pipette and add it to the graduated tube containing 0.1 N HCl. Thoroughly mix it with blood. Keep it aside undisturbed for 7- 10 minutes. After 9 -10 minutes, about 95% of the final brown colour is attained. The resulting brown fluid is then diluted with distilled water or 0.1 N Hydrochloric Acid until it matches with the brown glass standard. Read the value of haemoglobin from the
-
17
scale by noting the height of the column of the diluted acid haematin. The values are always represented in gm%.
Precautions: 1. Measure the blood accurately up to the mark i.e. 20 l. 2. Wipe off the blood sticking on the outside of the pipette. 3. Air bubbles formation while mixing blood and acid should be avoided. 4. Dilution with water or Acid should be accurate. If the match point is passed, the
whole process must be repeated. 5. The same time interval should be observed on each occasion the instrument is
used. It should be standardized under same conditions. 6. In making comparisons, several rapid readings must be made and the average
of these taken; otherwise the eye will become fatigued and erroneous readings will be accepted.
b. Alkali-Haematin Method: Take 0.05 ml of blood in a tube containing 4 ml of N/10 HCl left at room temperature for 48 minutes and then diluted to 5 ml with 1N NaOH.
OR Dilute 0.05 ml of blood to 6 ml with N/10 NaOH. Heat in a boiling water bath for 4 to 5 minutes, cool and read against the standard.
Advantage: 1. The addition of excess of alkali produces a true solution of haematin and much better
solution of plasma proteins and fat where as the acid haematin method is affected by even non-haemoglobin substances (Protein and lipid) in both plasma and cell stroma. Moreover acid haematin is in colloidal suspension rather than a trace solution and makes it unsatisfactory for photometry.
2. With alkali haematin, even carboxyhemoglobin, methemoglobin and sulfhemoglobin forming 2-12% of the total haemoglobin are also converted to haematin, which is not possible with acid.
Disadvantage: With alkali-haematin method, the blood of the new born and young infants carrying small amount of foetal haemoglobin is alkali resistant.
-
18
c. Cynamethemoglobin Method: Ferricyanide converts haemoglobin iron from the ferrous to the ferric state to form methemoglobin which then combines with Potassium Cyanide to produce the stable pigment cyanmethemaglobin. Composition of Drabkin's diluent: NaHCO3 = 1.0 gm,
Potassium ferricyanide = 200 mg, Potassium cyanide = 50 mg,
Distilled water = 1000 ml (Turbid fluid should be discarded) Keep the solution in a brown bottle in cool place. Procedure: Measure 0.02 ml of blood and dilute it with 5 ml of Drabkin's diluent. The optical density of this solution is then compared with that of standard. The colour intensity is measured in a photometer set at 540 nm band.
d. Cynahematin Method: This method has a high degree of accuracy. Take 0.02 ml of blood. Add 1.98 ml of N/10 HCl and leave it for 10 minutes for complete transformation of acid haematin. Then add 2 ml of 2% sodium cyanide and mix. Standard Solution: Weigh 28.8 mg of pure crystalline haemin (8.57% Iron). Transfer it to 1 litre volumetric flask. To this, add 200 ml of 5% sodium cyanide. Add distilled water to make the volume up to the neck of the flask. Keep it at room temperature till the haemin is dissolved. Then make the volume 1 litre with distilled water & mix. The colour intensity is then measured in colorimeter or photometer between 530 and 550 nm.
e. Pyridine-Haemochromogen Method: All haeme pigments are converted into pyridine- hemochromogen and the intensity of absorption of the latter is measured after calibration against crystalline haemin. But the smell of pyridine is unpleasant and the technique is exhaustive. Normal values of Haemoglobin in gm% Cattle - 11 (8-15) Horse - 14.4 (11-19) Sheep - 11.5 (9-15) Goat - 10.0 (8-15) Dog - 15 (12-18) Cat - 12 (8-15)
-
19
Exercise No. 6: Determine the haemoglobin content in gm% for the given sample.
Haemoglobin content in gm% in Name of Method Used Dog Cattle Sheep Buffalo Goat
Date: (Instructor)
-
20
EXERCISE NO 7: ERYTHROCYTE FRAGILITY TEST
Erythrocyte Fragility Test has been devised to measure the resistance of the erythrocytes to break down (haemolyse) when subjected to varying concentrations of hypotonic salt solutions i.e. osmotic fragility test. It was first proposed by Hamburger in 1883. It attempts to quantitate the resistance of these cells to haemolysis in decreasing strengths of hypotonic saline solutions. Requirement: Stock solution of 10% buffered sodium chloride. It is prepared by dissolving 90 gms of sodium chloride, dibasic sodium phosphate (Na2HPO4) 13.655 gms and monobasic sodium phosphate (NaH2PO4 : 2H2O) 2.43 gms and distilled water to 1 Litre. The solution is stored in a glass stoppered tightly closed bottle. Procedure: 1. Make 1% working solution from the stock solution by taking 1 ml of stock solution and
addition of distilled water of 9 ml to make total volume of 10 ml 2. From the working solution, make the test solutions of 0.25%, 0.50%, 0.90%
concentration of Sodium Chloride. The first two being hypotonic and the last isotonic solution.
3. The hypertonic solution is made by dissolving and diluting 2 ml of stock solution to 10 ml with distilled water.
4. Take 5 ml of each of these solutions in labelled test tubes and to each of these add 0.1 ml of blood and examine a drop of each under the microscope under high power.
5. In hypotonic solution, the erythrocytes will be swollen due to absorption of fluid through the membrane and subsequently burst after sometime. The ghost RBC i.e., membrane without pigment is visible. The red blood corpuscles will remain unaffected in isotonic solution while in hypertonic solution the erythrocytes will give shrunken or crenated appearance due to passage of contents through the semi-permeable membrane of erythrocytes.
