Policies and Procedures Manual School-Based Sealant ProgramsUniv+Sealant... · 2016-06-17 ·...
31
Policies and Procedures Manual School-Based Sealant Programs Preliminary Information (to be eliminated for final version of manual): The following is a basic list of program policies and procedures that may be used as a template to develop your program’s manual. A final document will be defined in partnership with your School corporation and/or Federally Qualified/Community Health Centers (FQ/CHC). Summary of the School Based Sealant Program The objective of the School-Based Sealant Program is to use your State law definitions that allows dental hygienists to provide school-based dental sealants under the prescriptive supervision of a licensed dentist or without it. (1) Recruit dentists, dental hygienists and dental assistants to work in new school-based dental programs supported by their surrounding FQ/CHCs; (2) Seek for support for the initial operation of the programs and help purchase portable dental equipment to provide services in these clinics; and (3) Locate and Target Title I schools in underserved areas, and develop and establish these new school-based dental sealant programs throughout these communities The participating dentists, hygienists and dental assistants will all be employees of the FQ/CHCs. Each FQ/CHC will work with one or more of the surrounding school corporations. Within each of the participating schools, the licensed dentist will provide examinations and write a prescription (dental chart) for the children consented defining which teeth are to be sealed by the dental hygienist. On a working day there may be two dental assistants, one to support each of the working dental hygienists. The hygienist will fulfill legal requirement by working under prescriptive supervision or not depending on the state regulation.
Transcript of Policies and Procedures Manual School-Based Sealant ProgramsUniv+Sealant... · 2016-06-17 ·...

Policies and Procedures
Manual
School-Based Sealant Programs
Preliminary Information (to be eliminated for final version of manual): The following is a basic list of program policies and procedures that may be used as a template to develop your program’s manual. A final document will be defined in partnership with your School corporation and/or Federally Qualified/Community Health Centers (FQ/CHC). Summary of the School Based Sealant Program The objective of the School-Based Sealant Program is to use your State law definitions that allows dental hygienists to provide school-based dental sealants under the prescriptive supervision of a licensed dentist or without it. (1) Recruit dentists, dental hygienists and dental assistants to work in new school-based dental programs supported by their surrounding FQ/CHCs; (2) Seek for support for the initial operation of the programs and help purchase portable dental equipment to provide services in these clinics; and (3) Locate and Target Title I schools in underserved areas, and develop and establish these new school-based dental sealant programs throughout these communities The participating dentists, hygienists and dental assistants will all be employees of the FQ/CHCs. Each FQ/CHC will work with one or more of the surrounding school corporations. Within each of the participating schools, the licensed dentist will provide examinations and write a prescription (dental chart) for the children consented defining which teeth are to be sealed by the dental hygienist. On a working day there may be two dental assistants, one to support each of the working dental hygienists. The hygienist will fulfill legal requirement by working under prescriptive supervision or not depending on the state regulation.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 2 of 31
Each child will have an informed consent form that will be signed by their parents/legal guardians prior to any screening exam or placement of dental sealants. The appropriate FQ/CHC will maintain the dental charts of the children being treated by the program. The FQ/CHCs will be responsible for all practice management activities for this program. These activities will include billing either: Medicaid, insurance or the child’s parents/legal guardian using a sliding fee scale consistent with the FQ/CHC’s dental clinic. The hygienists working for the program will also be responsible for surveying other schools in the community about their willingness to participate in periodic screenings of their students to determine their oral health status and their need for preventive services such as a dental sealant program.
1. Purpose The purpose of this manual is to provide a guide for program policies, procedures and guidelines to develop a school based sealant program. This document was created in partnership with IUSD, SWG and Health Resources and Services Administration (HRSA) proposal.
2. Scope The scope of this SOP will cover
1. Patient care procedures
2. Clinical procedures
3. Equipment uses and maintenance
4. Program monitoring and evaluation
This SOP will not cover: • Budgeting process • Billing Medicaid or patients
3. Terms and Definitions CHC: Community Health Centers FQHC: Federally Qualified Health Centers HRSA: Health Resources and Services Administration SI: Seal Indiana IUSD: Indiana University School of Dentistry SBSP: School Based Sealant Programs SBPP: School Based Preventive Programs DS: Dental Sealant
4. Elements of Standard Manual for School Based Sealant Programs Although each manual should be unique to its particular school-based sealant program, all manuals will have essentially the same elements. These elements include:

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 3 of 31
• Purpose
• Scope and/or Introduction
• Safety Precautions
• Equipment
• Identification and Scheduling of Sites
• Clinical Set-Up Procedures
• Infection Control Procedures
• Post Visit Procedures
• Follow Up Procedures
• Data Collection and Reporting
• Program Evaluation
• Attachments
• References
5. Safety Precautions
Hand washing -Hands or other skin areas are to be washed with liquid soap (antimicrobial preferred) or
an alcohol-based hand rub (if the hands are not visibly dirty)
Gloving -Powder-free latex, vinyl, nitrile, or other patient-care type gloves are to be worn by all
staff during all intraoral procedures, on all patients, and at all other times when there is a potential for exposure of the hands to body fluids.
Protective eyewear -Protective eyewear with side shields or a curved face shield that also protects the sides
of the eyes is to be worn by all staff during all intraoral procedures on all patients. -Prescription glasses are acceptable as long as side shields are attached and the
glasses are not too small. -Contaminated eyewear is to be washed with an antimicrobial hand washing agent
(using gloved hands), rinsed, and dried before reuse.
Masks
-A mask covering the NOSE AND MOUTH is to be worn by all staff during the
examination and treatment of all patients. A fresh mask is used with each patient and the
used mask discarded in the regular trash.
Protective clothing
-Protective clothing (a disposable gown that has a high neck, long-sleeves, knee-length,
or in some instances a long-sleeved laboratory coat) is to be worn by all staff during the
examination and treatment of all patients and when placing surface covers on units prior
to patient care.
Waste Management
-Dangerous substances or regulated materials should be removed off site and disposed
of properly

