Pineal Anlage Tumor: Case Report and Review of Literature · Pineal region tumors are a...
5
Central JSM Neurosurgery and Spine Cite this article: Ajayi O, Palma A, Sadanand V, Deisch J (2014) Pineal Anlage Tumor: Case Report and Review of Literature. JSM Neurosurg Spine 2(4): 1035. *Corresponding author OlaideAjayi, Department of Neurosurgery, Loma Linda University Medical Center, Loma Linda, CA. 92350, USA, Tel: 4077826285; Fax: 9095584825; Email: Submitted: 02 April 2014 Accepted: 30 April 2014 Published: 07 May 2014 Copyright © 2014 Ajayi et al. OPEN ACCESS Keywords • Pineal gland • Pineal anlage tumor • Primitive neuroepithelial component • Ectomesenchymal component Review Article Pineal Anlage Tumor: Case Report and Review of Literature Olaide Ajayi 1* , Atilio Palma 2 , Venkatraman Sadanand 1 and Jeremy Deisch 3 1 Department of Neurosurgery, Loma Linda University Medical Center, USA, 2 School of Medicine, Loma Linda University, USA 3 Department of Surgical Pathology, Loma Linda University Medical Center, USA INTRODUCTION The pineal gland is a midline organ located posterior to the third ventricle in the quadrigeminal cistern. It is surrounded by the splenium of the corpus callosum above, the thalami laterally, and the quadrigeminal plate and vermis below, together delineating the pineal region [1]. Histologically, the human pineal gland parenchyma is mainly composed of pineocytes with a few supportive astrocytes, is subdivided into lobules imparting a glandular appearance, and is invested by leptomeninges [2]. Lesions of the pineal region are occasionally encountered, and may be non-neoplastic (i.e. pineal cysts) or neoplastic. Pineal neoplasms are relatively rare, accounting for 3-8% of pediatric and less than one percent of adult brain tumors [3]. Pineal region tumors are a heterogenous group of neoplasms, owing to the presence of various cell types present in a small region that can each undergo neoplastic transformation. Germ cell tumors are the most common tumors of the pineal region. Ependymomas, astrocytomas (both localized and diffuse), choroid plexus neoplasms, and meningiomas also may occur, but are much less common. Neoplasms unique to this region are presumed to arise from pineocytes, the resident synaptophysin- positive neuroepithelial cells of the pineal gland. These “pineal parenchymal neoplasms” span a spectrum of biologic aggression, with pineocytomas and pineoblastomas showing the least and most aggressive clinical courses, respectively. Of the tumors unique to the pineal region, the pineal anlage shows the most unusual pathologic features, and is extremely rare. Although not officially recognized as a stand-alone entity by the World Health Organization (WHO), the 2007 WHO Classification of Tumours of the Central Nervous System describes pineal anlage tumors as rare pineoblastomas with melanin production and cartilaginous and/or rhabdomyoblasticdifferentiation [4-6]. Pineal anlage tumors were first described by Schmidbauer and colleagues in 1989 as a pineal region tumor in a 9-year-old girl that exhibited neuronal, retinoblastic and ectomesenchymal differentiation [7]. In the following years, only six other cases of pineal anlage tumors showing the described pathologic features have been reported [6-11]. These tumors showed variable pathologic findings, including primitive neuroepithelial proliferations, neural rosettes, skeletal muscle, pigmented cells, and cartilage. Olaya described a case of a pineal anlage tumor in a 5-month- old boy treated at our institution in 2010 [6]. We report the clinical presentation, neuroradiologicfindings, histopathology, and immunophenotype of a second case of pineal anlage tumor treated at our institution. CLINICAL PRESENTATION An 11-month-old female was brought to the Emergency Department for a four-day history of worsening lethargy, vomiting, and seizures. During the seizure episodes, she would stare and lose postural maintenance and visual tracking. Neurologic examination was significant for lethargy, with eye opening and bilateral upper and lower extremity movement only to deep stimulation. The patient underwent emergent external ventriculostomy drain (EVD) placement, with significant subsequent improvement in her level of alertness. She was admitted to the intensive care unit and started on intravenous dexamethasone. The pre-surgical laboratory workup included serum tumor markers for germ cell neoplasia (βHCG, α-fetoprotein, carcinoembryonic antigen); all were within normal limits. RADIOGRAPHIC FEATURES A head computed tomography (CT) scan was performed, which demonstrated a hyperdense mass in the pineal region with concomitant obstructive non-communicating hydrocephalus of the lateral and third ventricles. A subsequent brain MRI showed a 3 cm mass in the pineal region, with mild diffusion restriction (Figure 1-A). After administration of gadolinium, the mass showed heterogeneous, primarily central enhancement (Figure 1-B). There was mass effect affecting the posterior midbrain and pons, with effacement of the cerebral aqueduct and obstructive non-communicating hydrocephalus (Figure 1-C). Cervical, thoracic, and lumbar spine MRI imaging did not reveal any evidence of spinal region leptomeningeal or parenchymal involvement (“drop metastases”).