-
21
Exercise No. 7: Erythrocyte Fragility Test. Observations:-
Date: (Instructor)
-
22
EXPERIMENT NO. 8: BLOOD GROUPING
Landsteiner in 1901 demonstrated that human beings could be classified into 4 groups depending on whether their red cells contain A or B agglutinogen or both AB or neither i.e., O. He also showed that there are antibodies (agglutinins) to A and B agglutinogen named Anti-A and Anti-B and that a person's serum does not contain the antibody for the antigen present in his own red cells but carries antibodies against the agglutinogens he doesnt possess. So the ABO blood group system is as follows: Group Agglutinogen/Antigen Agglutinin/Antibody in Serum A A Anti-B B B Anti-A AB A and B None O None Anti-A
So far, in human beings 14 blood group systems have been identified. Requirement: 1. Blood samples. 2. Anti-Serum for A and B. Procedure: 1. The suspension of RBC is obtained by placing one drop of blood from the finger into
3 ml of normal saline solution. OR 0.5 ml of blood is expelled into a test tube containing about 10 ml of Normal Saline Solution, the tube is gently shaken to wash the cells, the supernatant fluid is poured off after centrifugation and fresh saline is added to make a 1% or 2% suspension.
2. One drop of anti-serum-B is placed on left side of a glass slide and 1 drop of anti-serum-A on the right side. One drop of unknown cell suspension is mixed with each of the antisera followed by tilting of the slide back and forth for 3-5 minutes.
3. Cover the drop with a cover slip and examine under the microscope. On the basis of clumping seen, the samples are classified into various groups as follows : No Clumping - Group-O. Clumping with Antiserum - A - Group - A. Clumping with Antiserum - B - Group - B. Clumping with both Antisera - Group - AB.
-
23
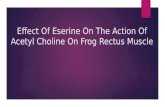
Slide testing method for ABO and Rhesus D:
Blood group O positive: neither anti-A nor anti-B have agglutinated, but anti-Rh has
Result: Blood group B negative: anti-A and anti-Rh have not agglutinated but anti-B has
In the slide testing method shown above, three drops of blood are placed on a cavity glass slide with liquid reagents. Agglutination indicates the presence of blood group antigens in the blood.
ABO blood group antigens present on red blood cells and IgM antibodies present in the serum
Blood Group Systems: - The blood group system in different species is given in the table below:
Species Blood Group Blood Group Technique used for blood Systems Factors typing
1. Human being 14 100+ Agglutination 2. Cattle 12 80+ Haemolytic 3. Sheep 8 30+ Haemolytic Agglutination 4. Horses 8 30+ -do- 5. Pigs 15 65+ Agglutination Haemolytic Antiglobulin 6. Dogs 11 15+ -do- 7. Cats 2 2+ Haemolytic Agglutination 8. Chicken 12 30+ Agglutination
-
24
Exercise No. 8: Determine the Blood Group.
S. No. Name of the student Blood group
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
----------------------------------------------------------- -----------
Date: (Instructor)
-
25
EXERCISE NO. 9: TO DETERMINE TOTAL ERYTHROCYTE COUNT (TEC)
Principle: It consists of an accurate dilution of a measured quantity of blood with a fluid which is Isotonic with the blood and prevents coagulation. Apparatus: 1. A Thoma RBC diluting pipette: It consists of a capillary tube graduated in tenths, which opens into a bulb containing a red coloured glass bead. 2. Diluting Solutions: Any of the following diluting solutions can be used for diluting the blood for TEC. I Hayem's Solution: Sodium Sulphate -2.5 gm Sodium chloride -0.5 gm Mercuric chloride -0.25 gm Distilled water -100 ml II Toisson's Fluid Sodium Chloride -1 gm Sodium Sulphate -8 gm Methyl Violet -0.025 gm Neutral Glycerine -30 ml Distilled water -180 ml Note: The Toisson's fluid has certain disadvantages as: a) The specific gravity is very high so the Red Corpuscles do not settle out in it readily. b) The leukocytes are also stained blue and the counting of White Blood Corpuscles can
also be done but the dilution for red corpuscles is too much to afford for leukocyte enumeration.
c) The fungi grow in it rapidly, therefore it requires frequent filtering III Normal Saline: 0.9% IV Ringer's Solution: Sodium Chloride -0.8 gm Potassium Chloride -0.0075 gm Calcium Chloride -0.01gm Sodium Bi-carbonate -0.01gm DW- -to make 100 ml V Locke's Solution: Sodium Chloride -0.9 gm Potassium Chloride -0.042 gm
-
26
Calcium Chloride -0.024 gm Sodium Bicarbonate -0.02 gm Glucose -0.2 gm DW- -to make 100 ml Hayem's solution is the best but it should not be more than two or three weeks old.