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 4 of 31
6. Equipment The following is a list of equipment used for a sealant program
Portable dental sealant units
Portable dental chairs
Portable lights
Portable tray stands
Curing lights
Equipment Maintenance All portable equipment should be cleaned and disinfected before being packed and put away. Each time portable equipment is set up the directions should be read and followed carefully to maintain the best and longest service from your equipment.
Portable dental sealant unit/air compressor:
-Visual checks should be performed regularly to look for mechanical damage that
could affect safe operation or loose or missing items.
Portable dental chair:
-The use of barrier covers and mild cleaning solutions is recommended as the
primary asepsis approach on chair upholstery
-The use of barrier covers extends the life of chair upholstery and can be replaced
between patients
Portable light:
-Make sure correct wattage is available to power lights and
-Make sure appropriate replacement bulbs are available.
Portable tray stand:
-When maintained properly the stand is lightweight and highly portable
Curing lights
-After each use, disinfectant all surfaces.
-Use a barrier sleeve to prevent cross contamination
For additional information please refer to the specific instruction manuals of all equipment.
7. Consenting Process The American Academy of Pediatric Dentistry (AAPD) recognizes that informed consent is essential in the delivery of health care. The informed consent process allows the patient or the custodial parent or, in the case of minors, legal guardian to participate in and retain autonomy over the health care received. Informed consent also may decrease liability from claims associated with miscommunication. These guideline reflect that informed consent is governed by the statutes and case laws of individual states and that oral careproviders should review applicable state law and regulations. (1,2) The following should be included in the informed consent:

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 5 of 31
Name and date of birth of pediatric patient;
Name and relationship to the pediatric patient/legal basis on which the person is
consenting on behalf of the patient;
Description of the procedure in simple terms;
Disclosure of known adverse risk(s) of the proposed treatment specific to that
procedure;
Professionally-recognized or evidence-based alternative treatment(s) to
recommended therapy and risk(s);
Place for custodial parent or legal guardian to indicate that all questions have been asked and adequately answered;
Places for signatures of the custodial parent or legal guardian, dentist, and an office staff member as a witness.In Indiana the parent/legal guardian must give permission for the patient to be treated by signing a legal consent form. (An example is included in Attachement 1. Seal Indiana Consent Form). Produce consenting forms for parents in English, Spanish, Burmese and/or any other languages as needed using certified translators. Create forms for HIPPA compliance. These forms should be in compliance with HIPPA regulations established by the USDH and state law. (3)
To increase number of consented children, it is suggested parents be contacted during special events organized by the schools. Information about the program could be introduced to the parents during parent registration/orientation day or sent home in the child’s school registration packet.
8. Identification and Scheduling of Sites The program will address the dental access needs of children in Dental Health
Professional Shortage areas by expanding the dental workforce available and
increasing its efficiency to provide preventive services to children, in a sustainable
manner.
-The FQHC will establish a partnership with the surrounding school corporations in
designated dental health profession shortage areas, inner city and rural areas.
-Once, these areas are located, the priority population will be low-income children
who attend Title I schools (lowest income schools).
The school-based dental coordinator will be responsible for recruiting these schools
and working with the school nurse and/or health aide to market the programs
services to the low income families that need preventive dental services. .

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 6 of 31
9. Recruitment of Participants
1. Establish procedures for the program coordinator to travel to partner schools and help
the school nurse and/or health aid recruit children who could benefit from the program’s
services.
SBSP can use fliers, e mail communication, phone calls to parents or guardians of
children not receiving preventive dental services. An example is included in
Attachment 2. Marketing tools.
2. Establish procedures to schedule number of working days per month to visit the school
according to the number of consented children. This will depend on how many days the
program will work per week.
An Ideal number of consented children should be established for each day of visit
(20-30 may be ideal number of children)
Please see Attachment 3. Guidelines for a site visit.
10. Clinical Set-Up Procedures 1. Arrive at the time scheduled at site for each day.
-Time at each school may vary and the setting up of the equipment will need to be accounted for.
2. Upon arrival, the school-based dental program coordinator will meet with the contact
person (school nurse/health aide) to find out where the program will be unloading and
setting up their dental clinic. If staying multiple days in a row, the coordinator will need to
find out if the equipment will be able to stay set up and stored in a room that will be
locked overnight until the next scheduled return.
3. The school-based dental program team should unload the dental equipment/supplies
and set up the dental clinic by following the manual of operation for the dental equipment
used.
-An example is included in Attachment 4. Room requirements for a clinic. 4. Once the equipment is set up everything should be checked over to make sure it is in
proper working condition.
5. The dental supplies should be placed onto a clean surface that is covered with a
disposable tablecloth.
-An example is included in Attachment 5. Supply/Equipment daily list for packing.
6. Once the clinic is ready to start providing services the coordinator will need to meet with
the school nurse to speak about patient flow, lunch/recess times, special classes and
any other activities that might interrupt or interfere the work of the dental clinic
throughout the day.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 7 of 31
11. Infection Control Procedures The goal of infection control is to prevent patients and staff from developing an associated infectious disease by following the Center for Disease Control’s infection guidelines.
Each person who is part of the staff of the program must go through the required
proper training of blood borne diseases and infection control procedures
Each individual must accept personal responsibility for practicing proper infection
control and should be an advocate of infection control.
All staff working for the program must have a TB test done annually, Hepatitis B
Immunization and show immunity records for other immunizations.
All staff must follow the exposure incident protocol.
All staff must follow barrier protection policies including hand washing, gloving,
protective eyewear, masks, protective clothing, proper placement and removal of
surface covers and proper cleaning and disinfection of contaminated surfaces.
The staff must protect patient charts from contamination during chair side recording
of patient’s oral status
Each school-based dental program is required to follow their FQHC’s instrument
sterilization procedures, which should be in compliance with CDC policies. (4)
Each school-based dental program is required to follow their FQHC’s waste
management procedures by careful handling and proper disposal of sharps and other
regulated medical waste, which should be in compliance with CDC polices.
Each school-based dental program is required to follow their aseptic techniques
Each school-based dental program is required to follow their general clinical asepsis
protocol
12. Clinical Diagnosis and Procedures Performed by the Dentist Dentists participating in the program need to train and calibrate on how to select teeth for dental sealants.
Suggested Training a. Dentist could be trained following the International Caries Assessment Index
(ICDAS). Pitt and fissures with an ICDAS score 0-3 will be selected for sealant
placement. It’s a simple, logical, evidence-based system for detection and
classification of caries in dental education, clinical practice, dental research
and dental public health.
Training can be accomplished using the following sites/ links http://www.skipcomer.net/projects/dentistry/dental_caries.html http://www.icdas.org/