Transcript of Pineal Anlage Tumor: Case Report and Review of Literature · Pineal region tumors are a...

Central JSM Neurosurgery and Spine
Cite this article: Ajayi O, Palma A, Sadanand V, Deisch J (2014) Pineal Anlage Tumor: Case Report and Review of Literature. JSM Neurosurg Spine 2(4): 1035.
*Corresponding authorOlaideAjayi, Department of Neurosurgery, Loma Linda University Medical Center, Loma Linda, CA. 92350, USA, Tel: 4077826285; Fax: 9095584825; Email:
Submitted: 02 April 2014
Accepted: 30 April 2014
Published: 07 May 2014
Copyright© 2014 Ajayi et al.
OPEN ACCESS
Keywords•Pineal gland•Pineal anlage tumor•Primitive neuroepithelial component•Ectomesenchymal component
Review Article
Pineal Anlage Tumor: Case Report and Review of LiteratureOlaide Ajayi1*, Atilio Palma2, Venkatraman Sadanand1 and Jeremy Deisch3
1Department of Neurosurgery, Loma Linda University Medical Center, USA,2School of Medicine, Loma Linda University, USA 3Department of Surgical Pathology, Loma Linda University Medical Center, USA
INTRODUCTIONThe pineal gland is a midline organ located posterior to the
third ventricle in the quadrigeminal cistern. It is surrounded by the splenium of the corpus callosum above, the thalami laterally, and the quadrigeminal plate and vermis below, together delineating the pineal region [1]. Histologically, the human pineal gland parenchyma is mainly composed of pineocytes with a few supportive astrocytes, is subdivided into lobules imparting a glandular appearance, and is invested by leptomeninges [2]. Lesions of the pineal region are occasionally encountered, and may be non-neoplastic (i.e. pineal cysts) or neoplastic. Pineal neoplasms are relatively rare, accounting for 3-8% of pediatric and less than one percent of adult brain tumors [3]. Pineal region tumors are a heterogenous group of neoplasms, owing to the presence of various cell types present in a small region that can each undergo neoplastic transformation. Germ cell tumors are the most common tumors of the pineal region. Ependymomas, astrocytomas (both localized and diffuse), choroid plexus neoplasms, and meningiomas also may occur, but are much less common. Neoplasms unique to this region are presumed to arise from pineocytes, the resident synaptophysin-positive neuroepithelial cells of the pineal gland. These “pineal parenchymal neoplasms” span a spectrum of biologic aggression, with pineocytomas and pineoblastomas showing the least and most aggressive clinical courses, respectively. Of the tumors unique to the pineal region, the pineal anlage shows the most unusual pathologic features, and is extremely rare. Although not officially recognized as a stand-alone entity by the World Health Organization (WHO), the 2007 WHO Classification of Tumours of the Central Nervous System describes pineal anlage tumors as rare pineoblastomas with melanin production and cartilaginous and/or rhabdomyoblasticdifferentiation [4-6]. Pineal anlage tumors were first described by Schmidbauer and colleagues in 1989 as a pineal region tumor in a 9-year-old girl that exhibited neuronal, retinoblastic and ectomesenchymal differentiation [7]. In the following years, only six other cases of pineal anlage tumors showing the described pathologic features have been reported [6-11]. These tumors showed variable pathologic findings, including primitive neuroepithelial proliferations, neural rosettes, skeletal muscle, pigmented cells, and cartilage.