3. Counting Chamber: It is a heavy glass slide in the centre of which are two ruled platforms. These are separated from each other by a central moat and from the elevated bars on each side by transverse moats. These lateral bars are so ground that a cover slip resting on them lies exactly 0.1 mm above the ruled platforms. On each platform is engraved a ruled area 3 mm on each side (9 sq mm). This area is divided into 9 large squares (Primary squares) which are again sub divided, the 8 outside squares being divided into 16 medium small squares (Secondary squares) and the central one into 400 smallest squares (Tertiary squares). Each of the largest squares is 1 mm on the side or 1 sq mm in area. Each of the medium squares is 0.25 mm on side. One smallest square in the central largest square is 0.05 mm on side or 0.0025 mm2 in area. In the improved Neubauer's chamber, the 400 smallest squares in the central square are arranged into 25 groups of 16 squares separated by "split" boundary lines (double line). Method: Draw blood by suction into a Thoma red cell pipette up to 0.5 mark or if anaemic to mark 1. Wipe off the blood sticking on the outer surface of the pipette. In case the blood has slightly passed 0.5 mark, it should be adjusted by touching the tip of the pipette against cloth or cotton. The diluent is then drawn up to 101 mark. While drawing the diluent, the pipette is then rotated between the finger and thumb in order to mix the blood thoroughly with the diluent. Hold the pipette horizontally and mix for half a minute. For uniform mixing, hold the pipette loosely in one hand and rotate the attached rubber tube with thumb and index finger of the other hand. Rotation in one direction should be avoided. Mixing should be repeated each time before expelling a drop for examination. Keep the Neubauers chamber on a smooth surface. The cover glass is then placed on the counting chamber. Several drops of fluid are expelled from the pipette and discarded. This is done to expel the Hayems fluid in the capillary which is not mixed up with the blood. A small drop of mixed fluid is then placed between the cover glass and the ruled platform. The fluid will run under the cover glass by the capillary action. The fluid should completely cover the chamber and none should run over the sides.
-
27
Allow the blood to settle for few minutes and examine for the uniform distribution of the red corpuscles in the chamber under low power. Then place under the high power objective of microscope and count the erythrocytes in the central small squares. The number of cells in the four corner groups of 16 squares and one central one is recorded. Count in L (inverted or upright) form and omitting the cells lying on or outside the opposite line. 3mm
3mm
1mm 1mm 1mm Counting Area in Neubauer's Chamber
Calculations: Total Erythrocyte count = N x 10,000 N = Total count of RBC in 5 squares If the dilution is 1 to 200 (blood drawn to the 0.5 mark), then the total of cells found in the 5 groups of 16 squares is multiplied by 10,000 in order to give the number of cells per cu mm of blood. If the dilution is 1 to 100, then total number of cells is multiplied by 5,000. The length of the side arm of smallest square is =0.05 mm The area of the smallest squares is = 0.0025 sq. mm. i.e. (0.05 x 0.05 = 0.0025) The depth = 0.1 mm Total volume = 0.1 x 0.0025 = 0.00025 cumm Since 80 such squares are counted the area covered is =0.00025x80=0.02 cumm or the number of cells counted per cumm is = 1/0.02 or 50 as the dilution was 1 to 200. The multiplication factor is = 50 x 200 = 10,000
-
28
Precautions: 1. Neubauer chamber should be free from dust or grease 2. Wash the counting chamber with lukewarm water or wipe with alcohol. 3. Wash the pipette three times each with water/alcohol and ether of equal volume 4. After washing dry the pipette. 5. A horse hair (never a wire) should be used in removing blood which has clotted in
the pipette. It is extremely important to avoid making even the slightest crack in the bore of the pipette.
6. Always use pipette, counting and cover glass certified by the US Bureau of Standards. If it is expensive, then one such set in the laboratory can be used as a basis of comparison.
7. In case Hayem's fluid is used and coarse particles are observed which could be produced by a. clumping of red corpuscles due to cold hemagglutinin, can be prevented by warming the Hayems fluid before use.
b. The coarse particles may also be produced by precipitation of globulins by heavy metals in the diluting fluid. c. In cirrhosis of liver and a typical pneumonia, cold hemagglutinin may be formed.
Such pseudo agglutination can be prevented by using Gower's solution i.e.: Sodium Sulphate -12.5 gm Acetic Acid -33.3 gm Distilled water -100 ml
or
By adding 0.01 gm gelatine to100 ml of the Hayem's solution. The red blood corpuscles count in different animals under normal conditions is as follows:
Species RBC Count Species RBC Count (millions/ l) (millions/ l) Cattle 6-8 Buffalo 6-8 Sheep 8-15 (10-13) Goat 13-20 Horse 6-9 - 12.0 Dogs 5.5 - 8.8 Rabbit 4.8 - 8.5 Poultry 1.6 - 1.5 Cat 6-8 Man 5-6 Woman 4 -5 Elephant 2.4 Camel 5.4
-
29
Exercise No. 9: To Determine Total Erythrocyte Count (TEC):
Species Total Erythrocyte Count (Millions/l)
Cattle -------------------------
Buffalo -------------------------
Dog ------------------------
Poultry -------------------------
Date: (Instructor)
-
30
EXERCISE NO. 10: TO DETERMINE TOTAL LEUKOCYTE COUNT (TLC)
Principle: It is carried out on the same principle as the erythrocyte count. The only differences are: 1. The dilution of the blood is less as their number is less. 2. The diluent contains 3% acetic acid which destroys the erythrocyte. The presence of
colouring material gentian violet stains the leukocytes and makes them more visible. 3. The count is made in 4 large (1 mm sq) squares of the Neubauer counting chamber. Apparatus: 1. Neubauer counting chamber 2. Cover slip 3. Thoma WBC diluting pipette containing white bead in the bulb. 4. Turk's fluid: Glacial acetic acid - 3 ml Gentian Violet - 1 ml Distilled water to make the volume 100 ml Method: Draw the blood by sucking into a thoma white cell pipette containing white bead to the mark 0.5. Wipe off the excessive blood sticking to the outer side of the pipette. The blood in excess than the mark 0.5 may be drawn out by applying against the cotton or cloth and draw Turks fluid into diluting pipette upto mark 11. Keep the pipette horizontal on the palm of the hand and mix thoroughly by rotation with the other hand. Mixing with Turk's fluid causes haemolysis of RBC (Acetic acid) and stains WBC (Gentian violet). After mixing for 1 minute expel several drops of fluid from the stem of the pipette containing only the Turks fluid. A small drop of mixed fluid is then placed between cover slip and the ruled chamber. Allow it to settle for some time and examine under 10X power of the microscope in four corner group of sixteen squares. The counting is made in L form or up and down omitting the cells lying on the other lines. This is done to remove the error of recounting.
