Post Natal Health: How to best care for our patients after ...
47
Post Natal Health: How to best care for our patients after childbirth 56 th Annual Northern Michigan Update June 25, 2021 Anita K Hernandez, MD Clinical Assistant Professor of Family Medicine Family Mother Baby Service Director
Transcript of Post Natal Health: How to best care for our patients after ...

Post Natal Health: How to best care for our patients after childbirth
56th Annual Northern Michigan UpdateJune 25, 2021
Anita K Hernandez, MDClinical Assistant Professor of Family Medicine
Family Mother Baby Service Director

Disclosures
• None
Family Medicine

• The postpartum period and the Fourth Trimester– Defined
• Mental Health• Blood Pressure• Lactation and Breastfeeding issues• Follow up of Gestational Diabetes• Pelvic Floor Concerns• Family Planning
Outline
Family Medicine

• 12 weeks postpartum• ?should it be more• As many as 40% of women do not attend a
postpartum visit
The Fourth Trimester
Family Medicine

• Elevated risk of thromboembolism• Post partum hemorrhage can occur up to 12
weeks postpartum• Fever may be endometritis
The Fourth Trimester- attention!
Family Medicine
• The postpartum period and the Fourth Trimester– Defined
• Mental Health• Blood Pressure• Lactation and Breastfeeding issues• Follow up of Gestational Diabetes• Pelvic Floor Concerns• Family Planning
Outline
Family Medicine

• Adjustment– Less time for self– Less sleep– Less exercise– Less outdoor time
• Hormonal roller coaster• Off and on psychiatric
medications– Pregnancy– Lactation
Mental Health
Family Medicine
https://www.architecturaldigest.com/gallery/roller-coaster-designs

• Onset– First month up to first year
Mental Health: Postpartum depression
Family Medicine
“Baby Blues”- just the first two weeks!

• Edinburgh Postnatal Depression Scale
Mental Health
Family Medicine
http://www.fresno.ucsf.edu/pediatrics/downloads/edinburghscale.pdf

• Treated similarly to other depression• Support services• Therapy• Medication
– Most antidepressants are considered safe in lactation, especially SSRIs (monitor baby)
– Always better to treat than not treat• Lab work up: TSH (8% incidence autoimmune
thyroiditis)
Mental Health: Postpartum depression
Family Medicine

• Treat to achieve euthymia for 6-9 months• Consider tapering medication• Consider in context of previous mental health
history.
Mental Health: Postpartum depression
Family Medicine

• Postpartum anxiety• Postpartum psychosis• Exacerbation of previous diagnoses
– ADHD– Bipolar disorder
Mental Health: other disorders
Family Medicine
• Mental health disorders in the other parent– 10% incidence in fathers to one year
postpartum– 3-6 mo after the birth is the highest risk– Increased risk of depression up to age 5 of
the child• Intimate Partner Violence• Adoptive Parents
Mental Health: the family
Family Medicine
• The postpartum period and the Fourth Trimester– Defined
• Mental Health• Blood Pressure• Lactation and Breastfeeding issues• Follow up of Gestational Diabetes• Pelvic Floor Concerns• Family Planning
Outline
Family Medicine

• Gestational Hypertension • Chronic hypertension with or without severe
features • Preeclampsia with or without severe features
Blood Pressure
Family Medicine
Risk factor for future cardiovascular disease, stroke, and thrombotic disease
• No evidence based guidelines for treatment postpartum
• May follow up on medications– Beta blockers (labetalol), CCB (Nifedipine)
• Continue medication if needed. • Wean medication if BP normal• Watch for chronic hypertension• If future fertility desired, avoid switching to ace –
inhibitor, ARB, mineralocorticoid antagonists, nitroprusside
Blood Pressure
Family Medicine

• Follow up in postpartum period– Annual follow-up
• Blood pressure• Discussion of lifestyle changes• Body weight monitoring
Blood pressure
Family Medicine

