Population Health Management (PHM) · 1/29/2014 · PHM is a tricky discussion for healthcare ......
45
Population Health Management (PHM) January 29, 2014 1
Transcript of Population Health Management (PHM) · 1/29/2014 · PHM is a tricky discussion for healthcare ......
Population Health Management (PHM) January 29, 2014
1
1/29/2014 2
• What is PHM?
• What is triggering the need for PHM? Why Now?
• What are 5 steps to a reasonable PHM strategy?
• What’s a Physician’s perspective of PHM?
• Open discussion about PHM
CONFIDENTIAL |
Population Health Management Agenda

What is PHM?
CONFIDENTIAL | 4 1/29/2014
Population Health Management (PHM) is: a cradle to grave view of high-quality, cost-effective lifetime health management, with a focus on prevention.
PHM helps: • Promote health among the healthy. • Provide early identification and interventions to those at risk. • Prioritize resources for the chronically ill, utilize lowest-cost care
settings, prevent emergency room visits, minimize costly procedures.
PHM is a tricky discussion for healthcare executives. Executed successfully, PHM helps shift from high-risk to low-risk treatment and prevention. However, this model isn’t completely rewarded now with fee for service still a significant portion of the healthcare payment mix, but it’s still needed to contain costs.
Population Health Management What is it?

What is triggering the need for PHM? Why Now?

1/29/2014 CONFIDENTIAL | 6
An Aging Population Healthcare Reform
(Accountable Care Act)
• There are 50 Million Medicare Beneficiaries – INCREASING BY OVER 10,000 per day
• 50% of Medicare patients that enter the skilled setting have a major or extreme illness
• Expansion of Managed Care
• Bundled Payments
• Readmission Penalties
• Continued reimbursement cuts to control Federal/State cost
Two key trends are creating a need for Population Health Management:
Population Health Management Why Now?
1/29/2014 CONFIDENTIAL | 7
The Affordable Care Act (ACA) aspires to:
Population Health Management Why Now?
• Restrain the rate of growth of payments to Medicare Advantage plans
• Restrain the rate of growth in unit payments to hospitals and other providers
• Promote value-based payment systems (i.e. Bundled Payments)
• Make major investments to reduce fraud and abuse.
1/29/2014 CONFIDENTIAL | 8
The Affordable Care Act provides CMS the flexibility to implement a wide range of innovations designed to transform the delivery system by paying for value not volume.
Population Health Management Why Now?
These innovations include: • Fostering the growth of ACO’s • Promoting Managed Care • Creating Primary Care Medical Homes • Bundling payments for acute and
post-acute care • Reducing the frequency of readmissions • Reducing hospital acquired infections • Reducing fraudulent activity
1/29/2014 CONFIDENTIAL | 9
Healthcare in this country is at a tipping point, requiring unprecedented changes in how we organize and deliver it.
Population Health Management Why Now?
Examples: • Seniors represent only 13 percent of the U.S.
population yet account for 36% of healthcare total costs, at $1.01 trillion.1
• Diabetes will double in the next 25 years, and
related spend is expected to rise from $45 to $171 billion.”2
• Costs related to Alzheimer’s and other dementias
are projected to increase from $203 billion in 2013 to $1.2 trillion in 2050. 3
As a result, controlling costs sooner vs. later is a top national priority.
1 - Centers for Medicare and Medicaid Services (CMS) and Deloitte, 2011. 2 - American Diabetes Association: http://care.diabetesjournals.org/content/32/12/2225.full 3 - Alzheimer’s Association. http://www.alz.org/alzheimers_disease_facts_and_figures.asp

1/29/2014 CONFIDENTIAL | 10
Population Health Management Why Now?
Adoption Rates: • According to a 2012 study, 58% of healthcare organizations are
shifting towards PHM, versus a silo approach of disease management.
• Nearly half without a PHM strategy planned to launch in 2013
Proponents • Employers use it to address insurance costs with smoking
cessation, weight loss, and dietary programs.
• Insurers use it to encourage people of all risk profiles to stay on top of primary care, annual physicals, and routine screenings.
• Managed care uses it to reward those with quality outcomes for CMS’s focus diagnoses, prevent hospital readmissions, and contain episodic costs when reimbursements are capitated.