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 8 of 31
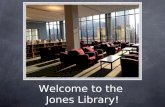
b.
Diagnosis flow chart by Zero Domenick
Communicate in appropriate, culturally-competent communication with patients,
school nurses and staff. In US services to diverse populations may need to be
provided, there are increasing numbers of Hispanics/ Latinos, Indian, Burmese, Asian
cultures and the proportion may vary from site to site. Recruiting personnel with
No Treatment
No Disease ICDAS 0
Remineralize
Initial Lesion
ICDAS 1
Primary Prevention at the Patient Level
Secondary Prevention Tertiary Prevention (Care)
Initial Lesion
ICDAS 2
Arrest Sealant
Moderate Lesion
ICDAS 3
Minimal Surgical
Moderate Lesion
ICDAS 4
Traditional Surgical
Extensive Lesion
ICDAS 5
EndodonticTreatment
Extensive Lesion
ICDAS 6
Caries Risk Assessment at the Patient Level
Extraction
Caries Lesion Activity Assessment
Caries Risk Assessment at the Tooth Surface Level
Staging of Lesion Severity
Radiographs and Other Diagnostic Aids
DIAGNOSIS
Additional Information that Informs Diagnosis

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 9 of 31
experience cultural issues and from different backgrounds that can speak other
languages is important. The Team should receive training on an ongoing basis in the
use of practical methods for cross-cultural encounters in order to elicit information
and negotiate with patients and parents in a culturally competent manner.
12. General Clinical Procedures
1. Before the child is seated in the dental chair, there needs to be a review and verification of the consent form to make sure that you have the correct patient.
a. Review that consent for treatment is properly signed and the medical history has been completed.
b. Verify the name of the children and ask for the birthdate to confirm information is correct
c. Check the medical and dental history to verify there are no contraindications for treatment and that the health of the children is not to be compromised with the services provided.
d. At this time you will explain to the child why they are there and a brief summary of what will be done during their visit.
2. Establish a procedure to teach oral hygiene and tooth brushing instructions while at the same time performing a toothbrush prophy of teeth to be sealed. Do not use toothpaste during the tooth brush prophy.
3. After the toothbrush prophy has been completed the dentist should complete a full oral hard and soft tissue examination and write a dental prescription based on the established criteria for which teeth, if any, need to be sealed. (An example is included in Attachment 6. Dental chart).
4. Since working under the new law, the dental hygienist has 45 days to return to the site and preform the dental sealants described in the dental prescription written by the licensed dentist.
5. Define the procedures for placing a good sealant. Suggested Procedure: a. Assess patient cooperation and isolation if possible before starting any
procedure b. Make sure the fissure system of the tooth to be sealed is clean and has no
calculus or remaining plaque or food. c. Clean and dry the tooth, placing etchant on the tooth for at least 20 seconds. d. Remove etchant with a cotton roll or with water until it has disappeared. e. Drying the tooth until the appearance of etched enamel (Chalky-white), which
normally takes 20 seconds. f. Place the sealant material, using the sealant applicator or with a microbrush. g. Make sure sealant is placed on all the fissure system and avoid overflowing.
Some manufacturer’s state to wait up to 15 seconds before curing to allow time for the sealant to flow to the bottom of the fissure.
h. Choose an appropriate curing light time depending on strength and intensity (see manufacturer’s instructions).

