Posterior Cordectomy. Our Experience
5
Acta Otorrinolaringol Esp. 2012;63(1):26---30 www.elsevier.es/otorrino ORIGINAL ARTICLE Posterior Cordectomy. Our Experience Mikel Landa, ∗ I˜ nigo Luqui, Javier Gómez, Zuri˜ ne Martínez Unidad de Foniatría, Servicio de ORL, Hospital Donostia, San Sebastián, Guipúzcoa, Spain Received 2 March 2011; accepted 30 June 2011 KEYWORDS Bilateral vocal fold paralysis; Laser surgery; Respiratory distress Abstract Objective: Several surgical procedures have been proposed for the treatment of respiratory distress secondary to bilateral cord palsy. We performed a retrospective study of our experience in posterior cordectomy with a laser CO 2 , analysing the improvement of dyspnoea and voice quality after surgery. Methods: This was a retrospective study of 13 cases (9 female, 4 male). The age range was 25---79 years. Iatrogenic post-thyroidectomy (4 cases) was the most common aetiology of bilateral laryngeal palsy in our study. We assessed the subjective improvement of respiratory function and voice quality after laser surgery using the Spanish adaptation of the Voice Handicap Index (VHI). Results: Dyspnoea improved in all patients. Two cases had a worsening of dyspnoea in the immediate postoperative period and one case was successfully solved with a new surgical intervention. After surgery, most of patients suffered from mild or middle dysphonia. Conclusions: The posterior cordectomy is an easy, safe, and effective treatment for dyspnoea secondary to bilateral laryngeal palsy, maintaining acceptable voice quality. © 2011 Elsevier España, S.L. All rights reserved. PALABRAS CLAVE Parálisis cuerda vocal bilateral; Cirugía laser; Insuficiencia respiratoria Cordectomía posterior. Nuestra experiencia Resumen Introducción y objetivos: La paralisis bilateral en adducción de las cuerdas vocales ocasiona una disnea de intensidad variable, que puede ser tratada con diferentes procedimientos quirúrgi- cos. Se realiza una revisión retrospectiva de nuestros casos tratados mediante cordectomía posterior con laser CO 2 , analizando tanto el resultado respiratorio (mejoría de la disnea) como el resultado vocal. Métodos: Se realiza un estudio retrospectivo de 13 casos (9 mujeres y 4 varones) con edades comprendidas entre 25 y 79 a˜ nos. En nuestra serie la causa más frecuente de la parálisis laríngea bilateral es la tiroidectomía (4 casos). Please cite this article as: Landa M, et al. Cordectomía posterior. Nuestra experiencia. Acta Otorrinolaringol Esp. 2012;63:26---30. ∗ Corresponding author. E-mail address: [email protected] (M. Landa). 2173-5735/$ – see front matter © 2011 Elsevier España, S.L. All rights reserved.
-
Upload
mikel-landa -
Category
Documents
-
view
216 -
download
1
Transcript of Posterior Cordectomy. Our Experience

A
O
P
M
U
R
2
cta Otorrinolaringol Esp. 2012;63(1):26---30
www.elsevier.es/otorrino
RIGINAL ARTICLE
osterior Cordectomy. Our Experience�
ikel Landa,∗ Inigo Luqui, Javier Gómez, Zurine Martínez
nidad de Foniatría, Servicio de ORL, Hospital Donostia, San Sebastián, Guipúzcoa, Spain
eceived 2 March 2011; accepted 30 June 2011
KEYWORDSBilateral vocal foldparalysis;Laser surgery;Respiratory distress
AbstractObjective: Several surgical procedures have been proposed for the treatment of respiratorydistress secondary to bilateral cord palsy. We performed a retrospective study of our experiencein posterior cordectomy with a laser CO2, analysing the improvement of dyspnoea and voicequality after surgery.Methods: This was a retrospective study of 13 cases (9 female, 4 male). The age range was 25---79years. Iatrogenic post-thyroidectomy (4 cases) was the most common aetiology of bilaterallaryngeal palsy in our study.