Calculation: Total Leukocyte count (T.L.C) = X x 50 X = Total number of cells counted in all four squares 50 = Multiplication factor
-
31
Multiplication factor = _____20_____ = 50 1x 1 x 0.1 x 4 where 20 = dilution 1x1 = area of one large square 0.1 = depth between the cover slip and counting chamber 4 = No. of large squares in which counting is done.
Note: 1. Uniform distribution is ascertained only when the variation between the 4 squares
is not more than 8 cells during the normal count. 2. During leukaemia the dilution should be made in erythrocyte pipette and the
correction applied, accordingly.
Normal value of WBC Cattle - 5000 - 12000/l Buffalo- 9000 - 15000/l
-
32
Exercise No. 10: Enumeration of Total Leukocyte Count (TLC).
Results: Species Total Leukocyte Count (Thousands/l)
Cattle --------------
Buffalo --------------
Dog -------------
Poultry -------------
Date: (Instructor)
-
33
EXERCISE NO. 11: PREPARATION OF BLOOD SMEAR FOR DIFFERENTIAL LEUKOCYTE COUNT (DLC)
The blood smear can be made either on cover glass or glass slide. 1. Cover Glass Technique: Though it is difficult but this is preferred to the use of slides because of their thinner preparations and more even distribution of the leukocytes.
The cover glass in the right hand is held just over a freshly drawn drop of blood. It will spread over the glass by capillary action. The drop should be about two to three mm in diameter. Avoid touching of the cover slips to the skin. This cover glass is held in the left hand in the cross wise fashion. The blood will spread quickly and uniformly between the two surfaces. The two cover glasses are separated by drawing apart the cover glasses horizontally in the opposite direction rather than vertically, before the blood spreads completely. If the separation is not done immediately the clotting will take place and it will be difficult to separate. If the preparation is successful, the blood will be spread evenly and the RBC will neither overlap nor Rouleaux. 2. Slide Technique: A drop of blood larger than that used for the cover glass method is placed on the surface of the slide near one end. The slide is then held between two fingers and steadied with the little finger of the left hand. The blood may be spread by means of another glass slide known as spreader which is held in right hand. The spreader is held just to the left of the drop of blood and then it is pulled back to edge of the drop. The blood will spread out behind the spreader which is then pushed to the left. The movement must be quick and steady.
The smear will be thin or thick according to the movement of the spreader i.e. slow or rapid and depending on the angle at which the spreader slide is held. The angle should be about 30 degree. A good smear should be smooth, homogeneous and without serrations, have even edges and should occupy approximately the middle third of the slide. The slide is good for RBC examination, parasites but a differential count is not satisfactory since the polymorphs are pushed to the edges and the lymphocytes remain scattered throughout the smear. Fixation of Smears:
The blood is allowed to dry on the glass in the open air. With most stains, fixation is brought about in the first minute when the undiluted stains which contain alcohol is applied to the smear for 5 minutes. Some stains do not require prefixing as the fixation is done by the stain itself because these contain alcohol e.g. Leishman's stain.
-
34
Stains and Staining of Blood Films: The aniline dyes which commenced in 1877 were first used by Ehrlich for the staining of blood films. Most recently, the modifications of Ramanowasky stain have been commonly used. The stains used are: I. Leishman's Stain: Dissolve 0.15 gms of Leishman's powder in 100 ml of pure acetone free methyl alcohol. Place the Leishman's stain in a clean and dry glass pestle mortar and dissolve in little alcohol. Repeat the process till whole of the powder is dissolved. The stain is then filtered and ready for use or use readymade Leishman's stain. Technique: 1. Place the freshly prepared, air dried film, with its smeared surface upward on a
staining rack. 2. Put on undiluted Leishmans stain for one to two minutes to fix the smears. 3. Add double the quantity of neutral distilled water or buffer water with the help of a
dropper and mix the fluids by sucking and expelling them with the dropper. 4. Let it remain for 10 minutes to stain the slide. 5. Wash and dry in the air after blotting gently with a filter paper. 6. Examine under oil immersion lens. II. GIEMSA STAIN (1902) Composition: Azur II Eosin = 3 gms. Azur II = 0.8 gms. Glycerine chemically pure = 250 ml Dissolve chemically pure Azur II - Eosin and Azur II in pure anhydrous glycerine at 600C. Then methyl alcohol is added and mixture is allowed to stand overnight. It is filtered and kept in stoppered bottle. Rapid Technique: 1. Fix the blood film in Methyl Alcohol for three to five minutes. 2. Dilute the stock solution 1 in 10 with buffer (pH 7.0) 3. Put in the fixed smears in diluted stain for half to one hour 4. Wash with buffer water. 5. Wash, blot dry and examine under oil immersion lens. 6. This method is good for trypanosomes examination. Slow Technique: 1. Dilute the stain 1 in 20 with buffer water. 2. Place the fixed slide in the diluted stain for 16 to 24 hours. Wash, blot, dry and
examine under oil immersion lens. The slow method is used for staining of spirochetes etc. It is good method for differential leukocyte count.
-
35
III. Wright's Stain (1902). Similar to Leishman's stain technique. It is prepared by heating methylene blue with sodium bicarbonate. Then mixture is mixed with Eosin or use ready made solution. Technique: 1. Fresh smear is placed either in racks or on two glass rods placed parallel fixed in
wooden blocks. The width between the two glass rods should be less than the length of the slides.