• Small communities use it to wisely manage scarce resources

What are 5 steps to a reasonable PHM strategy?
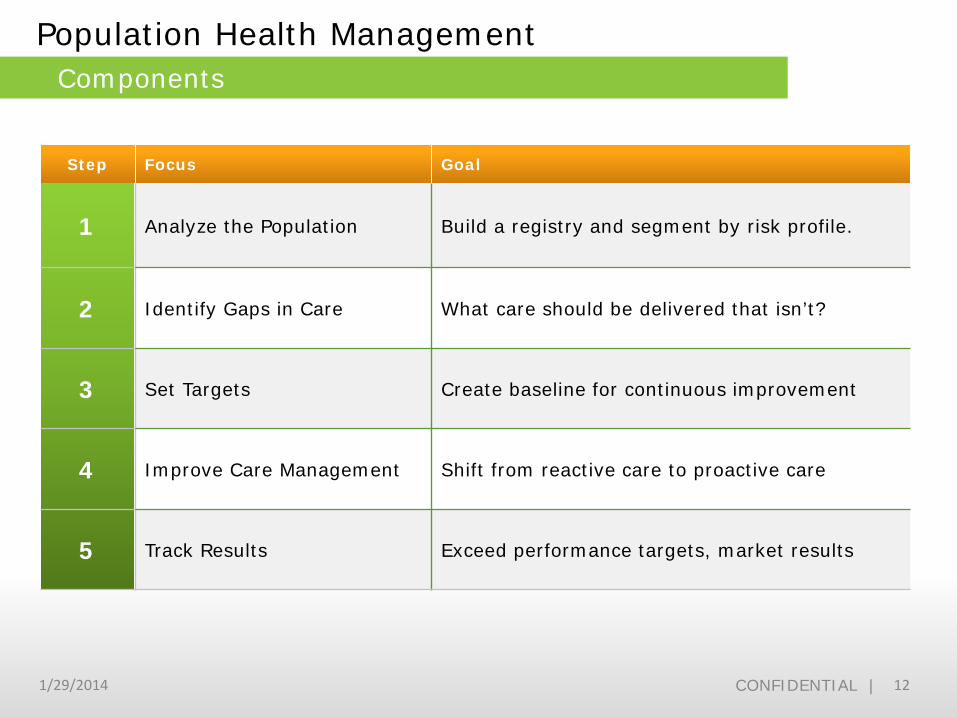
Step Focus Goal
1 Analyze the Population Build a registry and segment by risk profile.
2 Identify Gaps in Care What care should be delivered that isn’t?
3 Set Targets Create baseline for continuous improvement
4 Improve Care Management Shift from reactive care to proactive care
5 Track Results Exceed performance targets, market results
1/29/2014 CONFIDENTIAL | 12
Population Health Management Components
1/29/2014 CONFIDENTIAL | 13
Step 1 Collect Data
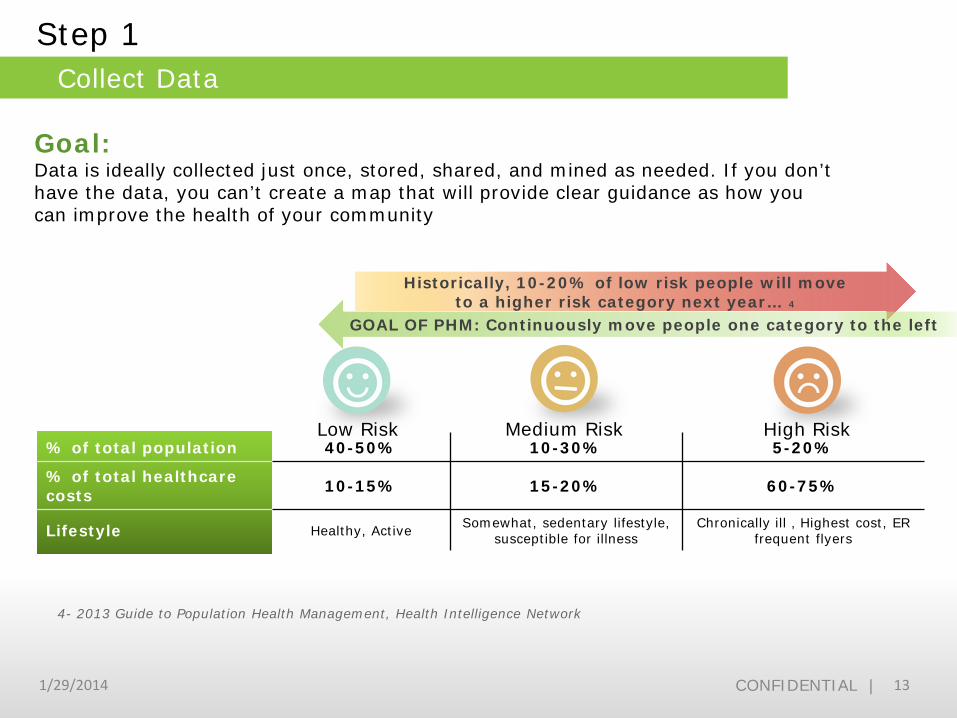
Low Risk Medium Risk High Risk % of total population 40-50% 10-30% 5-20%
% of total healthcare costs 10-15% 15-20% 60-75%
Lifestyle Healthy, Active Somewhat, sedentary lifestyle, susceptible for illness
Chronically ill , Highest cost, ER frequent flyers
Historically, 10-20% of low risk people will move to a higher risk category next year… 4
GOAL OF PHM: Continuously move people one category to the left
4- 2013 Guide to Population Health Management, Health Intelligence Network
Goal: Data is ideally collected just once, stored, shared, and mined as needed. If you don’t have the data, you can’t create a map that will provide clear guidance as how you can improve the health of your community
1/29/2014 CONFIDENTIAL | 14
Step 1 Collect Data
4- 2013 Guide to Population Health Management, Health Intelligence Network
Best practice in small communities: Under the Affordable Care Act, Critical Access Hospitals (as non-profits) are required to conduct a community needs assessment and create an implementation plan every three years. 7 Mitchell County Hospital, for example, identified managing obesity, diabetes, and COPD as top priorities based on the results of their community needs assessment.
Challenge: Data mining. Historical silos of care, regulations, and payment systems have resulted in silos of IT. The availability of cross-continuum registries that can be mined is limited; as a result, asking a data expert for help with data aggregation may prove useful.