We assessed the subjective improvement of respiratory function and voice quality after lasersurgery using the Spanish adaptation of the Voice Handicap Index (VHI).Results: Dyspnoea improved in all patients. Two cases had a worsening of dyspnoea in theimmediate postoperative period and one case was successfully solved with a new surgicalintervention.
After surgery, most of patients suffered from mild or middle dysphonia.Conclusions: The posterior cordectomy is an easy, safe, and effective treatment for dyspnoeasecondary to bilateral laryngeal palsy, maintaining acceptable voice quality.© 2011 Elsevier España, S.L. All rights reserved.
PALABRAS CLAVEParálisis cuerda vocalbilateral;Cirugía laser;Insuficiencia
Cordectomía posterior. Nuestra experiencia
ResumenIntroducción y objetivos: La paralisis bilateral en adducción de las cuerdas vocales ocasiona unadisnea de intensidad variable, que puede ser tratada con diferentes procedimientos quirúrgi-
respiratoria cos. Se realiza una revisión retrospectiva de nuestros casos tratados mediante cordectomíaposterior con laser CO2, analizando tanto el resultado respiratorio (mejoría de la disnea) comoel resultado vocal.Métodos: Se realiza un estudio retrospectivo de 13 casos (9 mujeres y 4 varones) con edadescomprendidas entre 25 y 79 anos. En nuestra serie la causa más frecuente de la parálisis laríngeabilateral es la tiroidectomía (4 casos).
� Please cite this article as: Landa M, et al. Cordectomía posterior. Nuestra experiencia. Acta Otorrinolaringol Esp. 2012;63:26---30.∗ Corresponding author.
E-mail address: [email protected] (M. Landa).
173-5735/$ – see front matter © 2011 Elsevier España, S.L. All rights reserved.

Posterior Cordectomy. Our Experience 27
Se valora la mejoría de su disnea según la opinión subjetiva de los pacientes y la disfoníagenerada, utilizando la versión espanola del Voice Handicap Index (VHI).Resultados: Todos los pacientes mejoraron significativamente de su disnea. Dos pacientestuvieron que ser ingresados por disnea la primera semana del postoperatorio y uno de ellosfue reintervenido. Tras la intervención la mayoría de los pacientes sufrieron una disfonía leveo moderada.Conclusiones: La cordectomía posterior es un tratamiento fácil y seguro, que proporcionabuenos resultados respiratorios con una disfonía leve o moderada en la mayoría de los casos.© 2011 Elsevier España, S.L. Todos los derechos reservados.
Cu
ptar
R
Ayertc
typcgua(bvt
dc
D
Bcot
itsp
Introduction
Laryngeal paralysis in adduction is an uncommon conditionthat can cause dyspnoea of varying intensity and that canbe treated with different surgical procedures.
Posterior cordectomy is a surgical intervention, firstdescribed by Dennis and Kashima in 1989,1 which is indicatedin dyspnoea by bilateral vocal fold paralysis in adduction.
Recurrent bilateral paralysis represents 25% of all casesof recurrent paralysis2,3 and its most common cause is iatro-genic (especially after thyroidectomy2,4). It is difficult todistinguish from cricoarytenoid joint ankylosis, although itis important to do so because their surgical managementsare different.
Clinically, it is characterised by dyspnoea of varyingintensity, with little or no dysphonia and without dysphagia.
In addition to tracheotomy, the surgical treatment ofthis problem includes several options. Resection techniques(cordectomy and arytenoidectomy) are the most commonlyused, but there are also other alternatives such as ary-tenoidopexy or nerve reinnervation.
Breathing voice is sacrificed in all surgical proceduresexcept reinnervation.
Posterior cordectomy is a simple operation to per-form, almost without complications. Some modifications toimprove the outcome have been described. We believe that,at present, it is the technique of choice because it providesthe best balance between respiratory and phonatory results,without causing aspiration.