2. Stain the smear and cover the smear with stain. 3. Keep it for one minute. Fixation is complete during this phase. 4. Dilute the stain with distilled water approximately using the same volume of water as
that of stain. A greenish metallic scum comes up and the margin shows a reddish tinge.
5. Wash the stain after 3 or 4 minute until the film is yellowish or pink and examine under oil immersion lens.
Precautions: 1. The stain should not dry on the slide. 2. Water should not run over the edges of the cover glass or slide. 3. The stain should be floated off the slide by adding water.
Examination of stained blood smears: The stained blood smears are examined for parasites, protozoa, bacteria and Differential Leukocyte Count and many more purposes.
Differential Leukocyte Count (DLC): It is used for the clinical examination. A good slide, better staining is a good index for accurate DLC. The smear should be prepared from a free flowing drop of blood and fixed and stained immediately. Technique: 1. Draw a smear, fix, stain and examine under oil immersion lens. 2. Count different leukocytes and record with the help of mechanical cell counter and
find out the percentage. The four field counting method is the best. In this 50 cells in each field are counted
by moving the field from edge to the centre and back. Repeat the process till 100 cells are counted. Counting is done with the help of blood cell counter which has a separate key for each type of blood cell and the total is attained automatically. After counting 100 cells the counter gives a bell. Thus, the percentage of each cell can be read directly. In case
-
36
the counter is not available then it can be done with the help of Tally counting as given below: Neutrophils IIII IIII IIII IIII IIII IIII III = 33 Lymphocytes IIII IIII IIII IIII IIII IIII = 35 Monocytes IIII IIII IIII IIII = 20 Eosinophils IIII IIII = 10 Basophils II = 2
________
100
Neutrophil Eosinophil Basophil
Granulocytes
Monocyte Large and small lymphocytes
Agranulocytes
-
37
Exercise No. 11: Determine the Differential Leukocyte count (%) in different species of animals.
Species Neutrophil Lymphocyte Monocyte Eosinophil Basophil Cattle
Buffalo
Sheep
Goat
Dog
Poultry
Date: (Instructor)
-
38
EXERCISE NO. 12: THROMBOCYTE (PLATELET) COUNT
A. Collection of blood 1. Venous blood is preferred to capillary blood, and it should be drawn with a plastic
syringe and placed in a siliconized test tube containing 2.5 to 5 mg di-sodium EDTA/2 ml of whole blood to eliminate clumping.
B. Accuracy of Count 1. At best, thrombocyte counts are often unsatisfactory; the thrombocytes have their
own effective characteristics that allow them to avoid being counted, or they are confused with artefacts. Their small size, irregular distribution, rapid disintegration, ready agglutination and adhesion make accurate, reproducible counting difficult.
2. The thickness of the haemocytometer does not allow the oil immersion objective to be used with the direct method, and difficulty is encountered in distinguishing thrombocytes from other particles such as dust and debris.
3. The phase microscope with appropriate equipment provides the best method but is usually not available
C. Indirect method It is the simplest and most practical for the average person 1. A stained blood smear is examined and the number of thrombocytes is noted in
several representative fields and averaged. a. Any of the routine blood stains, including new methylene blue can be used. b. Finding 3 or less thrombocytes per oil immersion field suggests a thrombocytopenia.
In some cases of thrombocytopenia, it is not unusual to find only a few or no thrombocytes on the entire slide.
c. The number of thrombocytes can be compared to the number of leukocytes in the smear, and this relative number may be transposed into an absolute number by the following calculation:
Number of thrombocytes/ microliter = No. of thrombocytes --------------------------X total WBC count/microliter 100 leukocytes
D. Direct method: 1. Blood is drawn into an erythrocyte-diluting pipette to the 0.5 mark and the diluting fluid is drawn to the 101 mark similar to the erythrocyte count. Diluents that may be used include the following: a. Rees-Ecker: Sodium citrate -3.8 g Formaldehyde 40% -0.2 ml
-
39
Brilliant cresyl blue -0.1 g Distilled water -100 ml Keep stoppered and in refrigerator. Filter before use. b. 1% ammonium oxalate: Ammonium oxalate 1H2O -1.1 g Distilled Water -q.s. to100 ml Store in refrigerator to avoid bacterial growth c. 1 or 2% disodium EDTA in 0.85% sodium chloride. A crystal or two of brilliant cresyl blue can be added. 2. Mix thoroughly for 5 min, preferably in a mechanical rotator. 3. Expel and discard the first 4 drops before filling both chambers of the haemocytometer. To prevent evaporation, place the top of a Petri dish containing a wet filter paper or a wet pledget of cotton over the haemocytometer. 4. Allow 15 min for cells to settle. 5. With the illumination partially reduced, count the thrombocytes in the entire central ruled area on each side of the haemocytometer. a. The central ruled area is the one usually used for erythrocytes. b. 2x25 small squares or 50 groups of 16 very small squares are counted for a total of 2 sq. mm. c. Use the fine adjustment to focus on each cell to identify the thrombocytes as lilac coloured, oval, rod or comma shaped, and considerably smaller in size than the leukocytes that are also visible.
Calculation: No. of thrombocytes/ microliter = No. of thrombocytes x 1000
The results obtained should be checked by making a survey of the blood smear to determine if there is good correlation between the two methods.
-
40
Exercise No. 12: Enumeration of Thrombocytes (Platelet count).
Results: Species Thrombocytes/Platelet Count (Lakhs/l)
Cattle -------------------
Buffalo -------------------
Dog -------------------
Poultry -------------------
Date: (Instructor)
-
41
EXERCISE NO. 13: DETERMINATION OF BLOOD PRESSURE.
