Poor prognosis in non-Caucasian patients with early-onset mycosis fungoides
5
Poor prognosis in non-Caucasian patients with early-onset mycosis fungoides Grace Sun, MS, a Cindy Berthelot, MD, a Yafang Li, MS, b Donald A. Glass, II, MD, PhD, c Dornechia George, MD, c Amit Pandya, MD, c Razelle Kurzrock, MD, d and Madeleine Duvic, MD a Houston and Dallas, Texas Background: Mycosis fungoides (MF), the most common cutaneous T-cell lymphoma, is most often seen in middle-aged to elderly men. Objective: We conducted a retrospective study of the demographics and prognosis of patients with onset of MF before age 40 years. Methods: Demographic data (age, sex, and race) and histology from 1074 patents with cutaneous T-cell lymphoma were stratified by age of onset and race and analyzed using Chi-square test. Results: Women presented before age 40 years more often than men (P = .038). Early onset of MF was diagnosed in 30 of 92 (32.6%) African American (AA), 31 of 87 (35.6%) Hispanic, and 103 of 809 (12.7%) Caucasian patients. MF was significantly more common in AA (P = .0008) and Hispanic (P = .0002) patients. Early-onset MF was more common among 21 of 60 AA women (35%, P = .0174) and 19 of 40 Hispanic women (47.5%, P = .0002) than among 50 of 350 Caucasian women (14.5%). Progression from initial TNM stage occurred in only 5 (10%) Caucasian, one (5%) Hispanic, and 8 (38%) AA women who presented before age 40 years. Six of 8 AA women who progressed died of their disease whereas two were long-term survivors after allogeneic transplantation. Limitations: This was a retrospective study at one cancer center. Conclusion: Although MF is considered to be a disease of middle-aged men, early-onset MF is more common among AA and Hispanic women. AA women with early onset may have a poor prognosis and should be considered for more aggressive therapy, including allogeneic transplantation. ( J Am Acad Dermatol 2009;60:231-5.) M ycosis fungoides (MF) is the most common form of cutaneous T-cell lymphoma (CTCL), with an incidence of 6.4 cases per 1,000,000 per year. 1 The median age of MF at presentation is 60 to 69 years, with a 1.9:1 male:fe- male ratio. The clinical course for most patients is best characterized as indolent, with a large cohort analyzed by Weinstock and Horm 2 showing a me- dian survival of 9.7 years. Although it is mostly seen in older adults, MF also occurs in patients younger than 40 years, with similar clinical findings and course. 3,4 The incidence of MF is consistently higher in Caucasian than in African American (AA) popula- tions; however, AA patients with MF have a worse prognosis than other ethnic groups. 5 Considering age, sex, and ethnic group, young AA women are among the least likely to develop MF, although their From the Departments of Dermatology, a Epidemiology, b and Gastrointestinal Oncology, d University of Texas M.D. Anderson Cancer Center, Houston; Department of Dermatology, Univer- sity of Texas, Southwestern at Dallas. c Supported in part by Sherry L. Anderson Cutaneous T-cell Lym- phoma Research Fund, the National Institutes of Health grant K24-CA86815 (Dr Duvic), and M.D. Anderson Core Grant CA16672. Conflicts of interest: None declared. Accepted for publication September 12, 2008. Reprint requests: Madeleine Duvic, MD, Department of Dermatology, University of Texas M.D. Anderson Cancer Center, 1452 Holcombe Blvd, Box 1452, Houston, TX 77030- 4009. E-mail: [email protected]. Published online November 21, 2008. 0190-9622/$36.00 ª 2008 by the American Academy of Dermatology, Inc. doi:10.1016/j.jaad.2008.09.063 Abbreviations used: AA: African American CTCL: cutaneous T-cell lymphoma MF: mycosis fungoides 231
Transcript of Poor prognosis in non-Caucasian patients with early-onset mycosis fungoides

Poor prognosis in non-Caucasian patients withearly-onset mycosis fungoides
Grace Sun, MS,a Cindy Berthelot, MD,a Yafang Li, MS,b Donald A. Glass, II, MD, PhD,c
Dornechia George, MD,c Amit Pandya, MD,c Razelle Kurzrock, MD,d and Madeleine Duvic, MDa
Houston and Dallas, Texas
Background: Mycosis fungoides (MF), the most common cutaneous T-cell lymphoma, is most often seenin middle-aged to elderly men.