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 10 of 31
i. Verify the sealant integrity and if it stayed in the tooth check for bubbles or defects and re apply sealant if necessary with an explorer.
j. After placing the sealant, you rinse the patient’s mouth with water to eliminate sealant and etchant remnants and avoid the patient to swallow these dental materials. (bisphosphonates issue)
k. Check the patient’s occlusion and bite with articulating paper. If necessary remove excess sealant material with a carver or discoid cleoid.
6. Develop procedures to enter patient data and findings electronically so daily, monthly and quarterly reports can be generated. Records should be kept locked at all time.
7. Develop a report of the visit for the legal guardian/parent for every child seen by the program. There should be three copies for each patient seen; one for the patient, one for the school and one to be kept by the school-based dental program. Each parent report should explain the child’s dental health, the treatment provided, the need for follow-up and when indicated, billing information. (An example is included in Attachment 7. Parent Report).
8. End of the day dental clinic shut down. Suggested Procedure a. Use an enzyme solution that should be run through the lines. b. Clean and disinfect all portable equipment c. Pack all portable dental equipment in the appropriate and safe places.
13. Post Visit Procedures There needs to be a designated storage area for your dental equipment and supplies. This area should be a safe place where everything can be stored overnight and when your dental program is not traveling. Some of the medicines and dental materials need to be stored in ambient temperatures so you need to make sure that this applies.
14. Follow Up Procedures
Follow up procedures need to be developed for consented children who receive an exam and/or dental sealants.
1. Let the school nurse know of any children who have severe caries and are in need of immediate follow up restorative treatment.
2. Contact the legal guardian/parent for children with reported severe dental caries and are in need of immediate attention.
3. Refer children with severe caries back to the FQHC to have their restorative treatment done
Develop procedures for follow up and assessment of dental sealants retention placed on a yearly basis.
1. The initial consent form that is filled out by the legal guardian/parent should cover for
a first visit and a recheck visit. Ideally the consent form should be cover this visits; It
is advisable to state that it should be legal to see a child for 24 months afterwards
which allows for a recheck visit.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 11 of 31
2. When the program returns to a school, a recheck list of the children who had sealants
placed the previous year should be created. New consents should be obtained for
new and recheck children. If a child on the recheck list has a new consent form for
the new visit then any new treatment can be done. If the child does not have a new
consent form then only the sealants done in the previous year can be checked and
repaired if needed.
3. The licensed dentist will provide an exam, in this the dentist will verify that:
If dental treatment was indicated this was provided by assessing presence of
restorations, extractions and treatment done
New oral findings
Assess dental sealants placed using the following retention criteria. If a sealant
needs to be replaced a new prescription will be created.
If the recheck child has not received treatment or needs further treatment this
should be stated in the parent report. A follow up is indicated for children in
need of dental treatment as stated in this section.
Suggested Criteria Following this criteria the licensed dentist will determine the need or not to repair or replace a dental sealant. (5)
Clinical Criteria for Assessing Retention of Sealants
Narrative Description clinical
Retained (R)
Sealant covering more than 90% of the fissure system after prolonged air drying (>5s)
Partially Retained (PR)
Sealant covering less than 90% and more than 70% of the fissure system after prolonged air drying (>5s)
Partially Absent (PA)
Sealant covering less than 70% of the fissure system after prolonged air drying (>5s)
Absent (A)
Sealant or traces of sealant covering less than 30% of the fissure system after prolonged air drying (>5s)
15. Data Collection, Reporting and Quality Assurance Develop data collection procedures Suggested Procedures:
a. Record data in the children’s dental chart
I. A unique identifier for each child will need to be established, this
could be accomplished by having child by his/her name and DOB. A
standard format that will be used across all programs will be

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 12 of 31
developed; this should be compatible with any statistical software
package.
II. All basic demographic variables should be included; age,
race/ethnicity, gender and SES (or some proxy of SES). This
information should be included in the consent form and in the
medical/dental history form. A standard format to be used across all
programs with especially clear definitions for race/ethnicity and SES
will be established.
b. Transfer the data to a central data processing center
c. Clean the data and place in a dataset
d. Analyze the measurable outcomes that were established in the protocol
The following performance measures should be recorded, at a minimum:
Total Number of Children receiving an oral exam
o After the second year, First exam and Subsequent exam Number of children with caries DMFT (decayed, missing and filled teeth) for children receiving an oral
exam, including cavitated and non cavitated caries lesions
Number of Children seen below 6 years of age
Number of Children seen between 6-7 years of age o Number of unduplicated children seen who were 6-7 years old and
Received a dental sealant or had a sealant on at least one permanent 1st molar
Number of Children between 8-9 years of age o Number of unduplicated children seen who were 8-9 years old and
Received a dental sealant or had a sealant on at least one permanent 1st molar
Number of Children above 10 years of age o Number of unduplicated children seen who were above 10 years old and
Received a dental sealant or had a sealant on at least one permanent 1st molar
Average cost per children receiving a dental exam
Number of Children receiving sealants. o Number of dental sealants placed.
Number of dental sealants placed on first molars and second molars
Average cost per sealant placed
Number of new patients receiving an oral exam, and get one dental sealant on a permanent molar
o Number of new patients receiving an oral exam, and get two or more dental sealants on a permanent molar
o The second year will include a recheck category
Number of children diagnosed with caries lesions receiving follow up care
Number of children receiving toothbrush prophy
Number of children receiving fluoride treatment

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 13 of 31
Number of new and repeated sites the program visits
Average cost per site visit
Number of days providing services
The collection of these outcomes satisfies the following Oral Health Performance Measure: Percentage of 6-9 year old children who have received a dental sealant on at least one permanent first molar. Because the CDC currently recommends measuring dental sealants in 6-9 year old children, the Division of Maternal Child Health (MCH) at ISDH has set the above performance measure to reflect the current CDC guidelines. MCH plans to report this percentage in sub-categories of children; that is, in 6-7 and 8-9 year old children (8-9 year old children will be a proxy measure for third graders). The program may calculate the percentages to meet the MCH requirements using the following data:
The number of unduplicated children seen during each quarter who are 6-7 years old at
the end of the quarter;
The number of unduplicated children seen during the quarter who are 6-7 years old at
the end of the quarter and had a dental sealant on at least one permanent first molar;
The number of unduplicated children seen during the quarter who are 8-9 years old at
the end of the quarter; and
The number of unduplicated children seen the quarter who are 8-9 years old at the end
of the quarter and had a dental sealant on at least one permanent first molar.
This is the minimal individual primary data that needs to be recorded in each child’s chart, the format of the data will be established once the software program is decided. This will help that a statistician/epidemiologist can obtain individual calculated data, such as, knowing the date of the exam, the child’s DOB, and then calculate the age of the child at the exam date. Also from the individual primary data and the individual calculated data a statistician/epidemiologist can derive the performance measures for a group of children over a specified period of time. Develop a quality plan to ensure that the program meets all the stated objectives.
The plan will consist of: a. A Quality Assurance Plan that will list the independent reviews that will be
performed by a quality assurance officer
b. A Quality Control Plan that will list the internal reviews that will be performed to
meet our quality targets. This list of internal reviews will include random chart
audits and second checks by program personnel.
c. The computer systems of participants should be compatible with the software
program and programs used by other centers.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 14 of 31
16. Program Evaluation FQ/CHCs will be responsible for sending out program evaluations to the sites that host the school-based dental program at the completion of years 1, 2 and 3. These survey evaluations will be developed in year 1. (An example is included in Attachment 8. Program Evaluation) The Evaluation for the school-based program will cover these categories:
Quality of team and services
Consent process and convenience
Overall experience
Preferred dates of return
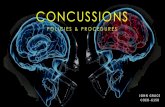
17. SBSP Flow Chart
18. References 1. American Dental Association. Principles of Ethics and Code of Professional Conduct. Available at: “http://www.ada.org/prof/prac/law/code/index.asp”.. 2. Sfikis P. A duty to disclose: Issues to consider in securing informed consent. J Am Dent Assoc 2003;134(10):1329-33.3 http://www.sfdda.org/web/pdf/ga/Indiana%20Dental%20Act.pdf 3. Health Information Privacy (HIPPA) http://www.hhs.gov/ocr/privacy/ 4. Guidelines and Recommendations. Recommended Infection Control Practices for Dentistry, Centers for Disease Control and Prevention. http://www.cdc.gov/oralhealth/infectioncontrol/guidelines/index.htm
Following Site Visit SBSP Site Visit and clinical
procedures Prior to Site Visit
The program coordinator will target Title 1 schools in
underserved areas that could benefit from the services of the
SBSP.
The coordinator will work with the school nurse to schedule site visit dates, market the
program to interested families and ensure that all children needed to be seen are fully
consented for treatment before the site visit date.
The coordinator will stay in contact with the school nurse
and provide any extra help they may need.
The coordinator will keep the calendar up to date with any informatin for the SBSP team
Dental services provided on the first visit will include an exam
done by a licensed dentist. The dentist will write a prescription defining which teeth are to be
sealed on each consented patient.
The Indiana law will allow a licensed hygienist to return to the
site within 45 days to place the sealants.
Contact legal guardian/parent for children with reported
severe caries and are in need of immediate attention
These children in need of follow up treatment may be referred back to the FQHC to have their
restorative treament done.
The recorded data in each patient's dental chart will be transferred to a
central data processing center.
The SBSP will summarize the data of participation and services provied for each site and send a report to
each school.
After the final visit, each child will receive a parent report explaining what treatment was provided and if there is
any additional follow up treatment needed.
Inform school nurse of any children who have severe caries and are in need of
immediate dental treatment.
The SBSP will be responsible for sending out a program evaluation
for each site visited. The evaluation will cover:
-Quality of team and services
-Consent and martketing process
-Overall experience
-Preferred dates of return