Blood Pressure It is the lateral pressure exerted by the blood against the wall of the blood vessel. It is a normal terminology, because without blood pressure the circulation of blood would cease. It is the difference in the pressure at the two ends of the vessels which keeps the flow of blood from the arterial to venous blood vessels. The blood pressure is high in the arteries and the flow is high and pulsatile and in vein the pressure is less or almost zero and without any pulsation. Determination of Blood Pressure Direct - Method Procedure: The blood pressure is determined by catheterization of any of the artery i.e. Carotid, Brachial or Femoral. Carotid Artery Catheterization:
1. Secure the animal and tie it properly without any restraint. 2. Clean and shave about 2 sq inches area of the skin over the jugular furrow. 3. Inject I/M, local anaesthesia i.e 2% procaine hydrochloride solution in the area
and isolate the carotid artery. 4. Pass a polyethylene catheter (P.E. 200 I.D; 0.14 cm length 90 cm) filled with
heparinized saline into the carotid artery. 5. Tie the catheter with the thread along with the artery. 6. Connect the catheter with the U shaped mercury manometer through rubber
tubing and a three way cannula. (Three way cannula is used to flush away the coagulated blood in the catheter if it is present). Before making connections between carotid artery and the manometer always keep slightly higher pressure in manometer than the normal systolic pressure of the animal so that the blood may not rush into catheter filled with heparinized saline solution, when the connection is restored, and the blood should stay only up to the tip of the catheter.
7. On restoring the connections between the catheter and the manometer, the mercury column will rise on the opposite column of U shaped mercury manometer having a pointer floating on the mercury.
8. The column of mercury shows upward and downward deflections. 9. Record the deflection by a pointer on a kymograph. 10. Two types of deflections are recorded, one of low amplitude (B.P.) and other of
higher amplitude building up slowly and steadily (Respiration), record to stability.
-
42
11. Disconnect the three way cannula and bring the open end of the catheter at the level of the heart or aorta of the animal. The column of the mercury will fall along the pointer. Mark the line where the pointer is stabilised.
12. Measure the maximum and minimum height from the base line and multiply with 2 to determine the systolic and diastolic pressures. (The height in mm Hg is multiplied by 2 as the mercury column is deflected in double column).
13. Determine the pulse pressure by subtracting the diastolic pressure from the systolic pressure.
14. Determine the mean arterial pressure by adding 1/3 of the pulse pressure to the diastolic pressure.
Indirect Method: Auscultation / Palpation Method: The term auscultation means the detection and study of sounds. The palpation means the feeling of pulse. The blood pressure in indirect method is determined by the use of Sphygmomanometer. Sphygmomanometer Method: The sphygmomanometer consists of a cuff. The cuff encloses a rubber bag wrapped by a cloth. The rubber bag has two attachments, one for the manometer and the other for the bulb which has the arrangement for inlet and outlet of air, regulated by screw knob.
1. Wrap the cuff round the arm above the elbow. 2. Close the outlet on the bulb and make the connections between bulb and
manometer.
3. Inflate the rubber bag in the cuff until it exceeds the arterial systolic pressure (20-30 mm Hg above the normal systolic pressure).
4. Place the stethoscope on the cubital fossa on the elbow joint or feel the radial pulse towards the side of the thumb.
5. Start releasing the pressure by opening the outlet on the bulb and hear the sound or feel the pulse.
6. When there is no flow of blood no sound is heard/no pulse is felt. As the pressure in the cuff falls just below the systolic pressure the flow of blood will produce turbulence and a sound is heard or a pulse will be felt with the index finger. Note the pressure. Because this is the peak pressure during systole of the ventricle so it is called SYSTOLIC PRESSURE, which is greater enough to force the blood under the inflated cuff.
-
43
7. Then allow the pressure in the inflated cuff to fall further. The intensity of the sound increases and finally the sound muffles or disappears. Note the pressure. It is the minimum pressure in the artery during the diastole of the ventricle. So it is called DIASTOLIC PRESSURE.
8. Deflate the cuff more, the murmur finally disappears completely. The sounds disappear because after the cuff pressure is below diastolic pressure the blood flows throughout the cardiac cycle without any turbulence so there is no sound.
Central Venous Pressure (CVP): It is measured with the help of apparatus called CVP Saline manometer set. It carries a three way cannula connected on one side with a scale and on other side with a bottle which carries the normal saline solution. The third end is connected with the help of a catheter to jugular vein of patient. To record the CVP, the scale is kept at the level of heart. The saline manometer is filled with saline expelling air-bubbles from the tubes on all sides. One end is connected to jugular vein of the patient through a catheter or a hypodermic needle. By clamping the tubing from where fluid comes, it is made air tight. The connections are made between the vein and the scale by moving three way cannula and direction is indicated by various arrows. Immediately after connection, there is fall in saline column and wherever it stabilizes, that observation indicates the central venous pressure i.e. CVP. It is expressed in centimetre (cm) saline column.
-
44
Exercise No. 13: To measure the blood pressure by direct and indirect method.
Observations: By Indirect Method
Name of Method used: ----------------------------------------------
S. No. Name of Student B.P (mm of Hg) Systolic/Diastolic
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
-------- ---------------------------------------------------------- ---------------------
Date: (Instructor)
-
45
EXERCISE NO. 14: ELECTROCARDIOGRAPHY
Electrocardiography (E.C.G): The study of electrical activities of the cardiac muscle is termed as Electro-cardiography. The instrument used to record the cardiac potentials (electrocardiogram) is called electrocardiograph. Since the body is a good conductor of electricity, the electric field generated inside the heart spreads over the different parts of the body which can be detected by connecting two suitable points on the body surface in a circuit with the help of a sensitive device called E.C.G. The electrocardiogram is normally recorded by the use of three types of lead systems. 1. Standard Lead System 2. Augmented Lead System 3. Chest Lead System.