Methods
We conducted a retrospective study of 13 patients whounderwent posterior cordectomy due to bilateral vocal foldparalysis in adduction, between June 1998 and January2008. Of these, 9 were female and 4 were male. Theirages ranged between 25 and 79 years. Classifying by aetiol-ogy we found: 4 after thyroidectomy, 1 following traumaticbrain injury, 1 due to multinodular goitre, 2 following com-bined treatment with radiotherapy and chemotherapy dueto laryngeal squamous cell carcinoma, 2 from neurologicaldisease (both with multisystem atrophy), and 3 of unknownaetiology (Table 1).
Clinically, all patients presented dyspnoea on moderate
exertion with nocturnal stridor. Two patients had previouslyundergone surgical procedures for this problem (1 of themon 2 occasions --- cordectomy and arytenoidectomy with cor-dopexy --- and the other, arytenoidopexy).p
ma
We used electrocautery in all cases except for 1, in whichO2 laser was used, due to technical problems. No patientnderwent tracheotomy at the time of the intervention.
We performed prior tracheotomy in only 1 case. Thisatient was scheduled for total thyroidectomy surgery (dueo large multinodular goitre with intrathoracic extension)nd removal of a pituitary adenoma. The tracheotomy wasemoved after 1 month, without any problems.
esults
ll cases presented significant improvement in dyspnoea 1ear after the intervention. Two patients suffered a wors-ning of their dyspnoea in the first 2 weeks after surgery,equiring hospital admission. One of them received drugreatment with good response and the other underwentordectomy.
To assess the degree of dysphonia generated, we usedhe Spanish version of the Voice Handicap Index (VHI) 1ear after the intervention. We excluded the patients whoresented dysphonia before surgery, that is, patients withancer (2), neurological cases (2), patients who had under-one surgery on 2 previous occasions, and patients whonderwent cordectomy. Of the 7 remaining cases, 2 suffered
mild dysphonia (VHI under 30), 4 a moderate dysphoniaVHI between 30 and 60) and 1 a severe dysphonia (VHIetween 60 and 90). All patients were satisfied with theocal outcome, except for the one who underwent cordec-omy (Table 1).
The 2 cancer patients and the 2 neurological patientsied due to their underlying diseases, without requiring tra-heostomy in any case.
iscussion
ilateral paralysis of both vocal folds accounts for 25% ofases of recurrent paralysis.2,3 The most common causef bilateral recurrent paralysis is the iatrogenic, especiallyhyroidectomy.3,4
It may appear as sudden dyspnoea (usually in themmediate postoperative period, perhaps requiring urgentracheostomy) or, even more frequently, as dyspnoea uponmall and moderate efforts. It does not usually cause dys-honia (and when it does appear, it is mild) or deglutitive
roblems.Whenever possible, it is advisable to wait at least 6onths before performing surgery, because there may be
spontaneous recovery of the paralysis.5

28 M. Landa et al.
Table 1 Scheme of Cases Studied and Vocal Result With VHI.
Age Aetiology PriorSurgery
CO2 Laser PriorTracheotomy
PostoperativeDyspnoea
Reintervention VHI
Case 1 79 Thyroidectomy + 78Case 2 47 Thyroidectomy + + 51Case 3 61 Thyroidectomy + + 33Case 4 77 Thyroidectomy + + +Case 5 56 Thyroid goitre + + 7Case 6 23 BT + + + 75Case 7 82 Neurological +Case 8 54 Neurological +Case 9 55 Oncological +Case 10 72 Oncological +Case 11 75 Unknown + 10Case 12 50 Unknown + 54Case 13 76 Unknown 33
c1tntlarehwsa
ice(tpa
tbIrs
1fms
bf
twcv
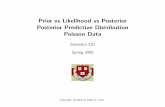
Figure 1 Posterior cordectomy. Immediate postoperativeperiod (the day after the intervention).
BT: brain trauma; VHI: Voice Handicap Index.
The first surgical intervention for this problem was aordoventriculectomy performed by Chevalier Jackson6 in922. In 1941, King proposed an arytenoidopexy with sutureo the omohyoid muscle and Kelly performed an exter-al arytenoidectomy that same year.6 Thornell carried outhe first endoscopic arytenoidectomy (1948), which Ossoffater repeated with CO2 laser in 1983.7 In 1989, Dennisnd Kashima1 published posterior cordectomy, an even moreestricted procedure on the glottis. With the development ofndolaryngeal microsurgery and lasers, external approachesave been practically abandoned (except in children, inhom endoscopic approaches can still be performed8,9;
ome authors have obtained better results with externalpproaches10,11).