Olaya described a case of a pineal anlage tumor in a 5-month-old boy treated at our institution in 2010 [6]. We report the clinical presentation, neuroradiologicfindings, histopathology, and immunophenotype of a second case of pineal anlage tumor treated at our institution.
CLINICAL PRESENTATION An 11-month-old female was brought to the Emergency
Department for a four-day history of worsening lethargy, vomiting, and seizures. During the seizure episodes, she would stare and lose postural maintenance and visual tracking. Neurologic examination was significant for lethargy, with eye opening and bilateral upper and lower extremity movement only to deep stimulation. The patient underwent emergent external ventriculostomy drain (EVD) placement, with significant subsequent improvement in her level of alertness. She was admitted to the intensive care unit and started on intravenous dexamethasone. The pre-surgical laboratory workup included serum tumor markers for germ cell neoplasia (βHCG, α-fetoprotein, carcinoembryonic antigen); all were within normal limits.
RADIOGRAPHIC FEATURES A head computed tomography (CT) scan was performed,
which demonstrated a hyperdense mass in the pineal region with concomitant obstructive non-communicating hydrocephalus of the lateral and third ventricles. A subsequent brain MRI showed a 3 cm mass in the pineal region, with mild diffusion restriction (Figure 1-A). After administration of gadolinium, the mass showed heterogeneous, primarily central enhancement (Figure 1-B). There was mass effect affecting the posterior midbrain and pons, with effacement of the cerebral aqueduct and obstructive non-communicating hydrocephalus (Figure 1-C). Cervical, thoracic, and lumbar spine MRI imaging did not reveal any evidence of spinal region leptomeningeal or parenchymal involvement (“drop metastases”).

Central
Ajayi et al. (2014)Email:
JSM Neurosurg Spine 2(4): 1035 (2014) 2/5
OPERATIVE MANAGEMENTThe patient was taken to the operating room emergently for
an endoscopic third ventriculostomy and endoscopic biopsy of the tumor via a right frontal approach. She was taken back to the operating room six days later, where she underwent a right occipital transcortical craniotomy for resection of the tumor. A subsequent post-operative MRI showed gross total resection of the tumor (Figure 1-D).
PATHOLOGIC FEATURESThe initial endoscopic biopsy specimen obtained from the
first hospital day yielded a 0.6 cm aggregate of tan gelatinous tissue fragments and clotted blood. The cellular areas showed a densely-cellular, sheet-like proliferation of small, primitive cells with scant cytoplasm, and high nucleus to cytoplasm (N:C) ratio. There was moderate variation in the size and shape of the nuclei, vesicular to coarsely-granular chromatin, and indistinct chromocenters. Nucleoli were not prominent. These features were consistent with so-called “small round blue cell” tumor. Mitotic figures and apoptotic bodies were frequently encountered throughout the tumor. Immunohistochemical studies performed on the formalin-fixed, paraffin-embedded biopsy material demonstrated patchy granular cytoplasmic synaptophysin immunoreactivity, cytoplasmic process Neurofilament protein (NFP) staining, and a markedly elevated Ki-67 labeling index (~90%). A negative placental alkaline phosphatase (PLAP) stain militated against germ cell neoplasia. No heterologous elements were seen in the limited biopsy material. The initial biopsy was assigned a final pathologic diagnosis of “pineoblastoma, WHO grade IV”.