1/29/2014 CONFIDENTIAL | 15
Step 2 Identify Gaps in Care
Goal: Based on disease profiles, what care should be delivered that isn’t?
Technology: Predictive analytics, community needs survey results.
Proactive services (e.g., dietary) “Every patient admitted that is recognized as having a dietary problem, whether it’s diabetes, obesity, metabolic problems, kidney failure, renal disease, liver failure, etc.; we identified a need to have our dietician consult with them to come up with a specific diet,” offers Tom Hericks.
Best practices in small communities: The community survey in Faulkton, South Dakota, for example, surfaced needs and key roles for specialized services, prevention, and outreach, to address diabetes, obesity, and cardiac care. Findings included:
Service lines “We identified needs for multiple outreach clinics; and providers (physicians) to come here periodically for 9 or 10 specialties,” according to Tom Hericks, Director of Nursing. “Our goals are to provide services close to home, keep people at home, and out of the hospital.”
Follow up According to Karla Hall, Clinic Manager, “When working with the geriatric population, for example, our big challenges is with health maintenance and preventative care—i.e., getting patients back for appointments, keeping them healthy, and out of the hospital.”
1/29/2014 CONFIDENTIAL | 16
Step 3 Set Targets
Goal: Create baseline for continuous improvement.
Cost
What are the biggest drivers of cost, by disease lifecycle and episodic? How can we address?
Efficiency
What work can be shifted to resources other than physicians?
Quality
• Patient safety • Patient Satisfaction • Patient Outcomes • Barriers to care • Preventative care
(Well Male Exams)
1/29/2014 CONFIDENTIAL | 17
Step 3 Set Targets
Lose a ton “We wanted to help the community lose two thousand pounds of weight collectively, so we launched a ‘fight the fat’ program,” Fenske explained. “We got the community involved with healthy food choices and exercise. When the community achieved that goal, we got media attention including television coverage.”