The most commonly used techniques are resections,ncluding cordectomy (endoscopic or external), which oftenauses severe dysphonia.5,6 Arytenoidectomy (external orndoscopic) has aspiration as a major complication5,12,13
although some technical variants have been describedhat avoid it) or cricoid necrosis (especially in irradiatedatients).5 Lastly, posterior cordectomy achieves sufficientir passage with moderate vocal sacrifice.1
Possible non-resection surgical procedures include ary-enoidopexy, which can be external or endoscopic (Lichten-erger has designed instrumentation that facilitates it5,6).ts main advantage is that arytenoidopexy is potentiallyeversible, while its main disadvantage is that its resultseem to worsen over time.14
Laryngeal reinnervation was first described by Tucker in976,15 with excellent results16 (he used a myoneural pediclerom the hypoglossal loop to the posterior cricoarytenoiduscle).3 The intervention is technically difficult and has
hown worse results in other series.6
Other procedures such as a laryngeal pacemaker17 orotulinum toxin18 may become important alternatives in theuture.
Posterior cordectomy consists in a transverse incision of
he vocal fold in front of its insertion into the vocal process,hich must completely sever the elastic cone reaching thericoid perichondrium5 (Figs. 1 and 2). Some authors employariants of posterior cordectomy, such as procedures on bothFigure 2 Posterior cordectomy. Final outcome (at 3 monthspostoperatively).

C
Datfatao
C
T
R
1
1
1
12
tratamiento de la inmovilidad laríngea bilateral en adducción.Anales ORL Iber-Amer. 2001;28:341---9.
Posterior Cordectomy. Our Experience
vocal folds12,19,20 or extending the resection to the ventric-ular band or the vocal fold or vocal process.21---23 Although itwas originally described with CO2 laser, it can also be per-formed with KTP laser23---25 or with electrocautery, as in 1case within our series.
Some authors employ a prior tracheotomy,7,13 althoughwe generally do not consider it necessary and have only usedit in 1 case.
This intervention is simple to perform, but its maindrawback is the appearance of dyspnoea in the immediatepostoperative period (15% of our cases). This dyspnoea iscaused by granulomas, oedema, or crusts attached to thesurgical site during scarring.12,25 Nevertheless, it is transientand can be treated medically (with anti-inflammatory drugs,antibiotics, mucolytics, humidifiers, etc.).
It is important to distinguish whether the bilateral immo-bility of the vocal folds is caused by recurrent paralysisor cricoarytenoid ankylosis, although few series make thisdistinction.5,19,26 Cricoarytenoid ankylosis is mainly dueto endotracheal intubation,5,26 followed by autoimmunediseases (Wegener, rheumatoid arthritis27). Cricoarytenoidankylosis can be resolved through other surgical proce-dures such as sectioning scar tissue or adhesions that fixthe arytenoids, intra-articular injection of corticosteroids orothers.6 Laryngeal electromyography can be of great help indifferentiating both conditions, as well as in establishing aprognosis in recurrent paralysis.3,5,6
With respect to respiratory outcomes, almost all stud-ies report satisfactory results, between 95%24 and 100% ofcases (as in our series), although with reoperation ratesranging from 50%21,24,25 to 33% as in the first communicationby Dennis and Kashima1 or 7% as in our series. The param-eters used to measure these results differ from 1 study tothe next. Some, including ours, use the subjective improve-ment of dyspnoea or the degree of patient satisfaction,24
while others use the percentage of decannulations8,21
or pulmonary function tests (flow volume curves,1 bodyplethysmography19,22,23).