The subsequent craniotomy and surgical resection yielded a 3 cm aggregate of gelatinous tan tissue fragments. Neuropathologic
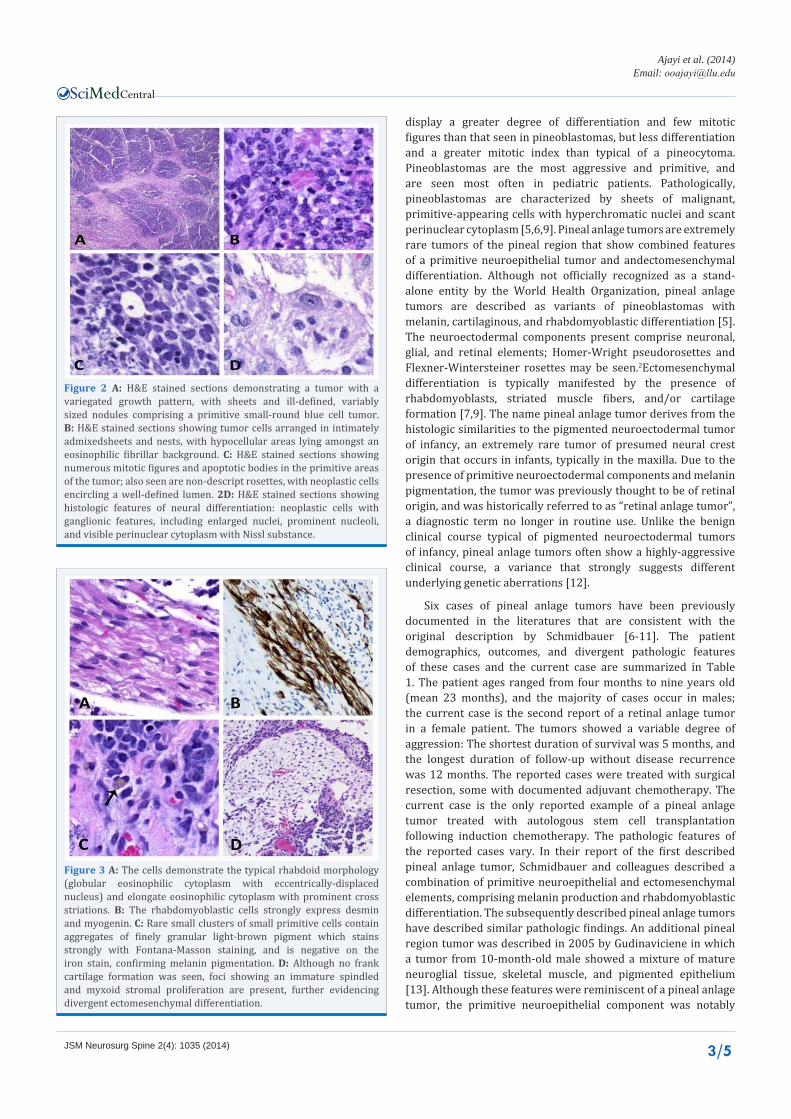
examination of multiple hematoxylin and eosin (H&E) stained sections demonstrated a tumor with a variegated growth pattern, with sheets and ill-defined, variably sized nodules comprising a primitive small-round blue cell tumor identical to that seen in the endoscopic biopsy. The sheets and nests were intimately admixed with hypocellular areas lying amongst an eosinophilic fibrillar background (Figure 2-A,B). Mitotic figures and apoptotic bodies were most numerous in the primitive areas. Rare non-descript rosettes were present, with neoplastic cells encircling a well-defined lumen (Figure 2-C). Cytoplasmic luminal polarization typical of Flexner-Wintersteiner (“retinoblastic”) rosettes was not apparent. In between the nests of primitive small round blue cells, the tumor showed histologic features of neural differentiation, namely neoplastic cells showing ganglionic features, with enlarged nuclei, prominent nucleoli, and visible perinuclear cytoplasm with Nissl substance. In these areas, the tumor cells lied amongst a background of neuropil (Figure 2-D). Immunohistochemical studies showed strong widespread synaptophysin immunoreactivity in both the primitive cells and the areas of neuropil formation. The NFP immunostain showed fibrillar staining in both the primitive and maturing areas. The Ki-67 immunostain revealed a variable labeling index, highest in the primitive areas (~90%), and lowest in the areas of ganglioneural maturation. A conspicuous finding in the resection material was the presence of numerous cells with features of rhabdomyoblastic differentiation, characterized by elongate, spindled cells with primitive nuclei and abundant eosinophilic cytoplasm. When viewed in cross sections, the cells show the typical rhabdoid morphology (globular eosinophilic cytoplasm with eccentrically-displaced nucleus). In longitudinal sections, the cells demonstrated elongate eosinophilic cytoplasm with prominent cross striations (Figure 3-A). The foci of rhadomyoblastic differentiation were present both within the primitive areas and the foci of neural maturation. By immunohistochemistry, the rhabdomyoblastic cells strongly express desmin and myogenin (Figure 3-B). These rhabdomyoblastic features were notably absent in the initial endoscopic biopsy specimen, reflecting the limited amount of tissue analyzed. Rare small clusters of small primitive cells contain aggregates of finely granular light-brown pigment; the pigment stains strongly with Fontana-Masson staining, and is negative on the iron stain, confirming melanin pigmentation (Figure 3-C). Although no frank cartilage formation was seen, foci showing an immature spindled and myxoid stromal proliferation are present, further evidencing divergent ectomesenchymal differentiation (Figure 3-D). Occasional large aggregates of dystrophic calcifications are randomly distributed. Necrosis or microvascular proliferation was not seen.