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 15 of 31
5. Soto Rojas AE, Escoffie-Ramírez M, Perez-Ferrera G, Guido JA, Mantilla, A. Martinez-Mier EA. Retention of Dental Sealants Placed on Sound Teeth and Incipient Caries Lesions as Part of a Service Learning Program in Rural Areas in Mexico. Int J Paediatr Dent 2012 Nov;22(6):451-8 For further information about SBSP please also refer to the Indiana Law Code this is a shortened version of the Indiana Law on mobile dental programs. ARTICLE 4. MOBILE DENTAL FACILITIES AND PORTABLE DENTAL OPERATIONS Rule 1. Applicability; Exceptions 828 IAC 4-1-1 Applicability Authority: IC 25-14-1-13 Affected: IC 25-14 Sec. 1. This article applies to the operator of a mobile dental facility or portable dental operation who: (1) provides dental services; and (2) does not have a physically stationary office in the county where the services are provided. (State Board of Dentistry; 828 IAC 4-1-1; filed May 2, 2002, 10:24 a.m.: 25 IR 2736; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-1-2 Exceptions Authority: IC 25-14-1-13 Affected: IC 25-13-1-10; IC 25-13-1-11; IC 25-14 Sec. 2. (a) Federal, state, and local governmental agencies are exempt from the requirements of this rule. 828 IAC 4-2-2 “Mobile dental facility or portable dental operation” Defined Authority: IC 25-14-1-13 Affected: IC 25-14 Sec. 2.“Mobile dental facility or portable dental operation” means either of the following: (1) Any self-contained facility in which dentistry will be practiced, which may be moved, towed, or transported from one (1) location to another. (2) Any nonfacility in which dental equipment, utilized in the practice of dentistry, is transported to and utilized on a temporary basis at an out-of-office location, including, but not limited to: (A) other dentists’ offices; (B) patients’ homes; 59 (C) schools; (D) nursing homes; or (E) other institutions. (State Board of Dentistry; 828 IAC 4-2-2; filed May 2, 2002, 10:24 a.m.: 25 IR 2736; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) Rule 3. Registration 828 IAC 4-3-1 Application Authority: IC 25-14-1-13 Affected: IC 25-14

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 16 of 31
Sec. 1. (a) In order to operate a mobile dental facility or portable dental operation, the operator shall register with the board. (b) The applicant shall complete an application in the form and manner required by the board. (c) The applicant shall pay the registration fee at the time of application as set by the board by rule. (d) The applicant shall provide the board with evidence of compliance with the requirements of this rule. (e) The applicant shall submit proof of radiographic equipment inspection with the application for registration. (State Board of Dentistry; 828 IAC 4-3-1; filed May 2, 2002, 10:24 a.m.: 25 IR 2737; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-2 Official business or mailing address Authority: IC 25-14-1-13 Affected: IC 25-14 Sec. 2. (a) The operator of a mobile dental facility or portable dental operation shall maintain an official business or mailing address of record, which shall not be a post office box and which shall be filed with the board. (b) The operator of a mobile dental facility or portable dental operation shall maintain an official telephone number of record, which shall be filed with the board. (c) The board shall be notified within thirty (30) days of any change in the address or telephone number of record. (d) All written or printed documents available from or issued by the mobile dental facility or portable dental operation shall contain the official address and telephone number of record for the mobile dental facility or portable dental operation. (e) When not in transit, all dental and official records shall be maintained at the official office address of record. (State Board of Dentistry; 828 IAC 4-3-2; filed May 2, 2002, 10:24 a.m.: 25 IR 2737; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-3 Written procedures; communication facilities; conformity with requirements; driver requirements Authority: IC 25-14-1-13 Affected: IC 12-15; IC 12-17.6; IC 25-14 Sec. 3. The operator of a mobile facility, mobile unit, or portable dental operation shall ensure the following: (1) There is a written procedure for emergency follow-up care for patients treated in the mobile dental facility and that such procedure includes arrangements for treatment in a dental facility that is permanently established in the area where services were provided. (2) The mobile dental facility has communication facilities that will enable the operator thereof to contact necessary parties in the event of a medical or dental emergency. The communications facilities must enable the patient or the parent or guardian of the patient treated to contact the operator for emergency care, follow-up care, or information about treatment received. The provider who renders follow-up care must also be able to contact the operator and receive treatment information, including radiographs. (3) The mobile dental facility conforms to all applicable federal, state, and local laws, regulations, and ordinances dealing with radiographic equipment, flammability, construction, sanitation, zoning, infectious waste management, universal precautions, OSHA guidelines, and federal Centers for Disease Control Guidelines, and the applicant possesses all applicable county and city licenses or permits to operate the unit. (4) The driver of the unit possesses a valid Indiana driver’s license appropriate for the operation of the vehicle. (5) No services are performed on minors without a signed consent