We used the Spanish version of the VHI to evaluate thevocal results.28,29 This is a questionnaire with 3 parts (func-tional, physical, and emotional), with 10 questions each,which are answered with a value of 0---4, that is, with amaximum score of 120. A VHI below 30 is considered as amild dysphonia, between 30 and 60 as moderate dysphonia,between 60 and 90 as intense dysphonia, and between 90and 120 as severe dysphonia. Other studies use patients’subjective assessments19,20,24 or resort to other parame-ters (Yanagihara scale based on spectrogram,21 Göttingenscale,19 or Dejonckhere scale26). We obtained good vocalresults in most cases (85% of mild or moderate dysphoniain our series) and all patients reported being satisfied withtheir voice.
Neither our series nor any of those reviewed reporteddeglutitive disorders after the intervention.
Some studies compared the outcome between poste-rior cordectomy and arytenoidectomy,26,30 without findingsignificant differences in either vocal or respiratoryresults. Nevertheless, they have found that arytenoidec-tomy often causes subclinical aspiration whereas pos-terior cordectomy does not.26 No differences in out-
come were found when using either CO2 or KTPlaser.21,24,251
29
onclusions
yspnoea caused by bilateral paralysis of vocal folds indduction is rare, but it represents a delicate problem. Pos-erior cordectomy is a rapid, simple intervention that hasew complications. In most cases, this intervention provides
sufficient increase in glottic space (similar results to otherechniques), with a mild or moderate dysphonia withoutspiration. We believe that, at present, this is the techniquef choice in this pathology.
onflict of Interests
he authors have no conflicts of interest to declare.
eferences
1. Dennis DP, Kashima H. Carbon dioxide laser posterior cordec-tomy for treatment of bilateral vocal cord paralysis. Ann OtolRhinol Laryngol. 1989;98:930---4.
2. León X, Venegas MP, Orus C, Quer M, Maranillo E, Sanudo JR.Inmovilidad glótica: estudio retrospectivo de 229 casos. ActaOtorrinolaringol Esp. 2001;52:486---92.
3. Benninger MS, Michael S, Gillen JB, John B, Altman JS.Changing etiology of vocal fold immobility. Laryngoscope.1998;108:1346---50.
4. Tucker HM. Rehabilitation of the immobile vocal fold. In:Fried MP, editor. The Larynx. A multidisciplinary approach. 2nded. St. Louis: Mosby; 1996. p. 209---18.
5. Eckel HE. Lasers for benign diseases of the larynx, hypopharynxand trachea. In: Huttebrink KB, editor. Lasers in otorhinolaryn-gology. Stuttgart---New York: Thieme; 2005. p. 102---4.
6. Gardner GM. Estenosis glótica posterior e inmovilidad bilateralde las cuerdas vocales. In: Clínicas otorrinolaringológi-cas norteamericanas. Trastornos de la voz y fonocirugía,parte I. Mexico D.F.: McGraw-Hill Interamericana; 2000.p. 793---813.
7. Ossoff RH, Karlan MS, Sisson GA. Endoscopic laser arytenoidec-tomy. Lasers Surg Med. 1983;2:293---9.
8. Friedman EM, de Jong AL, Sulek M. Pediatric bilateral vocal foldimmobility: the role of carbon dioxide laser posterior transversepartial cordectomy. Ann Otol Rhinol Laryngol. 2001;110:723---8.
9. Kutschera J, Friedrich G, Urlersberger B, Eber E, Mueller W.Endoscopic laser posterior cordectomy in a newborn withbilateral vocal fold paralysis and cerebro-oculo-fascio skeletal(Pena-Shokeir II) syndrome. Eur J Pediatr. 2004;163:120---1.
0. Martínez Vidal J, Martínez Moran A, Vázquez Barro JC,Deus Abelenda C. Tratamiento de la parálisis en línea media.In: Ortega del Alamo P, Martínez Vidal J, Suarez Nieto C, edi-tors. Estenosis laringotraqueales. Ponencia oficial de la SEORLy PCF. Badalona: EUROMEDICE. Ediciones Médicas, S.L.; 2005.p. 169---74.