DISCUSSIONA variety of tumors may present in the pineal region, reflecting
the different types of native tissues that reside in the locale. Of these, tumors arising from the native neuroepithelial cell, pineocytes, are unique to this location. These “pineal parenchymal neoplasms” comprise pineocytomas, pineal parenchymal tumors of intermediate differentiation, pineoblastomas, and pineal anlage tumors. Pineocytomas are tumors that are most often encountered in young adults and contain well-differentiated tumor cells with eosinophilic cytoplasm and rosette formation. Pineal parenchymal tumors of intermediate differentiation
Figure 1 A: Pre-operative sagittal non-contrast T1-weighted brain MRI showing a hypo-intense pineal region mass. B: Pre-operative sagittal T1 weighted brain MRI with contrast showing a pineal region mass with heterogeneous contrast enhancement. C: Pre-operative axial FLAIR brain MRI showing enlargement of the lateral ventricles. D: Post-operative sagittal non-contrast T1-weighted brain MRI showing gross total resection of the pineal region mass.
Central
Ajayi et al. (2014)Email:
JSM Neurosurg Spine 2(4): 1035 (2014) 3/5
display a greater degree of differentiation and few mitotic figures than that seen in pineoblastomas, but less differentiation and a greater mitotic index than typical of a pineocytoma.Pineoblastomas are the most aggressive and primitive, and are seen most often in pediatric patients. Pathologically, pineoblastomas are characterized by sheets of malignant, primitive-appearing cells with hyperchromatic nuclei and scant perinuclear cytoplasm [5,6,9]. Pineal anlage tumors are extremely rare tumors of the pineal region that show combined features of a primitive neuroepithelial tumor and andectomesenchymal differentiation. Although not officially recognized as a stand-alone entity by the World Health Organization, pineal anlage tumors are described as variants of pineoblastomas with melanin, cartilaginous, and rhabdomyoblastic differentiation [5]. The neuroectodermal components present comprise neuronal, glial, and retinal elements; Homer-Wright pseudorosettes and Flexner-Wintersteiner rosettes may be seen.2Ectomesenchymal differentiation is typically manifested by the presence of rhabdomyoblasts, striated muscle fibers, and/or cartilage formation [7,9]. The name pineal anlage tumor derives from the histologic similarities to the pigmented neuroectodermal tumor of infancy, an extremely rare tumor of presumed neural crest origin that occurs in infants, typically in the maxilla. Due to the presence of primitive neuroectodermal components and melanin pigmentation, the tumor was previously thought to be of retinal origin, and was historically referred to as “retinal anlage tumor”, a diagnostic term no longer in routine use. Unlike the benign clinical course typical of pigmented neuroectodermal tumors of infancy, pineal anlage tumors often show a highly-aggressive clinical course, a variance that strongly suggests different underlying genetic aberrations [12].