• The postpartum period and the Fourth Trimester– Defined
• Mental Health• Blood Pressure• Lactation and Breastfeeding issues• Gestational Diabetes• Pelvic Floor Concerns• Family Planning
Outline
Family Medicine

• 80% initiate breastfeeding or chestfeeding• Recommended for 12-24 months• Reasons for stopping (top 3)
– Insufficient milk supply – Inadequate latch– Painful nipples or breasts*
Lactation and Breastfeeding Issues
Family Medicine

• Utilize your friendly neighborhood lactation consultant (www.ilca.org)
• Social media support groups• La leche league (www.llli.org) • Doulas
Lactation and Breastfeeding issues
Family Medicine
• 22 yo G1P1 presents to your office 5 months postpartum for breast mass. She has recently returned to work and is experiencing a tender mass in her right breast. Exam reveals a tender nodule in the upper outer quadrant. She is otherwise feeling well. Which is most likely?
• A) breast cancer• B) mastitis• C) blocked milk duct• D) sebaceous cyst
Lactation and breastfeeding issues
Family Medicine

• 22 yo G1P1 presents to your office 5 months postpartum for breast mass. She has recently returned to work and is experiencing a tender mass in her right breast. Exam reveals a tender nodule in the upper outer quadrant. She is otherwise feeling well. Which is most likely?
• A) breast cancer• B) mastitis• C) blocked milk duct• D) sebaceous cyst
Lactation and breastfeeding issues
Family Medicine
• Generally a tender nodule, may shrink when pressed on and milk is expressed
• No other symptoms• May recur• Can develop into mastitis• Pumping is a risk
Lactation and breastfeeding issues: blocked milk duct
Family Medicine

• Treatment:– Massage during feedings– Use electric toothbrush or massager– Warm compress x 20 min– NSAIDS– Avoid constricting clothing– Check breast pump flange size– Lactation consult
Lactation and breastfeeding issues: blocked milk duct
Family Medicine

• 22 yo G1P1 presents to your office 5 months postpartum for breast mass. She has recently returned to work and is experiencing a tender mass in her right breast. She notes she feels achy and very fatigued. Exam reveals temperature of 101F and a tender nodule in the upper outer quadrant with small amount of erythema. Which is most likely?
• A) breast cancer• B) mastitis• C) blocked milk duct• D) sebaceous cyst
Lactation and breastfeeding issues
Family Medicine

• 22 yo G1P1 presents to your office 5 months postpartum for breast mass. She has recently returned to work and is experiencing a tender mass in her right breast. She notes she feels achy and very fatigued. Exam reveals temperature of 101F and a tender nodule in the upper outer quadrant with small amount of erythema. Which is most likely?
• A) breast cancer• B) mastitis• C) blocked milk duct• D) sebaceous cyst
Lactation and breastfeeding issues
Family Medicine
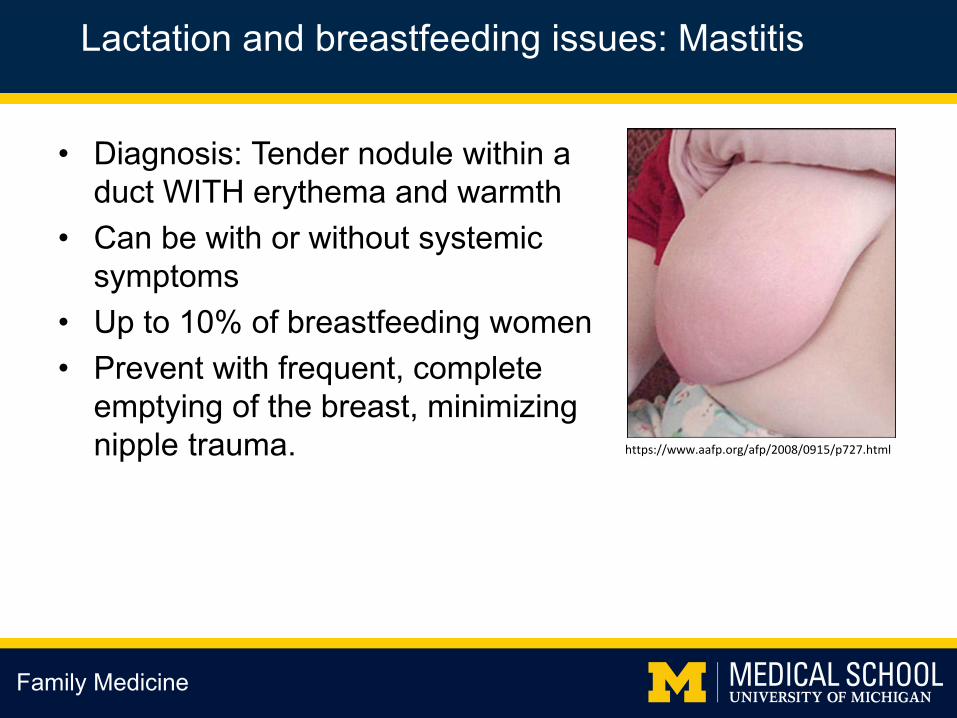
• Diagnosis: Tender nodule within a duct WITH erythema and warmth
• Can be with or without systemic symptoms
• Up to 10% of breastfeeding women• Prevent with frequent, complete
emptying of the breast, minimizing nipple trauma.
Lactation and breastfeeding issues: Mastitis
Family Medicine
https://www.aafp.org/afp/2008/0915/p727.html