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 17 of 31
form from the parent or guardian, which indicates that: (A) if the minor already has a dentist, the parent or guardian should continue to arrange dental care through that provider; and (B) the treatment of the child by the mobile dental facility may affect the future benefits that the child may receive under: (i) private insurance; (ii) Medicaid (IC 12-15); or (iii) the children’s health insurance program (IC 12-17.6). (6) A mobile dental facility that accepts a patient and provides preventive treatment, including prophylaxis, radiographs, and fluoride, but does not follow-up with treatment when such treatment is clearly indicated, is considered to be abandoning the patient. Arrangements must be made for treatment services. (State Board of Dentistry; 828 IAC 4-3-3; filed May 2, 2002, 10:24 a.m.: 25 IR 2737; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-4 Physical requirements for mobile dental facility Authority: IC 25-14-1-13 Affected: IC 25-14 Sec. 4. The operator shall ensure that the mobile dental facility or portable dental operation has the following: (1) Ready access to a ramp or lift if services are provided to disabled persons. (2) A properly functioning sterilization system. (3) Ready access to an adequate supply of potable water, including hot water. (4) Ready access to toilet facilities. (5) A covered galvanized, stainless steel, or other noncorrosive container for deposit of refuse and waste materials. (State Board of Dentistry; 828 IAC 4-3-4; filed May 2, 2002, 10:24 a.m.: 25 IR 2738; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-5 Identification of personnel; notification of changes in written procedures; display of licenses Authority: IC 25-14-1-13 Affected: IC 25-14 Sec. 5. (a) The operator shall identify and advise the board in writing within thirty (30) days of any personnel change relative to all licensed dentists and licensed dental hygienists associated with the mobile dental facility or portable dental operation by providing the full name, address, telephone numbers, and license numbers where applicable. (b) The operator shall advise the board in writing within thirty (30) days of any change in the written procedure for emergency follow-up care for patients treated in the mobile dental facility, including arrangements for treatment in a dental facility, which is permanently established in the area. The permanent dental facility shall be identified in the written procedure. (c) Each dentist and dental hygienist providing dental services in the mobile dental facility or portable dental operation shall prominently 60 display his or her Indiana dental or Indiana dental hygienist license in plain view of patients. (State Board of Dentistry; 828 IAC 4-3-5; filed May 2, 2002, 10:24 a.m.: 25 IR 2738; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-6 Identification of location of services

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 18 of 31
Authority: IC 25-14-1-13 Affected: IC 25-14 Sec. 6. (a) Each operator of a mobile dental facility or portable dental operation shall maintain a written or electronic record detailing for each location where services are provided: (1) the street address of the service location; (2) the dates of each session; (3) the number of patients served; and (4) the types of dental services provided and quantity of each service provided. (b) The written or electronic record shall be made available to the board within ten (10) days of a request by the board. Costs for such records shall be borne by the mobile dental facility. (State Board of Dentistry; 828 IAC 4-3-6; filed May 2, 2002, 10:24 a.m.: 25 IR 2738; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-7 Licensed dentist in charge Authority: IC 25-14-1-13 Affected: IC 25-14 Sec. 7. A mobile dental facility or portable dental operation shall at all times be in the charge of a dentist licensed to practice dentistry in Indiana. A dentist licensed to practice dentistry in Indiana shall be present at all times that clinical services are rendered. (State Board of Dentistry; 828 IAC 4-3-7; filed May 2, 2002, 10:24 a.m.: 25 IR 2738; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-8 Prohibited operations Authority: IC 25-14-1-13 Affected: IC 25-13; IC 25-14 Sec. 8. The operator of a mobile dental facility or portable dental operation is prohibited from hiring, employing, allowing to be employed, or permitting to work in or about a mobile dental facility or portable dental operation, any person who performs or practices any occupation regulated under IC 25-13 or IC 25-14 who is not duly licensed by the board. (State Board of Dentistry; 828 IAC 4-3-8; filed May 2, 2002, 10:24 a.m.: 25 IR 2738; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-9 Information for patients Authority: IC 25-14-1-13 Affected: IC 25-14 Sec. 9. (a) During or at the conclusion of each patient’s visit to the mobile dental facility or portable dental operation, the patient shall be provided with an information sheet. If the patient has provided consent to an institutional facility to access the patient’s dental health records, the institution shall also be provided with a copy of the information sheet. An institutional facility includes, but is not limited to, a long term care facility or school. (b) An information sheet shall include the following: (1) Pertinent contact information as required by this article. (2) The name of the dentist and other dental staff who provided services. (3) A description of the treatment rendered, including billed service codes and fees associated with treatment, and tooth numbers when appropriate.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 19 of 31
(4) If necessary, referral information to another dentist as required by this article. (State Board of Dentistry; 828 IAC 4-3-9; filed May 2, 2002, 10:24 a.m.: 25 IR 2738; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-10 Cessation of operations Authority: IC 25-14-1-13 Affected: IC 16-39; IC 25-14 Sec. 10. (a) Upon cessation of operation by the mobile dental facility or portable dental operation, the operator shall notify the board within thirty (30) days of the last day of operations in writing of the final disposition of patient records and charts. (b) If the mobile dental facility or portable dental operation is sold, a new registration application must be filed with the board. (c) Upon choosing to discontinue practice or services in a community, the operator of a mobile dental facility or portable dental operation shall: (1) notify all of the operator’s active patients in writing, or by publication once a week for three (3) consecutive weeks in a newspaper of general circulation in the community, that the operator intends to discontinue the mobile dental facility’s or portable dental operation’s practice in the community; and (2) encourage the patients to seek the services of another dentist. (d) The operator shall make reasonable arrangements with the active patients of the mobile dental facility or portable dental operation for the transfer of the patient’s records, including radiographs or copies thereof, to the succeeding practitioner or, at the written request of the patient, to the patient, in compliance with IC 16-39. (e) As used in this section, “active patient” applies and refers to a person whom the mobile dental facility or portable dental operation has examined, treated, cared for, or otherwise consulted with during the two (2) year period prior to discontinuation of practice, or moving from or leaving the community. (f) Nothing in this section supersedes the requirements of IC 16-39. (State Board of Dentistry; 828 IAC 4-3-10; filed May 2, 2002, 10:24 a.m.: 25 IR 2739; readopted filed Sep 26, 2008, 10:49 a.m.: 20081015-IR- 828080336RFA) 828 IAC 4-3-11 Renewal of registration Authority: IC 25-14-1-13 Affected: IC 25-14
18. Attachments (1-8) Attachment 1: Seal Indiana Consent Form Attachment 2: Marketing tools Attachment 3: Guidelines for a site visit Attachment 4: Room Requirements Attachment 5: Supply/Equipment list for packing Attachment 6: Dental Chart Attachment 7: Parent Report Attachment 8: Program Evaluation