Six cases of pineal anlage tumors have been previously documented in the literatures that are consistent with the original description by Schmidbauer [6-11]. The patient demographics, outcomes, and divergent pathologic features of these cases and the current case are summarized in Table 1. The patient ages ranged from four months to nine years old (mean 23 months), and the majority of cases occur in males; the current case is the second report of a retinal anlage tumor in a female patient. The tumors showed a variable degree of aggression: The shortest duration of survival was 5 months, and the longest duration of follow-up without disease recurrence was 12 months. The reported cases were treated with surgical resection, some with documented adjuvant chemotherapy. The current case is the only reported example of a pineal anlage tumor treated with autologous stem cell transplantation following induction chemotherapy. The pathologic features of the reported cases vary. In their report of the first described pineal anlage tumor, Schmidbauer and colleagues described a combination of primitive neuroepithelial and ectomesenchymal elements, comprising melanin production and rhabdomyoblastic differentiation. The subsequently described pineal anlage tumors have described similar pathologic findings. An additional pineal region tumor was described in 2005 by Gudinaviciene in which a tumor from 10-month-old male showed a mixture of mature neuroglial tissue, skeletal muscle, and pigmented epithelium [13]. Although these features were reminiscent of a pineal anlage tumor, the primitive neuroepithelial component was notably
Figure 2 A: H&E stained sections demonstrating a tumor with a variegated growth pattern, with sheets and ill-defined, variably sized nodules comprising a primitive small-round blue cell tumor. B: H&E stained sections showing tumor cells arranged in intimately admixedsheets and nests, with hypocellular areas lying amongst an eosinophilic fibrillar background. C: H&E stained sections showing numerous mitotic figures and apoptotic bodies in the primitive areas of the tumor; also seen are non-descript rosettes, with neoplastic cells encircling a well-defined lumen. 2D: H&E stained sections showing histologic features of neural differentiation: neoplastic cells with ganglionic features, including enlarged nuclei, prominent nucleoli, and visible perinuclear cytoplasm with Nissl substance.
Figure 3 A: The cells demonstrate the typical rhabdoid morphology (globular eosinophilic cytoplasm with eccentrically-displaced nucleus) and elongate eosinophilic cytoplasm with prominent cross striations. B: The rhabdomyoblastic cells strongly express desmin and myogenin. C: Rare small clusters of small primitive cells contain aggregates of finely granular light-brown pigment which stains strongly with Fontana-Masson staining, and is negative on the iron stain, confirming melanin pigmentation. D: Although no frank cartilage formation was seen, foci showing an immature spindled and myxoid stromal proliferation are present, further evidencing divergent ectomesenchymal differentiation.

Central
Ajayi et al. (2014)Email:
JSM Neurosurg Spine 2(4): 1035 (2014) 4/5
absent; only mature elements were seen. Thus, the described tumor is likely to show less aggressive clinical course, and should not be included amongst the other reports of more typical pineal anlage tumors.
Due to the extreme rarity of pineal anlage tumors, the prognosis and treatment are not well characterized. The aggressive clinical course followed by pineal anlage tumors mirrors that seen in many pineoblastomas. The prognosis of pineoblastomas is determined primarily by the extent of disease at diagnosis and extent of tumoral resection. Studies of pineal parenchymal neoplasms have associated histologic features of proliferation with biologic behavior; elevated MIB-1 labeling indices (a marker of proliferative activity) were associated with a poor prognosis and leptomeningeal dissemination [9].
Despite the unique histologic appearance, pineal anlage tumors lack characteristic radiologic features. Thus, the radiologic differential diagnoses typically encompass the entire spectrum of pineal region pathology. Pineal anlage tumors tend to be large in size (>4 cm), often with compression of the cerebral aqueduct and/or involvement of the tectalplate. On CT, these tumors are hyperdense in comparison to adjacent brain due to high cellularity, and may show dispersed foci of calcification. These tumors are usually iso-intense to hypo-intense to the adjacent brain parenchyma on T1-weighted MRI sequences, and iso-intense to adjacent brain on T2-weighted MRI. There is heterogeneous contrast enhancement and diffusion restriciction (due to high cellularity) on DWI and ADC. Central necrosis may also be seen, resembling other pineal tumors in terms of presentation and radiological appearance [6,14].