Objective: We conducted a retrospective study of the demographics and prognosis of patients with onsetof MF before age 40 years.
Methods: Demographic data (age, sex, and race) and histology from 1074 patents with cutaneous T-celllymphoma were stratified by age of onset and race and analyzed using Chi-square test.
Results: Women presented before age 40 years more often than men (P = .038). Early onset of MF wasdiagnosed in 30 of 92 (32.6%) African American (AA), 31 of 87 (35.6%) Hispanic, and 103 of 809 (12.7%)Caucasian patients. MF was significantly more common in AA (P = .0008) and Hispanic (P = .0002) patients.Early-onset MF was more common among 21 of 60 AA women (35%, P = .0174) and 19 of 40 Hispanicwomen (47.5%, P = .0002) than among 50 of 350 Caucasian women (14.5%). Progression from initial TNMstage occurred in only 5 (10%) Caucasian, one (5%) Hispanic, and 8 (38%) AA women who presentedbefore age 40 years. Six of 8 AA women who progressed died of their disease whereas two were long-termsurvivors after allogeneic transplantation.
Limitations: This was a retrospective study at one cancer center.
Conclusion: Although MF is considered to be a disease of middle-aged men, early-onset MF is morecommon among AA and Hispanic women. AA women with early onset may have a poor prognosis andshould be considered for more aggressive therapy, including allogeneic transplantation. ( J Am AcadDermatol 2009;60:231-5.)
Mycosis fungoides (MF) is the most commonform of cutaneous T-cell lymphoma(CTCL), with an incidence of 6.4 cases
per 1,000,000 per year.1 The median age of MF at
From the Departments of Dermatology,a Epidemiology,b and
Gastrointestinal Oncology,d University of Texas M.D. Anderson
Cancer Center, Houston; Department of Dermatology, Univer-
sity of Texas, Southwestern at Dallas.c
Supported in part by Sherry L. Anderson Cutaneous T-cell Lym-
phoma Research Fund, the National Institutes of Health grant
K24-CA86815 (Dr Duvic), and M.D. Anderson Core Grant CA16672.
Conflicts of interest: None declared.
Accepted for publication September 12, 2008.
Reprint requests: Madeleine Duvic, MD, Department of
Dermatology, University of Texas M.D. Anderson Cancer
Center, 1452 Holcombe Blvd, Box 1452, Houston, TX 77030-
4009. E-mail: [email protected].
Published online November 21, 2008.
0190-9622/$36.00
ª 2008 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2008.09.063
presentation is 60 to 69 years, with a 1.9:1 male:fe-male ratio. The clinical course for most patients isbest characterized as indolent, with a large cohortanalyzed by Weinstock and Horm2 showing a me-dian survival of 9.7 years. Although it is mostly seenin older adults, MF also occurs in patients youngerthan 40 years, with similar clinical findings andcourse.3,4
The incidence of MF is consistently higher inCaucasian than in African American (AA) popula-tions; however, AA patients with MF have a worseprognosis than other ethnic groups.5 Consideringage, sex, and ethnic group, young AA women areamong the least likely to develop MF, although their
Abbreviations used:
AA: African AmericanCTCL: cutaneous T-cell lymphomaMF: mycosis fungoides
231

J AM ACAD DERMATOL
FEBRUARY 2009
232 Sun et al
Table I. Demographics and age of onset of patients with mycosis fungoides
Race Men Men aged \ 40 y Men aged $ 40 y Women Women aged \ 40 y Women aged $ 40 y Total in race subset
Caucasian 459 53 406 350 50 300 809African
American41 9 32 81 21 60 122
Hispanic 59 12 47 59 19 40 118Asian 18 6 12 7 3 4 25All races 577 80 497 497 93 404 1074
cases are likely to be more severe. We report 8 casesof aggressive MF presenting in AA women before theage of 40 years.