Candace Fenske, CEO, shared that Madelia Community Hospital has been doing community health assessments for over two decades, long before the government requirement to do so under the Affordable Care Act. Fenkse summarized, “our assessments have recently helped us uncover the barriers to healthy life choices. We learned why do people not eat fruits and vegetables? Why do people continue to use tobacco? Why do people not find the time to exercise, keep their weight down, or maintain a healthy lifestyle?” Collectively these answers or understanding of barriers were very helpful as Madelia Community Hospital established baselines for the following improvements:
Go for grants Fenske explained, We received a State grant to help get children and people more active. We branded it the Madelia Active Living Coalition. From our initiatives, you will see more active people in our community than there were 10 years ago.”
Employer partnerships Under leadership of Ellen Delatorre, Interpreter/Hispanic Outreach Coordinator, launched the “Eliminating Health Disparities” initiative through the Minnesota Department of Health to create greater access to healthcare for Spanish speaking individuals. “When I go into the plants I talk about mostly prevention,” explained Delatorre.
1/29/2014 CONFIDENTIAL | 18
Step 4 Improve Care Management
Goal: Shift from “Reactive” care to “Proactive” care
Low Risk Medium Risk High Risk • Portal access • Wellness programs • On-demand
education • Group counseling
• Care plan follow up • Diagnosis based education • Automatically triggered
diagnosis based reminders
• Health Coaches • Constant Nurse contact
for chronically ill • Coordinated care
1/29/2014 CONFIDENTIAL | 19
Step 4 Improve Care Management
Challenges Physician workflow Physicians will be challenged with shifting from mindset of encounters to one of wellness. Payors will also have to catch up, and shift from 10 minute encounters to 30 minute visits essential for a thorough wellness exam
Consumer reach A RAND Report stated that patients with chronic care only got about 55 percent of all of the things needed to take care of their condition.
Consumer accountability The biggest challenge by far is modifying behavior: getting consumers to follow through with appointments, taking medications, and making healthy lifestyle choices, etc. Consumer incentives are becoming available, from lower premiums to gift cards to cash rewards. To achieve health goals, people must be accountable for their own health care