There are no unique clinical signs or symptoms that are characteristic of pineal anlage tumors. Similar to the clinical presentation of other tumors of the pineal region, pineal anlage tumors may be associated with hydrocephalus due to compression of the cerebral aqueduct and/or Parinaud’s syndrome due to compression of the tectal plate [6,15].
The pathologic differential for pineal anlage tumors is limited due to the unique histologic features. When a tumor of the pineal region with mixed primitive neuroectodermal and ectomesenchymal features is encountered, several entities besides retinal anlage tumor should be considered. A teratoma with primitive neuroectodermal component is distinguished by representation by all three germinal layers;
endodermal (e.g. enteric, respiratory) or cutaneous components typical of teratomas are lacking in pineal anlage tumors. Another strong consideration is medulloblastoma variants with divergent differentiation, i.e. medulloblastoma with myogenic differentiation and/or melanotic differentiation. In this case, the lack of cerebellar parenchymal involvement by neuroradiology or intraoperative observation militated against a medulloblastoma variant. In equivocal cases, ancillary molecular testing to evaluate for cytogenetic abnormalities suggestive of medulloblastoma (isochromosome 17q, MYC amplification) may be useful in establishing the pathologic diagnosis. Finally, an ectomesenchymoma is a consideration, due to the combination of rhabdomyoblastic and neural differentiation. However, ectomesenchymomas typically occur in the soft tissue and are considered rhabdomyosarcoma variants in which the neuroectodermal component is inconspicuous; there are no reports of ectomesenchymomas occurring in the pineal region [5,9].
In summary, pineal anlage tumors are rare tumors that occur in the pineal region of young children, most often male infants. The pre-surgical workup includes appropriate neuroimaging of the brain and spinal cord and cerebrospinal fluid examination to evaluate for leptomeningeal disease. Serum tumor markers are often performed to exclude germ cell neoplasia. Due to the lack of characteristic clinical or radiologic findings, tissue examination is required for diagnosis of pineal anlage tumors. Although the divergent ectomesenchymal pathologic features are often prominent and easily identifiable, retrieval of small tissue fragments at the time of initial biopsy may yield tissue that is not representative of the entire tumor. As seen in this case, this sampling artifact may lead to a diagnostic discrepancy between the initial biopsy and the definitive resection specimen. Thus, this case illustrates the need to retrieve as much tissue as possible at the time of biopsy to ensure accurate initial pathologic diagnosis. Despite the rarity of these tumors, pathologists who perform neuro-pathologic examination of brain biopsies should be aware of this entity, and include it in their pathologic differential diagnosis of pineal region tumors. Specific treatment modalities or protocols for pineal anlage tumors have not been established. As is the case with all pineal parenchymal neoplasms, surgical intervention is indicated, with the goal of gross total resection. Following surgery, most cases of pineal anlage tumors are treated on protocols designed for pineoblastomas and primitive
Report Age Sex Outcome Divergent Features
Schmidbauer et al, 1989 9 Y F Death after 5 months Melanin, skeletal muscle
Raisanen et al, 1990 1 Y M Unknown Melanin, skeletal muscle, cartilage
McGrogan et al, 1992 9 M M Death after 9 months; Melanin, cartilage
Berns et al, 2006 9 M M Unknown Melanin, cartilage
Olaye et al, 2010 5 M M > 12 months recurrence free survival, s/p five cycles chemotherapy Melanin, cartilage, skeletal muscle
Ahuja et al, 2011 4 M M Alive at 6 months, s/p four cycles of chemotherapy Melanin, cartilage
Current case 11 M FAlive without evidence of residual/recurrent disease at 6 months, s/p chemotherapy and autologous stem cell transplantation
Melanin, skeletal muscle, immature myxoid spindled stroma
Table 1: Clinical Characteristics, Outcome, and Divergent Pathologic Features of Pineal Anlage Tumors.