METHODSOur CTCL database of 1206 patients seen between
1989 and 2007 was reviewed to stratify patientsaccording to sex, race, age, and disease stage. Theinformation in the database was collected prospec-tively for the purpose of later retrospective dataanalysis. In all, 132 patients, for whom data wereincomplete, were eliminated from the analysis, leav-ing 1074 patients. Caucasian, AA, Hispanic, andAsian groups were analyzed. Because of the smallnumber of Asian patients, only Caucasian, AA, andHispanic groups were stratified according to ageabove and below 40 years and analyzed using theChi-square method to determine whether there weresignificant differences between the groups.Bonferroni correction was used for pairwise com-parisons of multiple stages. The 2-sided t test wasused for comparison of male with female patients.The Cochran-Armitage test was used as a trend testfor analysis of race and stage.
From the database we also identified womenyounger than 40 years who had aggressive oradvanced MF. Aggressive MF was defined as rapidprogression from stable, mild disease to stage IVdisease within 1 year, occurring at any time duringthe course of the illness. Among all women given adiagnosis of MF before age 40 years, there were 8 AAwomen and one Caucasian woman with aggressiveMF.
The clinical course and pertinent diagnostic re-sults of 9 rapidly progressing women were examinedfor age at onset, diagnosis, and overall survival.Progression was defined as an increase in TNM stage.Markers of disease severity included blood involve-ment, large cell transformation, and presence ofextracutaneous disease and T-cell gene rearrange-ments by polymerase chain reaction. Patients werestaged at time of diagnosis or with progression withmedical history, laboratory tests, imaging studies,lymph node biopsy in setting of lymphadenopathy,
and bone-marrow biopsy. Response to therapy wasbased on skin-weighted assessments plus imaging.Complete response was defined as a complete dis-appearance of clinical lesions for at least 1 month;partial response was a disappearance of more than50% of clinical lesions; no response, was a disap-pearance of less than 50% of clinical lesions; andprogressive disease was an increase by more than25% above baseline.
RESULTSAt the time of analysis, our database contained
1074 patients with CTCL who had complete dataavailable for sex, age, and racial stratification. Table Iillustrates the distribution of patients according torace, sex, and age. CTCLs (MF and Sezary syndrome)were more common in men than in women whocomprised 46.3% of patients (2-sided t test, P = .016)as previously reported by others.1
Women (93 of 404, 23.0%) presented before theage of 40 years more often than men (80 of 577,13.9%, P = .0383), as has been previously reported.2
As in Table II, AA (30 of 92, 32.6%) and Hispanic (31of 87, 35.6%) patients were more than twice as likelyto present with MF before the age of 40 yearsthan Caucasian patients (103 of 809, 12.7%; P values.0008 and .0002, respectively). When sex was takeninto account, there were statistically significant
Table II. Chi square comparisons of patients withmycosis fungoides presenting before age 40 yearsby race and sex
Patients with MF before age 40 y
Chi-square
P value
All women [ all men .0383African American [ Caucasian .0008Hispanic [ Caucasian .0002African American women [ Caucasian women .0174Hispanic women [ Caucasian women .0013African American men [ Caucasian men .0911Hispanic men [ Caucasian men .0872
MF, Mycosis fungoides.

J AM ACAD DERMATOL
VOLUME 60, NUMBER 2
Sun et al 233
Table III. Stage at diagnosis and progression in women younger than 40 years
Race Stage IA Stage IB Stage IIA Stage IIB Stage III Stage IVA Stage IVB Progressed Died of disease
Caucasian 64% (32) 16% (8) 4% (2) 6% (3) 2% (1) 6% (3) 2% (1) 10% (5) 6% (3)African American 29% (6) 23% (5) 5% (1) 10% (2) 0 19% (4) 14% (3) 38% (8) 33% (7)Hispanic 42% (8) 37% (7) 0 5% (1) 5% (1) 11% (2) 0 5% (1) 0
Percentages are followed by raw numbers in parentheses (percent of patients of a race/No. of patients).
differences in early age of onset comparingCaucasian with non-Caucasian women. AA (21 of60, 35.0%, P = .0174) and Hispanic (19 of 40, 47.5%,P = .0013) women presented before the age of 40years more often than Caucasian women (50 of 350,14.3%; P values .0174 and .0002, respectively). Thisdifference in age of onset was not observed if wecompared AA (9 of 32, 28.1%, P = .0911) andHispanic (12 of 47, 25.5%, P = .087) men withCaucasian men (53 of 459, 11.5%).