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 20 of 31

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 21 of 31

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 22 of 31
Attachment 2
Dental Sealant Program
For Immediate Release
Fill in DATE
SEALANT PROGRAM COMING TO Fill in SITE
The dental sealant program will provide preventive dental care this year for children enrolled in Fill in SITE on Fill in
Day, Month, Date, year. A temporary dental clinic will be set up inside Fill in SITE, where services will include
examinations, dental sealants, and fluoride varnish. Children will also receive individual brushing instruction and a
toothbrush prophy, along with a toothbrush and toothpaste.
Sealants are thin plastic coatings applied to the tiny grooves on the chewing surfaces of the back teeth. This is where most
tooth decay in children and teens occurs. Sealants protect the chewing surfaces from decay by keeping germs and pieces
of food out. The Surgeon General’s report on oral health indicates that sealants can reduce decay in school children by
more than 70 percent.
A fluoride varnish treatment provides added protection against decay for all teeth.
To have their children participate, parents should complete, sign and check mark YES the SEALANT PROGRAM consent,
being sent home by Fill in SITE. For children enrolled in Medicaid/Hoosier Healthwise, the entire cost of preventive
dental treatment (toothbrush prophy, dental exam, sealants and fluoride) is covered. A sliding fee scale, based on family
income, and a cap on services is available for those without insurance.
The SEALANT program is staffed by licensed dentists who provide exams along with staff member and dental hygienists
who provide the sealants.
The Sealant program operates with support of the Indiana State Department of Health and is endorsed by the Indiana
Dental Association.
For more information, or call
or Fill in site, at Fill in site’s telephone number.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 23 of 31
SEALANT PROGRAM COMING TO NAME OF SITE NAME OF SITE: DAY, MONTH, DATE, YEAR
THE XX SEALANT PROGRAM is a local mobile dental program operated by XXX,
with support of IN Department of Health.
THE SEALANT PROGRAM provides preventive dental care including exams, toothbrush cleanings, sealants and a fluoride varnish
for children who are NOT receiving regular dental care or dental sealants.
Medicaid pays 100% for preventive dental care.
Reduced fees and grants available for children without Hoosier Healthwise!
PARENTS: SIGN, CHECK YES! & RETURN CONSENTS TO SCHOOL
*If you do not plan on your child being seen by us then please return the blank consent form to your school so that we can
recycle and use them for next year GO GREEN!
A dental sealant is a plastic material applied to the chewing surface of back teeth where decay occurs most often. Sealants protect
these teeth from plaque and acid that causes decay. Receiving sealants is comfortable, and no anesthetic is required.
A fluoride varnish treatment
provides added protection against decay for all teeth.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 24 of 31
Date: Fill In Date
To: Fill In School, RN Name
From: FQHC Program
Re: Visit to Fill in Site
Good Morning, School, RN
We are shipping # of English/# of Spanish XXX parental consents for all children
enrolled at Fill in Site in preparation for our scheduled site visit, Day, Month, Date, Year.
It generally takes our dental team
30 minutes to set up the temporary dental clinic (room requirements enclosed).
Each child should receive one consent, and parents/guardians are asked to sign, check
mark YES and then return the form to you within two weeks of our visit.
Medicaid pays 100% for preventive dental care for children. For families without
Medicaid, a sliding fee scale and a cap on services is included.
Following service, each child will receive a Report to the Parent (with a copy for
the school), explaining the services he/she received, informing parents if follow-up care is
needed, and indicating the amount they will be billed, if applicable.
children in need of follow-up, especially those with an urgent need for dental care.
We have emailed a publicity flyer and news release for use in publicizing our visit.
Some schools duplicate the flyer and send it home with the parental consents and/or use
the flyer/ release on the school website and in the school newsletter.
Please call at (XXX)-XXX or email at [email protected] if I can provide anything further or
answer any questions you may have. We look forward to serving the students of Fill in
Site and to working with you. Thank you for helping FQHC bring preventive dental care
to children in your area.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 25 of 31
Attachment 3
ROOM REQUIREMENTS SPECIFICATIONS, SUPPLIES &PREPARATION FOR A TEMPORARY
DENTAL CLINIC
A closed and properly ventilated room or space at least 35 x 35 feet
with no rugs, if possible, and large enough for
2 portable dental operatories, dental supplies and a waiting area for children.
2 tables (one for supplies and one for patient check-in/paperwork)
At least 2 available electrical plugs
Wireless Internet connection close by, if possible
6-8 folding chairs
1-2 large trash cans (cafeteria size)
Close to bathroom facility, if possible
Preferably no nurses clinics, unless it is large enough
If possible, the room should be clean and free of clutter in all areas. Tables
should be ready to use with nothing on them.
Preferably a room within close distance to a ramp or unloading dock/station if
this is not possible you could help us with a cart or dolly if available
No 2nd floor rooms unless there is an elevator on-site
Because of required infection control, rooms we are not allowed to use:
Basements that are not clean and appropriately furnished
Laundry facilities/ janitorial
Locker rooms with bathrooms
Hallways
Thank you for helping us with the setup of our dental clinic