• Without systemic symptoms-– Treat for up to 24 hours with supportive care
measures as per blocked milk duct• Warm compresses, cold compresses,
NSAIDS, rest, hydration• With systemic symptoms or no change within 24-
48 hrs– Antibiotics: dicloxacillin or cephalexin x 5-7
days• No improvement
– Consider breast milk culture– Consider US to r/o breast abscess
Lactation and breastfeeding issues: Mastitis
Family Medicine

• The postpartum period and the Fourth Trimester– Defined
• Mental Health• Blood Pressure• Lactation and Breastfeeding issues• Gestational Diabetes• Pelvic Floor Concerns• Family Planning
Outline
Family Medicine
• Diagnosed in pregnancy through a 1 hour screening glucose tolerance test followed by a 3 hour glucose tolerance test
• Diagnosis around 24-28 weeks• Different from any preexisting diabetes• If medications needed, generally stopped post
partum
Gestational Diabetes
Family Medicine

• Postpartum follow up– 2 hour 75 g fasting glucose tolerance
test 4-12 weeks postpartum– Screen every 1-3 years for diabetes– Lifestyle changes/annual follow up– 8x increase in lifetime risk of DM
Gestational Diabetes
Family Medicine
https://www.thermofisher.com/order/catalog/product/401009P#/401009P

• The postpartum period and the Fourth Trimester– Defined
• Mental Health• Blood Pressure• Lactation and Breastfeeding issues• Gestational Diabetes• Pelvic Floor Concerns• Family Planning
Outline
Family Medicine

• Urinary Incontinence• Constipation and
hemorrhoids• Prolonged pain or
dyspareunia
Pelvic Floor Concerns
Family Medicine

• Incidence: >1/4 women in first year• History: stress incontinence• Physical: pelvic exam, look for prolapse • Tests: urinalysis, consider post void residual
Pelvic Floor Concerns: Urinary Incontinence
Family Medicine

• Treatment: – Bladder training– Weight loss– Pelvic floor physical therapy/pelvic floor
muscle therapy• Improves symptoms at one year, no
evidence for long term benefit– Home exercises– Refer to urologic gynecology for refractory
symptoms
Pelvic Floor Concerns: Urinary Incontinence
Family Medicine

• Constipation: Up to 17% of women up to one year postpartum
• Symptomatic hemorrhoids: 1/3 of women• Evaluate for use of constipating medications
– Iron and pain medication
Pelvic floor concerns: Constipation and hemorrhoids
Family Medicine

• Treatment is similar• Stool softeners for hemorrhoids• Avoid prolonged straining• Utilize fiber, water, osmotic laxatives• Stool incontinence requires further evaluation
– Patients with h/o obstetrical anal sphincter injury (OASIS) should have specialist referral.
Pelvic Floor Concerns: Constipation and hemorrhoids
Family Medicine