I. Standard Lead System or Bipolar Lead System: When two poles of the body are connected, they form a lead. These are standard leads. Lead I, Lead II and Lead III. They are called standard as they were first used for ECG and are used as standard for other tracings of ECG. Lead I = Left arm - Right arm (the negative terminal of ECG is connected to the electrode on the right arm and positive to left arm i.e. when right arm is -ve to the left arm there is +ve or upward deflection). Lead II= Left Leg - Right arm (the negative terminal is connected to right arm and positive to left leg). Lead III= Left Leg - Left arm (the -ve terminal is connected to left arm and the positive terminal to left leg). The fourth electrode is applied to the right leg. This does not enter into the electrocardiographic picture but serves to ground the machine for all leads and thus helps to eliminate alternating current. Three standard leads are bipolar leads because they show the activity of the heart as viewed simultaneously from two different locations or poles i.e. double exposure view. They help in diagnosis of abnormal rhythms as double exposure characteristic exaggerates the amplitude of P waves and makes them more easily recognizable and may be confusing some times as waves in Lead III resemble a cardiac abnormality and yet may result from cardiac position and are normal.
-
46
II. Augmented Lead or Unipolar Lead System: It is used to eliminate double exposure of standard limb lead and obtain a picture of the electrical activity as seen from one extremity only. This is brought about by applying electrode to the desired limb (exploratory electrode applied either to right arm, left arm or the left leg as desired) and completing the circuit through an indifferent electrode whose voltage is approximately zero. The indifferent electrode is prepared by applying three electrodes to the extremities as usual, one to the left arm, the second to the right arm and the third to the left leg. The wires from these three electrodes are then connected to each other and this three tailed electrode is connected to machine as if it were a single electrode. The electrical activities of the heart as seen from these three points simultaneously neutralize each other and the result is a three part indifferent electrode whose voltage is always approximately zero. For obtaining the Unipolar electro-cardiogram as seen from the left arm only, the exploring electrode is applied to the left and indifferent electrode is applied to the left and right arm and to the left leg. Thus left arm tracing equals: Left arm = (Left arm + Right arm + Left leg i.e. ZERO) So the left arm potentials will be equal to left arm -ZERO The leads applied to all the three extremeties are called Unipolar leads or Vector leads. Vector is used to indicate the direction and magnitude of the single force which results when several forces of different magnitudes act simultaneously in different directions on a single point. The unipolar limb leads can be expressed as: VL = L - (L + R + F) VR= R - (L + R + F) VF = F - (L + R + F) Unfortunately, the unipolar limb leads are low in amplitude and difficult to study, so increase or augmenting their amplitude is required. Disconnecting lead from the three tailed indifferent electrode from that extremity to which the exploring electrode is already applied, the amplitude of the complexes will be increased by 50%. Thus aVL=L-(R+F), aVR=R-(L+F), aVF=F-(L+R).
III. Chest Leads: An indifferent electrode is formed by uniting all of the standard electrodes i.e. from left arm, right arm and left leg, through a resistance of 5,000 ohms each to a central terminal and this is connected to the negative terminal of the electrocardiograph. The potential at the central terminal remains at Zero. The positive terminal is connected to the electrode placed on the various areas of the chest. There are six standard positions on
-
47
the chest which are referred as V1, V2, V3, V4, V5 and V6. The placement of these chest leads is: V1= 4th intercostal space to right of sternum V2= 4th intercostal space to left of sternum V3= Mid way between left sternal border and mid clavicular line in a line joining position 2 and 4. V4= 5th intercostal space in mid clavicular line. V5= 5th Intercostal space in left anterior axillary line V6= 5th intercostal space on left mid axillary line. The electrical potentials in the auricle and ventricle appear in the form of deflections called P wave, QRS and T wave. The cardiac potentials are recorded on ECG paper which is ruled horizontally and vertically, and the paper is allowed to move at a speed of 25mm/sec. Before making a record, the machine is to be calibrated.
Evaluation of E.C.G. Tracings: The different waves recorded are - P wave, QRS and T wave. P WAVE: It denotes the electrical activity over the atria i.e. wave of atrial depolarization. It is mostly positive in all the three leads. The potential in standard lead system is 0.2- 0.3 mV and the duration varies between 0.08 - 0.12 sec. Atrial repolarization is absent because ventricular depolarization superimposes it. Atrial repolarization is called atrial T wave. When ventricle is prevented from depolarization and also the gain of amplifier is increased considerably. The T wave will appear as a low voltage with downward deflection.
QRS Complex (Ventricular depolarization): It is the resultant of the left and right bundles, Purkinje fibres and left and right ventricular cardiac muscle electrical activity. Its direction, amplitude and shape depend upon the position of the heart. Q denotes the potential on the ventricular septum. R at the apex and S at the base of the ventricle. The base of the ventricle is the last part to be depolarized. The QRS is normally 1mV and lasts for 0.06 to 0.10 sec.
T Wave: (Ventricular repolarization): The amplitude is normally about 0.3 mV and lasts for 0.16 sec.
PR-Interval: Extends from origin of P wave to origin of QRS complex. As Q wave is mostly absent, the interval is called PR rather than PQ. The time elapsing between the
-
48
activation of the SA node and the activation of AV node (Auriculo - ventricular conduction time) normally measures about 0.16 and not more than 0.20 sec.