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 26 of 31
Picture 1.

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 27 of 31
Attachment 4
Daily Supply List Baskets
Contaminated Instrument Containers
Hand Sanitizer
Instruments mirrors and explorers, cleoid discoid
Cavi Wipes
Vacu Kleen
Vaseline
Patient Napkins/Extra Sunglasses
Plastic Cups
Extra cotton rolls/Gauze
Rubber Bands
Air/Water Covers
Curing light covers
Air/Water tips
Articulating paper
Covers for new light
Toothpaste
5-7 yr old Tooth Brushes
#35 Tooth Brushes
2 Boxes of Small Gloves
2 Boxes of Medium Gloves
2 Boxes of Large Gloves
1 Bag of regular gowns
1 Bag of X-Large gowns
Table Cloth
1 Box of facemasks
Safety Glasses
.25 fluoride
.4 fluoride
Patient Hand mirror
Sealant Kits
Saliva Ejectors
Extras bag
Chair Kits
Echant
Sealant Material
Deionized Water

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 28 of 31
Pictures 2
Picture 3
Picture 4

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 29 of 31
Attachment 6

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 30 of 31
Attachment 7
REPORT TO PARENTS/GUARDIANS
On _______________________ your child _____________________________________________ had an appointment
at school with the dentist and the School Based Sealant Program team from FQHC. This is a report of that visit.
Your child’s dental decay treatment needs:
□ No obvious dental decay. Please continue with regular dental examinations.
□ Dental decay may be present but cannot be confirmed without x-rays. Please take your child to a dentist for a complete
examination with x-rays.
□ Dental decay was detected. Please make an appointment with a local dentist for follow-up treatment.
□ Severe dental decay was detected. Please make an appointment with a local dentist immediately.
□ Your child is experiencing pain and/or infection and needs an immediate appointment with a local dentist.
Your child and dental Sealants
□ Your child received dental sealants on _________ teeth. The sealants will protect the biting surface of back teeth from
dental decay. You will be able to see the sealants because they have an opaque, white appearance.
□ Your child did not receive sealants because:
□ Incomplete tooth eruption (try later) □ decay present □ sealants already present
□ Your child was too afraid □ Could not keep teeth dry □ uncooperative □ other:
□ The sealants placed by us at a previous visit were examined.
□ All were intact. □ ___ were intact. □ ___ were repaired. □ ___ were replaced.
Fluoride Varnish Treatment
□ Your child received a fluoride treatment that was painted on his/her teeth. This varnish is a very effective treatment that
remains on the teeth longer than fluoride gel treatments. While it remains on the teeth, they may appear yellow. This color
will disappear over several hours and/or will brush away with normal tooth brushing.
Your child’s oral hygiene, prevention and other treatment needs:
□ Your child has good oral health, keep up with the good work.
□ Your child has fair oral health needs to brush more often and/ or better.
□ Your child has poor oral health and needs assistance in brushing more often and/ or better.
Attachment 8
SEAL INDIANA recently provided preventive dental services at your school or community center.
We want to provide the best services possible. You can help us achieve this goal by evaluating our
services. Please complete this brief survey and FAX to 317.274.5425 within a few days, if possible.
Your comments will be taken seriously. Thank you for your help!
NOTES

Policies and Procedures Manual for School-Based Sealant Programs
Revision: Draft 1 Date: Jan 2016 Page: 31 of 31
Seal Indiana Program 317.278.9094 [email protected]
Was this your first visit by Seal Indiana?
Are you the: School Title I Director Principal Other___________________________
PLEASE RATE: Please circle the appropriate rating
Excellent
Good
Fair
Poor
QUALITY OF TEAM AND SERVICES Communication and scheduling with program manager.
Professionalism and responsiveness of on-site team.
Efficiency and use of time by on-site team.
Kindness and concern of on-site team for children.
Comment:
4
4
4
4
3
3
3
3
2
2
2
2
1
1
1
1
CONSENT PROCESS AND CONVENIENCE Ease in using the written materials. (Were the consent forms and fee schedule understandable/
acceptable?) Hosting Seal Indiana events
Likelihood of recommending Seal Indiana to others.
Comment and/or Referral:
4
4
4
3
3
3
2
2
2
1
1
1
OVERALL EXPERIENCE Quality of overall experience with Seal Indiana.
Satisfaction with your community’s participation.
Likelihood of scheduling another visit. If fair or poor, please
comment.
If any other suggestions, please comment below:
4
4
4
3
3
3
2
2
2
1
1
1
Please indicate preferred dates or month for 2013/14 visit: ______________________________
If your children were assisted by the DELTA GRANT, we encourage you to write a brief anecdote
(below or on a second page) conveying how the grant helped the children. Your thanks will be
conveyed to Delta and will assist Seal Indiana when writing future grant requests.
Name________________________________________________________
School/Corporation____________________________________________