Among women who presented before age 40years, disease progression and stage were signifi-cantly different by race and ethnicity as shown inTable III. When we examined disease progressionamong women with early-onset MF, 5 of 50 (10%)Caucasian, one of 19 (5%) Hispanic, and 8 of 21(38%) AA women had disease progression, as de-fined as an increase in TNM stage at any time in theirdisease course. Disease-specific survival differedamong the groups: 3 of 50 (6%) Caucasian, 0 of 19Hispanic, and 7 of 21 (33%) AA women died fromtheir disease (Table III).
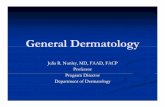
In pairwise comparisons, AA women were morelikely to progress than Caucasian women (oddsratio = 5.54, 95% confidence interval 1.55-19.85,P = .0086) but progression between Caucasian andHispanic women was not significant. Forty of 50(80%) Caucasian women and 15 of 19 (78%) Hispanicwomen with early-onset MF presented as stage IA orIB compared with only 11 of 21 (52%) AA women.Only 4 of 50 (8%) Caucasian women and 2 of 19(11%) Hispanic women were stage IVat presentationcompared with 7 of 21 (33%) AA women (Fig 1). AAwomen were significantly more likely to die of MFthan Caucasian women (odds ratio = 7.83, 95%confidence interval 1.79-34.35, P = .0064). None ofthe Hispanic women died.
Clinical course of 8 AA women with aggressiveMF
Of 8 AA women with early-onset and aggressiveMF, 6 died of disease (Table IV). Five patients wereinitially given the incorrect diagnosis, 3 of eczema. Atthe time of diagnosis and staging, two were stage IB,two were IIB, and 4 were IVB. Median age of onsetwas 27 years (range 19-37) and the median age at
confirmed diagnosis was 33.5 years (range 20-38).The mean time to diagnosis from first onset was 3.576 3.76 years. Mean time from diagnosis to death was7.04 years (SD = 5.99 years) with a median of 5.13years (range 2-18.5 years). One patient lived 18.5years after diagnosis, which was considerably longerthan the other 5 patients, thus the median may bemore representative of survival length than themean.
FourAAwomen developed Sezary syndromeand 6had large cell transformation in their skin. Six hadextracutaneous disease involving bone marrow, liver,or spleen (Table IV). Skin infections most commonlyencountered included recurrent Staphylococcus au-reus, methicillin-resistant Staphylococcus aureus,Enterococcus, coagulase-negative Staphylococcus,and group A beta-hemolytic Streptococcus for whichpatients received appropriate antibiotics. Six womenhad elevated lactate dehydrogenase levels at initialpresentation.
TreatmentAll received standard therapies for MF including
psoralen plus ultraviolet A with either bexarotene or
Fig 1. Plot of the percentages of Caucasian versus AfricanAmerican females (in Table III) by their TNM stage at timeof initial staging.

J AM ACAD DERMATOL
FEBRUARY 2009
234 Sun et al
Table IV. Age and stage at onset, progression, and death of young African American women with aggressivemycosis fungoides
Patient
No.