• Low libido may contribute– Up to a year for return of normal estrogen
levels– Longer if breastfeeding– Generally average libido lower than prior to
pregnancy• Most patients report some sexual concern
postpartum
Pelvic Floor Concerns: Pain and dyspareunia
Family Medicine
• Vaginal dryness: first line lubricants, consider topical estrogen – Caution with breastfeeding.
• Rate of dyspareunia NOT affected by mode of delivery.
• Treatment: multimodal– Counseling, sex therapy, lifestyle changes,
assessing pelvic floor function, supplements/medications
Pelvic Floor Concerns: Pain and dyspareunia
Family Medicine

• The postpartum period and the Fourth Trimester– Defined
• Mental Health• Blood Pressure• Lactation and Breastfeeding issues• Gestational Diabetes• Pelvic Floor Concerns• Family Planning
Outline
Family Medicine

• Assess method of family planning.• Motivational interviewing helpful
– Decrease in rapid repeat pregnancy– Increased use of LARCs
• Patients struggle to follow through with plan-important to ask
Family Planning
Family Medicine
Earliest ovulation: 25
days post partum!

• Lactational amenorrhea method– 2% failure rate if used appropriately– Exclusively breastfeeding– Up to 6 months postpartum– No period since birth– Less reliable once infant is eating solid food.
Family Planning
Family Medicine

• Intrauterine devices (IUD)– Post-placental
• Expulsion risk– 6+ weeks
• Estrogen containing contraceptives- no sooner than 21 days post partum, ideally >6 weeks– VTE risk– ?breastfeeding implications– WHO vs CDC
Family Planning: some key points
Family Planning
• Progestin methods– Implant: no apparent negative effect on
breastfeeding• Immediate postpartum placement
– Depot medroxyprogesterone acetate• ?DMPA effect on developing rat brain
– WHO- delay through 6 weeks if breastfeeding
• CDC: weigh risks/benefits, immediate ok– Progestin-only pills:
• No cautions or restrictions of use
Family Planning: some key points
Family Medicine

Summary
Family Medicine
• The postpartum period/ fourth trimester time period is up to one year and beyond
• Pay close attention to mental health of the whole family in the time after childbirth and/or pregnancy loss.
• Women who have had elevated blood pressure and/or gestational diabetes need close attention to lifestyle changes and ongoing screening for the development of diabetes and cardiovascular disease.
• Breastfeeding parents should receive specialized attention for follow up concerns. Be aware of common lactation concerns.
• Sexual dysfunction, low libido, constipation, and urinary incontinence are common in the postpartum period
• Discuss future desire for fertility and help patients and family choose the method that best fits them for family planning. Avoid estrogen containing methods in the immediate post partum period.

Questions?
Family Medicine

• Berens, P. (2021, January 25). Overview of the postpartum period: Normal physiology and routine maternal care. UpToDate. https://www.uptodate.com
• Committee on Obstetric Practice. Committee Opinion No 746: Optimizing Postpartum Care. Obstet Gynecol. 2018:125 (5):e140-e150.
• Fisher, Sheehan and Garfield, C. Opportunities to Detect and Manage Perinatal Depression in Men. Am Fam Physician. 2016 May 15;93(10):824-825.
• Langan, R and Goodbred, A. Identification and Management of Peripartum Depression. Am Fam Physician. 2016 May 15;93(10):852-858.
• Paladine, H, Blenning, C, and Strangas, Y. Postpartum Care: An Approach to the Fourth Trimester. Am Fam Physician. 2019 October 15;100(8):486-491.
• Sonalkar, S and Mody, S. (2020, June 24). Postpartum Contraception: Counseling and methods. UpToDate. https://www.uptodate.com
• Westerfield, K and Koenig, K. Breastfeeding: Common Questions and Answers. Am Fam Physician. 2018 Sep 15;98(6):368-376
References
Family Medicine