Best practices in small communities After hours clinics “For continuing chronic-care issues, we have projects through a waiver program that we’re trying to put in clinics after-hours, so that we can help people manage COPD and diabetes,” according to Joe Wright, CFO, Mitchell County Hospital.
Telephonic case management Carolina Behavioral Health Alliance uses telephonic case management in rural areas or when decentralization doesn’t justify face-to-face interactions.
1/29/2014 CONFIDENTIAL | 20
Step 5 Track Results
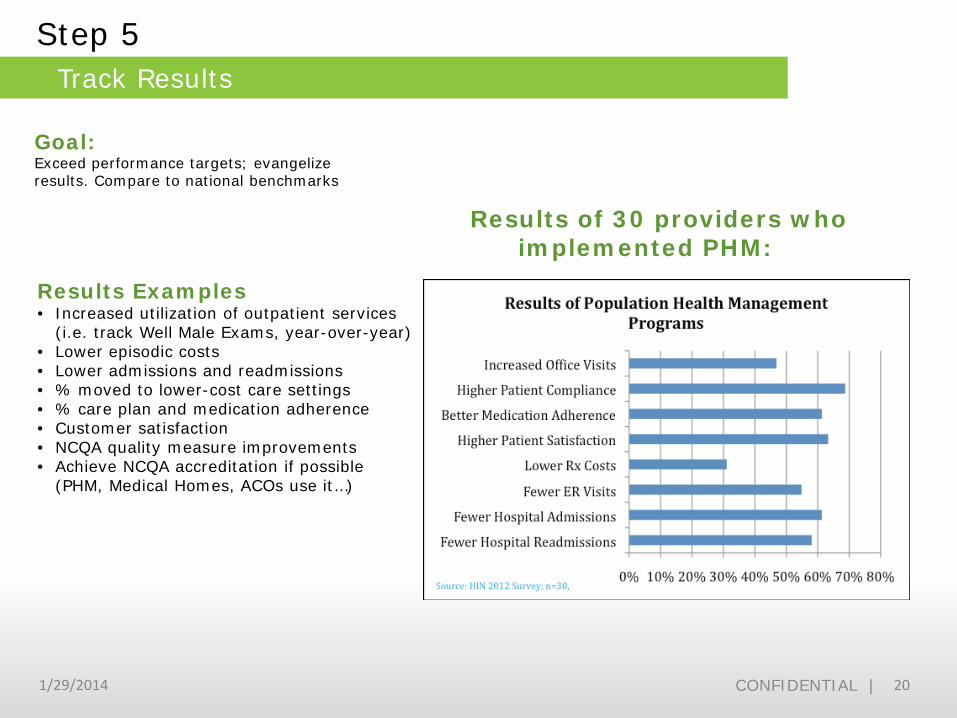
Goal: Exceed performance targets; evangelize results. Compare to national benchmarks
Results Examples • Increased utilization of outpatient services
(i.e. track Well Male Exams, year-over-year) • Lower episodic costs • Lower admissions and readmissions • % moved to lower-cost care settings • % care plan and medication adherence • Customer satisfaction • NCQA quality measure improvements • Achieve NCQA accreditation if possible
(PHM, Medical Homes, ACOs use it…)
Results of 30 providers who implemented PHM:
1/29/2014 CONFIDENTIAL | 21
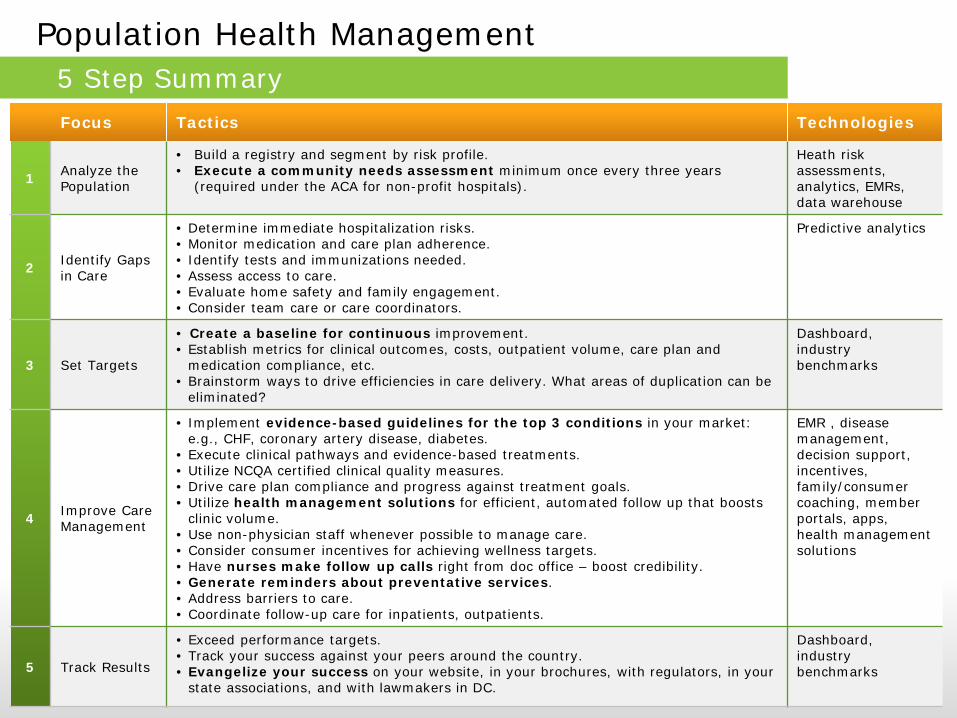
Population Health Management 5 Step Summary Focus Tactics Technologies
1 Analyze the Population
• Build a registry and segment by risk profile. • Execute a community needs assessment minimum once every three years
(required under the ACA for non-profit hospitals).
Heath risk assessments, analytics, EMRs, data warehouse
2 Identify Gaps in Care
• Determine immediate hospitalization risks. • Monitor medication and care plan adherence. • Identify tests and immunizations needed. • Assess access to care. • Evaluate home safety and family engagement. • Consider team care or care coordinators.
Predictive analytics
3 Set Targets
• Create a baseline for continuous improvement. • Establish metrics for clinical outcomes, costs, outpatient volume, care plan and
medication compliance, etc. • Brainstorm ways to drive efficiencies in care delivery. What areas of duplication can be
eliminated?
Dashboard, industry benchmarks
4 Improve Care Management
• Implement evidence-based guidelines for the top 3 conditions in your market: e.g., CHF, coronary artery disease, diabetes.