Age at
onset, y
Age at
diagnosis, y
Time from
symptoms
to diagnosis, y
Stage at
diagnosis
Progression of MF:
SS, LCT, EC sites TCR
Baseline
LDH (IU/L)
Age at
death, y
Time from
diagnosis to
death, y
1 28 30.58 2.83 IVB No, SS, LCT, BM Vb 842 33.75 3.172 25 25.42 5 IVB No SS, BM Vg I, IV 1575 29.08 3.673 19 20.42 1.42 IVA IVB SS, LCT, liver Vg I, II 810 N/A N/A4 31 38.25 7.25 IB IVB, LCT, BM Vb, Vg 828 46.08 7.835 X 34 X IB IVA, LCT Vg 551 52.5 18.56 37.08 37.42 0.33 IIB IVA SS, LCT Vg I, II 496 39.72 2.57 27.67 31.17 2.5 IVA IVB, LCT X 397 N/A N/A8 24 34.25 10.25 IIB IVB X 960 40.83 6.58
BM, Bone marrow; EC, extra cutaneous disease; LCT, large cell transformation; LDH, lactate dehydrogenase; MF, mycosis fungoides; N/A, not
applicable; SS, Sezary syndrome; TCR, T-cell receptor gene rearrangement; Vb, V beta; Vg, V gamma; X, not available.
interferon alfa for stage IB or extracorporal photo-pheresis for patients with blood involvement.Denileukin diftitox, combined chemotherapy withCMED (cytoxan, methotrexate, etoposide, and dex-amethasone),6 or ESHAP (etoposide, Solu-Medrol,high-dose Ara-C, and platinum),7 or single-agentgemcitabine8 were administered to patients whodeveloped nodal or visceral disease. Experimentaltherapy including vorinostat9 or targeted therapieswere given if standard therapies failed.
Of 8 AA women with aggressive MF, only the twowho were treated with total body electron beamradiation followed by allogeneic transplantation re-main alive. One was a 19-year-old AA patient whopresented with exfoliative erythroderma, blood,node, and liver involvement (stage IVB) and whoremains in complete remission 7 years after a relateddonor transplantation. The second surviving AAwoman presented with blood and bone-marrowinvolvement (IVB), and after allogeneic transplanta-tion relapsed with limited skin plaques (T1 N0 M0)controlled with topical Mustargen ointment.
DISCUSSIONThis is a retrospective analysis of a prospectively
collected, large cohort of patients with CTCL evalu-ated at our cancer center between 1989 and 2007 todetermine whether ethnic differences exist in earlyonset or severity of disease. Our data were derivedfrom physician- or self-referred patients with CTCLcompared with broader cancer registry data recentlyreported by Criscione and Weinstock.1 Their surveil-lance, epidemiology, and end results (SEER) andcancer registry survey data found the incidence ofCTCL in the United States between 1973 and 2002increased by 2.9 3 10�6 per decade and was presentin 6.4 per million persons overall. The incidence washigher in men (8.7/million persons) than women(4.6/million) and differences decreased with age.
CTCL was more common in AAs (9.0/million) than inCaucasians (6.1/million) but Hispanics were notevaluated.
Although our data confirmed that men are overallmore likely to have CTCL than women, we noted thatwomen are more likely to present before age 40years (P = .038). AA (P = .008) and Hispanic patientspresent with MF before age 40 years significantlymore often than Caucasians. The difference may beattributed to the higher incidence of AA and Hispanicwomen given a diagnosis before age 40 years.Criscione and Weinstock.1 also noted similar trendswith ethnic differences decreasing with age ofpatients.
There are few articles examining age or sex withrelation to prevalence of MF in AAs or Hispanics.Koch et al10 reviewed patients with onset of symp-toms before age 20 years and suggested that MF maybe underdiagnosed in younger patients. Only 4% to20% of patients with MF had onset of symptomsbefore age 20 years. Most AA patients reported havehypopigmented MF with favorable prognosis.11-13
Female sex appears to be a risk factor, particularlyin AAs. Although only 46% of all patients werefemale, among AAs there were 81 women comparedwith 41 men, a ratio of 1.98:1. Between 1998 and2002 we identified 13 new AA women with MF andonly 5 men with AA in our cohort, in contrast to a1:1.9 female:male ratio reported for all patients withMF. This same relationship held true for AA patientswith symptoms before the age of 40 years (20women and 9 men, respectively).