1. Bower CM, Sukgi SC, Cotton RT. Arytenoidectomy in children.Ann Otol Rhinol Laryngol. 1994;103:271---8.
2. Steiner W, Ambrosch P. Laser microsurgery for benign diseasesof the larynx. In: Steiner W, Ambrosch P, editors. Endoscopiclaser surgery of the upper aerodigestive tract. Stuttgart---NewYork: Thieme; 2000. p. 27---9.
3. Izquierdo J, Campos A, Armengot M, Basterra J. La aritenoidec-tomía subtotal y cordectomía posterior con láser CO en el
4. Perouse R, Coulombeau B, Arias C, Casanova C. Aryténö-dopexie selon la technique de Lichtenberger: intérêt dans

3
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
0
les inmobilités laringées bilaterales. Rev Laryngol Otol Rhinol.2006;127:353---6.
5. Tucker HM. Human laryngeal reinnervation. Laryngoscope.1976;86:769---79.
6. Tucker HM. Long term results of nerme-muscle pediclerein-nervation for laryngeal paralysis. Ann Otol Rhinol Laryngol.1989;98:674---6.
7. Zealear DL, Rainey CL, Herzon GD, et al. Electrical pacingof the paralyzed human larynx. Ann Otol Rhinol Laryngol.1996;105:689---93.
8. Cohen SR, Thompson JW. Use of botulinum toxin to lat-eralize true vocal cords: a biomedical method to relievebilateral abductor vocal cord paralysis. Ann Otol Rhinol Laryn-gol. 1987;96:534---41.
9. Olthoff A, Zeiss D, Laskawi R, Kruse E, Steiner W. Lasermicrosurgical bilateral posterior cordectomy for the treatmentof bilateral vocal fold paralysis. Ann Otol Rhinol Laryngol.2005;114:599---604.
0. Khalifa MC. Simultaneous bilateral posterior cordectomy inbilateral vocal fold paralysis. Otolaryngol Head Neck Surg.2005;132:249---50.
1. Bingenzahn W, Hoefler H. Minimally invasive laser surgeryfor the treatment of bilateral fold paralysis. Laryngoscope.
1996;106:791---3.2. Reker U, Rudert H. Modified posterior Dennis and Kashimacordectomy in treatment of bilateral recurrent nerve paralysis.Laryngorhinootologie. 1998;77:213---8.
3
M. Landa et al.
3. Manolopoulos L, Stavroulaki P, Yiotakis J, Segas J,Adamopoulos G. CO2 and KTP-532 laser cordectomy for bilateralvocal fold paralysis. J Laryngol Otol. 1999;113:637---41.
4. Ferri E, García Purrinos FJ. Tratamiento quirúrgico endoscópicocon láser diodo de la parálisis laríngea en adducción. Acta Otor-rinolaringol Esp. 2006;57:270---4.
5. Segas J, Stavroulakis P, Manolopoulos L, Yiotakis J,Adamapoulos G. Management of bilateral vocal fold paralysis:experience at the University of Athens. Otolaryngol Head NeckSurg. 2001;124:68---71.
6. Lawson G, Remacle M, Hamoir M, Jamart J. Posterior cordec-tomy and subtotal arytenoidectomy for the treatment ofbilateral vocal fold immobility: functional results. J Voice.1996;10:314---9.
7. Landa M, Rodríguez L, Rivas A, Abrego M, Zulueta A,Arteche D, et al. Obstrucción respiratoria aguda porartritis reumatoide laríngea. Acta Otorrinolaringol Esp.1994;45:379---81.
8. Jacobson BH, Johnson A, Grywalsky C, Silbergleit A, Jacobson G,Benningger MS, et al. The voice handicap index (VHI): develop-ment and validation. Am J Speech Lang Pathol. 1997;6:66---70.
9. Nunez Batalla F. Validación de la versión traducida al espanoldel Índice de Incapacidad Vocal (Voice Handicap Index). Acta
Otorrinolaringol Esp. 2007;58:385.0. Eckel HE, Vossing M. Endolaryngeal surgical procedures in glottisexpansion in bilateral recurrent nerve paralysis. Laryngorhi-nootologie. 1996;75:215---22.