• Execute clinical pathways and evidence-based treatments. • Utilize NCQA certified clinical quality measures. • Drive care plan compliance and progress against treatment goals. • Utilize health management solutions for efficient, automated follow up that boosts
clinic volume. • Use non-physician staff whenever possible to manage care. • Consider consumer incentives for achieving wellness targets. • Have nurses make follow up calls right from doc office – boost credibility. • Generate reminders about preventative services. • Address barriers to care. • Coordinate follow-up care for inpatients, outpatients.
EMR , disease management, decision support, incentives, family/consumer coaching, member portals, apps, health management solutions
5 Track Results
• Exceed performance targets. • Track your success against your peers around the country. • Evangelize your success on your website, in your brochures, with regulators, in your
state associations, and with lawmakers in DC.
Dashboard, industry benchmarks
The Physician’s perspective… What is it and why do I care? Dr. D Eric Westberg
CONFIDENTIAL | 23 1/29/2014
Population Health Management • The approach to health that looks beyond the
individual and identifies groups that need specific types of care
• A set of interventions aimed across the Health Continuum, from the healthiest to those with catastrophic illness.
Population Health Management Definition – Based on Perspective
CONFIDENTIAL | 24 1/29/2014
Who or what is our Population? Perspective colors definition • Those engaged in public health
look at larger populations by geography and move inward
• Providers prefer a more specific approach: A framework of a clinical delivery system oriented around patients in a practice, in contrast with a public health system oriented around geography - Human Capitol Blog
Population Health Management Who?
CONFIDENTIAL | 25 1/29/2014
• The goal of PHM is to keep people as healthy as possible and prevent their chronic illness from worsening
• There is an intentionality to what goes into managing patients, including stratification, determining out-of-office needs, and organizing into panels of patient’s that meet certain criteria… we are thinking about them in terms of clusters where we have strong evidence-based guidelines for managing these chronic illnesses
Population Health Management Why?

1/29/2014 CONFIDENTIAL | 26
Population Health Management Incentives
Future trends in reimbursement
ACO’s – membership vs association
Quality measures and reporting
Improvement in local care
What will make me a better provider
1/29/2014 CONFIDENTIAL | 27
Population Health Management Disincentives
Fee for service model and lack of reimbursement Work to populate, manage and utilize Staffing
CONFIDENTIAL | 28 1/29/2014
Population • Community
• Facility patient group
• Individual providers patients
• Patients with a specific diagnosis
• Patients with anything else in common you
feel like
Population Health Management Key is defining Population

CONFIDENTIAL | 29 1/29/2014
• Patient registries
• Care managers
• Data analytics
• Patient portal
• Nurse lines
• Integration of Clinical Decision Support
Population Health Management Tools
CONFIDENTIAL | 30 1/29/2014
Complimentary Care settings and techniques • Group visits
• Remote monitoring
• Telemedicine and Telehealth
• Behavior modification and
motivation techniques
Population Health Management Tools

CONFIDENTIAL | 31 1/29/2014
• Corner stone of accountable care
• Another name for a list of patients who meet a certain criteria, usually for a high risk or an important condition
Population Health Management Patient Registries
CONFIDENTIAL | 32 1/29/2014
Quality efforts • Groups that need certain tests performed
Risk reduction • Identify those who are at risk of bad or
expensive things happening
Population Health Management Patient Registries
CONFIDENTIAL | 33 1/29/2014
Common examples • Coumadin Clinic
• Diabetics patients
• CHF patients
Population Health Management Patient Registries
CONFIDENTIAL | 34 1/29/2014
Integrated with Clinical Decision Support • Makes doing the right thing the easy thing to do
• Prompts, reminders, pop-ups etc. Regular reports etc
Population Health Management Patient Registries
CONFIDENTIAL | 35 1/29/2014
• Direct Data Access
• Reports
• Decision Support
• Analytics
Population Health Management Output
CONFIDENTIAL | 36 1/29/2014
How do we know we have a system that is actually making a difference?
Need a system or set of metrics which can be used to determine if the goals of the program are being met
Population Health Management Output
CONFIDENTIAL | 37 1/29/2014
Who?
• Nurses as Full time care managers
• Triage staff
• Clinic nurses
• Others?
Population Health Management Care Managers
CONFIDENTIAL | 38 1/29/2014
• Patient communication
• Patient accountability?