Among 81 AA women in our cohort, 21 presentedbefore age 40 years and 8 of these progressed fromearly to advanced MF ( $ stage IIB) within 1 year.They had poor prognostic factors: elevated lactatedehydrogenase levels, large cell transformation, andextracutaneous disease.14,15 These patients wererefractory to standard therapies. Six of the 8 died of

J AM ACAD DERMATOL
VOLUME 60, NUMBER 2
Sun et al 235
their disease without allogeneic transplantation. Themedian overall survival from diagnosis to death was5.1 years. The reason why young AA women mayhave more aggressive MF is unknown but is likely tobe multifactorial. Our clinical experience suggeststhat young women with aggressive MF (large celltransformation or Sezary syndrome) should be con-sidered for allogeneic transplantation, and that find-ing a match for AA patients may pose a significantchallenge. In conclusion, generalizations regardingthe incidence, prevalence, and prognosis of MF maynot apply equally across race, sex, and age, and thisinformation should be used for risk stratification andtherapy choice.
REFERENCES
1. Criscione VD, Weinstock MA. Incidence of cutaneous T-cell
lymphoma in the United States, 1973-2002. Arch Dermatol
2007;143:854-9.
2. Weinstock MA, Horm JW. Mycosis fungoides in the United
States: increasing incidence and descriptive epidemiology.
JAMA 1988;260:42-6.
3. Crowley JJ, Nikko A, Varghese A, Hoppe RT, Kim YH. Mycosis
fungoides in young patients: clinical characteristics and out-
come. J Am Acad Dermatol 1998;38:696-701.
4. Quaglino P, Zaccagna A, Verrone A, Dardano F, Bernengo MG.
Mycosis fungoides in patients under 20 years of age: report of
7 cases, review of the literature and study of the clinical
course. Dermatology 1999;199:8-14.
5. Weinstock MA, Gardstein B. Twenty-year trends in the
reported incidence of mycosis fungoides and associated
mortality. Am J Public Health 1999;89:1240-4.
6. Maor MH, Velasquez WS, Fuller LM, Silvermintz KB. Stomach
conservation in stages IE and IIE gastric non-Hodgkin’s lym-
phoma. J Clin Oncol 1990;8:266-71.
7. Velasquez WS, McLaughlin P, Tucker S, Hagemeister FB, Swan
F, Rodriguez MA, et al. ESHAPean effective chemotherapy
regimen in refractory and relapsing lymphoma: a 4-year
follow-up study. J Clin Oncol 1994;12:1169-76.
8. Duvic M. Systemic monotherapy vs combination therapy for
CTCL: rationale and future strategies. Oncology (Huntingt)
2007;21(Suppl):33-40.
9. Duvic M, Vu J. Vorinostat in cutaneous T-cell lymphoma. Drugs
Today (Barc) 2007;43:585-99.
10. Koch SE, Zackheim HS, Williams ML, Fletcher V, LeBoit PE.
Mycosis fungoides beginning in childhood and adolescence.
J Am Acad Dermatol 1987;17:563-70.
11. Stone ML, Styles AR, Cockerell CJ, Pandya AG. Hypopigmented
mycosis fungoides: a report of 7 cases and review of the
literature. Cutis 2001;67:133-8.
12. Akaraphanth R, Douglass MC, Lim HW. Hypopigmented my-
cosis fungoides: treatment and a 6(1/2)-year follow-up of 9
patients. J Am Acad Dermatol 2000;42:33-9.
13. Whitmore SE, Simmons-O’Brien E, Rotter FS. Hypopigmented
mycosis fungoides. Arch Dermatol 1994;130:476-80.
14. Diamandidou E, Colome M, Fayad L, Duvic M, Kurzrock R.
Prognostic factor analysis in mycosis fungoides/Sezary
syndrome. J Am Acad Dermatol 1999;40:914-24.
15. Diamandidou E, Colome-Grimmer M, Fayad L, Duvic M,
Kurzrock R. Transformation of mycosis fungoides/Sezary syn-
drome: clinical characteristics and prognosis. Blood 1998;92:
1150-9.