Central
Ajayi et al. (2014)Email:
JSM Neurosurg Spine 2(4): 1035 (2014) 5/5
neuroectodermal tumors, with combined chemotherapy and radiotherapy. Due to the adverse effects on the developing central nervous system, craniospinal radiotherapy is often withheld in patients without cerebrospinal fluid dissemination or tumoral recurrence following chemotherapy. High dose chemotherapy with autologous stem-cell rescue, performed in this case, may be a promising regimen in first adjuvant therapy to delay radiotherapy in infants and very young children [16]. At six months follow-up, our patient was alive and stable, without radiologic evidence of residual or recurrent disease.
REFERENCES1. Yamamoto I. Pineal region tumor: surgical anatomy and approach. J
Neurooncol. 2001; 54: 263-275.
2. Perry A, Brat D. Practical Surgical Neuropathology: A Diagnostic Approach. 1st edn. Churchhill Livingstone Elsevier. Philadelphina. 2010; 151-163.
3. Rejis J, Bouillot P, Rouby-Volot F, Figarella-Brander D, Dufour H, Peragut JC. Pineal Region Tumors and the Role of Stereotactic Biopsy: Review of the Mortality, Morbidity and Diagnostic Rates in 370 Cases. J Neurosurg. 1996; 39: 907-914.
4. Fuller GN, Scheithauer BW. The 2007 Revised World Health Organization (WHO) Classification of Tumours of the Central Nervous System: newly codified entities. Brain Pathol. 2007; 17: 304-307.
5. Louis D, Ohgaki H, Wiestler O, Cavenee W. World Health Organization Classification of Tumours of the Central Nervous System. 4th edn. Internation al Agency for Research on Cancer. Lyon. 2007.
6. Olaya JE, Raghavan R, Totaro L, Zouros A. Pineal anlage tumor in a
5-month-old boy. J Neurosurg Pediatr. 2010; 5: 636-640.
7. Schmidbauer M, Budka H, Pilz P. Neuroepithelial and ectomesenchymal differentiation in a primitive pineal tumor (“pineal anlage tumor”). Clin Neuropathol. 1989; 8: 7-10.
8. Ahuja A, Sharma MC, Suri V, Sarkar C, Sharma BS, Garg A. Pineal anlage tumour - a rare entity with divergent histology. J Clin Neurosci. 2011; 18: 811-813.
9. Berns S, Pearl G. Review of pineal anlage tumor with divergent histology. Arch Pathol Lab Med. 2006; 130: 1233-1235.
10. McGrogan G, Rivel J, Vital C, Guerin J. A pineal tumour with features of “pineal anlage tumour”. Acta Neurochir (Wien). 1992; 117: 73-77.
11. Raisanen J, Vogel H, Horoupian DS. Primitive pineal tumor with retinoblastomatous and retinal/ciliary epithelial differentiation: an immunohistochemical study. J Neurooncol. 1990; 9: 165-170.
12. Neville B, Damm D, Allen C, Bouquot J. Oral and Maxillofacial Pathology. 3rd edn. Saunders Elsevier. St. Louis. 2009; 533-535.
13. Gudinaviciene I, Pranys D, Zheng P, Kros JM. A 10-month-old boy with a large pineal tumor. Brain Pathol. 2005; 15: 263-264, 267.
14. Gasparetto EL, Cruz Jr LC, Doring TM, Araújo B, Dantas MA, Chimelli L, et al. Diffusion-weighted MR images and pineoblastoma: diagnosis and follow-up. Arq Neuropsiquiatr. 2008; 66: 64-68.
15. Donat JF, Okazaki H, Gomez MR, Reagan TJ, Baker HL Jr, Laws ER Jr. Pineal tumors. A 53-year experience. Arch Neurol. 1978; 35: 736-740.
16. Gururangan S, McLaughlin C, Quinn J, Rich J, Reardon D, Halperin EC, et al. High-dose chemotherapy with autologous stem-cell rescue in children and adults with newly diagnosed pineoblastomas. J Clin Oncol. 2003; 21: 2187-2191.
Ajayi O, Palma A, Sadanand V, Deisch J (2014) Pineal Anlage Tumor: Case Report and Review of Literature. JSM Neurosurg Spine 2(4): 1035.
Cite this article