Population Health Management Patient portal

Open PHM Q & A

HIMSS Population Health Task Force
1/29/2014 41 CONFIDENTIAL |
C&BI Task Forces
Population Health Task Force CHAIR: William Beach, PhD, Hodges University This group creates resources and tools to help healthcare organizations use C&BI to execute population health management initiatives to include creating tactical C&BI strategies around data and analytics as well as strategies for organizational planning and patient engagement.
1/29/2014 42 CONFIDENTIAL |
What is Our Problem?
Data • Data: Lack of a sound approach for data analytics and
predictive modeling in population health
• Data – Organizational Change: Lack of structured Change Management in support of translating data into action I population health initiatives.
• Data Flow – General: Lack of understanding of the data flow across the continuum of care creating silos (sharing data across organizations, e.g. as in an ACO; sharing data within organizations).
• Data Flow – Public Health: Fewer than half of local public health departments are receiving and processing data for immunization registries, electronic lab reporting and syndromic surveillance – the three public health requirement under meaningful us of EHRs.
1/29/2014 43 CONFIDENTIAL |
What is Our Problem?
Data (continued)
• Data – Population Health: data needs and timeliness of data for population health.
• Data – Sources: Pharmacy, outside sources, commercial data; how to obtain and integrate data.
Patient-Centered • Patient-Centered/Disease Management – Providers
identifying patients: There is a need to help identify patients who need more help controlling their chronic disease, and to better understand when and where people develop symptoms of their chronic disease.
• Uncover the uses of HIT to define and identify populations and sub-populations of interest, describe the health status and needs of the patient
1/29/2014 44 CONFIDENTIAL |
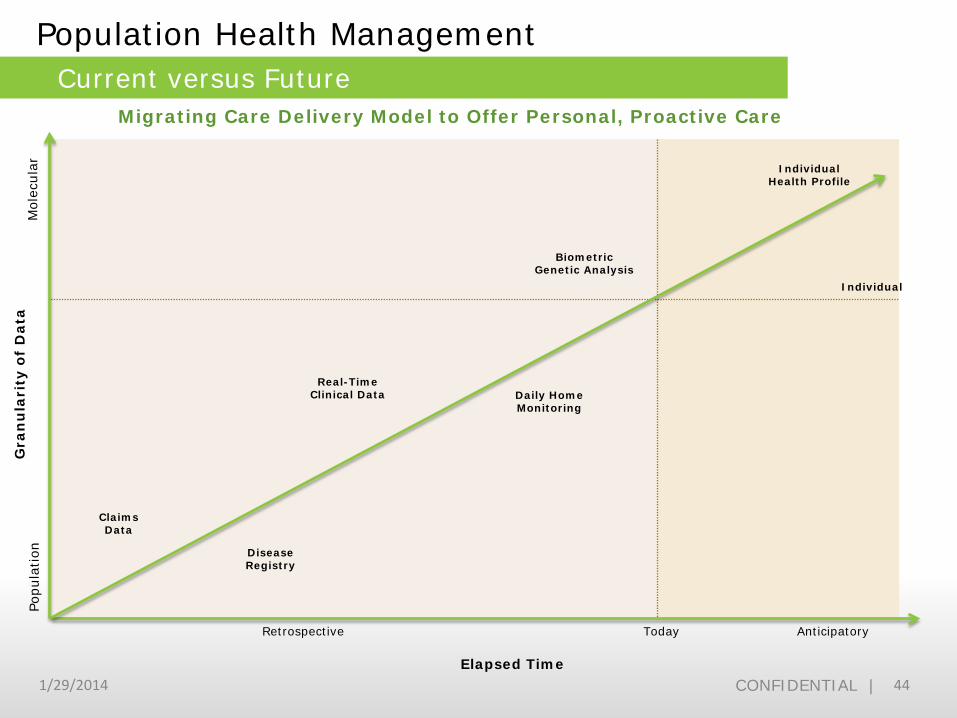
Current versus Future
Retrospective Today Anticipatory
Biometric Genetic Analysis
Population Health Management
Individual Health Profile
Individual
Real-Time Clinical Data
Claims Data
Disease Registry
Daily Home Monitoring
Popu
lation
M
olec
ular
Migrating Care Delivery Model to Offer Personal, Proactive Care
Gra
nu
lari
ty o
f D
ata
Elapsed Time

Questions