Q-T Interval: Extends from origin of QRS to the termination of T wave. It is also known as intraventricular conduction time or electrical systole. It is affected by the beat of the heart. At heart rate of 70 per minute the Q-T interval is about 0.36 sec. and at 120/min, it is 0.28 sec.
S-T Segment: Extends from termination of QRS to the beginning of T Wave. It is also called isoelectric phase and normally it is at the base line level. It gets elevated during the cardiac abnormalities.
S-T Interval: Extends from the termination of QRS to the termination of T wave.
R-R Interval: Extending between two RR of two QRS complexes. It denotes total time taken per beat. To evaluate the heart rate per minute divide 60 by R-R interval (60/R-R interval) where 60 is the factor to convert seconds to minutes.
-
49
Exercise No. 14: Evaluate the ECG tracing recorded.
Date: (Instructor)
-
50
EXERCISE NO. 15: TO RECORD RESPIRATION RATE, HEART RATE AND PULSE RATE IN DOMESTIC ANIMALS
Respiration Rate: Normally, two terms are used i.e. respiration and breathing. The term respiration and breathing are not synonyms. In fact, breathing is a part of respiration. Breathing begins with the movement of chest and the subsequent effect on the movement of air into and out of the lungs. Respiration includes i) movement of air into the lungs (i) oxygenation of pulmonary blood (iii) transportation of oxygenated blood from lungs to tissues (iv) utilization of O2 and production of CO2 at tissue level (v) transportation of CO2 by blood from tissue to lungs (vi) movements of CO2 from lungs into the atmosphere. The respiratory mechanism/respiration rate is divided into two parts. (A) Inspiration and (B) Expiration. The rate and the amplitude of the respiratory movement in the different animals can be recorded by the use of following methods. Physical methods: 1. Paper method: The respiration rate of animals can be recorded by placing a paper
strip close to the nostrils. The paper will move towards the nostrils during inspiration and pushed away during expiration. The pull and push of the paper will constitute one respiration. To record the respiration rate count the number of times the paper is pushed per minute.
2. Abdominal method/Flank method: The respiration rate in the animal is mostly recorded by standing at the back of the animal and making the observations on the rise and fall of the abdominal flank (Differentiate it from the rise and fall of the left abdominal flank at the time of ruminal contraction). The respiration rate of the animal will be the number of times the flank rises per minute.
Precautions: Always stand at the back of the animal and observe the fall and rise of the flank unnoticed by the animal otherwise the animal once disturbed will not give the normal respiration rate as during disturbance the respiration rate gets increased. 3. Auscultation method: The respiration rate is recorded by placing a stethoscope over the chest and recording the respiratory sounds during inspiration and expiration. Experimental Methods: 1. Cannula method: Insert a cannula or catheter into the pleural cavity between two
ribs with the care to prevent the entrance of more than a small bubble of air through the opening. Connect the catheter with a tambour/ manometer fitted with a pointer to write on a kymograph. During inspiration, with the fall in pressure the pointer will
-
51
show downward deflection and during expiration due to increase in pressure in the catheter, the pointer will show upward deflection. Take the upward and downward deflection of the writing pen as one respiration. Count the number of respirations per minute.
2. Tracheal cannula: Insert a tracheal cannula in the tracheal tube and connect it to a tambour with recorder. Inspiration will decrease the pressure in the endotracheal tube, tambour and recorder showing a downward movement of the writing lever, expiration will cause an upward movement of writing point.
3. Pneumograph or Stethograph method: The pneumograph /stethograph is tied around the chest. The pneumograph is connected to a recorder. During inspiration the capacity of the pheumograph is increased and the writing lever move lower and expiration showing upward movement.
The stethograph, a metallic cylinder is closed at both the ends (as compared to pneumograph which a rubber coil is enclosing a rubber tubing open at one end) and has a rubber diaphragm. The string is tied to the centre of each membrane and the apparatus tied around the thorax. A tambour is connected by rubber tubing to a side tube of the stethograph. Inspiration pulls up the rubber diaphragm which creates a negative pressure in stethograph tube and tambour. Expiration produces the opposite effect.
4. Chest Plethysmograph: The plethysmograph is connected to a spirometer. The sheath and inflated rubber bag of the plethysmograph are tied over the thorax of animal. During inspiration the air from the inflated bag goes into the spirometer, whose inner cylinder is raised which has a writing pen. During expiration the inner cylinder again returns to the same level.
5. Body Plethysmograph: It is used for measuring respiration rate and the respiratory volumes.
6. Transducers: Recently electronic device has been employed for recording the respiration rate. The thermister transducer is placed before the nostrils i.e. in the respiratory air stream just below the nasal passage and above the lips. The transducer is held in position by adhesive tape. The transducer is connected to a preamplifier of polyrite physiograph which magnifies pressure changes many times and feed it to the writing pen through a motor. During inspiration the pen gives downward movement and during expiration upward movement.
7. Benodict-Roth respiration apparatus: This apparatus is used for the metabolic studies. The metabolic apparatus also imparts the information about the respiratory frequency of the animal.
-
52
Determination of Heart Rate/Pulse Rate/Cardiac Sounds: Heart rate is the number of times the heart beats per minute. The heart rate can be determined by using either of these methods i.e. by auscultation, by palpation, by E.C.G. or by heart rate meter. Auscultation method: For the record of the heart rate/minute, place a stethoscope on the left side of the chest/thorax on the 4th/5th intercostal space and record the cardiac sounds i.e. lub and dub. The lub and dub forms one heart beat or count the total number of sounds per minute and divide them by two to get heart beat/heart rate per minute. Palpation method: For recording the pulse. In cattle, the record of pulse is made from the coccygeal artery; dogs- femoral artery; man- radial artery. Electrocardiographic technique: The